nursing care of patients with hepatobiliary disorders c. cummings rn, edd
TRANSCRIPT

Nursing Care of Patients with Hepatobiliary Disorders
C. Cummings RN, EdD.

Anatomy
Liver
Pancreas
Duodenum
Gall Bladder
Common Bile Duct
Hepatic Duct
Sphincter of Oddi
Cystic Duct
Diaphragm

Pancreas
• Exocrine- 80% of organ, acinar cells with digestive enzymes:– What are they?
• Endocrine- islets of langerhans – Alpha cells- ?– Beta cells- ?

Acute Pancreatitis
• Cause:– Pancreatic enzymes destroy ductal tissue and cancreatic
cells autodigestion and fibrosis– Can be life threatening– NHP- necrotizing hemorrhagic pancreatitis
• 20%, diffuse bleeding– Enzymes are activated before they reach the duodenum– Toxic injury to pancreatic cells

Four major physiologic processes
• Lipolysis– Caused by lipase, release fatty acids and combine
with I Ca causes?– Proteolysis– Caused by trypsin, splits proteins into smaller
polypeptides what??

Four major physiologic processes
• Necrosis of the Blood Vessels– Caused by elastase, elastic fibers of the blood vessels and
ducts dissolve what?– Kallikrein releases vasoactive peptides, bradykinin and
kinin what? and increased ?• Inflammation
– Leukocytes form around hemorrhagic and necrotic areas pus, abcess formation and if walled off pancreatic what??
Why does enzyme activation occur?
• Bile Reflux- obstruction of CBD• Hypersecretion-obstruction theory- pancreatic duct
ruptures • Alcohol induced changes- stimulates hydrochloric
acid and secretin production exocrine functions, also causes edema of the duodenum and ampulla of Vater, this obstructs flow, may also decrease tone at sphincter of Oddi and cause duodenal reflux

Other causes
Besides alcohol ingestion and biliary disorders, can also be caused by: Trauma- blunt or surgical (whipple/ ERCP) Pancreatic obstruction- such as? Metabolic disturbances- hyperlipidemia,
hyperparathyroid Renal failure or transplant Ulcers that lead to peritonitis Coxsackievirus B infections Drug toxicities- such as?

Complications
• Pancreatic infection• Peritonitis• Hypovolemia• Hemorrhage• ARF• Paralytic ileus• Septic Shock• What are other
complications??

Symptoms of Acute Pancreatitis
• What is predominant symptom?
• Where is it?• When is it worse?• Jaundice• Cullen’s sign- what is that?• Turner’s sign- and that?
• Bowel sounds may be decreased or absent
• Abdominal tenderness• Watch for signs of shock• Respiratory effusions/ SOB• Assess for excessive alcohol
intake

Turner’s sign
Laboratory Diagnoses• Elevated Serum
– What are major enzymes?– Trypsin– Elastase
• Also, increased serum– Glucose– Bilirubin– Alanine aminotransferase– Leukocyte count
• Decreased– Calcium and magnesium

Diagnoses for Acute Pancreatitis
• What are two primary nursing diagnoses?• Nausea• Risk for fluid volume deficit• Risk for infection• Risk for ineffective breathing pattern• Risk for activity and sleep disturbances

Collaborative Diagnoses
• What are two potential nursing diagnoses?• Potential for Hypovolemic or Septic Shock• Potential for ARDS• Potential for Paralytic Ileus• Potential for MOSF

Nursing Interventions
• Acute Pain • What is primary method to relieve pain, other than medication?
• IV fluids for hydration• Replacement of Ca and Mg• NG drainage and suction• Assess for return of bowel
sounds and pain control

Pain Control• Opiods, IV and PCA• Demerol for relief of spasms
at the sphincter of Oddi, but it has problems with breakdown and is rarely used now
• Fentanyl patch• Epidural morphine with
bipivacaine• Pain may last how long?

