nps 1960, usa to provide primary health care in...
TRANSCRIPT

NPs 1960, USA to provide primary health care in under
resourced/disadvantaged communities. Loretta Ford and
Henry silver
(Walsh, Crumbie and Revely 2003)
Western Australia
1997, investigation (Judge Antoinette Kennedy) into the role of remote area nurses recognised many were working outside their scope of practice.
Implementing the NP role could legitimise those activities
Change in political climate= desire to expand the role

Supported by the AGPC report on the Australian health
care workforce Australian Government Productivity Commission (2005) Australia’s Health Workforce Position
Paper Canberra: Productivity Commission
Despite the support many challenges
› Medical resistance
› Pharmacology and prescribing resistance and law
changes
› Accredited courses
› Designation
“A Nurse Practitioner is a registered nurse educated to function in an advanced clinical role.
The scope of practice of the Nurse Practitioner will be determined by the context in which the Nurse Practitioner is authorised to practice and will include legislative authority not current within the scope of nursing practice”
National Nursing Organisation 2000

Dynamic practice that incorporates application of
high-level knowledge and skills in extended
practice across stable, unpredictable and
complex situations.
Advanced comprehensive health assessments
High level of clinical proficiency in procedures,
treatments and interventions
Extended practice competencies
Professional efficiency whereby practice is structured in a
nursing model and enhanced by autonomy &
accountability.
Established therapeutic links
Applies extended practice competencies

Clinical leadership that influences & progresses clinical care,
policy & collaboration through levels of health service
Engages in, and leads clinical collaboration that
optimises outcomes for patients /clients and
communities

Nurses Act 1992, Nurses Amendment Act 2003
Medical Act 1984
Misuse of Drug Act 1981
Pharmacy Act 1964
Poisons Act 1964
Radiation Safety Act 1975
Road Traffic Act 1974
Registration (AHPRA)- Endorsed
Nurse Practitioner Code of Practice
Designation of Practice Area (Director General or Department of Health)
Clinical Protocols
Drug formulary
Monitoring and evaluation

Enrolled Nurse
Registered Nurse
Clinical Nurse
School Teacher
Clinical Nurse Specialist
Nurse Practitioner

Bachelor of Nursing
Post Graduate Studies
Orthopaedic Certificate
Graduate Diploma Education
Graduate Diploma in Clinical Nursing
Master of Nursing (Nurse Practitioner) Flinders South Australia/ECU
Identifying the need-clinical expertise Increasing complexity of the patients
Increasing presentations, admissions,
support of orthopaedic patients in outlying areas
(ICU, NOSA, General wards, ED)
increasing needs of the community-early
discharge
A business case

Role • Coordinates the clinical management of all minimal trauma fractures
• Mx. complex acute medical conditions/co-morbidities timely manners
Peri-operative management optimising pt. condition
Maintaining consistent and comprehensive approach
Encouraging compliance/education #hip pathway
Facilitates discharge planning
Enhance rehabilitation outcomes
› Cost effective- Reducing length of stay

Peri-operative Mx › Pre and post op x-rays/bloods/ECG/Fluid
Mx/Transfusions/Benzodiazepine withdrawal nicotine, insulin infusion, prophylactic AB’s
Pain Mx
VTE prophylaxis
UTI
Constipation
Nausea and vomiting
Osteoporosis

Scope Outcomes
Nurse Practitioner All medically stable orthopaedic patients requiring surgery. All medically stable minimal trauma patients
being conservatively managed.
Identify patients suitable for Ortho NP CPG
MEDICAL PRACTITIONER +/- Nurse
Practitioner
Exclusion Criteria Complex orthopaedic patients (e.g. multi-trauma
patients) Medically unstable orthopaedic patients Palliative Intent
Identify patients not suitable for Ortho NP CPG→ exit CPG refer orthopaedic +/- Orthogeriatric team
ASSESSMENT & INTERVENTION
Primary Survey Airway Breathing
Circulation
Identify patients not suitable for Ortho NP CPG→ exit CPG refer orthopaedic
+/- Orthogeriatric team

Scope Outcomes
History Presenting injury/condition Planned orthopaedic surgical interventions Risk factors1
As per Risk Ax Tools (VTE/Falls/Pressure areas,
withdrawal drug/alcohol) Relevant past medical history medication use (including anticoagulants/anti-platelets) Renal function Weight
Allergies
Identify patients not suitable for Ortho NP CPG→ exit CPG refer orthopaedic +/- Orthogeriatric team
Focused clinical assessment
Haemodynamically stable Trauma injuries- open wounds Fracture type
Potential compartment syndrome Muscular skeletal examination General examination Vital signs
Differential diagnosis→ exit CPG refer to Orthopaedic +/- Orthogeriatric Team.

