nutrition diagnosis: a critical step in the nutrition care
TRANSCRIPT

i
Nutrition Diagnosis: A Critical Step in the Nutrition Care Process
Table of Contents
Section I: The Nutrition Care Process Nutrition Care Process and Model Article ....................................................................1
Section II: Development of Standardized Language ADA’s Standardized Language Model and Current Status ..........................................13
Section III: Introduction to Nutrition Diagnosis Introduction to Nutrition Diagnosis.............................................................................18
Section IV: Nutrition Diagnosis Terms and Definitions Nutrition Terms and Definitions ..................................................................................22
Section V: Nutrition Diagnosis Reference Sheets Single Page List of Terminology..................................................................................32
Section VI: Appendix Procedure for Nutrition Diagnostic Controlled Vocabulary/Terminology
Maintenance/Review ..................................................................................................154
Acknowledgements Task Force Members..................................................................................................160 Consultants ................................................................................................................161 Research Reviewers ...................................................................................................162
Feedback Form ......................................................................................................................165Camera Ready Pocket Guide .................................................................................................167
Please check the ADA Web site for additional materials
http://www.eatright.org/Member/index_10708.cfm?CFID=11486918&CFTOKEN=27367992http://www.eatright.org/Member/83_12962.cfm

Nutrition Care Process and Model: ADA adopts roadmap to quality care and outcomes managementKAREN LACEY, MS, RD; ELLEN PRITCHETT, RD
The establishment and implementation of a standardizedNutrition Care Process (NCP) and Model were identified aspriority actions for the profession for meeting goals of the
ADA Strategic Plan to “Increase demand and utilization of ser-vices provided by members” and “Empower members to com-pete successfully in a rapidly changing environment” (1). Pro-viding high-quality nutrition care means doing the right thing atthe right time, in the right way, for the right person, and achiev-ing the best possible results. Quality improvement literatureshows that, when a standardized process is implemented, lessvariation and more predictability in terms of outcomes occur(2). When providers of care, no matter their location, use aprocess consistently, comparable outcomes data can be gener-ated to demonstrate value. A standardized Nutrition Care Pro-cess effectively promotes the dietetics professional as theunique provider of nutrition care when it is consistently used asa systematic method to think critically and make decisions toprovide safe and effective nutrition care (3).
This article describes the four steps of ADA’s Nutrition CareProcess and the overarching framework of the Nutrition CareModel that illustrates the context within which the NutritionCare Process occurs. In addition, this article provides the ratio-nale for a standardized process by which nutrition care is pro-vided, distinguishes between the Nutrition Care Process andMedical Nutrition Therapy (MNT), and discusses future impli-cations for the profession.
BACKGROUNDPrior to the adoption of this standardized Nutrition Care Pro-cess, a variety of nutrition care processes were utilized by prac-titioners and taught by dietetics educators. Other allied health
professionals, including nursing, physical therapy, and occupa-tional therapy, utilize defined care processes specific to theirprofession (4-6). When asked whether ADA should develop astandardized Nutrition Care Process, dietetics professionalswere overwhelmingly in favor and strongly supportive of havinga standardized Nutrition Care Process for use by registereddietitians (RD) and dietetics technicians, registered (DTR).
The Quality Management Committee of the House of Dele-gates (HOD) appointed a Nutrition Care Model Workgroup inMay 2002 to develop a nutrition care process and model. Thefirst draft was presented to the HOD for member input andreview in September 2002. Further discussion occurred duringthe October 2002 HOD meeting, in Philadelphia. Revisionswere made accordingly, and the HOD unanimously adopted thefinal version of the Nutrition Care Process and Model on March31, 2003 “for implementation and dissemination to the dieteticsprofession and the Association for the enhancement of thepractice of dietetics.”
SETTING THE STAGE
Definition of Quality/Rationale for a StandardizedProcessThe National Academy of Science’s (NAS) Institute of Medi-cine (IOM) has defined quality as “The degree to which healthservices for individuals and populations increase the likelihoodof desired health outcomes and are consistent with currentprofessional knowledge” (7,8). The quality performance of pro-viders can be assessed by measuring the following: (a) theirpatients’ outcomes (end-results) or (b) the degree to whichproviders adhere to an accepted care process (7,8). The Com-mittee on Quality of Health Care in America further states thatit is not acceptable to have a wide quality chasm, or a gap,between actual and best possible performance (9). In an effortto ensure that dietetics professionals can meet both require-ments for quality performance noted above, the American Di-etetic Association (ADA) supports a standardized NutritionCare Process for the profession.
Standardized Process versus Standardized CareADA’s Nutrition Care Process is a standardized process fordietetics professionals and not a means to provide standardizedcare. A standardized process refers to a consistent structureand framework used to provide nutrition care, whereas stan-
K. Lacey is lecturer and Director of Dietetic Programs
at the University of Wisconsin-Green Bay, Green Bay. She
is also the Chair of the Quality Management Committee.
E. Pritchett is Director, Quality and Outcomes at ADA
headquarters in Chicago, IL.
If you have questions regarding the Nutrition Care Pro-
cess and Model, please contact Ellen Pritchett, RD, CPHQ,
Director of Quality and Outcomes at ADA,
Copyright © 2003 by the American Dietetic Association.
0002-8223/03/10308-0014$35.00/0
doi: 10.1053/jada.2003.50564
OF PROFESSIONAL INTEREST
Journal of THE AMERICAN DIETETIC ASSOCIATION / 1061Edition: 2006 1
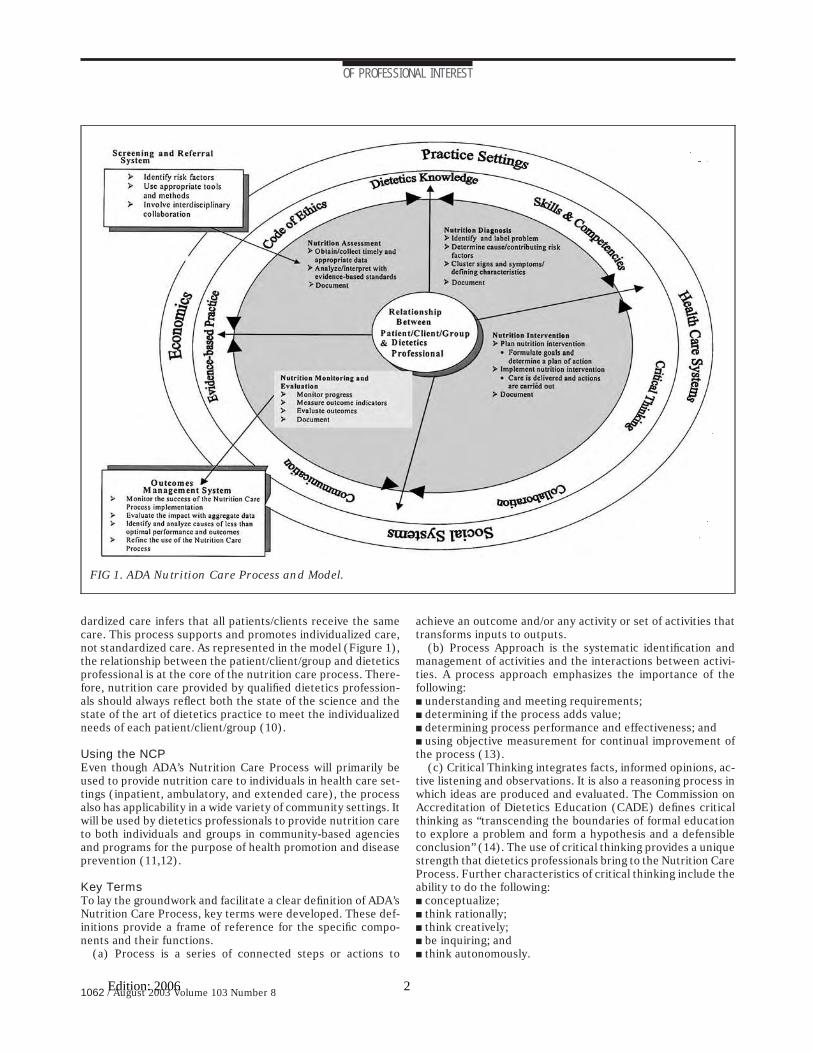
dardized care infers that all patients/clients receive the samecare. This process supports and promotes individualized care,not standardized care. As represented in the model (Figure 1),the relationship between the patient/client/group and dieteticsprofessional is at the core of the nutrition care process. There-fore, nutrition care provided by qualified dietetics profession-als should always reflect both the state of the science and thestate of the art of dietetics practice to meet the individualizedneeds of each patient/client/group (10).
Using the NCPEven though ADA’s Nutrition Care Process will primarily beused to provide nutrition care to individuals in health care set-tings (inpatient, ambulatory, and extended care), the processalso has applicability in a wide variety of community settings. Itwill be used by dietetics professionals to provide nutrition careto both individuals and groups in community-based agenciesand programs for the purpose of health promotion and diseaseprevention (11,12).
Key TermsTo lay the groundwork and facilitate a clear definition of ADA’sNutrition Care Process, key terms were developed. These def-initions provide a frame of reference for the specific compo-nents and their functions.
(a) Process is a series of connected steps or actions to
achieve an outcome and/or any activity or set of activities thattransforms inputs to outputs.
(b) Process Approach is the systematic identification andmanagement of activities and the interactions between activi-ties. A process approach emphasizes the importance of thefollowing:■ understanding and meeting requirements;■ determining if the process adds value;■ determining process performance and effectiveness; and■ using objective measurement for continual improvement ofthe process (13).
(c) Critical Thinking integrates facts, informed opinions, ac-tive listening and observations. It is also a reasoning process inwhich ideas are produced and evaluated. The Commission onAccreditation of Dietetics Education (CADE) defines criticalthinking as “transcending the boundaries of formal educationto explore a problem and form a hypothesis and a defensibleconclusion” (14). The use of critical thinking provides a uniquestrength that dietetics professionals bring to the Nutrition CareProcess. Further characteristics of critical thinking include theability to do the following:■ conceptualize;■ think rationally;■ think creatively;■ be inquiring; and■ think autonomously.
FIG 1. ADA Nutrition Care Process and Model.
OF PROFESSIONAL INTEREST
1062 / August 2003 Volume 103 Number 8Edition: 2006 2

(d) Decision Making is a critical process for choosing the bestaction to meet a desired goal.
(e) Problem Solving is the process of the following:■ problem identification;■ solution formation;■ implementation; and■ evaluation of the results.
(f) Collaboration is a process by which several individuals orgroups with shared concerns are united to address an identifiedproblem or need, leading to the accomplishment of what eachcould not do separately (15).
DEFINITION OF ADA’S NCPUsing the terms and concepts described above, ADA’s Nutri-tion Care Process is defined as “a systematic problem-solvingmethod that dietetics professionals use to critically think andmake decisions to address nutrition related problems and pro-vide safe and effective quality nutrition care.”
The Nutrition Care Process consists of four distinct, but in-terrelated and connected steps: (a) Nutrition Assessment, (b)Nutrition Diagnosis, (c) Nutrition Intervention, and d) Nutri-tion Monitoring and Evaluation. These four steps were finalizedbased on extensive review and evaluation of previous worksdescribing nutrition care (16-24). Even though each stepbuilds on the previous one, the process is not linear. Criticalthinking and problem solving will frequently require that die-tetics professionals revisit previous steps to reassess, add, orrevise nutrition diagnoses; modify intervention strategies;and/or evaluate additional outcomes. Figure 2 describes eachof these four steps in a similar format consisting of the follow-ing:■ definition and purpose;■ key components or substeps with examples as appropriate;■ critical thinking characteristics;■ documentation elements; and■ considerations for continuation, discontinuation, or dis-charge of care.
Providing nutrition care using ADA’s Nutrition Care Processbegins when a patient/client/group has been identified at nutri-tion risk and needs further assistance to achieve or maintainnutrition and health goals. It is also important to recognize thatpatients/clients who enter the health care system are morelikely to have nutrition problems and therefore benefit fromreceiving nutrition care in this manner. The Nutrition CareProcess cycles through the steps of assessment, diagnosis, in-tervention, and monitoring and evaluation. Nutrition care caninvolve one or more cycles and ends, ideally, when nutritiongoals have been achieved. However, the patient/client/groupmay choose to end care earlier based on personal or externalfactors. Using professional judgment, the dietetics professionalmay discharge the patient/client/group when it is determinedthat no further progress is likely.
PURPOSE OF NCPADA’s Nutrition Care Process, as described in Figure 2, givesdietetics professionals a consistent and systematic structureand method by which to think critically and make decisions. Italso assists dietetics professionals to scientifically and holisti-cally manage nutrition care, thus helping patients better meettheir health and nutrition goals. As dietetics professionals con-sistently use the Nutrition Care Process, one should expect ahigher probability of producing good outcomes. The NutritionCare Process then begins to establish a link between quality
and professional autonomy. Professional autonomy resultsfrom being recognized for what we do well, not just for who weare. When quality can be demonstrated, as defined previouslyby the IOM (7,8), then dietetics professionals will stand out asthe preferred providers of nutrition services. The NutritionCare Process, when used consistently, also challenges dieteticsprofessionals to move beyond experience-based practice toreach a higher level of evidence-based practice (9,10).
The Nutrition Care Process does not restrict practice butacknowledges the common dimensions of practice by the fol-lowing:■ defining a common language that allows nutrition practice tobe more measurable;■ creating a format that enables the process to generate quan-titative and qualitative data that can then be analyzed and in-terpreted; and■ serving as the structure to validate nutrition care and show-ing how the nutrition care that was provided does what it in-tends to do.
DISTINCTION BETWEEN MNT AND THE NCPMedical Nutrition Therapy (MNT) was first defined by ADA inthe mid-1990s to promote the benefits of managing or treatinga disease with nutrition. Its components included an assess-ment of nutritional status of patients and the provision of eitherdiet modification, counseling, or specialized nutrition thera-pies. MNT soon became a widely used term to describe a widevariety of nutrition care services provided by dietetics profes-sionals. Since MNT was first introduced, dietetics professionalshave gained much credibility among legislators and otherhealth care providers. More recently, MNT has been redefinedas part of the 2001 Medicare MNT benefit legislation to be“nutritional diagnostic, therapy, and counseling services for thepurpose of disease management, which are furnished by a reg-istered dietitian or nutrition professional” (25).
The intent of the NCP is to describe accurately the spectrumof nutrition care that can be provided by dietetics profession-als. Dietetics professionals are uniquely qualified by virtue ofacademic and supervised practice training and appropriatecertification and/or licensure to provide a comprehensive arrayof professional services relating to the prevention or treatmentof nutrition-related illness (14,26). MNT is but one specifictype of nutrition care. The NCP articulates the consistent andspecific steps a dietetics professional would use when deliver-ing MNT, but it will also be used to guide nutrition educationand other preventative nutrition care services. One of the keydistinguishing characteristics between MNT and the other nu-trition services using the NCP is that MNT always involves anin-depth, comprehensive assessment and individualized care.For example, one individual could receive MNT for diabetesand also nutrition education services or participate in a com-munity-based weight loss program (27). Each service woulduse the Nutrition Care Process, but the process would be im-plemented differently; the components of each step of the pro-cess would be tailored to the type of service.
By articulating the steps of the Nutrition Care Process, thecommonalities (the consistent, standardized, four-step pro-cess) of nutrition care are emphasized even though the processis implemented differently for different nutrition services. Witha standardized Nutrition Care Process in place, MNT should notbe used to describe all of the nutrition services that dieteticsprofessionals provide. As noted above, MNT is the only appli-cation of the Nutrition Care Process (28-31). This change in
OF PROFESSIONAL INTEREST
Journal of THE AMERICAN DIETETIC ASSOCIATION / 1063Edition: 2006 3

STEP 1. NUTRITION ASSESSMENT
Basic Definition &Purpose
“Nutrition Assessment” is the first step of the Nutrition Care Process. Its purpose is to obtainadequate information in order to identify nutrition-related problems. It is initiated by referral and/orscreening of individuals or groups for nutritional risk factors. Nutrition assessment is a systematicprocess of obtaining, verifying, and interpreting data in order to make decisions about the nature andcause of nutrition-related problems. The specific types of data gathered in the assessment will varydepending on a) practice settings, b) individual/groups’ present health status, c) how data are relatedto outcomes to be measured, d) recommended practices such as ADA’s Evidence Based Guides forPractice and e) whether it is an initial assessment or a reassessment. Nutrition assessment requiresmaking comparisons between the information obtained and reliable standards (ideal goals). Nutritionassessment is an on-going, dynamic process that involves not only initial data collection, but alsocontinual reassessment and analysis of patient/client/group needs. Assessment provides thefoundation for the nutrition diagnosis at the next step of the Nutrition Care Process.
Data Sources/Tools forAssessment
� Referral information and/or interdisciplinary records� Patient/client interview (across the lifespan)� Community-based surveys and focus groups� Statistical reports; administrative data� Epidemiological studies
Types of Data Collected � Nutritional Adequacy (dietary history/detailed nutrient intake)� Health Status (anthropometric and biochemical measurements, physical & clinical conditions,
physiological and disease status)� Functional and Behavioral Status (social and cognitive function, psychological and emotional
factors, quality-of-life measures, change readiness)
Nutrition AssessmentComponents
� Review dietary intake for factors that affect health conditions and nutrition risk� Evaluate health and disease condition for nutrition-related consequences� Evaluate psychosocial, functional, and behavioral factors related to food access, selection,
preparation, physical activity, and understanding of health condition� Evaluate patient/client/group’s knowledge, readiness to learn, and potential for changing behaviors� Identify standards by which data will be compared� Identify possible problem areas for making nutrition diagnoses
Critical Thinking The following types of critical thinking skills are especially needed in the assessment step:� Observing for nonverbal and verbal cues that can guide and prompt effective interviewing
methods;� Determining appropriate data to collect;� Selecting assessment tools and procedures (matching the assessment method to the situation);� Applying assessment tools in valid and reliable ways;� Distinguishing relevant from irrelevant data;� Distinguishing important from unimportant data;� Validating the data;� Organizing & categorizing the data in a meaningful framework that relates to nutrition problems;
and� Determining when a problem requires consultation with or referral to another provider.
Documentation ofAssessment
Documentation is an on-going process that supports all of the steps in the Nutrition Care Process.Quality documentation of the assessment step should be relevant, accurate, and timely. Inclusion ofthe following information would further describe quality assessment documentation:� Date and time of assessment;� Pertinent data collected and comparison with standards;� Patient/client/groups’ perceptions, values, and motivation related to presenting problems;� Changes in patient/client/group’s level of understanding, food-related behaviors, and other clinical
outcomes for appropriate follow-up; and� Reason for discharge/discontinuation if appropriate.
Determination forContinuation of Care
If upon the completion of an initial or reassessment it is determined that the problem cannot bemodified by further nutrition care, discharge or discontinuation from this episode of nutrition caremay be appropriate.
FIG 2. ADA Nutrition Care Process.
OF PROFESSIONAL INTEREST
1064 / August 2003 Volume 103 Number 8Edition: 2006 4

STEP 2. NUTRITION DIAGNOSISBasic Definition &
Purpose“Nutrition Diagnosis” is the second step of the Nutrition Care Process, and is the identification andlabeling that describes an actual occurrence, risk of, or potential for developing a nutritional problemthat dietetics professionals are responsible for treating independently. At the end of the assessmentstep, data are clustered, analyzed, and synthesized. This will reveal a nutrition diagnostic categoryfrom which to formulate a specific nutrition diagnostic statement. Nutrition diagnosis should not beconfused with medical diagnosis, which can be defined as a disease or pathology of specific organsor body systems that can be treated or prevented. A nutrition diagnosis changes as thepatient/client/group’s response changes. A medical diagnosis does not change as long as thedisease or condition exists. A patient/client/group may have the medical diagnosis of “Type 2diabetes mellitus”; however, after performing a nutrition assessment, dietetics professionals maydiagnose, for example, “undesirable overweight status” or “excessive carbohydrate intake.”Analyzing assessment data and naming the nutrition diagnosis(es) provide a link to setting realisticand measurable expected outcomes, selecting appropriate interventions, and tracking progress inattaining those expected outcomes.
Data Sources/Tools forDiagnosis
� Organized and clustered assessment data� List(s) of nutrition diagnostic categories and nutrition diagnostic labels� Currently the profession does not have a standardized list of nutrition diagnoses. However ADA
has appointed a Standardized Language Work Group to begin development of standardizedlanguage for nutrition diagnoses and intervention. (June 2003)
Nutrition DiagnosisComponents (3distinct parts)
1. Problem (Diagnostic Label)The nutrition diagnostic statement describes alterations in the patient/client/group’s nutritional status.
A diagnostic label (qualifier) is an adjective that describes/qualifies the human response such as:� Altered, impaired, ineffective, increased/decreased, risk of, acute or chronic.2. Etiology (Cause/Contributing Risk Factors)The related factors (etiologies) are those factors contributing to the existence of, or maintenance of
pathophysiological, psychosocial, situational, developmental, cultural, and/or environmentalproblems.
� Linked to the problem diagnostic label by words “related to” (RT)� It is important not only to state the problem, but to also identify the cause of the problem.▫ This helps determine whether or not nutritional intervention will improve the condition or correct
the problem.▫ It will also identify who is responsible for addressing the problem. Nutrition problems are either
caused directly by inadequate intake (primary) or as a result of other medical, genetic, orenvironmental factors (secondary).
▫ It is also possible that a nutrition problem can be the cause of another problem. For example,excessive caloric intake may result in unintended weight gain. Understanding the cascade ofevents helps to determine how to prioritize the interventions.
▫ It is desirable to target interventions at correcting the cause of the problem whenever possible;however, in some cases treating the signs and symptoms (consequences) of the problem may alsobe justified.
� The ranking of nutrition diagnoses permits dietetics professionals to arrange the problems in orderof their importance and urgency for the patient/client/group.
3. Signs/Symptoms (Defining Characteristics)The defining characteristics are a cluster of subjective and objective signs and symptoms
established for each nutrition diagnostic category. The defining characteristics, gathered duringthe assessment phase, provide evidence that a nutrition related problem exists and that theproblem identified belongs in the selected diagnostic category. They also quantify the problemand describe its severity:
� Linked to etiology by words “as evidenced by” (AEB);� The symptoms (subjective data) are changes that the patient/client/group feels and expresses
verbally to dietetics professionals; and� The signs (objective data) are observable changes in the patient/client/group’s health status.
Nutrition DiagnosticStatement (PES)
Whenever possible, a nutrition diagnostic statement is written in a PES format that states theProblem (P), the Etiology (E), and the Signs & Symptoms (S). However, if the problem is either a risk(potential) or wellness problem, the nutrition diagnostic statement may have only two elements,Problem (P), and the Etiology (E), since Signs & Symptoms (S) will not yet be exhibited in the patient.A well-written Nutrition Diagnostic Statement should be:1. Clear and concise2. Specific: patient/client/group-centered3. Related to one client problem4. Accurate: relate to one etiology5. Based on reliable and accurate assessment dataExamples of Nutrition Diagnosis Statements (PES or PE)� Excessive caloric intake (problem) “related to” frequent consumption of large portions of high fat
meals (etiology) “as evidenced by” average daily intake of calories exceeding recommendedamount by 500 kcal and 12-pound weight gain during the past 18 months (signs)
FIG 2 cont’d.
OF PROFESSIONAL INTEREST
Journal of THE AMERICAN DIETETIC ASSOCIATION / 1065Edition: 2006 5

� Inappropriate infant feeding practice RT lack of knowledge AEB infant receiving bedtime juice in abottle
� Unintended weight loss RT inadequate provision of energy by enteral products AEB 6-poundweight loss over past month
� Risk of weight gain RT a recent decrease in daily physical activity following sports injury
Critical Thinking The following types of critical thinking skills are especially needed in the diagnosis step:� Finding patterns and relationships among the data and possible causes;� Making inferences (“if this continues to occur, then this is likely to happen”);� Stating the problem clearly and singularly;� Suspending judgment (be objective and factual);� Making interdisciplinary connections;� Ruling in/ruling out specific diagnoses; and� Prioritizing the relative importance of problems for patient/client/group safety.
Documentation ofDiagnosis
Documentation is an on-going process that supports all of the steps in the Nutrition Care Process.Quality documentation of the diagnosis step should be relevant, accurate, and timely. A nutritiondiagnosis is the impression of dietetics professionals at a given point in time. Therefore, as moreassessment data become available, the documentation of the diagnosis may need to be revised andupdated.Inclusion of the following information would further describe quality documentation of this step:� Date and time; and� Written statement of nutrition diagnosis.
Determination forContinuation of Care
Since the diagnosis step primarily involves naming and describing the problem, the determination forcontinuation of care seldom occurs at this step. Determination of the continuation of care is moreappropriately made at an earlier or later point in the Nutrition Care Process.
STEP 3. NUTRITION INTERVENTION
Basic Definition &Purpose
“Nutrition Intervention” is the third step of the Nutrition Care Process. An intervention is a specificset of activities and associated materials used to address the problem. Nutrition interventions arepurposefully planned actions designed with the intent of changing a nutrition-related behavior, riskfactor, environmental condition, or aspect of health status for an individual, target group, or thecommunity at large. This step involves a) selecting, b) planning, and c) implementing appropriateactions to meet patient/client/groups’ nutrition needs. The selection of nutrition interventions is drivenby the nutrition diagnosis and provides the basis upon which outcomes are measured and evaluated.Dietetics professionals may actually do the interventions, or may include delegating or coordinatingthe nutrition care that others provide. All interventions must be based on scientific principles andrationale and, when available, grounded in a high level of quality research (evidence-basedinterventions).Dietetics professionals work collaboratively with the patient/client/group, family, or caregiver tocreate a realistic plan that has a good probability of positively influencing the diagnosis/problem. Thisclient-driven process is a key element in the success of this step, distinguishing it from previousplanning steps that may or may not have involved the patient/client/group to this degree ofparticipation.
Data Sources/Tools forInterventions
� Evidence-based nutrition guides for practice and protocols� Current research literature� Current consensus guidelines and recommendations from other professional organizations� Results of outcome management studies or Continuous Quality Index projects.� Current patient education materials at appropriate reading level and language� Behavior change theories (self-management training, motivational interviewing, behavior
modification, modeling)
Nutrition InterventionComponents
This step includes two distinct interrelated processes:1. Plan the nutrition intervention (formulate & determine a plan of action)� Prioritize the nutrition diagnoses based on severity of problem; safety; patient/client/group’s need;
likelihood that nutrition intervention will impact problem and patient/client/groups’ perception ofimportance.
� Consult ADA’s MNT Evidence-Based Guides for Practice and other practice guides. Theseresources can assist dietetics professionals in identifying science-based ideal goals and selectingappropriate interventions for MNT. They list appropriate value(s) for control or improvement of thedisease or conditions as defined and supported in the literature.
� Determine patient-focused expected outcomes for each nutrition diagnosis. The expectedoutcomes are the desired change(s) to be achieved over time as a result of nutrition intervention.They are based on nutrition diagnosis; for example, increasing or decreasing laboratory values,decreasing blood pressure, decreasing weight, increasing use of stanols/sterols, or increasingfiber. Expected outcomes should be written in observable and measurable terms that are clearand concise. They should be patient/client/group-centered and need to be tailored to what isreasonable to the patient’s circumstances and appropriate expectations for treatments andoutcomes.
FIG 2 cont’d.
OF PROFESSIONAL INTEREST
1066 / August 2003 Volume 103 Number 8Edition: 2006 6

� Confer with patient/client/group, other caregivers or policies and program standards throughoutplanning step.
� Define intervention plan (for example write a nutrition prescription, provide an education plan orcommunity program, create policies that influence nutrition programs and standards).
� Select specific intervention strategies that are focused on the etiology of the problem and that areknown to be effective based on best current knowledge and evidence.
� Define time and frequency of care including intensity, duration, and follow-up.� Identify resources and/or referrals needed.2. Implement the nutrition intervention (care is delivered and actions are carried out)� Implementation is the action phase of the nutrition care process. During implementation, dietetics
professionals:▫ Communicate the plan of nutrition care;▫ Carry out the plan of nutrition care; and▫ Continue data collection and modify the plan of care as needed.� Other characteristics that define quality implementation include:▫ Individualize the interventions to the setting and client;▫ Collaborate with other colleagues and health care professionals;▫ Follow up and verify that implementation is occurring and needs are being met; and▫ Revise strategies as changes in condition/response occurs.
Critical Thinking Critical thinking is required to determine which intervention strategies are implemented based onanalysis of the assessment data and nutrition diagnosis. The following types of critical thinking skillsare especially needed in the intervention step:� Setting goals and prioritizing;� Transferring knowledge from one situation to another;� Defining the nutrition prescription or basic plan;� Making interdisciplinary connections;� Initiating behavioral and other interventions;� Matching intervention strategies with client needs, diagnoses, and values;� Choosing from among alternatives to determine a course of action; and� Specifying the time and frequency of care.
Documentation ofNutrition Interventions
Documentation is an on-going process that supports all of the steps in the Nutrition Care Process.Quality documentation of nutrition interventions should be relevant, accurate, and timely. It shouldalso support further intervention or discharge from care. Changes in patient/client/group’s level ofunderstanding and food-related behaviors must be documented along with changes in clinical orfunctional outcomes to assure appropriate care/case management in the future. Inclusion of thefollowing information would further describe quality documentation of this step:� Date and time;� Specific treatment goals and expected outcomes;� Recommended interventions, individualized for patient;� Any adjustments of plan and justifications;� Patient receptivity;� Referrals made and resources used;� Any other information relevant to providing care and monitoring progress over time;� Plans for follow-up and frequency of care; and� Rationale for discharge if appropriate.
Determination forContinuation of Care
If the patient/client/group has met intervention goals or is not at this time able/ready to make neededchanges, the dietetics professional may include discharging the client from this episode of care aspart of the planned intervention.
STEP 4. NUTRITION MONITORING AND EVALUATION
Basic Definition &Purpose
“Nutrition Monitoring and Evaluation” is the fourth step of the Nutrition Care Process. Monitoringspecifically refers to the review and measurement of the patient/client/group’s status at a scheduled(preplanned) follow-up point with regard to the nutrition diagnosis, intervention plans/goals, andoutcomes, whereas Evaluation is the systematic comparison of current findings with previous status,intervention goals, or a reference standard. Monitoring and evaluation use selected outcomeindicators (markers) that are relevant to the patient/client/group’s defined needs, nutrition diagnosis,nutrition goals, and disease state. Recommended times for follow-up, along with relevant outcomesto be monitored, can be found in ADA’s Evidence Based Guides for Practice and other evidence-based sources.The purpose of monitoring and evaluation is to determine the degree to which progress is beingmade and goals or desired outcomes of nutrition care are being met. It is more than just “watching”what is happening, it requires an active commitment to measuring and recording the appropriateoutcome indicators (markers) relevant to the nutrition diagnosis and intervention strategies. Data fromthis step are used to create an outcomes management system. Refer to Outcomes ManagementSystem in text.
FIG 2 cont’d.
OF PROFESSIONAL INTEREST
Journal of THE AMERICAN DIETETIC ASSOCIATION / 1067Edition: 2006 7
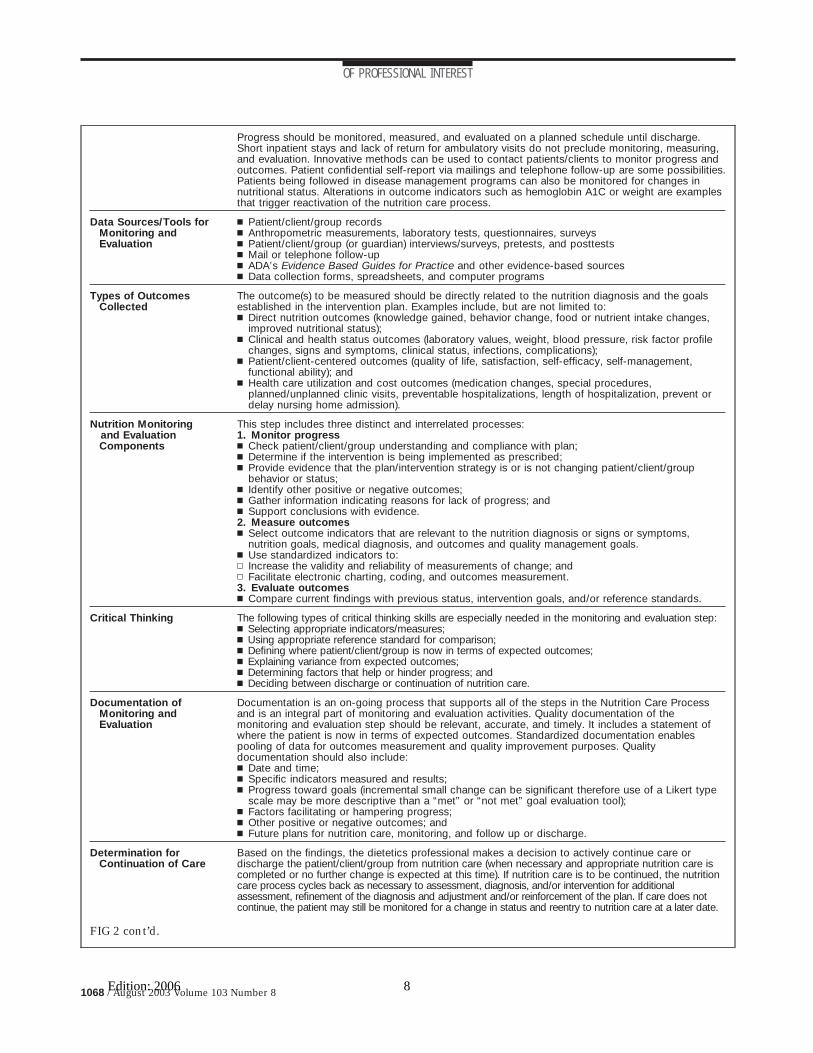
Progress should be monitored, measured, and evaluated on a planned schedule until discharge.Short inpatient stays and lack of return for ambulatory visits do not preclude monitoring, measuring,and evaluation. Innovative methods can be used to contact patients/clients to monitor progress andoutcomes. Patient confidential self-report via mailings and telephone follow-up are some possibilities.Patients being followed in disease management programs can also be monitored for changes innutritional status. Alterations in outcome indicators such as hemoglobin A1C or weight are examplesthat trigger reactivation of the nutrition care process.
Data Sources/Tools forMonitoring andEvaluation
� Patient/client/group records� Anthropometric measurements, laboratory tests, questionnaires, surveys� Patient/client/group (or guardian) interviews/surveys, pretests, and posttests� Mail or telephone follow-up� ADA’s Evidence Based Guides for Practice and other evidence-based sources� Data collection forms, spreadsheets, and computer programs
Types of OutcomesCollected
The outcome(s) to be measured should be directly related to the nutrition diagnosis and the goalsestablished in the intervention plan. Examples include, but are not limited to:� Direct nutrition outcomes (knowledge gained, behavior change, food or nutrient intake changes,
improved nutritional status);� Clinical and health status outcomes (laboratory values, weight, blood pressure, risk factor profile
changes, signs and symptoms, clinical status, infections, complications);� Patient/client-centered outcomes (quality of life, satisfaction, self-efficacy, self-management,
functional ability); and� Health care utilization and cost outcomes (medication changes, special procedures,
planned/unplanned clinic visits, preventable hospitalizations, length of hospitalization, prevent ordelay nursing home admission).
Nutrition Monitoringand EvaluationComponents
This step includes three distinct and interrelated processes:1. Monitor progress� Check patient/client/group understanding and compliance with plan;� Determine if the intervention is being implemented as prescribed;� Provide evidence that the plan/intervention strategy is or is not changing patient/client/group
behavior or status;� Identify other positive or negative outcomes;� Gather information indicating reasons for lack of progress; and� Support conclusions with evidence.2. Measure outcomes� Select outcome indicators that are relevant to the nutrition diagnosis or signs or symptoms,
nutrition goals, medical diagnosis, and outcomes and quality management goals.� Use standardized indicators to:▫ Increase the validity and reliability of measurements of change; and▫ Facilitate electronic charting, coding, and outcomes measurement.3. Evaluate outcomes� Compare current findings with previous status, intervention goals, and/or reference standards.
Critical Thinking The following types of critical thinking skills are especially needed in the monitoring and evaluation step:� Selecting appropriate indicators/measures;� Using appropriate reference standard for comparison;� Defining where patient/client/group is now in terms of expected outcomes;� Explaining variance from expected outcomes;� Determining factors that help or hinder progress; and� Deciding between discharge or continuation of nutrition care.
Documentation ofMonitoring andEvaluation
Documentation is an on-going process that supports all of the steps in the Nutrition Care Processand is an integral part of monitoring and evaluation activities. Quality documentation of themonitoring and evaluation step should be relevant, accurate, and timely. It includes a statement ofwhere the patient is now in terms of expected outcomes. Standardized documentation enablespooling of data for outcomes measurement and quality improvement purposes. Qualitydocumentation should also include:� Date and time;� Specific indicators measured and results;� Progress toward goals (incremental small change can be significant therefore use of a Likert type
scale may be more descriptive than a “met” or “not met” goal evaluation tool);� Factors facilitating or hampering progress;� Other positive or negative outcomes; and� Future plans for nutrition care, monitoring, and follow up or discharge.
Determination forContinuation of Care
Based on the findings, the dietetics professional makes a decision to actively continue care ordischarge the patient/client/group from nutrition care (when necessary and appropriate nutrition care iscompleted or no further change is expected at this time). If nutrition care is to be continued, the nutritioncare process cycles back as necessary to assessment, diagnosis, and/or intervention for additionalassessment, refinement of the diagnosis and adjustment and/or reinforcement of the plan. If care does notcontinue, the patient may still be monitored for a change in status and reentry to nutrition care at a later date.
FIG 2 cont’d.
OF PROFESSIONAL INTEREST
1068 / August 2003 Volume 103 Number 8Edition: 2006 8

describing what dietetics professionals do is truly a paradigmshift. This new paradigm is more complete, takes in more pos-sibilities, and explains observations better. Finally, it allowsdietetics professionals to act in ways that are more likely toachieve the results that are desired and expected.
NUTRITION CARE MODELThe Nutrition Care Model is a visual representation that re-flects key concepts of each step of the Nutrition Care Processand illustrates the greater context within which the NutritionCare Process is conducted. The model also identifies other fac-tors that influence and impact on the quality of nutrition careprovided. Refer to Figure 1 for an illustration of the model asdescribed below:■ Central Core: Relationship between patient/client/group anddietetics professional;■ Nutrition Care Process: Four steps of the nutrition care pro-cess (Figure 2);■ Outer rings:■ Middle ring: Strengths and abilities that dietetics profession-als bring to the process (dietetics knowledge, skills, and com-petencies; critical thinking, collaboration, and communication;evidence-based practice, and Code of Ethics) (32);■ Outer ring: Environmental factors that influence the process(practice settings, health care systems, social systems, andeconomics);■ Supporting Systems:■ Screening and Referral System as access to Nutrition Care;and■ Outcomes Management System as a means to provide contin-uous quality improvement to the process.
The model is intended to depict the relationship with whichall of these components overlap, interact, and move in a dy-namic manner to provide the best quality nutrition care possi-ble.
Central to providing nutrition care is the relationship be-tween the patient/client/group and the dietetics professional.The patient/client/groups’ previous educational experiencesand readiness to change influence this relationship. The edu-cation and training that dietetics professionals receive havevery strong components devoted to interpersonal knowledgeand skill building such as listening, empathy, coaching, andpositive reinforcing.
The middle ring identifies abilities of dietetics professionalsthat are especially applicable to the Nutrition Care Process.These include the unique dietetics knowledge, skill, and com-petencies that dietetics professionals bring to the process, inaddition to a well-developed capability for critical thinking, col-laboration, and communication. Also in this ring is evidence-based practice that emphasizes that nutrition care must incor-porate currently available scientific evidence, linking what isdone (content) and how it is done (process of care). The Codeof Ethics defines the ethical principles by which dietetics pro-fessionals should practice (33). Dietetics knowledge and evi-dence-based practice establish the Nutrition Care Process asunique to dietetics professionals; no other health care profes-sional is qualified to provide nutrition care in this manner. How-ever, the Nutrition Care Process is highly dependent on collab-oration and integration within the health care team. As statedabove, communication and participation within the health careteam are critical for identification of individuals who are appro-priate for nutrition care.
The outer ring identifies some of the environmental factors
such as practice settings, health care systems, social systems,and economics. These factors impact the ability of the patient/client/group to receive and benefit from the interventions ofnutrition care. It is essential that dietetics professionals assessthese factors and be able to evaluate the degree to which theymay be either a positive or negative influence on the outcomesof care.
Screening and Referral SystemBecause screening may or may not be accomplished by dietet-ics professionals, nutrition screening is a supportive systemand not a step within the Nutrition Care Process. Screening isextremely important; it is an identification step that is outsidethe actual “care” and provides access to the Nutrition CareProcess.
The Nutrition Care Process depends on an effective screen-ing and/or referral process that identifies clients who wouldbenefit from nutrition care or MNT. Screening is defined by theUS Preventive Services Task Force as “those preventive ser-vices in which a test or standardized examination procedure isused to identify patients requiring special intervention” (34).The major requirements for a screening test to be consideredeffective are the following:■ Accuracy as defined by the following three components:� Specificity: Can it identify patients with a condition?� Sensitivity: Can it identify those who do not have the condi-tion?� Positive and negative predictive; and■ Effectiveness as related to likelihood of positive health out-comes if intervention is provided.
Screening parameters need to be tailored to the populationand to the nutrition care services to be provided. For example,the screening parameters identified for a large tertiary acutecare institution specializing in oncology would be vastly differ-ent than the screening parameters defined for an ambulatoryobstetrics clinic. Depending on the setting and institutionalpolicies, the dietetics professional may or may not be directlyinvolved in the screening process. Regardless of whether die-tetics professionals are actively involved in conducting thescreening process, they are accountable for providing inputinto the development of appropriate screening parameters toensure that the screening process asks the right questions.They should also evaluate how effective the screening processis in terms of correctly identifying clients who require nutritioncare.
In addition to correctly identifying clients who would benefitfrom nutrition care, a referral process may be necessary toensure that the client has an identifiable method of being linkedto dietetics professionals who will ultimately provide the nutri-tion care or medical nutrition therapy. While the nutritionscreening and referral is not part of the Nutrition Care Process,it is a critical antecedent step in the overall system (35).
Outcomes Management SystemAn outcomes management system evaluates the effectivenessand efficiency of the entire process (assessment, diagnosis,interventions, cost, and others), whereas the fourth step of theprocess “nutrition monitoring and evaluations” refers to theevaluation of the patient/client/group’s progress in achievingoutcomes.
Because outcomes management is a system’s commitment toeffective and efficient care, it is depicted outside of the NCP.Outcomes management links care processes and resource uti-
OF PROFESSIONAL INTEREST
Journal of THE AMERICAN DIETETIC ASSOCIATION / 1069Edition: 2006 9

lization with outcomes. Through outcomes management, rele-vant data are collected and analyzed in a timely manner so thatperformance can be adjusted and improved. Findings are com-pared with such things as past levels of performance; organiza-tional, regional, or national norms; and standards or bench-marks of optimal performance. Generally, this information isreported to providers, administrators, and payors/funders andmay be part of administrative databases or required reportingsystems.
It requires an infrastructure in which outcomes for the pop-ulation served are routinely assessed, summarized, and re-ported. Health care organizations use complex informationmanagement systems to manage resources and track perfor-mance. Selected information documented throughout the nu-trition care process is entered into these central informationmanagement systems and structured databases. Examples ofcentralized data systems in which nutrition care data should beincluded are the following:■ basic encounter documentation for billing and cost account-ing;■ tracking of standard indicators for quality assurance and ac-creditation;■ pooling data from a large series of patients/clients/groups todetermine outcomes; and■ specially designed studies that link process and outcomes todetermine effectiveness and cost effectiveness of diagnosticand intervention approaches.
The major goal of outcomes management is to utilize col-lected data to improve the quality of care rendered in the fu-ture. Monitoring and evaluation data from individuals arepooled/aggregated for the purposes of professional account-ability, outcomes management, and systems/processes im-provement. Results from a large series of patients/clients canbe used to determine the effectiveness of intervention strate-gies and the impact of nutrition care in improving the overallhealth of individuals and groups. The effects of well-monitoredquality improvement initiatives should be reflected in measur-able improvements in outcomes.
Outcomes management comprehensively evaluates the twoparts of IOM’s definition of quality: outcomes and process. Mea-suring the relationship between the process and the outcome isessential for quality improvement. To ensure that the quality ofpatient care is not compromised, the focus of quality improve-ment efforts should always be directed at the outcome of care(36-43).
FUTURE IMPLICATIONS
Impact on Coverage for ServicesQuality-related issues are gaining in importance worldwide.Even though our knowledge base is increasing, the scientificevidence for most clinical practices in all of medicine is modest.So much of what is done in health care does not maximizequality or minimize cost (44). A standardized Nutrition CareProcess is a necessary foundation tool for gathering valid andreliable data on how quality nutrition care provided by qualifieddietetics professionals improves the overall quality of healthcare provided. Implementing ADA’s Nutrition Care Processprovides a framework for demonstrating that nutrition careimproves outcomes by the following: (a) enhancing the healthof individuals, groups, institutions, or health systems; (b) po-tentially reducing health care costs by decreasing the need formedications, clinic and hospital visits, and preventing or delay-
ing nursing home admissions; and (c) serving as the basis forresearch, documenting the impact of nutrition care providedby dietetics professionals (45-47).
Developing Scopes and Practice StandardsThe work group reviewed the questions raised by delegatesregarding the role of the RD and DTR in the Nutrition CareProcess. As a result of careful consideration of this importantissue, it was concluded that describing the various types oftasks and responsibilities appropriate to each of these creden-tialed dietetics professionals was yet another professional issuebeyond the intent and purpose of developing a standardizedNutrition Care Process.
A scope of practice of a profession is the range of servicesthat the profession is authorized to provide. Scopes of practice,depending on the particular setting in which they are used, canhave different applications. They can serve as a legal documentfor state certification/licensure laws or they might be incorpo-rated into institutional policy and procedure guidelines or jobdescriptions. Professional scopes of practice should be basedon the education, training, skills, and competencies of eachprofession (48).
As previously noted, a dietetics professional is a person who,by virtue of academic and clinical training and appropriate cer-tification and/or licensure, is uniquely qualified to provide acomprehensive array of professional services relating to pre-vention and treatment of nutrition-related conditions. A Scopeof Practice articulates the roles of the RD, DTR, and advanced-practice RD. Issues to be addressed for the future include thefollowing: (a) the need for a common scope with specializedguidelines and (b) recognition of the rich diversity of practicevs exclusive domains of practice regulation.
Professional standards are “authoritative statements thatdescribe performance common to the profession.” As such,standards should encompass the following:■ articulate the expectations the public can have of a dieteticsprofessional in any practice setting, domain, and/or role;■ expect and achieve levels of practice against which actualperformance can be measured; and■ serve as a legal reference to describe “reasonable and pru-dent” dietetics practice.
The Nutrition Care Process effectively reflects the dieteticsprofessional as the unique provider of nutrition care when it isconsistently used as a systematic method to think critically andmake decisions to provide safe and effective care. ADA’s Nutri-tion Care Process will serve as a guide to develop scopes ofpractice and standards of practice (49,50). Therefore, the workgroup recommended that further work be done to use the Nu-trition Care Process to describe roles and functions that can beincluded in scopes of practice. In May 2003, the Board of Di-rectors of ADA established a Practice Definitions Task Forcethat will identify and differentiate the terms within the profes-sion that need clarification for members, affiliates, and DPGsrelated to licensure, certification, practice acts, and advancedpractice. This task force is also charged to clarify the scope ofpractice services, clinical privileges, and accountabilities pro-vided by RDs/DTRs based on education, training, and experi-ence.
Education of Dietetics StudentsIt will be important to review the current CADE EducationalStandards to ensure that the language and level of expectedcompetencies are consistent with the entry-level practice of
OF PROFESSIONAL INTEREST
1070 / August 2003 Volume 103 Number 8Edition: 2006 10

the Nutrition Care Process. Further work by the Commissionon Dietetic Registration (CDR) may need to be done to makerevisions on the RD and DTR exams to evaluate entry-levelcompetencies needed to practice nutrition care in this way.Revision of texts and other educational materials will also needto incorporate the key principles and steps of this new process(51).
Education and Credentialing of MembersEven though dietetics professionals currently provide nutritioncare, this standardized Nutrition Care Process includes somenew principles, concepts, and guidelines in each of its steps.This is especially true of steps 2 and 4 (Nutrition Diagnosis andNutrition Monitoring and Evaluation). Therefore, the implica-tions for education of dietetics professionals and their practiceare great. Because a large number of dietetics professionals stillare employed in health care systems, a comprehensive educa-tional plan will be essential. A model to be considered whenplanning education is the one used to educate dietetics profes-sionals on the Professional Development Portfolio (PDP) Pro-cess (52). Materials that could be used to provide memberswith the necessary knowledge and skills in this process couldinclude but not be limited to the following:■ articles in the Journal of the American Dietetic Associa-tion;■ continuing professional education lectures and presentationsat affiliate and national meetings;■ self-study materials; case studies, CD-ROM workbooks, andothers;■ hands-on workshops and training programs;■ Web-based materials; and■ inclusion in the learning needs assessment and codes of theProfessional Development Portfolio.
Through the development of this educational strategic plan,the benefits to dietetics professionals and other stakeholderswill need to be a central theme to promote the change in prac-tice that comes with using this process to provide nutritioncare.
Evidence-Based PracticeThe pressure to do more with less is dramatically affecting all ofhealth care, including dietetics professionals. This pressure isforcing the health care industry to restructure to be more effi-cient and cost-effective in delivering care. It will require the useof evidenced-based practice to determine what practices arecritical to support outcomes (53,54). The Nutrition Care Pro-cess will be invaluable as research is completed to evaluate theservices provided by dietetics professionals (55). The NutritionCare Process will provide the structure for developing themethodology and data collection in individual settings, and thepractice-based research networks ADA is in the process of ini-tiating.
Standardized LanguageAs noted in Step 2 (Nutrition Diagnosis), having a standardtaxonomy for nutrition diagnosis would be beneficial. Work inthe area of articulating the types of interventions used by die-tetics professionals has already begun by the Definitions WorkGroup under the direction of ADA’s Research Committee. Fur-ther work to define terms that are part of the Nutrition CareProcess will need to continue. Even though the work groupprovided a list of terms relating to the definition and key con-cepts of the process, there are opportunities to articulate fur-
ther terms that are consistently used in this process. The Boardof Directors of ADA in May 2003 approved continuation andexpansion of a task force to address a comprehensive systemthat includes a process for developing and validating standard-ized language for nutrition diagnosis, intervention, and out-comes.
SUMMARYJust as maps are reissued when new roads are built and riverschange course, this Nutrition Care Process and Model reflectsrecent changes in the nutrition and health care environment. Itprovides dietetics professionals with the updated “road map” tofollow the best path for high-quality patient/client/group-cen-tered nutrition care.
References1. American Dietetic Association Strategic Plan. Available at: http://eatright.org(member only section). Accessed June 2, 2003.2. Wheeler D. Understanding Variation: The Key to Managing Chaos. 2nd ed.Knoxville, TN: SPC Press; 2000.3. Shojania KG, Duncan BW, McDonald KM, Wachter RM. Making HealthCare Safer: A Critical Analysis of Patient Safety Practices. Evidence Report/Technology Assessment No. 43 (Prepared by the University of California atSan Francisco-Stanford Evidence-based Practice Center under Contract No.290-97-0013). Rockville, MD: Agency for Healthcare Research and Quality;2001. Report No.: AHRQ Publication No. 01-E058.4. Potter, Patricia A, Perry, Anne G. Basic Nursing Theory and Practice. 4thed. St Louis: C.V. Mosby; 1998.5. American Physical Therapy Association. Guide to Physical Therapist Prac-tice. 2nd ed. Alexandria, VA; 2001.6. The Guide to Occupational Therapy Practice. Am J Occup Ther. 1999;53:3.Available at http://nweb.pct.edu/homepage/student/NUNJOL02/ot%20process.ppt. Accessed May 30, 2003.7. Kohn KN, ed. Medicare: A strategy for Quality Assurance, Volume I. Com-mittee to Design a Strategy for Quality Review and Assurance in Medicare.Washington, DC: Institute of Medicine. National Academy Press; 1990.8. Kohn L, Corrigan J, Donaldson M, eds. To Err Is Human: Building a SaferHealth System. Washington, DC: Committee on Quality of Health Care inAmerica, Institute of Medicine. National Academy Press; 2000.9. Institute of Medicine. Crossing the Quality Chasm: A New Health System forthe 21st Century. Committee on Quality in Health Care in America. RonaBriere, ed. Washington, DC: National Academy Press; 2001.10. Splett P. Developing and Validating Evidence-Based Guides for Practice:A Tool Kit for Dietetics Professionals. American Dietetic Association; 1999.11. Endres JB. Community Nutrition. Challenges and Opportunities. UpperSaddle River, NJ: Prentice-Hall, Inc; 1999.12. Splett P. Planning, Implementation and Evaluation of Nutrition Programs.In: Sharbaugh CO, ed. Call to Action: Better Nutrition for Mothers, Children,and Families. Washington, DC: National Center for Education in Maternal andChild Health (NCEMCH); 1990.13. Batalden PB, Stoltz PA. A framework for the continual improvement ofhealth care: Building and applying professional and improvement knowledgeto test changes in daily work. Jt Comm J Qual Improv. 1993;19:424-452.14. CADE Accreditation Handbook. Available at: http://www.eatright.com/cade/standards.html. Accessed March 20, 2003.15. Alfaro-LeFevre R. Nursing process overview. Applying Nursing Process.Promoting Collaborative Care. 5th ed. Lippincott; 2002.16. Grant A, DeHoog S. Nutrition Assessment Support and Management.Northgate Station, WA; 1999.17. Sandrick, K. Is nutritional diagnosis a critical step in the nutrition careprocess? J Am Diet Assoc. 2002;102:427-431.18. King LS. What is a diagnosis? JAMA. 1967;202:154.19. Doenges ME. Application of Nursing Process and Nursing Diagnosis: AnInteractive Text for Diagnostic Reasoning, 3rd ed. Philadelphia, PA: FA DavisCo; 2000.20. Gallagher-Alred C, Voss AC, Gussler JD. Nutrition intervention and patientoutcomes: a self-study manual. Columbus, OH: Ross Products Division,Abbott Laboratories; 1995.21. Splett P, Myers EF. A proposed model for effective nutrition care. J AmDiet Assoc. 2001;101:357-363.22. Lacey K, Cross N. A problem-based nutrition care model that is diagnosticdriven and allows for monitoring and managing outcomes. J Am Diet Assoc.2002;102:578-589.23. Brylinsky C. The Nutrition Care Process. In: Mahan K, Escott-Stump S,
OF PROFESSIONAL INTEREST
Journal of THE AMERICAN DIETETIC ASSOCIATION / 1071Edition: 2006 11

eds. Krause’s Food, Nutrition and Diet Therapy, 10th ed. Philadelphia, PA:W.B. Saunders Company; 2000:431-451.24. Hammond MI, Guthrie HA. Nutrition clinic: An integrated component of anundergraduate curriculum. J Am Diet Assoc. 1985;85:594.25. Final MNT Regulations. CMS-1169-FC. Federal Register, November 1,2001. Department of Health and Human Services. 42 CFR Parts: 405, 410,411, 414, and 415. Available at: http://cms.hhs.gov/physicians/pfs/cms1169fc.asp. Accessed June 27, 2003.26. Commission on Dietetic Registration CDR Certifications and State Licen-sure. Available at: http://www.cdrnet.org/certifications/index.htm. AccessedMay 30, 2003.27. Medicare Coverage Policy Decision: Duration and Frequency of the Med-ical Nutrition Therapy (MNT) Benefit (No. CAG-00097N). Available at: http://cms.hhs.gov/ncdr/memo.asp?id�53. Accessed June 2, 2003.28. American Dietetic Association Medical Nutrition Therapy Evidence-BasedGuides For Practice. Hyperlipidemia Medical Nutrition Therapy Protocol. CD-ROM; 2001.29. American Dietetic Association. Medical Nutrition Therapy Evidence-Based Guides for Practice. Nutrition Practice Guidelines for Type 1 and 2Diabetes Mellitus CD-ROM; 2001.30. American Dietetic Association. Medical Nutrition Therapy Evidence-Based Guides for Practice. Nutrition Practice Guidelines for Gestational Dia-betes Mellitus. CD-ROM; 2001.31. American Dietetic Association Medical Nutrition Therapy Evidence-BasedGuides For Practice. Chronic Kidney Disease (non-dialysis) Medical NutritionTherapy Protocol. CD-ROM; 2002.32. Gates G. Ethics opinion: Dietetics professionals are ethically obligated tomaintain personal competence in practice. J Am Diet Assoc. May 2003;103:633-635.33. Code of Ethics for the Profession of Dietetics. J Am Diet Assoc. 1999;99:109-113.34. US Preventive Services Task Force. Guide to Clinical Preventive Services,2nd ed. Washington, DC: US Department of Health and Human Services,Office of Disease Prevention and Health Promotion; 1996.35. Identifying patients at risk: ADA’s definitions for nutrition screening andnutrition assessment. J Am Diet Assoc. 1994;94:838-839.36. Donabedian A. Explorations in Quality Assessment and Monitoring. Vol-ume I: The Definition of Quality and Approaches to Its Assessment. Ann Arbor,MI: Health Administration Press; 1980.37. Carey RG, Lloyd RC. Measuring Quality Improvement in Health Care: AGuide to Statistical Process Control Applications. New York, Quality Re-sources; 1995.38. Eck LH, Slawson DL, Williams R, Smith K, Harmon-Clayton K, Oliver D. Amodel for making outcomes research standard practice in clinical dietetics.J Am Diet Assoc. 1998;98:451-457.39. Ireton-Jones CS, Gottschlich MM, Bell SJ. Practice-Oriented NutritionResearch: An Outcomes Measurement Approach. Gaithersburg, MD: AspenPublishers, Inc.; 1998.40. Kaye GL. Outcomes Management: Linking Research to Practice. Colum-bus, OH: Ross Products Division, Abbott Laboratories; 1996.41. Splett P. Cost Outcomes of Nutrition Intervention, a Three Part Mono-graph. Evansville, IN: Mead Johnson & Company; 1996.
42. Plsekk P. 1994. Tutorial: Planning for data collection part I: Asking theright question. Qual Manage Health Care. 2:76-81.43. American Dietetic Association. Israel D, Moore S, eds. Beyond NutritionCounseling: Achieving Positive Outcomes Through Nutrition Therapy. 1996.44. Stoline AM, Weiner JP. The New Medical Marketplace: A Physician’sGuide to the Health Care System in the 1990s. Baltimore: Johns HopkinsPress; 1993.45. Mathematica Policy Research, Inc. Best Practices in Coordinated CareMarch 22, 2000. Available at: http://www.mathematica-mpr.com/PDFs/bestpractices.pdf. Accessed February 22, 2003.46. Bisognano MA. New skills needed in medical leadership: The key toachieving business results. Qual Prog. 2000;33:32-41.47. Smith R. Expanding medical nutrition therapy: An argument for evidence-based practices. J Am Diet Assoc. 2003;103:313-314.48. National Council of State Boards of Nursing Model Nursing Practice Act.Available at: http://www.ncsbn.org/public/regulation/nursing_practice_model_practice_act.htm. Accessed June 27, 2003.49. Professional policies of the American College of Medical Quality (ACMQ).Available at: http://www.acmq.org/profess/list.htm. Accessed June 27, 2003.50. American Dietetic Association. Standards of professional practice. J AmDiet Assoc. 1998;98:83-85.51. O’Neil EH and the Pew Health Professions Commission. RecreatingHealth Professional Practice for a New Century. The Fourth Report of the PewHealth Professions Commission. Pew Health Professions Commission; De-cember 1998.52. Weddle DO. The professional development portfolio process: Settinggoals for credentialing. J Am Diet Assoc. 2002;102:1439-1444.53. Sackett DL, Rosenberg WMC, Gray J, Haynes RB, Richardson WS.Evidence based medicine: What it is and what it isn’t. Br Med J. 1996;312:71-72.54. Myers EF, Pritchett E, Johnson EQ. Evidence-based practice guides vs.protocols: What’s the difference? J Am Diet Assoc. 2001;101:1085-1090.55. Manore MM, Myers EF. Research and the dietetics profession: Making abigger impact. J Am Diet Assoc. 2003;103:108-112.
The Quality Management Committee Work Group devel-oped the Nutrition Care Process and Model with inputfrom the House of Delegates dialog (October 2002 HODmeeting, in Philadelphia, PA). The work group membersare the following: Karen Lacey, MS, RD, Chair; ElviraJohnson, MS, RD; Kessey Kieselhorst, MPA, RD; Mary JaneOakland, PhD, RD, FADA; Carlene Russell, RD, FADA; Pa-tricia Splett, PhD, RD, FADA; Suzanne Bertocchi, DTR,and Tamara Otterstein, DTR; Ellen Pritchett, RD; EstherMyers, PhD, RD, FADA; Harold Holler, RD, and KarriLooby, MS, RD. The work group would like to extend aspecial thank you to Marion Hammond, MS, and NaoimiTrossler, PhD, RD, for their assistance in development ofthe Nutrition Care Process and Model.
OF PROFESSIONAL INTEREST
1072 / August 2003 Volume 103 Number 8Edition: 2006 12