Other management of pain
• Anticholinergics, atropine, glucagon, calcitonin, histamine receptor antagonists (Zantac), protease inhibitors are used for what?
• Antibiotics– Ceftazidime, cefuroxime, imipenem (Primaxin)

Other Management of PainSurgery
ERCP (endoscopic retrograde cholangiopancreatography)- used to open sphincter
Pseudocystojejunostomy or Pseudocystogastrotomy to drain abcess or pseudocyst
JP drains or sump tubes may be used for excessive drainage

ERCP

ERCP

Imbalanced nutrition: less than body requirements
• Maintain on NPO, may have NGT• May not eat for 7-10 days• Receive nutritional support through what?• Begin back on what kind of diet? What should
they not take in?• Diet teaching and teaching on signs of chronic
progression should be stressed with the patient

Chronic Pancreatitis• Usually develops after repeated episodes of acute
pancreatitis• What is the most common cause?• Types:
– Chronic Calcifying Pancreatitis- alcohol induced, proteins plug the ducts
– lead to atrophy and dilation – ulceration and inflammation – fibrosis, intraductal calification and cystic sacs
develop– Hard, firm organ with pancreatic insufficiency

Chronic Pancreatitis
• Type– Chronic Obstructive Pancreatitis
• Inflammation, spasm and obstruction of the sphincter of Oddi
• Inflammation and sclerotic lesions occur at the head of the pancreas obstruction and backflow of secretion

Chronic Pancreatitis with pseudocysts

Results
• Loss of exocrine function:– Aqueous bicarbonate- neutralizes duodenal
contents – Pancreatic enzymes- what do they do?– Enzyme secretion is reduced by 80%
steatorrhea, what do the stools look like?– Fat malabsorption wt loss and muscle wasting
and edema r/t loss of albumin

Results
• Pancreatic endocrine dysfunction causes what disease?
• May also have pulmonary complications from edema and pancreatic ascites
• ARDS may develop• Chronic pancreatitis is a major risk factor for
pancreatic cancer

Symptoms of Chronic Pancreatitis• Intense abdominal pain and tenderness• Ascites• What type of stools?• Respiratory compromise• Wt loss or gain?• Jaundice• What does the urine look like? Why?• Signs of diabetes• Elevated lipase and amylase• Elevated bilirubin, alkaline phosphatase and glucose• Definitive dx- by biopsy to look for calcification

Nursing Management
• Manage pain- how?• Enzyme replacement- dietary supplements,
pancrease, viokase, cotazyme, donnazyme- take before or during meals, take according to number of stools/day and wipe lips after
• Insulin therapy• NPO or TPN for days, then what kind of diet?• Histamine receptor blockers to decrease acid• Octreotide (Sandostatin) like somatostatin may be
used for diarrhea to slow motility

Health teaching
• Surgery is not an option, unless there is a cyst, obstruction or possible transplant for diabetes
• Diet and alcohol avoidance is stressed• Medication compliance with insulin,
pancreatic enzymes• Skin care for irritation r/t steatorrhea• What should the patient monitor?

Case Study
• 44 year old female admitted with abdominal pain, nausea and vomiting. She states that she has a lot of gas pain that wakes her up in the night.
• What do you suspect?

Case Study
• What are the symptoms of GB disease?• What can precipitate it?• What is the treatment?• How can you prepare her for surgery? How do
you decide between laparoscopic and open?• What needs to be done postop?

Case Study
• What structures are located in the RUQ of the abdomen?
• Which of the above organs are palpable in the RUQ?
• Given the patient’s diagnosis, what lab values would be important to evaluate?
• List 4 preop preparations that to be done.
Case Study
• The patient undergoes a laproscopic cholecystectomy, why is a T-tube inserted?
• What type of postoperative care would be required?
• The patient is sent home with the T-tube, what care would be appropriate?
• What type of diet should they be on?

Case Study
• The patient is medicated with Morphine and the pain has decreased from 10-4 in 1 hour, what else could be done for his pain?
• What data charted in the assessment is consistent with common bile duct obstruction?
• The patient spikes a temp of 38.6, a CXR is ordered and the patient is started on an antibiotic, imipenem. What should be done before the antibiotic is started?

Case Study
• She is ready for discharge
• What type of teaching is needed?
• What should be avoided, what about care of the T-tube?

