obesità, infiammazione e malattie reumatologiche: è ... · obesità e malattie reumatiche:...
TRANSCRIPT

Obesità, infiammazione e malattie reumatologiche:è possibile un approccio terapeutico integrato?
Prof. Fausto [email protected]
Clinica Reumatologica – Early Arthritis Clinic - Dipartimento di Scienze Cliniche e Molecolari -
Università Politecnica delle Marche, Ancona

Both overweight
and obesity are
associated with
the incidence of
multiple
comorbidities
Including
rheumatic
disorders
Obesità e malattie reumatiche: elementi fisiopatologici e potenziali biomarkers
Obesità e rischio di insorgenza della malattia reumatica: profilo epidemiologico e predittori
Obesità ed impatto sull’attività e severità dellamalattia reumatica
Obesità e risposta al trattamento con farmacibiologici
Obesità ed approccio terapeutico integrato
OBESITA’ & MALATTIE REUMATICHE
1
3
2
4
5

Obesità e malattie reumatiche: elementi fisiopatologici e potenziali biomarkers
Obesità e rischio di insorgenza della malattia reumatica: profilo epidemiologico e predittori
Obesità ed impatto sull’attività e severità dellamalattia reumatica
Obesità e risposta al trattamento con farmacibiologici
Obesità ed approccio terapeutico integrato
OBESITA’ & MALATTIE REUMATICHE
1

Obesity rarely exists on its own; instead,
it tends to coexist with other
comorbidities, including metabolic,
cardiovascular, and rheumatic and
musculoskeletal diseases (RMDs). In the
case of RMDs, evidence is rapidly
accumulating on common mechanistic
pathways implicated in the inflammatory
states seen between RMDs and obesity
The chronic state of low-grade
inflammation present in the obese
condition and the multiple
pleiotropic effects of adipokines
on the immune system has been
implicated in the pathogenesis of
several inflammatory conditions
including rheumatic autoimmune
and inflammatory diseases
Evaluating the effects of weight
loss on the
inflammatory/autoimmune
disease course appears to be
crucial in terms of potential
clinical and also
pharmacoeconomics
perspectives.

Potential
mechanisms
explaining the
link between
obesity and
inflammatory
arthritis.
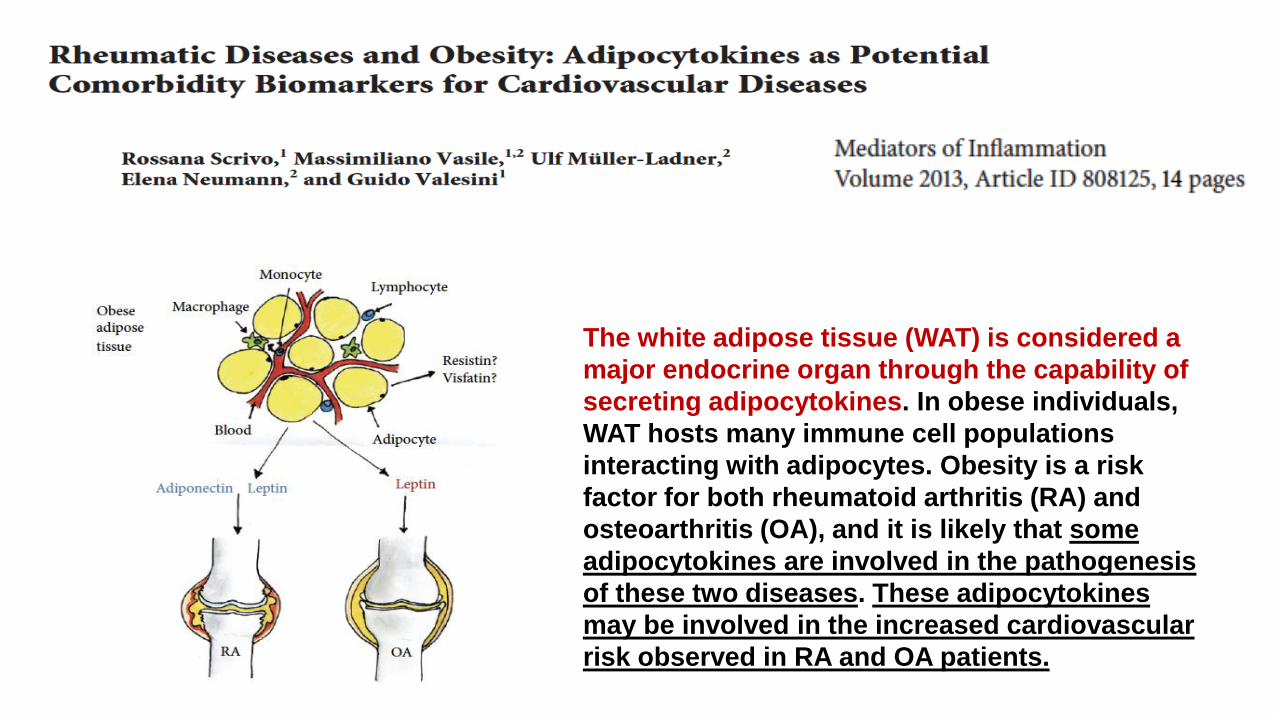
The white adipose tissue (WAT) is considered a
major endocrine organ through the capability of
secreting adipocytokines. In obese individuals,
WAT hosts many immune cell populations
interacting with adipocytes. Obesity is a risk
factor for both rheumatoid arthritis (RA) and
osteoarthritis (OA), and it is likely that some
adipocytokines are involved in the pathogenesis
of these two diseases. These adipocytokines
may be involved in the increased cardiovascular
risk observed in RA and OA patients.