American Dietetic Association’s Standardized Nutrition Language: Current Status
Introduction Evidence-based dietetic practice relies on
concise, consistent, and standardized terminology to create and retrieve digital sources of evidence.1 This is essential for documenting nutrition diagnoses, interventions and outcomes in electronic health records. A task force of the American Dietetic Association (ADA) has begun to refine and disseminate standardized nutrition language. The language is built on the Nutrition Care Process and Model that maps quality nutrition care and outcomes, and recognizes several existing terminologies used by other health professions. This paper will describe the logic model for the development of the standardized nutrition language, the Nutrition Care Process it is built upon, and its current status.
The project goal is to support nutrition practice, education, research, and policy with data. It is assumed that practicing Dietitians, educators, and researchers will use the standardized nutrition language to document care, aggregate data, and study the evidence. Standardized terminology will provide the foundation for developing a national dietitian care database.
The Nutrition Care ProcessThe ADA Nutrition Care Model workgroup
published the Nutrition Care Process (NCP) and Model in August 2003.2 It provides a definition of the NCP, describes its steps and framework. The NCP is “a systematic problem-solving method that dietetics professionals use to critically think and make decisions to address nutrition related problems and provide safe and effective quality nutrition care.”2, p1063 The four steps of the NCP, similar to those of other clinical professions, are: a) Nutrition Assessment, b) Nutrition Diagnosis, c) Nutrition Intervention, and d) Nutrition Monitoring and Evaluation. Allowing for the reality of an iterative and comprehensive clinical process, the NCP is not linear and it includes, but is not limited to, Medical Nutrition Therapy. Medical Nutrition Therapy is “nutritional diagnostic, therapy, and counseling services for the purpose of disease management, which are furnished by a registered dietitian or nutrition professional.”3 The context of the NCP and surrounding influences are captured in the Model framework.
Standardized terms are being developed for each step of the NCP. Nutrition Assessment is “a systematic process of obtaining, verifying, and interpreting data in order to make decisions about the nature and cause of nutrition-related problems.”2, p1064
The Nutrition Assessment includes signs and symptoms. Nutrition Diagnosis is “the identification and labeling that describes an actual occurrence, risk of, or potential for developing a nutritional problem that dietetics professionals are responsible for treating independently.” 2, p.1065
Nutrition Interventions are “purposely planned actions designed with the intent of changing a nutrition-related behavior, risk factor, environmental condition, or aspect of health status for an individual, target group, or the community at large.”2, p.1066
Interventions are directed to influence the etiology or effects of a diagnosis. Nutrition Monitoring is “the review and measurement of the patient/client/group’s status at a scheduled (preplanned) follow-up point with regard to the nutrition diagnosis, intervention plans/goals, and outcomes.” Evaluation is “the systematic comparison of current findings with previous status, intervention goals, or a reference standard.”2, p.1067 Evaluation may measure changes in signs and symptoms. The NCP steps guide the delivery of nutrition health services, education, and research and define categories for documentation of nutrition care.
Development: Comparison with Nursing In comparison with the development of
various nursing terminologies, the ADA nutrition language development has been much more rapid and centralized, due perhaps to comparatively smaller numbers of nutrition professionals and growing sophistication in information technology. Nursing terminologies work began in the 1970s, including the North American Nursing Diagnosis (NANDA)4 terminology, the Clinical Care Classification (CCC),5 and others. NANDA is specific to nursing diagnosis, while the CCC addresses diagnoses, interventions, and outcomes. The Nursing Minimum Data Set6 which includes patient information, nursing diagnoses, nursing interventions, nursing outcomes, intensity level of nursing care, and a unique provider number is an over-arching framework for the various discrete nursing terminologies, similar to the NCP.
Edition: 2006
Portions of this document have been submitted for publication elsewhere
13

Why Does Dietetics Practice Need a Standardized Language?
There is currently no agreed upon mechanism by which dietetics professionals can communicate with each other or other healthcare professionals. Because of this lack of agreement, there is no easy way to classify, measure, and report on the outcomes of nutrition interventions in various patient populations. The Nutrition Care Process includes nutrition diagnosis and nutrition intervention as unique steps that provide Registered Dietitians a mechanism to consistently document and communicate the work of dietetics[13]. There is currently no agreed upon terminology used in dietetics practice making it impossible to gather and aggregate data needed for research, education, and reimbursement justification via outcomes analysis.
Logic Model
A Logic Model is a simplified picture that describes the logical relationships among the resources invested, the activities that take place, and the benefits to be realized from the project and the environment in which the system/project occurs. With the help of an informatics consultant, the Standardized Language Task Force adopted a Project Logic Model that identifies the expected outcomes and impact of the Standardized Language of Dietetics. The goal of the dietetics terminology was seen to be "To provide data to foster nutrition practice, education, research, and policy". Three time frames for evaluating the impact of the standardized language were agreed upon. The most immediate impacts were thought to include recommendations for coordination with existing terminologies, review of the structure of the dietetics terminology, to "cross-walk" the new terminology with existing terminologies to see if overlap exists, to review existing intervention terms, and to identify relevant policy issues regarding standardized nutrition language. Intermediate impacts were thought to include selection of a structure for the nutrition diagnostic labels, cross-walk of the intervention terms, to plan for generation of nutrition outcomes measures, create strategies for ongoing maintenance and updates of the language, to design and implement pilot testing of the standardized language, and to draft legislative and policy agendas. The ultimate impact was agreed to include delivery of quality, cost-effective nutrition care, national growth of nutrition care, inclusion of the standardized language in dietetics education and research, development of a national data warehouse for nutrition research, and support of policies designed to foster nutrition practice, education, and research.
Several assumptions were necessary in development of this logic model. The Task Force was in agreement that nutrition is an essential component of high quality health care. There was heightened awareness of the need for data to document the processes and outcomes of nutrition care in a variety of settings. It was also assumed that educators, practicing dietitians, and researchers would accept and implement the standardized language and would be willing to share data using the terminology for targeted studies and ultimately a national database.
Nutrition Diagnostic Labels To date, over 60 Nutrition Diagnostic Labels
have been defined by ADA work with focus groups, domain experts, and membership committees. Standardized Language Task Force members judged the match between nutrition diagnoses terms and similar terms listed in the National Library of Medicine’s Unified Medical Language System (UMLS); many terms have synonyms. One of the robust terminologies in the UMLS is SNOMED-CT. Staff from SNOMED-CT were contacted to discuss the process of submitting nutrition terms.
The Nutrition Diagnostic Labels include 3 domains: Clinical, Behavioral-Environmental, and Intake. The domains, sub-classes, and specific diagnoses are defined in the most recent version, a summary of which follows.11
DOMAIN: INTAKE Defined as “actual problems related to intake of energy, nutrients, fluids, bioactive substances through oral diet or nutrition support (enteral or parenteral nutrition)” Class: Caloric Energy Balance Defined as “actual or estimated changes in energy (kcal)”Class: Oral or Nutrition Support Intake Defined as “actual or estimated food and beverage intake from oral diet or nutrition support compared with patient goal” Class: Fluid Intake Balance Defined as “actual or estimated fluid intake compared with patient goal” Class: Bioactive Substances Balance Defined as “actual or observed intake of bioactive substances, including single or multiple functional food components, ingredients, dietary supplements, alcohol”Class: Nutrient Balance Defined as “actual or estimated intake of specific nutrient groups or single nutrients as compared with desired levels” Sub-Class: Fat and Cholesterol Balance
Edition: 2006
Portions of this document have been submitted for publication elsewhere
14

Sub-Class: Protein Balance) Sub-Class: Carbohydrate and Fiber Balance Sub-Class: Vitamin Balance
Sub-Class: Mineral BalanceDOMAIN: CLINICAL
Defined as “nutritional findings/problems identified that relate to medical or physical conditions” Class: Functional Balance Defined as “change in physical or mechanical functioning that interferes with or prevents desired nutritional consequences” Class: Biochemical Balance Defined as “change in capacity to metabolize nutrients as a result of medications, surgery, or as indicated by altered lab values” Class: Weight Balance Defined as “chronic weight or changed weight status when compared with usual or desired body weight”
DOMAIN: BEHAVIORAL-ENVIRONMENTAL
Defined as “nutritional findings/problems identified that relate to knowledge, attitudes/beliefs, physical environment, or access to food and food safety” Class: Knowledge and Beliefs Defined as “actual knowledge and beliefs as reported, observed, or documented” Class: Physical Activity Balance and Function Defined as “actual physical activity, self-care, and quality of life problems as reported, observed or documented” Class: Food Safety and Access Defined as “actual problems with food access or food safety” © ADA
Problem-Etiology-Signs/Symptoms Statements A Nutrition Diagnosis is best written as a PES
statement pertaining to one patient/client or group, specific to one problem (P) and one etiology (E), and based on assessment of signs and symptoms (S).2
Implementation of PES statements in clinical practice is being tested in two pilot studies by ADA members. Examples of PES statements are a)”Overweight/obesity (problem) related to continued intake of high fat foods (etiology) resulting in ~300 extra kcal/day as evidenced by a BMI of 30(sign/symptom), and b) Impaired ability to prepare foods/meals (problem) related to fatigue (etiology) as evidenced by patient/client only consuming one meal per day.”11 Interventions are often guided by the etiology of each problem. Signs and symptoms may provide measures to evaluate outcomes and the effectiveness of care. It is possible that the standardized terms for assessments will be considered relevant outcome measures.
Nutrition Interventions Following principles for standardized
terminologies,12 the ADA has begun to identify and define Nutrition Intervention terms. A Task Force meeting in February 2005 identified categories of interventions including: Treatments/Procedures, Education, Counseling, and Referral/ Coordination. These categories are similar to those in nursing terminologies but differing by not including monitoring/assessment as an intervention, which is a separate step in the Nutrition Care Process. Synonyms to the intervention terms will be searched in the UMLS and domain experts will judge the extent of the matches. The Nutrition Intervention Labels will be submitted SNOMED-CT or other existing coding system that will be included in the UMLS.
Future Work Definition of Nutrition Assessment terms and
their relationship with Outcome terms is planned. In addition, activities to communicate the standardized language to educators, administrators, clinicians, and researchers are planned. The ADA believes that consistent standardized terminology will improve patient care by enhancing the education, practice, and research of nutrition professionals. The use of standardized nutrition language by nutrition professionals in the U.S. is in synch with similar international efforts.
References 1. Bakken S. An informatics infrastructure is essential for evidence-based practice. JAMIA2001;8:199-201. 2. Lacey K, Pritchett E. Nutrition care process and model: ADA adopts road map to quality care and outcomes management. JADA. 2003 Aug; 103 (8):1061-72. 3. Final Medical Nutrition Therapy regulations. CMS-1169-FC. Federal Register, Nov.1, 2001. DHHS 42 CFR Parts: 405, 410, 411, 414, and 415. Retrieved Mar. 7, 2005 from http://cms.hhs.gov/physicians/pfs/cms1169fc.asp.4. North American Nursing Diagnosis Association. Retrieved Mar. 7, 2005 from http://www.nanda.org/5. Saba V (2005). Clinical Care Classification System. Retrieved Mar. 7, 2005 from http://www.sabacare.com6. Werley H, Lang NM. Identification of the nursing minimum data set. New York: Springer, 1988. 7. Alternative Billing Codes. Retrieved Mar. 7, 2005 from http://www.alternativelink.com/ali/home/
Edition: 2006
Portions of this document have been submitted for publication elsewhere
15

8. National Library of Medicine (2005). Unified Medical Language System. Retrieved Mar. 7, 2005 from http://www.nlm.nih.gov/research/umls/umlsmain.html9. College of American Pathologists. SNOMED CT. Skokie, IL: author, 2005. Retrieved Mar. 7, 2005 from http://www.snomed.org/10. Logical Observation Identifiers Names and Codes. Retrieved Mar. 7, 2005 from http://www.loinc.org/11. Escott-Stump S, Hutson V, Lacey K, Myers E, Oakland MJ, Splett P. Nutrition Diagnosis: What’s In It For My Practice? JADA in press 2005. 12. Cimino JJ. Desiderata for Controlled Medical Vocabularies in the Twenty-First Century. Methods of Information in Medicine; 1998;37:394-403
Edition: 2006
Portions of this document have been submitted for publication elsewhere
16

Introduction to nutrition diagnoses/problems: The new component of the nutrition care process
Introduction
The ADA has embarked on an extensive project to identify and define nutrition diagnoses/problems for the profession of dietetics. This standardized language of nutrition diagnoses/problems is an integral component in the Nutrition Care Process, a process designed to improve the consistency and quality of individualized patient/client care and the predictability of the patient/client outcomes. In fact, several other allied professional, including nursing, physical therapy, and occupational therapy, utilize defined care processes (1).
Not only will creating this standard language help dietetic professionals better document their nutrition care, it will serve to help achieve Association strategic goals of promoting demand for dietetic professionals and help them be more competitive in the market place. It will also provide a minimum data set and common data elements for future research that includes services of dietetic professionals.
ADA’s Standardized Language Task Force developed a conceptual framework for the standardized nutrition language and identified the nutrition diagnoses/problems. The framework outlines the domains within which the diagnoses/problems would fall and the flow of the nutrition care process in relation to the continuum of health, disease and disability. Sixty-twodiagnoses/problems have been identified. A worksheet has been developed for each diagnosis/problem and expert has been incorporated.
The methodology for developing sets of terms such as these includes systematically collecting data from multiple sources simultaneously. We collected data from a selected group of dietitians prior to starting the project (from ADA recognized leaders and award winners), from the 12 member task force during the development, from several small group discussions (community, ambulatory, acute care, and long term care) and from expert researcher reviewers.
The methodology for continued development and refinement of these terms has been identified. As with the ongoing updating of the American Medical Association CPT codes, these will also be published on an annual basis. The process to submit your suggested changes is included in this packet. In addition, the terms have been included in one ongoing research project in an ambulatory setting. A second descriptive research study identifying the use of the terms will be planned and conducted through the Dietetics Practice Based Research Network in 2005-2006. As each of the research studies are completed their findings will be incorporated into future versions of these terms. Future iterations and changes to the diagnoses/problems and the worksheets are expected as this standard language evolves. Once the initial research is completed we will formally submit these terms to become part of nationally recognized health care databases. We have already begun the dialogue with these groups to let them know the direction that we are headed and to keep them appraised of our progress.
Edition: 2006 17
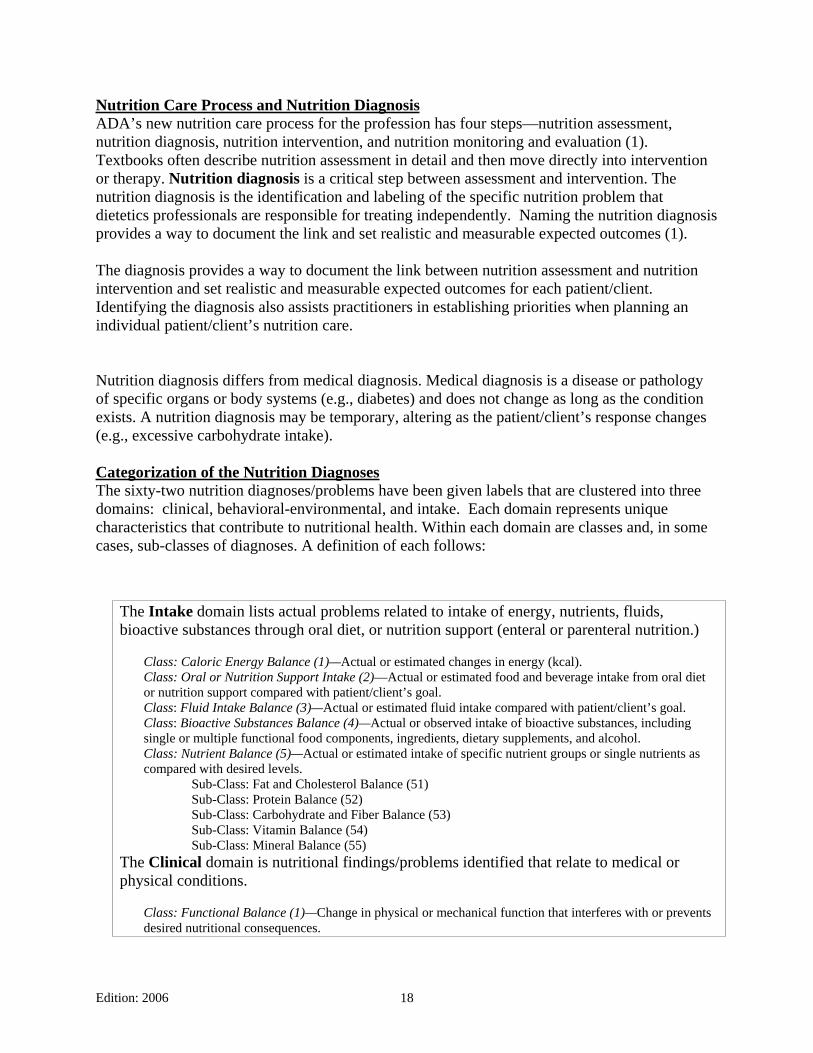
Nutrition Care Process and Nutrition DiagnosisADA’s new nutrition care process for the profession has four steps—nutrition assessment, nutrition diagnosis, nutrition intervention, and nutrition monitoring and evaluation (1). Textbooks often describe nutrition assessment in detail and then move directly into intervention or therapy. Nutrition diagnosis is a critical step between assessment and intervention. The nutrition diagnosis is the identification and labeling of the specific nutrition problem that dietetics professionals are responsible for treating independently. Naming the nutrition diagnosis provides a way to document the link and set realistic and measurable expected outcomes (1).
The diagnosis provides a way to document the link between nutrition assessment and nutrition intervention and set realistic and measurable expected outcomes for each patient/client. Identifying the diagnosis also assists practitioners in establishing priorities when planning an individual patient/client’s nutrition care.
Nutrition diagnosis differs from medical diagnosis. Medical diagnosis is a disease or pathology of specific organs or body systems (e.g., diabetes) and does not change as long as the condition exists. A nutrition diagnosis may be temporary, altering as the patient/client’s response changes (e.g., excessive carbohydrate intake).
Categorization of the Nutrition DiagnosesThe sixty-two nutrition diagnoses/problems have been given labels that are clustered into three domains: clinical, behavioral-environmental, and intake. Each domain represents unique characteristics that contribute to nutritional health. Within each domain are classes and, in some cases, sub-classes of diagnoses. A definition of each follows:
The Intake domain lists actual problems related to intake of energy, nutrients, fluids, bioactive substances through oral diet, or nutrition support (enteral or parenteral nutrition.)
Class: Caloric Energy Balance (1)—Actual or estimated changes in energy (kcal). Class: Oral or Nutrition Support Intake (2)—Actual or estimated food and beverage intake from oral diet or nutrition support compared with patient/client’s goal. Class: Fluid Intake Balance (3)—Actual or estimated fluid intake compared with patient/client’s goal. Class: Bioactive Substances Balance (4)—Actual or observed intake of bioactive substances, including single or multiple functional food components, ingredients, dietary supplements, and alcohol.
Class: Nutrient Balance (5)—Actual or estimated intake of specific nutrient groups or single nutrients as compared with desired levels. Sub-Class: Fat and Cholesterol Balance (51) Sub-Class: Protein Balance (52) Sub-Class: Carbohydrate and Fiber Balance (53) Sub-Class: Vitamin Balance (54) Sub-Class: Mineral Balance (55) The Clinical domain is nutritional findings/problems identified that relate to medical or physical conditions.
Class: Functional Balance (1)—Change in physical or mechanical function that interferes with or prevents desired nutritional consequences.
Edition: 2006 18
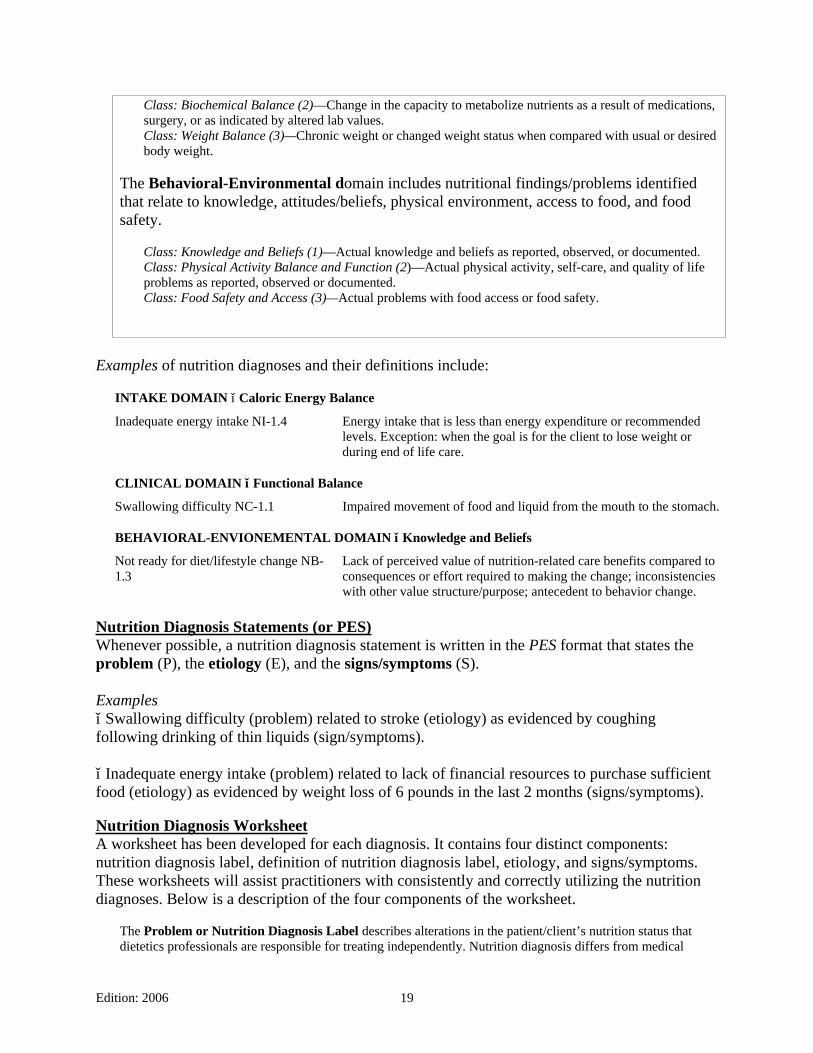
Class: Biochemical Balance (2)—Change in the capacity to metabolize nutrients as a result of medications, surgery, or as indicated by altered lab values.
Class: Weight Balance (3)—Chronic weight or changed weight status when compared with usual or desired body weight.
The Behavioral-Environmental domain includes nutritional findings/problems identified that relate to knowledge, attitudes/beliefs, physical environment, access to food, and food safety.
Class: Knowledge and Beliefs (1)—Actual knowledge and beliefs as reported, observed, or documented. Class: Physical Activity Balance and Function (2)—Actual physical activity, self-care, and quality of life problems as reported, observed or documented.
Class: Food Safety and Access (3)—Actual problems with food access or food safety.
Examples of nutrition diagnoses and their definitions include:
INTAKE DOMAIN Caloric Energy Balance
Inadequate energy intake NI-1.4 Energy intake that is less than energy expenditure or recommended levels. Exception: when the goal is for the client to lose weight or during end of life care.
CLINICAL DOMAIN Functional Balance
Swallowing difficulty NC-1.1 Impaired movement of food and liquid from the mouth to the stomach.
BEHAVIORAL-ENVIONEMENTAL DOMAIN Knowledge and Beliefs
Not ready for diet/lifestyle change NB-1.3
Lack of perceived value of nutrition-related care benefits compared to consequences or effort required to making the change; inconsistencies with other value structure/purpose; antecedent to behavior change.
Nutrition Diagnosis Statements (or PES)Whenever possible, a nutrition diagnosis statement is written in the PES format that states the problem (P), the etiology (E), and the signs/symptoms (S).
Examples Swallowing difficulty (problem) related to stroke (etiology) as evidenced by coughing
following drinking of thin liquids (sign/symptoms).
Inadequate energy intake (problem) related to lack of financial resources to purchase sufficient food (etiology) as evidenced by weight loss of 6 pounds in the last 2 months (signs/symptoms).
Nutrition Diagnosis Worksheet A worksheet has been developed for each diagnosis. It contains four distinct components: nutrition diagnosis label, definition of nutrition diagnosis label, etiology, and signs/symptoms. These worksheets will assist practitioners with consistently and correctly utilizing the nutrition diagnoses. Below is a description of the four components of the worksheet.
The Problem or Nutrition Diagnosis Label describes alterations in the patient/client’s nutrition status that dietetics professionals are responsible for treating independently. Nutrition diagnosis differs from medical
Edition: 2006 19

diagnosis in that a nutrition diagnosis changes as the patient/client response changes. The medical diagnosis does not change as long as the disease or condition exists. A nutrition diagnosis allows the dietetics professional to identify realistic and measurable outcomes, formulate interventions, and monitor and evaluate change.
The Definition of Nutrition Diagnosis Label briefly describes the Nutrition Diagnosis Label to differentiate a discrete problem area.
The Etiology (Cause/Contributing Risk Factors) are those factors contributing to the existence of, or maintenance of pathophysiological, psychosocial, situational, developmental, cultural, and/or environmental problems. It is linked to the diagnosis label by the words “related to.”
The Signs/Symptoms (Defining Characteristics) consist of subjective and/or objective data used to determine whether the patient/client has the nutrition diagnosis specified. These are the signs and symptoms gathered through nutrition assessment. It is linked to the etiology by the words “as evidenced by.”
Organization of Data in Signs/Symptoms (Defining Characteristics) Dietetics professionals use clinical judgment to determine the nutrition diagnosis based on data collected from the first step of the nutrition care process: nutrition assessment. Therefore, the items listed in the signs/symptoms (defining characteristics) are organized according to nutrition assessment category.
Nutrition assessment is the systematic process for obtaining, verifying, and interpreting data needed to make decisions about the nature and cause of the nutrition-related problem. The process of nutrition assessment consists of collecting biochemical data, anthropometric measurements, physical examination findings, food/nutrition history, and client history. On the nutrition diagnosis worksheet, the signs/symptoms are classified by nutrition assessment categories.
Biochemical Data include laboratory data, for example, electrolytes, glucose, Hemoglobin A1C, thyroid, and lipid panel.
Anthropometric Measurements include, for instance, height, weight, body mass index (BMI), growth rate, and rate of weight change.
Nutrition-Focused Physical Examination includes oral health, general physical appearance, muscle and subcutaneous fat wasting, and affect.
Food and Nutrition History consists of four areas: Food consumption, nutrition and health awareness and management, physical activity and exercise, and food availability.
Food consumption may include factors such as, food and nutrient intake, meal and snack patterns, environmental cues to eating, and current diets and/or food modifications.
Nutrition and health awareness and management includes, for example, knowledge and beliefs about nutrition recommendations, self-monitoring/management practices, and past nutrition counseling and education.
Physical activity and exercise consists of activity patterns, amount of sedentary time (e.g., TV, phone, computer), and exercise intensity, frequency, and duration.
Food availability encompasses factors such as, food planning, purchasing, preparation abilities and limitations, food safety practices, food/nutrition program utilization, and food insecurity.
Edition: 2006 20

Client History consists of four areas: Medication and supplement history, social history, medical/health history, and personal history.
Medication and supplement history includes, for instance, prescription and over the counter drugs, herbal and dietary supplements, and illegal drugs.
Social history may include items, such as, socioeconomic status, social and medical support, cultural and religious beliefs, housing situation, and social isolation/connection.
Medical/health history includes chief nutrition complaint, present/past illness, disease or complication risk, family medical history, mental/emotional health, and cognitive abilities.
Personal history consists of factors including age, occupation, role in family, and education level.
SummaryNutrition diagnosis is the critical link in the nutrition care process between assessment and intervention. Interventions can then be clearly targeted to address either the etiology or signs and symptoms of the specific nutrition diagnosis/problem identified. Using a standardized terminology for identifying the nutrition diagnosis/problem will make one aspect of the critical thinking that dietetics professionals do visible to other professionals as well as provide a clear method of communicating among dietetics professionals. Implementation of a standard language throughout the profession, with tools to assist practitioners, will make this bold initiative a success. Ongoing input is critical as the standardized language is created to ensure a proper foundation for its future implementation.
Reference1. Lacey K, Pritchett E. Nutrition care process and model: ADA adopts road map to quality care and outcomes management. J Am Diet Assoc. 2003;103:1061-1072.
Edition: 2006 21

NUTRITION DIAGNOSTIC TERMINOLOGY
INTAKE NI Defined as “actual problems related to intake of energy, nutrients, fluids, bioactive substances through oral diet or nutrition support”
Caloric Energy Balance (1) Defined as “actual or estimated changes in energy (kcal)”
Hypermetabolism NI-1.1 (Increased energy needs)
Increased energy expenditure NI-1.2 Hypometabolism NI-1.3
(Decreased energy needs) Inadequate energy intake NI-1.4 Excessive energy intake NI-1.5
Oral or Nutrition Support Intake (2) Defined as “actual or estimated food and beverage intake from oral diet or nutrition support compared with patient goal”
Inadequate oral food/ NI-2.1 beverage intake
Excessive oral food/ NI-2.2 beverage intake
Inadequate intake from NI-2.3 enteral/parenteral nutrition infusion
Excessive intake from NI-2.4 enteral/parenteral nutrition
Inappropriate infusion of NI-2.5 enteral/parenteral nutrition (use with caution)
Fluid Intake (3) Defined as “actual or estimated fluid intake compared against patient goal”
Inadequate fluid intake NI-3.1Excessive fluid intake NI-3.2
Bioactive Substances (4) Defined as “actual or observed intake of bioactive substances, including single or multiple functional food components, ingredients, dietary supplements, alcohol”
Inadequate bioactive NI-4.1 substance intake
Excessive bioactive NI-4.2 substance intake
Excessive alcohol intake NI-4.3
Nutrient (5) Defined as “actual or estimated intake of specific nutrient groups or single nutrients as compared with desired levels”
Increased nutrient needs NI-5.1 (specify) ___________________________
Evident protein- energy NI-5.2 malnutrition
Inadequate protein- NI-5.3 energy intake
Decreased nutrient needs NI-5.4 (specify) ___________________________
Edition: 2006 22
Imbalance of nutrients NI-5.5
Fat and Cholesterol (51) Inadequate fat intake NI-51.1 Excessive fat intake NI-51.2 Inappropriate intake NI-51.3
of food fats (specify) ______________________ Protein (52)
Inadequate protein intake NI-52.1 Excessive protein intake NI-52.2 Inappropriate intake NI-52.3
of amino acids (specify) ______________________ Carbohydrate and Fiber Intake (53)
Inadequate carbohydrate NI-53.1 intake
Excessive carbohydrate NI-53.2 intake
Inappropriate intake of NI-53.3 types of carbohydrate (specify) ______________________
Inconsistent NI-53.4 carbohydrate intake
Inadequate fiber intake NI-53.5 Excessive fiber intake NI-53.6
Vitamin Intake (54) Inadequate vitamin NI-54.1
intake (specify) _________________ Excessive vitamin NI-54.2
intake (specify) _________________ A CThiamin DRiboflavin ENiacin KFolate Other _______
Mineral Intake (55) Inadequate mineral intake NI-55.1
(specify) Calcium IronPotassium Zinc Other __________
Excessive mineral intake NI-55.2 (specify)
Calcium IronPotassium Zinc Other __________
CLINICAL NC Defined as “nutritional findings/problems identified as related to medical or physical conditions”
Functional (1) Defined as “change in physical or mechanical functioning that interferes with or prevents desired nutritional consequences”
Swallowing difficulty NC-1.1 Chewing (masticatory) difficulty NC-1.2 Breastfeeding difficulty NC-1.3 Altered GI function NC-1.4
Biochemical (2) Defined as “change in capacity to metabolize nutrients as a result of medications, surgery, or as indicated by altered lab values”
Impaired nutrient utilization NC-2.1 Altered nutrition-related NC-2.2
laboratory values Food medication interaction NC-2.3
Weight (3) Defined as “chronic weight or changed weight status when compared with usual or desired body weight”
Underweight NC-3.1 Involuntary weight loss NC-3.2 Overweight/obesity NC-3.3 Involuntary weight gain NC-3.4
BEHAVIORAL- ENVIRONMENTAL NB Defined as “nutritional findings/problems identified as related to knowledge, attitudes/beliefs, physical environment, or food supply and safety”
Knowledge and Beliefs (1) Defined as “actual knowledge and beliefs as observed or documented”
Food and nutrition-related NB-1.1 knowledge deficit
Harmful beliefs/attitudes NB-1.2 about food or nutrition- related topics (use with caution)
Not ready for diet/ NB-1.3 lifestyle change
Self monitoring deficit NB-1.4 Disordered eating pattern NB-1.5 Limited adherence to nutrition- NB-1.6
related recommendations Undesirable food choices NB-1.7
Physical Activity and Function (2) Defined as “actual physical activity, self-care, and quality of life problems as reported, observed or documented”
Physical inactivity NB-2.1 Excessive exercise NB-2.2 Inability or lack of desire NB-2.3
to manage self care Impaired ability to NB-2.4
prepare foods/meals Poor nutrition quality of life NB-2.5 Self-feeding difficulty NB-2.6
Food Safety and Access (3) Defined as “actual problems with food access or food safety”
Intake of unsafe food NB-3.1Limited access to food NB-3.2
#1 Problem ____________________________________________________________________________________________________________ Etiology ____________________________________________________________________________________________________________ Signs/Symptoms _____________________________________________________________________________________________________#2 Problem ____________________________________________________________________________________________________________ Etiology ____________________________________________________________________________________________________________ Signs/Symptoms _____________________________________________________________________________________________________#3 Problem ____________________________________________________________________________________________________________ Etiology ____________________________________________________________________________________________________________ Signs/Symptoms ___________________________________________________________________________________________
Date Identified Date Resolved

NU
TR
ITIO
N D
IAG
NO
SIS
TE
RM
S A
ND
DE
FIN
ITIO
NS
Nu
trit
ion
Dia
gn
os
tic
Te
rm
Te
rm
Nu
mb
er
De
fin
itio
n o
f D
iag
no
sti
c T
erm
Re
fere
nc
e
Sh
ee
t
Pa
ge
Nu
mb
ers
DO
MA
IN:
IN
TA
KE
Defi
ned
as “
actu
al p
rob
lem
s r
ela
ted
to
inta
ke o
f en
erg
y, n
utr
ien
ts, fl
uid
s, b
ioacti
ve
su
bsta
nces t
hro
ug
h o
ral d
iet
or
nu
trit
ion
su
pp
ort
(e
nte
ral o
r p
are
nte
ral n
utr
itio
n)”
NI
Cla
ss:
Cal
ori
c E
ner
gy
Bal
ance
(1)
D
efin
ed a
s “a
ctu
al o
r es
tim
ated
ch
ang
es in
en
erg
y (k
cal)
”
Hyp
erm
etab
olis
m (
Incr
ease
d en
ergy
nee
ds)
NI-
1.1
Res
ting
met
abol
ic r
ate
(RM
R)
abov
e pr
edic
ted
requ
irem
ents
due
to
str
ess,
trau
ma,
inju
ry, s
epsi
s, o
r di
seas
e. N
ote:
RM
R is
the
sum
of m
etab
olic
pro
cess
es o
f act
ive
cell
mas
s re
late
d to
the
mai
nten
ance
of n
orm
al b
ody
func
tions
and
reg
ulat
ory
bala
nce
durin
g re
st.
1-2
Incr
ease
d en
ergy
exp
endi
ture
NI-
1.2
Res
ting
met
abol
ic r
ate
(RM
R)
abov
e pr
edic
ted
requ
irem
ents
due
to
bod
y co
mpo
sitio
n, m
edic
atio
ns, e
ndoc
rine,
neu
rolo
gic,
or
gene
tic c
hang
es. N
ote:
RM
R is
the
sum
of m
etab
olic
pro
cess
es
of a
ctiv
e ce
ll m
ass
rela
ted
to th
e m
aint
enan
ce o
f nor
mal
bod
y fu
nctio
ns a
nd r
egul
ator
y ba
lanc
e du
ring
rest
.
3
Hyp
omet
abol
ism
(D
ecre
ased
ene
rgy
need
s)N
I-1.
3 R
estin
g m
etab
olic
rat
e (R
MR
) be
low
pre
dict
ed r
equi
rem
ents
due
to
bod
y co
mpo
sitio
n, m
edic
atio
ns, e
ndoc
rine,
neu
rolo
gic,
or
gene
tic c
hang
es
4-5
Inad
equa
te e
nerg
y in
take
NI-
1.4
Ene
rgy
inta
ke th
at is
less
than
ene
rgy
expe
nditu
re, e
stab
lishe
d re
fere
nce
stan
dard
s, o
r re
com
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
. E
xcep
tion:
whe
n th
e go
al is
wei
ght l
oss
or
6-7
Edi
tion:
200
6 23
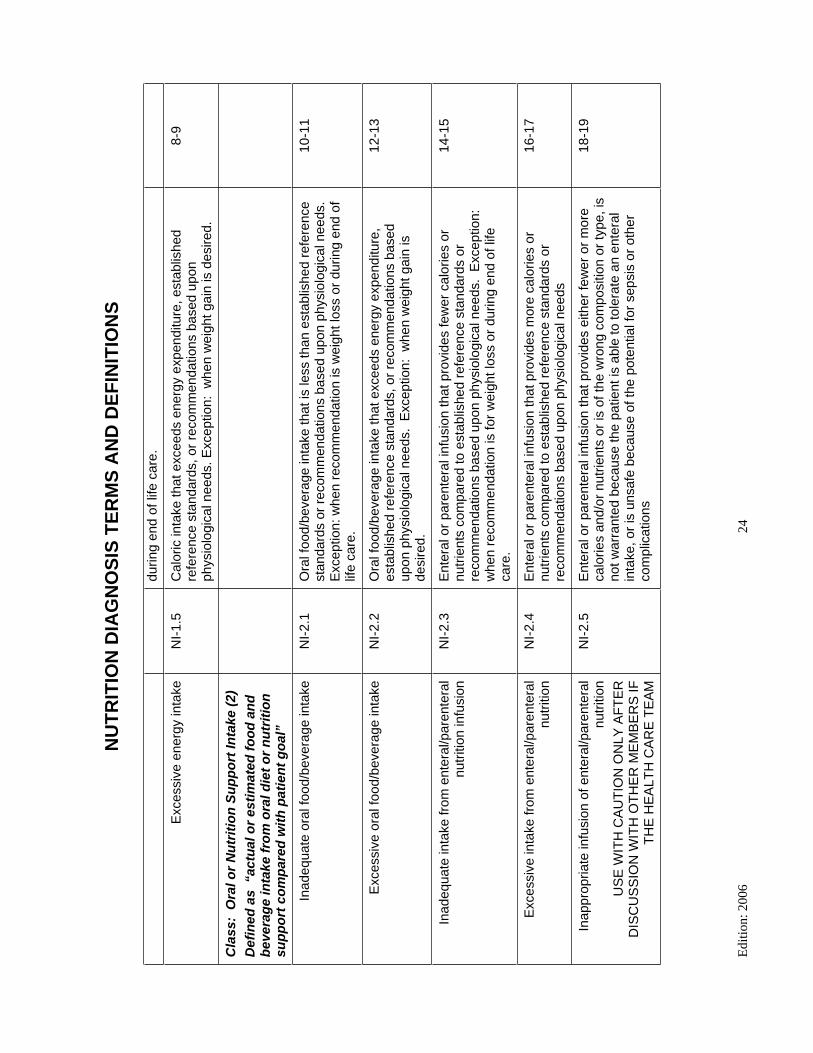
NU
TR
ITIO
N D
IAG
NO
SIS
TE
RM
S A
ND
DE
FIN
ITIO
NS
durin
g en
d of
life
car
e.
Exc
essi
ve e
nerg
y in
take
NI-
1.5
Cal
oric
inta
ke th
at e
xcee
ds e
nerg
y ex
pend
iture
, est
ablis
hed
refe
renc
e st
anda
rds,
or
reco
mm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds. E
xcep
tion:
whe
n w
eigh
t gai
n is
des
ired.
8-9
Cla
ss:
Ora
l or
Nu
trit
ion
Su
pp
ort
Inta
ke (
2)
Def
ined
as
“ac
tual
or
esti
mat
ed f
oo
d a
nd
b
ever
age
inta
ke f
rom
ora
l die
t o
r n
utr
itio
n
sup
po
rt c
om
par
ed w
ith
pat
ien
t g
oal
”
Inad
equa
te o
ral f
ood/
beve
rage
inta
keN
I-2.
1O
ral f
ood/
beve
rage
inta
ke th
at is
less
than
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
. E
xcep
tion:
whe
n re
com
men
datio
n is
wei
ght l
oss
or d
urin
g en
d of
lif
e ca
re.
10-1
1
Exc
essi
ve o
ral f
ood/
beve
rage
inta
keN
I-2.
2O
ral f
ood/
beve
rage
inta
ke th
at e
xcee
ds e
nerg
y ex
pend
iture
, es
tabl
ishe
d re
fere
nce
stan
dard
s, o
r re
com
men
datio
ns b
ased
up
on p
hysi
olog
ical
nee
ds.
Exc
eptio
n: w
hen
wei
ght g
ain
is
desi
red.
12-1
3
Inad
equa
te in
take
from
ent
eral
/par
ente
ral
nutr
ition
infu
sion
NI-
2.3
Ent
eral
or
pare
nter
al in
fusi
on th
at p
rovi
des
few
er c
alor
ies
or
nutr
ient
s co
mpa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
re
com
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
. E
xcep
tion:
w
hen
reco
mm
enda
tion
is fo
r w
eigh
t los
s or
dur
ing
end
of li
fe
care
.
14-1
5
Exc
essi
ve in
take
from
ent
eral
/par
ente
ral
nutr
ition
NI-
2.4
Ent
eral
or
pare
nter
al in
fusi
on th
at p
rovi
des
mor
e ca
lorie
s or
nu
trie
nts
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or
reco
mm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
16-1
7
Inap
prop
riate
infu
sion
of e
nter
al/p
aren
tera
l nu
triti
onU
SE
WIT
H C
AU
TIO
N O
NLY
AF
TE
R
DIS
CU
SS
ION
WIT
H O
TH
ER
ME
MB
ER
S IF
T
HE
HE
ALT
H C
AR
E T
EA
M
NI-
2.5
Ent
eral
or
pare
nter
al in
fusi
on th
at p
rovi
des
eith
er fe
wer
or
mor
e ca
lorie
s an
d/or
nut
rient
s or
is o
f the
wro
ng c
ompo
sitio
n or
type
, is
not w
arra
nted
bec
ause
the
patie
nt is
abl
e to
tole
rate
an
ente
ral
inta
ke, o
r is
uns
afe
beca
use
of th
e po
tent
ial f
or s
epsi
s or
oth
er
com
plic
atio
ns
18-1
9
Edi
tion:
200
6 24

NU
TR
ITIO
N D
IAG
NO
SIS
TE
RM
S A
ND
DE
FIN
ITIO
NS
Cla
ss:
Flu
id In
take
(3)
D
efin
ed a
s “a
ctu
al o
r es
tim
ated
flu
id in
take
co
mp
ared
wit
h p
atie
nt
go
al”
Inad
equa
te fl
uid
inta
keN
I-3.
1Lo
wer
inta
ke o
f flu
id c
onta
inin
g fo
ods
or s
ubst
ance
s co
mpa
red
to
esta
blis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
up
on p
hysi
olog
ical
nee
ds
20-2
1
Exc
essi
ve fl
uid
inta
keN
I-3.
2H
ighe
r in
take
of f
luid
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
22
-23
Cla
ss:
Bio
acti
ve S
ub
stan
ces
(4)
Def
ined
as
“act
ual
or
ob
serv
ed in
take
of
bio
acti
ve s
ub
stan
ces,
incl
ud
ing
sin
gle
or
mu
ltip
le f
un
ctio
nal
fo
od
co
mp
on
ents
, in
gre
die
nts
, die
tary
su
pp
lem
ents
, alc
oh
ol”
Inad
equa
te b
ioac
tive
subs
tanc
e in
take
NI-
4.1
Low
er in
take
of b
ioac
tive
subs
tanc
es c
onta
inin
g fo
ods
or
subs
tanc
es c
ompa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
re
com
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
24-2
5
Exc
essi
ve b
ioac
tive
subs
tanc
e in
take
NI-
4.2
Hig
her
inta
ke o
f bio
activ
e su
bsta
nces
oth
er th
an tr
aditi
onal
nu
trie
nts,
suc
h as
func
tiona
l foo
ds, b
ioac
tive
food
com
pone
nts,
di
etar
y su
pple
men
ts, f
ood
conc
entr
ates
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
26-2
7
Exc
essi
ve a
lcoh
ol in
take
NI-
4.3
Inta
ke a
bove
the
sugg
este
d lim
its fo
r al
coho
l 28
-29
Cla
ss:
Nu
trie
nt
(5)
D
efin
ed a
s “a
ctu
al o
r es
tim
ated
inta
ke o
f sp
ecif
ic n
utr
ien
t g
rou
ps
or
sin
gle
nu
trie
nts
as
co
mp
ared
wit
h d
esir
ed le
vels
”
Incr
ease
d nu
trie
nt (
spec
ify)
need
sN
I-5.
1 In
crea
sed
need
for
a sp
ecifi
c nu
trie
nt c
ompa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed u
pon
30-3
1
Edi
tion:
200
6 25

NU
TR
ITIO
N D
IAG
NO
SIS
TE
RM
S A
ND
DE
FIN
ITIO
NS
phys
iolo
gica
l nee
ds
Evi
dent
pro
tein
-ene
rgy
mal
nutr
ition
NI-
5.2
Inad
equa
te in
take
of p
rote
in a
nd/o
r en
ergy
32
-33
Inad
equa
te p
rote
in-e
nerg
y in
take
NI-
5.3
Inad
equa
te in
take
of p
rote
in a
nd/o
r en
ergy
com
pare
d to
es
tabl
ishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed
upon
phy
siol
ogic
al n
eeds
of s
hort
or
rece
nt d
urat
ion
34-3
5
Dec
reas
ed n
utrie
nt (
spec
ify)
need
sN
I-5.
4 D
ecre
ased
nee
d fo
r a
spec
ific
nutr
ient
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
36-3
7
Imba
lanc
e of
nut
rient
sN
I-5.
5 A
n un
desi
rabl
e co
mbi
natio
n of
inge
sted
nut
rient
s, s
uch
that
the
amou
nt o
f one
nut
rient
inge
sted
inte
rfer
es w
ith o
r al
ters
ab
sorp
tion
and/
or u
tiliz
atio
n of
ano
ther
nut
rient
38-3
9
S
ub
-Cla
ss:
Fat
an
d C
ho
lest
ero
l (5
1)
Inad
equa
te fa
t int
ake
NI-
51.1
Low
er fa
t int
ake
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or
reco
mm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds. E
xcep
tion:
w
hen
reco
mm
enda
tion
is fo
r w
eigh
t los
s or
dur
ing
end
of li
fe
care
.
40
Exc
essi
ve fa
t int
ake
NI-
51.2
Hig
her
fat i
ntak
e co
mpa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
re
com
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
41
-42
Inap
prop
riate
inta
ke o
f foo
d fa
ts (
spec
ify)
NI-
51.3
In
take
of w
rong
type
or
qual
ity o
f foo
d fa
ts c
ompa
red
to
esta
blis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
up
on p
hysi
olog
ical
nee
ds
43-4
4
S
ub
-Cla
ss:
Pro
tein
(52
)
Inad
equa
te p
rote
in in
take
NI-
52.1
Low
er in
take
of p
rote
in c
onta
inin
g fo
ods
or s
ubst
ance
s co
mpa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed
upon
phy
siol
ogic
al n
eeds
45
Exc
essi
ve p
rote
in in
take
NI-
52.2
Inta
ke a
bove
the
reco
mm
ende
d le
vel a
nd/o
r ty
pe o
f pro
tein
co
mpa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
46
-47
Edi
tion:
200
6 26

NU
TR
ITIO
N D
IAG
NO
SIS
TE
RM
S A
ND
DE
FIN
ITIO
NS
reco
mm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
Inap
prop
riate
inta
ke o
f am
ino
acid
s (s
peci
fy)
NI-
52.3
Inta
ke th
at is
mor
e or
less
than
rec
omm
ende
d le
vel a
nd/o
r ty
pe
of a
min
o ac
ids
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or
reco
mm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
48-4
9
S
ub
-Cla
ss:
Car
bo
hyd
rate
an
d
Fib
er (
53)
Inad
equa
te c
arbo
hydr
ate
inta
keN
I-53
.1Lo
wer
inta
ke o
f car
bohy
drat
e co
ntai
ning
food
s or
sub
stan
ces
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or
reco
mm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
50
Exc
essi
ve c
arbo
hydr
ate
inta
keN
I-53
.2In
take
abo
ve th
e re
com
men
ded
leve
l and
type
of c
arbo
hydr
ate
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or
reco
mm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
51-5
2
Inap
prop
riate
inta
ke o
f typ
es o
f car
bohy
drat
e (s
peci
fy)
NI-
53.3
Inta
ke o
r th
e ty
pe o
r am
ount
of c
arbo
hydr
ate
that
is a
bove
or
belo
w th
e es
tabl
ishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
ba
sed
upon
phy
siol
ogic
al n
eeds
53-5
4
Inco
nsis
tent
car
bohy
drat
e in
take
NI-
53.4
Inco
nsis
tent
tim
ing
of c
arbo
hydr
ate
inta
ke th
roug
hout
the
day,
da
y to
day
, or
a pa
ttern
of c
arbo
hydr
ate
inta
ke th
at is
not
co
nsis
tent
with
rec
omm
ende
d pa
ttern
bas
ed u
pon
phys
iolo
gica
l ne
eds
55-5
6
Inad
equa
te fi
ber
inta
keN
I-53
.5Lo
wer
inta
ke o
f fib
er c
onta
inin
g fo
ods
or s
ubst
ance
s co
mpa
red
to
esta
blis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
up
on p
hysi
olog
ical
nee
ds
57-5
8
Exc
essi
ve fi
ber
inta
keN
I-53
.6H
ighe
r in
take
of f
iber
con
tain
ing
food
s or
sub
stan
ces
com
pare
d to
rec
omm
enda
tions
bas
ed u
pon
patie
nt/c
lient
con
ditio
n
59-6
0
S
ub
-Cla
ss:
Vit
amin
(54
)
Inad
equa
te v
itam
in in
take
(sp
ecify
)N
I-54
.1
Low
er in
take
of v
itam
in c
onta
inin
g fo
ods
or s
ubst
ance
s co
mpa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed
upon
phy
siol
ogic
al n
eeds
61-6
3
Edi
tion:
200
6 27

NU
TR
ITIO
N D
IAG
NO
SIS
TE
RM
S A
ND
DE
FIN
ITIO
NS
Exc
essi
ve v
itam
in in
take
(sp
ecify
)N
I-54
.2
Hig
her
inta
ke o
f vita
min
con
tain
ing
food
s or
sub
stan
ces
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or
reco
mm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
64-6
5
S
ub
-Cla
ss:
Min
eral
(55
)
Inad
equa
te m
iner
al in
take
(sp
ecify
)N
I-55
.1
Low
er in
take
of m
iner
al c
onta
inin
g fo
ods
or s
ubst
ance
s co
mpa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
re
com
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
66-6
7
Exc
essi
ve m
iner
al in
take
NI-
55.2
Hig
her
inta
ke o
f min
eral
from
food
s, s
uppl
emen
ts, m
edic
atio
ns o
r w
ater
, com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or
reco
mm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
68-6
9
DO
MA
IN:
CL
INIC
AL
Defi
ned
as “
nu
trit
ion
al fi
nd
ing
s/p
rob
lem
s
iden
tifi
ed
th
at
rela
te t
o m
ed
ical o
r p
hys
ical
co
nd
itio
ns
”
NC
Cla
ss:
Fu
nct
ion
al (
1)
Def
ined
as
“ch
ang
e in
ph
ysic
al o
r m
ech
anic
al f
un
ctio
nin
g t
hat
inte
rfer
es w
ith
o
r p
reve
nts
des
ired
nu
trit
ion
al
con
seq
uen
ces”
Sw
allo
win
g di
fficu
ltyN
C-1
.1
Impa
ired
mov
emen
t of f
ood
and
liqui
d fr
om th
e m
outh
to th
e st
omac
h 70
Che
win
g (m
astic
ator
y) d
iffic
ulty
NC
-1.2
Im
paire
d ab
ility
to m
anip
ulat
e or
mas
ticat
e fo
od fo
r sw
allo
win
g 71
-73
Bre
astfe
edin
g di
fficu
ltyN
C-1
.3
Inab
ility
to s
usta
in n
utrit
ion
thro
ugh
brea
stfe
edin
g 74
-75
Alte
red
GI f
unct
ion
NC
-1.4
Cha
nges
in a
bilit
y to
dig
est o
r ab
sorb
nut
rient
s 76
-77
Cla
ss:
Bio
chem
ical
(2)
D
efin
ed a
s “c
han
ge
in c
apac
ity
to
met
abo
lize
nu
trie
nts
as
a re
sult
of
Edi
tion:
200
6 28

NU
TR
ITIO
N D
IAG
NO
SIS
TE
RM
S A
ND
DE
FIN
ITIO
NS
med
icat
ion
s, s
urg
ery,
or
as in
dic
ated
by
alte
red
lab
val
ues
” Impa
ired
nutr
ient
util
izat
ion
NC
-2.1
C
hang
es in
abi
lity
to a
bsor
b or
met
abol
ize
nutr
ient
s an
d bi
oact
ive
subs
tanc
es
78-7
9
Alte
red
nutr
ition
-rel
ated
labo
rato
ry v
alue
s N
C-2
.2C
hang
es in
abi
lity
to e
limin
ate
by-p
rodu
cts
of d
iges
tive
and
met
abol
ic p
roce
sses
80
-81
Foo
d m
edic
atio
n in
tera
ctio
nN
C-2
.3
Und
esira
ble/
harm
ful i
nter
actio
n(s)
bet
wee
n fo
od a
nd o
ver
the
coun
ter
(OT
C)
med
icat
ions
, pre
scrib
ed m
edic
atio
ns, h
erba
ls,
bota
nica
ls, a
nd/o
r di
etar
y su
pple
men
ts th
at d
imin
ishe
s,
enha
nces
, or
alte
rs e
ffect
of n
utrie
nts
and/
or m
edic
atio
ns
82-8
3
Cla
ss:
Wei
gh
t (3
) D
efin
ed a
s “c
hro
nic
wei
gh
t o
r ch
ang
ed
wei
gh
t st
atu
s w
hen
co
mp
ared
wit
h u
sual
or
des
ired
bo
dy
wei
gh
t”
Und
erw
eigh
tN
C-3
.1
Low
bod
y w
eigh
t com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or
reco
mm
enda
tions
84
-85
Invo
lunt
ary
wei
ght l
oss
NC
-3.2
Dec
reas
e in
bod
y w
eigh
t tha
t is
not p
lann
ed o
r de
sire
d 86
-87
Ove
rwei
ght/o
besi
tyN
C-3
.3
Incr
ease
d ad
ipos
ity c
ompa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
88
-89
Invo
lunt
ary
wei
ght g
ain
NC
-3.4
W
eigh
t gai
n ab
ove
that
whi
ch is
des
ired
or e
xpec
ted
90-9
1
DO
MA
IN:
BE
HA
VIO
RA
L-
EN
VIR
ON
ME
NT
AL
Defi
ned
as “
nu
trit
ion
al fi
nd
ing
s/p
rob
lem
s
iden
tifi
ed
th
at
rela
te t
o k
no
wle
dg
e,
att
itu
des/b
eliefs
, p
hys
ical en
vir
on
men
t, o
r
access t
o f
oo
d a
nd
fo
od
safe
ty”
NB
Cla
ss:
Kn
ow
led
ge
and
Bel
iefs
(1)
Edi
tion:
200
6 29