Cholecystectomy
• Removal of the Gallbladder• Can be done open or laproscopic• Signs are nausea, vomiting, abdominal pain• Risk Factors:
– Fat, Female, Forty and Fertile– lap cholecystectomy
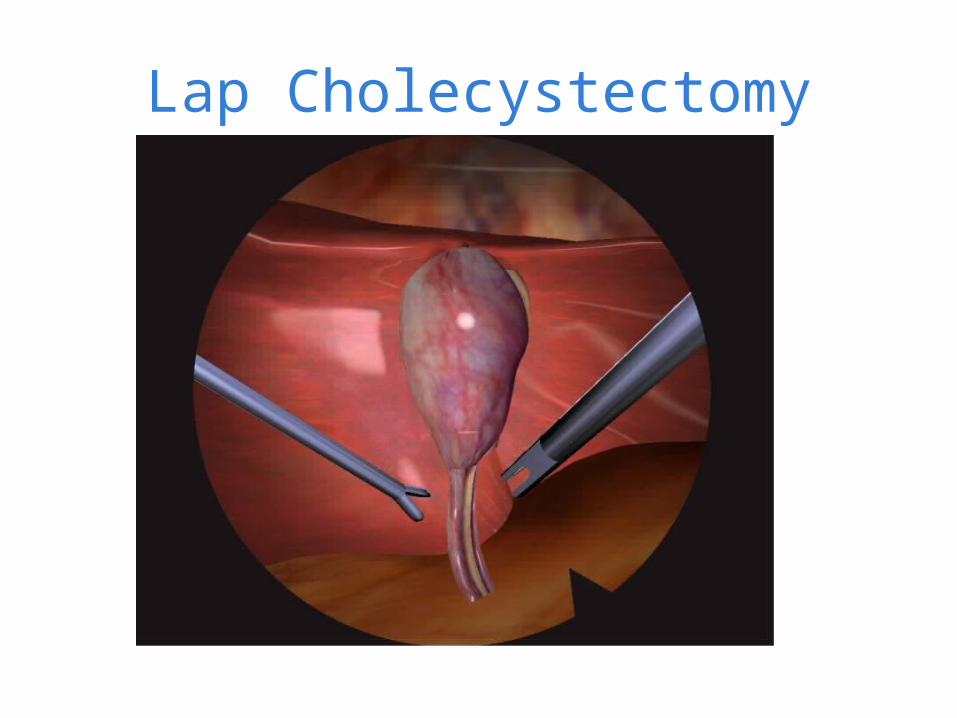
Lap Cholecystectomy

T-tube

Post-operative Care
• Pain control- demerol or PCA• NPO until bowel sounds return, then clear
liquids to DAT• Diet depends on what patient can tolerate• T-tube may remain in for 1-6 weeks
– Monitor drainage, should be bile colored– Less than 1000ml/day– Never irrigate, aspirate or clamp a T-tube without
an MD order

Disorders of the Liver
• Largest organ in the body and is located in the RUQ
• Large right lobe and smaller left lobe
• Made up of lobules• Bile is made in hepatocytes,
secreted into bile canaliculi• Receives 1500 ml of
blood/min

Liver Functions 400 functions Storage:
What types of vitamins and minerals?
Protective: Kupfer cells, phagocytic,
destroy bacteria, anemic RBC’s
Detoxifies what?
Metabolism: Makes proteins, for
what? Breaks down amino acids
to remove ammonia, converted to what?
Synthesizes plasma proteins, albumin, prothrombin and fibrinogen
Stores and releases glycogen
Breaks down and stores fatty acids and triglycerides
Forms and secretes what substance?

Liver Disorders
• Cirrhosis/ Liver Failure
• Hepatitis

Case Study
53 year old male admitted to the ED with abdominal pain, nausea and vomiting, weight loss. His abdomen is large and tender. His skin is light yellow. He has a fruity odor to his breath.
What do you suspect?

Case Study
• What lab work should be done?• What interventions would you perform and
why?• Your patient becomes belligerent after a few
hours and wants to leave, what would you do?• What radiology studies may be done?

Case Study
• His liver enzymes are extremely elevated and he is becoming confused. He is admitted to the floor.
• What symptoms are you likely to see in this patient?
• He starts to vomit blood, what does this mean and what may be done?
• What medications may be given to this patient?

Case Study
• He has improved and is now ready for discharge.
• What kind of teaching would this patient need?
• What should be done about rehab?