Scope Outcomes
Working diagnosis and Investigations
Imaging X-ray suspected fracture Pelvic X-ray (suspected hip #) Chest X-ray Post-op X-ray
Abdominal X-ray (Constipation protocol) Bone densitometry (DXA) (OP protocol)
Differential diagnosis→ exit CPG refer to Orthopaedic +/- Orthogeriatric Team. Routine pre and Post-op x-rays Facilitate early diagnosis and rehab goals (post –op)

Scope Outcomes
Pathology Laboratory Test Clinical biochemistry tests Blood glucose Serum urea and electrolytes Serum calcium
Cardiac markers Thyroid function test LFTs: alanine transferase (ALT), gamma glutamyl transpeptidase (GGT), alkaline phosphate (AP), bilirubin and albumin Therapeutic drug monitoring -digoxin Haematology test
Full blood count Coagulation profile Erythrocyte sedimentation rate and C-reactive protein Blood transfusion testing Blood group, antibody screen and crossmatch (as
per routine pre-op and post-op guidelines Microbiology Urine microscopy, culture and sensitivity Blood Cultures Osteoporosis Bloods Ca, Vitamin D, LFT, Creatinine/eGFR, PTH, TFT
Identification of abnormalities and initiate treatment refer to Orthopaedic +/- Orthogeriatric Team. Implement
VTE Risk assessment and Mx Therapeutic Mx as per anticoagulation chart Transfusion protocol Ab’s as per UTI protocol
OP medications as per OP protocol
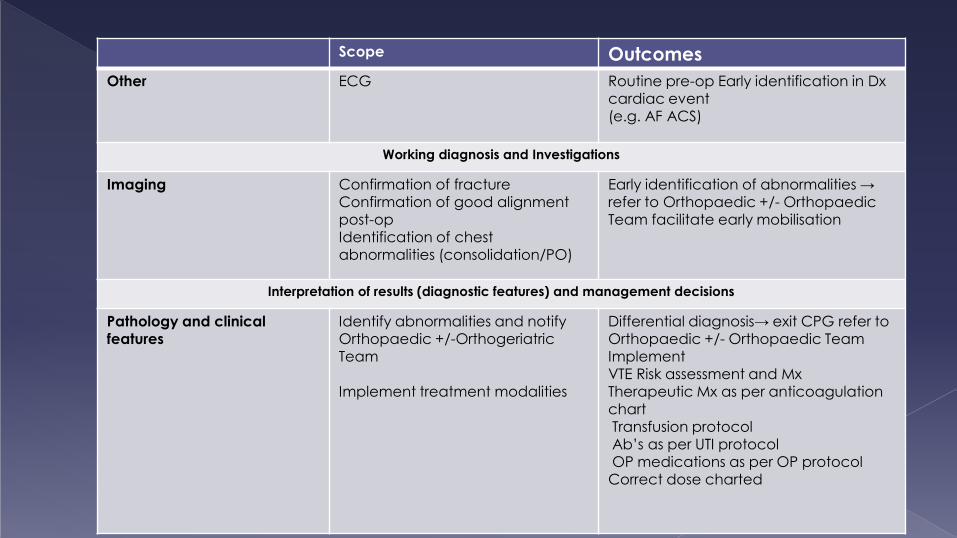
Scope Outcomes
Other ECG Routine pre-op Early identification in Dx cardiac event (e.g. AF ACS)
Working diagnosis and Investigations
Imaging Confirmation of fracture Confirmation of good alignment post-op
Identification of chest abnormalities (consolidation/PO)
Early identification of abnormalities → refer to Orthopaedic +/- Orthopaedic Team facilitate early mobilisation
Interpretation of results (diagnostic features) and management decisions
Pathology and clinical features
Identify abnormalities and notify Orthopaedic +/-Orthogeriatric Team Implement treatment modalities
Differential diagnosis→ exit CPG refer to Orthopaedic +/- Orthopaedic Team Implement VTE Risk assessment and Mx Therapeutic Mx as per anticoagulation
chart Transfusion protocol Ab’s as per UTI protocol OP medications as per OP protocol Correct dose charted

Scope Outcomes
Associated Care Patient education/family education Pre and Post –op care Discharge planning Rehabilitation goals and referral to rehab
facilities OP education and referral
Identify patients not suitable for Ortho NP CPG→ exit CPG refer orthopaedic +/- Orthogeriatric team
Acute Referral Referral to Orthopaedic +/- Orthogeriatric Team Duty Anaesthetist APS
Interpreter Allied Health
Prompt referral Improved pain management Early identification of D/C Requirements for rehab
Referrals As appropriate to allied health team members Referrals may be made for specific patient problems or as required to
-HITH - Interpreter -Pharmacist -- Physiotherapist - Occupational therapist -Social work - Aboriginal liaison officer
-Drug and alcohol counsellor