NU
TR
ITIO
N D
IAG
NO
SIS
TE
RM
S A
ND
DE
FIN
ITIO
NS
Def
ined
as
“act
ual
kn
ow
led
ge
and
bel
iefs
as
rep
ort
ed, o
bse
rved
, or
do
cum
ente
d”
Foo
d an
d nu
triti
on-r
elat
ed k
now
ledg
e de
ficit
NB
-1.1
In
com
plet
e or
inac
cura
te k
now
ledg
e ab
out f
ood,
nut
ritio
n or
nu
triti
on-r
elat
ed in
form
atio
n an
d gu
idel
ines
e.g
. nut
rient
re
quire
men
ts, c
onse
quen
ces
of fo
od b
ehav
iors
, life
sta
ge
requ
irem
ents
, nut
ritio
n re
com
men
datio
ns, d
isea
ses
and
cond
ition
s, p
hysi
olog
ical
func
tion,
or
prod
ucts
92-9
3
Har
mfu
l bel
iefs
/atti
tude
s ab
out f
ood
or
nutr
ition
-rel
ated
topi
csU
SE
WIT
H C
AU
TIO
N T
O B
E S
EN
SIT
IVE
TO
P
AT
IEN
T C
ON
CE
RN
S
NB
-1.2
Bel
iefs
/atti
tude
s an
d pr
actic
es a
bout
food
, nut
ritio
n, a
nd n
utrit
ion-
rela
ted
topi
cs th
at a
re in
com
patib
le w
ith s
ound
nut
ritio
n pr
inci
ples
, nut
ritio
n ca
re o
r di
seas
e/co
nditi
on
94-9
5
Not
rea
dy fo
r di
et/li
fest
yle
chan
geN
B-1
.3
Lack
of p
erce
ived
val
ue o
f nut
ritio
n-re
late
d ca
re b
enef
its
com
pare
d to
con
sequ
ence
s or
effo
rt r
equi
red
to m
akin
g th
e ch
ange
; inc
onsi
sten
cies
with
oth
er v
alue
str
uctu
re/p
urpo
se;
ante
cede
nt to
beh
avio
r ch
ange
96-9
7
Sel
f mon
itorin
g de
ficit
NB
-1.4
Lack
of d
ata
reco
rdin
g to
trac
k pe
rson
al p
rogr
ess
98-9
9
Dis
orde
red
eatin
g pa
ttern
NB
-1.5
Bel
iefs
, atti
tude
s, th
ough
ts a
nd b
ehav
iors
rel
ated
to fo
od, e
atin
g,
and
wei
ght m
anag
emen
t, in
clud
ing
clas
sic
eatin
g di
sord
ers
as
wel
l as
less
sev
ere,
sim
ilar
cond
ition
s th
at n
egat
ivel
y im
pact
he
alth
100-
102
Lim
ited
adhe
renc
e to
nut
ritio
n-re
late
d re
com
men
datio
nsN
B-1
.6La
ck o
f nut
ritio
n-re
late
d ch
ange
s as
per
inte
rven
tion
agre
ed u
pon
by c
lient
or
popu
latio
n 10
3-10
4
Und
esira
ble
food
cho
ices
NB
-1.7
F
ood
and/
or b
ever
age
choi
ces
that
are
inco
nsis
tent
with
US
R
ecom
men
ded
Die
tary
Inta
ke, U
S D
ieta
ry G
uide
lines
, or
with
the
Foo
d G
uide
Pyr
amid
or
with
targ
ets
defin
ed in
the
nutr
ition
pr
escr
iptio
n or
nut
ritio
n ca
re p
roce
ss
105-
106
Cla
ss:
Ph
ysic
al A
ctiv
ity
and
Fu
nct
ion
(2)
D
efin
ed a
s “a
ctu
al p
hys
ical
act
ivit
y, s
elf-
care
, an
d q
ual
ity
of
life
pro
ble
ms
as
Edi
tion:
200
6 30

NU
TR
ITIO
N D
IAG
NO
SIS
TE
RM
S A
ND
DE
FIN
ITIO
NS
rep
ort
ed, o
bse
rved
or
do
cum
ente
d”
Phy
sica
l ina
ctiv
ityN
B-2
.1Lo
w le
vel o
f act
ivity
/sed
enta
ry b
ehav
ior
to th
e ex
tent
that
it
redu
ces
ener
gy e
xpen
ditu
re a
nd im
pact
s he
alth
10
7-10
8
Exc
essi
ve e
xerc
ise
NB
-2.2
An
amou
nt o
f exe
rcis
e th
at e
xcee
ds th
at w
hich
is n
eces
sary
to
impr
ove
heal
th a
nd/o
r at
hlet
ic p
erfo
rman
ce
109-
110
Inab
ility
of l
ack
of d
esire
to m
anag
e se
lf ca
re
NB
-2.3
Lack
of c
apac
ity o
r un
will
ingn
ess
to im
plem
ent m
etho
ds to
su
ppor
t hea
lthfu
l foo
d an
d nu
triti
on-r
elat
ed b
ehav
ior
111-
112
Impa
ired
abili
ty to
pre
pare
food
s/m
eals
NB
-2.4
Cog
nitiv
e or
phy
sica
l im
pairm
ent t
hat p
reve
nts
prep
arat
ion
of
food
s/m
eals
11
3-11
4
Poo
r nu
triti
on q
ualit
y of
life
NB
-2.5
D
imin
ishe
d N
QO
L sc
ores
rel
ated
to fo
od im
pact
, sel
f-im
age,
ps
ycho
logi
cal f
acto
rs s
ocia
l/int
erpe
rson
al, p
hysi
cal,
or s
elf-
effic
acy
115-
116
Sel
f fee
ding
diff
icul
tyN
B-2
.6
Impa
ired
actio
ns to
pla
ce fo
od in
mou
th
117-
118
Cla
ss:
Fo
od
Saf
ety
and
Acc
ess
(3)
Def
ined
as
“act
ual
pro
ble
ms
wit
h f
oo
d
acce
ss o
r fo
od
saf
ety”
Inta
ke o
f uns
afe
food
NB
-3.1
Inta
ke o
f foo
d an
d/or
flui
ds in
tent
iona
lly o
r un
inte
ntio
nally
co
ntam
inat
ed w
ith to
xins
, poi
sono
us p
rodu
cts,
infe
ctio
us a
gent
s,
mic
robi
al a
gent
s, a
dditi
ves,
alle
rgen
s, a
nd/o
r ag
ents
of
biot
erro
rism
119-
120
Lim
ited
acce
ss to
food
NB
-3.2
Dim
inis
hed
abili
ty to
acq
uire
food
from
sou
rces
(e.
g. s
hopp
ing,
ga
rden
ing,
mea
l del
iver
y), d
ue to
fina
ncia
l con
stra
ints
, phy
sica
l im
pairm
ent,
care
give
r su
ppor
t, or
uns
afe
livin
g co
nditi
ons
(e.g
. cr
ime
hind
ers
trav
el to
gro
cery
sto
re).
Lim
itatio
n to
food
bec
ause
of
con
cern
s ab
out w
eigh
t or
agin
g.
121-
122
Edi
tion:
200
6 31

INTA
KE D
OMAI
N C
aloric
Ene
rgy B
alanc
e
HY
PE
RM
ET
AB
OL
ISM
(NI-
1.1)
De
fin
itio
n
Res
ting
met
abol
ic r
ate
(RM
R)
abov
e pr
edic
ted
requ
irem
ents
due
to s
tres
s, tr
aum
a, in
jury
, sep
sis,
or
dise
ase.
Not
e: R
MR
is th
e su
m o
f m
etab
olic
pro
cess
es o
f ac
tive
cell
mas
s re
late
d to
the
mai
nten
ance
of
norm
al b
ody
func
tions
and
reg
ulat
ory
bala
nce
duri
ng r
est.
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems:
Cat
abol
ic il
lnes
s
Infe
ctio
n
Seps
is
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a In
sulin
res
ista
nce
(dif
ficu
lt to
con
trol
blo
od g
luco
se)
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
min
atio
n F
indi
ngs
Feve
r
Incr
ease
d he
art r
ate
Incr
ease
d re
spir
ator
y ra
te
Mea
sure
d R
MR
> e
stim
ated
or
expe
cted
RM
R
Foo
d/N
utri
tion
His
tory
C
lient
His
tory
C
ondi
tions
ass
ocia
ted
with
a d
iagn
osis
or
trea
tmen
t of,
e.g
., A
IDS/
HIV
, bur
ns, c
hron
ic o
bstr
uctiv
e pu
lmon
ary
dise
ase,
hi
p/lo
ng b
one
frac
ture
, inf
ectio
n, s
urge
ry, t
raum
a, h
yper
thyr
oidi
sm (
pre-
or u
ntre
ated
), s
ome
canc
ers
(spe
cify
)
Med
icat
ions
ass
ocia
ted
with
R
MR
Edi
tion:
200
6 32

INTA
KE D
OMAI
N C
aloric
Ene
rgy B
alanc
e
HY
PE
RM
ET
AB
OL
ISM
(NI-
1.1)
Refe
ren
ces:
1.
Bitz
C, T
oubr
o S,
Lar
sen
TM
, Har
der
H, R
enni
e K
L, J
ebb
SA, A
stru
p A
. Inc
reas
ed 2
4 ho
ur e
nerg
y ex
pend
iture
in T
ype
2 di
abet
es m
ellit
us. D
iabe
tes
Car
e. 2
004;
27:2
416-
21.
2.
Dic
kers
on R
N, R
oth-
You
sey
L. M
edic
atio
n ef
fect
s on
met
abol
ic r
ate:
A s
yste
mat
ic r
evie
w. U
npub
lishe
d da
ta.
3.
Fran
kenf
ield
D, R
oth-
You
sey
L, C
omph
er C
. Com
pari
son
of p
redi
ctiv
e eq
uatio
ns to
mea
sure
d re
stin
g m
etab
olic
rat
e in
hea
lthy
nono
bese
and
obe
se in
divi
dual
s, a
sys
tem
atic
rev
iew
. In
pres
s
Edi
tion:
200
6 33

INTA
KE D
OMAI
N C
aloric
Ene
rgy B
alanc
e
INC
RE
AS
ED
EN
ER
GY
EX
PE
ND
ITU
RE
(N
I-1.
2)
De
fin
itio
n
Res
ting
met
abol
ic r
ate
(RM
R)
abov
e pr
edic
ted
requ
irem
ents
due
to b
ody
com
posi
tion,
med
icat
ions
, end
ocri
ne, n
euro
logi
c, o
r ge
netic
cha
nges
. Not
e: R
MR
is th
e su
m o
f m
etab
olic
pro
cess
es o
f ac
tive
cell
mas
s re
late
d to
the
mai
nten
ance
of
norm
al b
ody
func
tions
and
reg
ulat
ory
bala
nce
duri
ng r
est.
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems:
Ana
bolis
m o
r gr
owth
Vol
unta
ry o
r in
volu
ntar
y ph
ysic
al a
ctiv
ity/m
ovem
ent
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Uni
nten
tiona
l wei
ght l
oss
of 1
0% in
6 m
onth
s, 5
% in
1 m
onth
Evi
denc
e of
nee
d fo
r ac
cele
rate
d or
cat
ch u
p gr
owth
or
wei
ght g
ain
in c
hild
ren;
abs
ence
of
norm
al g
row
th
Incr
ease
d pr
opor
tiona
l lea
n bo
dy m
ass
Phy
sica
l Exa
min
atio
n F
indi
ngs
Mea
sure
d R
MR
> e
stim
ated
or
expe
cted
RM
R
Foo
d/N
utri
tion
His
tory
In
crea
sed
phys
ical
act
ivity
, e.g
., en
dura
nce
athl
ete
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
Park
inso
n’s
dise
ase,
cer
ebra
l pal
sy, A
lzhe
imer
’s d
isea
se, o
ther
de
men
tia
Refe
ren
ces:
1.
Fran
kenf
ield
D, R
oth-
You
sey
L, C
omph
er C
. Com
pari
son
of p
redi
ctiv
e eq
uatio
ns to
mea
sure
d re
stin
g m
etab
olic
rat
e in
hea
lthy
nono
bese
and
obe
se in
divi
dual
s, a
sys
tem
atic
rev
iew
. In
pres
s.
Edi
tion:
200
6 34

INTA
KE D
OMAI
N C
aloric
Ene
rgy B
alanc
e
HY
PO
ME
TA
BO
LIS
M(N
I-1.
3)
De
fin
itio
n
Res
ting
met
abol
ic r
ate
(RM
R)
belo
w p
redi
cted
req
uire
men
ts d
ue to
bod
y co
mpo
sitio
n, m
edic
atio
ns, e
ndoc
rine
, neu
rolo
gic,
or
gene
tic c
hang
es
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems:
Los
s of
lean
bod
y m
ass,
wei
ght l
oss
Med
icat
ions
, e.g
., m
idaz
olam
, pro
pran
alol
, glip
izid
e
End
ocri
ne c
hang
es, e
.g.,
hypo
thyr
oidi
sm
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a In
crea
sed
TSH
, dec
reas
ed T
4, T
3 (h
ypot
hyro
idis
m)
Ant
hrop
omet
ric
Dat
a D
ecre
ased
wei
ght o
r m
id-a
rm m
uscl
e ci
rcum
fere
nce
Wei
ght g
ain
(e.
g., h
ypot
hyro
idis
m)
Gro
wth
stu
ntin
g or
fai
lure
, bas
ed o
n N
atio
nal C
ente
r fo
r H
ealth
Sta
tistic
s (N
CH
S) g
row
th s
tand
ards
Phy
sica
l Exa
m F
indi
ngs
Dec
reas
ed o
r no
rmal
adi
pose
and
som
atic
pro
tein
sto
res
Mea
sure
d R
MR
< e
stim
ated
or
expe
cted
RM
R
Foo
d/N
utri
tion
His
tory
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
hypo
thyr
oidi
sm, a
nore
xia
nerv
osa,
mal
nutr
ition
, fai
lure
to
thri
ve, P
rade
r-W
illi s
yndr
ome,
hyp
oton
ic c
ondi
tions
Bra
dyca
rdia
, hyp
oten
sion
, de
crea
sed
bow
l mot
ility
, slo
w b
reat
hing
rat
e, lo
w b
ody
tem
pera
ture
(in
sig
nifi
cant
wei
ght l
oss)
Col
d in
tole
ranc
e, h
air
loss
, dec
reas
ed e
ndur
ance
, dif
ficu
lty c
once
ntra
ting,
dec
reas
ed li
bido
, fee
lings
of
anxi
ety/
depr
essi
on
Edi
tion:
200
6 35
INTA
KE D
OMAI
N C
aloric
Ene
rgy B
alanc
e
HY
PO
ME
TA
BO
LIS
M(N
I-1.
3)
Refe
ren
ces:
1.
Bro
zek
J. S
tarv
atio
n an
d nu
triti
onal
reh
abili
tatio
n; a
qua
ntita
tive
case
stu
dy. J
Am
Die
t Ass
oc. 1
952;
28:9
17-9
26.
2.
Col
lins
S. U
sing
mid
dle
uppe
r ar
m c
ircu
mfe
renc
e to
ass
ess
seve
re a
dult
mal
nutr
ition
dur
ing
fam
ine.
JA
MA
. 199
6;27
6:39
1-39
5.
3.
Det
zer
MJ,
Lei
tenb
erg
H, P
oehl
man
ET
, Ros
en J
C, S
ilber
g N
T, V
ara
LS.
Res
ting
met
abol
ic r
ate
in w
omen
with
bul
imia
ner
vosa
: a c
ross
sec
tiona
l and
trea
tmen
t stu
dy. A
m J
Clin
Nut
r.19
94;6
0:32
7-33
2.4.
D
icke
rson
RN
, Rot
h-Y
ouse
y L
. Med
icat
ion
effe
cts
on m
etab
olic
rat
e: A
sys
tem
atic
rev
iew
. Unp
ublis
hed
data
. 5.
Fr
anke
nfie
ld D
, Rot
h-Y
ouse
y L
, Com
pher
C. C
ompa
riso
n of
pre
dict
ive
equa
tions
to m
easu
red
rest
ing
met
abol
ic r
ate
in h
ealth
y no
nobe
se a
nd o
bese
indi
vidu
als,
a s
yste
mat
ic r
evie
w. I
n pr
ess.
6.
Ker
ruis
h K
P, O
’Con
ner
JO, H
umph
ries
IR
J, K
ohn
MR
, Cla
rke
SD, B
riod
y JN
, Tho
mso
n E
J, W
righ
t KA
, Gas
kin
KJ,
Bau
r L
A. B
ody
com
posi
tion
in a
dole
scen
ts w
ith a
nore
xia
nerv
osa.
Am
J C
lin
Nut
r. 2
002;
75:3
1-37
. 7.
M
ollin
ger
LA
, Spu
rr G
B, e
l Gha
til A
Z, B
arbo
riak
JS,
Roo
ney
CB
, Dav
idof
f D
D. D
aily
ene
rgy
expe
nditu
re a
nd b
asil
met
abol
ic r
ates
of
patie
nts
with
spi
nal c
ord
inju
ry. A
rch
Phy
s M
ed R
ehab
il.19
85;6
6:42
0-42
6.
8.
Oba
rzan
ek E
, Les
em M
D, J
imer
son
DC
. Res
ting
met
abol
ic r
ate
of a
nore
xia
nerv
osa
patie
nts
duri
ng w
eigh
t gai
n. A
m J
Clin
Nut
r. 1
994;
60:6
66-6
75.
9.
Pavl
ovic
M, Z
aval
ic M
, Cor
ovic
N, S
tilin
ovic
L, M
alin
ar M
. Los
s of
bod
y m
ass
in e
x pr
ison
ers
of w
ar. E
ur J
Cli
n N
utr.
199
3;47
:808
-814
.
Edi
tion:
200
6 36

INTA
KE D
OMAI
N C
aloric
Ene
rgy B
alanc
e
INA
DE
QU
AT
E E
NE
RG
Y I
NT
AK
E (
NI-
1.4)
De
fin
itio
n
Ene
rgy
inta
ke th
at is
less
than
ene
rgy
expe
nditu
re, e
stab
lishe
d re
fere
nce
stan
dard
s, o
r re
com
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
Exc
eptio
n: w
hen
the
goal
is w
eigh
t los
s or
dur
ing
end
of li
fe c
are.
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems:
Path
olog
ic o
r ph
ysio
logi
c ca
uses
whi
ch r
esul
t in
incr
ease
d en
ergy
req
uire
men
ts o
r de
crea
sed
abili
ty to
con
sum
e st
uffi
ness
ene
rgy,
e.g
., in
crea
sed
nutr
ient
ne
eds
due
to p
rolo
nged
cat
abol
ic il
lnes
s
Lac
k of
acc
ess
to f
ood
or a
rtif
icia
l nut
ritio
n, e
.g. e
cono
mic
con
stra
ints
, cul
tura
l or
relig
ious
pra
ctic
es r
estr
ictin
g fo
od g
iven
to e
lder
ly a
nd/o
r ch
ildre
n
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or d
isor
dere
d ea
ting
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a C
hol
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
min
atio
n F
indi
ngs
Wei
ght l
oss
Poor
den
titio
n
Edi
tion:
200
6 37

INTA
KE D
OMAI
N C
aloric
Ene
rgy B
alanc
e
INA
DE
QU
AT
E E
NE
RG
Y I
NT
AK
E (
NI-
1.4)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Insu
ffic
ient
ene
rgy
inta
ke f
rom
die
t com
pare
d to
nee
ds b
ased
on
estim
ated
or
mea
sure
d re
stin
g m
etab
olic
rat
e
Res
tric
tion
or o
mis
sion
of
ener
gy d
ense
foo
ds f
rom
die
t
Food
avo
idan
ce a
nd/o
r la
ck o
f in
tere
st in
foo
d
Inab
ility
to in
depe
nden
tly c
onsu
me
food
s/fl
uids
(di
min
ishe
d jo
int m
obili
ty o
f w
rist
, ha
nd, o
r di
gits
)
Pare
nter
al o
r en
tera
l nut
ritio
n in
suff
icie
nt to
mee
t nee
ds b
ased
on
estim
ated
or
mea
sure
d re
stin
g m
etab
olic
rat
e
Clie
nt H
isto
ry
Exc
essi
ve c
onsu
mpt
ion
of a
lcoh
ol o
r ot
her
drug
s th
at r
educ
e hu
nger
Refe
ren
ces:
1 N
atio
nal A
cade
my
of S
cien
ces,
Ins
titut
e of
Med
icin
e. D
ieta
ry R
efer
ence
Int
akes
for
Ene
rgy,
Car
bohy
drat
e, F
iber
, Fat
, Fat
ty A
cids
, Cho
lest
erol
, Pro
tein
, and
Am
ino
Aci
ds. W
ashi
ngto
n, D
C:
Nat
iona
l Aca
dem
y Pr
ess;
200
2.
Edi
tion:
200
6 38

INTA
KE D
OMAI
N C
aloric
Ene
rgy B
alanc
e
EX
CE
SS
IVE
EN
ER
GY
IN
TA
KE
(N
I-1.
5)
De
fin
itio
n
Cal
oric
inta
ke th
at e
xcee
ds e
nerg
y ex
pend
iture
, est
ablis
hed
refe
renc
e st
anda
rds,
or
reco
mm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds. E
xcep
tion:
whe
n w
eigh
t ga
in is
des
ired
.
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems:
Har
mfu
l bel
iefs
/atti
tude
s ab
out f
ood,
nut
ritio
n, a
nd n
utri
tion-
rela
ted
topi
cs
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Lac
k of
acc
ess
to h
ealth
ful f
ood
choi
ces,
e.g
., fo
od p
rovi
ded
by c
areg
iver
, ped
iatr
ics,
hom
eles
s
Lac
k of
val
ue f
or b
ehav
ior
chan
ge, c
ompe
ting
valu
es
Men
tal i
llnes
s, d
epre
ssio
n
Med
icat
ions
that
incr
ease
app
etite
, e.g
. ste
roid
s
Ove
rfee
ding
of
pare
nter
al/e
nter
al n
utri
tion
(TPN
/EN
)
Unw
illin
g or
uni
nter
este
d in
red
ucin
g en
ergy
inta
ke
Failu
re to
adj
ust f
or li
fest
yle
chan
ges
and
decr
ease
d m
etab
olis
m (
e.g.
agi
ng)
Res
olut
ion
of p
rior
hyp
erm
etab
olis
m w
ithou
t red
uctio
n in
inta
ke
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Edi
tion:
200
6 39

INTA
KE D
OMAI
N C
aloric
Ene
rgy B
alanc
e
EX
CE
SS
IVE
EN
ER
GY
IN
TA
KE
(N
I-1.
5)Nu
tritio
n As
sess
men
t Cat
egor
y Po
tent
ial In
dica
tors
of t
his N
utrit
ion
Diag
nosis
(one
or m
ore m
ust b
e pre
sent
) B
ioch
emic
al D
ata
Ove
rfee
ding
of
TPN
/EN
(us
ually
see
n ea
rly
afte
r in
itiat
ion
of f
eedi
ng):
Hyp
ergl
ycem
ia
Hyp
okal
emia
< 3
.5 m
Eq/
l
Hyp
opho
spha
tem
ia <
1.0
mE
q/l
Abn
orm
al li
ver
func
tion
test
s
Ant
hrop
omet
ric
Mea
sure
men
ts
Bod
y fa
t per
cent
age
>25%
for
men
and
> 3
2% f
or w
omen
BM
I >
25
Wei
ght g
ain
Phy
sica
l Exa
m F
indi
ngs
Incr
ease
d bo
dy a
dipo
sity
Ove
rfee
ding
TPN
/EN
:
Incr
ease
d re
spir
atio
ns
Foo
d/N
utri
tion
His
tory
O
bser
vatio
ns o
r re
port
s of
inta
ke o
f hi
gh c
alor
ic d
ensi
ty o
r la
rge
port
ions
of
food
s/be
vera
ges
Obs
erva
tions
, rep
orts
or
calc
ulat
ion
of T
PN/E
N a
bove
est
imat
ed o
r m
easu
red
(e.g
., in
dire
ct c
alor
imet
ry)
calo
ric
expe
nditu
re
Met
abol
ic c
art/i
ndir
ect c
alor
imet
ry m
easu
rem
ent,
e.g.
, res
pira
tory
quo
tient
>1.
0
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
obes
ity, o
verw
eigh
t, m
etab
olic
syn
drom
e, d
epre
ssio
n, o
r an
xiet
y di
sord
er
Refe
ren
ces:
1.
McC
lave
SA
, Low
en C
C, K
lebe
r M
J, M
cCon
nell
JW, J
ung
LY
, Gol
dsm
ith L
J. C
linic
al u
se o
f th
e re
spir
ator
y qu
otie
nt o
btai
ned
from
indi
rect
cal
orim
etry
. J P
aren
ter
Ent
eral
Nut
r. 2
003;
27:2
1-26
. 2.
M
cCla
ve S
A, L
owen
CC
, Kle
ber
MJ,
Nic
hols
on J
F, J
imm
erso
n SC
, McC
onne
ll JW
, Jun
g L
Y. A
re p
atie
nts
fed
appr
opri
atel
y ac
cord
ing
to th
eir
calo
ric
requ
irem
ents
? J
Par
ente
r E
nter
al N
utr.
1998
;22:
375-
381.
3.
O
verw
eigh
t and
Obe
sity
: Hea
lth C
onse
quen
ces.
ww
w.s
urge
onge
nera
l.gov
/topi
cs/o
besi
ty/c
allto
actio
n/fa
ct_c
onse
quen
ces.
htm
. Acc
esse
d A
ugus
t 28,
200
4.
Edi
tion:
200
6 40

INTA
KE D
OMAI
N O
ral o
r Nut
ritio
n Su
ppor
t Int
ake
INA
DE
QU
AT
E O
RA
L F
OO
D/B
EV
ER
AG
E I
NT
AK
E (
NI-
2.1)
De
fin
itio
n
Ora
l foo
d/be
vera
ge in
take
that
is le
ss th
an e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds. E
xcep
tion:
whe
n th
e go
al is
w
eigh
t los
s or
dur
ing
end
of li
fe c
are.
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems:
Phys
iolo
gic
caus
es, e
.g. i
ncre
ased
nut
rien
t nee
ds d
ue to
pro
long
ed c
atab
olic
illn
ess
Lac
k of
acc
ess
to f
ood,
e.g
. eco
nom
ic c
onst
rain
ts, c
ultu
ral o
r re
ligio
us p
ract
ices
, res
tric
ting
food
giv
en to
eld
erly
and
/or
child
ren
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit c
once
rnin
g su
ffic
ient
ora
l foo
d/be
vera
ge in
take
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or d
isor
dere
d ea
ting
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
min
atio
n F
indi
ngs
Dry
ski
n, m
ucou
s m
embr
anes
, poo
r sk
in tu
rgor
Wei
ght l
oss,
insu
ffic
ient
gro
wth
vel
ocity
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Insu
ffic
ient
inta
ke o
f en
ergy
or
high
qua
lity
prot
ein
from
die
t whe
n co
mpa
red
to r
equi
rem
ents
Eco
nom
ic c
onst
rain
ts th
at li
mit
food
ava
ilabi
lity
Edi
tion:
200
6 41

INTA
KE D
OMAI
N O
ral o
r Nut
ritio
n Su
ppor
t Int
ake
INA
DE
QU
AT
E O
RA
L F
OO
D/B
EV
ER
AG
E I
NT
AK
E (
NI-
2.1)
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f c
atab
olic
illn
ess
such
as
AID
S, tu
berc
ulos
is, a
nore
xia
nerv
osa,
se
psis
or
infe
ctio
n fr
om r
ecen
t sur
gery
), d
epre
ssio
n, a
cute
or
chro
nic
pain
Prot
ein
and/
or n
utri
ent m
alab
sorp
tion
Exc
essi
ve c
onsu
mpt
ion
of a
lcoh
ol o
r ot
her
drug
s th
at r
educ
e hu
nger
Med
icat
ions
that
cau
se a
nore
xia
Refe
ren
ces:
1.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r E
nerg
y, C
arbo
hydr
ate,
Fib
er, F
at, F
atty
Aci
ds, C
hole
ster
ol, P
rote
in, a
nd A
min
o A
cids
. Was
hing
ton,
DC
: N
atio
nal A
cade
my
Pres
s; 2
002.
2.
N
atio
nal A
cade
my
of S
cien
ces,
Ins
titut
e of
Med
icin
e. D
ieta
ry R
efer
ence
Int
akes
for
Wat
er, P
otas
sium
, Sod
ium
, Chl
orid
e, a
nd S
ulfa
te. W
ashi
ngto
n, D
C: N
atio
nal A
cade
my
Pres
s; 2
002.
Edi
tion:
200
6 42

INTA
KE D
OMAI
N O
ral o
r Nut
ritio
n Su
ppor
t Int
ake
EX
CE
SS
IVE
OR
AL
FO
OD
/BE
VE
RA
GE
IN
TA
KE
(N
I-2.
2)
De
fin
itio
n
Ora
l foo
d/be
vera
ge in
take
that
exc
eeds
ene
rgy
expe
nditu
re, e
stab
lishe
d re
fere
nce
stan
dard
s, o
r re
com
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
. E
xcep
tion:
w
hen
wei
ght g
ain
is d
esir
ed.
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems:
Har
mfu
l bel
iefs
/atti
tude
s ab
out f
ood,
nut
ritio
n, a
nd n
utri
tion-
rela
ted
topi
cs
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Lac
k of
acc
ess
to h
ealth
ful f
ood
choi
ces,
e.g
., fo
od p
rovi
ded
by c
areg
iver
, ped
iatr
ics,
hom
eles
s
Lac
k of
val
ue f
or b
ehav
ior
chan
ge, c
ompe
ting
valu
es
Inab
ility
to li
mit
or r
efus
e of
fere
d fo
ods
Lac
k of
foo
d pl
anni
ng, p
urch
asin
g, a
nd p
repa
ratio
n sk
ills
Los
s of
app
etite
aw
aren
ess
Med
icat
ions
that
incr
ease
app
etite
, e.g
. ste
roid
s, a
ntid
epre
ssan
ts
Unw
illin
g or
uni
nter
este
d in
red
ucin
g in
take
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a V
aria
ble
high
blo
od g
luco
se le
vels
Abn
orm
al H
gb A
1C
Ant
hrop
omet
ric
Mea
sure
men
ts
Wei
ght g
ain
not a
ttrib
uted
to f
luid
ret
entio
n or
nor
mal
gro
wth
Phy
sica
l Exa
m F
indi
ngs
Evi
denc
e of
aca
ntho
sis
nigr
ican
s
Edi
tion:
200
6 43

INTA
KE D
OMAI
N O
ral o
r Nut
ritio
n Su
ppor
t Int
ake
EX
CE
SS
IVE
OR
AL
FO
OD
/BE
VE
RA
GE
IN
TA
KE
(N
I-2.
2)F
ood/
Nut
ritio
n H
isto
ry
Rep
orts
or
obse
rvat
ions
of:
Inta
ke o
f hi
gh c
alor
ic d
ensi
ty f
oods
/bev
erag
es (
juic
e, s
oda,
or
alco
hol)
at m
eals
and
/or
snac
ks
Inta
ke o
f la
rge
port
ions
of
food
s/be
vera
ges,
foo
d gr
oups
, or
spec
ific
foo
d ite
ms
Inta
ke th
at e
xcee
ds e
stim
ated
or
mea
sure
d en
ergy
nee
ds
Hig
hly
vari
able
dai
ly c
alor
ic in
take
Bin
ge e
atin
g pa
ttern
s
Freq
uent
, exc
essi
ve f
ast f
ood
or r
esta
uran
t int
ake
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
obes
ity, o
verw
eigh
t, or
met
abol
ic s
yndr
ome,
dep
ress
ion,
an
xiet
y di
sord
er
Res
ting
met
abol
ic r
ate
mea
sure
men
t ref
lect
ing
exce
ss in
take
, e.g
., re
spir
ator
y qu
otie
nt >
1.0
Refe
ren
ces:
1.
Ove
rwei
ght a
nd O
besi
ty: H
ealth
Con
sequ
ence
s. w
ww
.sur
geon
gene
ral.g
ov/to
pics
/obe
sity
/cal
ltoac
tion/
fact
_con
sequ
ence
s.ht
m. A
cces
sed
Aug
ust 2
8, 2
004.
Posi
tion
of th
e A
mer
ican
Die
tetic
A
ssoc
iatio
n: W
eigh
t man
agem
ent.
J A
m D
iet A
ssoc
. 200
2;10
2:11
45-1
155.
2.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: T
otal
die
t app
roac
h to
com
mun
icat
ing
food
and
nut
ritio
n in
form
atio
n. J
Am
Die
t Ass
oc 2
002;
102:
100-
108.
3.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: T
he r
ole
of d
iete
tics
prof
essi
onal
s in
hea
lth p
rom
otio
n an
d di
seas
e pr
even
tion.
J A
m D
iet A
ssoc
. 200
2;10
2:16
80-1
687.
Edi
tion:
200
6 44

INTA
KE D
OMAI
N O
ral o
r Nut
ritio
n Su
ppor
t Int
ake
INA
DE
QU
AT
E I
NT
AK
E F
RO
M E
NT
ER
AL
/PA
RE
NT
ER
AL
(E
N/T
PN
) N
UT
RIT
ION
IN
FU
SIO
N (
NI-
2.3)
De
fin
itio
n
Ent
eral
or
pare
nter
al in
fusi
on th
at p
rovi
des
few
er c
alor
ies
or n
utri
ents
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal
need
s. E
xcep
tion:
whe
n th
e go
al is
wei
ght l
oss
or d
urin
g en
d of
life
car
e.
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Alte
red
abso
rptio
n or
met
abol
ism
of
nutr
ient
s, e
.g.,
med
icat
ions
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit (
patie
nt/c
lient
, car
egiv
er, s
uppl
ier)
-- in
corr
ect f
orm
ula/
form
ulat
ion
give
n, e
.g.,
wro
ng e
nter
al f
eedi
ng, m
issi
ng
com
pone
nt o
f T
PN
Lac
k of
, com
prom
ised
, or
inco
rrec
t acc
ess
for
deliv
erin
g E
N/T
PN
Incr
ease
d bi
olog
ical
dem
and
of n
utri
ents
, e.g
., ac
cele
rate
d gr
owth
, wou
nd h
ealin
g, c
hron
ic in
fect
ion,
mul
tiple
fra
ctur
es
Into
lera
nce
of E
N/T
PN
Infu
sion
vol
ume
not r
each
ed o
r sc
hedu
le f
or in
fusi
on in
terr
upte
d
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a C
hole
ster
ol <
160
mg/
dL
Vita
min
/min
eral
abn
orm
aliti
es
Cal
cium
< 9
.2 m
g/dL
Vita
min
K--
Prol
onge
d pr
othr
ombi
n tim
e (P
T),
par
tial t
hrom
bopl
astin
tim
e (P
TT
)
Cop
per
< 70
µg/
dL
Zin
c <
12 µ
mol
/L
Iron
< 5
0 µ
g/dL
; iro
n bi
ndin
g ca
paci
ty <
250
µg/
dL
Edi
tion:
200
6 45
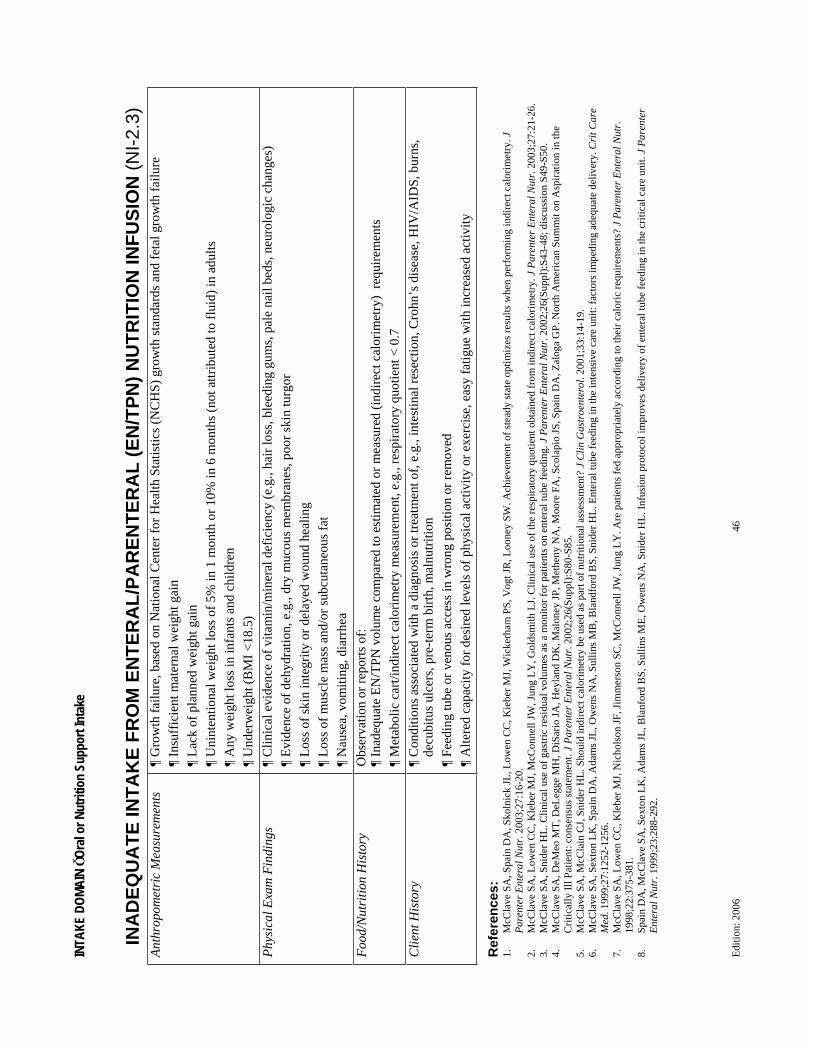
INTA
KE D
OMAI
N O
ral o
r Nut
ritio
n Su
ppor
t Int
ake
INA
DE
QU
AT
E I
NT
AK
E F
RO
M E
NT
ER
AL
/PA
RE
NT
ER
AL
(E
N/T
PN
) N
UT
RIT
ION
IN
FU
SIO
N (
NI-
2.3)
Ant
hrop
omet
ric
Mea
sure
men
ts
Gro
wth
fai
lure
, bas
ed o
n N
atio
nal C
ente
r fo
r H
ealth
Sta
tistic
s (N
CH
S) g
row
th s
tand
ards
and
fet
al g
row
th f
ailu
re
Insu
ffic
ient
mat
erna
l wei
ght g
ain
Lac
k of
pla
nned
wei
ght g
ain
Uni
nten
tiona
l wei
ght l
oss
of 5
% in
1 m
onth
or
10%
in 6
mon
ths
(not
attr
ibut
ed to
flu
id)
in a
dults
A
ny w
eigh
t los
s in
infa
nts
and
child
ren
Und
erw
eigh
t (B
MI
<18
.5)
Phy
sica
l Exa
m F
indi
ngs
Clin
ical
evi
denc
e of
vita
min
/min
eral
def
icie
ncy
(e.g
., ha
ir lo
ss, b
leed
ing
gum
s, p
ale
nail
beds
, neu
rolo
gic
chan
ges)
E
vide
nce
of d
ehyd
ratio
n, e
.g.,
dry
muc
ous
mem
bran
es, p
oor
skin
turg
or
Los
s of
ski
n in
tegr
ity o
r de
laye
d w
ound
hea
ling
Los
s of
mus
cle
mas
s an
d/or
sub
cuta
neou
s fa
t N
ause
a, v
omiti
ng, d
iarr
hea
Foo
d/N
utri
tion
His
tory
O
bser
vatio
n or
rep
orts
of:
In
adeq
uate
EN
/TPN
vol
ume
com
pare
d to
est
imat
ed o
r m
easu
red
(ind
irec
t cal
orim
etry
) r
equi
rem
ents
M
etab
olic
car
t/ind
irec
t cal
orim
etry
mea
sure
men
t, e.
g., r
espi
rato
ry q
uotie
nt <
0.7
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
inte
stin
al r
esec
tion,
Cro
hn’s
dis
ease
, HIV
/AID
S, b
urns
, de
cubi
tus
ulce
rs, p
re-t
erm
bir
th, m
alnu
triti
on
Feed
ing
tube
or
veno
us a
cces
s in
wro
ng p
ositi
on o
r re
mov
ed
Alte
red
capa
city
for
des
ired
leve
ls o
f ph
ysic
al a
ctiv
ity o
r ex
erci
se, e
asy
fatig
ue w
ith in
crea
sed
activ
ity
Refe
ren
ces:
1.
McC
lave
SA
, Spa
in D
A, S
koln
ick
JL, L
owen
CC
, Kie
ber
MJ,
Wic
kerh
am P
S, V
ogt J
R, L
oone
y SW
. Ach
ieve
men
t of
stea
dy s
tate
opt
imiz
es r
esul
ts w
hen
perf
orm
ing
indi
rect
cal
orim
etry
. JP
aren
ter
Ent
eral
Nut
r. 2
003;
27:1
6-20
. 2.
M
cCla
ve S
A, L
owen
CC
, Kle
ber
MJ,
McC
onne
ll JW
, Jun
g L
Y, G
olds
mith
LJ.
Clin
ical
use
of
the
resp
irat
ory
quot
ient
obt
aine
d fr
om in
dire
ct c
alor
imet
ry. J
Par
ente
r E
nter
al N
utr.
200
3;27
:21-
26.
3.
McC
lave
SA
, Sni
der
HL
. Clin
ical
use
of
gast
ric
resi
dual
vol
umes
as
a m
onito
r fo
r pa
tient
s on
ent
eral
tube
fee
ding
. J P
aren
ter
Ent
eral
Nut
r. 2
002;
26(S
uppl
):S4
3-48
; dis
cuss
ion
S49-
S50.
4.
M
cCla
ve S
A, D
eMeo
MT
, DeL
egge
MH
, DiS
ario
JA
, Hey
land
DK
, Mal
oney
JP,
Met
heny
NA
, Moo
re F
A, S
cola
pio
JS, S
pain
DA
, Zal
oga
GP
. Nor
th A
mer
ican
Sum
mit
on A
spir
atio
n in
the
Cri
tical
ly I
ll Pa
tient
: con
sens
us s
tate
men
t. J
Par
ente
r E
nter
al N
utr.
200
2;26
(Sup
pl):
S80-
S85.
5.
M
cCla
ve S
A, M
cCla
in C
J, S
nide
r H
L. S
houl
d in
dire
ct c
alor
imet
ry b
e us
ed a
s pa
rt o
f nu
triti
onal
ass
essm
ent?
J C
lin G
astr
oent
erol
. 200
1;33
:14-
19.
6.
M
cCla
ve S
A, S
exto
n L
K, S
pain
DA
, Ada
ms
JL, O
wen
s N
A, S
ullin
s M
B, B
land
ford
BS,
Sni
der
HL
. Ent
eral
tube
fee
ding
in th
e in
tens
ive
care
uni
t: fa
ctor
s im
pedi
ng a
dequ
ate
deliv
ery.
Cri
t Car
e M
ed. 1
999;
27:1
252-
1256
. 7.
M
cCla
ve S
A, L
owen
CC
, Kle
ber
MJ,
Nic
hols
on J
F, J
imm
erso
n SC
, McC
onne
ll JW
, Jun
g L
Y. A
re p
atie
nts
fed
appr
opri
atel
y ac
cord
ing
to th
eir
calo
ric
requ
irem
ents
? J
Par
ente
r E
nter
al N
utr.
1998
;22:
375-
381.
8.
Sp
ain
DA
, McC
lave
SA
, Sex
ton
LK
, Ada
ms
JL, B
lanf
ord
BS,
Sul
lins
ME
, Ow
ens
NA
, Sni
der
HL
. Inf
usio
n pr
otoc
ol im
prov
es d
eliv
ery
of e
nter
al tu
be f
eedi
ng in
the
crit
ical
car
e un
it. J
Par
ente
r E
nter
al N
utr.
199
9;23
:288
-292
.
Edi
tion:
200
6 46

INTA
KE D
OMAI
N O
ral o
r Nut
ritio
n Su
ppor
t Int
ake
EX
CE
SS
IVE
IN
TA
KE
FR
OM
EN
TE
RA
L O
R P
AR
EN
TE
RA
L N
UT
RIT
ION
(N
I-2.
4)
De
fin
itio
n
Ent
eral
or
pare
nter
al in
fusi
on th
at p
rovi
des
mor
e ca
lori
es o
r nu
trie
nts
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal
need
s.
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Phys
iolo
gic
caus
es, e
.g. d
ecre
ased
nee
ds r
elat
ed to
low
act
ivity
leve
ls w
ith c
ritic
al il
lnes
s or
org
an f
ailu
re
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit o
n th
e pa
rt o
f th
e ca
regi
ver,
pat
ient
/clie
nt o
r cl
inic
ian
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a E
leva
ted
BU
N:c
reat
inin
e ra
tio (
prot
ein)
Hyp
ergl
ycem
ia (
carb
ohyd
rate
)
Hyp
erca
pnia
Ele
vate
d liv
er e
nzym
es
Ant
hrop
omet
ric
Mea
sure
men
ts
Wei
ght g
ain
in e
xces
s of
lean
tiss
ue a
ccre
tion
Phy
sica
l Exa
min
atio
n F
indi
ngs
Ede
ma
with
exc
ess
flui
d ad
min
istr
atio
n
Foo
d/N
utri
tion
His
tory
R
epor
t or
obse
rvat
ion
of
Doc
umen
ted
inta
ke f
rom
ent
eral
or
pare
nter
al n
utri
ents
that
is c
onsi
sten
tly a
bove
rec
omm
ende
d in
take
for
car
bohy
drat
e,
prot
ein,
and
fat
(e.
g.36
Kca
l/kg
for
wel
l, ac
tive
adul
ts, 2
5 K
cal/k
g or
as
mea
sure
d by
indi
rect
cal
orim
etry
for
cri
tical
ly
ill a
dults
, 0.8
g/k
g pr
otei
n fo
r w
ell a
dults
, 1.5
g/k
g pr
otei
n fo
r cr
itica
lly il
l adu
lts, 4
mg/
kg/m
inut
e of
dex
tros
e fo
r cr
itica
lly il
l adu
lts, 1
.2 g
/kg
lipid
for
adu
lts, o
r 3
gm/k
g fo
r ch
ildre
n)
Edi
tion:
200
6 47

INTA
KE D
OMAI
N O
ral o
r Nut
ritio
n Su
ppor
t Int
ake
EX
CE
SS
IVE
IN
TA
KE
FR
OM
EN
TE
RA
L O
R P
AR
EN
TE
RA
L N
UT
RIT
ION
(N
I-2.
4)C
lient
His
tory
U
se o
f dr
ugs
that
red
uce
requ
irem
ents
or
impa
ir m
etab
olis
m o
f en
ergy
, pro
tein
, fat
or
flui
d.
Unr
ealis
tic e
xpec
tatio
ns o
f w
eigh
t gai
n or
idea
l wei
ght
Rec
eivi
ng s
igni
fica
nt c
alor
ie in
take
fro
m li
pid
or d
extr
ose
infu
sion
s, o
r pe
rito
neal
dia
lysi
s or
in a
ssoc
iatio
n w
ith o
ther
m
edic
al tr
eatm
ents
Refe
ren
ces:
1.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r E
nerg
y, C
arbo
hydr
ate,
Fib
er, F
at, F
atty
Aci
ds, C
hole
ster
ol, P
rote
in, a
nd A
min
o A
cids
. Was
hing
ton,
DC
: N
atio
nal A
cade
my
Pres
s, 2
002.
2.
N
atio
nal A
cade
my
of S
cien
ces,
Ins
titut
e of
Med
icin
e. D
ieta
ry R
efer
ence
Int
akes
for
Wat
er, P
otas
sium
, Sod
ium
, Chl
orid
e, a
nd S
ulfa
te. W
ashi
ngto
n, D
C: N
atio
nal A
cade
my
Pres
s, 2
004.
3.
A
arsl
and
A, C
hink
es D
, Wol
fe R
R. H
epat
ic a
nd w
hole
-bod
y fa
t syn
thes
is in
hum
ans
duri
ng c
arbo
hydr
ate
over
feed
ing.
Am
J C
lin N
utr.
199
7;65
:177
4-17
82.
4.
McC
lave
SA
, Low
en C
C, K
lebe
r M
J, e
t al.
Are
pat
ient
s fe
d ap
prop
riat
ely
acco
rdin
g to
thei
r ca
lori
c re
quir
emen
ts?
J P
aren
Ent
er N
utr.
199
8;22
:375
-381
. 5.
M
cCla
ve S
A, L
owen
CC
, Kle
ber
MJ,
McC
onne
ll JW
, Jun
g L
Y, G
olds
mith
LJ.
Clin
ical
use
of
the
resp
irat
ory
quot
ient
obt
aine
d fr
om in
dire
ct c
alor
imet
ry. J
Par
en E
nter
Nut
r. 2
003;
27:2
1-26
. 6.
W
olfe
RR
, O'D
onne
ll T
F, J
r., S
tone
MD
, Ric
hman
d D
A, B
urke
JF.
Inv
estig
atio
n of
fac
tors
det
erm
inin
g th
e op
timal
glu
cose
infu
sion
rat
e in
tota
l par
ente
ral n
utri
tion.
Met
abol
ism
: C
linic
al &
E
xper
imen
tal.
1980
;29:
892-
900.
Edi
tion:
200
6 48

INTA
KE D
OMAI
N O
ral o
r Nut
ritio
n Su
ppor
t Int
ake
INA
PP
RO
PR
IAT
E I
NF
US
ION
OF
EN
TE
RA
L O
R P
AR
EN
TE
RA
L N
UT
RIT
ION
(N
I-2.
5)U
se w
ith
cau
tion
–on
ly a
fter
dis
cuss
ion
wit
h o
ther
hea
lth
tea
m m
ember
s
De
fin
itio
n
Ent
eral
or
pare
nter
al in
fusi
on th
at p
rovi
des
eith
er f
ewer
or
mor
e ca
lori
es a
nd/o
r nu
trie
nts
or is
of
the
wro
ng c
ompo
sitio
n or
type
, is
not w
arra
nted
bec
ause
the
patie
nt/c
lient
is a
ble
to to
lera
te a
n en
tera
l int
ake,
or
is u
nsaf
e be
caus
e of
the
pote
ntia
l for
sep
sis
or o
ther
com
plic
atio
ns
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems:
Phys
iolo
gic
caus
es, e
.g. i
mpr
ovem
ent i
n pa
tient
/clie
nt s
tatu
s, a
llow
ing
retu
rn to
tota
l or
part
ial o
ral d
iet;
chan
ges
in th
e co
urse
of
dise
ase
resu
lting
in
chan
ges
in n
utri
ent r
equi
rem
ents
Prod
uct o
r kn
owle
dge
defi
cit o
n th
e pa
rt o
f th
e ca
regi
ver
or c
linic
ian
End
of
life
care
if p
atie
nt/c
lient
or
fam
ily d
o no
t des
ire
nutr
ition
sup
port
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a A
bnor
mal
live
r fu
nctio
n te
sts
in p
atie
nt/c
lient
on
long
term
(m
ore
than
3-6
wee
ks)
feed
ing
Abn
orm
al le
vels
of
mar
kers
spe
cifi
c fo
r va
riou
s nu
trie
nts,
e.g
., hy
per
phos
phat
emia
in p
atie
nt/c
lient
rec
eivi
ng f
eedi
ngs
with
a h
igh
phos
phor
us c
onte
nt, h
ypok
alem
ia in
pat
ient
/clie
nt r
ecei
ving
fee
ding
s w
ith lo
w p
otas
sium
con
tent
Ant
hrop
omet
ric
Mea
sure
men
ts
Wei
ght g
ain
in e
xces
s of
lean
tiss
ue a
ccre
tion
Wei
ght l
oss
Phy
sica
l Exa
min
atio
n F
indi
ngs
Ede
ma
with
exc
ess
flui
d ad
min
istr
atio
n
Com
plic
atio
ns s
uch
as: f
atty
live
r in
the
abse
nce
of o
ther
cau
ses
Los
s of
sub
cuta
neou
s fa
t and
mus
cle
stor
es
Edi
tion:
200
6 49

INTA
KE D
OMAI
N O
ral o
r Nut
ritio
n Su
ppor
t Int
ake
INA
PP
RO
PR
IAT
E I
NF
US
ION
OF
EN
TE
RA
L O
R P
AR
EN
TE
RA
L N
UT
RIT
ION
(N
I-2.
5)F
ood/
Nut
ritio
n H
isto
ry
Rep
ort o
r ob
serv
atio
n of
Doc
umen
ted
inta
ke f
rom
ent
eral
or
pare
nter
al n
utri
ents
that
is c
onsi
sten
tly a
bove
or
belo
w r
ecom
men
ded
inta
ke f
or
carb
ohyd
rate
, pro
tein
, and
/or
fat–
esp
ecia
lly r
elat
ed to
pat
ient
/clie
nt’s
abi
lity
to c
onsu
me
an o
ral d
iet t
hat m
eets
nee
ds a
t th
is p
oint
in ti
me
Doc
umen
ted
inta
ke o
f ot
her
nutr
ient
s th
at is
con
sist
ently
abo
ve o
r be
low
that
rec
omm
ende
d
Nau
sea,
vom
iting
, dia
rrhe
a, h
igh
gast
ric
resi
dual
vol
ume
Clie
nt H
isto
ry
His
tory
of
ente
ral o
r pa
rent
eral
nut
ritio
n in
tole
ranc
e
Refe
ren
ces:
1.
Aar
slan
d A
, Chi
nkes
D, W
olfe
RR
. Hep
atic
and
who
le-b
ody
fat s
ynth
esis
in h
uman
s du
ring
car
bohy
drat
e ov
erfe
edin
g. A
m J
Clin
Nut
r. 1
997;
65:1
774-
1782
. 2.
M
cCla
ve S
A, L
owen
CC
, Kle
ber
MJ,
Nic
hols
on J
F, J
imm
erso
n SC
, McC
onne
ll JW
, Jun
g L
Y. A
re p
atie
nts
fed
appr
opri
atel
y ac
cord
ing
to th
eir
calo
ric
requ
irem
ents
? J
Par
ente
r E
nter
al N
utr.
1998
;22:
375-
381.
3.
M
cCla
ve S
A, L
owen
CC
, Kle
ber
MJ,
McC
onne
ll JW
, Jun
g L
Y, G
olds
mith
LJ.
Clin
ical
use
of
the
resp
irat
ory
quot
ient
obt
aine
d fr
om in
dire
ct c
alor
imet
ry. J
Par
ente
r E
nter
al N
utr.
200
3;27
:21-
26.
4.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r E
nerg
y, C
arbo
hydr
ate,
Fib
er, F
at, F
atty
Aci
ds, C
hole
ster
ol, P
rote
in, a
nd A
min
o A
cids
. Was
hing
ton,
DC
: N
atio
nal A
cade
my
Pres
s; 2
002.
5.
N
atio
nal A
cade
my
of S
cien
ces,
Ins
titut
e of
Med
icin
e. D
ieta
ry R
efer
ence
Int
akes
for
Wat
er, P
otas
sium
, Sod
ium
, Chl
orid
e, a
nd S
ulfa
te, W
ashi
ngto
n D
C. N
atio
nal A
cade
my
Pres
s, 2
004.
6.
N
atio
nal A
cade
my
of S
cien
ces,
Ins
titut
e of
Med
icin
e. D
ieta
ry R
efer
ence
Int
akes
for
Cal
cium
, Pho
spho
rus,
Mag
nesi
um, V
itam
in D
, and
Flu
orid
e. W
ashi
ngto
n, D
.C. N
atio
nal A
cade
my
Pres
s: 1
997.
7.
N
atio
nal A
cade
my
of S
cien
ces,
Ins
titut
e of
Med
icin
e. D
ieta
ry R
efer
ence
Int
akes
for
Vita
min
C, V
itam
in E
, Sel
eniu
m, a
nd C
arot
enoi
ds. W
ashi
ngto
n, D
.C. N
atio
nal A
cade
my
Pres
s: 2
000.
8.
W
olfe
RR
, O'D
onne
ll T
F, J
r., S
tone
MD
, Ric
hman
d D
A, B
urke
JF.
Inv
estig
atio
n of
fac
tors
det
erm
inin
g th
e op
timal
glu
cose
infu
sion
rat
e in
tota
l par
ente
ral n
utri
tion.
Met
abol
ism
: C
linic
al &
E
xper
imen
tal.
1980
;29:
892-
900.
Edi
tion:
200
6 50

INTA
KE D
OMAI
N F
luid
Inta
ke
INA
DE
QU
AT
E F
LU
ID I
NT
AK
E (
NI-
3.1)
De
fin
itio
n
Low
er in
take
of
flui
d co
ntai
ning
foo
ds o
r su
bsta
nces
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Phys
iolo
gic
caus
es, e
.g. i
ncre
ased
flu
id n
eeds
due
to c
limat
e/te
mpe
ratu
re c
hang
e; in
crea
sed
exer
cise
or
cond
ition
s le
adin
g to
incr
ease
d fl
uid
loss
es; f
ever
ca
usin
g in
crea
sed
inse
nsib
le lo
sses
, dec
reas
ed th
irst
sen
satio
n, u
se o
f dr
ugs
that
red
uce
thir
st
Lac
k of
acc
ess
to f
luid
, e.g
., ec
onom
ic c
onst
rain
ts, c
ultu
ral o
r re
ligio
us p
ract
ices
, una
ble
to a
cces
s fl
uid
inde
pend
ently
, suc
h as
, eld
erly
or
child
ren
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or d
isor
dere
d ea
ting;
dem
entia
res
ultin
g in
dec
reas
ed r
ecog
nitio
n of
thir
st
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a Pl
asm
a or
ser
um o
smol
ality
gre
ater
than
290
mO
sm/k
g
BU
N,
Na
Ant
hrop
omet
ric
Mea
sure
men
ts
Acu
te w
eigh
t los
s
Phy
sica
l Exa
min
atio
n F
indi
ngs
Dry
ski
n an
d m
ucou
s m
embr
anes
, poo
r sk
in tu
rgor
Uri
ne o
utpu
t <30
mL
/hr
Foo
d/N
utri
tion
His
tory
R
epor
t or
obse
rvat
ion
of
Insu
ffic
ient
inta
ke o
f fl
uid
whe
n co
mpa
red
to r
equi
rem
ents
Thi
rst
Dif
ficu
lty s
wal
low
ing
Edi
tion:
200
6 51

INTA
KE D
OMAI
N F
luid
Inta
ke
INA
DE
QU
AT
E F
LU
ID I
NT
AK
E (
NI-
3.1)
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
Alz
heim
er’s
dis
ease
or
othe
r de
men
tia r
esul
ting
in
decr
ease
d re
cogn
ition
of
thir
st, d
iarr
hea
Use
of
drug
s th
at r
educ
e th
irst
Refe
ren
ces:
1.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r W
ater
, Pot
assi
um, S
odiu
m, C
hlor
ide,
and
Sul
fate
, Was
hing
ton,
DC
: Nat
iona
l Aca
dem
y Pr
ess;
200
4.
2.
Gra
ndje
an A
C, C
ampb
ell,
SM. H
ydra
tion:
Flu
ids
for
Life
. M
onog
raph
Ser
ies.
Was
hing
ton
D.C
. Int
erna
tiona
l Lif
e Sc
ienc
es I
nstit
ute
Nor
th A
mer
ica,
200
4.
3.
Gra
ndje
an A
C, R
eim
ers
KJ,
Buy
ckx
ME
: H
ydra
tion:
Iss
ues
for
the
21st
Cen
tury
. N
utri
tion
Rev
iew
s 20
03;6
1:26
1-27
1.
Edi
tion:
200
6 52