Cirrhosis
• Scarring of the liver, caused by a chronic, irreversible reaction to hepatic inflammation and necrosis
• Causes:– #1 cause?– #2 cause?
• Destruction of hepatocytes, tissue becomes nodular, block bile ducts and blood flow from fibrous connective tissue
• Liver begins enlarged and then shrinks

Cirrhosis
Complications• Compensated and Decompensated Cirrhosis• Liver failure
– Portal hypertension, what is this?– Ascites, why?– Bleeding esophageal varices– Coagulation defects, why?– Jaundice, what causes this?– Portal systemic encephalopathy and coma– Hepatorenal syndrome– Bacterial peritonitis

Liver Dysfunction
PSE Esophageal Varices
Bleeding
Jaundice
Hepatorenal Syndrome
Ascites
Bacterial Peritonitis

Portal Hypertension
• Increase in pressure within the portal vein• Increased resistance or blockage in the flow of blood
through the portal vein• Seeks collateral circulation • Blood flows back into the spleen, causing
splenomegaly• What veins become dilated?• Can lead to esphageal varices, caput medusa (what is
that??) and hemorroids

Ascites• Accumulation of free fluid within the peritoneal cavity• Increased hydrostatic pressure from the portal hypertension
causes fluid to leak into cavity• Albumin accumulates in peritoneal fluid and this reduces the
circulating proteins, this decreases serum colloid osmotic pressure and can lead to a decrease in what?
• Decrease in intravascular circulation causes renal vasoconstriction, triggers the renin-angiotensin system. This causes Na and water retention, which does what to fluid hydrostatic pressure and fluid volume?, where does the fluid accumulate?

Ascites

Bleeding esophageal varices• Blood backs up from liver into esophageal and gastric
vessels• Increased pressure, causes esophageal vessels to become
fragile and distended• Life threatening emergency, significant blood loss and this
can lead to what?• Bleeding is manifested as hematemesis and melena, what
does that mean?• Any activity that increases abdominal pressure can lead to
bleeding, such as what?• Also, then to have portal hypertensive gastropathy, this
leads to slow GI bleeds and cause chronic anemia

Coagulation defects
• Decrease in the synthesis of bile, this prevents the absorption of fat-soluble vitamins and clotting factors are not produced
• What fat soluble vitamin is predominant in clotting?• What lab values would be abnormal?• Splenomegaly results from the backup of blood, this
destroys platelets and leads to thrombocytopenia, one of earliest signs of liver dysfunction

Jaundice
• Hepatocellular disease and intrahepatic obstruction are the cause
• Liver cells can not excrete bilirubin, what are the liver cells called?
• Excessive circulating bilirubin• Obstruction jaundice is from edema, fibrosis and
scarring that block bile ducts• Excess bilirubin causes the skin to become yellow
gold, sclera are yellow and skin is pruritic and “frosty”

Portal system encephalopathy
• PSE or hepatic coma in later stages• Altered level of consciousness, impaired thinking and
neuromuscular disorders• Can reverse the encephalopathy with early
intervention• Liver is unable to detoxify substances and ammonia
is most common cause• Some encephalopathy may occur without elevated
ammonia, may be other toxins

Portal systemic encephalopathy Factors that may precipitate:
High-protein diet Infections Hypovolemia Hypokalemia Constipation GI bleeding, large protein load in intestines Drugs, such as hypnotics, opioids, sedatives, analgesics
and diuretics Paracentesis or shunting of veins may also cause Why does protein increase encephalopathy??

Stages of encephalopathy• Prodromal
– Personality changes, agitation, emotional lability, impaired thinking, fatigue, slurred speech, inability to concentrate
• Impending– Mental confusion, disoriented to person, place and time,
asterixis (liver flap) how do you test for this?• Stuporous
– Drowsy, but arousable, muscle twitching, hyperreflexia, abnormal EEG
• Comatose– Unresponsive, 85% lead to death, obtunded, response to
pain, no asterixis, positive babinski, muscle rigidity, fetor hepaticus, seizures, why seizures?

Hepatorenal syndrome
• Often cause of death• Sudden decrease in urinary flow• Elevated BUN and Creatinine levels and
decreased urine sodium excretion• Increased urine osmolarity, what is that?• Why is there a decrease in fluid volume to the
kidneys?