Adipokine serum
levels in autoimmune
rheumatic diseases.
Adipokines, mainly
produced by adipose
tissue, have mixed pro-
and anti-inflammatory
properties.

Adiposity triggers metabolicinflammation, in which various
adipokines released from adipose tissuesinduce pro-inflammatory cytokines in
the synovium and chondrocytes, ultimately leading to cartilage matrix
damage and subchondral bone remodelling
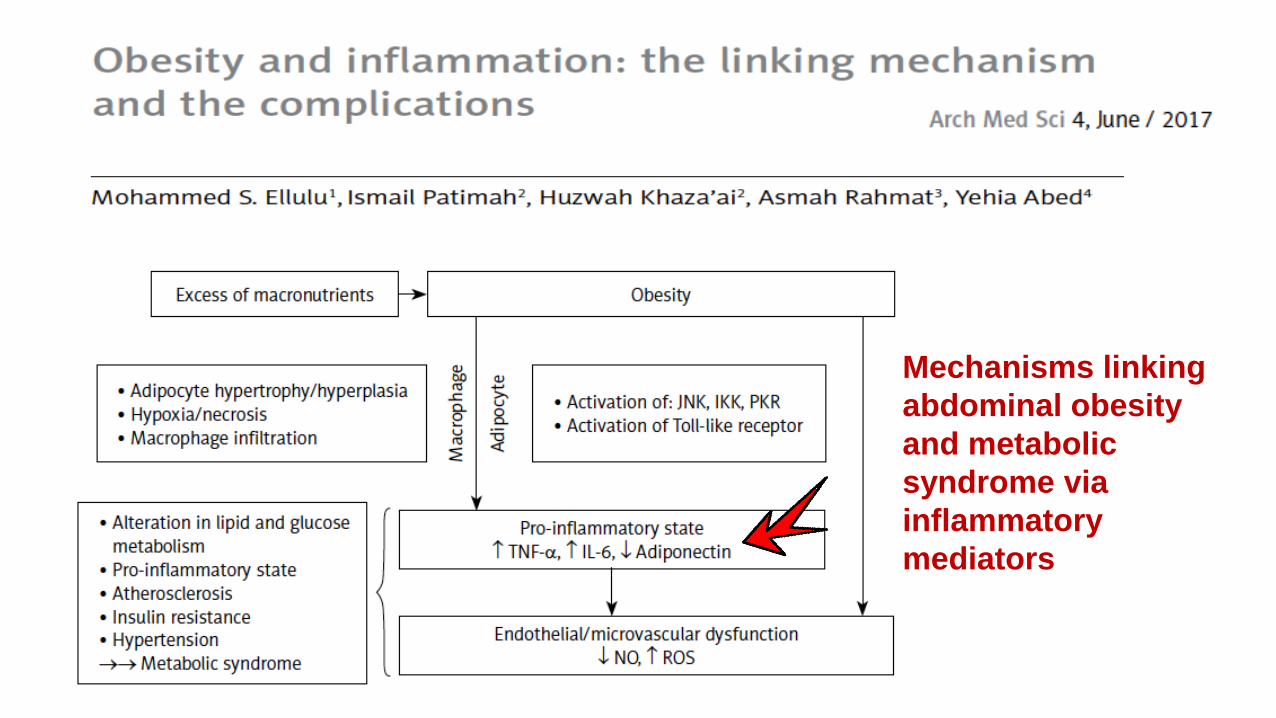
Mechanisms linking
abdominal obesity
and metabolic
syndrome via
inflammatory
mediators
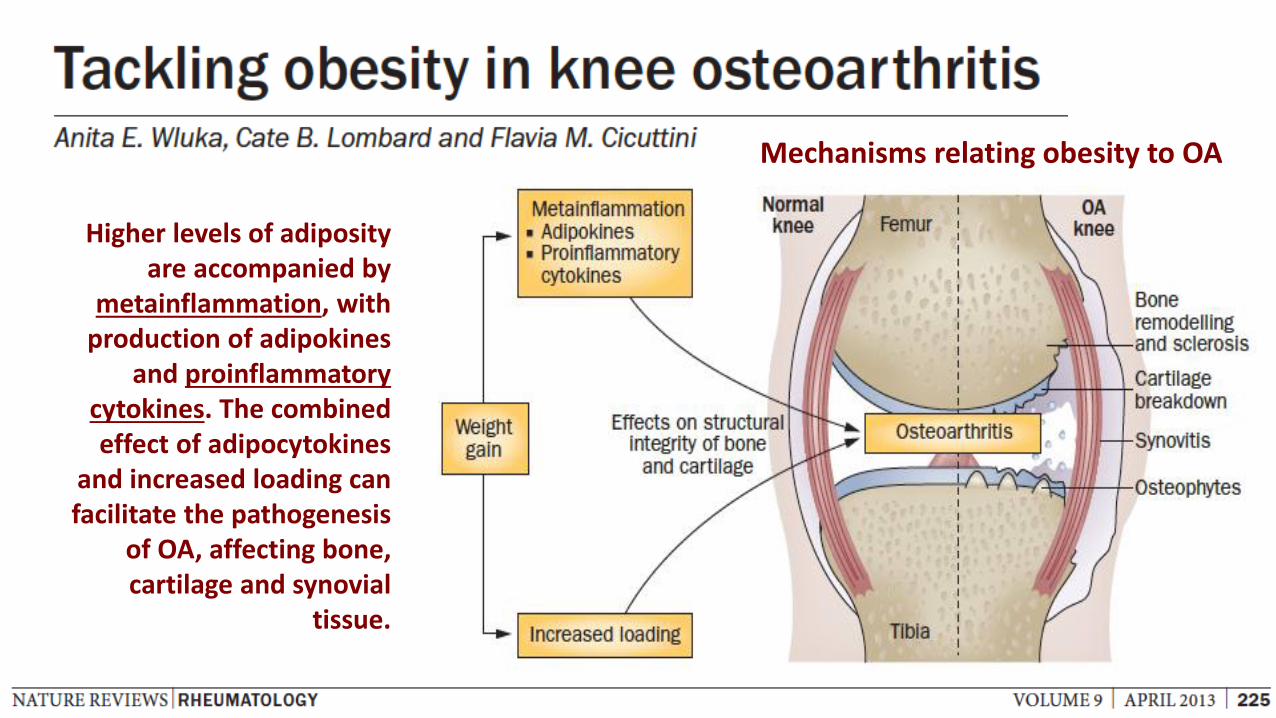
Mechanisms relating obesity to OA
Higher levels of adiposityare accompanied by