INTA
KE D
OMAI
N F
luid
Inta
ke
EX
CE
SS
IVE
FL
UID
IN
TA
KE
(N
I-3.
2)
De
fin
itio
n
Hig
her
inta
ke o
f fl
uid
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Phys
iolo
gic
caus
es, e
.g. d
ecre
ased
flu
id lo
sses
due
to k
idne
y, li
ver
or c
ardi
ac f
ailu
re; d
imin
ishe
d w
ater
and
sod
ium
loss
es d
ue to
cha
nges
in e
xerc
ise
or
clim
ate,
Syn
drom
e of
inap
prop
riat
e di
uret
ic h
orm
one
(SIA
DH
)
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or d
isor
dere
d ea
ting
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a L
ower
ed p
lasm
a os
mol
arity
(27
0-28
0 m
Osm
/kg)
, onl
y if
pos
itive
flu
id b
alan
ce is
in e
xces
s of
pos
itive
sal
t bal
ance
Dec
reas
ed s
erum
sod
ium
in S
IAD
H
Ant
hrop
omet
ric
Mea
sure
men
ts
Wei
ght g
ain
Phy
sica
l Exa
min
atio
n F
indi
ngs
Ede
ma
in th
e sk
in o
f th
e le
gs, s
acra
l are
a, o
r di
ffus
ely;
wee
ping
of
flui
ds f
rom
low
er le
gs
Asc
ites
Pulm
onar
y ed
ema
as e
vide
nced
by
shor
tnes
s of
bre
ath;
ort
hopn
ea; c
rack
les
or r
ales
Foo
d/N
utri
tion
His
tory
R
epor
t or
obse
rvat
ion
of
Flui
d in
take
in e
xces
s of
rec
omm
ende
d in
take
Exc
essi
ve s
alt i
ntak
e
Inab
ility
to to
lera
te s
olid
foo
ds n
eces
sita
ting
a liq
uid
diet
Edi
tion:
200
6 53
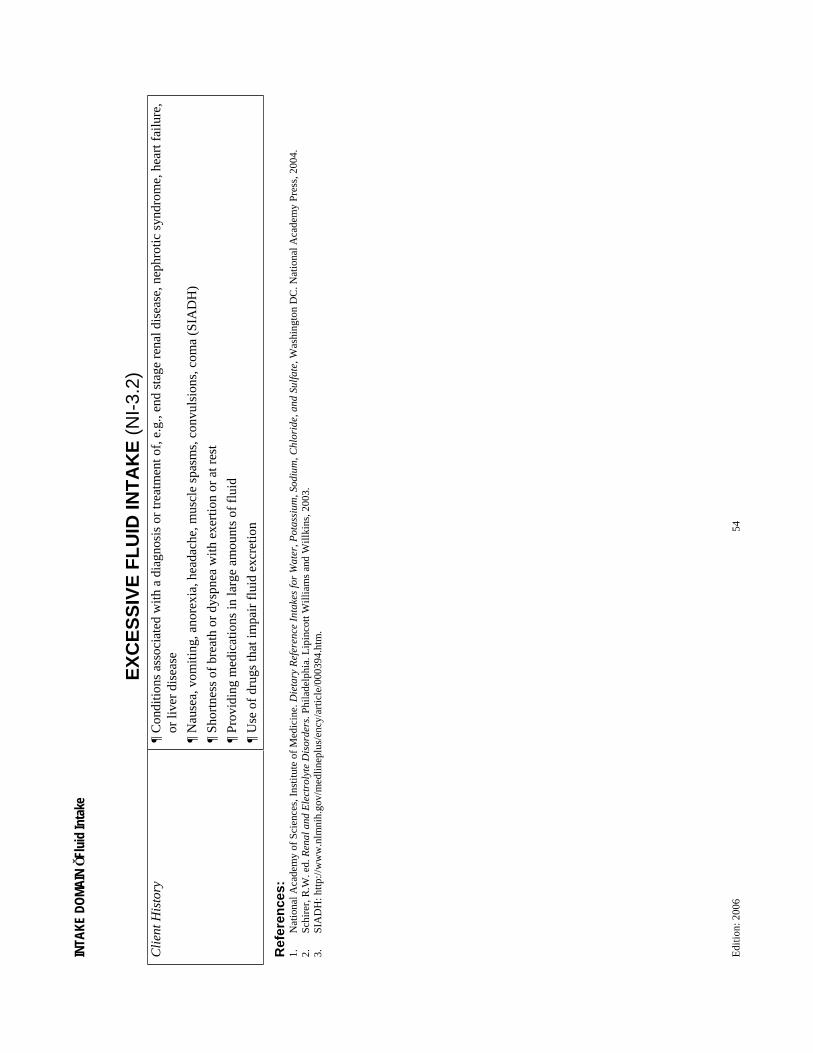
INTA
KE D
OMAI
N F
luid
Inta
ke
EX
CE
SS
IVE
FL
UID
IN
TA
KE
(N
I-3.
2)C
lient
His
tory
C
ondi
tions
ass
ocia
ted
with
a d
iagn
osis
or
trea
tmen
t of,
e.g
., en
d st
age
rena
l dis
ease
, nep
hrot
ic s
yndr
ome,
hea
rt f
ailu
re,
or li
ver
dise
ase
Nau
sea,
vom
iting
, ano
rexi
a, h
eada
che,
mus
cle
spas
ms,
con
vuls
ions
, com
a (S
IAD
H)
Shor
tnes
s of
bre
ath
or d
yspn
ea w
ith e
xert
ion
or a
t res
t
Prov
idin
g m
edic
atio
ns in
larg
e am
ount
s of
flu
id
Use
of
drug
s th
at im
pair
flu
id e
xcre
tion
Refe
ren
ces:
1.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r W
ater
, Pot
assi
um, S
odiu
m, C
hlor
ide,
and
Sul
fate
, Was
hing
ton
DC
. Nat
iona
l Aca
dem
y Pr
ess,
200
4.
2.
Schi
rer,
R.W
. ed.
Ren
al a
nd E
lect
roly
te D
isor
ders
. Phi
lade
lphi
a. L
ipin
cott
Will
iam
s an
d W
illki
ns, 2
003.
3.
SI
AD
H: h
ttp://
ww
w.n
lmni
h.go
v/m
edlin
eplu
s/en
cy/a
rtic
le/0
0039
4.ht
m.
Edi
tion:
200
6 54

INTA
KE D
OMAI
N B
ioac
tive S
ubst
ance
s
INA
DE
QU
AT
E B
IOA
CT
IVE
SU
BS
TA
NC
E I
NT
AK
E (
NI-
4.1)
De
fin
itio
n
Low
er in
take
of
bioa
ctiv
e su
bsta
nces
con
tain
ing
food
s or
sub
stan
ces
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal
need
s
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Lim
ited
acce
ss to
foo
d co
ntai
ning
sub
stan
ce
Alte
red
GI
func
tion,
e.g
., pa
in o
r di
scom
fort
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Foo
d/N
utri
tion
His
tory
O
bser
vatio
ns o
r re
port
s of
:
Low
inta
ke o
f pl
ant f
oods
con
tain
ing:
Solu
ble
fibe
r, e
.g.,
psyl
lium
( to
tal a
nd L
DL
cho
lest
erol
)
Soy
prot
ein
( to
tal a
nd L
DL
cho
lest
erol
)
-glu
can,
e.g
., w
hole
oat
pro
duct
s (
tota
l and
LD
L c
hole
ster
ol)
Low
inta
ke o
f pl
ant f
oods
con
tain
ing:
Pla
nt s
tero
l and
sta
nol e
ster
s, e
.g.,
fort
ifie
d m
arga
rine
s (
tota
l and
LD
L c
hole
ster
ol)
Lac
k of
ava
ilabl
e fo
ods/
prod
ucts
with
bio
activ
e su
bsta
nce
in m
arke
ts
Edi
tion:
200
6 55

INTA
KE D
OMAI
N B
ioac
tive S
ubst
ance
s
INA
DE
QU
AT
E B
IOA
CT
IVE
SU
BS
TA
NC
E I
NT
AK
E (
NI-
4.1)
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
card
iova
scul
ar d
isea
se, e
leva
ted
chol
este
rol
Dis
com
fort
or
pain
ass
ocia
ted
with
inta
ke o
f fo
ods
rich
in b
ioac
tive
subs
tanc
es, e
.g.,
solu
ble
fibe
r,
-glu
can,
soy
pro
tein
Refe
ren
ces:
1.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Fun
ctio
nal f
oods
. J A
m D
iet A
ssoc
. 200
4;10
4:81
4-82
6.
Edi
tion:
200
6 56

INTA
KE D
OMAI
N B
ioac
tive S
ubst
ance
s
EX
CE
SS
IVE
BIO
AC
TIV
E S
UB
ST
AN
CE
IN
TA
KE
(N
I-4.
2)
De
fin
itio
n
Hig
her
inta
ke o
f bi
oact
ive
subs
tanc
es o
ther
than
trad
ition
al n
utri
ents
, suc
h as
fun
ctio
nal f
oods
, bio
activ
e fo
od c
ompo
nent
s, d
ieta
ry s
uppl
emen
ts, f
ood
conc
entr
ates
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Con
tam
inat
ion,
mis
Ter
min
g, m
isus
e, r
ecen
t bra
nd c
hang
e, r
ecen
t dos
e in
crea
se, r
ecen
t for
mul
atio
n ch
ange
of
subs
tanc
e co
nsum
ed
Freq
uent
inta
ke o
f fo
od c
onta
inin
g bi
oact
ive
subs
tanc
e
Alte
red
GI
func
tion,
e.g
., pa
in o
r di
scom
fort
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a L
ab v
alue
s in
dica
ting
exce
ssiv
e in
take
of
the
spec
ific
sub
stan
ce, s
uch
as r
apid
dro
p in
cho
lest
erol
fro
m in
take
of
stan
ol o
r st
erol
est
ers
and
a st
atin
dru
g an
d re
late
d di
etar
y ch
ange
s or
med
icat
ions
Incr
ease
d he
patic
enz
yme
refl
ectin
g he
pato
cellu
lar
dam
age
Ant
hrop
omet
ric
Mea
sure
men
ts
Wei
ght l
oss
as a
res
ult o
f m
alab
sorp
tion
or m
aldi
gest
ion
Phy
sica
l Exa
m F
indi
ngs
Con
stip
atio
n or
dia
rrhe
a re
late
d to
exc
essi
ve in
take
Neu
rolo
gic
chan
ges,
e.g
., an
xiet
y, m
enta
l sta
tus
chan
ges
Car
diov
ascu
lar
chan
ges,
e.g
., he
art r
ate,
EK
G c
hang
es, b
lood
pre
ssur
e
Edi
tion:
200
6 57

INTA
KE D
OMAI
N B
ioac
tive S
ubst
ance
s
EX
CE
SS
IVE
BIO
AC
TIV
E S
UB
ST
AN
CE
IN
TA
KE
(N
I-4.
2)F
ood/
Nut
ritio
n H
isto
ry
Obs
erva
tions
or
repo
rts
of:
Hig
h in
take
of
plan
t foo
ds c
onta
inin
g:
Soy
prot
ein
( to
tal a
nd L
DL
cho
lest
erol
)
-glu
can,
e.g
., w
hole
oat
pro
duct
s (
tota
l and
LD
L c
hole
ster
ol)
Hig
h in
take
of
food
s co
ntai
ning
: Pla
nt s
tero
l and
sta
nol e
ster
s, e
.g.,
fort
ifie
d m
arga
rine
s (
tota
l and
LD
L c
hole
ster
ol)
or
othe
r fo
ods
base
d up
on f
ood
Ter
m
Subs
tanc
es w
hich
inte
rfer
e w
ith d
iges
tion
or a
bsor
ptio
n of
foo
dstu
ffs
Rea
dy a
cces
s to
ava
ilabl
e fo
ods/
prod
ucts
with
bio
activ
e su
bsta
nce,
e.g
., as
fro
m d
ieta
ry s
uppl
emen
t ven
dors
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
card
iova
scul
ar d
isea
se, e
leva
ted
chol
este
rol,
hype
rten
sion
,
Dis
com
fort
or
pain
ass
ocia
ted
with
inta
ke o
f fo
ods
rich
in b
ioac
tive
subs
tanc
es, e
.g.,
solu
ble
fibe
r,
-glu
can,
soy
pro
tein
Atte
mpt
s to
use
sup
plem
ents
or
bioa
ctiv
e su
bsta
nces
for
wei
ght l
oss,
trea
t con
stip
atio
n, p
reve
nt o
r cu
re c
hron
ic o
r ac
ute
dise
ase
Refe
ren
ces:
1.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Sup
plem
ents
: A
fram
ewor
k fo
r ev
alua
ting
safe
ty. W
ashi
ngto
n, D
C: N
atio
nal A
cade
my
Pres
s; 2
004.
2.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: F
unct
iona
l foo
ds. J
Am
Die
t Ass
oc. 2
004;
104:
814-
826.
Edi
tion:
200
6 58

INTA
KE D
OMAI
N B
ioac
tive S
ubst
ance
s
EX
CE
SS
IVE
AL
CO
HO
L I
NT
AK
E (
NI-
4.3)
De
fin
itio
n
Inta
ke a
bove
the
sugg
este
d lim
its f
or a
lcoh
ol
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Har
mfu
l bel
iefs
/atti
tude
s ab
out f
ood,
nut
ritio
n, a
nd n
utri
tion-
rela
ted
topi
cs
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Lac
k of
val
ue f
or b
ehav
ior
chan
ge, c
ompe
ting
valu
es
Alc
ohol
add
ictio
n
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a E
leva
ted
aspa
rtat
e am
inot
rans
fera
se (
AST
), g
amm
a-gl
utam
yl tr
ansf
eras
e (G
GT
), c
arbo
hydr
ate-
defi
cien
t tra
nsfe
rrin
, mea
n co
rpus
cula
r vo
lum
e, b
lood
alc
ohol
leve
ls
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Inta
ke o
f >
2 dr
inks
*/da
y (m
en)
Inta
ke o
f >
1 dr
ink*
/day
(w
omen
)
Bin
ge d
rink
ing
Con
sum
ptio
n of
any
alc
ohol
whe
n co
ntra
indi
cate
d
*1 d
rink
= 5
oz.
win
e, 1
2 oz
bee
r, 1
oz.
dis
tille
d al
coho
l
Edi
tion:
200
6 59

INTA
KE D
OMAI
N B
ioac
tive S
ubst
ance
s
EX
CE
SS
IVE
AL
CO
HO
L I
NT
AK
E (
NI-
4.3)
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
seve
re h
yper
trig
lyce
ride
mia
, ele
vate
d bl
ood
pres
sure
, de
pres
sion
, liv
er d
isea
se, p
ancr
eatit
is
New
med
ical
dia
gnos
is o
r ch
ange
in e
xist
ing
diag
nosi
s or
con
ditio
n
His
tory
of
exce
ssiv
e al
coho
l int
ake
Giv
ing
birt
h to
an
infa
nt w
ith f
etal
alc
ohol
syn
drom
e
Dri
nkin
g du
ring
pre
gnan
cy d
espi
te k
now
ledg
e of
ris
k
Une
xpla
ined
fal
ls
Refe
ren
ces:
1.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
The
rol
e of
die
tetic
s pr
ofes
sion
als
in h
ealth
pro
mot
ion
and
dise
ase
prev
entio
n. J
Am
Die
t Ass
oc. 2
002;
102:
1680
-168
7.
Edi
tion:
200
6 60

INTA
KE D
OMAI
N N
utrie
nt
INC
RE
AS
ED
NU
TR
IEN
T (
SP
EC
IFY
) N
EE
DS
(N
I-5.
1)
De
fin
itio
n
Incr
ease
d ne
ed f
or a
spe
cifi
c nu
trie
nt c
ompa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Alte
red
abso
rptio
n or
met
abol
ism
of
nutr
ient
, e.g
., fr
om m
edic
atio
ns
Com
prom
ise
of o
rgan
s re
late
d to
GI
func
tion,
e.g
. pan
crea
s, li
ver
Dec
reas
ed f
unct
iona
l len
gth
of in
test
ine,
e.g
., sh
ort b
owel
syn
drom
e
Dec
reas
ed o
r co
mpr
omis
ed f
unct
ion
of in
test
ine,
e.g
., C
elia
c di
seas
e, C
rohn
’s d
isea
se
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Incr
ease
d de
man
d of
nut
rien
t, e.
g., a
ccel
erat
ed g
row
th, w
ound
hea
ling,
chr
onic
infe
ctio
n
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a D
ecre
ased
cho
lest
erol
< 1
60 m
g/dL
, alb
umin
, pre
albu
min
, C r
eact
ive
prot
ein,
indi
catin
g in
crea
sed
stre
ss a
nd in
crea
sed
met
abol
ic n
eeds
Ele
ctro
lyte
/min
eral
(e.
g., p
otas
sium
, mag
nesi
um, p
hosp
horu
s) a
bnor
mal
ities
Uri
nary
or
feca
l los
ses
of s
peci
fic
or r
elat
ed n
utri
ent (
e.g.
, fec
al f
at, d
-xyl
ose
test
)
Vita
min
and
/or
min
eral
def
icie
ncy
Ant
hrop
omet
ric
Mea
sure
men
ts
Gro
wth
fai
lure
, bas
ed o
n N
atio
nal C
ente
r fo
r H
ealth
Sta
tistic
s (N
CH
S) g
row
th s
tand
ards
and
fet
al g
row
th f
ailu
re
Uni
nten
tiona
l wei
ght l
oss
of 5
% in
1 m
onth
or
10%
in 6
mon
ths
Und
erw
eigh
t (B
MI
<18
.5)
Edi
tion:
200
6 61

INTA
KE D
OMAI
N N
utrie
nt
INC
RE
AS
ED
NU
TR
IEN
T (
SP
EC
IFY
) N
EE
DS
(N
I-5.
1)P
hysi
cal E
xam
inat
ion
Fin
ding
s C
linic
al e
vide
nce
of v
itam
in/m
iner
al d
efic
ienc
y (e
.g.,
hair
loss
, ble
edin
g gu
ms,
pal
e na
il be
ds)
Los
s of
ski
n in
tegr
ity o
r de
laye
d w
ound
hea
ling
Los
s of
mus
cle
mas
s, s
ubcu
tane
ous
fat
Foo
d/N
utri
tion
His
tory
O
bser
vatio
n or
rep
orts
of:
Inad
equa
te in
take
of
food
s/su
pple
men
t con
tain
ing
need
ed n
utri
ent a
s co
mpa
red
to e
stim
ated
req
uire
men
ts
Inta
ke o
f fo
ods
that
do
not c
onta
in s
uffi
cien
t qua
ntiti
es o
f av
aila
ble
nutr
ient
(e.
g. o
ver
proc
esse
d, o
verc
ooke
d, o
r st
ored
im
prop
erly
)
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit (
e.g.
, lac
k of
info
rmat
ion,
inco
rrec
t inf
orm
atio
n or
non
-com
plia
nce
with
in
take
of
need
ed n
utri
ent)
Clie
nt H
isto
ry
Feve
r
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
inte
stin
al r
esec
tion,
Cro
hn’s
dis
ease
, HIV
/AID
S, b
urns
, pr
essu
re u
lcer
s, p
re-t
erm
bir
th, m
alnu
triti
on
Med
icat
ions
aff
ectin
g ab
sorp
tion
or m
etab
olis
m o
f ne
eded
nut
rien
t
Refe
ren
ces:
1.
Bey
er P
. Gas
troi
ntes
tinal
dis
orde
rs: R
oles
of
nutr
ition
and
the
diet
etic
s pr
actit
ione
r. J
Am
Die
t Ass
oc. 1
998;
98:2
72-2
77.
2.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion
and
Die
titia
ns o
f C
anad
a: N
utri
tion
inte
rven
tion
in th
e ca
re o
f pe
rson
s w
ith h
uman
imm
unod
efic
ienc
y vi
rus
infe
ctio
n. J
Am
Die
t Ass
oc.
2004
;104
:142
5-14
41.
Edi
tion:
200
6 62

INTA
KE D
OMAI
N N
utrie
nt
EV
IDE
NT
PR
OT
EIN
EN
ER
GY
MA
LN
UT
RIT
ION
(N
I-5.
2)
De
fin
itio
n
Inad
equa
te in
take
of
prot
ein
and/
or e
nerg
y ov
er p
rolo
nged
per
iods
of
time
resu
lting
in lo
ss o
f fa
t sto
res
and/
or m
uscl
e w
astin
g
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Phys
iolo
gic
caus
es, e
.g. a
ltere
d nu
trie
nt n
eeds
due
to p
rolo
nged
cat
abol
ic il
lnes
s, m
alab
sorp
tion
Lac
k of
acc
ess
to f
ood,
e.g
., ec
onom
ic c
onst
rain
ts, c
ultu
ral o
r re
ligio
us p
ract
ices
, res
tric
ting
food
giv
en to
eld
erly
and
/or
child
ren
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit,
e.g.
, avo
idan
ce o
f hi
gh q
ualit
y pr
otei
n fo
ods
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or e
atin
g di
sord
ers
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a N
orm
al s
erum
alb
umin
leve
l (un
com
plic
ated
mal
nutr
ition
)
Alb
umin
< 3
.4 m
g/dL
(di
seas
e/tr
aum
a re
late
d m
alnu
triti
on)
Ant
hrop
omet
ric
Mea
sure
men
ts
BM
I <
18.5
indi
cate
s un
derw
eigh
t
Failu
re to
thri
ve, e
.g. f
ailu
re to
atta
in d
esir
able
gro
wth
rat
es
Inad
equa
te m
ater
nal w
eigh
t gai
n
Wei
ght l
oss
of >
10%
in 6
mon
ths
Und
erw
eigh
t with
mus
cle
was
ting
Nor
mal
or
slig
htly
und
erw
eigh
t, st
unte
d gr
owth
in c
hild
ren
Edi
tion:
200
6 63

INTA
KE D
OMAI
N N
utrie
nt
EV
IDE
NT
PR
OT
EIN
EN
ER
GY
MA
LN
UT
RIT
ION
(N
I-5.
2)P
hysi
cal E
xam
Fin
ding
s U
ncom
plic
ated
mal
nutr
ition
: T
hin,
was
ted
appe
aran
ce; s
ever
e m
uscl
e w
astin
g; m
inim
al b
ody
fat;
spar
se, t
hin,
dry
, eas
ily
pluc
kabl
e ha
ir; d
ry, t
hin
skin
; obv
ious
bon
y pr
omin
ence
s, o
ccip
ital w
astin
g; lo
wer
ed b
ody
tem
pera
ture
, blo
od p
ress
ure,
he
art r
ate,
cha
nges
in h
air
or n
ails
con
sist
ent w
ith in
suff
icie
nt p
rote
in in
take
Dis
ease
/trau
ma
rela
ted
mal
nutr
ition
: T
hin
to n
orm
al a
ppea
ranc
e, w
ith p
erip
hera
l ede
ma,
asc
ites
or a
nasa
rca;
low
er
extr
emiti
es; s
ome
mus
cle
was
ting
with
ret
entio
n of
som
e bo
dy f
at; e
nlar
ged
fatty
live
r; d
yspi
gmen
tatio
n of
hai
r (f
lag
sign
) an
d sk
in
Del
ayed
wou
nd h
ealin
g
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f
Insu
ffic
ient
ene
rgy
inta
ke f
rom
die
t com
pare
d to
est
imat
ed o
r m
easu
red
RM
R
Insu
ffic
ient
inta
ke o
f hi
gh q
ualit
y pr
otei
n w
hen
com
pare
d to
req
uire
men
ts
Food
avo
idan
ce a
nd/o
r la
ck o
f in
tere
st in
foo
d
Clie
nt H
isto
ry
Chr
onic
or
acut
e di
seas
e or
trau
ma,
geo
grap
hic
loca
tion
and
soci
o-ec
onom
ic s
tatu
s as
soci
ated
with
alte
red
nutr
ient
inta
ke
of in
dige
nous
phe
nom
enon
Seve
re p
rote
in a
nd/o
r nu
trie
nt m
alab
sorp
tion
(e.g
. ext
ensi
ve b
owel
res
ectio
n)
Exc
essi
ve c
onsu
mpt
ion
of a
lcoh
ol o
r ot
her
drug
s th
at r
educ
e hu
nger
Refe
ren
ces:
1.
Wel
lcom
e T
rust
Wor
king
Par
ty. C
lass
ific
atio
n of
infa
ntile
mal
nutr
ition
. Lan
cet 1
970;
2:30
2-30
3.
2.
Sere
s D
S, R
esur
rect
ion,
LB
. Kw
ashi
orko
r: D
ysm
etab
olis
m v
ersu
s m
alnu
triti
on. N
utr
Clin
Pra
c 20
03;1
8:29
7-30
1.
3.
Jelli
ffe
DB
, Jel
liffe
EF.
Cau
satio
n of
kw
ashi
orko
r: T
owar
d a
mul
tifac
tora
l con
sens
us. P
edia
tric
s 19
92:9
0:11
0-11
3.4.
C
ente
rs f
or D
isea
se C
ontr
ol a
nd P
reve
ntio
n w
ebsi
te: h
ttp://
ww
w.c
dc.g
ov/n
ccdp
hp/d
npa/
bmi/b
mi-
adul
t.htm
. A
cces
sed
Oct
ober
5, 2
004.
5.
Fu
hrm
an M
P, C
harn
ey P
, Mue
ller
CM
. Hep
atic
pro
tein
s an
d nu
triti
on a
sses
smen
t. J
Am
Die
t Ass
oc. 2
004;
104:
1258
-126
4.
6.
U.S
. Dep
artm
ent o
f H
ealth
and
Hum
an S
ervi
ces.
The
Int
erna
tiona
l Cla
ssifi
catio
n of
Dis
ease
s, 9
th R
evis
ion,
4th E
d. W
ashi
ngto
n C
D: P
ublic
atio
n N
o. (
PHS)
91-
1260
, 199
1.
Edi
tion:
200
6 64

INTA
KE D
OMAI
N N
utrie
nt
INA
DE
QU
AT
E P
RO
TE
IN E
NE
RG
Y I
NT
AK
E (
NI-
5.3)
De
fin
itio
n
Inad
equa
te in
take
of
prot
ein
and/
or e
nerg
y co
mpa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds o
f sh
ort o
r re
cent
du
ratio
n
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Shor
t-te
rm p
hysi
olog
ic c
ause
s, e
.g. i
ncre
ased
nut
rien
t nee
ds d
ue to
cat
abol
ic il
lnes
s, m
alab
sorp
tion
Rec
ent l
ack
of a
cces
s to
foo
d, e
.g.,
econ
omic
con
stra
ints
, cul
tura
l or
relig
ious
pra
ctic
es, r
estr
ictin
g fo
od g
iven
or
food
sel
ecte
d
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit,
e.g.
, avo
idan
ce o
f al
l fat
s fo
r ne
w d
ietin
g pa
ttern
Rec
ent o
nset
of
psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or e
atin
g di
sord
ers
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a N
orm
al a
lbum
in (
in th
e se
tting
of
norm
al li
ver
func
tion
desp
ite d
ecre
ase
prot
ein-
ener
gy in
take
)
Ant
hrop
omet
ric
Mea
sure
men
ts
Inad
equa
te m
ater
nal w
eigh
t gai
n (m
ild b
ut n
ot s
ever
e)
Wei
ght l
oss
of 5
-7%
ove
r pa
st 3
mon
ths
in a
dults
, any
wei
ght l
oss
in c
hild
ren
Nor
mal
or
slig
htly
und
erw
eigh
t
Gro
wth
fai
lure
in c
hild
ren
Phy
sica
l Exa
m F
indi
ngs
Slow
wou
nd h
ealin
g in
pre
ssur
e ul
cer
or s
urgi
cal p
atie
nt/c
lient
Edi
tion:
200
6 65

INTA
KE D
OMAI
N N
utrie
nt
INA
DE
QU
AT
E P
RO
TE
IN E
NE
RG
Y I
NT
AK
E (
NI-
5.3)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f
Insu
ffic
ient
ene
rgy
inta
ke f
rom
die
t com
pare
d to
est
imat
ed o
r m
easu
red
RM
R o
r re
com
men
ded
leve
ls
Res
tric
tion
or o
mis
sion
of
food
gro
ups
such
as
dair
y or
mea
t gro
up f
oods
(pr
otei
n); b
read
or
milk
gro
up f
oods
(en
ergy
)
Rec
ent f
ood
avoi
danc
e an
d/or
lack
of
inte
rest
in f
ood
Lac
k of
abi
lity
to p
repa
re m
eals
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f m
ild p
rote
in-e
nerg
y m
alnu
triti
on, r
ecen
t illn
ess,
e.g
. pul
mon
ary
or
card
iac
failu
re, f
lu, i
nfec
tion,
sur
gery
Nut
rien
t mal
abso
rptio
n (e
.g. b
aria
tric
sur
gery
, dia
rrhe
a, s
teat
orrh
ea)
Exc
essi
ve c
onsu
mpt
ion
of a
lcoh
ol o
r ot
her
drug
s th
at r
educ
e hu
nger
Patie
nt/c
lient
rep
orts
of
hung
er in
the
face
of
inad
equa
te a
cces
s to
foo
d su
pply
Patie
nt/c
lient
rep
orts
lack
of
abili
ty to
pre
pare
mea
ls
Patie
nt/c
lient
rep
orts
lack
of
fund
s fo
r pu
rcha
se o
f ap
prop
riat
e fo
ods
Refe
ren
ces:
1.
Cen
ters
for
Dis
ease
Con
trol
and
Pre
vent
ion
web
site
: http
://w
ww
.cdc
.gov
/ncc
dphp
/dnp
a/bm
i/bm
i-ad
ult.h
tm.
Acc
esse
d O
ctob
er 5
, 200
4.
2.
Fuhr
man
MP,
Cha
rney
P, M
uelle
r C
M. H
epat
ic p
rote
ins
and
nutr
ition
ass
essm
ent.
J A
m D
iet A
ssoc
. 200
4;10
4:12
58-1
264.
3.
U
.S. D
epar
tmen
t of
Hea
lth a
nd H
uman
Ser
vice
s. T
he I
nter
natio
nal C
lass
ifica
tion
of D
isea
ses,
9th R
evis
ion,
4th E
d. W
ashi
ngto
n C
D: P
ublic
atio
n N
o. (
PHS)
91-
1260
, 199
1.
Edi
tion:
200
6 66

INTA
KE D
OMAI
N N
utrie
nt
DE
CR
EA
SE
D N
UT
RIE
NT
(S
PE
CIF
Y)
NE
ED
S (
NI-
5.4)
De
fin
itio
n
Dec
reas
ed n
eed
for
a sp
ecif
ic n
utri
ent c
ompa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Ren
al d
ysfu
nctio
n
Liv
er d
ysfu
nctio
n
Alte
red
chol
este
rol m
etab
olis
m/r
egul
atio
n
Hea
rt f
ailu
re
Food
into
lera
nces
, e.g
., ir
rita
ble
bow
el s
yndr
ome
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a C
hole
ster
ol >
200
mg/
dL, L
DL
cho
lest
erol
> 1
00 m
g/dL
, HD
L c
hole
ster
ol <
40
mg/
dL, t
rigl
ycer
ides
> 1
50 m
g/dL
Phos
phor
us >
5.5
mg/
dL
Glo
mer
ular
filt
ratio
n ra
te (
GFR
) <
90 m
L/m
in/1
.73
m2
Ele
vate
d B
UN
, Cr,
pot
assi
um
Liv
er f
unct
ion
test
s in
dica
ting
seve
re li
ver
dise
ase
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Ede
ma/
flui
d re
tent
ion
Inte
rdia
lytic
wei
ght g
ain
grea
ter
than
exp
ecte
d
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Inta
ke h
ighe
r th
an r
ecom
men
ded
for
fat,
phos
phor
us, s
odiu
m, p
rote
in, f
iber
Edi
tion:
200
6 67
INTA
KE D
OMAI
N N
utrie
nt
DE
CR
EA
SE
D N
UT
RIE
NT
(S
PE
CIF
Y)
NE
ED
S (
NI-
5.4)
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent t
hat r
equi
re a
spe
cifi
c ty
pe a
nd/o
r am
ount
of
nutr
ient
, e.g
., ca
rdio
vasc
ular
dis
ease
(fa
t), e
arly
ren
al d
isea
se (
prot
ein,
pho
s), E
SRD
(ph
os, s
odiu
m, p
otas
sium
, flu
id),
adv
ance
d liv
er
dise
ase
(pro
tein
), h
eart
fai
lure
(so
dium
, flu
id),
irri
tabl
e bo
wel
dis
ease
/Cro
hn’s
fla
re u
p (f
iber
)
Dia
gnos
is o
f hy
pert
ensi
on, c
onfu
sion
rel
ated
to li
ver
dise
ase
Refe
ren
ces:
1.
Apa
rici
o M
, Cha
uvea
u P,
Com
be C
. L
ow p
rote
in d
iets
and
out
com
es o
f re
nal p
atie
nts.
J N
ephr
ol. 2
001;
14:4
33-9
. 2.
B
eto
JA, B
ansa
l VK
. Med
ical
nut
ritio
n th
erap
y in
chr
onic
kid
ney
failu
re: I
nteg
ratin
g cl
inic
al p
ract
ice
guid
elin
es. J
Am
Die
t Ass
oc. 2
004;
104:
404-
409.
3.
C
upis
ti A
, Mor
elli
E, D
’Ale
ssan
dro
C, L
upet
ti S,
Bar
sott
i G. P
hosp
hate
con
trol
in c
hron
ic u
rem
ia: d
on’t
for
get d
iet.
J N
ephr
ol.
2003
;16:
29-3
3.
4.
Dur
ose
CL
, Hol
dsw
orth
M, W
atso
n V
, Prz
ygro
dzka
F. K
now
ledg
e of
die
tary
res
tric
tions
and
the
med
ical
con
sequ
ence
s of
non
com
plia
nce
by p
atie
nts
on h
emod
ialy
sis
are
not p
redi
ctiv
e of
die
tary
co
mpl
ianc
e. J
Am
Die
t Ass
oc. 2
004;
104:
35-4
1.
5.
Floc
h M
H, N
aray
an R
. D
iet i
n th
e ir
rita
ble
bow
el s
yndr
ome.
Clin
Gas
troe
nter
ol.
2002
;35:
pS45
-pS5
2.
6.
Kat
o J,
Kob
une
M, N
akam
ura
T, K
uroj
wa
G, T
akad
a K
, Tak
imot
o R
, Sat
o Y
, Fuj
ikaw
a K
, Tak
ahas
hi M
, Tak
ayam
a T
, Ike
da T
, Niit
su Y
. Nor
mal
izat
ion
of e
leva
ted
hepa
tic 8
-hyd
roxy
-2’-
deox
ygua
nosi
ne le
vels
in c
hron
ic h
epat
itis
C p
atie
nts
by p
hleb
otom
y an
d lo
w ir
on d
iet.
Can
cer
Res
. 200
1;61
:869
7-87
02.
7.
Lee
Sh,
Mol
assi
otis
A.
Die
tary
and
flu
id c
ompl
ianc
e in
Chi
nese
hem
odia
lysi
s pa
tient
s. I
nt J
Nur
s St
ud.
2002
;39:
695-
704.
8.
Po
duva
l RD
, Wol
gem
uth
C, F
erre
ll J,
Ham
mes
MS.
Hyp
erph
osph
atem
ia in
dia
lysi
s pa
tient
s: is
the
re a
rol
e fo
r fo
cuse
d co
unse
ling?
J R
en N
utr.
200
3;13
:219
-223
. 9.
T
ando
n N
, Tha
kur
V, G
upta
n R
K, S
arin
SK
. Ben
efic
ial i
nflu
ence
of
an in
dige
nous
low
-iro
n di
et o
n se
rum
indi
cato
rs o
f ir
on s
tatu
s in
pat
ient
s w
ith c
hron
ic li
ver
dise
ase.
Br
J N
utr.
200
0;83
:235
-23
9.
10.
Zri
nyi M
, Juh
asz
M, B
alla
J, K
aton
a E
, Ben
T, K
akuk
G, P
all D
. Die
tary
sel
f-ef
fica
cy: d
eter
min
ant o
f co
mpl
ianc
e be
havi
ours
and
bio
chem
ical
out
com
es in
hae
mod
ialy
sis
patie
nts.
Nep
hrol
Dia
l Tr
ansp
lant
. 200
3;19
:186
9-73
.
Edi
tion:
200
6 68

INTA
KE D
OMAI
N N
utrie
nt
IMB
AL
AN
CE
OF
NU
TR
IEN
TS
(N
I-5.
5)
De
fin
itio
n
An
unde
sira
ble
com
bina
tion
of in
gest
ed n
utri
ents
, suc
h th
at th
e am
ount
of
one
nutr
ient
inge
sted
inte
rfer
es w
ith o
r al
ters
abs
orpt
ion
and/
or u
tiliz
atio
n of
ano
ther
nu
trie
nt
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Con
sum
ptio
n of
hig
h do
se n
utri
ent s
uppl
emen
ts
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Har
mfu
l bel
iefs
/atti
tude
s ab
out f
ood,
nut
ritio
n an
d nu
triti
on-r
elat
ed in
form
atio
n
Food
fad
dism
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Dat
a
Phy
sica
l Exa
m F
indi
ngs
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Hig
h in
take
of
iron
sup
plem
ents
( z
inc
abso
rptio
n)
Hig
h in
take
of
zinc
sup
plem
ents
( c
oppe
r st
atus
)
Hig
h in
take
of
man
gane
se (
iron
sta
tus)
Clie
nt H
isto
ry
Dia
rrhe
a or
con
stip
atio
n (i
ron
supp
lem
ents
)
Epi
gast
ric
pain
, nau
sea,
vom
iting
, , d
iarr
hea
(zin
c su
pple
men
ts)
Con
trib
utes
to th
e de
velo
pmen
t of
anem
ia (
man
gane
se s
uppl
emen
ts)
Edi
tion:
200
6 69

INTA
KE D
OMAI
N N
utrie
nt
IMB
AL
AN
CE
OF
NU
TR
IEN
TS
(N
I-5.
5)R
efe
ren
ces:
1.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r V
itam
in A
, Vita
min
K, A
rsen
ic, B
oron
, Chr
omiu
m, C
oppe
r, I
odin
e, I
ron,
Man
gane
se, M
olyb
denu
m, N
icke
l,Si
licon
, Van
adiu
m, Z
inc.
Was
hing
ton,
DC
: Nat
iona
l Aca
dem
y Pr
ess;
200
1.
2.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r C
alci
um, P
hosp
horu
s, M
agne
sium
, Vita
min
D, a
nd F
luor
ide.
Was
hing
ton,
DC
: Nat
iona
l Aca
dem
y Pr
ess;
199
7.
Edi
tion:
200
6 70

INTA
KE D
OMAI
N F
at an
d Ch
oles
tero
l
INA
DE
QU
AT
E F
AT
IN
TA
KE
(N
I-51
.1)
De
fin
itio
n
Low
er f
at in
take
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
. Exc
eptio
n: w
hen
the
goal
is w
eigh
t los
s or
du
ring
end
of
life
care
.
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Inap
prop
riat
e fo
od c
hoic
es, e
.g.,
econ
omic
con
stra
ints
, cul
tura
l or
relig
ious
pra
ctic
es, r
estr
ictin
g fo
od g
iven
to e
lder
ly a
nd/o
r ch
ildre
n, s
peci
fic
food
cho
ices
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit,
e.g.
pro
long
ed a
dher
ence
to a
ver
y lo
w f
at d
iet
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or d
isor
dere
d ea
ting
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a T
rien
e: te
trae
ne r
atio
>0.
2
Ant
hrop
omet
ric
Mea
sure
men
ts
Wei
ght l
oss
if in
suff
icie
nt c
alor
ies
cons
umed
Phy
sica
l Exa
min
atio
n F
indi
ngs
Rou
gh, s
caly
ski
n th
at b
ecom
es d
erm
atiti
s w
ith e
ssen
tial f
atty
aci
d de
fici
ency
Foo
d/N
utri
tion
His
tory
R
epor
t or
obse
rvat
ion
of
Inta
ke o
f es
sent
ial f
atty
aci
d co
ntai
ning
foo
ds c
onsi
sten
tly p
rovi
ding
less
than
10%
of
calo
ries
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
prol
onge
d ca
tabo
lic il
lnes
s (e
.g. A
IDS,
tube
rcul
osis
, an
orex
ia n
ervo
sa, s
epsi
s or
sev
ere
infe
ctio
n fr
om r
ecen
t sur
gery
)
Seve
re f
at m
alab
sorp
tion
with
bow
el r
esec
tion,
pan
crea
tic in
suff
icie
ncy,
or
hepa
tic d
isea
se a
ccom
pani
ed b
y st
eato
rrhe
a
Refe
ren
ces:
1.
Die
tary
Ref
eren
ce I
ntak
es fo
r E
nerg
y, C
arbo
hydr
ate,
Fib
er, F
at, F
atty
Aci
ds, C
hole
ster
ol, P
rote
in, a
nd A
min
o A
cids
. Ins
titut
e of
Med
icin
e of
the
Nat
iona
l Aca
dem
ies.
Nat
iona
l Aca
dem
y Pr
ess,
W
ashi
ngto
n, D
.C. 2
002.
Edi
tion:
200
6 71

INTA
KE D
OMAI
N F
at an
d Ch
oles
tero
l
EX
CE
SS
IVE
FA
T I
NT
AK
E (
NI-
51.2
)
De
fin
itio
n
Hig
her
fat i
ntak
e co
mpa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Har
mfu
l bel
iefs
/atti
tude
s ab
out f
ood,
nut
ritio
n, a
nd n
utri
tion-
rela
ted
topi
cs
Lac
k of
acc
ess
to h
ealth
ful f
ood
choi
ces,
e.g
., fo
od p
rovi
ded
by c
areg
iver
, ped
iatr
ics,
hom
eles
s
Cha
nges
in ta
ste
and
appe
tite
or p
refe
renc
e
Lac
k of
val
ue f
or b
ehav
ior
chan
ge, c
ompe
ting
valu
es
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a C
hole
ster
ol >
200
mg/
dL, L
DL
cho
lest
erol
> 1
00 m
g/dL
, HD
L c
hole
ster
ol <
40
mg/
dL, t
rigl
ycer
ides
> 1
50 m
g/dL
Ele
vate
d se
rum
am
ylas
e an
d/or
lipa
se
Ele
vate
d L
FTs,
T. B
ili
Tri
ene-
tetr
aene
rat
io >
0.4
Feca
l fat
> 7
gms/
24
hour
s
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Evi
denc
e of
xan
thom
as
Evi
denc
e of
ski
n le
sion
s
Edi
tion:
200
6 72

INTA
KE D
OMAI
N F
at an
d Ch
oles
tero
l
EX
CE
SS
IVE
FA
T I
NT
AK
E (
NI-
51.2
)F
ood/
Nut
ritio
n H
isto
ry
Rep
orts
or
obse
rvat
ions
of:
Freq
uent
or
larg
e po
rtio
ns o
f hi
gh f
at f
oods
Freq
uent
foo
d pr
epar
atio
n w
ith a
dded
fat
Freq
uent
con
sum
ptio
n of
hig
h ri
sk li
pids
(i.e
. sat
urat
ed f
at, t
rans
fat
, cho
lest
erol
)
Rep
ort o
f fo
ods
cont
aini
ng f
at a
bove
die
t pre
scri
ptio
n
Inad
equa
te in
take
of
esse
ntia
l lip
ids
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
hype
rlip
idem
ia, c
ystic
fib
rosi
s, a
ngin
a, a
rthe
rosc
lero
sis,
pa
ncre
atic
, liv
er, a
nd b
iliar
y di
seas
es, p
ost-
tran
spla
ntat
ion
Med
icat
ion,
e.g
., pa
ncre
atic
enz
ymes
, cho
lest
erol
or
othe
r lip
id lo
wer
ing
med
icat
ions
Dia
rrhe
a, c
ram
ping
, ste
ator
rhea
, epi
gast
ric
pain
Fam
ily h
isto
ry o
f hy
perl
ipid
emia
, ath
eros
cler
osis
or
panc
reat
itis.
Refe
ren
ces:
1.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r E
nerg
y, C
arbo
hydr
ate,
Fib
er, F
at, F
atty
Aci
ds, C
hole
ster
ol, P
rote
in, a
nd A
min
o A
cids
. Was
hing
ton,
DC
: N
atio
nal A
cade
my
Pres
s; 2
002.
2.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: W
eigh
t man
agem
ent.
J A
m D
iet A
ssoc
. 200
2;10
2:11
45-1
155.
3.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: T
otal
die
t app
roac
h to
com
mun
icat
ing
food
and
nut
ritio
n in
form
atio
n. J
Am
Die
t Ass
oc. 2
002;
102:
100-
108.
4.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: T
he r
ole
of d
iete
tics
prof
essi
onal
s in
hea
lth p
rom
otio
n an
d di
seas
e pr
even
tion.
J A
m D
iet A
ssoc
. 200
2;10
2:16
80-1
687.
Edi
tion:
200
6 73

INTA
KE D
OMAI
N F
at an
d Ch
oles
tero
l INA
PP
RO
PR
IAT
E I
NT
AK
E O
F F
OO
D F
AT
S (
NI-
51.3
)
De
fin
itio
n
Inta
ke o
f w
rong
type
or
qual
ity o
f fo
od f
ats
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Har
mfu
l bel
iefs
/atti
tude
s ab
out f
ood,
nut
ritio
n, a
nd n
utri
tion-
rela
ted
topi
cs
Lac
k of
acc
ess
to h
ealth
ful f
ood
choi
ces,
e.g
., fo
od p
rovi
ded
by c
areg
iver
, ped
iatr
ics,
hom
eles
s
Cha
nges
in ta
ste
and
appe
tite
or p
refe
renc
e
Lac
k of
val
ue f
or b
ehav
ior
chan
ge, c
ompe
ting
valu
es
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a C
hole
ster
ol >
200
mg/
dL, L
DL
cho
lest
erol
> 1
00 m
g/dL
, HD
L c
hole
ster
ol <
40
mg/
dL, t
rigl
ycer
ides
> 1
50 m
g/dL
Ele
vate
d se
rum
am
ylas
e an
d/or
lipa
se
Ele
vate
d L
FTs,
T. B
ili,
c-re
activ
e pr
otei
n
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Evi
denc
e of
xan
thom
as
Evi
denc
e of
ski
n le
sion
s
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Freq
uent
foo
d pr
epar
atio
n w
ith a
dded
fat
that
is n
ot o
f de
sire
d ty
pe f
or c
ondi
tion
Freq
uent
con
sum
ptio
n of
fat
s th
at a
re u
ndes
irab
le f
or c
ondi
tion
(i.e
. sat
urat
ed f
at, t
rans
fat
, cho
lest
erol
, om
ega-
6 fa
tty a
cids
)
Inad
equa
te in
take
of
mon
ouns
atur
ated
, pol
yuns
atur
ated
, or
omeg
a-3
fatty
aci
ds
Edi
tion:
200
6 74

INTA
KE D
OMAI
N F
at an
d Ch
oles
tero
l INA
PP
RO
PR
IAT
E I
NT
AK
E O
F F
OO
D F
AT
S (
NI-
51.3
)C
lient
His
tory
C
ondi
tions
ass
ocia
ted
with
a d
iagn
osis
or
trea
tmen
t of
diab
etes
, car
diac
dis
ease
s, o
besi
ty, l
iver
or
bilia
ry d
isor
ders
Dia
rrhe
a, c
ram
ping
, ste
ator
rhea
, epi
gast
ric
pain
Fam
ily h
isto
ry o
f di
abet
es-r
elat
ed h
eart
dis
ease
, hyp
erlip
idem
ia, a
ther
oscl
eros
is o
r pa
ncre
atiti
s.
Clie
nt d
esir
es to
impl
emen
t a M
edite
rran
ean-
type
die
t
Refe
ren
ces:
1.
de L
orge
ril M
, Sal
en P
, Mar
tin J
-L, M
onja
ud I
, Del
aye
J, M
amel
le N
: Med
iterr
anea
n di
et, t
radi
tiona
l ris
k fa
ctor
s, a
nd th
e ra
te o
f ca
rdio
vasc
ular
com
plic
atio
ns a
fter
myo
card
ial i
nfar
ctio
n. F
inal
re
port
of
the
Lyo
n D
iet H
eart
Stu
dy. C
ircu
lati
on. 1
999;
99:
779-
785.
2.
Fr
anz
MJ,
Ban
tle J
P, B
eebe
CA
, Bru
nzel
l JD
, Chi
asso
n J-
L, G
arg
A, H
olzm
eist
er L
A, H
oogw
erf
B, M
ayer
-Dav
is E
, Moo
radi
an A
D, P
urne
ll JQ
, Whe
eler
M: T
echn
ical
rev
iew
. Evi
denc
e-ba
sed
nutr
ition
pri
ncip
les
and
reco
mm
enda
tions
for
the
trea
tmen
t and
pre
vent
ion
of d
iabe
tes
and
rela
ted
com
plic
atio
ns. D
iabe
tes
Car
e. 2
002;
202:
148-
198.
3.
K
noop
s K
TB
, de
Gro
tt L
CPG
M, K
rom
hout
D, P
erri
n A
-E, V
arel
a )
M-V
, Men
otti
A, v
an S
tave
ren
WA
: Med
iter
rane
an d
iet,
lifes
tyle
fac
tors
, and
10-
year
mor
talit
y in
eld
erly
Eur
opea
n m
en a
nd
wom
en. J
AM
A. 2
004;
292:
1433
-143
9,
4.
Kri
s-E
ther
ton
PM, H
arri
s W
S, A
ppel
LJ,
for
the
Nut
riti
on C
omm
ittee
: AH
A s
cien
tific
sta
tem
ent.
Fish
con
sum
ptio
n, f
ish
oil,
omeg
a-3
fatty
aci
ds, a
nd c
ardi
ovas
cula
r di
seas
e. C
ircu
lati
on.
2002
;106
:274
7-27
57.
5.
Pana
giot
akos
DB
, Pits
avos
C, P
olyc
hron
opou
los
E, C
hrys
ohoo
u C
, Zam
pela
s A
, Tri
chop
oulo
u A
. Can
a M
edite
rran
ean
diet
mod
erat
e th
e de
velo
pmen
t and
clin
ical
pro
gres
sion
of
coro
nary
hea
rt
dise
ase?
A s
yste
mat
ic r
evie
w. M
ed S
ci M
onit.
200
4;10
:RA
193-
RA
198.
6.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: W
eigh
t man
agem
ent.
J A
m D
iet A
ssoc
. 200
2;10
2:11
45-1
155.
7.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: T
otal
die
t app
roac
h to
com
mun
icat
ing
food
and
nut
ritio
n in
form
atio
n. J
Am
Die
t Ass
oc. 2
002;
102:
100-
108.
8.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: T
he r
ole
of d
iete
tics
prof
essi
onal
s in
hea
lth p
rom
otio
n an
d di
seas
e pr
even
tion.
J A
m D
iet A
ssoc
. 200
2;10
2:16
80-1
687.
9.
Z
hao
G, E
ther
ton
TD
, Mar
tin K
R, W
est S
G, G
illes
PJ,
Kri
s-E
ther
ton
PM. D
ieta
ry a
lpha
-lin
olen
ic a
cid
redu
ces
infl
amm
ator
y an
d lip
id c
ardi
ovas
cula
r ri
sk f
acto
rs in
hyp
erch
oles
tero
lem
ic m
en a
nd
wom
en. J
Nut
r. 2
004;
134:
2991
-299
7.
Edi
tion:
200
6 75

INTA
KE D
OMAI
N P
rote
in
INA
DE
QU
AT
E P
RO
TE
IN I
NT
AK
E (
NI-
52.1
)
De
fin
itio
n
Low
er in
take
of
prot
ein
cont
aini
ng f
oods
or
subs
tanc
es c
ompa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Phys
iolo
gic
caus
es, e
.g. i
ncre
ased
nut
rien
t nee
ds d
ue to
pro
long
ed c
atab
olic
illn
ess,
mal
abso
rptio
n, a
ge o
r co
nditi
on
Lac
k of
acc
ess
to f
ood,
e.g
., ec
onom
ic c
onst
rain
ts, c
ultu
ral o
r re
ligio
us p
ract
ices
, res
tric
ting
food
giv
en to
eld
erly
and
/or
child
ren
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or d
isor
dere
d ea
ting
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
min
atio
n F
indi
ngs
Die
t His
tory
R
epor
t or
obse
rvat
ion
of
Insu
ffic
ient
inta
ke o
f pr
otei
n to
mee
t req
uire
men
ts
Cul
tura
l or
relig
ious
pra
ctic
es th
at li
mit
prot
ein
inta
ke
Eco
nom
ic c
onst
rain
ts th
at li
mit
food
ava
ilabi
lity
Prol
onge
d ad
here
nce
to a
ver
y lo
w p
rote
in w
eigh
t los
s di
et
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
seve
re p
rote
in m
alab
sorp
tion
such
as
bow
el r
esec
tion
Refe
ren
ces:
1.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r E
nerg
y, C
arbo
hydr
ate,
Fib
er, F
at, F
atty
Aci
ds, C
hole
ster
ol, P
rote
in, a
nd A
min
o A
cids
. Was
hing
ton
DC
: N
atio
nal A
cade
my
Pres
s; 2
002.
Edi
tion:
200
6 76

INTA
KE D
OMAI
N P
rote
in
EX
CE
SS
IVE
PR
OT
EIN
IN
TA
KE
(N
I-52
.2)
De
fin
itio
n
Inta
ke a
bove
the
reco
mm
ende
d le
vel o
f pr
otei
n co
mpa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Liv
er d
ysfu
nctio
n
Ren
al d
ysfu
nctio
n
Har
mfu
l bel
iefs
/atti
tude
s ab
out f
ood,
nut
ritio
n an
d nu
triti
on-r
elat
ed to
pics
Lac
k of
acc
ess
to s
peci
aliz
ed p
rote
in p
rodu
cts
Met
abol
ic a
bnor
mal
ity
Food
fad
dism
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a A
ltere
d la
bora
tory
val
ues
e.g.
B
UN
, g
lom
erul
ar f
iltra
tion
rate
(al
tere
d re
nal s
tatu
s)
Ant
hrop
omet
ric
Mea
sure
men
ts
Gro
wth
stu
ntin
g or
fai
lure
bas
ed o
n N
CH
S gr
owth
cha
rts
(met
abol
ic d
isor
ders
)
Phy
sica
l Exa
m F
indi
ngs
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Hig
her
than
rec
omm
ende
d to
tal p
rote
in in
take
, e.g
., ea
rly
rena
l dis
ease
, adv
ance
d liv
er d
isea
se w
ith c
onfu
sion
Inap
prop
riat
e su
pple
men
tatio
n
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
earl
y re
nal d
isea
se o
r ad
vanc
ed li
ver
dise
ase
with
con
fusi
on
Edi
tion:
200
6 77

INTA
KE D
OMAI
N P
rote
in
EX
CE
SS
IVE
PR
OT
EIN
IN
TA
KE
(N
I-52
.2)
Refe
ren
ces:
1.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Foo
d an
d nu
triti
on m
isin
form
atio
n. J
Am
Die
t Ass
oc. 2
002;
102:
260-
266.
2.
B
eto
JA, B
ansa
l VK
. Med
ical
nut
ritio
n th
erap
y in
chr
onic
kid
ney
failu
re: I
nteg
ratin
g cl
inic
al p
ract
ice
guid
elin
es. J
Am
Die
t Ass
oc. 2
004;
104:
404-
409.
3.
B
rand
le E
, Sie
bert
h H
G, H
autm
ann
RE
. Eff
ect o
f ch
roni
c di
etar
y pr
otei
n in
take
on
the
rena
l fun
ctio
n in
hea
lthy
subj
ects
. Eur
J C
lin
Nut
r. 1
996;
50:7
34-7
40.
4.
Fras
setto
LA
, Tod
d K
M, M
orri
s R
C J
r, S
ebas
tian
A. E
stim
atio
n of
net
end
ogen
ous
nonc
arbo
nic
acid
pro
duct
ion
in h
uman
s fr
om d
iet,
pota
ssiu
m a
nd p
rote
in c
onte
nts.
Am
J C
lin N
utr.
199
8;68
:576
-58
3.
5.
Frie
dman
N, e
d. A
bsor
ptio
n an
d U
tiliz
atio
n of
Am
ino
Aci
ds, V
ol. I
. Boc
a R
aton
, FL
: CR
C P
ress
, 198
9, p
p229
-242
. 6,
H
ooge
veen
EK
, Kos
tens
e PJ
, Jag
er A
, Hei
ne R
J, J
akob
s C
, Bou
ter
LM
, Don
ker
AJ,
Ste
how
er C
D. S
erum
hom
ocys
tein
e le
vel a
nd p
rote
in in
take
are
rel
ated
to r
isk
of m
icro
albu
min
uria
: the
Hoo
rn
stud
y. K
idne
y In
t. 19
98;5
4:20
3-20
9.
7.
R
udm
an D
, DiF
ulco
TJ,
Gal
ambo
s JT
, Sm
ith R
B 3
rd, S
alam
AA
, War
ren
WD
. Max
imum
rat
e of
exc
retio
n an
d sy
nthe
sis
of u
rea
in n
orm
al a
nd c
irrh
otic
sub
ject
s. J
Cli
n In
vest
. 197
3.;5
2:22
41-
2249
.
Edi
tion:
200
6 78

INTA
KE D
OMAI
N P
rote
in
INA
PP
RO
PR
IAT
E I
NT
AK
E O
F A
MIN
O A
CID
S (
SP
EC
IFY
) (N
I-52
.3)
De
fin
itio
n
Inta
ke th
at is
mor
e or
less
than
rec
omm
ende
d le
vel a
nd/o
r ty
pe o
f am
ino
acid
s co
mpa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Liv
er d
ysfu
nctio
n
Ren
al d
ysfu
nctio
n
Har
mfu
l bel
iefs
/atti
tude
s ab
out f
ood,
nut
ritio
n an
d nu
triti
on-r
elat
ed to
pics
Mis
used
spe
cial
ized
pro
tein
pro
duct
s
Met
abol
ic a
bnor
mal
ity
Food
fad
dism
Inbo
rn e
rror
s of
met
abol
ism
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a A
ltere
d la
bora
tory
val
ues
e.g.
B
UN
, g
lom
erul
ar f
iltra
tion
rate
(al
tere
d re
nal s
tatu
s); i
ncre
ased
uri
nary
3-m
ethy
l-hi
stid
ine
Ele
vate
d sp
ecif
ic a
min
o ac
ids
(inb
orn
erro
rs o
f m
etab
olis
m)
Ure
mia
, azo
tem
ia (
rena
l pat
ient
s)
Ele
vate
d ho
moc
yste
ine
or a
mm
onia
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Phys
ical
or
neur
olog
ical
cha
nges
(in
born
err
ors
of m
etab
olis
m)
Edi
tion:
200
6 79