Medications
Analgesia
Antibiotics Antacid Anti-emetics
Aperients Antifungal
As per NP Pain management protocol
As per UTI protocol As per orthopaedic surgical prophylaxis (IV cephazolin/ mupirocin) Mylanta As per nausea and vomiting protocol
As per constipation protocol Fluconazole (oral) Nystatin (Nilstat) Oral Clotrimazole (Canestin Cream) (topical)
Assist in effective pain relief
Prompt treatment of infections identified Improve compliance with prophylactic protocol Relief of indigestion Assist in effective nausea and pain management Prevent and treat constipation
Treatment of simple Candida infections (throat and vagina)

Medications
Benzodiazepine
Drugs for eye infections Intravenous Fluids Nicotine
Diazepam (As per drug/alcohol
withdrawal chart, Benzodiazepine withdrawal chart, Amphetamine withdrawal Chart, Cannabis Withdrawal chart) Chloramphenicol 1% ointment Chloramphenicol 0.5% eye drops
Normal Saline Red blood cells
As per SCGH Withdrawal guidelines and nicotine Dependency Assessment
Assist in management of reducing
withdrawal symptoms Treatment of conjunctivitis and
simple eye infections common to the elderly patient Assist in maintaining hydration Assist in treating hypovolaemia as per orthopaedic transfusion
protocol Encourage cessation of smoking whilst undergoing surgery. Reduce the incidence of aggression related to withdrawal

Medications
Osteoporosis
VTE prophylaxis protocol
As per OP protocol
As per Risk Assessment Tool for
Venous Thromboembolism (VTE) and Department of
Orthopaedics VTE Prophylaxis (Jan 2011)
Assist in improving initiation of OP
treatment and prevention Reduce incidence of VTE Improve compliance of risk assessment and prophylactic administration
References
A guide for assessing older people in hospitals(2004) Developed by the Centre for Applied Gerontology, Bundoora Extended Care Centre, Northern Health. Commissioned on behalf of the Australian Health Ministers’ Advisory Council (AHMAC) by the AHMAC Care of Older Australian Working Group. Australian Medicine Handbook Pty. Ltd. July 2011 Best practice approaches to minimise functional decline in the older person across the acute, sub-acute and residential aged care settings: Update 2007 Best practice approaches to minimise functional decline in the older person across the acute, sub-acute and residential aged care settings (2004) British Orthopaedic Association (2007) The Care of Patients with Fragility Fracture Brown, A.F.T and Cadogan, M.D. 2006. Emergency Medicine emergency and Acute Medicine: Diagnosis and Management (5th. Ed), Hodder Arnold, London. Dandy, D., Edwards. D. Essential Orthopaedics and Trauma 3rd. Ed (1998) eTG Complete Therapeutic Guidelines 2011 (http://online.tg.org.au.qelibresources.health.wa.gov.au/ip/) Management of hip fracture in older people. A national clinical guideline (2009) Scottish Intercollegiate Guideline Network. MIMS Online 2011 SCGH Withdrawal Guidelines and Nicotine Dependency Assessment SCGH Alcohol Withdrawal Chart SCGH Amphetamine Withdrawal Chart SCGH Benzodiazepine Withdrawal Chart SCGH Cannabis Withdrawal Chart
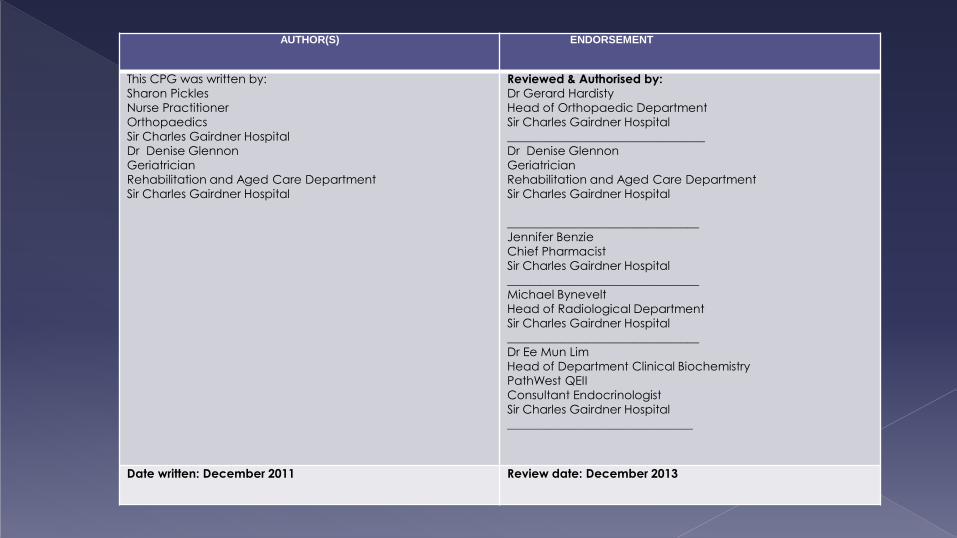
AUTHOR(S) ENDORSEMENT
This CPG was written by: Sharon Pickles
Nurse Practitioner
Orthopaedics
Sir Charles Gairdner Hospital
Dr Denise Glennon
Geriatrician
Rehabilitation and Aged Care Department
Sir Charles Gairdner Hospital
Reviewed & Authorised by: Dr Gerard Hardisty
Head of Orthopaedic Department
Sir Charles Gairdner Hospital
_________________________________
Dr Denise Glennon
Geriatrician
Rehabilitation and Aged Care Department
Sir Charles Gairdner Hospital
________________________________
Jennifer Benzie
Chief Pharmacist
Sir Charles Gairdner Hospital
________________________________
Michael Bynevelt
Head of Radiological Department Sir Charles Gairdner Hospital
________________________________
Dr Ee Mun Lim
Head of Department Clinical Biochemistry
PathWest QEII
Consultant Endocrinologist
Sir Charles Gairdner Hospital
_______________________________
Date written: December 2011 Review date: December 2013