metainflammation, with production of adipokines
and proinflammatorycytokines. The combinedeffect of adipocytokines
and increased loading can facilitate the pathogenesis
of OA, affecting bone, cartilage and synovial
tissue.
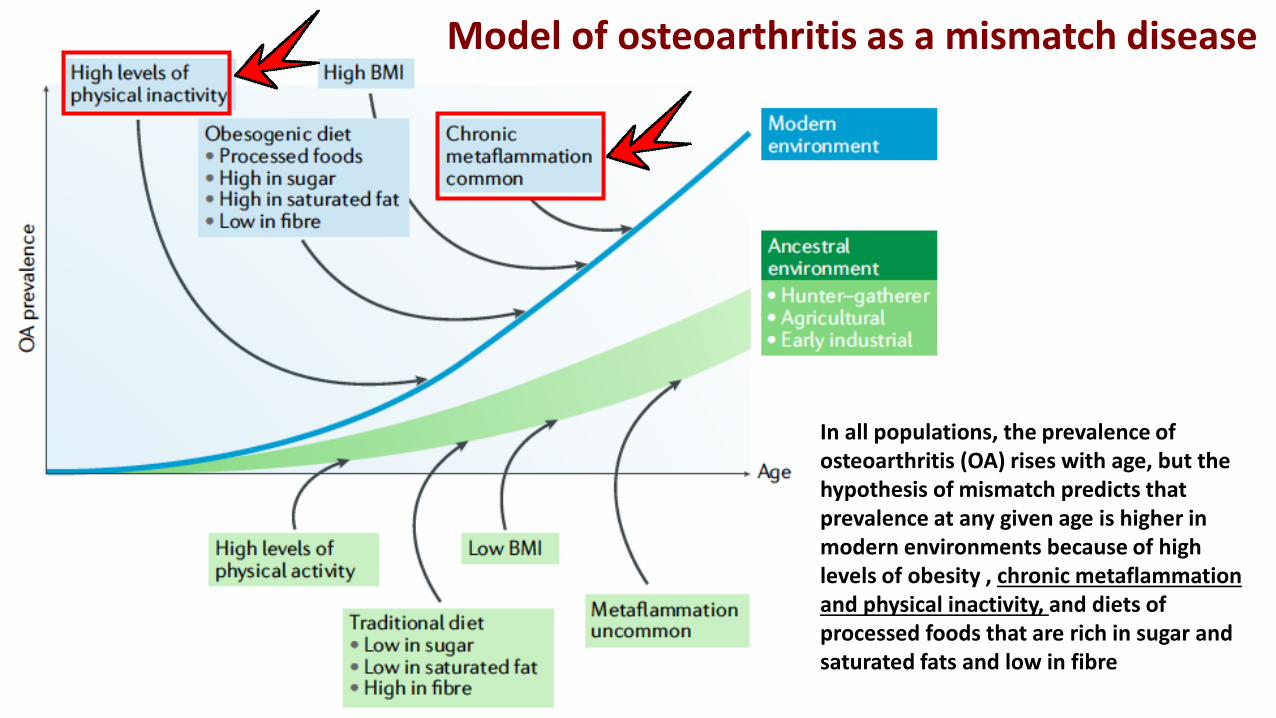
In all populations, the prevalence of osteoarthritis (OA) rises with age, but the hypothesis of mismatch predicts thatprevalence at any given age is higher in modern environments because of high levels of obesity , chronic metaflammationand physical inactivity, and diets of processed foods that are rich in sugar and saturated fats and low in fibre
Model of osteoarthritis as a mismatch disease