INTA
KE D
OMAI
N P
rote
in
INA
PP
RO
PR
IAT
E I
NT
AK
E O
F A
MIN
O A
CID
S (
SP
EC
IFY
) (N
I-52
.3)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Hig
her
than
rec
omm
ende
d am
ino
acid
inta
ke, e
.g.,
earl
y re
nal d
isea
se, a
dvan
ced
liver
dis
ease
, inb
orn
erro
r of
met
abol
ism
Hig
her
than
rec
omm
ende
d ty
pe o
f am
ino
acid
s fo
r pr
escr
ibed
PE
N th
erap
y
Inap
prop
riat
e su
pple
men
tatio
n, a
s fo
r at
hlet
es
Hig
her
than
rec
omm
ende
d ty
pe o
f pr
otei
n, e
.g.,
exce
ss p
heny
lala
nine
inta
ke
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f ill
ness
that
req
uire
s PE
N th
erap
y
His
tory
of
use
of a
min
o ac
ids
or p
rote
in p
owde
rs f
or a
thle
tic e
nhan
cem
ent
His
tory
of
inbo
rn e
rror
of
met
abol
ism
Refe
ren
ces:
1.
Bet
o JA
, Ban
sal V
K. M
edic
al n
utri
tion
ther
apy
in c
hron
ic k
idne
y fa
ilure
: Int
egra
ting
clin
ical
pra
ctic
e gu
idel
ines
. J A
m D
iet A
ssoc
. 200
4;10
4:40
4-40
9.
2.
Bra
ndle
E, S
iebe
rth
HG
, Hau
tman
n R
E. E
ffec
t of
chro
nic
diet
ary
prot
ein
inta
ke o
n th
e re
nal f
unct
ion
in h
ealth
y su
bjec
ts. E
ur J
Cli
n N
utr.
199
6;50
:734
-740
. 3.
C
ohn
RM
, Rot
h K
S. H
yper
amm
onia
, ban
e of
the
brai
n. C
lin P
edia
tr. 2
004;
43:6
83.
4.
Fras
setto
LA
, Tod
d K
M, M
orri
s R
C J
r, S
ebas
tian
A. E
stim
atio
n of
net
end
ogen
ous
nonc
arbo
nic
acid
pro
duct
ion
in h
uman
s fr
om d
iet,
pota
ssiu
m a
nd p
rote
in c
onte
nts.
Am
J C
lin N
utr.
199
8;68
:576
-58
3.
5.
Frie
dman
N, e
d. A
bsor
ptio
n an
d U
tiliz
atio
n of
Am
ino
Aci
ds, V
ol. I
. Boc
a R
aton
, FL
: CR
C P
ress
, 198
9, p
p229
-242
. 6.
H
ooge
veen
EK
, Kos
tens
e PJ
, Jag
er A
, Hei
ne R
J, J
akob
s C
, Bou
ter
LM
, Don
ker
AJ,
Ste
how
er C
D. S
erum
hom
ocys
tein
e le
vel a
nd p
rote
in in
take
are
rel
ated
to r
isk
of m
icro
albu
min
uria
: the
Hoo
rn
stud
y. K
idne
y In
t. 19
98;5
4:20
3-20
9.
7.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: F
ood
and
nutr
ition
mis
info
rmat
ion.
J A
m D
iet A
ssoc
. 200
2;10
2:26
0-26
6.
8.
Rud
man
D, D
iFul
co T
J, G
alam
bos
JT, S
mith
RB
3rd
, Sal
am A
A, W
arre
n W
D. M
axim
um r
ate
of e
xcre
tion
and
synt
hesi
s of
ure
a in
nor
mal
and
cir
rhot
ic s
ubje
cts.
J C
lin I
nves
t. 19
73.;5
2:22
41-2
249.
Edi
tion:
200
6 80

INTA
KE D
OMAI
N C
arbo
hydr
ate a
nd F
iber
Inta
ke
INA
DE
QU
AT
E C
AR
BO
HY
DR
AT
E I
NT
AK
E (
NI-
53.1
)
De
fin
itio
n
Low
er in
take
of
carb
ohyd
rate
con
tain
ing
food
s or
sub
stan
ces
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Phys
iolo
gic
caus
es, e
.g. i
ncre
ased
ene
rgy
need
s du
e to
incr
ease
d ac
tivity
leve
l or
met
abol
ic c
hang
e, m
alab
sorp
tion
Lac
k of
acc
ess
to f
ood,
e.g
., ec
onom
ic c
onst
rain
ts, c
ultu
ral o
r re
ligio
us p
ract
ices
, res
tric
ting
food
giv
en to
eld
erly
and
/or
child
ren
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or d
isor
dere
d ea
ting
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
min
atio
n F
indi
ngs
Ket
one
smel
l on
brea
th
Die
t His
tory
R
epor
t or
obse
rvat
ion
of
Car
bohy
drat
e in
take
bel
ow r
ecom
men
ded
amou
nts
Inab
ility
to in
depe
nden
tly c
onsu
me
food
s/fl
uids
, e.g
., di
min
ishe
d m
obili
ty in
han
d, w
rist
, or
digi
ts
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
panc
reat
ic in
suff
icie
ncy,
hep
atic
dis
ease
, cel
iac
dise
ase,
se
izur
e di
sord
er, c
arbo
hydr
ate
mal
abso
rptio
n, o
r lo
w c
arbo
hydr
ate
diet
s
Refe
ren
ces:
1.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r E
nerg
y, C
arbo
hydr
ate,
Fib
er, F
at, F
atty
Aci
ds, C
hole
ster
ol, P
rote
in, a
nd A
min
o A
cids
. Was
hing
ton
DC
: N
atio
nal A
cade
my
Pres
s; 2
002.
Edi
tion:
200
6 81

INTA
KE D
OMAI
N C
arbo
hydr
ate a
nd F
iber
Inta
ke
EX
CE
SS
IVE
CA
RB
OH
YD
RA
TE
IN
TA
KE
(N
I-53
.2)
De
fin
itio
n
Inta
ke a
bove
the
reco
mm
ende
d le
vel a
nd ty
pe o
f ca
rboh
ydra
te c
ompa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Phys
iolo
gic
caus
es r
equi
ring
mod
ifie
d ca
rboh
ydra
te in
take
, e.g
., di
abet
es m
ellit
us, l
acta
se d
efic
ienc
y, s
ucra
se-i
som
alta
se d
efic
ienc
y, a
ldol
ase-
B d
efic
ienc
y
Cul
tura
l or
relig
ious
pra
ctic
es th
at in
terf
ere
with
the
abili
ty to
red
uce
carb
ohyd
rate
inta
ke
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit,
e.g.
, ina
bilit
y to
acc
ess
suff
icie
nt in
form
atio
n co
ncer
ning
app
ropr
iate
car
bohy
drat
e in
take
Food
and
nut
ritio
n co
mpl
ianc
e lim
itatio
ns, e
.g.,
lack
of
will
ingn
ess
or f
ailu
re to
mod
ify
carb
ohyd
rate
inta
ke in
res
pons
e to
rec
omm
enda
tions
fro
m a
di
etiti
an o
r ph
ysic
ian
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or d
isor
dere
d ea
ting
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a H
yper
glyc
emia
(fa
stin
g bl
ood
suga
r >1
26m
g/dL
)
Hem
oglo
bin
A1C
>6%
Abn
orm
al o
ral g
luco
se to
lera
nce
test
(2
hour
pos
t loa
d gl
ucos
e >
200
mg/
dL)
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
min
atio
n F
indi
ngs
Den
tal c
arie
s
Dia
rrhe
a in
res
pons
e to
car
bohy
drat
e fe
edin
g
Edi
tion:
200
6 82

INTA
KE D
OMAI
N C
arbo
hydr
ate a
nd F
iber
Inta
ke
EX
CE
SS
IVE
CA
RB
OH
YD
RA
TE
IN
TA
KE
(N
I-53
.2)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Cul
tura
l or
relig
ious
pra
ctic
es th
at d
o no
t sup
port
mod
ific
atio
n of
die
tary
car
bohy
drat
e in
take
Eco
nom
ic c
onst
rain
ts th
at li
mit
avai
labi
lity
of a
ppro
pria
te f
oods
Car
bohy
drat
e in
take
that
is c
onsi
sten
tly a
bove
rec
omm
ende
d am
ount
s
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
diab
etes
mel
litus
, inb
orn
erro
rs o
f ca
rboh
ydra
te
met
abol
ism
, lac
tase
def
icie
ncy,
sev
ere
infe
ctio
n, s
epsi
s, o
r ob
esity
Chr
onic
use
of
med
icat
ions
that
cau
se h
yper
glyc
emia
, e.g
. ste
roid
s
Panc
reat
ic in
suff
icie
ncy
resu
lting
in r
educ
ed in
sulin
pro
duct
ion
Refe
ren
ces:
1.
Bow
man
BA
, Rus
sell
RM
. Pre
sent
Kno
wle
dge
in N
utri
tion.
8th E
d. W
ashi
ngto
n, D
C: I
LSI
Pre
ss, 2
001.
2.
C
lem
ent S
, Bra
ithw
aite
SS,
McG
ee M
F, A
hman
n A
, et a
l. M
anag
emen
t of
diab
etes
in h
ospi
tals
. Dia
bete
s C
are.
200
4;27
:553
-592
. 3.
N
atio
nal A
cade
my
of S
cien
ces,
Ins
titut
e of
Med
icin
e. D
ieta
ry R
efer
ence
Int
akes
for
Ene
rgy,
Car
bohy
drat
e, F
iber
, Fat
, Fat
ty A
cids
, Cho
lest
erol
, Pro
tein
, and
Am
ino
Aci
ds. W
ashi
ngto
n, D
C:
Nat
iona
l Aca
dem
y Pr
ess;
200
2.
4.
The
Exp
ert C
omm
ittee
on
the
Dia
gnos
is a
nd C
lass
ific
atio
n of
Dia
bete
s M
ellit
us. D
iagn
osis
and
cla
ssif
icat
ion
of d
iabe
tes
mel
litu
s.D
iabe
tes
Car
e. 2
004;
27:p
S5-p
S10.
Edi
tion:
200
6 83

INTA
KE D
OMAI
N C
arbo
hydr
ate a
nd F
iber
Inta
ke
INA
PP
RO
PR
IAT
E I
NT
AK
E O
F T
YP
ES
OF
CA
RB
OH
YD
RA
TE
S (
SP
EC
IFY
) (N
I-53
.3)
De
fin
itio
n
Inta
ke o
r th
e ty
pe o
r am
ount
of
carb
ohyd
rate
that
is a
bove
or
belo
w th
e es
tabl
ishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Phys
iolo
gic
caus
es r
equi
ring
car
eful
use
of
mod
ifie
d ca
rboh
ydra
te, e
.g.,
diab
etes
mel
litus
, met
abol
ic s
yndr
ome,
hyp
ogly
cem
ia, c
elia
c di
seas
e, a
llerg
ies,
ob
esity
Cul
tura
l or
relig
ious
pra
ctic
es th
at in
terf
ere
with
the
abili
ty to
reg
ulat
e ty
pes
of c
arbo
hydr
ate
cons
umed
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit,
e.g.
, ina
bilit
y to
acc
ess
suff
icie
nt in
form
atio
n co
ncer
ning
mor
e ap
prop
riat
e ca
rboh
ydra
te ty
pes
and/
or
amou
nts
Food
and
nut
ritio
n co
mpl
ianc
e lim
itatio
ns, e
.g.,
lack
of
will
ingn
ess
or f
ailu
re to
mod
ify
carb
ohyd
rate
inta
ke in
res
pons
e to
rec
omm
enda
tions
fro
m a
di
etiti
an, p
hysi
cian
, or
care
give
r
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or d
isor
dere
d ea
ting
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a H
ypog
lyce
mia
or
hype
rgly
cem
ia d
ocum
ente
d on
reg
ular
bas
is w
hen
com
pare
d w
ith g
oal o
f m
aint
aini
ng g
luco
se
leve
ls a
t or
belo
w 1
40 m
g/dl
thro
ugho
ut th
e da
y
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
min
atio
n F
indi
ngs
Edi
tion:
200
6 84

INTA
KE D
OMAI
N C
arbo
hydr
ate a
nd F
iber
Inta
ke
INA
PP
RO
PR
IAT
E I
NT
AK
E O
F T
YP
ES
OF
CA
RB
OH
YD
RA
TE
S (
SP
EC
IFY
) (N
I-53
.3)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Dia
rrhe
a in
res
pons
e to
hig
h re
fine
d ca
rboh
ydra
te in
take
Eco
nom
ic c
onst
rain
ts th
at li
mit
avai
labi
lity
of a
ppro
pria
te f
oods
Car
bohy
drat
e in
take
that
is d
iffe
rent
fro
m r
ecom
men
ded
type
s
Alle
rgic
rea
ctio
ns to
cer
tain
car
bohy
drat
e fo
ods
or f
ood
grou
ps
Lim
ited
know
ledg
e of
car
bohy
drat
e co
mpo
sitio
n of
foo
ds o
r of
car
bohy
drat
e m
etab
olis
m
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
diab
etes
mel
litus
, obe
sity
, met
abol
ic s
yndr
ome,
hy
pogl
ycem
ia
Chr
onic
use
of
med
icat
ions
that
cau
se a
ltere
d gl
ucos
e le
vels
, e.g
. ste
roid
s, a
ntid
epre
ssan
ts, a
ntip
sych
otic
s
Refe
ren
ces:
1.
Bow
man
BA
, Rus
sell
RM
. Pre
sent
Kno
wle
dge
in N
utri
tion.
8th E
d. W
ashi
ngto
n, D
C: I
LSI
Pre
ss, 2
001.
2.
C
lem
ent S
, Bra
ithw
aite
SS,
McG
ee M
F, A
hman
n A
, et a
l. M
anag
emen
t of
diab
etes
in h
ospi
tals
. Dia
bete
s C
are.
200
4;27
:553
-592
. 3.
Fr
anz
MJ,
Ban
tle J
P, B
eebe
CA
, Bru
nzel
l JD
, Chi
asso
n J-
L, G
arg
A, H
olzm
eist
er L
A, H
oogw
erf
B, M
ayer
-Dav
is E
, Moo
radi
an A
D, P
urne
ll JQ
, Whe
eler
M: T
echn
ical
rev
iew
. Evi
denc
e-ba
sed
nutr
ition
pri
ncip
les
and
reco
mm
enda
tions
for
the
trea
tmen
t and
pre
vent
ion
of d
iabe
tes
and
rela
ted
com
plic
atio
ns. D
iabe
tes
Car
e 20
02;2
02:1
48-1
98.
4.
Sh
eard
NF,
Cla
rk N
G, B
rand
-Mill
er J
C, F
ranz
MJ,
Pi-
Sun
yer
FX, M
ayer
-Dav
is E
, Kul
karn
i K, G
eil P
: A s
tate
men
t by
the
Am
eric
an D
iabe
tes
Ass
ocia
tion.
Die
tary
car
bohy
drat
e (a
mou
nt a
nd ty
pe)
in th
e pr
even
tion
and
man
agem
ent o
f di
abet
es. D
iabe
tes
Car
e 20
04;2
7:22
66-2
271.
5.
G
ross
LS,
Li L
, For
d E
S, L
iu S
: Inc
reas
ed c
onsu
mpt
ion
of r
efin
ed c
arbo
hydr
ates
and
epi
dem
ic o
r ty
pe 2
dia
bete
s in
the
Uni
ted
Stat
es: a
n ec
olog
ic a
sses
smen
t. A
m J
Cli
n N
utr
2004
;79:
774-
779.
6.
Fr
ench
S, L
in B
-H, G
uthe
rie
JF: N
atio
nal t
rend
s in
sof
t dri
nk c
onsu
mpt
ion
amon
g ch
ildre
n an
d ad
oles
cent
s ag
e 6
to17
yea
rs: p
reva
lenc
e, a
mou
nts,
and
sou
rces
, 197
7/19
78 to
199
4/19
98. J
Am
Die
t A
ssoc
2003
;103
L13
26-1
331,
7.
N
atio
nal A
cade
my
of S
cien
ces,
Ins
titut
e of
Med
icin
e. D
ieta
ry R
efer
ence
Int
akes
for
Ene
rgy,
Car
bohy
drat
e, F
iber
, Fat
, Fat
ty A
cids
, Cho
lest
erol
, Pro
tein
, and
Am
ino
Aci
ds. W
ashi
ngto
n, D
C:
Nat
iona
l Aca
dem
y Pr
ess;
200
2.
8.
Tef
f K
L, E
lliot
t SS
, Tsc
höp
M, K
ieff
er T
J, R
ader
D, H
eim
an M
, Tow
nsen
d R
R, K
eim
NL
, D’A
less
io D
, Hav
el P
J: D
ieta
ry f
ruct
ose
redu
ces
circ
ulat
ing
insu
lin a
nd le
ptin
, atte
nuat
es p
ostp
rand
ial
supp
ress
ion
of g
hrel
in, a
nd in
crea
ses
trig
lyce
ride
s in
wom
en. J
Cli
n E
ndoc
rino
l Met
ab 2
004;
89:2
963-
2972
.9.
T
he E
xper
t Com
mitt
ee o
n th
e D
iagn
osis
and
Cla
ssif
icat
ion
of D
iabe
tes
Mel
litus
. Dia
gnos
is a
nd c
lass
ific
atio
n of
dia
bete
s m
elli
tus.
Dia
bete
s C
are.
200
4;27
:pS5
-pS1
0.
Edi
tion:
200
6 85
INTA
KE D
OMAI
N C
arbo
hydr
ate a
nd F
iber
Inta
ke
INC
ON
SIS
TE
NT
CA
RB
OH
YD
RA
TE
IN
TA
KE
(N
I-53
.4)
De
fin
itio
n
Inco
nsis
tent
tim
ing
of c
arbo
hydr
ate
inta
ke th
roug
hout
the
day,
day
to d
ay, o
r a
patte
rn o
f ca
rboh
ydra
te in
take
that
is n
ot c
onsi
sten
t with
rec
omm
ende
d pa
ttern
ba
sed
upon
phy
siol
ogic
or
med
icat
ion
need
s
Eti
olog
y(C
ause
/Con
trib
utin
g R
isk
Fac
tors
)Fa
ctor
s ga
ther
ed d
urin
g th
e nu
triti
on a
sses
smen
t pro
cess
that
con
trib
ute
to th
e ex
iste
nce
or th
e m
aint
enan
ce o
f pa
thop
hysi
olog
ical
, psy
chos
ocia
l, si
tuat
iona
l, de
velo
pmen
tal,
cultu
ral,
and/
or e
nvir
onm
enta
l pro
blem
s.
Phys
iolo
gic
caus
es r
equi
ring
car
eful
tim
ing
and
cons
iste
ncy
in th
e am
ount
of
carb
ohyd
rate
, e.g
., di
abet
es m
ellit
us, h
ypog
lyce
mia
Cul
tura
l, re
ligio
us p
ract
ices
, or
lifes
tyle
fac
tors
that
inte
rfer
e w
ith th
e ab
ility
to r
egul
ate
timin
g of
car
bohy
drat
e co
nsum
ptio
n
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit,
e.g.
, ina
bilit
y to
acc
ess
suff
icie
nt in
form
atio
n co
ncer
ning
mor
e ap
prop
riat
e tim
ing
of c
arbo
hydr
ate
inta
ke
Food
and
nut
ritio
n co
mpl
ianc
e lim
itatio
ns, e
.g.,
lack
of
will
ingn
ess
or f
ailu
re to
mod
ify
carb
ohyd
rate
tim
ing
in r
espo
nse
to r
ecom
men
datio
ns f
rom
a
diet
itian
, ph
ysic
ian,
or
care
give
r
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or d
isor
dere
d ea
ting
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nu
trit
ion
Assessm
en
t C
ate
go
ry
Po
ten
tial In
dic
ato
rs o
f th
is N
utr
itio
n D
iag
no
sis
(o
ne
or
mo
re m
ust
be p
resen
t)
Bio
chem
ical
Dat
a H
ypog
lyce
mia
or
hype
rgly
cem
ia d
ocum
ente
d on
reg
ular
bas
is a
ssoc
iate
d w
ith in
cons
iste
nt c
arbo
hydr
ate
inta
ke
Wid
e va
riat
ions
in b
lood
glu
cose
leve
ls
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
min
atio
n F
indi
ngs
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Eco
nom
ic c
onst
rain
ts th
at li
mit
avai
labi
lity
of a
ppro
pria
te f
oods
Car
bohy
drat
e in
take
that
is d
iffe
rent
fro
m r
ecom
men
ded
type
s or
inge
sted
on
an ir
regu
lar
basi
s
Edi
tion:
200
6 86
INTA
KE D
OMAI
N C
arbo
hydr
ate a
nd F
iber
Inta
ke
INC
ON
SIS
TE
NT
CA
RB
OH
YD
RA
TE
IN
TA
KE
(N
I-53
.4)
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
diab
etes
mel
litus
, obe
sity
, met
abol
ic s
yndr
ome,
hy
pogl
ycem
ia
Use
of
insu
lin o
r in
sulin
sec
reta
gogu
es
Chr
onic
use
of
med
icat
ions
that
cau
se a
ltere
d gl
ucos
e le
vels
, e.g
. ste
roid
s, a
ntid
epre
ssan
ts, a
ntip
sych
otic
s
Refe
ren
ces:
1.
Bow
man
BA
, Rus
sell
RM
. Pre
sent
Kno
wle
dge
in N
utri
tion.
8th E
d. W
ashi
ngto
n, D
C: I
LSI
Pre
ss, 2
001.
2.
C
lem
ent S
, Bra
ithw
aite
SS,
McG
ee M
F, A
hman
n A
, et a
l. M
anag
emen
t of
diab
etes
in h
ospi
tals
. Dia
bete
s C
are.
200
4;27
:553
-592
. 3.
C
ryer
PE
, Dav
is S
N, S
ham
oon
H: T
echn
ical
rev
iew
. Hyp
ogly
cem
ia in
dia
bete
s. D
iabe
tes
Car
e 20
03;2
6L19
02-1
912.
4.
Fr
anz
MJ,
Ban
tle J
P, B
eebe
CA
, Bru
nzel
l JD
, Chi
asso
n J-
L, G
arg
A, H
olzm
eist
er L
A, H
oogw
erf
B, M
ayer
-Dav
is E
, Moo
radi
an A
D, P
urne
ll JQ
, Whe
eler
M: T
echn
ical
rev
iew
. Evi
denc
e-ba
sed
nutr
ition
pri
ncip
les
and
reco
mm
enda
tions
for
the
trea
tmen
t and
pre
vent
ion
of d
iabe
tes
and
rela
ted
com
plic
atio
ns. D
iabe
tes
Car
e 20
02;2
02:1
48-1
98.
5.
N
atio
nal A
cade
my
of S
cien
ces,
Ins
titut
e of
Med
icin
e. D
ieta
ry R
efer
ence
Int
akes
for
Ene
rgy,
Car
bohy
drat
e, F
iber
, Fat
, Fat
ty A
cids
, Cho
lest
erol
, Pro
tein
, and
Am
ino
Aci
ds. W
ashi
ngto
n, D
C:
Nat
iona
l Aca
dem
y Pr
ess;
200
2.
6.
Rab
asa-
Lho
ret R
, Gar
on J
, Lan
gelie
r H
, Poi
sson
D, C
hias
son
J-L
: The
eff
ects
of
mea
l car
bohy
drat
e co
nten
t on
insu
lin r
equi
rem
ents
in ty
pe 1
pat
ient
s w
ith d
iabe
tes
trea
ted
inte
nsiv
ely
wit
h th
e ba
sal b
olus
(ul
tral
ente
-reg
ular
) in
sulin
reg
imen
. Dia
bete
s C
are
1999
;22:
667-
673.
7.
Sa
voca
MR
, Mill
er C
K, L
udw
ig D
A: F
ood
habi
ts a
re r
elat
ed to
gly
cem
ic c
ontr
ol a
mon
g pe
ople
with
type
2 d
iabe
tes
mel
litus
. J A
m D
iet A
ssoc
200
4;10
4:56
0-56
6.
8.
The
Exp
ert C
omm
ittee
on
the
Dia
gnos
is a
nd C
lass
ific
atio
n of
Dia
bete
s M
ellit
us. D
iagn
osis
and
cla
ssif
icat
ion
of d
iabe
tes
mel
litu
s.D
iabe
tes
Car
e. 2
004;
27:p
S5-p
S10.
9.
W
olev
er T
MS,
Ham
ad S
, Chi
asso
n J-
L, J
osse
RG
, Lei
ter
LA
, Rod
ger
NW
, Ros
s SA
, Rya
n E
A: D
ay-t
o-da
y co
nsis
tenc
y in
am
ount
and
sou
rce
of c
arbo
hydr
ate
inta
ke a
ssoc
iate
d w
ith im
prov
ed
gluc
ose
cont
rol i
n ty
pe 1
dia
bete
s. J
Am
Col
l Nut
r 19
99; 1
8:24
2-24
7.
Edi
tion:
200
6 87

INTA
KE D
OMAI
N C
arbo
hydr
ate a
nd F
iber
Inta
ke IN
AD
EQ
UA
TE
FIB
ER
IN
TA
KE
(N
I-53
.5)
De
fin
itio
n
Low
er in
take
of
fibe
r co
ntai
ning
foo
ds o
r su
bsta
nces
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Lac
k of
acc
ess
to f
iber
con
tain
ing
food
s
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or d
isor
dere
d ea
ting
Prol
onge
d ad
here
nce
to a
low
fib
er o
r lo
w r
esid
ue d
iet
Dif
ficu
lty c
hew
ing
or s
wal
low
ing
high
fib
er f
oods
Eco
nom
ic c
onst
rain
ts th
at li
mit
avai
labi
lity
of a
ppro
pria
te f
oods
Inab
ility
or
unw
illin
gnes
s to
pur
chas
e or
con
sum
e fi
ber
cont
aini
ng f
oods
Inap
prop
riat
e fo
od p
repa
ratio
n pr
actic
es, e
.g.,
relia
nce
on o
ver
proc
esse
d, o
verc
ooke
d fo
ods
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
min
atio
n F
indi
ngs
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Insu
ffic
ient
inta
ke o
f fi
ber
whe
n co
mpa
red
to r
ecom
men
ded
amou
nts
(38
g/da
y fo
r m
en a
nd 2
5 g/
day
for
wom
en)
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
ulce
r di
seas
e, in
flam
mat
ory
bow
el d
isea
se, o
r sh
ort b
owel
sy
ndro
me
trea
ted
with
a lo
w f
iber
die
t
Low
sto
ol v
olum
e
Edi
tion:
200
6 88

INTA
KE D
OMAI
N C
arbo
hydr
ate a
nd F
iber
Inta
ke IN
AD
EQ
UA
TE
FIB
ER
IN
TA
KE
(N
I-53
.5)
Refe
ren
ces:
1.
DiP
alm
a JA
. Cur
rent
trea
tmen
t opt
ions
for
chr
onic
con
stip
atio
n. R
ev G
astr
oent
erol
Dis
ord
2004
;2:S
34-S
42.
2.
Hig
gins
PD
, Joh
anso
n JF
. Epi
dem
iolo
gy o
f co
nstip
atio
n in
Nor
th A
mer
ica:
a s
yste
mat
ic r
evie
w. A
m J
Gas
troe
nter
ol 2
004;
99:7
50-7
59.
3.
Lem
bo A
, Cam
ilier
i M. C
hron
ic c
onst
ipat
ion.
New
Eng
J M
ed 2
003;
349:
360-
368.
4.
N
atio
nal A
cade
my
of S
cien
ces,
Ins
titut
e of
Med
icin
e. D
ieta
ry R
efer
ence
Int
akes
for
Ene
rgy,
Car
bohy
drat
e, F
iber
, Fat
, Fat
ty A
cids
, Cho
lest
erol
, Pro
tein
, and
Am
ino
Aci
ds. W
ashi
ngto
n, D
C:
Nat
iona
l Aca
dem
y Pr
ess;
200
2.
5.
Tal
ley
NJ.
Def
initi
on, e
pide
mio
logy
, and
impa
ct o
f ch
roni
c co
nstip
atio
n. R
ev G
astr
oent
erol
Dis
ord
2004
;2:S
3-S1
0.
Edi
tion:
200
6 89

INTA
KE D
OMAI
N C
arbo
hydr
ate a
nd F
iber
Inta
ke
EX
CE
SS
IVE
FIB
ER
IN
TA
KE
(N
I-53
.6)
De
fin
itio
n
Hig
her
inta
ke o
f fi
ber
cont
aini
ng f
oods
or
subs
tanc
es c
ompa
red
to r
ecom
men
datio
ns b
ased
upo
n pa
tient
/clie
nt c
ondi
tion
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit a
bout
des
irab
le q
uant
ities
of
fibe
r fo
r in
divi
dual
con
ditio
n
Har
mfu
l bel
iefs
or
attit
udes
abo
ut f
ood
or n
utri
tion-
rela
ted
topi
cs, e
.g.,
obse
ssio
n w
ith b
owel
fre
quen
cy a
nd h
abits
Lac
k of
kno
wle
dge
abou
t app
ropr
iate
fib
er in
take
for
con
ditio
n
Poor
den
titio
n, G
I st
rict
ure
or d
ysm
otili
ty
Food
pre
para
tion
or e
atin
g pa
ttern
s th
at in
volv
e on
ly h
igh
fibe
r fo
ods
to th
e ex
clus
ion
of o
ther
nut
rien
t-de
nse
food
s
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
min
atio
n F
indi
ngs
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Fibe
r in
take
hig
her
than
tole
rate
d or
gen
eral
ly r
ecom
men
ded
for
curr
ent m
edic
al c
ondi
tion
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
ulce
r di
seas
e, ir
rita
ble
bow
el s
yndr
ome,
infl
amm
ator
y bo
wel
dis
ease
, sho
rt b
owel
syn
drom
e, d
iver
ticul
itis,
obs
truc
tive
cons
tipat
ion,
pro
laps
ing
hem
orrh
oids
, gas
troi
ntes
tinal
st
rict
ure,
eat
ing
diso
rder
s, o
r m
enta
l illn
ess
with
obs
essi
ve-c
ompu
lsiv
e te
nden
cies
Nau
sea,
vom
iting
, exc
essi
ve f
latu
lenc
e, d
iarr
hea,
abd
omin
al c
ram
ping
, hig
h st
ool v
olum
e or
fre
quen
cy th
at c
ause
s di
scom
fort
to th
e in
divi
dual
, obs
truc
tion,
phy
tobe
zoar
Edi
tion:
200
6 90

INTA
KE D
OMAI
N C
arbo
hydr
ate a
nd F
iber
Inta
ke
EX
CE
SS
IVE
FIB
ER
IN
TA
KE
(N
I-53
.6)
Refe
ren
ces:
1.
DiP
alm
a JA
. Cur
rent
trea
tmen
t opt
ions
for
chr
onic
con
stip
atio
n. R
ev G
astr
oent
erol
Dis
ord
2004
;2:p
S34-
pS42
. 2.
H
iggi
ns P
D, J
ohan
son
JF. E
pide
mio
logy
of
cons
tipat
ion
in N
orth
Am
eric
a: a
sys
tem
atic
rev
iew
. Am
J G
astr
oent
erol
200
4;99
:750
-759
. 3.
L
embo
A, C
amili
eri M
. Chr
onic
con
stip
atio
n. N
ew E
ng J
Med
. 200
3;34
9:36
0-36
8.
4.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es f
or E
nerg
y, C
arbo
hydr
ate,
Fib
er, F
at, F
atty
Aci
ds, C
hole
ster
ol, P
rote
in, a
nd A
min
o A
cids
. Was
hing
ton,
DC
: N
atio
nal A
cade
my
Pres
s; 2
002.
5.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: H
ealth
impl
icat
ions
of
diet
ary
fibe
r. J
Am
Die
t Ass
oc. 2
002;
102:
993-
1000
. 6.
T
alle
y N
J. D
efin
ition
, epi
dem
iolo
gy, a
nd im
pact
of
chro
nic
cons
tipat
ion.
Rev
Gas
troe
nter
ol D
isor
d. 2
004;
2:pS
3-pS
10.
7.
van
den
Ber
g H
, van
der
Gaa
g M
, Hen
drik
s H
. Inf
luen
ce o
f lif
esty
le o
n vi
tam
in b
ioav
aila
bilit
y. I
nt J
Vita
m N
utr
Res
. 200
2;72
:53-
5.
8.
Wal
d A
. Irr
itabl
e bo
wel
syn
drom
e. C
urr
Trea
t Opt
ions
Gas
troe
nter
ol. 1
999;
2:13
-19.
Edi
tion:
200
6 91

INTA
KE D
OMAI
N V
itam
in In
take
INA
DE
QU
AT
E V
ITA
MIN
IN
TA
KE
(SP
EC
IFY
)(N
I-54
.1)
De
fin
itio
n
Low
er in
take
of
vita
min
con
tain
ing
food
s or
sub
stan
ces
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Phys
iolo
gic
caus
es, e
.g. i
ncre
ased
nut
rien
t nee
ds d
ue to
pro
long
ed c
atab
olic
illn
ess,
dis
ease
sta
te, m
alab
sorp
tion,
or
med
icat
ions
Lac
k of
acc
ess
to f
ood,
e.g
., ec
onom
ic c
onst
rain
ts, c
ultu
ral o
r re
ligio
us p
ract
ices
, res
tric
ting
food
giv
en to
eld
erly
and
/or
child
ren
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit c
once
rnin
g fo
od s
ourc
es o
f vi
tam
ins
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or e
atin
g di
sord
ers
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Edi
tion:
200
6 92

INTA
KE D
OMAI
N V
itam
in In
take
INA
DE
QU
AT
E V
ITA
MIN
IN
TA
KE
(SP
EC
IFY
)(N
I-54
.1)
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a V
itam
in A
-ser
um r
etin
ol <
0.3
5 m
mol
/L
Vita
min
C –
pla
sma
conc
entr
atio
ns <
.2 m
g/dL
Vita
min
D-
ioni
zed
calc
ium
< .9
8 m
mol
/L w
ith e
leva
ted
para
thyr
oid
horm
one,
nor
mal
ser
um c
alci
um, a
nd s
erum
ph
osph
orus
< 2
.6 m
g/dL
Vita
min
E-
plas
ma
alph
a-to
coph
erol
<18
mol
/g
Vita
min
K –
ele
vate
d pr
othr
ombi
n tim
e; a
ltere
d IN
R (
with
out a
nti-
coag
ulat
ion
ther
apy)
Thi
amin
– e
ryth
rocy
te tr
ansk
etol
ase
activ
ity >
1.2
0 m
cg/m
l/h
Rib
ofla
vin
– er
ythr
ocyt
e gl
utat
hion
e re
duct
ase
> 1
.2 I
U/m
g he
mog
lobi
n
Nia
cin
– N
’met
hyl-
nico
tinam
ide
excr
etio
n <5
.8 µ
mol
/day
Vita
min
B6
– pl
asm
a pr
yrdo
xal 5
’pho
spha
te <
20 n
ml/L
Vita
min
B12
– s
erum
con
cent
ratio
n <1
80 p
mol
/L; e
leva
ted
hom
ocys
tein
e
Folic
aci
d—se
rum
con
cent
ratio
n <7
nm
ol/L
; red
cel
l fol
ate
< 31
5 nm
ol/L
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Vita
min
A –
nig
ht b
lindn
ess,
Bito
t’s
spot
s, x
erop
thal
mia
, fol
licul
ar h
yper
kera
tosi
s
Vita
min
C –
fol
licul
ar h
yper
kera
tosi
s, p
etic
hiae
, ecc
hym
osis
, coi
led
hair
s, in
flam
ed a
nd b
leed
ing
gum
s, p
erif
olic
ular
he
mor
rhag
es, j
oint
eff
usio
ns, a
rthr
algi
a, a
nd im
pair
ed w
ound
hea
ling
Vita
min
D –
wid
enin
g at
end
s of
long
bon
es, r
achi
tic r
osar
y in
chi
ldre
n, r
icke
ts, o
steo
mal
acia
Rib
ofla
vin
– so
re th
roat
, hyp
erem
ia, e
dem
a of
pha
ryng
eal a
nd o
ral m
ucou
s m
embr
anes
, che
ilosi
s, a
ngul
ar s
tom
atiti
s,
glos
sitis
, seb
orrh
eic
derm
atiti
s, a
nd n
orm
oshr
omic
, nor
moc
ytin
ane
mia
with
pur
e er
ythr
ocyt
e cy
topl
asia
of
the
bone
m
arro
w
Nia
cin
– sy
mm
etri
cal,
pigm
ente
d ra
sh o
n ar
eas
expo
sed
to s
unlig
ht, b
righ
t red
tong
ue, p
ella
gra
Vita
min
B6
– se
borr
heic
der
mat
itis,
sto
mat
itis,
che
ilosi
s, g
loss
itis,
con
fusi
on, d
epre
ssio
n
Vita
min
B12
– ti
nglin
g an
d nu
mbn
ess
in e
xtre
miti
es, d
imin
ishe
d vi
brat
ory
and
posi
tion
sens
e, m
otor
dis
turb
ance
s in
clud
ing
gait
dist
urba
nces
Edi
tion:
200
6 93

INTA
KE D
OMAI
N V
itam
in In
take
INA
DE
QU
AT
E V
ITA
MIN
IN
TA
KE
(SP
EC
IFY
)(N
I-54
.1)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Die
tary
his
tory
ref
lect
s in
adeq
uate
inta
ke o
f fo
ods
cont
aini
ng s
peci
fic
vita
min
s as
com
pare
d to
req
uire
men
ts o
r re
com
men
ded
leve
l
Die
tary
his
tory
ref
lect
s ex
cess
ive
cons
umpt
ion
of f
oods
that
do
not c
onta
in a
vaila
ble
vita
min
s, e
.g. o
ver
proc
esse
d, o
ver
cook
ed, o
r im
prop
erly
sto
red
food
s
Clie
nt H
isto
ry
Prol
onge
d us
e of
sub
stan
ces
know
n to
incr
ease
vita
min
req
uire
men
ts o
r re
duce
vita
min
abs
orpt
ion
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
mal
abso
rptio
n as
a r
esul
t of
celia
c di
seas
e, s
hort
bow
el
synd
rom
e, o
r in
flam
mat
ory
bow
el
Cer
tain
env
iron
men
tal c
ondi
tions
, e.g
. inf
ants
exc
lusi
vely
fed
bre
ast m
ilk w
ith li
mite
d ex
posu
re to
sun
light
(V
itam
in D
)
Refe
ren
ces:
1.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r V
itam
in A
, Vita
min
K, A
rsen
ic, B
oron
, Chr
omiu
m, C
oppe
r, I
odin
e, I
ron,
Man
gane
se, M
olyb
denu
m, N
icke
l,Si
lico
n, V
anad
ium
, and
Zin
c. W
ashi
ngto
n, D
.C. N
atio
nal A
cade
my
Pres
s: 2
000.
2.
N
atio
nal A
cade
my
of S
cien
ces,
Ins
titut
e of
Med
icin
e. D
ieta
ry R
efer
ence
Int
akes
for
Thia
min
e, R
ibof
lavi
n, N
iaci
n, V
itam
in B
6, F
olat
e, V
itam
in B
12, P
anto
then
ic A
cid,
Bio
tin,
and
Cho
line
Was
hing
ton,
D.C
. Nat
iona
l Aca
dem
y Pr
ess:
200
0.
3.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r V
itam
in C
, Vita
min
E, S
elen
ium
, and
Car
oten
oids
. Was
hing
ton,
D.C
. Nat
iona
l Aca
dem
y Pr
ess:
200
0.
4.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r C
alci
um, P
hosp
horu
s, M
agne
sium
, Vita
min
D, a
nd F
luor
ide.
Was
hing
ton,
D.C
. Nat
iona
l Aca
dem
y Pr
ess:
19
97.
Edi
tion:
200
6 94

INTA
KE D
OMAI
N V
itam
in In
take
EX
CE
SS
IVE
VIT
AM
IN I
NT
AK
E(S
PE
CIF
Y)
(NI-
54.2
)
De
fin
itio
n
Hig
her
inta
ke o
f vi
tam
in c
onta
inin
g fo
ods
or s
ubst
ance
s co
mpa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
bas
ed u
pon
phys
iolo
gica
l nee
ds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Phys
iolo
gic
caus
es, e
.g. d
ecre
ased
nut
rien
t nee
ds d
ue to
pro
long
ed im
mob
ility
or
chro
nic
rena
l dis
ease
Acc
ess
to f
oods
and
sup
plem
ents
in e
xces
s of
nee
ds, e
.g.,
cultu
ral o
r re
ligio
us p
ract
ices
, ina
ppro
pria
te f
ood
and
supp
lem
ents
giv
en to
pre
gnan
t wom
en,
elde
rly
or c
hild
ren
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit c
once
rnin
g fo
od a
nd s
uppl
emen
tal s
ourc
es o
f vi
tam
ins
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or e
atin
g di
sord
ers
Acc
iden
tal o
verd
ose
from
ora
l and
sup
plem
enta
l for
ms,
ent
eral
or
pare
nter
al s
ourc
es
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a V
itam
in D
- io
nize
d ca
lciu
m >
.98
with
ele
vate
d pa
rath
yroi
d ho
rmon
e, n
orm
al s
erum
cal
cium
, and
ser
um p
hosp
horu
s >
2.6
Vita
min
K –
slo
wed
pro
thro
mbi
n tim
e or
alte
red
INR
Nia
cin
– N
’met
hyl-
nico
tinam
ide
excr
etio
n >5
.8 µ
mol
/day
Vita
min
B6
– pl
asm
a pr
yrdo
xal 5
’pho
spha
te >
20 n
oml/L
Vita
min
A –
ser
um r
etin
ol c
once
ntra
tion
> 60
µg/
dL
Ant
hrop
omet
ric
Mea
sure
men
ts
Edi
tion:
200
6 95

INTA
KE D
OMAI
N V
itam
in In
take
EX
CE
SS
IVE
VIT
AM
IN I
NT
AK
E(S
PE
CIF
Y)
(NI-
54.2
)P
hysi
cal E
xam
Fin
ding
s V
itam
in A
– c
hang
es in
the
skin
and
muc
ous
mem
bran
es; d
ry li
ps (
chei
litis
), e
arly
-dry
ness
of
the
nasa
l muc
osa
and
eyes
; la
ter-
dryn
ess,
ery
them
a, s
calin
g an
d pe
elin
g of
the
skin
, hai
r lo
ss, a
nd n
ail f
ragi
lity.
Hea
dach
e, n
ause
a, a
nd v
omiti
ng.
Infa
nts
may
hav
e bu
lgin
g fo
ntan
elle
; chi
ldre
n m
ay d
evel
op b
one
alte
ratio
ns.
Vita
min
D –
ele
vate
d se
rum
cal
cium
(hy
perc
alce
mia
) an
d ph
osph
orus
(hy
perp
hosp
hate
mia
) le
vels
; ca
lcif
icat
ion
of s
oft
tissu
es (
calc
inos
is),
incl
udin
g th
e ki
dney
, lun
gs, h
eart
, and
eve
n th
e ty
mpa
nic
mem
bran
e of
the
ear,
whi
ch c
an r
esul
t in
deaf
ness
. Hea
dach
e an
d na
usea
. Inf
ants
giv
en e
xces
sive
am
ount
s of
vita
min
D m
ay h
ave
gast
roin
test
inal
ups
et, b
one
frag
ility
, and
ret
arde
d gr
owth
.
Vita
min
K –
hem
olyt
ic a
nem
ia in
adu
lts o
r se
ver
jaun
dice
in in
fant
s ha
ve b
een
note
d on
rar
e oc
casi
ons
Nia
cin
– hi
stam
ine
rele
ase
whi
ch c
ause
s fl
ushi
ng, a
ggra
vatio
n of
ast
hma
or li
ver
dise
ase
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f
His
tory
or
mea
sure
d in
take
ref
lect
s ex
cess
ive
inta
ke o
f fo
ods
and
supp
lem
ents
con
tain
ing
vita
min
s as
com
pare
d to
es
timat
ed r
equi
rem
ents
, inc
ludi
ng f
ortif
ied
cere
als,
mea
l rep
lace
men
ts, v
itam
in-m
iner
al s
uppl
emen
ts, o
ther
die
tary
su
pple
men
ts (
e.g.
, fis
h liv
er o
ils o
r ca
psul
es),
tube
fee
ding
, and
/or
pare
nter
al s
olut
ions
Inta
ke g
reat
er th
an U
L f
or v
itam
in A
(as
ret
inol
est
er, n
ot a
s -c
arot
ene)
is 6
00 µ
g/d
for
infa
nts
and
todd
lers
; 900
µg/
d fo
r ch
ildre
n 4-
8 yr
s, 1
700
µg/
d fo
r ch
ildre
n 9-
13 y
rs, 2
800
for
child
ren
14-1
8 yr
s, a
nd 3
000
µg/
d fo
r ad
ults
Inta
ke g
reat
er th
an U
L f
or v
itam
in D
is 2
5 µ
g/da
y fo
r in
fant
s an
d 50
µg/
day
for
child
ren
and
adul
ts
Nia
cin:
hig
h do
ses
of 1
to 2
g o
f N
A th
ree
times
per
day
can
hav
e si
de e
ffec
ts o
f cl
inic
al u
ses
of h
igh
dose
s of
1 to
2 g
of
NA
thre
e tim
es p
er d
ay
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
chro
nic
liver
or
kidn
ey d
isea
ses,
hea
rt f
ailu
re, c
ance
r
Refe
ren
ces:
1.
Alle
n L
H, H
aske
ll M
. Est
imat
ing
the
pote
ntia
l for
vita
min
A to
xici
ty in
wom
en a
nd y
oung
chi
ldre
n. J
Nut
r. 2
002;
132:
pS29
07-p
S291
9.
2.
Cro
quet
V, P
ilette
C, L
espi
ne A
, Vui
llem
in E
, Rou
ssel
et M
C, O
bert
i F, S
aint
And
re J
P, P
eriq
uet B
, Fra
ncoi
s S,
Ifr
ah N
, Cal
es P
. Hep
atic
hyp
er-v
itam
inos
is A
: im
port
ance
of
retin
yl e
ster
leve
l de
term
inat
ion.
Eur
J G
astr
oent
erol
Hep
atol
. 200
0;12
:361
-364
. 3.
K
rasi
nski
SD
, Rus
sell
RM
, Otr
adov
ec C
L, S
adow
ski J
A, H
artz
SC
, Jac
ob R
A, M
cGan
dy R
B. R
elat
ions
hip
of v
itam
in A
and
vita
min
E in
take
to f
astin
g pl
asm
a re
tinol
, ret
inol
-bin
ding
pro
tein
, re
tinyl
est
ers,
car
oten
e, a
lpha
-toc
ophe
rol,
and
chol
este
rol a
mon
g el
derl
y pe
ople
and
you
ng a
dults
: inc
reas
ed p
lasm
a re
tinyl
est
ers
amon
g vi
tam
in A
-sup
plem
ent u
sers
. Am
J C
lin N
utr.
198
9;49
:112
-12
0.
4.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r V
itam
in A
, Vita
min
K, A
rsen
ic, B
oron
, Chr
omiu
m, C
oppe
r, I
odin
e, I
ron,
Man
gane
se, M
olyb
denu
m, N
icke
l,Si
lico
n, V
anad
ium
, and
Zin
c. W
ashi
ngto
n, D
.C. N
atio
nal A
cade
my
Pres
s:20
00.
5.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r Th
iam
ine,
Rib
ofla
vin,
Nia
cin,
Vita
min
B6,
Fol
ate,
Vita
min
B12
, Pan
toth
enic
Aci
d, B
ioti
n, a
nd C
holin
eW
ashi
ngto
n, D
.C. N
atio
nal A
cade
my
Pres
s:20
00.
6.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r V
itam
in C
, Vita
min
E, S
elen
ium
, and
Car
oten
oids
. Was
hing
ton,
D.C
. Nat
iona
l Aca
dem
y Pr
ess:
2000
. 7.
R
usse
ll R
M. N
ew v
iew
s on
RD
As
for
olde
r ad
ults
. J A
m D
iet A
ssoc
. 199
7;97
:515
-518
.
Edi
tion:
200
6 96

INTA
KE D
OMAI
N M
iner
al In
take
INA
DE
QU
AT
E M
INE
RA
L I
NT
AK
E (
NI-
55.1
)D
efi
nit
ion
Low
er in
take
of
min
eral
con
tain
ing
food
s or
sub
stan
ces
com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Phys
iolo
gic
caus
es, e
.g. i
ncre
ased
nut
rien
t nee
ds d
ue to
pro
long
ed c
atab
olic
illn
ess,
mal
abso
rptio
n, h
yper
excr
etio
n, n
utri
ent/d
rug
and
nutr
ient
/nut
rien
t in
tera
ctio
n, g
row
th a
nd m
atur
atio
n
Lac
k of
acc
ess
to f
ood,
e.g
. eco
nom
ic c
onst
rain
ts, c
ultu
ral o
r re
ligio
us p
ract
ices
, res
tric
ting
food
giv
en to
eld
erly
and
/or
child
ren
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit c
once
rnin
g fo
od s
ourc
es o
f m
iner
als;
mis
-dia
gnos
is o
f la
ctos
e in
tole
ranc
e/la
ctas
e de
fici
ency
; per
cept
ion
of
conf
lictin
g nu
triti
on m
essa
ges
from
hea
lth p
rofe
ssio
nals
, ina
ppro
pria
te r
elia
nce
on s
uppl
emen
ts
Psyc
holo
gica
l cau
ses,
e.g
. dep
ress
ion
or e
atin
g di
sord
ers
Env
iron
men
tal c
ause
s, e
.g. i
nade
quat
ely
test
ed n
utri
ent b
ioav
aila
bilit
y of
for
tifie
d fo
ods,
bev
erag
es a
nd s
uppl
emen
ts, i
napp
ropr
iate
mar
ketin
g of
for
tifie
d fo
ods/
beve
rage
s/su
pple
men
ts a
s a
subs
titut
e fo
r na
tura
l foo
d so
urce
of
nutr
ient
(s)
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a C
alci
um –
bon
e m
iner
al c
onte
nt (
BM
C)
belo
w th
e yo
ung
adul
t mea
n. H
ypoc
alci
uria
, ser
um 2
5(O
H)D
< 3
2 ng
/mL
Phos
phor
us <
2.6
mg/
dL
Mag
nesi
um <
1.8
mg/
dL
Iron
– h
emog
lobi
n <1
30g/
L (
mal
es; <
120g
/L (
fem
ales
), e
tc.
Iodi
ne –
uri
nary
exc
retio
n <1
00µ
g/L
Cop
per
– se
rum
cop
per
<10µ
mol
/L, e
tc
Ant
hrop
omet
ric
Mea
sure
men
ts
Hei
ght l
oss
Phy
sica
l Exa
m F
indi
ngs
Cal
cium
– d
imin
ishe
d B
MD
, hyp
erte
nsio
n, P
CO
S, P
MS,
kid
ney
ston
es, c
olon
pol
yps,
obe
sity
Edi
tion:
200
6 97

INTA
KE D
OMAI
N M
iner
al In
take
INA
DE
QU
AT
E M
INE
RA
L I
NT
AK
E (
NI-
55.1
)F
ood/
Nut
ritio
n H
isto
ry
Obs
erva
tions
/rep
orts
of
insu
ffic
ient
min
eral
inta
ke f
rom
die
t com
pare
d to
rec
omm
ende
d in
take
Food
avo
idan
ce a
nd/o
r el
imin
atio
n of
who
le f
ood
grou
p(s)
fro
m d
iet
Lac
k of
inte
rest
in f
ood
Inap
prop
riat
e fo
od c
hoic
es a
nd/o
r ch
roni
c di
etin
g be
havi
or
Exc
essi
ve N
a in
take
, ina
dequ
ate
Vita
min
D in
take
/exp
osur
e
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
mal
abso
rptio
n as
a r
esul
t of
celia
c di
seas
e, s
hort
bow
el
synd
rom
e, o
r in
flam
mat
ory
bow
el d
isea
se
Oth
er s
igni
fica
nt m
edic
al d
iagn
oses
and
ther
apie
s
Est
roge
n st
atus
Geo
grap
hic
latit
ude
and
hist
ory
of U
VB
exp
osur
e/us
e of
sun
scre
en
Cha
nge
in li
ving
env
iron
men
t/ind
epen
denc
e
Use
of
popu
lar
pres
s/in
tern
et a
s so
urce
of
med
ical
and
/or
nutr
ition
info
rmat
ion
Refe
ren
ces:
1.
App
el L
J, M
oore
TJ,
Oba
rzan
ek E
, Vol
lmer
WM
, Sve
tkey
LP,
Sac
ks F
M, B
ray
GA
, Vog
t TM
, Cut
ler
JA, W
indh
ause
r M
M, L
in P
-H, K
aran
ja N
. A
clin
ical
tria
l of
the
effe
cts
of d
ieta
ry p
atte
rns
on
bloo
d pr
essu
re.
N E
ng J
Med
. 199
7;33
6:11
17-1
124.
2.
H
eane
y R
P. R
ole
of d
ieta
ry s
odiu
m in
ost
eopo
rosi
s. A
m J
Clin
Nut
r (i
n pr
ess)
200
5.
3.
Hea
ney,
RP.
Nut
rien
ts, i
nter
actio
ns, a
nd f
oods
. The
Im
port
ance
of
Sour
ce, I
n B
urck
hard
t P, D
awso
n-H
ughe
s B
, Hea
ney
RP,
Eds
. Nut
riti
onal
Asp
ects
of O
steo
poro
sis
2nd E
d. S
an D
iego
, CA
: E
lsev
ier,
200
4:61
-76.
4.
H
eane
y, R
P. N
utri
ents
, int
erac
tions
, and
foo
ds. S
erum
25-
hydr
oxy-
vita
min
D a
nd th
e he
alth
of
the
calc
ium
eco
nom
y, I
n B
urck
hard
t P, D
awso
n-H
ughe
s B
, Hea
ney
RP,
Eds
. Nut
ritio
nal A
spec
ts o
f O
steo
poro
sis
2nd E
d. S
an D
iego
, CA
: Els
evie
r, 2
004:
227-
244.
5.
H
eane
y R
P, R
affe
rty
K, B
ierm
an J
. Not
all
calc
ium
-for
tifi
ed b
ever
ages
are
equ
al. N
utr
Toda
y (i
n pr
ess)
. 200
4.
6.
Hea
ney
RP,
Dow
ell M
S, H
ale
CA
, Ben
dich
A. C
alci
um a
bsor
ptio
n va
ries
with
in th
e re
fere
nce
rang
e fo
r se
rum
25-
hydr
oxyv
itam
in D
.J A
m C
oll N
utr.
200
3;22
:142
-146
. 7.
H
eane
y R
P, D
owel
l MS,
Raf
fert
y K
, Bie
rman
J. B
ioav
aila
bilit
y of
the
calc
ium
in f
ortif
ied
soy
imita
tion
mil
k, w
ith s
ome
obse
rvat
ions
on
met
hod.
Am
J C
lin N
utr.
200
0;71
:116
6-11
69.
8.
H
olic
k M
F. F
unct
ions
of
vita
min
D: i
mpo
rtan
ce f
or p
reve
ntio
n of
com
mon
can
cers
, Typ
e I
diab
etes
and
hea
rt D
isea
se. p
p. 1
81-2
01. I
n: N
utri
tiona
l Asp
ects
of O
steo
poro
sis,
2nd
Edi
tion.
Bur
ckha
rdt
P, D
awso
n-H
ughe
s B
, Hea
ney
RP,
eds
. Els
evie
r In
c., S
an D
iego
, CA
, 200
4 9.
M
asse
y L
K, W
hitin
g SJ
. Die
tary
sal
t, ur
inar
y ca
lciu
m, a
nd b
one
loss
. J B
one
Min
er R
es. 1
1:73
1-73
6, 1
996.
10
. Su
araz
FL
, Sav
aian
o D
, Arb
isi P
, Lev
itt M
D. T
oler
ance
to th
e da
ily in
gest
ion
of tw
o cu
ps o
f m
ilk b
y in
divi
dual
s cl
aim
ing
lact
ose
into
lera
nce.
Am
J C
lin N
utr.
199
7;65
:150
2-15
06.
11.
Thy
s- J
acob
s S,
Don
ovan
D, P
apad
opou
los
A, S
arre
l P. B
ilezi
kian
JP.
Vita
min
D a
nd c
alci
um d
ysre
gula
tion
in th
e po
lycy
stic
ova
rian
syn
drom
e. S
tero
ids.
64:
430-
435,
199
9.
12.
Thy
s-Ja
cobs
S, S
tark
ey P
, Ber
nste
in D
, Tia
n J.
Cal
cium
car
bona
te a
nd th
e pr
emen
stru
al s
yndr
ome:
Eff
ects
on
prem
enst
rual
and
men
stru
al s
ympt
omat
olog
y. A
m J
Obs
tet G
ynec
ol. 1
998;
179:
444-
452.
13
. Z
emel
MB
, Tho
mps
on W
, Mils
tead
A, M
orri
s K
, Cam
pbel
l P. C
alci
um a
nd d
airy
acc
eler
atio
n of
wei
ght a
nd f
at lo
ss d
urin
g en
ergy
res
tric
tion
in o
bese
adu
lts. O
besi
ty R
es. 1
2:58
2-59
0, 2
004.
Edi
tion:
200
6 98

INTA
KE D
OMAI
N M
iner
al In
take
EX
CE
SS
IVE
MIN
ER
AL
IN
TA
KE
(N
I-55
.2)
De
fin
itio
n
Hig
her
inta
ke o
f m
iner
al f
rom
foo
ds, s
uppl
emen
ts, m
edic
atio
ns o
r w
ater
, com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns b
ased
upo
n ph
ysio
logi
cal n
eeds
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Har
mfu
l bel
iefs
/atti
tude
s ab
out f
ood,
nut
ritio
n, a
nd n
utri
tion-
rela
ted
topi
cs
Food
fad
dism
Acc
iden
tal o
ver-
supp
lem
enta
tion
Ove
rcon
sum
ptio
n of
a li
mite
d va
riet
y of
foo
ds
Lac
k of
kno
wle
dge
abou
t man
agem
ent o
f di
agno
sed
gene
tic d
isor
der
alte
ring
min
eral
hom
eost
asis
[he
moc
hrom
otos
is (
iron
), W
ilson
’s D
isea
se (
copp
er)]
Lac
k of
kno
wle
dge
abou
t man
agem
ent o
f di
agno
sed
dise
ase
stat
e re
quir
ing
min
eral
res
tric
tion
[cho
lest
atic
live
r di
seas
e (c
oppe
r an
d m
anga
nese
), r
enal
in
suff
icie
ncy
(pho
spho
rus,
mag
nesi
um, p
otas
sium
)]
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a C
hang
es in
app
ropr
iate
labo
rato
ry v
alue
s, s
uch
as:
TSH
(io
dine
sup
plem
enta
tion)
HD
L (
zinc
sup
plem
enta
tion)
ser
um f
erri
tin a
nd tr
ansf
erri
n sa
tura
tion
(iro
n ov
erlo
ad)
Hyp
erph
osph
atem
ia
Hyp
erm
agne
sem
ia
Edi
tion:
200
6
99