Bacterial Peritonitis
• Occurs spontaneously• Low concentrations of what type of proteins, that
protect against bacteria, cause this?• Bacteria are from the bowel and reach the ascitic
fluid when they are pulled through the bowel wall, what type of pressure would cause this?
• Symptoms are: fever, chills, abdominal pain and tenderness
• Diagnosis is made by culture of ascitic fluid and leukocyte count

Causes of Cirrhosis
• Alcoholic hepatitis- if alcohol intake is stopped, liver damage will reverse, if not, cellular necrosis continues. It may take years to develop
• Viral Hepatitis- C is most common, but B may also affect. It causes inflammation and cell damage
• Autoimmune hepatitis- autoantibodies• Steatohepatitis- “fatty liver” fat and cholesterol deposits
occur over time, cause is obesity and elevated lipids• Drugs and toxins- medications, such as illegal drug use,
chemotherapy, tylenol !• Biliary disease- primary biliary cirrhosis and primary
sclerosing cholangitis• Metabolic- hematochromatosis, what is that?, Alpha-
antitrypsin deficiency and cystic fibrosis, why?
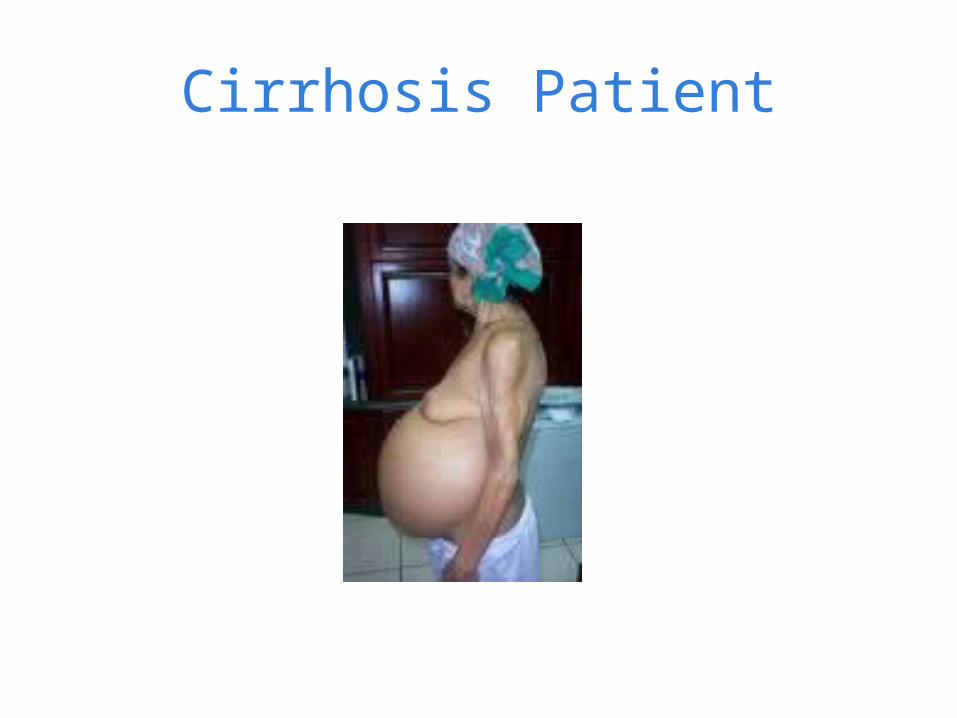
Cirrhosis Patient

Physical Manifestations
• Fatigue• Change in wt• GI symptoms• Abdominal pain and
tenderness• Pruritis• Jaundice and icterus (what’s
that?)• Dry skin and rashes• Petechiae and ecchymosis,
why?• Vascular lesions, “spider
angiomas” on nose, checks, shoulders
• Dependent edema

Physical manifestations
• Ascites, can lead to disruption in what major function?
• Tested by fluid wave, what is that?• How do you test for hepatomegaly?• Why would you measure abdominal girth?• Melena and fetor hepaticus may also be present,
what does this mean?• Amenorrhea, testicular atrophy and gynecomastia
may also occur because of inactive hormones that are normally made in the liver

Fluid Wave

Lab tests
Elevated values are: AST ALT LDH Alkaline phosphatase Bilirubin in serum and
urine Total protein Serum globulin
(immune response to liver disease)
Ammonia Prothrombin time
Decreased values are: Fecal urobilinogen Total protein (in chronic
disease) Serum albumin
Other assessments
• CT scan, Ultrasound of liver• Liver Biopsy, how is this done and what
precautions should be taken?• EGD- what does this mean and why would this
be done, what are they looking for?