Obesity and OA: a vicious cycle
Obesity can affect the pathogenesis of OA through biomechanical effects as well as via
increased metainflammation. Increasedobesity is associated with higher levels of
joint loading and reduced levels of physicalactivity, which in turn reduces muscle
strength. Combined, these effects can resultin the structural changes of OA. Structural
disease results in pain, which presents a barrier to physical activity, further reducing
energy expenditure and resulting in reducedmuscle mass and increased fat mass.

Obesità e malattie reumatiche: elementi fisiopatologici e potenziali biomarkers
Obesità e rischio di insorgenza della malattia reumatica: profilo epidemiologico e predittori
Obesità ed impatto sull’attività e severità dellamalattia reumatica
Obesità e risposta al trattamento con farmacibiologici
Obesità ed approccio terapeutico integrato
OBESITA’ & MALATTIE REUMATICHE
2

This national study has
demonstrated that the odds of
osteoarthritis (OA) was up to 7
times higher for obese
individuals, compared with
those classified as
underweight/normal weight. OA was up to 7 times higher
for obese individuals

Forest plot for the
aggregate risk of
knee osteoarthritis
for obesity versus
normal weight.

Meta-analysis of studies for osteoarthritis.

The incidence of knee, hip, and
hand OA increased with
increasing BMI, with a greater
increase for knee OA

Forest plot for the
aggregate risk of
knee osteoarthritis
with the increase of
a 5 kg/m2 of body
mass index.

In comparison with subjects of normal weight, without Heberden’s nodes, and with no history of kneeinjury, people with a combination of obesity, definite Heberden's nodesand previous knee injury had a relative risk of 78 (95% CI 17 ± 354).

The incidence of knee, hip,
and hand OA increased with
increasing BMI, with a greater
increase for knee OA

The incidence of knee, hip,
and hand OA increased with
increasing BMI, with a
greater increase for knee OA