INTA
KE D
OMAI
N M
iner
al In
take
EX
CE
SS
IVE
MIN
ER
AL
IN
TA
KE
(N
I-55
.2)
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Hai
r an
d na
il ch
ange
s (s
elen
ium
)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Hig
h in
take
of
food
s or
sup
plem
ents
con
tain
ing
min
eral
com
pare
d to
DR
Is
Dec
reas
ed a
ppet
ite (
zinc
sup
plem
enta
tion)
Clie
nt H
isto
ry
GI
dist
urba
nces
(ir
on, m
agne
sium
, cop
per,
zin
c, s
elen
ium
)
Cop
per
defi
cien
cy a
nem
ia (
zinc
)
Liv
er d
amag
e (c
oppe
r, ir
on),
ena
mel
or
skel
etal
flu
oros
is (
fluo
ride
)
Refe
ren
ces:
1.
Bow
man
BA
, Rus
sell
RM
, eds
. Pre
sent
Kno
wle
dge
in N
utri
tion.
8th E
d. W
ashi
ngto
n, D
C: I
LSI
Pre
ss; 2
001.
2.
N
atio
nal A
cade
my
of S
cien
ces,
Ins
titut
e of
Med
icin
e. D
ieta
ry R
efer
ence
Int
akes
for
Vita
min
A, V
itam
in K
, Ars
enic
, Bor
on, C
hrom
ium
, Cop
per,
Iod
ine,
Iro
n, M
anga
nese
, Mol
ybde
num
, Nic
kel,
Silic
on, V
anad
ium
, Zin
c. W
ashi
ngto
n, D
C: N
atio
nal A
cade
my
Pres
s; 2
001.
3.
Nat
iona
l Aca
dem
y of
Sci
ence
s, I
nstit
ute
of M
edic
ine.
Die
tary
Ref
eren
ce I
ntak
es fo
r C
alci
um, P
hosp
horu
s, M
agne
sium
, Vita
min
D, a
nd F
luor
ide.
Was
hing
ton,
DC
: Nat
iona
l Aca
dem
y Pr
ess;
199
7.
4.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Foo
d an
d nu
triti
on m
isin
form
atio
n. J
Am
Die
t Ass
oc. 2
002;
102:
260-
266.
Edi
tion:
200
6
100

CLIN
CAL
DOMA
IN
Func
tiona
l
SW
AL
LO
WIN
G D
IFF
ICU
LT
Y (
NC
-1.1
)
De
fin
itio
n
Impa
ired
mov
emen
t of
food
and
liqu
id f
rom
the
mou
th to
the
stom
ach
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Mec
hani
cal c
ause
s, e
.g.,
infl
amm
atio
n, s
urge
ry, s
tric
ture
, or
oral
, pha
ryng
eal a
nd e
soph
agea
l tum
ors
Mot
or c
ause
s, e
.g.,
neur
olog
ical
or
mus
cula
r di
sord
ers,
suc
h as
, cer
ebra
l pal
sy, s
trok
e, m
ultip
le s
cler
osis
, scl
erod
erm
a, p
rem
atur
ity
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Evi
denc
e of
deh
ydra
tion,
e.g
., dr
y m
ucou
s m
embr
anes
, poo
r sk
in tu
rgor
Foo
d/N
utri
tion
His
tory
O
bser
vatio
ns o
r re
port
s of
: C
ough
ing,
cho
king
, pro
long
ed c
hew
ing,
pou
chin
g of
foo
d, r
egur
gita
tion,
fac
ial e
xpre
ssio
n ch
ange
s du
ring
eat
ing,
pro
long
ed
feed
ing
time,
dro
olin
g, n
oisy
wet
upp
er a
irw
ay s
ound
s, f
eelin
g of
“fo
od g
ettin
g st
uck,
” pa
in w
hile
sw
allo
win
g D
ecre
ased
foo
d in
take
A
void
ance
of
food
s M
ealti
me
resi
stan
ce
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f dy
spha
gia,
ach
alas
ia
Rad
iolo
gica
l fin
ding
s, e
.g.,
abno
rmal
sw
allo
win
g st
udie
s
Rep
eate
d up
per
resp
irat
ory
infe
ctio
ns a
nd o
r pn
eum
onia
Refe
ren
ces:
1.
Bra
unw
ald
E, F
auci
AS,
Kas
per
DL
, Hau
ser
SL, L
ongo
DL
, Jam
eson
JL
, ed.
Har
riso
n’s
Pri
ncip
les
of I
nter
nal M
edic
ine.
15th
Edi
tion.
New
Yor
k, N
Y: M
cGra
w-H
ill,.2
001.
Edi
tion:
200
6
101

CLIN
CAL
DOMA
IN
Func
tiona
l
CH
EW
ING
(M
AS
TIC
AT
OR
Y)
DIF
FIC
UL
TY
(N
C-1
.2)
De
fin
itio
n
Impa
ired
abi
lity
to b
ite o
r ch
ew f
ood
in p
repa
ratio
n fo
r sw
allo
win
g
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Cra
niof
acia
l mal
form
atio
ns
Ora
l sur
gery
Neu
rom
uscu
lar
dysf
unct
ion
Part
ial o
r co
mpl
ete
eden
tulis
m
Soft
tiss
ue d
isea
se (
prim
ary
or o
ral m
anif
esta
tions
of
a sy
stem
ic d
isea
se)
Xer
osto
mia
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Mis
sing
teet
h
Alte
ratio
ns in
cra
nial
ner
ves
V, V
II, I
X, X
, XII
Dry
or
crac
ked
lips,
tong
ue
Ora
l les
ions
Impa
ired
tong
ue m
ovem
ent
Ill-
fitti
ng d
entu
res
or b
roke
n de
ntur
es
Edi
tion:
200
6
102

CLIN
CAL
DOMA
IN
Func
tiona
l
CH
EW
ING
(M
AS
TIC
AT
OR
Y)
DIF
FIC
UL
TY
(N
C-1
.2)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Dec
reas
ed in
take
of
food
A
ltera
tions
in f
ood
inta
ke f
rom
usu
al
Dec
reas
ed in
take
or
avoi
danc
e of
foo
d di
ffic
ult t
o fo
rm in
to a
bol
us, e
.g.,
nuts
, w
hole
pie
ces
of m
eat,
poul
try,
fis
h, f
ruits
, ve
geta
bles
A
void
ance
of
food
s of
age
-app
ropr
iate
text
ure
Spitt
ing
food
out
or
prol
onge
d fe
edin
g tim
e
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
alco
holis
m, A
lzhe
imer
’s, h
ead,
nec
k or
pha
ryng
eal c
ance
r,
cere
bral
pal
sy, c
left
lip/
pala
te, o
ral s
oft t
issu
e in
fect
ions
(e.
g., c
andi
dias
is, l
euko
plak
ia),
lack
of
deve
lopm
enta
l rea
dine
ss,
oral
man
ifes
tatio
ns o
f sy
stem
ic d
isea
se (
e.g.
, rhe
umat
oid
arth
ritis
, lup
us, C
rohn
’s d
isea
se, p
enph
igus
vul
gari
s, H
IV,
diab
etes
)R
ecen
t maj
or o
ral s
urge
ry
Wir
ed ja
w
Che
mot
hera
py w
ith o
ral s
ide
effe
cts
Rad
iatio
n th
erap
y to
ora
l cav
ity
Refe
ren
ces:
1.
Bai
ley
R, L
edik
we
JH, S
mic
ikla
s-W
righ
t H, M
itch
ell D
C, J
ense
n G
L. P
ersi
sten
t ora
l hea
lth p
robl
ems
asso
ciat
ed w
ith c
omor
bidi
ty a
nd im
pair
ed d
iet q
ualit
y in
old
er a
dults
. J A
m D
iet A
ssoc
.20
04;1
04:1
273-
1276
. 2.
C
hern
off
R, e
d. O
ral h
ealth
in th
e el
derl
y. G
eria
tric
Nut
ritio
n. G
aith
ersb
urg,
MD
: Asp
en P
ublis
hers
, 199
9.
3.
Dor
men
val V
, Moj
on P
, Bud
tz-J
orge
nsen
E. A
ssoc
iatio
n be
twee
n se
lf-a
sses
sed
mas
ticat
ory
abili
ty, n
utri
tiona
l sta
tus
and
saliv
ary
flow
rat
e in
hos
pita
lized
eld
erly
. Ora
l Dis
ease
s. 1
999;
5:32
-38.
4.
H
ildeb
rand
GH
, Dom
ingu
ez B
L, S
chor
k M
A, L
oesc
he W
J. F
unct
iona
l uni
ts, c
hew
ing,
sw
allo
win
g an
d fo
od a
void
ance
am
ong
the
elde
rly.
J P
rost
het D
ent.
1997
;77:
585-
595.
5.
H
iran
o H
, Ish
iyam
a N
, Wat
anab
e I,
Nas
u I.
Mas
ticat
ory
abili
ty in
rel
atio
n to
ora
l sta
tus
and
gene
ral h
ealth
in a
ging
. J N
utr
Hea
lth A
ging
. 199
9;3:
48-5
2.
6.
Huh
man
n M
, Tou
ger-
Dec
ker
R, B
yham
-Gra
y L
, O’S
ulli
van-
Mai
llet J
, Von
Hag
en S
. Com
pari
son
of d
ysph
agia
scr
eeni
ng b
y a
regi
ster
ed d
ietit
ian
in a
cute
str
oke
patie
nts
to s
peec
h la
ngua
ge
path
olog
ist’
s ev
alua
tion.
Top
Cli
n N
utr.
200
4;19
:239
-249
. 7.
K
adem
ani D
, Glic
k M
. Ora
l ulc
erat
ions
in in
divi
dual
s in
fect
ed w
ith h
uman
imm
unod
efic
ienc
y vi
rus:
clin
ical
pre
sent
atio
ns, d
iagn
osis
, man
agem
ent a
nd r
elev
ance
to d
isea
se p
rogr
essi
on.
Qui
ntes
senc
e In
tern
atio
nal.
1998
;29:
1103
-110
8.
8.
Kel
ler
HH
, Ost
bye
T, B
righ
t-Se
e E
. Pre
dict
ors
of d
ieta
ry in
take
in O
ntar
io s
enio
rs. C
an J
Pub
lic
Hea
lth.
199
7;88
:303
-309
. 9.
K
rall
E, H
ayes
C, G
arci
a R
. How
den
titio
n st
atus
and
mas
ticat
ory
func
tion
affe
ct n
utri
ent i
ntak
e. J
Am
Den
t Ass
oc. 1
998;
129:
1261
-126
9.
10.
Josh
ipur
a K
, Will
ett W
C, D
ougl
ass
CW
. The
impa
ct o
f ed
entu
lous
ness
on
food
and
nut
rien
t int
ake.
J A
m D
ent A
ssoc
. 199
6;12
7:45
9-46
7.
11.
Mac
kle
T, T
ouge
r-D
ecke
r R
, O’S
ulliv
an M
aille
t J, H
olla
nd, B
. R
egis
tere
d D
ietit
ians
’ us
e of
phy
sica
l ass
essm
ent p
aram
eter
s in
pra
ctic
e. J
Am
Die
t Ass
oc. 2
004;
103:
1632
-163
8.
12.
Mob
ley
C, S
aund
ers
M. O
ral h
ealth
scr
eeni
ng g
uide
lines
for
non
dent
al h
ealth
care
pro
vide
rs. J
Am
er D
iet A
ssoc
. 199
7;97
:pS1
23-1
26.
13.
Mor
se, D
. Ora
l and
pha
ryng
eal c
ance
r. I
n: R
Tou
ger-
Dec
ker
et a
l eds
. Nut
riti
on a
nd O
ral M
edic
ine.
Tot
owa
NJ:
Hum
ana
Pres
s, I
nc 2
005,
pag
es 2
05.2
22.
14.
Moy
niha
n P,
But
ler
T, T
hom
ason
J, J
epso
n N
. Nut
rien
t int
ake
in p
artia
lly d
enta
te p
atie
nts:
the
effe
ct o
f pr
osth
etic
reh
abili
tatio
n.J
Den
t. 20
00;2
8:55
7-56
3.
15.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Ora
l hea
lth a
nd n
utri
tion.
J A
m D
iet A
ssoc
. 200
3;10
3:61
5-62
5.
16.
Sayh
oun
NR
Lin
CL
, Kra
ll E
. Nut
riti
onal
sta
tus
of th
e ol
der
adul
t is
asso
ciat
ed w
ith d
entit
ion
stat
us. J
Am
Die
t Ass
oc. 2
003;
103:
61-6
6.
18.
Shei
ham
A, S
teel
e JG
. The
impa
ct o
f or
al h
ealth
on
stat
ed a
bilit
y to
eat
cer
tain
foo
ds; f
indi
ng f
rom
the
natio
nal d
iet a
nd n
utri
tion
surv
ey o
f ol
der
peop
le in
Gre
at B
rita
in. G
erod
onto
logy
.19
99;1
6:11
-20.
19
. Sh
ip J
, Duf
fy V
, Jon
es J
, Lan
gmor
e S.
Ger
iatr
ic o
ral h
ealth
and
its
impa
ct o
n ea
ting.
J A
m G
eria
tr S
oc. 1
996;
44:4
56-4
64.
Edi
tion:
200
6
103
CLIN
CAL
DOMA
IN
Func
tiona
l
CH
EW
ING
(M
AS
TIC
AT
OR
Y)
DIF
FIC
UL
TY
(N
C-1
.2)
20.
Tou
ger-
Dec
ker
R. C
linic
al a
nd la
bora
tory
ass
essm
ent o
f nu
triti
on s
tatu
s. D
ent C
lin N
orth
Am
eric
a. 2
003;
47:2
59-2
78.
21.
Tou
ger-
Dec
ker
R, S
iroi
s D
, Mob
ley
C (
eds)
. Nut
riti
on a
nd O
ral M
edic
ine.
Hum
ana
Pres
s, S
epte
mbe
r 20
04.
22.
Wal
ls A
W, S
teel
e JG
, She
iham
A, M
arce
nes
W, M
oyni
han
PJ. O
ral h
ealth
and
nut
ritio
n in
old
er p
eopl
e. J
Pub
lic H
ealth
Den
t. 20
00;6
0:30
4-30
7.
Edi
tion:
200
6
104

CLIN
CAL
DOMA
IN
Func
tiona
l
BR
EA
ST
FE
ED
ING
DIF
FIC
UL
TY
(N
C-1
.3)
De
fin
itio
n
Inab
ility
to s
usta
in in
fant
nut
ritio
n th
roug
h br
east
feed
ing
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Infa
nt: D
iffi
culty
latc
hing
on,
e.g
., tig
ht f
renu
lum
Poor
suc
king
abi
lity
Ora
l pai
n
Mal
nutr
ition
/mal
abso
rptio
n
Let
harg
y, s
leep
ines
s
Irri
tabi
lity
Swal
low
ing
diff
icul
ty
Moth
er: Pa
infu
l bre
asts
, nip
ples
Bre
ast o
r ni
pple
abn
orm
ality
Mas
titis
Perc
eptio
n of
inad
equa
te m
ilk s
uppl
y
Lac
k of
soc
ial,
cultu
ral,
or e
nvir
onm
enta
l sup
port
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a L
abor
ator
y ev
iden
ce o
f de
hydr
atio
n in
infa
nt
Ant
hrop
omet
ric
Mea
sure
men
ts
Any
wei
ght l
oss
or p
oor
wei
ght g
ain
in in
fant
Phy
sica
l Exa
m F
indi
ngs
Fren
ulum
abn
orm
ality
(in
fant
)
Edi
tion:
200
6
105

CLIN
CAL
DOMA
IN
Func
tiona
l
BR
EA
ST
FE
ED
ING
DIF
FIC
UL
TY
(N
C-1
.3)
Foo
d/N
utri
tion
His
tory
O
bser
vatio
ns o
r re
port
s of
(in
fant
):
Cou
ghin
g
Cry
ing,
latc
hing
on
and
off,
pou
ndin
g on
bre
asts
Dec
reas
ed f
eedi
ng f
requ
ency
/dur
atio
n, e
arly
ces
satio
n of
fee
ding
, and
/or
feed
ing
resi
stan
ce
Infa
nt le
thar
gy
Hun
ger,
lack
of
satie
ty a
fter
fee
ding
Few
er th
an s
ix w
et d
iape
rs in
24
hour
s
Infa
nt v
omiti
ng o
r di
arrh
ea
Obs
erva
tions
or
repo
rts
of (
mot
her)
:
Smal
l am
ount
of
milk
whe
n pu
mpi
ng
Lac
k of
con
fide
nce
in a
bilit
y to
bre
astf
eed
Doe
sn’t
hea
r in
fant
sw
allo
win
g
Con
cern
s re
gard
ing
mot
her’
s ch
oice
to b
reas
tfee
d/la
ck o
f su
ppor
t
Insu
ffic
ient
kno
wle
dge
of b
reas
tfee
ding
or
infa
nt h
unge
r/sa
tiety
sig
nals
Lac
k of
fac
ilitie
s or
acc
omm
odat
ions
at p
lace
of
empl
oym
ent o
r in
com
mun
ity f
or b
reas
tfee
ding
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f (i
nfan
t), e
.g.,
clef
t lip
/pal
ate,
thru
sh, p
rem
atur
e bi
rth,
mal
abso
rptio
n, in
fect
ion
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f (m
othe
r), e
.g.,
mas
titis
, can
didi
asis
, eng
orge
men
t, hi
stor
y of
bre
ast s
urge
ry
Refe
ren
ces:
1.
Bar
ron
SP, L
ane
HW
, Han
nan
TE
, Str
uem
pler
B, W
illia
ms
JC. F
acto
rs in
flue
ncin
g du
ratio
n of
bre
ast f
eedi
ng a
mon
g lo
w-i
ncom
e w
omen
. J A
m D
iet A
ssoc
. 198
8;88
:155
7-15
61.
2.
Bry
ant C
, Cor
eil J
, D’A
ngel
o SL
, Bai
ley
DFC
, Laz
arov
MA
. A s
trat
egy
for
prom
otin
g br
east
feed
ing
amon
g ec
onom
ical
ly d
isad
vant
aged
wom
en a
nd a
dole
scen
ts. N
AA
CO
G’s
Cli
n Is
su P
erin
atW
omen
’s H
ealth
Nur
s. 1
992;
3:72
3-73
0.
3.
Ben
tley
ME
, Cau
lfie
ld L
E, G
ross
SM
, Bro
nner
Y, J
ense
n J,
Kes
sler
LA
, Pai
ge D
M. S
ourc
es o
f in
flue
nce
on in
tent
ion
to b
reas
tfee
d am
ong
Afr
ican
-Am
eric
an w
omen
at e
ntry
to W
IC. J
Hum
Lac
t.19
99;1
5:27
-34.
4.
M
orel
and
JC, L
loyd
L, B
raun
SB
, Hei
ns J
N. A
new
teac
hing
mod
el to
pro
long
bre
astf
eedi
ng a
mon
g L
atin
os. J
Hum
Lac
t. 20
00;1
6:33
7-34
1.
5.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Bre
akin
g th
e ba
rrie
rs to
bre
astf
eedi
ng. J
Am
Die
t Ass
oc. 2
001;
101:
1213
-122
0.
6.
Woo
ldri
ge M
S, F
isch
er C
. Col
ic, "
over
feed
ing"
and
sym
ptom
s of
lact
ose
mal
abso
rptio
n in
the
brea
st-f
ed b
aby.
Lan
cet.
1988
;2:3
82-3
84.
Edi
tion:
200
6
106

CLIN
CAL
DOMA
IN
Func
tiona
l
AL
TE
RE
D G
AS
TR
OIN
TE
ST
INA
L (
GI)
FU
NC
TIO
N (
NC
-1.4
)
De
fin
itio
n
Cha
nges
in a
bilit
y to
dig
est o
r ab
sorb
nut
rien
ts
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Alte
ratio
ns in
GI
anat
omic
al s
truc
ture
, e.g
., ga
stri
c by
pass
, Rou
x E
n Y
Cha
nges
in th
e G
I tr
act m
otili
ty, e
.g.,
gast
ropa
resi
s
Com
prom
ised
GI
trac
t fun
ctio
n, e
.g.,
Cel
iac
dise
ase,
Cro
hn’s
dis
ease
, inf
ectio
n, r
adia
tion
ther
apy
Com
prom
ised
fun
ctio
n of
rel
ated
GI
orga
ns, e
.g. p
ancr
eas,
live
r
Dec
reas
ed f
unct
iona
l len
gth
of th
e G
I tr
act,
e.g.
, sho
rt b
owel
syn
drom
e
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a A
bnor
mal
dig
estiv
e en
zym
e an
d fe
cal f
at s
tudi
es
Abn
orm
al h
ydro
gen
brea
th te
st, d
-xyl
ose
test
, sto
ol c
ultu
re, a
nd g
astr
ic e
mpt
ying
and
/or
smal
l bow
el tr
ansi
t tim
e
Ant
hrop
omet
ric
Mea
sure
men
ts
Was
ting
due
to m
alnu
triti
on in
sev
ere
case
s
Phy
sica
l Exa
m F
indi
ngs
Dec
reas
ed m
uscl
e m
ass
Abd
omin
al d
iste
nsio
n
Incr
ease
d (o
r so
met
imes
dec
reas
ed)
bow
el s
ound
s
Edi
tion:
200
6
107

CLIN
CAL
DOMA
IN
Func
tiona
l
AL
TE
RE
D G
AS
TR
OIN
TE
ST
INA
L (
GI)
FU
NC
TIO
N (
NC
-1.4
)F
ood/
Nut
ritio
n H
isto
ry
Obs
erva
tions
or
repo
rts
of:
Avo
idan
ce o
r lim
itatio
n of
tota
l int
ake
or in
take
of
spec
ific
foo
ds/f
ood
grou
ps d
ue to
GI
sym
ptom
s, e
.g.,
bloa
ting,
cra
mpi
ng,
pain
, dia
rrhe
a, s
teat
orrh
ea (
grea
sy, f
loat
ing,
fou
l-sm
ellin
g st
ools
) es
peci
ally
fol
low
ing
inge
stio
n of
foo
d
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit,
e.g.
, lac
k of
info
rmat
ion,
inco
rrec
t inf
orm
atio
n or
non
-com
plia
nce
with
m
odif
ied
diet
or
med
icat
ion
sche
dule
Clie
nt H
isto
ry
Ano
rexi
a, n
ause
a, v
omiti
ng, d
iarr
hea,
ste
ator
rhea
, con
stip
atio
n, a
bdom
inal
pai
n
End
osco
pic
or c
olon
osco
pic
exam
inat
ion
resu
lts, b
iops
y re
sults
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
mal
abso
rptio
n, m
aldi
gest
ion,
ste
ator
rhea
, con
stip
atio
n,
dive
rtic
uliti
s, C
rohn
’s d
isea
se, i
nfla
mm
ator
y bo
wel
dis
ease
, cys
tic f
ibro
sis,
cel
iac
dise
ase,
irri
tabl
e bo
wel
syn
drom
e,
infe
ctio
n
Surg
ical
pro
cedu
res,
e.g
., es
opha
gect
omy,
dila
tatio
n, g
astr
ecto
my,
vag
otom
y, g
astr
ic b
ypas
s, b
owel
res
ectio
ns
Refe
ren
ces:
1.
Bra
unw
ald
E, F
auci
AS,
Kas
per
DL
, Hau
ser
SL, L
ongo
DL
, Jam
eson
JL
, ed.
Har
riso
n’s
Pri
ncip
les
of I
nter
nal M
edic
ine.
15th
Edi
tion.
New
Yor
k, N
Y: M
cGra
w-H
ill,.2
001.
Edi
tion:
200
6
108

CLIN
CAL
DOMA
IN
Bioc
hem
ical
IMP
AIR
ED
NU
TR
IEN
T U
TIL
IZA
TIO
N (
NC
-2.1
)
De
fin
itio
n
Cha
nges
in a
bilit
y to
abs
orb
or m
etab
oliz
e nu
trie
nts
and
bioa
ctiv
e su
bsta
nces
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Alte
ratio
ns in
gas
troi
ntes
tinal
ana
tom
ical
str
uctu
re
Com
prom
ised
fun
ctio
n of
the
GI
trac
t
Com
prom
ised
fun
ctio
n of
rel
ated
GI
orga
ns, e
.g. p
ancr
eas,
live
r
Dec
reas
ed f
unct
iona
l len
gth
of th
e G
I tr
act
Met
abol
ic d
isor
ders
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a A
bnor
mal
dig
estiv
e en
zym
e an
d fe
cal f
at s
tudi
es
Abn
orm
al h
ydro
gen
brea
th te
st, d
-xyl
ose
test
Abn
orm
al te
sts
for
inbo
rn e
rror
s of
met
abol
ism
Ant
hrop
omet
ric
Mea
sure
men
ts
Wei
ght l
oss
of 5
% in
one
mon
th, 1
0% in
six
mon
ths
Gro
wth
stu
ntin
g or
fai
lure
Phy
sica
l Exa
m F
indi
ngs
Abd
omin
al d
iste
nsio
n
Incr
ease
d or
dec
reas
ed b
owel
sou
nds
Evi
denc
e of
vita
min
, min
eral
def
icie
ncy,
e.g
., gl
ossi
tis, c
heilo
sis,
mou
th le
sion
s
Edi
tion:
200
6 10
9

CLIN
CAL
DOMA
IN
Bioc
hem
ical
IMP
AIR
ED
NU
TR
IEN
T U
TIL
IZA
TIO
N (
NC
-2.1
)F
ood/
Nut
ritio
n H
isto
ry
Obs
erva
tions
or
repo
rts
of:
Avo
idan
ce o
r lim
itatio
n of
tota
l int
ake
or in
take
of
spec
ific
foo
ds/f
ood
grou
ps d
ue to
GI
sym
ptom
s, e
.g.,
bloa
ting,
cra
mpi
ng,
pain
, dia
rrhe
a, s
teat
orrh
ea (
grea
sy, f
loat
ing,
fou
l-sm
ellin
g st
ools
) es
peci
ally
fol
low
ing
inge
stio
n of
foo
d
Clie
nt H
isto
ry
Dia
rrhe
a, s
teat
orrh
ea, a
bdom
inal
pai
n
End
osco
pic
or c
olon
osco
pic
exam
inat
ion
resu
lts, b
iops
y re
sults
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
mal
abso
rptio
n, m
aldi
gest
ion,
cys
tic f
ibro
sis,
cel
iac
dise
ase,
C
rohn
’s d
isea
se, i
nfec
tion,
rad
iatio
n th
erap
y, in
born
err
ors
of m
etab
olis
m
Surg
ical
pro
cedu
res,
e.g
., ga
stri
c by
pass
, bow
el r
esec
tion
Refe
ren
ces:
1.
Bey
er P
. Gas
troi
ntes
tinal
dis
orde
rs: R
oles
of
nutr
ition
and
the
diet
etic
s pr
actit
ione
r. J
Am
Die
t Ass
oc. 1
998;
98:2
72-2
77.
2.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Hea
lth im
plic
atio
ns o
f di
etar
y fi
ber.
J A
m D
iet A
ssoc
. 200
2;10
2:99
3-10
00.
Edi
tion:
200
6 11
0

CLIN
CAL
DOMA
IN
Bioc
hem
ical
AL
TE
RE
D N
UT
RIT
ION
-RE
LA
TE
D L
AB
OR
AT
OR
Y V
AL
UE
S (
SP
EC
IFY
) (N
C-2
.2)
De
fin
itio
n
Cha
nges
due
to b
ody
com
posi
tion,
med
icat
ions
, bod
y sy
stem
cha
nges
or
gene
tics
or c
hang
es in
abi
lity
to e
limin
ate
by-p
rodu
cts
of d
iges
tive
and
met
abol
ic
proc
esse
s
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Kid
ney,
live
r, c
ardi
ac, e
ndoc
rine
, neu
rolo
gic
and/
or p
ulm
onar
y dy
sfun
ctio
n
Oth
er o
rgan
dys
func
tion
that
lead
s to
bio
chem
ical
cha
nges
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a Fi
ndin
gs s
uch
as:
Incr
ease
d A
ST, A
LT
, T. b
ili, s
erum
am
mon
ia (
liver
dis
orde
rs)
Abn
orm
al B
UN
, Cr,
K, p
hosp
horu
s, g
lom
erul
ar f
iltra
tion
rate
(G
FR)
(kid
ney
diso
rder
s)
Alte
red
pO2
and
pCO
2 (p
ulm
onar
y di
sord
ers)
Abn
orm
al s
erum
lipi
ds
Abn
orm
al p
lasm
a gl
ucos
e le
vels
Oth
er f
indi
ngs
of a
cute
or
chro
nic
diso
rder
s th
at a
re a
bnor
mal
and
of
nutr
ition
al o
rigi
n or
con
sequ
ence
Ant
hrop
omet
ric
Mea
sure
men
ts
Rap
id w
eigh
t cha
nges
Oth
er a
nthr
opom
etri
c m
easu
res
that
are
alte
red
Phy
sica
l Exa
m F
indi
ngs
Jaun
dice
, ede
ma,
asc
ites,
itch
ing
(liv
er d
isor
ders
)
Ede
ma,
sho
rtne
ss o
f br
eath
(ca
rdia
c di
sord
ers)
Blu
e na
il be
ds, c
lubb
ing
(pul
mon
ary
diso
rder
s)
Edi
tion:
200
6 11
1

CLIN
CAL
DOMA
IN
Bioc
hem
ical
AL
TE
RE
D N
UT
RIT
ION
-RE
LA
TE
D L
AB
OR
AT
OR
Y V
AL
UE
S (
SP
EC
IFY
) (N
C-2
.2)
Foo
d/N
utri
tion
His
tory
O
bser
vatio
ns o
r re
port
s of
:
Ano
rexi
a, n
ause
a, v
omiti
ng
Inab
ility
to c
onsu
me
full
mea
ls d
ue to
sho
rtne
ss o
f br
eath
or
abdo
min
al d
iste
ntio
n
Inta
ke o
f fo
ods
high
in o
r ov
eral
l exc
ess
inta
ke o
f pr
otei
n, p
otas
sium
, pho
spho
rus,
sod
ium
, flu
id
Inad
equa
te in
take
of
mic
ronu
trie
nts
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit,
e.g.
, lac
k of
info
rmat
ion,
inco
rrec
t inf
orm
atio
n or
non
-com
plia
nce
with
m
odif
ied
diet
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
rena
l or
liver
dis
ease
, alc
ohol
ism
, car
dio-
pulm
onar
y di
sord
ers
Refe
ren
ces:
1.
Bet
o JA
, Ban
sal V
K.
Med
ical
nut
ritio
n th
erap
y in
chr
onic
kid
ney
failu
re: i
nteg
ratin
g cl
inic
al p
ract
ice
guid
elin
es. J
Am
Die
t Ass
oc. 2
004;
104:
404-
409.
2.
D
aver
n II
TJ,
Sch
arsc
hmid
t BF:
Bio
chem
ical
live
r te
sts.
In
Feld
man
M, S
char
schm
idt B
F, S
leis
enge
r M
H (
eds)
: Sle
isen
ger
and
For
dtra
n’s
Gas
roin
test
inal
and
Liv
er D
isea
se, e
d 6,
vol
2,
Phila
delp
hia,
PA
: WB
Sau
nder
s, 1
998,
pp
1112
-112
2.
3.
Dur
ose
CL
, Hol
dsw
orth
M, W
atso
n V
, Prz
ygro
dzka
F.
Kno
wle
dge
of d
ieta
ry r
estr
ictio
ns a
nd th
e m
edic
al c
onse
quen
ces
of n
onco
mpl
ianc
e by
pat
ient
s on
hem
odia
lysi
s ar
e no
t pre
dict
ive
of d
ieta
ry
com
plia
nce.
J A
m D
iet A
ssoc
. 200
4;10
4:35
-41.
4.
K
assi
ske
BL
, Lak
atua
JD
, Ma
JZ, L
ouis
TA
. A m
eta-
anal
ysis
of
the
effe
cts
of d
ieta
ry p
rote
in r
estr
icti
on o
n th
e ra
te o
f de
clin
e in
ren
al f
unct
ion.
Am
J K
idne
y D
is. 1
998;
31;9
54-9
61.
5.
Kni
ght E
L, S
tam
pfer
MJ,
Han
kins
on S
E, S
pieg
elm
an D
, Cur
han
GC
. The
impa
ct o
f pr
otei
n in
take
on
rena
l fun
ctio
n de
clin
e in
wom
en w
ith n
orm
al r
enal
fun
ctio
n or
mil
d re
nal i
nsuf
fici
ency
. Ann
In
tern
Med
. 200
3;13
8:46
0-46
7.
6.
Nak
ao T
, Mat
sum
oto,
Oka
da T
, Kan
azaw
a Y
, Yos
hino
M, N
agao
ka Y
, Tak
eguc
hi F
. Nut
ritio
nal m
anag
emen
t of
dial
ysis
pat
ient
s: b
alan
cing
am
ong
nutr
ient
inta
ke, d
ialy
sis
dose
, and
nut
ritio
nal
stat
us.
Am
J K
idne
y D
is. 2
003;
41:p
S133
-pS1
36.
7.
Nat
iona
l Kid
ney
Foun
datio
n, I
nc.
Part
5. E
valu
atio
n of
labo
rato
ry m
easu
rem
ents
for
clin
ical
ass
essm
ent o
f ki
dney
dis
ease
. A
m J
Kid
ney
Dis
. 20
02;3
9:pS
76-p
S92.
8.
N
atio
nal K
idne
y Fo
unda
tion,
Inc
. G
uide
line
9. A
ssoc
iatio
n of
leve
l of
GFR
with
nut
ritio
nal s
tatu
s. A
m J
Kid
ney
Dis
. 20
02;3
9:pS
128-
pS14
2.
Edi
tion:
200
6 11
2

CLIN
CAL
DOMA
IN
Bioc
hem
ical
FO
OD
ME
DIC
AT
ION
IN
TE
RA
CT
ION
(N
C-2
.3)
De
fin
itio
n
Und
esir
able
/har
mfu
l int
erac
tion(
s) b
etw
een
food
and
ove
r th
e co
unte
r (O
TC
) m
edic
atio
ns, p
resc
ribe
d m
edic
atio
ns, h
erba
ls, b
otan
ical
s, a
nd/o
r di
etar
y su
pple
men
ts th
at d
imin
ishe
s, e
nhan
ces,
or
alte
rs e
ffec
t of
nutr
ient
s an
d/or
med
icat
ions
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Com
bine
d in
gest
ion
or a
dmin
istr
atio
n of
med
icat
ion
and
food
that
res
ults
in u
ndes
irab
le/h
arm
ful i
nter
actio
n
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a A
ltera
tions
of
bioc
hem
ical
test
s ba
sed
upon
med
icat
ion
affe
ct a
nd p
atie
nt/c
lient
con
ditio
n
Ant
hrop
omet
ric
Mea
sure
men
ts
Alte
ratio
ns o
f an
thro
pom
etri
c m
easu
rem
ents
bas
ed u
pon
med
icat
ion
affe
ct a
nd p
atie
nt/c
lient
con
ditio
ns
e.g.
, wei
ght g
ain
and
cort
icos
tero
ids
Phy
sica
l Exa
m F
indi
ngs
Edi
tion:
200
6 11
3

CLIN
CAL
DOMA
IN
Bioc
hem
ical
FO
OD
ME
DIC
AT
ION
IN
TE
RA
CT
ION
(N
C-2
.3)
Foo
d/N
utri
tion
His
tory
O
bser
vatio
ns o
r re
port
s of
:
Inta
ke th
at is
pro
blem
atic
or
inco
nsis
tent
with
OT
C, p
resc
ribe
d dr
ugs,
her
bals
, bot
anic
als,
and
die
tary
sup
plem
ents
e.g.
, fis
h oi
ls a
nd p
rolo
nged
ble
edin
g
e.g.
, cou
mad
in, V
itam
in K
ric
h fo
ods
e.g.
, hig
h fa
t die
t whi
le o
n ch
oles
tero
l low
erin
g m
edic
atio
ns
e.g.
, iro
n su
pple
men
ts, c
onst
ipat
ion
and
low
fib
er d
iet
Inta
ke th
at d
oes
not s
uppo
rt r
epla
cem
ent o
r m
itiga
tion
of O
TC
, pre
scri
bed
drug
s, h
erba
ls, b
otan
ical
s, a
nd d
ieta
ry
supp
lem
ents
aff
ects
e.g.
, pot
assi
um w
astin
g di
uret
ics
Cha
nges
in a
ppet
ite o
r ta
ste
Clie
nt H
isto
ry
Mul
tiple
dru
gs (
OT
C, p
resc
ribe
d dr
ugs,
her
bals
, bot
anic
als,
and
die
tary
sup
plem
ents
) th
at a
re k
now
n to
hav
e fo
od
med
icat
ion
inte
ract
ions
Med
icat
ions
that
req
uire
nut
rien
t sup
plem
enta
tion
that
can
not
be
acco
mpl
ishe
d vi
a fo
od in
take
e.g.
, iso
niaz
id a
nd V
itam
in B
6
Re
fere
nc
e:
1.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Int
egra
tion
of n
utri
tion
and
phar
mac
othe
rapy
. J A
m D
iet A
ssoc
. 200
3;10
3:13
63-1
370.
Edi
tion:
200
6 11
4

CLIN
CAL
DOMA
IN
Weig
ht
UN
DE
RW
EIG
HT
(N
C-3
.1)
De
fin
itio
n
Low
bod
y w
eigh
t com
pare
d to
est
ablis
hed
refe
renc
e st
anda
rds
or r
ecom
men
datio
ns
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Dis
orde
red
eatin
g pa
ttern
Exc
essi
ve p
hysi
cal a
ctiv
ity
Har
mfu
l bel
iefs
/atti
tude
s ab
out f
ood,
nut
ritio
n, a
nd n
utri
tion-
rela
ted
topi
cs
Inad
equa
te e
nerg
y in
take
Incr
ease
d en
ergy
nee
ds
Lim
ited
acce
ss to
foo
d
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Wei
ght f
or a
ge le
ss th
an 5
th P
erce
ntile
for
Inf
ants
less
than
12
mon
ths
Dec
reas
ed s
kin
fold
thic
knes
s an
d M
AM
C
BM
I <
18.5
(m
ost a
dults
)
BM
I fo
r ol
der
adul
ts (
over
65
year
s) <
23
BM
I <
5th
per
cent
ile (
child
ren,
2-1
9 ye
ars)
Phy
sica
l Exa
m F
indi
ngs
Dec
reas
ed s
omat
ic p
rote
in s
tore
s, m
uscl
e w
astin
g (g
lute
al a
nd te
mpo
ral)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Inad
equa
te in
take
of
food
com
pare
d to
est
imat
ed o
r m
easu
red
need
s
Edi
tion:
200
6 11
5

CLIN
CAL
DOMA
IN
Weig
ht
UN
DE
RW
EIG
HT
(N
C-3
.1)
Lim
ited
supp
ly o
f fo
od in
hom
e
Die
ting,
foo
d fa
ddis
m
Hun
ger
Ref
usal
to e
at
Phys
ical
act
ivity
gre
ater
than
rec
omm
ende
d am
ount
Clie
nt H
isto
ry
Mal
nutr
ition
, vita
min
/min
eral
def
icie
ncy
Illn
ess
or p
hysi
cal d
isab
ility
Men
tal i
llnes
s, d
emen
tia, c
onfu
sion
Mea
sure
d re
stin
g m
etab
olic
rat
e (R
MR
) m
easu
rem
ent h
ighe
r th
an e
xpec
ted
and/
or e
stim
ated
RM
R
Med
icat
ions
that
aff
ect a
ppet
ite, e
.g. s
timul
ants
for
AD
HD
Ath
lete
, dan
cer,
gym
nast
Refe
ren
ces:
1.
Ass
essm
ent o
f nu
triti
onal
sta
tus.
In:
Kle
inm
an R
(ed
.). P
edia
tric
Nut
riti
on H
andb
ook,
5th e
d. A
mer
ican
Aca
dem
y of
Ped
iatr
ics,
200
4:40
7-42
3 2.
B
eck
AM
, Ove
sen
LW
. At w
hich
bod
y m
ass
inde
x an
d de
gree
of
wei
ght l
oss
shou
ld h
ospi
taliz
ed e
lder
ly p
atie
nts
be c
onsi
dere
d at
nut
ritio
nal r
isk?
Clin
Nut
r. 1
998;
17(5
):19
5-19
8
3.
Bla
um C
S, F
ries
BE
, Fia
taro
ne M
A. F
acot
ors
asso
ciat
ed w
ith lo
w b
ody
mas
s in
dex
and
wei
ght l
oss
in n
ursi
ng h
ome
resi
dent
s. J
Ger
onto
logy
: M
ed S
ci. 1
995;
50A
(3):
m16
2-M
168
4.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Dom
estic
foo
d an
d nu
triti
on s
ecur
ity. J
Am
Die
t Ass
oc. 2
002;
102:
1840
-184
7.
5.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Add
ress
ing
wor
ld h
unge
r, m
alnu
triti
on, a
nd f
ood
inse
curi
ty. J
Am
Die
t Ass
oc. 2
003;
103:
1046
-105
7.
6.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Nut
ritio
n in
terv
entio
n in
the
trea
tmen
t of
anor
exia
ner
vosa
, bul
imia
ner
vosa
, and
eat
ing
diso
rder
not
oth
erw
ise
spec
ifie
d (E
DN
OS
). J
Am
Die
t Ass
oc.
2001
;101
:810
-819
. 7.
Sc
hnei
der
SM, A
l-Ja
ouni
R, P
ivot
X, B
raul
io V
B, R
ampa
l P, H
ebue
rne
X. L
ack
of a
dapt
atio
n to
sev
ere
mal
nutr
ition
in e
lder
ly p
atie
nts.
Clin
Nut
r. 2
002;
21(6
):49
9-50
4 8.
Sp
ear
BA
. Ado
lesc
ent g
row
th a
nd d
evel
opm
ent.
J A
m D
iet A
ssoc
. 200
2 (s
uppl
);10
2:pS
23-
pS29
.
Edi
tion:
200
6 11
6

CLIN
CAL
DOMA
IN
Weig
ht
INV
OL
UN
TA
RY
WE
IGH
T L
OS
S (
NC
-3.2
)
De
fin
itio
n
Dec
reas
e in
bod
y w
eigh
t tha
t is
not p
lann
ed o
r de
sire
d
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Phys
iolo
gic
caus
es, e
.g. i
ncre
ased
nut
rien
t nee
ds d
ue to
pro
long
ed c
atab
olic
illn
ess
Lac
k of
acc
ess
to f
ood,
e.g
. eco
nom
ic c
onst
rain
ts, c
ultu
ral o
r re
ligio
us p
ract
ices
, res
tric
ting
food
giv
en to
eld
erly
and
/or
child
ren
Prol
onge
d ho
spita
lizat
ion
Psyc
holo
gica
l iss
ues
Lac
k of
sel
f fe
edin
g ab
ility
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Wei
ght l
oss
of 5
% w
ithin
30
days
, .7.
5% in
90
days
and
10%
in 1
80 d
ays
Phy
sica
l Exa
min
atio
n F
indi
ngs
Feve
r
Incr
ease
d he
art r
ate
Incr
ease
d re
spir
ator
y ra
te
Los
s of
sub
cuta
neou
s fa
t and
mus
cle
stor
es
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Nor
mal
or
usua
l int
ake
in f
ace
of il
lnes
s
Poor
inta
ke, c
hang
e in
eat
ing
habi
ts, s
kipp
ed m
eals
Cha
nge
in w
ay c
loth
es f
it
Edi
tion:
200
6 11
7
CLIN
CAL
DOMA
IN
Weig
ht
INV
OL
UN
TA
RY
WE
IGH
T L
OS
S (
NC
-3.2
)C
lient
His
tory
C
ondi
tions
ass
ocia
ted
with
a d
iagn
osis
or
trea
tmen
t of,
e.g
., A
IDS/
HIV
, bur
ns, c
hron
ic o
bstr
uctiv
e pu
lmon
ary
dise
ase,
hi
p/lo
ng b
one
frac
ture
, inf
ectio
n, s
urge
ry, t
raum
a, h
yper
thyr
oidi
sm (
pre-
or u
ntre
ated
), s
ome
type
s of
can
cer
or m
etas
tatic
di
seas
e (s
peci
fy)
Med
icat
ions
ass
ocia
ted
with
wei
ght l
oss,
suc
h as
cer
tain
ant
idep
ress
ants
or
canc
er c
hem
othe
rapy
Refe
ren
ces:
1.
Col
lins
N. P
rote
in-e
nerg
y m
alnu
triti
on a
nd in
volu
ntar
y w
eigh
t los
s: N
utri
tion
al a
nd p
harm
acol
ogic
str
ateg
ies
to e
nhan
ce w
ound
hea
ling.
Exp
ert O
pini
on P
harm
acot
her.
200
3;7:
1121
-114
0.
2.
Sple
tt PL
, Rot
h-Y
ouse
y L
L, V
ogel
zang
JL
. Med
ical
nut
ritio
n th
erap
y fo
r th
e pr
even
tion
and
trea
tmen
t of
unin
tent
iona
l wei
ght l
oss
in r
esid
entia
l hea
lthc
are
faci
litie
s. J
Am
Die
t Ass
oc. 2
003;
10
3:35
2-36
2.3.
W
alla
ce J
L, S
chw
artz
RS,
LaC
roix
AZ
, Uhl
man
n R
F, P
earl
man
RA
. Inv
olun
tary
wei
ght l
oss
in o
lder
pat
ient
s: in
cide
nce
and
clin
ical
sig
nifi
canc
e. J
Am
Ger
iatr
Soc
. 199
5;43
:329
-337
.
Edi
tion:
200
6 11
8
CLIN
CAL
DOMA
IN
Weig
ht
OV
ER
WE
IGH
T/O
BE
SIT
Y (
NC
-3.3
)
De
fin
itio
n
Incr
ease
d ad
ipos
ity c
ompa
red
to e
stab
lishe
d re
fere
nce
stan
dard
s or
rec
omm
enda
tions
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Dec
reas
ed e
nerg
y ne
eds
Dis
orde
red
eatin
g pa
ttern
Exc
ess
ener
gy in
take
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Not
rea
dy f
or d
iet/l
ifes
tyle
cha
nge
Phys
ical
inac
tivity
Incr
ease
d ps
ycho
logi
cal/l
ife
stre
ss
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
BM
I ab
ove
norm
ativ
e st
anda
rd f
or a
ge a
nd g
ende
r
Wai
st c
ircu
mfe
renc
e ab
ove
norm
ativ
e st
anda
rd f
or a
ge a
nd g
ende
r
Incr
ease
d sk
in f
old
thic
knes
s
Wei
ght f
or h
eigh
t abo
ve n
orm
ativ
e st
anda
rd f
or a
ge a
nd g
ende
r
Phy
sica
l Exa
m F
indi
ngs
Incr
ease
d bo
dy a
dipo
sity
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Ove
r co
nsum
ptio
n of
hig
h fa
t and
/or
calo
ric
dens
ity f
ood
or b
ever
age
Edi
tion:
200
6 11
9

CLIN
CAL
DOMA
IN
Weig
ht
OV
ER
WE
IGH
T/O
BE
SIT
Y (
NC
-3.3
)L
arge
por
tions
of
food
(po
rtio
n si
ze g
reat
er th
an tw
ice
than
rec
omm
ende
d)
Exc
essi
ve e
nerg
y in
take
Infr
eque
nt, l
ow d
urat
ion
and/
or lo
w in
tens
ity p
hysi
cal a
ctiv
ity
Lar
ge a
mou
nts
of s
eden
tary
act
iviti
es e
.g. T
V w
atch
ing,
rea
ding
, com
pute
r us
e in
bot
h le
isur
e an
d w
ork/
scho
ol
Unc
erta
inty
reg
ardi
ng n
utri
tion-
rela
ted
reco
mm
enda
tions
Inab
ility
to a
pply
nut
ritio
n-re
late
d re
com
men
datio
ns
Inab
ility
to m
aint
ain
wei
ght o
r re
gain
of
wei
ght
Unw
illin
gnes
s or
dis
inte
rest
in a
pply
ing
nutr
ition
-rel
ated
rec
omm
enda
tions
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
hypo
thyr
oidi
sm, m
etab
olic
syn
drom
e, e
atin
g di
sord
er n
ot
othe
rwis
e sp
ecif
ied,
dep
ress
ion
Phys
ical
dis
abili
ty o
r lim
itatio
n
His
tory
of
phys
ical
, sex
ual,
or e
mot
iona
l abu
se
Mea
sure
d re
stin
g m
etab
olic
rat
e (R
MR
) m
easu
rem
ent l
ower
than
exp
ecte
d an
d/or
est
imat
ed R
MR
Med
icat
ions
that
impa
ct R
MR
, e.g
., m
idaz
olam
, pro
pran
alol
, glip
izid
e
Refe
ren
ces:
1.
Cra
wfo
rd S
. Pr
omot
ing
diet
ary
chan
ge.
Can
J C
ardi
ol. 1
995;
11(s
uppl
A):
14A
-15A
. 2.
D
icke
rson
RN
, Rot
h-Y
ouse
y L
. Med
icat
ion
effe
cts
on m
etab
olic
rat
e: A
sys
tem
atic
rev
iew
. Unp
ublis
hed
data
.3.
K
uman
yika
SK
, Van
Hor
n L
, Bow
en D
, Per
ri M
G, R
olls
BJ,
Cza
jkow
ski S
M, S
chro
n E
. M
aint
enan
ce o
f di
etar
y be
havi
or c
hang
e. H
ealth
Psy
chol
. 200
0;19
(1 s
uppl
):S4
2-S5
6.
4.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Wei
ght m
anag
emen
t. J
Am
Die
t Ass
oc. 2
002;
102:
1145
-115
5.
5.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Tot
al d
iet a
ppro
ach
to c
omm
unic
atin
g fo
od a
nd n
utri
tion
info
rmat
ion.
J A
m D
iet A
ssoc
200
2;10
2:10
0-10
8.
6.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
The
rol
e of
die
tetic
s pr
ofes
sion
als
in h
ealth
pro
mot
ion
and
dise
ase
prev
entio
n. J
Am
Die
t Ass
oc. 2
002;
102:
1680
-168
7.
7.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Nut
ritio
n in
terv
entio
n in
the
trea
tmen
t of
anor
exia
ner
vosa
, bul
imia
ner
vosa
, and
eat
ing
diso
rder
not
oth
erw
ise
spec
ifie
d (E
DN
OS
). J
Am
Die
t Ass
oc.
2001
;101
:810
-819
. 8.
Sh
ephe
rd R
. R
esis
tanc
e to
cha
nges
in d
iet.
Pro
c N
utr
Soc.
200
2;61
:267
-272
. 9.
U
.S. P
reve
ntiv
e Se
rvic
es T
ask
Forc
e. B
ehav
iora
l cou
nsel
ing
in p
rim
ary
care
to p
rom
ote
a he
alth
y di
et. A
m J
Pre
v M
ed. 2
003;
24:9
3-10
0.
Edi
tion:
200
6 12
0

CLIN
CAL
DOMA
IN
Weig
ht
INV
OL
UN
TA
RY
WE
IGH
T G
AIN
(N
C-3
.4)
De
fin
itio
n
Wei
ght g
ain
abov
e th
at w
hich
is d
esir
ed o
r pl
anne
d
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Illn
ess
caus
ing
unex
pect
ed w
eigh
t gai
n be
caus
e of
hea
d tr
aum
a, im
mob
ility
, par
alys
is o
r re
late
d co
nditi
on
Chr
onic
use
of
med
icat
ions
kno
wn
to c
ause
wei
ght g
ain,
suc
h as
use
of
cert
ain
antid
epre
ssan
ts, a
ntip
sych
otic
s, c
ortic
oste
roid
s, c
erta
in H
IV m
edic
atio
ns
Con
ditio
n le
adin
g to
exc
essi
ve f
luid
wei
ght g
ains
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a D
ecre
ase
in s
erum
alb
umin
, hyp
onat
rem
ia, e
leva
ted
fast
ing
seru
m li
pid
leve
ls, e
leva
ted
fast
ing
gluc
ose
leve
ls, f
luct
uatin
g ho
rmon
e le
vels
Ant
hrop
omet
ric
Mea
sure
men
ts
Wei
ght h
isto
ry –
not
ing
any
incr
ease
in w
eigh
t gre
ater
than
pla
nned
or
desi
red,
suc
h as
10%
in 6
mon
ths
Not
icea
ble
chan
ge in
bod
y fa
t dis
trib
utio
n
Phy
sica
l Exa
min
atio
n F
indi
ngs
Fat a
ccum
ulat
ion
- ex
cess
ive
subc
utan
eous
fat
sto
res
Lip
odys
trop
hy a
ssoc
iate
d w
ith H
IV d
iagn
osis
- in
crea
se in
dor
soce
rvia
l fat
, bre
ast e
nlar
gem
ent,
incr
ease
d ab
dom
inal
gir
th
Ede
ma
Shor
tnes
s of
bre
ath
Sens
itivi
ty to
col
d, c
onst
ipat
ion,
and
hai
r lo
ss
Edi
tion:
200
6 12
1

CLIN
CAL
DOMA
IN
Weig
ht
INV
OL
UN
TA
RY
WE
IGH
T G
AIN
(N
C-3
.4)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Inta
ke c
onsi
sten
t with
est
imat
ed o
r m
easu
red
ener
gy n
eeds
Cha
nges
in r
ecen
t foo
d in
take
leve
l
Use
of
alco
hol,
narc
otic
s
Ext
rem
e hu
nger
with
or
with
out p
alpi
tatio
ns, t
rem
or, a
nd s
wea
ting
Phys
ical
inac
tivity
or
chan
ge in
phy
sica
l act
ivity
leve
l
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f as
thm
a, p
sych
iatr
ic il
lnes
ses,
rhe
umat
ic c
ondi
tions
, HIV
/AID
S,
Cus
hing
’s s
yndr
ome,
obe
sity
, Pra
der-
Will
i syn
drom
e
Flui
d ad
min
istr
atio
n ab
ove
requ
irem
ents
Cha
nge
in s
leep
hab
its, i
nsom
nia
Mus
cle
wea
knes
s
Fatig
ue
Med
icat
ions
ass
ocia
ted
with
incr
ease
d ap
petit
e
Refe
ren
ces:
1.
Lic
hten
stei
n K
, Del
aney
K, W
ard
D, P
alel
la F
. C
linic
al F
acto
rs a
ssoc
iate
d w
ith in
cide
nce
and
prev
alen
ce o
f fa
t atr
ophy
and
acc
umul
atio
n (a
bstr
act P
64).
Ant
ivir
The
r. 2
000;
5:6
1-62
2.
H
eath
KV
, Hog
g R
S, C
han
KJ,
Har
ris
M M
onte
ssor
i V, O
’Sha
ughn
essy
MV
, Mon
tane
r JS
. L
ipod
ystr
ophy
-ass
ocia
ted
mor
phol
ogic
al, c
hole
ster
ol a
nd tr
igly
ceri
de a
bnor
mal
ities
in a
pop
ulat
ion-
base
d H
IV/A
IDS
trea
tmen
t dat
abas
e. A
IDS.
200
1;15
:231
-239
. 3.
Sa
fri S
, Gru
nfel
d C
. Fat
dis
trib
utio
n an
d m
etab
olic
cha
nges
in p
atie
nts
with
HIV
infe
ctio
n. A
IDS.
199
9;13
:249
3-25
05.
4.
Sattl
er F
. B
ody
habi
tus
chan
ges
rela
ted
to li
pody
stro
phy.
Clin
Inf
ect D
is.
2003
;36:
pS84
-pS9
0.
Edi
tion:
200
6 12
2

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
FO
OD
AN
D N
UT
RIT
ION
-RE
LA
TE
D K
NO
WL
ED
GE
DE
FIC
IT (
NB
-1.1
)
De
fin
itio
n
Inco
mpl
ete
or in
accu
rate
kno
wle
dge
abou
t foo
d, n
utri
tion
or n
utri
tion-
rela
ted
info
rmat
ion
and
guid
elin
es e
.g. n
utri
ent r
equi
rem
ents
, con
sequ
ence
s of
foo
d be
havi
ors,
life
sta
ge r
equi
rem
ents
, nut
ritio
n re
com
men
datio
ns, d
isea
ses
and
cond
ition
s, p
hysi
olog
ical
fun
ctio
n, o
r pr
oduc
ts
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Har
mfu
l bel
iefs
/atti
tude
s ab
out f
ood,
nut
ritio
n, a
nd n
utri
tion-
rela
ted
topi
cs
Lac
k of
pri
or e
xpos
ure
to in
form
atio
n
Lan
guag
e or
cul
tura
l bar
rier
impa
ctin
g ab
ility
to le
arn
info
rmat
ion
Lea
rnin
g di
sabi
lity,
neu
rolo
gica
l or
sens
ory
impa
irm
ent
Prio
r ex
posu
re to
inco
mpa
tible
info
rmat
ion
Prio
r ex
posu
re to
inco
rrec
t inf
orm
atio
n
Unw
illin
g or
uni
nter
este
d in
lear
ning
info
rmat
ion
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Edi
tion:
200
6 12
3