Analgesics
Aspirin Tablet
Buprenorphine Transdermal Patch (Norspan)
(5mcg, 10mcg)
Buprenorphine sublingual immediate release (200mcg-400mcg) (As per
APS)
Hydromorphone HCL prolonged- release tablet (Jurnista PR) 4mg
Hydromorphone immediate release tablet
(0.5mg-4mg)
Oxycodone hydrochloride controlled release tablet (Oxycontin- 5mg,
10mg)
Oxycodone hydrochloride immediate release tablet/capsule (Endone
IR/Oxynorm 2-5-10mg)
Oxycodone hydrochloride liquid (1mg-10mg)
Oxycodone hydrochloride & Naloxone hydrochloride dihydrate
controlled release tablet (Targin CR)
(5/2.5, 10/5mg)
Paracetamol PO/PR/IV
Paracetamol Osteo (665mg)
Paracetamol /Codeine Tablet (500mg/8mg) (Panadeine)
Paracetamol/Codeine (500mg/30mg)
(Panadeine Forte Tablet)
Tramadol PO/IV (50mg-100mg)
Antacids Mylanta Aperients Bisocodyl tablets/suppository
Benefibre Coloxyl and Senna Epson salts Fleet enema Glycerine suppository Microlax enema Movicol
Picoprep Sorbitol

Antibacterials
Amoxycillin Amoxycillin with clavulanic acid Flucloxacillin Phenoxymethylpenicillin (penicillin V) Cephalexin Cephazolin Doxycycline Roxithromycin Metronidazole Trimethoprim Mupirocin ointment/cream (*As part of Hip pathway and all orthopaedic metal work implantation)
Antiemetic Metoclopromide hydrochloride Ondansetron Prochlorperazine
Antifungal
Fluconazole (oral) Nilstat (oral) Canestin Cream (Topical) Benzodiazepines Diazepam (as per withdrawal protocols) Drugs for eye infections Chloramphenicol ointment Chloramphenicol eye drops
IV Fluids Normal Saline 5% Dextrose Red Blood Cells (Transfusion as per Orthopaedic Transfusion Protocol)

Insulin Actrapid (as per fasting protocol) Patient’s usual insulin dose
NSAIDS Diclofenac Ibuprofen Indomethacin Naproxen
Osteoporosis Medications Vitamin D Cholecalciferol 25mcg
Vit D2, D3 Calcitriol Calcium Supplements Calcium Carbonate 600mg Calcium Citrate 500mg Bisphosphonates
Alendronate (patient’s usual meds) Fosamax (patient’s usual meds) Strontium(patient’s usual meds) Actonel Combi D (patient’s usual meds)
Pre admission clinics
Anaemia management
Outpatient clinics
Fragile bone clinic- Management of OP
Falls Clinic
Private consultant rooms

Funded until 2014
Annual report
Justify cost saving benefits
Justify clinical needs
Patient outcomes