Liver Biopsy

Nursing Diagnoses
• #1 is related to fluid volume, would it be excess or deficit fluid volume, what is it related to?
• What are two potential problems?• What collaborative problems are these
patients at risk for? (there are at least 7 or 8)
Nursing Management of Excess Fluid Volume
• Diet Therapy– Low Na diet, 500 to 2 gm/day– IV and oral fluid is restricted to 1-1.5 L/day– Vitamin supplements, thiamine, folate may be needed
• Drug Therapy– Diuretics, what are some?– What should you monitor for?– What electrolyte is affected by diuretics?– Antibiotics to prevent bacterial peritonitis

Management of Excess Fluid Volume
• Paracentesis– MD inserts a catheter into the abdomen to
remove and drain ascitic fluid– Should void first, HOB is elevated– Should monitor vital signs and drain slowly, why?– Cultures may be sent– What blood product may be given prior to
removing ascites fluid?

Paracentesis

Other measures
• Comfort:– Keep HOB elevated, use creams for pruritis– Monitor lung sounds and give O2 if needed– Monitor fluid and electrolyte levels
• Surgical:– Peritoneovenous shunt- catheter and one way valve to let fluid
flow from abdomen to superior vena cava, can have clots and infection
– Portacaval shunt- diverts blood from the liver to the kidney or inferior vena cava
– TIPS- transjugular intrahepatic portal-systemic shunt, track is made between the portal vein, hepatic veins and systemic circulation. The shunts are kept open with stents that are inserted and this increases the systemic circulation and decreases the portal hypertension

Peritoneal-venous Shunt
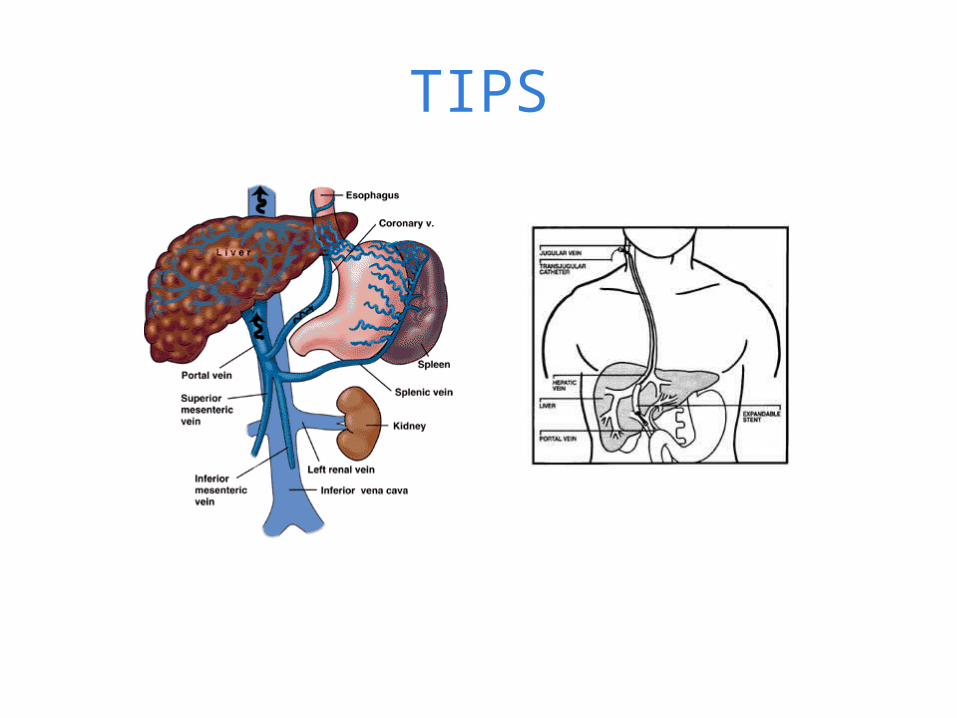
TIPS
Nursing Outcomes for Excess Fluid Volume
• Name 8 desired nursing outcomes for a patient with excess fluid volume
• 1.• 2.• 3.• 4.• 5.• 6.• 7.• 8.