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
FO
OD
AN
D N
UT
RIT
ION
-RE
LA
TE
D K
NO
WL
ED
GE
DE
FIC
IT (
NB
-1.1
)F
ood/
Nut
ritio
n H
isto
ry
Obs
erva
tions
or
repo
rts
of:
Ver
baliz
es in
accu
rate
or
inco
mpl
ete
info
rmat
ion
Prov
ides
inac
cura
te o
r in
com
plet
e w
ritte
n re
spon
se to
que
stio
nnai
re/w
ritte
n to
ol o
r is
una
ble
to r
ead
wri
tten
tool
Dem
onst
rate
s in
abili
ty to
app
ly f
ood
and
nutr
ition
-rel
ated
info
rmat
ion,
e.g
. sel
ect f
ood
base
d on
nut
ritio
n th
erap
y or
pre
pare
in
fant
fee
ding
as
inst
ruct
ed
Rel
ates
con
cern
s ab
out p
revi
ous
atte
mpt
s to
lear
n in
form
atio
n
Ver
baliz
es u
nwill
ingn
ess
or d
isin
tere
st in
lear
ning
info
rmat
ion
Clie
nt H
isto
ry
Clie
nt o
r ca
regi
ver
has
no p
rior
kno
wle
dge
of n
eed
for
food
and
nut
ritio
n-re
late
d re
com
men
datio
ns
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
men
tal i
llnes
s
New
med
ical
dia
gnos
is o
r ch
ange
in e
xist
ing
diag
nosi
s or
con
ditio
n
Refe
ren
ces:
1.
Cra
wfo
rd S
. Pr
omot
ing
diet
ary
chan
ge.
Can
J C
ardi
ol. 1
995;
11(s
uppl
A):
14A
-15A
. 2.
K
uman
yika
SK
, Van
Hor
n L
, Bow
en D
, Per
ri M
G, R
olls
BJ,
Cza
jkow
ski S
M, S
chro
n E
. M
aint
enan
ce o
f di
etar
y be
havi
or c
hang
e. H
ealth
Psy
chol
. 200
0;19
(1 s
uppl
):S4
2-S5
6.
3.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Wei
ght m
anag
emen
t. J
Am
Die
t Ass
oc. 2
002;
102:
1145
-115
5.
4.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Tot
al d
iet a
ppro
ach
to c
omm
unic
atin
g fo
od a
nd n
utri
tion
info
rmat
ion.
J A
m D
iet A
ssoc
200
2;10
2:10
0-10
8.
5.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
The
rol
e of
die
tetic
s pr
ofes
sion
als
in h
ealth
pro
mot
ion
and
dise
ase
prev
entio
n. J
Am
Die
t Ass
oc. 2
002;
102:
1680
-168
7.
6.
Shep
herd
R.
Res
ista
nce
to c
hang
es in
die
t. P
roc
Nut
r So
c. 2
002;
61:2
67-2
72.
7.
U.S
. Pre
vent
ive
Serv
ices
Tas
k Fo
rce.
Beh
avio
ral c
ouns
elin
g in
pri
mar
y ca
re to
pro
mot
e a
heal
thy
diet
. Am
J P
rev
Med
. 200
3;24
:93-
100.
Edi
tion:
200
6 12
4

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
HA
RM
FU
L B
EL
IEF
S/A
TT
ITU
DE
S O
R P
RA
CT
ICE
S A
BO
UT
FO
OD
, N
UT
RIT
ION
,
AN
D N
UT
RIT
ION
-RE
LA
TE
D T
OP
ICS
(N
B-1
.2)
Use
wit
h c
au
tion
: B
e se
nsi
tive
to p
ati
ent
con
cern
s
De
fin
itio
n
Bel
iefs
/atti
tude
s or
pra
ctic
es a
bout
foo
d, n
utri
tion,
and
nut
ritio
n-re
late
d to
pics
that
are
inco
mpa
tible
with
sou
nd n
utri
tion
prin
cipl
es, n
utri
tion
care
or
dise
ase/
cond
ition
(ex
clud
ing
diso
rder
ed e
atin
g pa
ttern
s an
d ea
ting
diso
rder
s)
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Dis
belie
f in
sci
ence
-bas
ed f
ood
and
nutr
ition
info
rmat
ion
Exp
osur
e to
inco
rrec
t foo
d an
d nu
triti
on in
form
atio
n
Eat
ing
beha
vior
ser
ves
a pu
rpos
e ot
her
than
nou
rish
men
t (e.
g. P
ICA
)
Des
ire
for
a cu
re f
or a
chr
onic
dis
ease
thro
ugh
the
use
of a
ltern
ativ
e th
erap
y
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Food
fet
ish,
PIC
A
Food
fad
dism
Inta
ke th
at r
efle
cts
an im
bala
nce
of n
utri
ents
/foo
d gr
oups
Avo
idan
ce o
f fo
ods/
food
gro
ups
(e.g
., su
gar,
whe
at, c
ooke
d fo
ods)
Edi
tion:
200
6 12
5

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
HA
RM
FU
L B
EL
IEF
S/A
TT
ITU
DE
S O
R P
RA
CT
ICE
S A
BO
UT
FO
OD
, N
UT
RIT
ION
,
AN
D N
UT
RIT
ION
-RE
LA
TE
D T
OP
ICS
(N
B-1
.2)
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
obes
ity, d
iabe
tes,
can
cer,
car
diov
ascu
lar
dise
ase,
men
tal i
llnes
s
Refe
ren
ces:
1.
Cha
pman
GE
, Bea
gan
B.
Wom
en's
per
spec
tives
on
nutr
ition
, hea
lth, a
nd b
reas
t can
cer.
J N
utr
Edu
c B
ehav
. 200
3;35
:135
-141
. 2.
G
onza
lez
VM
, Vito
usek
KM
. Fe
ared
foo
d in
die
ting
and
non-
diet
ing
youn
g w
omen
: a p
relim
inar
y va
lidat
ion
of th
e Fo
od P
hobi
a Su
rvey
. App
etite
. 200
4;43
:155
-173
. 3.
Jo
wet
t SL
, Sea
l CJ,
Phi
llips
E, G
rego
ry W
, Bar
ton
JR, W
elfa
re M
R. D
ieta
ry b
elie
fs o
f pe
ople
with
ulc
erat
ive
colit
is a
nd th
eir
effe
ct o
n re
laps
e an
d nu
trie
nt in
take
. C
lin
Nut
r. 2
004;
23:1
61-1
70.
4.
Mad
den
H, C
ham
berl
ain
K.
Nut
ritio
nal h
ealth
mes
sage
s in
wom
en's
mag
azin
es: a
con
flic
ted
spac
e fo
r w
omen
rea
ders
. J H
ealth
Psy
chol
ogy.
200
4;9:
583-
597.
5.
Pe
ters
CL
, She
lton
J, S
harm
a P.
An
inve
stig
atio
n of
fac
tors
that
infl
uenc
e th
e co
nsum
ptio
n of
die
tary
sup
plem
ents
. Hea
lth M
ark
Qua
rter
ly. 2
003;
21:1
13-1
35.
6.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Foo
d an
d nu
triti
on m
isin
form
atio
n. J
Am
Die
t Ass
oc. 2
002;
102:
260-
266.
7.
Po
vey
R, W
elle
ns B
, Con
ner
M. A
ttitu
des
tow
ards
fol
low
ing
mea
t, ve
geta
rian
and
veg
an d
iets
: an
exam
inat
ion
of th
e ro
le o
f am
biva
lenc
e. A
ppet
ite.
2001
;37:
15-2
6.
8.
Putte
rman
E, L
inde
n W
. App
eara
nce
vers
us h
ealth
: doe
s th
e re
ason
for
die
ting
affe
ct d
ietin
g be
havi
or?
J B
ehav
Med
. 200
4;27
:185
-204
. 9.
Sa
lmin
en E
, Hei
kkila
S, P
ouss
a T
, Lag
stro
m H
, Saa
rio
R, S
alm
inen
S. F
emal
e pa
tient
s te
nd to
alte
r th
eir
diet
fol
low
ing
the
diag
nosi
s of
rhe
umat
oid
arth
ritis
and
bre
ast c
ance
r. P
rev
Med
.20
02;3
4:52
9-53
5.
Edi
tion:
200
6 12
6

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
NO
T R
EA
DY
FO
R D
IET
/LIF
ES
TY
LE
CH
AN
GE
(N
B-1
.3)
De
fin
itio
n
Lac
k of
per
ceiv
ed v
alue
of
nutr
ition
-rel
ated
beh
avio
r ch
ange
com
pare
d to
cos
ts (
cons
eque
nces
or
effo
rt r
equi
red
to m
ake
chan
ges)
; con
flic
t w
ith p
erso
nal
valu
e sy
stem
; ant
eced
ent t
o be
havi
or c
hang
e
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Har
mfu
l bel
iefs
/atti
tude
s ab
out f
ood,
nut
ritio
n, a
nd n
utri
tion-
rela
ted
topi
cs
Cog
nitiv
e de
fici
ts o
r in
abili
ty to
foc
us o
n di
etar
y ch
ange
s
Lac
k of
soc
ial s
uppo
rt f
or im
plem
entin
g ch
ange
s
Den
ial o
f ne
ed to
cha
nge
Perc
eptio
n th
at ti
me,
inte
rper
sona
l or
fina
ncia
l con
stra
ints
pre
vent
cha
nges
Unw
illin
g or
uni
nter
este
d in
lear
ning
info
rmat
ion
Lac
k of
sel
f-ef
fica
cy f
or m
akin
g ch
ange
or
dem
oral
izat
ion
from
pre
viou
s fa
ilure
s at
cha
nge
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Neg
ativ
e bo
dy la
ngua
ge, e
.g. f
row
ning
, lac
k of
eye
con
tact
, def
ensi
ve p
ostu
re, l
ack
of f
ocus
, fid
getin
g (N
ote.
Bod
y la
ngua
ge v
arie
s by
cul
ture
.)
Edi
tion:
200
6 12
7
BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
NO
T R
EA
DY
FO
R D
IET
/LIF
ES
TY
LE
CH
AN
GE
(N
B-1
.3)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Den
ial o
f ne
ed f
or f
ood
and
nutr
ition
-rel
ated
cha
nges
Inab
ility
to u
nder
stan
d re
quir
ed c
hang
es
Failu
re to
kee
p ap
poin
tmen
ts/s
ched
ule
follo
w-u
p ap
poin
tmen
ts o
r en
gage
in c
ouns
elin
g
Prev
ious
fai
lure
s to
eff
ectiv
ely
chan
ge ta
rget
beh
avio
r
Def
ensi
vene
ss, h
ostil
ity o
r re
sist
ance
to c
hang
e
Lac
k of
eff
icac
y to
mak
e ch
ange
or
to o
verc
ome
barr
iers
to c
hang
e
Clie
nt H
isto
ry
New
med
ical
dia
gnos
is, c
hang
e in
exi
stin
g di
agno
sis
or c
ondi
tion,
or
chro
nic
non-
com
plia
nce
Refe
ren
ces:
1.
Cra
wfo
rd S
. Pr
omot
ing
diet
ary
chan
ge.
Can
J C
ardi
ol. 1
995;
11:1
4A-1
5A.
2.
Gre
ene,
GW
, Ros
si, S
R, R
ossi
, JS,
Vel
icer
, WF,
Fav
a, J
S, P
roch
aska
, JO
. D
ieta
ry a
pplic
atio
ns o
f th
e St
ages
of
Cha
nge
Mod
el.
J A
m D
iet A
ssoc
. 19
99; 9
9:67
3-67
8.
3.
Kum
anyi
ka S
K, V
an H
orn
L, B
owen
D, P
erri
MG
, Rol
ls B
J, C
zajk
owsk
i SM
, Sch
ron
E.
Mai
nten
ance
of
diet
ary
beha
vior
cha
nge.
Hea
lth P
sych
ol. 2
000;
19:p
S42-
pS56
. 4.
Pr
ocha
ska
JO, V
elic
er W
F.
The
Tra
nsth
eore
tical
Mod
el o
f be
havi
or c
hang
e. A
m J
Hea
lth
Pro
mot
ion.
199
7;12
: 38–
48.
5.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Tot
al d
iet a
ppro
ach
to c
omm
unic
atin
g fo
od a
nd n
utri
tion
info
rmat
ion.
J A
m D
iet A
ssoc
200
2;10
2:10
0-10
8.
6.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
The
rol
e of
die
tetic
s pr
ofes
sion
als
in h
ealth
pro
mot
ion
and
dise
ase
prev
entio
n. J
Am
Die
t Ass
oc. 2
002;
102:
1680
-168
7.
7.
Res
nico
w K
, Jac
kson
A, W
ang
T, D
e A
, McC
arty
F, D
udle
y W
, B
aron
owsk
i T. A
mot
ivat
iona
l int
ervi
ewin
g in
terv
entio
n to
incr
ease
fru
it an
d ve
geta
ble
inta
ke th
roug
h bl
ack
chur
ches
: Res
ults
of
the
Eat
for
Lif
e tr
ial.
Am
J P
ublic
Hea
lth.
2001
; 91:
1686
-169
3.
8.
Shep
herd
R.
Res
ista
nce
to c
hang
es in
die
t. P
roc
Nut
r So
c. 2
002;
61:2
67-2
72.
9.
U.S
. Pre
vent
ive
Serv
ices
Tas
k Fo
rce.
Beh
avio
ral c
ouns
elin
g in
pri
mar
y ca
re to
pro
mot
e a
heal
thy
diet
. Am
J P
rev
Med
. 200
3;24
:93-
100.
Edi
tion:
200
6 12
8

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
SE
LF
-MO
NIT
OR
ING
DE
FIC
IT (
NB
-1.4
)
De
fin
itio
n
Lac
k of
dat
a re
cord
ing
to tr
ack
pers
onal
pro
gres
s
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Lac
k of
soc
ial s
uppo
rt f
or im
plem
entin
g ch
ange
s
Lac
k of
val
ue f
or b
ehav
ior
chan
ge o
r co
mpe
ting
valu
es
Perc
eptio
n th
at la
ck o
f re
sour
ces,
e.g
., tim
e, f
inan
cial
, or
soci
al s
uppo
rt p
reve
nt s
elf-
mon
itori
ng
Cul
tura
l bar
rier
impa
ctin
g ab
ility
to tr
ack
pers
onal
pro
gres
s
Lea
rnin
g di
sabi
lity,
neu
rolo
gica
l, or
sen
sory
impa
irm
ent
Prio
r ex
posu
re to
inco
mpa
tible
info
rmat
ion
Not
rea
dy f
or d
iet/l
ifes
tyle
cha
nge
Unw
illin
g or
uni
nter
este
d in
trac
king
pro
gres
s
Lac
k of
foc
us a
nd a
ttent
ion
to d
etai
l, di
ffic
ulty
with
tim
e m
anag
emen
t and
/or
orga
niza
tion
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a R
ecor
ded
data
inco
nsis
tent
with
bio
chem
ical
dat
a, e
.g.,
diet
ary
inta
ke is
not
con
sist
ent w
ith b
ioch
emic
al d
ata
Ant
hrop
omet
ric
Mea
sure
men
ts
Rec
orde
d da
ta in
cons
iste
nt w
ith w
eigh
t sta
tus
or g
row
th p
atte
rn d
ata,
e.g
., di
etar
y in
take
is n
ot c
onsi
sten
t with
wei
ght
stat
us o
r gr
owth
pat
tern
Phy
sica
l Exa
m F
indi
ngs
Edi
tion:
200
6 12
9
BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
SE
LF
-MO
NIT
OR
ING
DE
FIC
IT (
NB
-1.4
)F
ood/
Nut
ritio
n H
isto
ry
Rep
orts
or
obse
rvat
ions
of:
Inco
mpl
ete
self
-mon
itori
ng r
ecor
ds, e
.g.,
gluc
ose,
foo
d, f
luid
inta
ke, w
eigh
t, ph
ysic
al a
ctiv
ity, o
stom
y ou
tput
rec
ords
Em
barr
assm
ent o
r an
ger
rega
rdin
g ne
ed f
or s
elf-
mon
itori
ng
Unc
erta
inty
of
how
to c
ompl
ete
mon
itori
ng r
ecor
ds
Unc
erta
inty
reg
ardi
ng c
hang
es th
at c
ould
/sho
uld
be m
ade
in r
espo
nse
to d
ata
in s
elf
mon
itori
ng r
ecor
ds
No
self
man
agem
ent e
quip
men
t, e.
g. n
o bl
ood
gluc
ose
mon
itor,
ped
omet
er
Clie
nt H
isto
ry
Dia
gnos
es a
ssoc
iate
d w
ith s
elf-
mon
itori
ng, e
.g.,
diab
etes
mel
litus
, obe
sity
, new
ost
omy
New
med
ical
dia
gnos
is o
r ch
ange
in e
xist
ing
diag
nosi
s or
con
ditio
n
Refe
ren
ces:
1.
Am
eric
an D
iabe
tes
Ass
ocia
tion.
Tes
ts o
f gl
ycem
ia in
dia
bete
s. D
iabe
tes
Car
e. 2
004;
27:p
S91-
pS93
. 2.
B
aker
RC
, Kir
sche
nbau
m D
S. W
eigh
t con
trol
dur
ing
the
holid
ays:
hig
hly
cons
iste
nt s
elf-
mon
itori
ng a
s a
pote
ntia
lly u
sefu
l cop
ing
mec
hani
sm. H
ealt
h P
sych
ol. 1
998;
17:3
67-3
70.
3.
Ber
kow
itz R
I, W
adde
n T
A, T
ersh
akov
ec A
M. B
ehav
ior
ther
apy
and
sibu
tram
ine
for
trea
tmen
t of
adol
esce
nt o
besi
ty. J
AM
A. 2
003;
289:
1805
-181
2.
4.
Cra
wfo
rd S
. Pr
omot
ing
diet
ary
chan
ge.
Can
J C
ardi
ol. 1
995;
11(s
uppl
A):
14A
-15A
. 5.
Je
ffer
y R
, Dre
wno
wsk
i A, E
pste
in L
, Stu
nkar
d A
, Wils
on G
, Win
g R
: Lon
g-te
rm m
aint
enan
ce o
f w
eigh
t los
s: c
urre
nt s
tatu
s. H
ealth
Psy
chol
ogy.
200
0;19
:5-1
6.
6.
Kum
anyi
ka S
K, V
an H
orn
L, B
owen
D, P
erri
MG
, Rol
ls B
J, C
zajk
owsk
i SM
, Sch
ron
E.
Mai
nten
ance
of
diet
ary
beha
vior
cha
nge.
Hea
lth P
sych
ol. 2
000;
19(1
sup
pl):
S42-
S56.
7.
L
icht
man
SW
, Pis
arka
K, B
erm
an E
R e
t al:
Dis
crep
ancy
bet
wee
n se
lf-r
epor
ted
and
actu
al c
alor
ic in
take
and
exe
rcis
e in
obe
se s
ubje
cts.
N E
ngl J
Med
. 19
92;3
27:1
893-
1898
. 8.
W
adde
n, T
A. C
hara
cter
istic
s of
suc
cess
ful w
eigh
t los
s m
aint
aine
rs. I
n: A
lliso
n D
B, P
i-Su
nyer
FX
, edi
tors
. Obe
sity
trea
tmen
t: e
stab
lishi
ng g
oals
, im
prov
ing
outc
omes
, and
rev
iew
ing
the
rese
arch
ag
enda
. New
Yor
k: P
lenu
m P
ress
; 199
5. p
. 103
-111
.
Edi
tion:
200
6 13
0

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
DIS
OR
DE
R E
AT
ING
PA
TT
ER
N (
NB
-1.5
)
De
fin
itio
n
Bel
iefs
, atti
tude
s, th
ough
ts a
nd b
ehav
iors
rel
ated
to f
ood,
eat
ing,
and
wei
ght m
anag
emen
t, in
clud
ing
clas
sic
eatin
g di
sord
ers
as w
ell a
s le
ss s
ever
e, s
imila
r co
nditi
ons
that
neg
ativ
ely
impa
ct h
ealth
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Fam
ilial
, soc
ieta
l, bi
olog
ical
/gen
etic
, and
/or
envi
ronm
enta
l rel
ated
obs
essi
ve d
esir
e to
be
thin
Wei
ght r
egul
atio
n/pr
eocc
upat
ion
sign
ific
antly
infl
uenc
es s
elf
este
em
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a E
leva
ted
chol
este
rol,
abno
rmal
lipi
d pr
ofile
s, h
ypog
lyce
mia
, hyp
okal
emia
[an
orex
ia n
ervo
sa (
AN
)]
Hyp
okal
emia
and
hyp
ochl
orem
ic a
lkal
osis
[bu
limia
ner
vosa
(B
N)]
H
ypot
ensi
on, b
rady
card
ia, l
ow b
ody
tem
pera
ture
, hyp
onat
rem
ia, a
nem
ia, h
ypot
hyro
id, l
euco
peni
a, e
leva
ted
BU
N (
AN
) U
rine
pos
itive
for
ket
ones
(A
N)
Ant
hrop
omet
ric
Mea
sure
men
ts
BM
I <
17.
5, a
rres
ted
grow
th a
nd d
evel
opm
ent,
failu
re to
gai
n w
eigh
t dur
ing
peri
od o
f ex
pect
ed g
row
th, w
eigh
t les
s th
an
85%
of
expe
cted
(A
N)
BM
I >
29 [
eatin
g di
sord
er n
ot o
ther
wis
e sp
ecif
ied
(ED
NO
S)]
Sign
ific
ant w
eigh
t flu
ctua
tion
(BN
)
Edi
tion:
200
6 13
1

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
DIS
OR
DE
R E
AT
ING
PA
TT
ER
N (
NB
-1.5
)P
hysi
cal E
xam
Fin
ding
s Se
vere
ly d
eple
ted
adip
ose
and
som
atic
pro
tein
sto
res
(AN
) L
anug
o ha
ir f
orm
atio
n on
fac
e an
d tr
unk,
bri
ttle
listle
ss h
air,
cya
nosi
s of
han
ds a
nd f
eet,
and
dry
skin
(A
N)
N
orm
al o
r ex
cess
adi
pose
and
nor
mal
som
atic
pro
tein
sto
res
(BN
, ED
NO
S)
Dam
aged
toot
h en
amel
(B
N)
Enl
arge
d pa
rotid
gla
nds
(BN
) Pe
riph
eral
ede
ma
(BN
) Sk
elet
al m
uscl
e lo
ss (
AN
) C
ardi
ac a
rrhy
thm
ias
(AN
, BN
) Ir
rita
bilit
y, d
epre
ssio
n (A
N, B
N)
Inab
ility
to c
once
ntra
te (
AN
) Po
sitiv
e R
usse
ll’s
Sign
(B
N)
callo
us o
n ba
ck o
f ha
nd f
rom
sel
f in
duce
d vo
miti
ng
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Avo
idan
ce o
f fo
od o
r ca
lori
e co
ntai
ning
bev
erag
es (
AN
, BN
) Fe
ar o
f fo
ods
or d
ysfu
nctio
nal t
houg
hts
rega
rdin
g fo
od o
r fo
od e
xper
ienc
es (
AN
, BN
)
Den
ial o
f hu
nger
(A
N)
Food
pre
occu
patio
n (A
N, B
N)
Kno
wle
dgea
ble
abou
t cur
rent
die
t fad
(A
N, B
N, E
DN
OS)
Fa
stin
g (A
N, B
N)
Inta
ke o
f la
rger
qua
ntity
of
food
in a
def
ined
tim
e pe
riod
, a s
ense
of
lack
of
cont
rol o
ver
eatin
g du
ring
the
epis
ode
(BN
, E
DN
OS)
E
xces
sive
phy
sica
l act
ivity
(A
N, B
N, E
DN
OS)
E
atin
g m
uch
mor
e ra
pidl
y th
an n
orm
al, u
ntil
feel
ing
unco
mfo
rtab
ly f
ull,
cons
umin
g la
rge
amou
nts
of f
ood
whe
n no
t fee
ling
phys
ical
ly h
ungr
y; e
atin
g al
one
beca
use
of b
eing
em
barr
asse
d by
how
muc
h on
e is
eat
ing;
fee
ling
disg
uste
d w
ith o
nese
lf,
depr
esse
d, o
r ve
ry g
uilty
aft
er o
vere
atin
g (E
DN
OS)
E
ats
in p
riva
te (
AN
, BN
) Ir
ratio
nal t
houg
hts
abou
t foo
d’s
affe
ct o
n th
e bo
dy (
AN
, BN
, ED
NO
S)
Patte
rn o
f ch
roni
c di
etin
g W
eigh
t pre
occu
patio
n
Exc
essi
ve r
elia
nce
on n
utri
tion
Ter
min
g an
d pr
eocc
upat
ion
with
nut
rien
t con
tent
of
food
s In
flex
ibili
ty w
ith f
ood
sele
ctio
n
Edi
tion:
200
6 13
2

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
DIS
OR
DE
R E
AT
ING
PA
TT
ER
N (
NB
-1.5
)C
lient
His
tory
B
rady
card
ia (
Hea
rt R
ate
<60
beat
s/m
in),
hyp
oten
sion
(sy
stol
ic <
90 m
m H
G),
and
ort
host
atic
hyp
oten
sion
(A
N)
Self
-ind
uced
vom
iting
, dia
rrhe
a, b
loat
ing,
con
stip
atio
n an
d fl
atul
ence
(B
N),
alw
ays
cold
(A
N)
Mis
use
of la
xativ
es, e
nem
as, d
iure
tics,
stim
ulan
ts a
nd o
r m
etab
olic
enh
ance
rs (
AN
,BN
)
Mus
cle
wea
knes
s, f
atig
ue, c
ardi
ac a
rrhy
thm
ias,
deh
ydra
tion
and
elec
trol
yte
imba
lanc
e (A
N, B
N)
D
iagn
osis
e.g
. ano
rexi
a ne
rvos
a, b
ulim
ia n
ervo
sa, b
inge
eat
ing,
eat
ing
diso
rder
not
oth
erw
ise
spec
ifie
d, a
men
orrh
ea,
His
tory
of
moo
d an
d an
xiet
y di
sord
ers
(e.g
., de
pres
sion
, obs
essi
ve c
ompu
lsiv
e di
sord
er),
per
sona
lity
diso
rder
s, s
ubst
ance
ab
use
diso
rder
s Fa
mily
his
tory
of
ED
, dep
ress
ion,
OC
D, a
nxie
ty d
isor
ders
(A
N, B
N)
Avo
idan
ce o
f so
cial
eve
nts
whe
re f
ood
is s
erve
d
Refe
ren
ces:
1.
And
erso
n G
H, K
enne
dy S
H, e
ds. T
he B
iolo
gy o
f Fea
st a
nd F
amin
e. N
ew Y
ork:
Aca
dem
ic P
ress
, 199
2.
2.
Am
eric
an P
sych
iatr
ic A
ssoc
iatio
n. D
iagn
ostic
and
sta
tistic
al m
anua
l for
men
tal d
isor
ders
(fo
urth
edi
tion,
text
rev
isio
n). A
PA P
ress
: Was
hing
ton
DC
; 200
0.
3.
Am
eric
an P
sych
iatr
ic A
ssoc
iatio
n. P
ract
ice
guid
elin
es f
or th
e tr
eatm
ent o
f pa
tient
s w
ith e
atin
g di
sord
ers.
Am
J P
sych
. 200
0;15
7 (s
uppl
):1-
39.
4.
Coo
ke R
A, C
ham
bers
JB
. Ano
rexi
a ne
rvos
a an
d th
e he
art.
Br
J H
osp
Med
. 199
5;54
:313
-317
. 5.
Fi
sher
M. M
edic
al c
ompl
icat
ions
of
anor
exia
and
bul
imia
ner
vosa
. Ado
l Med
Sta
t of t
he A
rt R
evie
ws.
199
2;3:
481-
502.
6.
G
rale
n SJ
, Lev
in M
P, S
mol
ak L
et a
l. D
ietin
g an
d di
sord
ered
eat
ing
duri
ng e
arly
and
mid
dle
adol
esce
nts:
Do
the
infl
uenc
es r
emai
n th
e sa
me?
Int
J E
atin
g D
isor
der.
199
0;9:
501-
512.
7.
H
arri
s JP
, Kri
epe
RE
, Ros
sbac
k C
N. Q
T p
rolo
ngat
ion
by is
opro
tere
nol i
n an
orex
ia n
ervo
sa. J
Ado
l Hea
lth. 1
993;
14:3
90-3
93.
8.
Kap
lan
AS,
Gar
funk
el P
E, e
ds. M
edic
al I
ssue
s an
d th
e E
atin
g D
isor
ders
: Th
e In
terf
ace.
New
Yor
k: B
runn
er/M
anze
l Pub
lishe
rs, 1
993.
9.
K
eys
A, B
roze
k J,
Hen
sche
l A, M
icke
lson
O, T
aylo
r H
L. T
he B
iolo
gy o
f Hum
an S
tarv
atio
n, 2
nd v
ol. M
inne
apol
is, M
N: U
nive
rsity
of
Min
neso
ta P
ress
, 195
0.
10.
Kir
kley
BG
. Bul
imia
: clin
ical
cha
ract
eris
tics,
dev
elop
men
t, an
d et
iolo
gy. J
Am
Die
t Ass
oc. 1
986;
86:4
68-4
75.
11.
Kre
ipe
RE
, Uph
off
M. T
reat
men
t and
out
com
e of
ado
lesc
ents
with
ano
rexi
a ne
rvos
a. A
dole
sc M
ed.1
992;
16:5
19-5
40.
12.
Kre
ipe
RE
, Bir
ndor
f D
O. E
atin
g di
sord
ers
in a
dole
scen
ts a
nd y
oung
adu
lts. M
edic
al C
linic
s of
Nor
th A
mer
ica.
200
0;84
(4):
1027
-104
9.
13.
Mor
dasi
ni R
, Klo
se G
, Gre
ter
H. S
econ
dary
type
II
hype
rlip
opro
tein
emia
in p
atie
nts
with
ano
rexi
a ne
rvos
a. M
etab
olis
m. 1
978;
27:7
1-79
. 14
. Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: N
utri
tion
inte
rven
tion
in th
e tr
eatm
ent o
f an
orex
ia n
ervo
sa, b
ulim
ia n
ervo
sa, a
nd e
atin
g di
sord
er n
ot o
ther
wis
e sp
ecif
ied
(ED
NO
S).
J A
m D
iet A
ssoc
.20
01;1
01:8
10-8
19.
15.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Nut
ritio
n in
terv
entio
n in
the
trea
tmen
t of
anor
exia
ner
vosa
, bul
imia
ner
vosa
, and
eat
ing
diso
rder
not
oth
erw
ise
spec
ifie
d (E
DN
OS
). J
Am
Die
t Ass
oc.
2001
;101
:810
-819
. 16
. R
ock
C, Y
ager
J. N
utri
tion
and
eatin
g di
sord
ers:
a p
rim
er f
or c
linic
ians
. Int
J E
atin
g D
is. 1
987;
6:26
7-28
0.
17.
Roc
k, C
L. N
utri
tiona
l and
med
ical
ass
essm
ent a
nd m
anag
emen
t of
eatin
g di
sord
ers.
Nut
r C
lin C
are.
199
9;2:
332-
343.
18
. Sc
hebe
ndac
h J,
Rei
cher
t-A
nder
son
P. N
utri
tion
in E
atin
g D
isor
ders
. In:
Kra
us’s
Nut
riti
on a
nd D
iet T
hera
py. M
ahan
K, E
scot
t-St
ump
S (e
ds).
McG
raw
- H
ill: N
ew Y
ork,
NY
; 200
0.
19.
Silb
er T
. Ano
rexi
a ne
rvos
a: M
orbi
dity
and
mor
talit
y. P
ed A
nn. 1
984;
13:
851-
859.
20
. Sw
enne
I. H
eart
ris
k as
soci
ated
with
wei
ght l
oss
in a
nore
xia
nerv
osa
and
eatin
g di
sord
ers:
ele
ctro
card
iogr
aphi
c ch
ange
s du
ring
the
earl
y ph
ase
of r
efee
ding
. Act
a P
aedi
atr.
200
0;89
:447
-452
. 21
. T
urne
r JM
, Bul
sara
MK
, McD
erm
ott B
M, B
yrne
GC
, Pri
nce
RL
, For
bes
DA
. Pr
edic
tors
of
low
bon
e de
nsity
in y
oung
ado
lesc
ent f
emal
es w
ith a
nore
xia
nerv
osa
and
othe
r di
etin
g di
sord
ers.
Int
J
Eat
ing
Dis
orde
rs.
2001
;30:
245-
251.
Edi
tion:
200
6 13
3

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
LIM
ITE
D A
DH
ER
EN
CE
TO
NU
TR
ITIO
N-R
EL
AT
ED
RE
CO
MM
EN
DA
TIO
NS
(N
B-1
.6)
De
fin
itio
n
Lac
k of
nut
ritio
n-re
late
d ch
ange
s as
per
inte
rven
tion
agre
ed u
pon
by c
lient
or
popu
latio
n
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Lac
k of
soc
ial s
uppo
rt f
or im
plem
entin
g ch
ange
s
Lac
k of
val
ue f
or b
ehav
ior
chan
ge o
r co
mpe
ting
valu
es
Perc
eptio
n th
at ti
me
or f
inan
cial
con
stra
ints
pre
vent
cha
nges
Prev
ious
lack
of
succ
ess
in m
akin
g he
alth
-rel
ated
cha
nges
Poor
und
erst
andi
ng o
f ho
w a
nd w
hy to
mak
e th
e ch
ange
Unw
illin
g or
uni
nter
este
d in
app
lyin
g in
form
atio
n
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a E
xpec
ted
labo
rato
ry o
utco
mes
are
not
ach
ieve
d
Ant
hrop
omet
ric
Mea
sure
men
ts
Exp
ecte
d an
thro
pom
etri
c ou
tcom
es a
re n
ot a
chie
ved
Phy
sica
l Exa
m F
indi
ngs
Neg
ativ
e bo
dy la
ngua
ge, e
.g. f
row
ning
, lac
k of
eye
con
tact
, fid
getin
g
Edi
tion:
200
6 13
4

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
LIM
ITE
D A
DH
ER
EN
CE
TO
NU
TR
ITIO
N-R
EL
AT
ED
RE
CO
MM
EN
DA
TIO
NS
(N
B-1
.6)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Exp
ecte
d fo
od/n
utri
tion-
rela
ted
outc
omes
are
not
ach
ieve
d In
abili
ty to
rec
all a
gree
d up
on c
hang
es
Failu
re to
com
plet
e an
y ag
reed
upo
n ho
mew
ork
Lac
k of
com
plia
nce
or in
cons
iste
nt c
ompl
ianc
e w
ith p
lan
Fa
ilure
to k
eep
appo
intm
ents
or
sche
dule
fol
low
-up
appo
intm
ents
L
ack
of a
ppre
ciat
ion
of th
e im
port
ance
of
mak
ing
reco
mm
ende
d nu
triti
on-r
elat
ed c
hang
es
Unc
erta
inty
as
to h
ow to
con
sist
ently
app
ly f
ood/
nutr
ition
info
rmat
ion
Clie
nt H
isto
ry
Refe
ren
ces:
1.
Cra
wfo
rd S
. Pr
omot
ing
diet
ary
chan
ge.
Can
J C
ardi
ol. 1
995;
11(s
uppl
A):
14A
-15A
. 2.
K
uman
yika
SK
, Van
Hor
n L
, Bow
en D
, Per
ri M
G, R
olls
BJ,
Cza
jkow
ski S
M, S
chro
n E
. M
aint
enan
ce o
f di
etar
y be
havi
or c
hang
e. H
ealth
Psy
chol
. 200
0;19
(1 s
uppl
):S4
2-S5
6.
3.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Tot
al d
iet a
ppro
ach
to c
omm
unic
atin
g fo
od a
nd n
utri
tion
info
rmat
ion.
J A
m D
iet A
ssoc
200
2;10
2:10
0-10
8.
4.
Shep
herd
R.
Res
ista
nce
to c
hang
es in
die
t. P
roc
Nut
r So
c. 2
002;
61:2
67-2
72.
5.
U.S
. Pre
vent
ive
Serv
ices
Tas
k Fo
rce.
Beh
avio
ral c
ouns
elin
g in
pri
mar
y ca
re to
pro
mot
e a
heal
thy
diet
. Am
J P
rev
Med
. 200
3;24
:93-
100.
Edi
tion:
200
6 13
5

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
UN
DE
SIR
AB
LE
FO
OD
CH
OIC
ES
(N
B-1
.7)
De
fin
itio
n
Food
and
/or
beve
rage
cho
ices
that
are
inco
nsis
tent
with
US
Rec
omm
ende
d D
ieta
ry I
ntak
e, U
S D
ieta
ry G
uide
lines
, or
with
the
Food
Gui
de P
yram
id o
r w
ith
targ
ets
defi
ned
in th
e nu
triti
on p
resc
ript
ion
or n
utri
tion
care
pro
cess
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Lac
k of
pri
or e
xpos
ure
to o
r m
isun
ders
tand
ing
of in
form
atio
n
Lan
guag
e, r
elig
ious
, or
cultu
ral b
arri
er im
pact
ing
abili
ty to
app
ly in
form
atio
n
Lea
rnin
g di
sabi
litie
s, n
euro
logi
cal o
r se
nsor
y im
pair
men
t
Hig
h le
vel o
f fa
tigue
or
othe
r si
de e
ffec
t of
ther
apy
Inad
equa
te a
cces
s to
rec
omm
ende
d fo
ods
Perc
eptio
n th
at f
inan
cial
con
stra
ints
pre
vent
sel
ectio
n of
foo
d ch
oice
s co
nsis
tent
with
rec
omm
enda
tions
Food
alle
rgie
s an
d av
ersi
ons
impe
ding
foo
d ch
oice
s co
nsis
tent
with
gui
delin
es
Lac
ks m
otiv
atio
n an
d or
rea
dine
ss to
app
ly o
r su
ppor
t sys
tem
s ch
ange
Unw
illin
g or
uni
nter
este
d in
lear
ning
info
rmat
ion
Psyc
holo
gica
l lim
itatio
ns
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a E
leva
ted
lipid
pan
el
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Find
ings
con
sist
ent w
ith v
itam
in/m
iner
al d
efic
ienc
y or
exc
ess
Edi
tion:
200
6 13
6

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Kno
wled
ge an
d Be
liefs
UN
DE
SIR
AB
LE
FO
OD
CH
OIC
ES
(N
B-1
.7)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Inta
ke in
cons
iste
nt w
ith U
S D
ieta
ry G
uide
lines
or
Food
Gui
de P
yram
id (
e.g.
, om
issi
on o
f en
tire
nutr
ient
gro
ups,
di
spro
port
iona
te in
take
[e.
g., j
uice
for
you
ng c
hild
ren]
)
Inac
cura
te o
r in
com
plet
e un
ders
tand
ing
of th
e gu
idel
ines
Inab
ility
to a
pply
gui
delin
e in
form
atio
n
Inab
ility
to (
e.g.
acc
ess)
, unw
illin
gnes
s, o
r di
sint
eres
t in
sele
ctin
g fo
od c
onsi
sten
t with
the
guid
elin
es
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
men
tal i
llnes
s
Refe
ren
ces:
1.
Bir
ch L
L, F
ishe
r JA
. App
etite
and
eat
ing
beha
vior
in c
hild
ren.
Ped
iatr
Cli
n N
orth
Am
.199
5:42
(4)9
31-9
53.
2.
But
te N
, Cob
b K
, Dw
yer
J, G
rane
y L
, Hei
rd W
, Ric
hard
K. T
he s
tart
hea
lthy
feed
ing
guid
elin
es f
or in
fant
s an
d to
ddle
rs. J
Am
Die
t Ass
oc.2
004:
104:
3:44
2-45
4.
3.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Wei
ght m
anag
emen
t. J
Am
Die
t Ass
oc. 2
002;
102:
1145
-115
5.
4.
Dol
ecek
TA
, Sta
mle
e J,
Cag
giul
a A
W, T
illot
son
JL, B
uzza
rd I
M. M
etho
ds o
f di
etar
y an
d nu
triti
onal
ass
essm
ent a
nd in
terv
entio
n an
d ot
her
met
hods
in th
e m
ultip
le r
isk
fact
or in
terv
entio
n tr
ial.
Am
J C
lin N
utr.
199
7;65
(sup
pl):
196S
-210
S.
5.
Eps
tein
LH
, Gor
dy C
C, R
ayno
r H
A, B
eddo
me
M, K
ilano
wsk
i CK
, Pal
uch
R. I
ncre
asin
g fr
uit a
nd v
eget
able
inta
ke a
nd d
ecre
asin
g fa
t and
sug
ar in
take
in f
amili
es a
t ris
k fo
r ch
ildho
od o
besi
ty.
Obe
sity
Res
.200
1:9:
171-
178.
6.
Fr
eela
nd-G
rave
s J,
Nitz
ke S
. Tot
al d
iet a
ppro
ach
to c
omm
unic
atin
g fo
od a
nd n
utri
tion
info
rmat
ion.
J A
m D
iet A
ssoc
200
2;10
2:10
0-10
8.
7.
Fren
ch S
A. P
rici
ng e
ffec
ts o
n fo
od c
hoic
es. J
Nut
r. 2
003;
133:
841S
-843
S.
8.
Gle
ns K
, Bas
il M
, Mar
iach
i E, G
oldb
erg
J, S
nyde
r D
. Why
Am
eric
ans
eat w
hat t
hey
do: t
aste
, nut
ritio
n, c
ost,
conv
enie
nce
and
wei
ght c
ontr
ol c
once
rns
as in
flue
nces
on
food
con
sum
ptio
n. J
Am
D
iet A
ssoc
. 199
8;98
:111
8-11
26.
9.
Ham
pl J
S, A
nder
son
JV, M
ullis
R. T
he r
ole
of d
iete
tics
prof
essi
onal
s in
hea
lth p
rom
otio
n an
d di
seas
e pr
even
tion.
J A
m D
iet A
ssoc
. 200
2;10
2:16
80-1
687.
10
. L
in S
H, G
uthr
ie J
, Fra
zao
E. A
mer
ican
chi
ldre
n’s’
die
ts a
re n
ot m
akin
g th
e gr
ade.
Foo
d R
evie
w. 2
001;
24(2
): 8
-17.
11
. Sa
tter
E. F
eedi
ng d
ynam
ics:
hel
ping
chi
ldre
n to
eat
wel
l. J
Ped
iatr
Hea
lthca
re. 1
995;
9:17
8-18
4.
12.
Stor
y M
, Hol
t K, S
ofka
D, e
ds. 2
002.
Bri
ght f
utur
es in
pra
ctic
e: N
utri
tion,
2nd
. Ed.
Arl
ingt
on, V
A N
atio
nal C
ente
r fo
r E
duca
tion
in M
ater
nal C
hild
Hea
lth.
13.
Pelto
GH
, Lev
itt E
, Tha
iru
L. I
mpr
ovin
g fe
edin
g pr
actic
es, c
urre
nt p
atte
rns,
com
mon
con
stra
ints
and
the
desi
gn o
f in
terv
enti
ons.
Foo
d N
utr
Bul
l. 20
03;2
4:45
-82.
Edi
tion:
200
6 13
7

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Phy
sical
Activ
ity an
d Fu
nctio
n
PH
YS
ICA
L I
NA
CT
IVIT
Y (
NB
-2.1
)
De
fin
itio
n
Low
leve
l of
activ
ity/s
eden
tary
beh
avio
r to
the
exte
nt th
at it
red
uces
ene
rgy
expe
nditu
re a
nd im
pact
s he
alth
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Fina
ncia
l con
stra
ints
that
may
pre
vent
suf
fici
ent l
evel
of
activ
ity
Har
mfu
l bel
iefs
/atti
tude
s ab
out p
hysi
cal a
ctiv
ity
Inju
ry o
r lif
esty
le c
hang
e th
at r
educ
es p
hysi
cal a
ctiv
ity o
r ac
tiviti
es o
f da
ily li
ving
Lac
k of
pri
or e
xpos
ure
for
need
for
phy
sica
l act
ivity
or
how
to in
corp
orat
e ex
erci
se, e
.g.,
phys
ical
dis
abili
ty, a
rthr
itis
Lac
k of
rol
e m
odel
s, e
.g.,
for
child
ren
Lac
k of
soc
ial s
uppo
rt a
nd/o
r en
viro
nmen
tal s
pace
or
equi
pmen
t
Lac
k of
saf
e en
viro
nmen
t for
phy
sica
l act
ivity
Lac
k of
val
ue f
or b
ehav
ior
chan
ge o
r co
mpe
ting
valu
es
Tim
e co
nstr
aint
s
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Edi
tion:
200
6 13
8

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Phy
sical
Activ
ity an
d Fu
nctio
n
PH
YS
ICA
L I
NA
CT
IVIT
Y (
NB
-2.1
)F
ood/
Nut
ritio
n H
isto
ry
Rep
orts
or
obse
rvat
ions
of:
Infr
eque
nt, l
ow d
urat
ion
and/
or lo
w in
tens
ity p
hysi
cal a
ctiv
ity
Lar
ge a
mou
nts
of s
eden
tary
act
iviti
es e
.g. T
V w
atch
ing,
rea
ding
, com
pute
r us
e in
bot
h le
isur
e an
d w
ork/
scho
ol
Bar
rier
s to
phy
sica
l act
ivity
, e.g
., tim
e co
nstr
aint
s, a
vaila
bilit
y of
a s
afe
envi
ronm
ent f
or e
xerc
ise
Clie
nt H
isto
ry
Low
car
dio-
resp
irat
ory
fitn
ess
and/
or
low
mus
cle
stre
ngth
Med
ical
dia
gnos
es th
at m
ay b
e as
soci
ated
with
or
resu
lt in
dec
reas
ed a
ctiv
ity, e
.g.,
arth
ritis
, chr
onic
fat
igue
syn
drom
e,
mor
bid
obes
ity, k
nee
surg
ery
Med
icat
ions
that
cau
se s
omno
lenc
e an
d de
crea
sed
cogn
ition
Psyc
holo
gica
l dia
gnos
is, e
.g.,
depr
essi
on, a
nxie
ty d
isor
ders
Refe
ren
ces:
1.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Wei
ght m
anag
emen
t. J
Am
Die
t Ass
oc. 2
002;
102:
1145
-115
5.
2.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Tot
al d
iet a
ppro
ach
to c
omm
unic
atin
g fo
od a
nd n
utri
tion
info
rmat
ion.
J A
m D
iet A
ssoc
200
2;10
2:10
0-10
8.
3.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
The
rol
e of
die
tetic
s pr
ofes
sion
als
in h
ealth
pro
mot
ion
and
dise
ase
prev
entio
n. J
Am
Die
t Ass
oc. 2
002;
102:
1680
-168
7.
Edi
tion:
200
6 13
9

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Phy
sical
Activ
ity an
d Fu
nctio
n
EX
CE
SS
IVE
EX
ER
CIS
E (
NB
-2.2
)
De
fin
itio
n
An
amou
nt o
f ex
erci
se th
at e
xcee
ds th
at w
hich
is n
eces
sary
to im
prov
e he
alth
and
/or
athl
etic
per
form
ance
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Dis
orde
red
eatin
g
Irra
tiona
l bel
iefs
/atti
tude
s ab
out f
ood,
nut
ritio
n, a
nd f
itnes
s
“Add
ictiv
e” b
ehav
iors
/per
sona
lity
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a E
leva
ted
liver
enz
ymes
, e.g
., L
DH
, SG
OT
Alte
red
mic
ronu
trie
nt s
tatu
s, e
.g.,
decr
ease
d se
rum
fer
ritin
, zin
c, a
nd I
GF-
bind
ing
prot
ein
Incr
ease
d he
mat
ocri
t
Supp
ress
ed im
mun
e fu
nctio
n
Poss
ibly
ele
vate
d co
rtis
ol le
vels
Ant
hrop
omet
ric
Mea
sure
men
ts
Wei
ght l
oss,
arr
este
d gr
owth
and
dev
elop
men
t, fa
ilure
to g
ain
wei
ght d
urin
g pe
riod
of
expe
cted
gro
wth
(re
late
d us
ually
to
diso
rder
ed e
atin
g)
Phy
sica
l Exa
m F
indi
ngs
Dep
lete
d ad
ipos
e an
d so
mat
ic p
rote
in s
tore
s (r
elat
ed u
sual
ly to
dis
orde
red
eatin
g)
Freq
uent
and
/or
prol
onge
d in
juri
es a
nd/o
r ill
ness
es
Chr
onic
fat
igue
Chr
onic
mus
cle
sore
ness
Edi
tion:
200
6 14
0

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Phy
sical
Activ
ity an
d Fu
nctio
n
EX
CE
SS
IVE
EX
ER
CIS
E (
NB
-2.2
)F
ood/
Nut
ritio
n H
isto
ry
Rep
orts
or
obse
rvat
ions
of:
Con
tinue
d/re
peat
ed h
igh
leve
ls o
f ex
erci
se e
xcee
ding
leve
ls n
eces
sary
to im
prov
e he
alth
and
/or
athl
etic
per
form
ance
Exe
rcis
e da
ily w
ithou
t res
t/reh
abili
tatio
n da
ys
Exe
rcis
e w
hile
inju
red/
sick
Fors
akin
g fa
mily
, job
, soc
ial r
espo
nsib
ilitie
s to
exe
rcis
e
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
anor
exia
ner
vosa
, bul
imia
ner
vosa
, bin
ge e
atin
g, e
atin
g di
sord
er
not o
ther
wis
e sp
ecif
ied,
am
enor
rhea
Evi
denc
e of
add
ictiv
e, o
bses
sive
, or
com
puls
ive
tend
enci
es
Re
fere
nc
e:
1.
Ais
sa-B
enha
ddad
A, B
ouix
D, K
hale
d S,
Mic
alle
f JP
, Mer
cier
J, B
ring
er J
, Bru
n JF
. Ear
ly h
emor
heol
ogic
asp
ects
of
over
trai
ning
in e
lite
athl
etes
. Cli
n H
emor
heol
Mic
roci
rc. 1
999;
20:1
17-1
25.
2.
Am
eric
an P
sych
iatr
ic A
ssoc
iatio
n. D
iagn
osti
c an
d St
atis
tica
l Man
ual o
f Men
tal D
isor
ders
. 4th
Ed.
Was
hing
ton,
DC
. Am
eric
an P
sych
iatr
ic A
ssoc
iatio
n.
3.
Dav
is C
, Bre
wer
H, R
atus
ny D
. Beh
avio
ral f
requ
ency
and
psy
chol
ogic
al c
omm
itm
ent:
nece
ssar
y co
ncep
ts in
the
stud
y of
exc
essi
ve e
xerc
isin
g. J
Beh
av M
ed. 1
993;
16:6
11-6
28
4.
Dav
is C
, Cla
ridg
e G
. The
eat
ing
diso
rder
as
addi
ctio
n: a
psy
chob
iolo
gica
l per
spec
tive.
Add
ict B
ehav
. 199
8;23
:463
-475
. 5.
D
avis
C, K
enne
dy S
H, R
avel
ski E
, Dio
nne
M. T
he r
ole
of p
hysi
cal a
ctiv
ity in
the
deve
lopm
ent a
nd m
aint
enan
ce o
f ea
ting
diso
rder
s. P
sych
ol M
ed. 1
994;
24:9
57-9
67.
6.
Kle
in D
A, B
enne
tt A
S, S
cheb
enda
ch J
, Fol
tin R
W, D
evlin
MJ,
Wal
sh B
T. E
xerc
ise
“add
ictio
n” in
ano
rexi
a ne
rvos
a: m
odel
dev
elop
men
t and
pilo
t dat
a. C
NS
Spec
tr. 2
004;
9:53
1-53
7.
7.
Lak
ier-
Sm
ith L
. Ove
rtra
inin
g, e
xces
sive
exe
rcis
e, a
nd a
ltere
d im
mun
ity: t
his
a he
lper
-1 v
s he
lper
-2 ly
mph
ocyt
e re
spon
se?
Spor
ts M
ed. 2
003;
33:3
47-3
64.
8.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Nut
ritio
n in
terv
entio
n in
the
trea
tmen
t of
anor
exia
ner
vosa
, bul
imia
ner
vosa
, and
eat
ing
diso
rder
not
oth
erw
ise
spec
ifie
d (E
DN
OS
). J
Am
Die
t Ass
oc.
2001
;101
:810
-819
. 9.
Sh
epha
rd R
J, S
hek
PN. A
cute
and
chr
onic
ove
r-ex
ertio
n: d
o de
pres
sed
imm
une
resp
onse
s pr
ovid
e us
eful
mar
kers
? In
t J S
port
s M
ed. 1
998;
19:1
59-1
71.
10.
Smith
LL
. Tis
sue
trau
ma:
the
unde
rlyi
ng c
ause
of
over
trai
ning
syn
drom
e? J
Str
engt
h C
ond
Res
. 200
4;18
:185
-93.
11
. U
rhau
sen
A, K
inde
rman
n W
. Dia
gnos
is o
f ov
ertr
aini
ng: w
hat t
ools
do
we
have
. Spo
rts
Med
. 200
2;32
:95-
102.
Edi
tion:
200
6 14
1

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Phy
sical
Activ
ity an
d Fu
nctio
n
INA
BIL
ITY
OR
LA
CK
OF
DE
SIR
E T
O M
AN
AG
E S
EL
F C
AR
E (
NB
-2.3
)
De
fin
itio
n
Lac
k of
cap
acity
or
unw
illin
gnes
s to
impl
emen
t met
hods
to s
uppo
rt h
ealth
ful f
ood
and
nutr
ition
-rel
ated
beh
avio
r
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Food
and
nut
ritio
n-re
late
d kn
owle
dge
defi
cit
Lac
k of
car
etak
er o
r so
cial
sup
port
for
impl
emen
ting
chan
ges
Lac
k of
dev
elop
men
tal r
eadi
ness
to p
erfo
rm s
elf
man
agem
ent t
asks
, e.g
. ped
iatr
ics
Lac
k of
val
ue f
or b
ehav
ior
chan
ge o
r co
mpe
ting
valu
es
Perc
eptio
n th
at la
ck o
f re
sour
ces
(tim
e, f
inan
cial
, sup
port
per
sons
) pr
even
t sel
f ca
re
Cul
tura
l bel
iefs
and
pra
ctic
es
Lea
rnin
g di
sabi
lity,
neu
rolo
gica
l or
sens
ory
impa
irm
ent
Prio
r ex
posu
re to
inco
mpa
tible
info
rmat
ion
Not
rea
dy f
or d
iet/l
ifes
tyle
cha
nge
Unw
illin
g or
uni
nter
este
d in
lear
ning
/app
lyin
g in
form
atio
n
No
self
man
agem
ent t
ools
or
deci
sion
gui
des
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Edi
tion:
200
6 14
2

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Phy
sical
Activ
ity an
d Fu
nctio
n
INA
BIL
ITY
OR
LA
CK
OF
DE
SIR
E T
O M
AN
AG
E S
EL
F C
AR
E (
NB
-2.3
)F
ood/
Nut
ritio
n H
isto
ry
Rep
orts
or
obse
rvat
ions
of:
Inab
ility
to in
terp
ret d
ata
or s
elf
man
agem
ent t
ools
Em
barr
assm
ent o
r an
ger
rega
rdin
g ne
ed f
or s
elf-
mon
itori
ng
Unc
erta
inty
reg
ardi
ng c
hang
es c
ould
/sho
uld
be m
ade
in r
espo
nse
to d
ata
in s
elf
mon
itori
ng r
ecor
ds
Clie
nt H
isto
ry
Dia
gnos
es th
at a
re a
ssoc
iate
d w
ith s
elf
man
agem
ent,
e.g.
, dia
bete
s m
ellit
us, o
besi
ty, c
ardi
ovas
cula
r di
seas
e, r
enal
or
liver
di
seas
e
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
cogn
itive
or
emot
iona
l im
pair
men
t
New
med
ical
dia
gnos
is o
r ch
ange
in e
xist
ing
diag
nosi
s or
con
ditio
n
Refe
ren
ces:
1.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Pro
vidi
ng n
utri
tion
serv
ices
for
infa
nts,
chi
ldre
n, a
nd a
dults
with
dev
elop
men
tal d
isab
ilitie
s an
d sp
ecia
l hea
lth c
are
need
s. J
Am
Die
t Ass
oc.
2004
;104
:97-
107.
2.
C
raw
ford
S.
Prom
otin
g di
etar
y ch
ange
. C
an J
Car
diol
. 199
5;11
(sup
pl A
):14
A-1
5A.
3.
Falk
LW
, Bis
ogni
CA
, Sob
al J
. Die
t cha
nge
proc
esse
s of
par
ticip
ants
in a
n in
tens
ive
hear
t pro
gram
.J N
utr
Edu
. 200
0;32
:240
-250
. 4.
G
lasg
ow R
E, H
amps
on S
E, S
tryc
ker
LA
, Rug
gier
o L
. Per
sona
l-m
odel
bel
iefs
and
soc
ial-
envi
ronm
enta
l bar
rier
s re
late
d to
dia
bete
s se
lf-m
anag
emen
t.D
iabe
tes
Car
e. 1
997;
20:5
56-5
61.
5.
Kee
nan
DP,
Abu
Sabh
a R
, Sig
man
-Gra
nt M
, Ach
terb
erg
C, R
uffi
ng J
. Fac
tors
per
ceiv
ed to
infl
uenc
e di
etar
y fa
t red
uctio
n be
havi
ors.
J N
utr
Edu
.199
9;31
:134
-144
. 6.
K
uman
yika
SK
, Van
Hor
n L
, Bow
en D
, Per
ri M
G, R
olls
BJ,
Cza
jkow
ski S
M, S
chro
n E
. M
aint
enan
ce o
f di
etar
y be
havi
or c
hang
e. H
ealt
h P
sych
ol. 2
000;
19(1
sup
pl):
S42-
S56.
7.
Sp
orny
, Lor
a A
,Con
tent
o, I
sobe
l R.S
tage
s of
cha
nge
in d
ieta
ry f
at r
educ
tion:
Soc
ial p
sych
olog
ical
cor
rela
tes.
J N
utr
Edu
. 199
5;27
:191
.
Edi
tion:
200
6 14
3

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Phy
sical
Activ
ity an
d Fu
nctio
n
IMP
AIR
ED
AB
ILIT
Y T
O P
RE
PA
RE
FO
OD
S/M
EA
LS
(N
B-2
.4)
De
fin
itio
n
Cog
nitiv
e or
phy
sica
l im
pair
men
t tha
t pre
vent
s pr
epar
atio
n of
foo
ds/m
eals
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Lea
rnin
g di
sabi
lity,
neu
rolo
gica
l or
sens
ory
impa
irm
ent
Los
s of
men
tal o
r co
gniti
ve a
bilit
y, e
.g.,
dem
entia
Phys
ical
dis
abili
ty
Hig
h le
vel o
f fa
tigue
or
othe
r si
de e
ffec
t of
ther
apy
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Foo
d/N
utri
tion
His
tory
O
bser
vatio
ns o
r re
port
s of
:
Dec
reas
ed o
vera
ll in
take
Exc
essi
ve c
onsu
mpt
ion
of c
onve
nien
ce f
oods
, pre
-pre
pare
d m
eals
, and
foo
ds p
repa
red
away
fro
m h
ome
resu
lting
in a
n in
abili
ty to
adh
ere
to n
utri
tion
pres
crip
tion
Unc
erta
inty
reg
ardi
ng a
ppro
pria
te f
oods
to p
repa
re b
ased
upo
n nu
triti
on p
resc
ript
ion
Inab
ility
to p
urch
ase
and
tran
spor
t foo
ds to
one
’s h
ome
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
cogn
itive
impa
irm
ent,
cere
bral
pal
sy, p
arap
legi
a, s
ight
im
pair
men
t, ri
goro
us th
erap
y re
gim
en, r
ecen
t sur
gery
Edi
tion:
200
6 14
4