Potential for Hemorrhage• Goal is to prevent bleeding• Drug therapy is to control HR and BP, this
decreases the hepatic venous pressure gradient, may use a Beta Blocker to do both and keep the HR about 55/min
• Gastric Intubation- NGT with iced saline or water lavage to vasoconstrict ulcerations
• device.

Potential for Hemorrhage
• Balloon Tamponade- esophagogastric- Blakemore tube- it has 2 balloons, an esophageal and gastric, one balloon in esophagus to compress varices, one larger in stomach to anchor tube, and another lumen for suctioning. Inserted through the mouth, once in place, balloons are inflated and clamped. Traction may be performed by anchoring it to a helmet

Potential for Hemorrhage• Complications of the Blakemore tube are aspiration, the
balloons may decompress and become lodged in the back of the pharynx. Blood and gastric contents may also be aspirated. The stomach balloon should always be deflated first and then the esophageal.
• Blood transfusions may be needed and emergently, PRBC’s and FFP

Potential for Hemorrhage
• Endoscopic- Band Ligation- small “O” bands are placed around the base of the varices, octreotide may be given at the time to decrease bleeding and secretions. Injection sclerotherapy may also be done to stop bleeding, a sclerosing agent is injected via endoscopy
• TIPS procedure or portal-systemic shunts may be needed
• What lab work should be monitored for these patients?

Banded esophageal Varices

Blakemore Tube

Portal Systemic Encephalopathy
• Ammonia is the probably cause, toxic to the brain• Drug Therapy- Lactulose- high molecular wt disaccharide,
it is thick and sticky with a sweet taste. It cleanses the GI tract and decreases the bacterial content, also creates and acid environment in the bowel and decreases the acid from 7-5, this keeps ammonia as an ion and pulls it into the colon. It may be given po or enema. Po is 20-30g q 4 hour. Monitor the number of stools and ammonia levels. It may cause cramping and often patients do not want to take it.

Portal-Systemic Encephalopathy
• Drug Therapy- Neomycin may also be used to cleanse the bowel and decrease protein breakdown, it can be given po or enema. Metronidazole (Flagyl) is also a bowel antibiotic with less renal side-effects
• Monitor the patient for neurologic changes, look for stupor, asterixis and fetor hepaticus
• Maintain patient safety

Patient Education
• Patient teaching should revolve around three main areas, what should be discussed under each?
• 1. Diet Therapy • 2. Drug Therapy • 3. Alcohol Abstinence• Goal is to have a decrease in ascites,
electrolytes WNL and no bleeding or PSE

Hepatitis
• Viral infection, can be acute or chronic, caused by one of five viruses, A-E, hepatitis F and G have been identified too
• Leads to inflammation of the liver cells• Can also be caused by exposure to chemicals, toxins
and medications• Can be secondary to infections from Epstein-Barr,
herpes, varicella and cytomegalovirus

Hepatitis

Types of Hepatitis
• Hepatitis A– HAV is an RNA virus– Spread fecal-oral, contaminated water, shellfish
and food contaminated by food handlers – Incubation is 15-50 days– Often the disease is mild and people don’t know
that they have it– Can lead to more severe liver disease in
compromised people

Types of Hepatitis• Hepatitis B
– HBV, it is a particle of DNA that is surrounded by a core and surface antigen
– Spread by:• Unprotected sex• Sharing needles or needle sticks• Blood transfusions, hemodialysis• Maternal-fetal route
– Symptoms occur in 25-180 days. They are:• Anorexia, nausea, vomiting, fever, fatigue, RUQ pain, dark
urine and light stool, joint pain and jaundice– Can lead to cirrhosis and liver failure– Often develop immunity and can become carriers

Hepatitis C• HCV is a single strand RNA virus• Transmitted blood to blood• Spread by:
– IV drug needle sharing– Blood, blood products or transplants– Needle stick injury with contaminated blood– Tattoos and intranasal cocaine
• Not transmitted by casual contact• Should not share razors, toothbrushes or pierced earrings• Incubation is 21-140 days, average 7 weeks• Most don’t know they are infected until it becomes chronic• Scarring leads to cirrhosis, can lead to liver cancer• Many receive liver transplants

Hepatitis D
• HDV is a defective RNA virus that needs helper function of HBV
• Coinfects and needs HBV for replication• Can be a superinfection and lead to a chronic
infection• Incubation is 14-56 days• Spread is mostly IV blood transmission

Hepatitis E
• HEV, single strand RNA virus• Transmitted by fecal-oral route, similar to HAV• Waterborne epidemic in India, now in Asia,
Africa, Middle East, Mexico and Central & South America
• Incubation of 15-64 days

Incidence
• 250,000 people in the US develop HAV• 200 million worldwide have HCV• 3.9 million have HCV in the US and 3 million have
chronic liver disease• Chronic hepatitis is through to be inflammation of
the liver for > 6 months• Usually the result of HCV or HBV• Can lead to fulminant liver failure, which is life-
threatening, due to total failure of the organ

Prevention
• What things can you tell a client to prevent the spread of hepatitis? (for both HAV and HBV/HCV)
• Which viruses have vaccines? • If exposed to the virus, is there anything that
can be taken?

Patient assessment• Assess for:
– Abdominal pain– Jaundice– Arthralgia– Myalgia, why?– Diarrhea– Changes in stool and urine
color– Fever, lethargy– Nausea/vomiting– History of contamination
• Liver Biopsy- confirmatory
• Labs:– Liver enzymes- AST, ALT, alk
phos, bilirubin all elevated– Enzyme assays- antibodies
to virus, anti-HAV, HBsAG (HBV surface antigen), anti HBcIgM (core antigen)
– Elisa for HCV and antiHCV– Anti-HDV and HEV– Usually present within 6
months

Nursing Diagnoses
• What do you think are the most common nursing diagnoses for Hepatitis?
• 1.• 2.• 3.• What interventions would be appropriate?

Nursing Interventions
• Drug Therapy– Use medications sparingly to rest liver– Antivirals, such as lamivudine (epivir-HBV) or
Hepsera– Interferon for HCV and HBV, SQ with ribavirin, take
the combination for 24-48 weeks until negative HCV RNA level

Home Care Education• What type of home care education would be appropriate?
– Discuss disease with family, especially spread– Discuss community resources, chronic, long term disease– Good handwashing, prevent spread of blood– Measures to prevent the spread of infection to the patient– Avoid alcohol– Allow for rest periods

Liver Transplantation• Assess patient both physically and psychologically prior to
transplantation• Contraindicated if:
– Severe cardiovascular or respiratory disease– Active alcohol or drug use– Metastatic disease– Inability to follow treatment or lack of appropriate caregiver
• Most transplants are cadaver livers, but some are donors of single lobes. Usually done with children
• Livers are obtained through the UNOS, United Network of Organ Sharing in cooperation with OPO, organ procurement organizations. In Jacksonville, we use Lifequest. There are presently 2300 people waiting for organ transplants within our area.
Liver Transplantation
• Most common complications are graft rejection and infection• Rejection can occur quickly or years out.• Medications to prevent rejection are:
– Cell-cept, Prograf, Imuran, Sirolimus, prednisone and FK-506
• Signs of rejection are RUQ pain, fever, tachycardia, decreased bile production and increased jaundice, elevated liver enzymes

Liver Transplantation
Infection Immunosuppressive therapy can cause rejection,
plus they are very debilitated, immobile and have multiple lines
Cytomegalovirus, mycobacterial and parasitic infections are most common
Usually on many antibioticsOther complications:
Hemorrhage, hepatic artery thrombosis, pulmonary atelectasis, electrolyte imbalances- usually Ca, Mg and K, ARF
Nursing Care
• Usually these patients are very ill, they may be in the ICU for many days, some are “fast-tracked”
• Return intubated, with a Swan line, arterial line and have continuous cardiac outputs and SvO2 readings.
• Some are on CVVH (continuous veno-venous hemofiltration) for renal perfusion
• Need a lot of psychological support


UNOS

Liver transplant video
• http://www.youtube.com/watch?v=If5dIwcGZY0Liver transplant surgery