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Phy
sical
Activ
ity an
d Fu
nctio
n
IMP
AIR
ED
AB
ILIT
Y T
O P
RE
PA
RE
FO
OD
S/M
EA
LS
(N
B-2
.4)
Refe
ren
ces:
1.
And
ren
E, G
rim
by G
. Act
ivity
lim
itatio
ns in
per
sona
l, do
mes
tic a
nd v
ocat
iona
l tas
ks: a
stu
dy o
f ad
ults
with
inbo
rn a
nd e
arly
acq
uire
d m
obili
ty d
isor
ders
. Dis
abil
Reh
abil.
200
4;26
:262
-271
.
2.
And
ren
E, G
rim
by G
. D
epen
denc
e in
dai
ly a
ctiv
ities
and
life
sat
isfa
ctio
n in
adu
lt su
bjec
ts w
ith c
ereb
ral p
alsy
or
spin
a bi
fida
: a f
ollo
w-u
p st
udy.
Dis
abil
Reh
abil.
200
4;26
:528
-536
. 3.
Fo
rtin
S, G
odbo
ut L
, Bra
un C
M. C
ogni
tive
stru
ctur
e of
exe
cutiv
e de
fici
ts in
fro
ntal
ly le
sion
ed h
ead
trau
ma
patie
nts
perf
orm
ing
activ
ities
of
daily
livi
ng. C
orte
x. 2
003;
39:2
73-2
91.
4.
God
bout
L, D
ouce
t C, F
iola
M. T
he s
crip
ting
of a
ctiv
ities
of
daily
livi
ng in
nor
mal
agi
ng: a
ntic
ipat
ion
and
shif
ting
defi
cits
with
pre
serv
atio
n of
seq
uenc
ing.
Bra
in C
ogn.
200
0;43
:220
-224
.
5.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Pro
vidi
ng n
utri
tion
serv
ices
for
infa
nts,
chi
ldre
n, a
nd a
dults
with
dev
elop
men
tal d
isab
ilitie
s an
d sp
ecia
l hea
lth c
are
need
s. J
Am
Die
t Ass
oc.
2004
;104
:97-
107.
6.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: D
omes
tic f
ood
and
nutr
ition
sec
urity
. J A
m D
iet A
ssoc
. 200
2;10
2:18
40-1
847.
7.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: A
ddre
ssin
g w
orld
hun
ger,
mal
nutr
ition
, and
foo
d in
secu
rity
. J A
m D
iet A
ssoc
. 200
3;10
3:10
46-1
057.
8.
Sand
stro
m K
, Alin
der
J, O
berg
B.
Des
crip
tions
of
func
tioni
ng a
nd h
ealth
and
rel
atio
ns to
a g
ross
mot
or c
lass
ific
atio
n in
adu
lts w
ith c
ereb
ral p
alsy
. Dis
abil
Reh
abil.
200
4;26
:102
3-10
31.
Edi
tion:
200
6 14
5
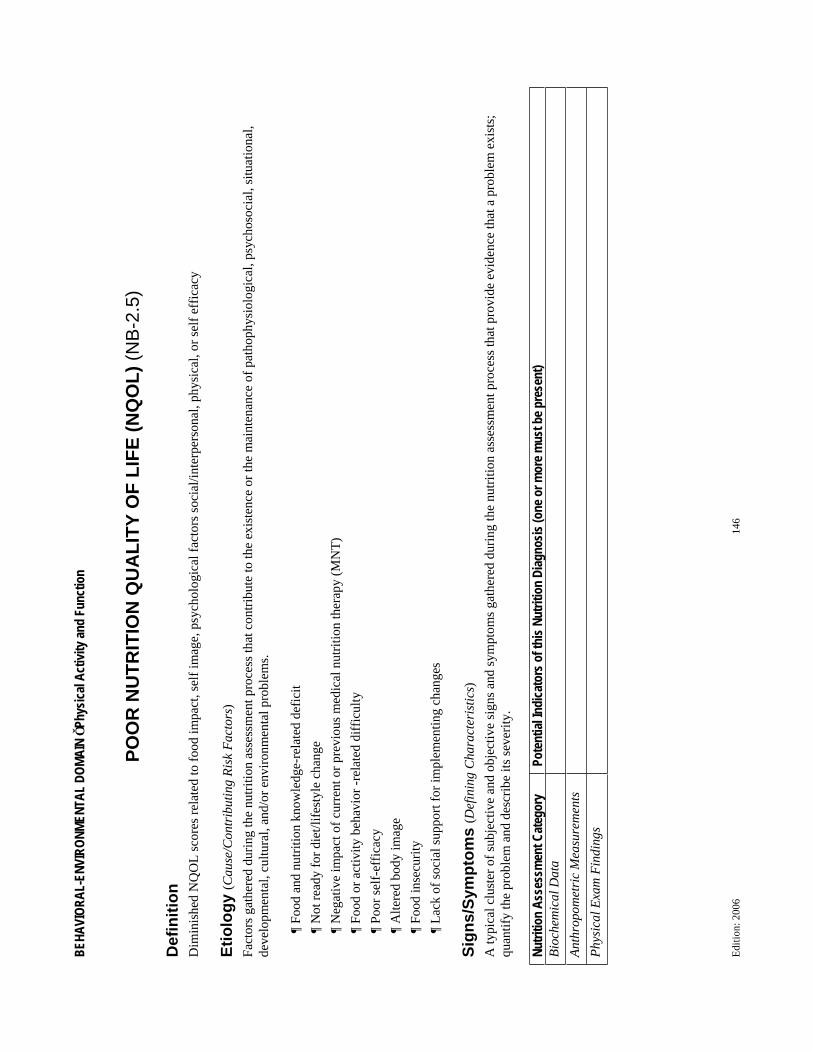
BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Phy
sical
Activ
ity an
d Fu
nctio
n
PO
OR
NU
TR
ITIO
N Q
UA
LIT
Y O
F L
IFE
(N
QO
L)
(NB
-2.5
)
De
fin
itio
n
Dim
inis
hed
NQ
OL
sco
res
rela
ted
to f
ood
impa
ct, s
elf
imag
e, p
sych
olog
ical
fac
tors
soc
ial/i
nter
pers
onal
, phy
sica
l, or
sel
f ef
fica
cy
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Food
and
nut
ritio
n kn
owle
dge-
rela
ted
defi
cit
Not
rea
dy f
or d
iet/l
ifes
tyle
cha
nge
Neg
ativ
e im
pact
of
curr
ent o
r pr
evio
us m
edic
al n
utri
tion
ther
apy
(MN
T)
Food
or
activ
ity b
ehav
ior
-rel
ated
dif
ficu
lty
Poor
sel
f-ef
fica
cy
Alte
red
body
imag
e
Food
inse
curi
ty
Lac
k of
soc
ial s
uppo
rt f
or im
plem
entin
g ch
ange
s
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Edi
tion:
200
6 14
6

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Phy
sical
Activ
ity an
d Fu
nctio
n
PO
OR
NU
TR
ITIO
N Q
UA
LIT
Y O
F L
IFE
(N
QO
L)
(NB
-2.5
)F
ood/
Nut
ritio
n H
isto
ry
Rep
orts
or
obse
rvat
ions
of:
Unf
avor
able
NQ
OL
rat
ing
Frus
trat
ion
or d
issa
tisfa
ctio
n w
ith M
NT
rec
omm
enda
tions
Inac
cura
te o
r in
com
plet
e in
form
atio
n re
late
d to
MN
T r
ecom
men
datio
ns
Inab
ility
to c
hang
e fo
od o
r ac
tivity
rel
ated
beh
avio
r
Con
cern
s ab
out p
revi
ous
atte
mpt
s to
lear
n in
form
atio
n
Unw
illin
gnes
s or
dis
inte
rest
in le
arni
ng in
form
atio
n
Clie
nt H
isto
ry
New
med
ical
dia
gnos
is o
r ch
ange
in e
xist
ing
diag
nosi
s or
con
ditio
n
Rec
ent o
ther
life
styl
e or
life
cha
nges
, e.g
., qu
it sm
okin
g, in
itiat
ed e
xerc
ise,
wor
k ch
ange
, hom
e re
loca
tion
Refe
ren
ces:
1.
Bar
r JT
, Sch
umac
her
GE
. The
nee
d fo
r a
nutr
ition
-rel
ated
qua
lity-
of-l
ife
mea
sure
. J A
m D
iet A
ssoc
. 200
3;10
3:17
7-18
0.
2.
Bar
r JT
, Sch
umac
her
GE
. Usi
ng f
ocus
gro
ups
to d
eter
min
e w
hat c
onst
itute
s qu
ality
of
life
in c
lient
s re
ceiv
ing
med
ical
nut
ritio
n th
erap
y: F
irst
ste
ps in
the
deve
lopm
ent o
f a
nutr
ition
qua
lity-
of-l
ife
surv
ey. J
Am
Die
t Ass
oc. 2
003;
103:
844-
851.
Edi
tion:
200
6 14
7
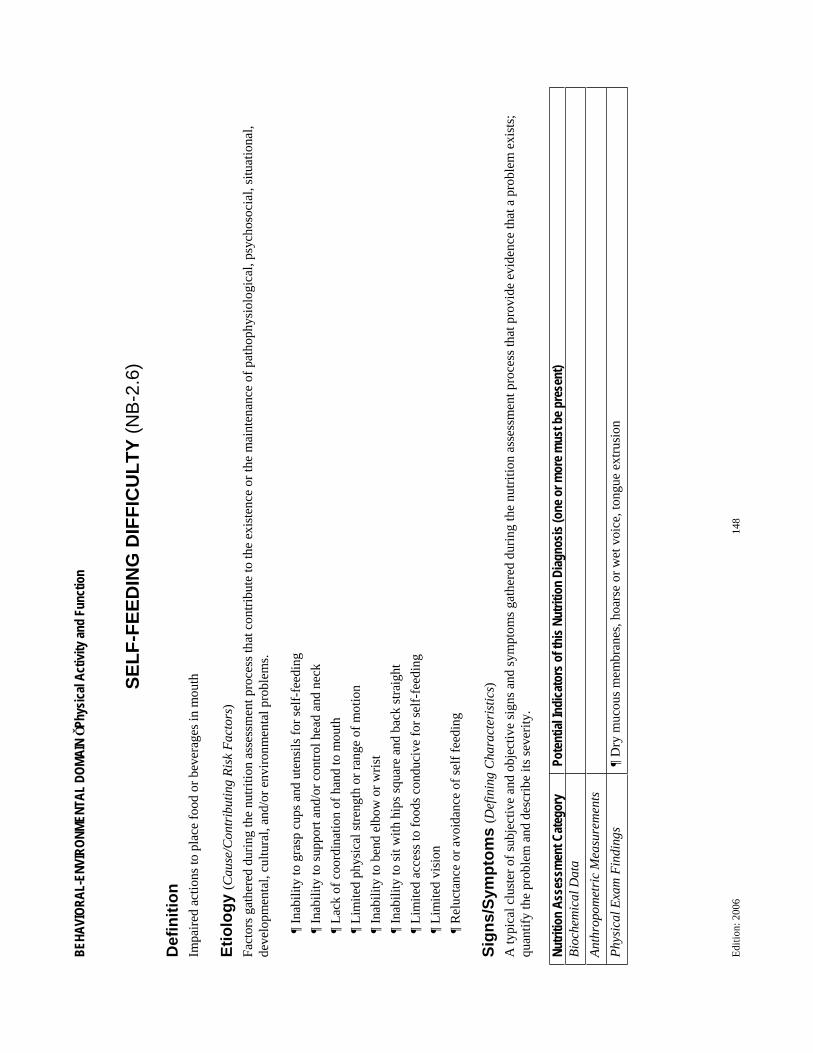
BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Phy
sical
Activ
ity an
d Fu
nctio
n
SE
LF
-FE
ED
ING
DIF
FIC
UL
TY
(N
B-2
.6)
De
fin
itio
n
Impa
ired
act
ions
to p
lace
foo
d or
bev
erag
es in
mou
th
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Inab
ility
to g
rasp
cup
s an
d ut
ensi
ls f
or s
elf-
feed
ing
Inab
ility
to s
uppo
rt a
nd/o
r co
ntro
l hea
d an
d ne
ck
Lac
k of
coo
rdin
atio
n of
han
d to
mou
th
Lim
ited
phys
ical
str
engt
h or
ran
ge o
f m
otio
n
Inab
ility
to b
end
elbo
w o
r w
rist
Inab
ility
to s
it w
ith h
ips
squa
re a
nd b
ack
stra
ight
Lim
ited
acce
ss to
foo
ds c
ondu
cive
for
sel
f-fe
edin
g
Lim
ited
visi
on
Rel
ucta
nce
or a
void
ance
of
self
fee
ding
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
m F
indi
ngs
Dry
muc
ous
mem
bran
es, h
oars
e or
wet
voi
ce, t
ongu
e ex
trus
ion
Edi
tion:
200
6 14
8

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Phy
sical
Activ
ity an
d Fu
nctio
n
SE
LF
-FE
ED
ING
DIF
FIC
UL
TY
(N
B-2
.6)
Foo
d/N
utri
tion
His
tory
R
epor
ts o
r ob
serv
atio
ns o
f:
Bei
ng p
rovi
ded
with
foo
ds th
at m
ay n
ot b
e co
nduc
ive
to s
elf-
feed
ing,
e.g
., pe
as, b
roth
-typ
e so
ups
Poor
lip
clos
ure,
dro
olin
g
Dro
ppin
g of
cup
s, u
tens
ils
Em
otio
nal d
istr
ess,
anx
iety
, or
frus
trat
ion
surr
ound
ing
mea
ltim
es
Failu
re to
rec
ogni
ze f
oods
Forg
ets
to e
at
Inap
prop
riat
e us
e of
foo
d
Ref
usal
to e
at o
r ch
ew
Dro
ppin
g of
foo
d fr
om u
tens
il (s
plas
hing
and
spi
lling
of
food
) on
rep
eate
d at
tem
pts
to f
eed
Ute
nsil
bitin
g
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
neur
olog
ical
dis
orde
rs, P
arki
nson
’s, A
lzhe
imer
’s, T
ardi
ve
dysk
ines
ia, m
ultip
le s
cler
osis
, str
oke,
par
alys
is, d
evel
opm
enta
l del
ay
Phys
ical
lim
itatio
ns, e
.g.,
frac
ture
d ar
ms,
trac
tion,
con
trac
ture
s
Surg
ery
requ
irin
g re
cum
bent
pos
ition
Dem
entia
/org
anic
bra
in s
yndr
ome
Dys
phag
ia
Wei
ght l
oss
Shor
tnes
s of
bre
ath
Tre
mor
s
Refe
ren
ces:
1.
Con
sulta
nt D
ietit
ians
in H
ealth
care
Fac
ilitie
s. D
inin
g Sk
ills
Supp
lem
ent:
Pra
ctic
al I
nter
vent
ions
for
Car
egiv
ers
of E
atin
g D
isab
led
Old
er A
dults
. Pen
saco
la, F
L: A
mer
ican
Die
tetic
Ass
ocia
tion,
19
92.
2.
Mor
ley
JE. A
nore
xia
of a
ging
: phy
siol
ogic
al a
nd p
atho
logi
c. A
m J
Clin
Nut
r. 1
997;
66:
760-
773.
3.
Po
sitio
n of
the
Am
eric
an D
iete
tic A
ssoc
iatio
n: P
rovi
ding
nut
ritio
n se
rvic
es f
or in
fant
s, c
hild
ren,
and
adu
lts w
ith d
evel
opm
enta
l dis
abili
ties
and
spec
ial h
ealth
car
e ne
eds.
J A
m D
iet A
ssoc
.20
04;1
04:9
7-10
7.
4.
Sand
man
P, N
orbe
rg A
, Ado
lfss
on R
, Eri
ksso
n S,
Nys
trom
L. P
reva
lenc
e an
d ch
arac
teri
stic
s of
per
sons
with
dep
ende
ncy
on f
eedi
ng a
t ins
titut
ions
. Sca
nd J
Car
ing
Sci.
1990
;4:1
21-1
27.
5.
Sieb
ens
H, T
rupe
E, S
iebe
ns A
, Coo
ke F
, Ans
hen
S, H
anau
er R
, Ost
er G
. Cor
rela
tes
and
cons
eque
nces
of
feed
ing
depe
nden
cy.
J A
m G
eria
tr S
oc. 1
986;
34:1
92-1
98.
6.
Vel
las
B, F
itten
LJ
eds.
Res
earc
h an
d P
ract
ice
in A
lzhe
imer
’s D
isea
se. N
ew Y
ork,
NY
: Spr
inge
r Pu
blis
hing
Com
pany
, 199
8.
Edi
tion:
200
6 14
9

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Foo
d Sa
fety
and
Acce
ss
INT
AK
E O
F U
NS
AF
E F
OO
D (
NB
-3.1
)
De
fin
itio
n
Inta
ke o
f fo
od a
nd/o
r fl
uids
inte
ntio
nally
or
unin
tent
iona
lly c
onta
min
ated
with
toxi
ns, p
oiso
nous
pro
duct
s, in
fect
ious
age
nts,
mic
robi
al a
gent
s, a
dditi
ves,
al
lerg
ens,
and
/or
agen
ts o
f bi
oter
rori
sm
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Lac
k of
kno
wle
dge
abou
t pot
entia
lly u
nsaf
e fo
od
Lac
k of
kno
wle
dge
abou
t pro
per
food
/fee
ding
, (in
fant
and
ent
eral
for
mul
a, b
reas
t milk
) st
orag
e an
d pr
epar
atio
n
Exp
osur
e to
con
tam
inat
ed w
ater
or
food
, e.g
., co
mm
unity
out
brea
k of
illn
ess
docu
men
ted
by s
urve
illan
ce a
nd/o
r re
spon
se a
genc
y
Men
tal i
llnes
s, c
onfu
sion
or
alte
red
awar
enes
s
Inad
equa
te f
ood
stor
age
equi
pmen
t/fac
ilitie
s, e
.g.,
refr
iger
ator
Inad
equa
te s
afe
food
sup
ply,
e.g
., in
adeq
uate
mar
kets
with
saf
e, u
ncon
tam
inat
ed f
ood
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a Po
sitiv
e st
ool c
ultu
re f
or in
fect
ious
cau
ses,
suc
h as
list
eria
, sal
mon
ella
, hep
atiti
s A
, E. c
oli,
cycl
ospo
ra
Tox
icol
ogy
repo
rts
for
drug
s, m
edic
inal
s, p
oiso
ns in
blo
od o
r fo
od s
ampl
es
Ant
hrop
omet
ric
Mea
sure
men
ts
Phy
sica
l Exa
min
atio
n F
indi
ngs
Evi
denc
e of
deh
ydra
tion,
e.g
., dr
y m
ucou
s m
embr
anes
, dam
aged
tiss
ues
Edi
tion:
200
6 15
0

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Foo
d Sa
fety
and
Acce
ss
INT
AK
E O
F U
NS
AF
E F
OO
D (
NB
-3.1
)F
ood/
Nut
ritio
n H
isto
ry
Obs
erva
tions
/rep
orts
of
inta
ke o
f po
tent
ial u
nsaf
e fo
ods
e.g.
, mer
cury
con
tent
of
fish
, non
-foo
d ite
ms
(pre
gnan
t and
lact
atin
g w
omen
)
e.g.
, raw
egg
s, u
npas
teur
ized
milk
pro
duct
s, s
oft c
hees
es, u
nder
cook
ed m
eats
(in
fant
s, c
hild
ren,
imm
unoc
ompr
omis
ed
pers
ons,
pre
gnan
t and
lact
atin
g w
omen
, and
eld
erly
)
e.g.
, wild
pla
nts,
ber
ries
, mus
hroo
ms
Obs
erva
tions
/ rep
orts
of
unsa
fe f
ood/
feed
ing
(ent
eral
and
infa
nt f
orm
ula,
bre
ast m
ilk)
stor
age
and
prep
arat
ion
prac
tices
Clie
nt H
isto
ry
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
food
bor
ne il
lnes
s, s
uch
as, b
acte
rial
, vir
al, a
nd p
aras
itic
infe
ctio
n, m
enta
l illn
ess,
dem
entia
Pois
onin
g by
dru
gs, m
edic
inal
s, a
nd b
iolo
gica
l sub
stan
ces
Pois
onin
g fr
om p
oiso
nous
foo
d st
uffs
and
poi
sono
us p
lant
s
Dia
rrhe
a, c
ram
ping
, blo
atin
g, f
ever
, nau
sea,
vom
iting
, vis
ion
prob
lem
s, c
hills
, diz
zine
ss, h
eada
che
Car
diac
, neu
rolo
gic,
res
pira
tory
cha
nges
Refe
ren
ces:
1.
Cen
ters
for
Dis
ease
Con
trol
& P
reve
ntio
n. D
iagn
osis
and
Man
agem
ent o
f Fo
odbo
rne
Illn
ess:
A p
rim
er f
or P
hysi
cian
s pa
ge.
Ava
ilab
le a
t: w
ww
.cdc
.gov
/mm
wr/
prev
iew
/mm
wrh
tml/r
r530
4a1.
htm
.A
cces
sed
July
2, 2
004.
2.
Fo
od S
afet
y an
d In
spec
tion
Serv
ice.
The
Fig
ht B
AC
Sur
vey
Too
l and
Dat
a E
ntry
Too
l pag
e. A
vaila
ble
at: w
ww
.fsi
s.us
da.g
ov/O
A/f
ses/
bac_
data
tool
.htm
. Acc
esse
d Ju
ly 2
, 200
4.
3.
Ger
ald
BL
, Per
kin
JE. F
ood
and
wat
er s
afet
y. J
Am
Die
t Ass
oc. 2
003;
103:
1203
-121
8.
4.
Part
ners
hip
for
Food
Saf
ety
Edu
catio
n. F
our
step
s pa
ge.
Ava
ilabl
e at
: ht
tp://
ww
w.f
ight
bac.
org/
four
step
s.cf
m?s
ectio
n=4.
Acc
esse
d Ju
ly 2
, 200
4.
Edi
tion:
200
6 15
1

BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Foo
d Sa
fety
and
Acce
ss
LIM
ITE
D A
CC
ES
S T
O F
OO
D (
NB
-3.2
)
De
fin
itio
n
Dim
inis
hed
abili
ty to
acq
uire
foo
d fr
om s
ourc
es (
e.g.
sho
ppin
g, g
arde
ning
, mea
l del
iver
y), d
ue to
fin
anci
al c
onst
rain
ts, p
hysi
cal i
mpa
irm
ent,
care
give
r su
ppor
t, or
un
safe
livi
ng c
ondi
tions
(e.
g. c
rim
e hi
nder
s tr
avel
to g
roce
ry s
tore
). L
imita
tion
to f
ood
beca
use
of c
once
rns
abou
t wei
ght o
r ag
ing.
Eti
olo
gy (
Cau
se/C
ontr
ibut
ing
Ris
k F
acto
rs)
Fact
ors
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at c
ontr
ibut
e to
the
exis
tenc
e or
the
mai
nten
ance
of
path
ophy
siol
ogic
al, p
sych
osoc
ial,
situ
atio
nal,
deve
lopm
enta
l, cu
ltura
l, an
d/or
env
iron
men
tal p
robl
ems.
Car
egiv
er in
tent
iona
lly o
r un
inte
ntio
nally
not
pro
vidi
ng a
cces
s to
foo
d, e
.g.,
unm
et n
eeds
for
foo
d or
eat
ing
assi
stan
ce, a
buse
/neg
lect
Com
mun
ity a
nd g
eogr
aphi
cal c
onst
rain
ts f
or s
hopp
ing
and
tran
spor
tatio
n
Lac
k of
fin
anci
al r
esou
rces
or
lack
of
acce
ss to
fin
anci
al r
esou
rces
to p
urch
ase
suff
icie
nt f
ood
Lim
ited
or a
bsen
t com
mun
ity s
uppl
emen
tal f
ood
prog
ram
s, e
.g.,
food
pan
try,
she
lter
Failu
re to
par
ticip
ate
in f
ood
prog
ram
s su
ch a
s W
IC, N
atio
nal S
choo
l Lun
ch P
rogr
am, f
ood
stam
ps
Phys
ical
or
psyc
holo
gica
l lim
itatio
ns th
at d
imin
ish
abili
ty to
sho
p, e
.g. w
alki
ng, s
ight
, men
tal/e
mot
iona
l hea
lth
Sig
ns
/Sym
pto
ms
(D
efin
ing
Cha
ract
eris
tics)
A ty
pica
l clu
ster
of
subj
ectiv
e an
d ob
ject
ive
sign
s an
d sy
mpt
oms
gath
ered
dur
ing
the
nutr
ition
ass
essm
ent p
roce
ss th
at p
rovi
de e
vide
nce
that
a p
robl
em e
xist
s;
quan
tify
the
prob
lem
and
des
crib
e its
sev
erity
.
Nutri
tion
Asse
ssm
ent C
ateg
ory
Pote
ntial
Indi
cato
rs o
f thi
s Nut
ritio
n Di
agno
sis (o
ne o
r mor
e mus
t be p
rese
nt)
Bio
chem
ical
Dat
a In
dica
tors
of
mac
ronu
trie
nt o
r vi
tam
in/m
iner
al s
tatu
s as
indi
cate
d by
phy
sica
l fin
ding
s, f
ood/
nutr
ition
and
clie
nt h
isto
ry
Ant
hrop
omet
ric
Mea
sure
men
ts
Gro
wth
fai
lure
, bas
ed o
n N
atio
nal C
ente
r fo
r H
ealth
Sta
tistic
s (N
CH
S) g
row
th s
tand
ards
Und
erw
eigh
t (B
MI
<18
.5)
Phy
sica
l Exa
m F
indi
ngs
Find
ings
con
sist
ent w
ith v
itam
in/m
iner
al d
efic
ienc
y
Edi
tion:
200
6 15
2
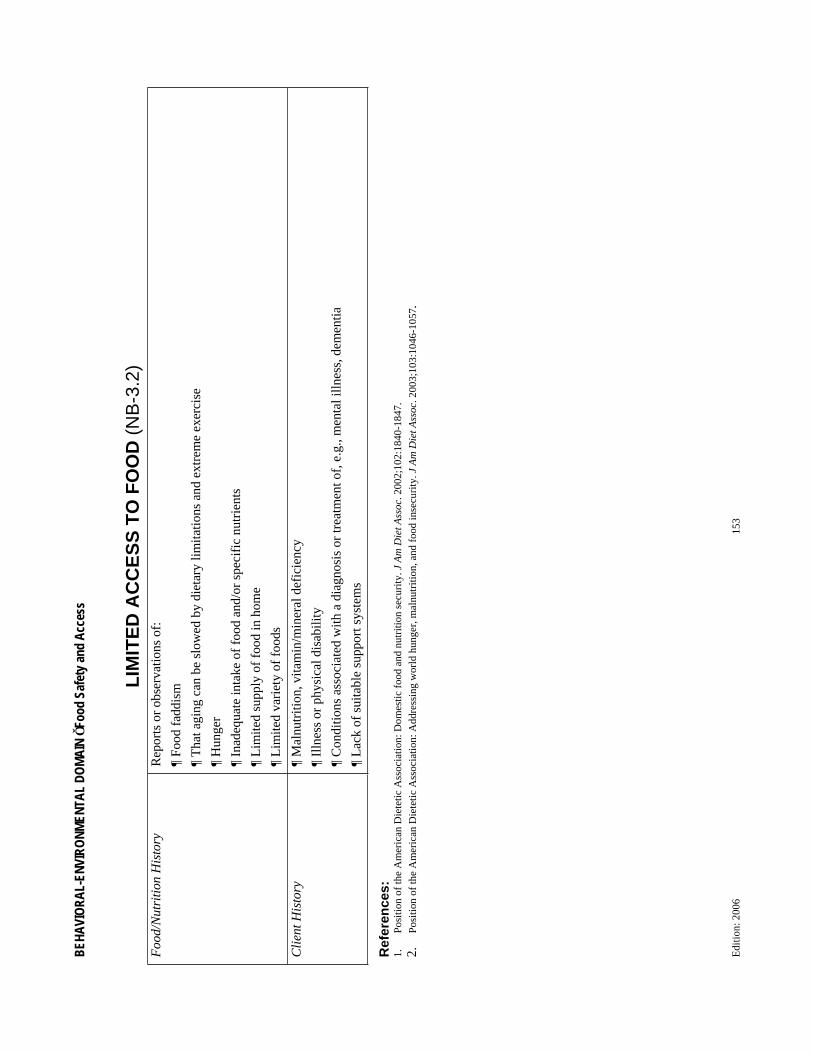
BEHA
VIOR
AL-E
NVIR
ONME
NTAL
DOM
AIN
Foo
d Sa
fety
and
Acce
ss
LIM
ITE
D A
CC
ES
S T
O F
OO
D (
NB
-3.2
)F
ood/
Nut
ritio
n H
isto
ry
Rep
orts
or
obse
rvat
ions
of:
Food
fad
dism
Tha
t agi
ng c
an b
e sl
owed
by
diet
ary
limita
tions
and
ext
rem
e ex
erci
se
Hun
ger
Inad
equa
te in
take
of
food
and
/or
spec
ific
nut
rien
ts
Lim
ited
supp
ly o
f fo
od in
hom
e
Lim
ited
vari
ety
of f
oods
Clie
nt H
isto
ry
Mal
nutr
ition
, vita
min
/min
eral
def
icie
ncy
Illn
ess
or p
hysi
cal d
isab
ility
Con
ditio
ns a
ssoc
iate
d w
ith a
dia
gnos
is o
r tr
eatm
ent o
f, e
.g.,
men
tal i
llnes
s, d
emen
tia
Lac
k of
sui
tabl
e su
ppor
t sys
tem
s
Refe
ren
ces:
1.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Dom
estic
foo
d an
d nu
triti
on s
ecur
ity. J
Am
Die
t Ass
oc. 2
002;
102:
1840
-184
7.
2.
Posi
tion
of th
e A
mer
ican
Die
tetic
Ass
ocia
tion:
Add
ress
ing
wor
ld h
unge
r, m
alnu
triti
on, a
nd f
ood
inse
curi
ty. J
Am
Die
t Ass
oc. 2
003;
103:
1046
-105
7.
Edi
tion:
200
6 15
3

SUBJECT: NUTRITION CONTROLLED VOCABULARY/TERMINOLOGY MAINTENANCE/REVIEW
AMERICAN DIETETIC ASSOCIATION 120 South Riverside Plaza Suite 2000 CHICAGO, ILLINOIS 60606-6995
Effective Date: April 2005 Revision Date: June 2006
Review Date: PURPOSE:This policy establishes the has established the process followed by the Nutrition Care Process/Standardized Language (NCP/SL) Committee to maintain a current Nutrition Care Process and list of nutrition controlled vocabulary terminology that document the Nutrition Care Process.
STRUCTURE:The NCP/SL Committee is a joint House of Delegates and Board of Directors Committee and provides semi-annual reports to both bodies.
PROCEDURES:The NCP/SL Committee accept proposals for modification or additions to the Nutrition Diagnostic Terminology as follows:
1. Any individual ADA member or Dietetic Practice Group can submit proposals for modification or additions by completing the attached two documents:
a. Proposed Nutrition Diagnostic Terminology Modification/Addition letter b. Reference worksheet for proposed modification/addition
2. The NCP/SL will review the submissions at their routine face-to-face meetings or teleconferences to establish the following:
a. Is the term already represented by an existing term? i. If so the new term can be added as a synonym for the existing term or
replace the existing term. ii. If not, then the term can be considered for addition to the list of terms as
long as it meets the need for describing elements of dietetic practice in the context of the nutrition care process.
b. Does the term overlap with an existing term, but add new elements? i. If yes, then the existing term can be modified to include the new elements
or the proposed term can be clarified to be distinctly different from the existing term through a dialogue with the proposal submitter.
ii. If no, then consider adding new term c. Is the term distinct and separate from all existing terms?
i. If yes, then ensure that the term is in the context of dietetic practice within the Nutrition Care Process and consider adding to list of terms.
ii. If no, then work with proposal submitter to discuss how to integrate into existing terms or create a separate term.
3. The NCP/SL will prepare a summary of comments and one representative of the NCPSL will confer with the proposal submitter after the initial discussion to answer questions and discuss the initial input from the NCP/SL Committee. If the proposal submitter is not satisfied with the direction proposed by the NCP/SL, then they will be invited to submit additional documentation and have time on the next teleconference/meeting agenda to personally present their concerns.
Edition: 2006 154

Edition: 2006 155
4. Changes or modifications accepted by the NCP/SL will be integrated into the list that is re-published on an annual basis.
STAFFING: Governance and Scientific Affairs and Research provide staff support for Research Committee functions.
Attachments 1. Template for Letter for submitting Proposal for Modifications to Nutrition Diagnostic
Terminology 2. Template for Letter for submitting Propposal for New Term for Nutrition Diagnostic
Terminology 3. Template for Reference Sheet to support modification/additions to Nutrition Diagnostic
Terminology 4. Sample Reference Sheet 5. Sample Case with PES statement

Edition: 2006 156
Attachment 1 to Nutrition Controlled Vocabulary/Terminology Maintenance Policy-Template for letter for proposing new term
Date
To: NCP/SL Committee Scientific Affairs and Research 120 South Riverside Plaza, Suite 2000 Chicago, IL 60606-6995 [email protected] and [email protected]
Subject: Proposed Addition to Nutrition Diagnostic Terminology
(1/We) would like to propose a new term, ____,_________________(Proposed term to add to the Nutrition Diagnostic Terminology list). The reason !/we believe that this term should be added is as follows: (insert concise rationale for change, may include brief example of when the situation arose that the current term was inadequately defined)
1. (insert first statement of rationale) 2. (Insert second statement of rationale, if applicable) 3. (Insert example of situation where this modification was needed)
Other terms which are similar with explanations of why they do not exactly match our new proposed term are as follows:
1. (Insert Number and Name) – (Insert 2-3 sentences to illustrate why the existing term does not meet your need)
2. (Insert Number and Name) – (Insert 2-3 sentences to illustrate why the existing term does not meet your need)
3. (Add as many as applicable)
Attached is the a reference sheet that includes the label, description, proposed domain and category, examples of etiologies and signs and symptoms and a case that illustrates when this term would be used and the corresponding PES statement that would be used in medical record documentation.
The point of contact for this proposal is ___________________________________ (insert name) who can be reached at ______( best contact telephone number0 and _______(e-mail address).
Thank you for considering our request
Signature block (Organizational unit if applicable)
Attachments 1. Reference Sheet 2. Case with PES statement

Edition: 2006 157
Attachment 2 to Nutrition Controlled Vocabulary/Terminology Maintenance Policy-Template for letter proposing modification of term
Date
To: NCP/SL Committee Scientific Affairs and Research 120 South Riverside Plaza, Suite 2000 Chicago, IL 60606-6995 [email protected] and [email protected]
Subject: Proposed Modification to existing term in Nutrition Diagnostic Terminology
(1/We) would like to propose a modification or the term, ____,, _________________(Number and Name from current Nutrition Diagnostic Terminology list). The reason !/we believe that this term should be modified is as follows: (insert concise rationale for change, may include brief example of when the situation arose that the current term was inadequately defined)
4. (insert first statement of rationale) 5. (Insert second statement of rationale, if applicable) 6. (Insert example of situation where this modification was needed)
Attached is the revised reference sheet that shows the changes highlighted or bolded for your consideration.
The point of contact for this proposal is ___________________________________ (insert name) who can be reached at ______( best contact telephone number0 and _______(e-mail address).
Thank you for considering our request
Signature block (Organizational unit if applicable)
Attachment Modified Reference Sheet for Term

Edition: 2006 158
Attachment 3 to Nutrition Controlled Vocabulary/Terminology Maintenance Policy -Template for Reference Sheet(Select CLINICAL/ FUNCTIONAL or BEHAVIORAL/ENVIRONMENTAL) DOMAIN (Select Category e.g. Functional Balance)
Nutrition Diagnostic Label (Leave number blank) (Insert 1-4 word label)
Definition of Nutrition Diagnostic Label (Insert 1 sentence or bullet that describe the intent of the label)
Etiology (Cause/Contributing Risk Factors) Factors gathered during the nutrition assessment process that contribute to the existence of or the maintenance of pathophysiological, psychosocial, situational, developmental, cultural, and/or environmental problems.
(Insert common etiologies for Nutrition Diagnostic Label)
Signs/Symptoms (Defining Characteristics) A typical cluster of subjective and objective signs and symptoms gathered during the nutrition assessment process that provide evidence that a problem exists; quantify the problem and describe its severity.
Nutrition Assessment Category Potential Indicators of this Nutrition Diagnosis (one or more must be present)
Biochemical Data (Insert as appropriate) Anthropometric Measurements (Insert as appropriate) Physical Exam Findings (Insert as appropriate) Food/Nutrition History (Insert as appropriate) Client History (Insert as appropriate) .

Edition: 2006 159
Attachment 3 to Nutrition Controlled Vocabulary/Terminology Maintenance Policy -Completed Reference SheetCLINICAL DOMAIN Functional Balance
Nutrition Diagnostic Label NC-1.1 Swallowing difficulty
Definition of Nutrition Diagnostic Label Impaired movement of food and liquid from the mouth to the stomach
Etiology (Cause/Contributing Risk Factors) Factors gathered during the nutrition assessment process that contribute to the existence of or the maintenance of pathophysiological, psychosocial, situational, developmental, cultural, and/or environmental problems.
Mechanical causes, e.g., inflammation, surgery, stricture, or oral, pharyngeal and esophageal tumors
Motor causes, e.g., neurological or muscular disorders, such as, cerebral palsy, stroke, multiple sclerosis, scleroderma, prematurity
Signs/Symptoms (Defining Characteristics) A typical cluster of subjective and objective signs and symptoms gathered during the nutrition assessment process that provide evidence that a problem exists; quantify the problem and describe its severity.
Nutrition Assessment Category Potential Indicators of this Nutrition Diagnosis (one or more must be present)
Biochemical Data Anthropometric Measurements Physical Exam Findings Evidence of dehydration, e.g., dry mucous membranes, poor
skin turgor Food/Nutrition History Observations or reports of :
Coughing, choking, prolonged chewing, pouching of food, regurgitation, facial expression changes during eating, prolonged feeding time, drooling, noisy wet upper airway sounds, feeling of “food getting stuck,” pain while swallowing
Decreased food intake Avoidance of foods Mealtime resistance
Client History Conditions associated with a diagnosis or treatment of dysphagia, achalasia
Radiological findings, e.g., abnormal swallowing studies Repeated upper respiratory infections and or pneumonia
.

2003 - 2005 Standardized Language Task Force and Terminology Expert Reviewers
Edition: 2006 160
Standardized Language Task Force
Chair Sylvia Escott-Stump, MA, RD, LDN Dietetic Programs Director East Carolina University 155 Rivers Building, Dept. NUHM Greenville, NC 27858 Task Force Member 2003-2005
Peter Beyer, MS, RD, LD Associate Professor University of Kansas Medical Center 7315 Rosewood Drive Prairie Village, KS 66208-2458Task Force Member 2003-2005
Christina Biesemeier MS, RD, LDN, FADA 313 Logans Circle Franklin TN 37067-1363 Task Force Member 2003-2005
Pam Charney, MS, RD, CNSD 10772 Country Walk Court Dayton, OH 45458-4752Task Force Member 2003-2005
Marion Franz, MS, RD, CDE 6635 Limerick Dr. Minneapolis, MN 55439-1260 Task Force Member 2003-2005
Karen Lacey, MS, RD, CD 500 Saint Mary’s Blvd Green Bay, WI 54301-2610 Task Force Member 2003-2005
Kathleen Niedert, MBA, RD, LD, FADA PO Box 843 110 Ardis Street Hudson, IA 50643-0843 Task Force Member 2003-2005
Mary Jane Oakland, PhD, RD, LD, FADA 1612 Truman Drive Ames, IA 50010-4344 Task Force Member 2003-2005
Patricia Splett, PhD, MPH, RD Splett & Associates 3219 Midland Avenue St. Paul, MN 55110 Task Force Member 2003-2005
Frances Tyus, MS, RD, LD 19412 Mayfair Ln Cleveland, OH 44128-2727 Task Force Member 2003-2005
Naomi Trostler, PhD, RD Institute of Biochemistry, Food Science, and Nutrition Faculty of Agriculture, Food and Environmental Quality Sciences The Hebrew University of Jerusalem PO Box 12 Rehovot 76100, IsraelTask Force Member 2004-2005
Robin Leonhardt, RD 1905 North 24th Street Sheboygan, WI 53081-2124 Attended Face to Face Meeting in Summer
2003
Staff LiaisonsEsther Myers, PhD, RD, FADA Director of Scientific Affairs and Research ADA Headquarters 120 South Riverside Plaza Suite 2000 Chicago, IL 60619 Work (312) 899-4860 Fax (312) 899-4757 E-mail: [email protected]
Ellen Pritchett, RD, CPHQ Director, Quality and Outcomes ADA Headquarters 120 South Riverside Plaza Suite 2000 Chicago, IL 60619 Work (312) 899-4823 Fax (312) 899-4757 E-mail: [email protected] Liaison 2003-2005
Lt Col Vivian Hutson, MA,MHA,RD,LD, FACHEStaff Liaison 2003-2004

2003 - 2005 Standardized Language Task Force and Terminology Expert Reviewers
Edition: 2006 161
Consultants
Donna G. Pertel, MEd, RD 5 Bonny Lane Clinton, CT 06413
Patricia Splett, PhD, MPH, RD Splett & Associates 3219 Midland Avenue St. Paul, MN 55110
Melinda L. Jenkins, Ph.D., FNP Assistant Professor of Clinical Nursing Columbia University School of Nursing 630 W. 168 St., mail code 6 New York, NY 10032
Annalynn Skipper, MS, RD, FADA P.O. Box 45 Oak Park, IL 60303
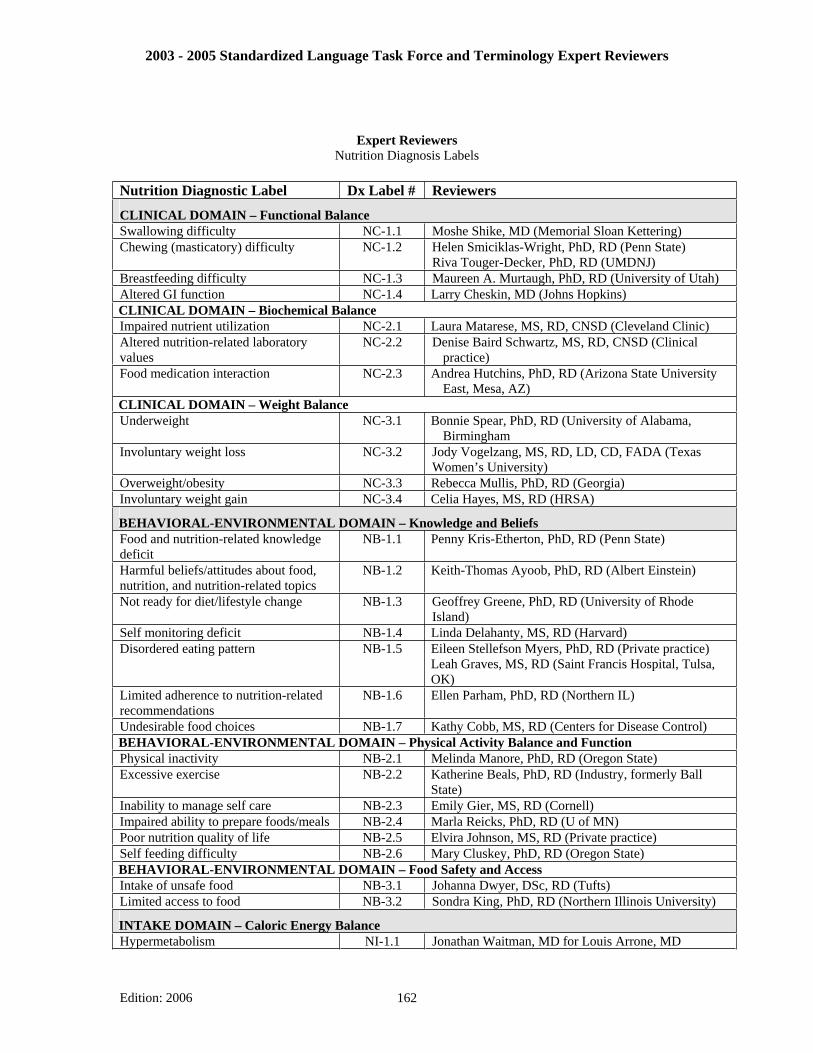
2003 - 2005 Standardized Language Task Force and Terminology Expert Reviewers
Expert Reviewers Nutrition Diagnosis Labels
Nutrition Diagnostic Label Dx Label # Reviewers
CLINICAL DOMAIN – Functional Balance Swallowing difficulty NC-1.1 Moshe Shike, MD (Memorial Sloan Kettering) Chewing (masticatory) difficulty NC-1.2 Helen Smiciklas-Wright, PhD, RD (Penn State)
Riva Touger-Decker, PhD, RD (UMDNJ) Breastfeeding difficulty NC-1.3 Maureen A. Murtaugh, PhD, RD (University of Utah) Altered GI function NC-1.4 Larry Cheskin, MD (Johns Hopkins) CLINICAL DOMAIN – Biochemical Balance Impaired nutrient utilization NC-2.1 Laura Matarese, MS, RD, CNSD (Cleveland Clinic) Altered nutrition-related laboratory values
NC-2.2 Denise Baird Schwartz, MS, RD, CNSD (Clinical practice)
Food medication interaction NC-2.3 Andrea Hutchins, PhD, RD (Arizona State University East, Mesa, AZ)
CLINICAL DOMAIN – Weight Balance Underweight NC-3.1 Bonnie Spear, PhD, RD (University of Alabama,
Birmingham Involuntary weight loss NC-3.2 Jody Vogelzang, MS, RD, LD, CD, FADA (Texas
Women’s University) Overweight/obesity NC-3.3 Rebecca Mullis, PhD, RD (Georgia) Involuntary weight gain NC-3.4 Celia Hayes, MS, RD (HRSA)
BEHAVIORAL-ENVIRONMENTAL DOMAIN – Knowledge and Beliefs Food and nutrition-related knowledge deficit
NB-1.1 Penny Kris-Etherton, PhD, RD (Penn State)
Harmful beliefs/attitudes about food, nutrition, and nutrition-related topics
NB-1.2 Keith-Thomas Ayoob, PhD, RD (Albert Einstein)
Not ready for diet/lifestyle change NB-1.3 Geoffrey Greene, PhD, RD (University of Rhode Island)
Self monitoring deficit NB-1.4 Linda Delahanty, MS, RD (Harvard) Disordered eating pattern NB-1.5 Eileen Stellefson Myers, PhD, RD (Private practice)
Leah Graves, MS, RD (Saint Francis Hospital, Tulsa, OK)
Limited adherence to nutrition-related recommendations
NB-1.6 Ellen Parham, PhD, RD (Northern IL)
Undesirable food choices NB-1.7 Kathy Cobb, MS, RD (Centers for Disease Control) BEHAVIORAL-ENVIRONMENTAL DOMAIN – Physical Activity Balance and Function Physical inactivity NB-2.1 Melinda Manore, PhD, RD (Oregon State) Excessive exercise NB-2.2 Katherine Beals, PhD, RD (Industry, formerly Ball
State)Inability to manage self care NB-2.3 Emily Gier, MS, RD (Cornell) Impaired ability to prepare foods/meals NB-2.4 Marla Reicks, PhD, RD (U of MN) Poor nutrition quality of life NB-2.5 Elvira Johnson, MS, RD (Private practice) Self feeding difficulty NB-2.6 Mary Cluskey, PhD, RD (Oregon State) BEHAVIORAL-ENVIRONMENTAL DOMAIN – Food Safety and Access Intake of unsafe food NB-3.1 Johanna Dwyer, DSc, RD (Tufts) Limited access to food NB-3.2 Sondra King, PhD, RD (Northern Illinois University)
INTAKE DOMAIN – Caloric Energy Balance Hypermetabolism NI-1.1 Jonathan Waitman, MD for Louis Arrone, MD
Edition: 2006 162

2003 - 2005 Standardized Language Task Force and Terminology Expert Reviewers
(Cornell) Increased energy expenditure (when part of hypermetabolism)
NI-1.2 Jonathan Waitman, MD for Louis Arrone, MD (Cornell)
Hypometabolism NI-1.3 Edith Lerner, PhD (Case Western Reserve University) Inadequate energy intake NI-1.4 Joel Mason, MD (Tufts) Excessive energy intake NI-1.5 Jim Hill, MD (University of Colorado) INTAKE DOMAIN – Oral or Nutrition Support Intake Inadequate oral food/beverage intake NI-2.1 Anne Voss, PhD, RD (Ross Labs) Excessive oral food/beverage intake NI-2.2 Jessica Krenkel, MS, RD (University of Nevada) Inadequate intake from enteral/parenteral nutrition
NI-2.3 Kenneth Kudsk, MD (University of Wisconsin)
Excessive intake from enteral/parenteral nutrition
NI-2.4 Annalynn Skipper, MS, RD (University of Nebraska Lincoln)
Inappropriate infusion of enteral/parenteral nutrition
NI-2.5 Annalynn Skipper, MS, RD (University of Nebraska-Lincoln)
INTAKE DOMAIN – Fluid Intake Balance Inadequate fluid intake NI-3.1 Ann Grandjean, EdD, RD (International Center for
Sports Nutrition) Excessive fluid intake NI-3.2 Joel Kopple, MD (UCLA) INTAKE DOMAIN – Bioactive Substances Balance Inadequate bioactive substance intake NI-4.1 Johanna Lappe, PhD, RN (Creighton) Excess bioactive substance NI-4.2 Elizabeth Jeffery, PhD (Univ. of IL, Champaign) Excessive alcohol intake NI-4.3 Janice Harris, PhD, RD (University of Kansas) INTAKE DOMAIN – Nutrient Balance Increased nutrient (specify) needs NI-5.1 Carol Braunschweig, PhD, RD (University of Illinois,
Chicago)Evident protein-energy malnutrition NI-5.2 Charlette R. Gallagher Allred, PhD, RD (Retired-Ross
Labs) Inadequate protein energy intake NI-5.3 Trisha Fuhrman, MS, RD (Caremark) Decreased nutrient (specify) needs NI-5.4 Jeannmarie Beiseigel, PhD, RD (USDA) Imbalance of nutrients NI-5.5 Molly Kretsch, PhD, RD (USDA) INTAKE DOMAIN – Nutrient Balance – Fat and Cholesterol BalanceInadequate fat intake NI-51.1 Alice Lichtenstein, DSc (Tufts) Excessive fat intake NI-51.2 Wendy Mueller Cunnigham, PhD, RD (Cal State) Inappropriate intake of food fats NI-51.3 Nancy Lewis, PhD, RD (University of Nebraska-
Lincoln) INTAKE DOMAIN – Nutrient Balance – Protein BalanceInadequate protein intake NI-52.1 Don Layman, PhD (University of Illinois-Champaign) Excessive or unbalanced protein intake NI-52.2 Linda A. Vaughan, PhD, RD (Arizona State) Inappropriate intake of amino acids NI-52.3 Allison Yates, PhD, RD (Industry, formerly Director of
the IOM Food and Nutrition Board) INTAKE DOMAIN – Nutrient Balance – Carbohydrate BalanceInadequate carbohydrate intake NI-53.1 Robert Wolfe, PhD (University of Texas Medical
Branch) Excessive carbohydrate intake NI-53.2 Anne Daly, MS, RD Inappropriate intake of types of carbohydrate
NI-53.3 Lyn Wheeler, MS, RD, CD, FADA, CDE (Indiana University School of Medicine)
Inconsistent intake of carbohydrate NI-53.4 Maggie Powers, MS, RD, CDE (International Diabetes Center)
Inadequate fiber intake NI-53.5 Joanne Slavin, PhD, RD (University of Minnesota) Excess fiber intake NI-53.6 Judith Marlett, PhD, RD (University of Wisconsin) INTAKE DOMAIN – Nutrient Balance – Vitamin BalanceInadequate vitamin intake (specify) NI-54.1 Laurie A. Kruzich, MS, RD (Iowa State)
Kristina Penniston, PhD, RD (University of Wisconsin)
Edition: 2006 163

2003 - 2005 Standardized Language Task Force and Terminology Expert Reviewers
Excess vitamin intake NI-54.2 Kristina Penniston, PhD, RD (University of Wisconsin) INTAKE DOMAIN – Nutrient Balance – Mineral BalanceInadequate mineral intake (specify) NI-55.1 Bob Heaney, MD (Creighton) Excessive mineral intake NI-55.2 Joan Fischer, PhD, RD (University of Georgia)
Edition: 2006 164

2003 - 2005 Standardized Language Task Force and Terminology Expert Reviewers
Edition: 2006 165

FEEDBACK FORM
Please provide us with feedback on revisions you would suggest to this reference for Nutrition Diagnosing. Please indicate whether each section should still be included and also identify what questions you would like answered in the next version as well as additional materials that you would find helpful.
PleaseCheck Yes or No
The following items should be included in the next version: YES NO
Introduction to Nutrition Diagnosis Terminology Nutrition Care Process and Model Article ADA’s Standardized Language Model and Current Status Procedure for submitting proposed changes Single Page list of Terminology Eight pages of Terms and Definitions (Table of Contents to next document) Reference Sheets (128 pages)
What questions would you like answered in the 2007 version?
What additional materials would be helpful in the 2007 version?
Please remove from packet and mail form or e-mail information to:
Scientific Affairs and Research Standardized Language/Nutrition Care Process Committee 120 South Riverside Plaza Suite 2000 Chicago, IL 60606-6995
Edition: 2006 165

Edition: 2006 166

INTAKE NIDefi ned as “actual problems related to intake of energy, nutrients, fl uids, bioactive substances through oral diet or nutrition support”Caloric Energy Balance (1)Defi ned as “actual or estimated changes in energy (kcal)”
� Hypermetabolism (Increased energy needs) NI-1.1� Increased energy expenditure NI-1.2� Hypometabolism (Decreased energy needs) NI-1.3� Inadequate energy intake NI-1.4� Excessive energy intake NI-1.5
Oral or Nutrition Support Intake (2)Defi ned as “actual or estimated food and beverage intake from oral diet or nutrition support” compared with patient goal”
� Inadequate oral food/beverage intake NI-2.1� Excessive oral food/beverage intake NI-2.2� Inadequate intake from NI-2.3
enteral/parenteral nutrition infusion� Excessive intake from NI-2.4
enteral/parenteral nutrition� Inappropriate infusion of NI-2.5
enteral/parenteral nutrition (use with caution)Fluid Intake (3)Defi ned as “actual or estimated fl uid intake compared against patient goal”
� Inadequate fl uid intake NI-3.1� Excessive fl uid intake NI-3.2
Bioactive Substances (4)Defi ned as “actual or observed intake of bioactive substances, including single or multiple functional food components, ingredients, dietary supplements, alcohol”
� Inadequate bioactive substance intake NI-4.1� Excessive bioactivesubstance intake NI-4.2� Excessive alcohol intake NI-4.3
Nutrient (5)Defi ned as “actual or estimated intake of specifi c nutrient groups or single nutrients as compared with desired levels”
� Increased nutrient needs NI-5.1 (specify) _______________________________________
� Evident protein- energy malnutrition NI-5.2� Inadequate protein-energy intake NI-5.3� Decreased nutrient needs NI-5.4
(specify) _______________________________________� Imbalance of nutrients NI-5.5Fat and Cholesterol (51)� Inadequate fat intake NI-51.1� Excessive fat intake NI-51.2� Inappropriate intake of food fats NI-51.3
(specify) _______________________________________ Protein (52)
� Inadequate protein intake NI-52.1� Excessive protein intake NI-52.2� Inappropriate intake of amino acids NI-52.3
(specify) _______________________________________ Carbohydrate and Fiber Intake (53)
� Inadequate carbohydrate intake NI-53.1 � Excessive carbohydrate intake NI-53.2� Inappropriate intake of types of carbohydrate NI-53.3
(specify) _______________________________________� Inconsistent carbohydrate intake NI-53.4� Inadequate fi ber intake NI-53.5� Excessive fi ber intake NI-53.6
Vitamin Intake (54)� Inadequate vitamin intake (specify) NI-54.1� Excessive vitamin intake (specify) NI-54.2
� A � C� Thiamin � D� Ribofl avin � E� Niacin � K� Folate � Other ________________
Mineral Intake (55)� Inadequate mineral intake (specify) NI-55.1
� Calcium � Iron� Potassium � Zinc� Other ___________________________________
� Excessive mineral intake (specify) NI-55.2 � Calcium � Iron� Potassium � Zinc� Other ___________________________________
CLINICAL NCDefi ned as “nutritional fi ndings/problems identifi ed as related to medical or physical conditions”Functional (1)Defi ned as “change in physical or mechanical functioning that interferes with or prevents desired nutritional consequences”
� Swallowing diffi culty NC-1.1� Chewing (masticatory) diffi culty NC-1.2� Breastfeeding diffi culty NC-1.3� Altered GI function NC-1.4
Biochemical (2)Defi ned as “change in capacity to metabolize nutrients as a result of medications, surgery, or as indicated by altered lab values”
� Impaired nutrient utilization NC-2.1� Altered nutrition-related laboratory values NC-2.2� Food medication interaction NC-2.3
Weight (3) Defi ned as “chronic weight or changed weight status when compared with usual or desired body weight”
� Underweight NC-3.1� Involuntary weight loss NC-3.2� Overweight/obesity NC-3.3� Involuntary weight gain NC-3.4
BEHAVIORAL-ENVIRONMENTAL NBDefi ned as “nutritional fi ndings/problems identifi ed as related to knowledge, attitudes/beliefs, physical environment, or food supply and safety”Knowledge and Beliefs (1)Defi ned as “actual knowledge and beliefs as observed or documented”
� Food and nutrition-related knowledge defi cit NB-1.1� Harmful beliefs/attitudes about food or NB-1.2
nutrition-related topics (use with caution)� Not ready for diet/lifestyle change NB-1.3� Self monitoring defi cit NB-1.4� Disordered eating pattern NB-1.5� Limited adherence to nutrition- NB-1.6
related recommendations� Undesirable food choices NB-1.7
Physical Activity and Function (2)Defi ned as “actual physical activity, self-care, and quality of life problems as reported, observed or documented”
� Physical inactivity NB-2.1� Excessive exercise NB-2.2� Inability or lack of desire to manage self care NB-2.3� Impaired ability to prepare foods/meals NB-2.4� Poor nutrition quality of life NB-2.5� Self-feeding diffi culty NB-2.6
Food Safety and Access (3)Defi ned as “actual problems with food access or food safety”
� Intake of unsafe food NB-3.1� Limited access to food NB-3.2
Edition: 2006
NUTRITION DIAGNOSTIC TERMINOLOGY NUTRITION DIAGNOSTIC TERMINOLOGYNUTRITION DIAGNOSTIC TERMINOLOGYNUTRITION DIAGNOSTIC TERMINOLOGY
167