The overall and dose-
response meta-analysis
showed that increased BMI
was associated with an
increased risk for rheumatoid
arthritis, which might present
a prevention strategy for the
prevention or control of
rheumatoid arthritis.
Sixteen studies that included a total of
406,584 participants were included in
the meta-analysis
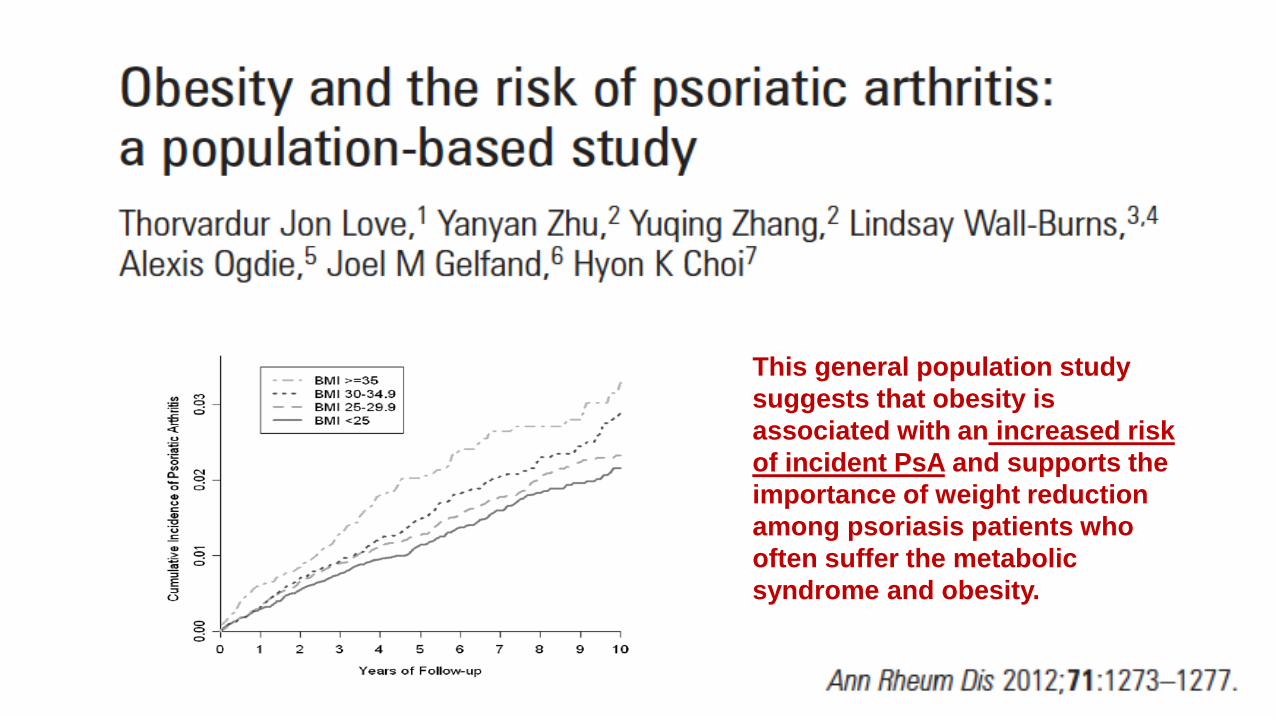
This general population study
suggests that obesity is
associated with an increased risk
of incident PsA and supports the
importance of weight reduction
among psoriasis patients who
often suffer the metabolic
syndrome and obesity.

Two large prospective studies
that suggest obesity is a risk
factor for PsA.
These studies offer valuable new
information on the link between obesity
and PsA and provide a potential
opportunity to reduce the occurrence of
PsA by encouraging a reduction in
weight, a modifiable risk factor.
Understanding and
implementation of
these measures could
reduce the severe
comorbidity associated
with psoriatic disease.

Fibromyalgia is a chronic disorder of
uncertain etiology, characterized by
widespread pain, muscle tenderness, and
decreased pain threshold to pressure and
other stimuli.
Epidemiological data show that
fibromyalgia patients have higher
prevalence of obesity (40%) and
overweight (30%) in multiple studies
compared with healthy patients
Among mechanisms proposed,
there are the following: impaired
physical activity, cognitive and
sleep disturbances, psychiatric
comorbidity and depression,
dysfunction of thyroid
gland, dysfunction of the GH/IGF-1
axis, impairment of the
endogenous opioid system.

Obesità e malattie reumatiche: elementi fisiopatologici e potenziali biomarkers
Obesità e rischio di insorgenza della malattia reumatica: profilo epidemiologico e predittori
Obesità ed impatto sull’attività e severità dellamalattia reumatica
Obesità e risposta al trattamento con farmacibiologici
Obesità ed approccio terapeutico integrato
OBESITA’ & MALATTIE REUMATICHE
3

Pain and functional disability
are more severe in obese and
overweight knee OA patients
compared to those with
normal BMI, and obesity is an
independent predictor of
functional disability.
Obesity is an independent risk factor for functional disability in patients with knee OA.
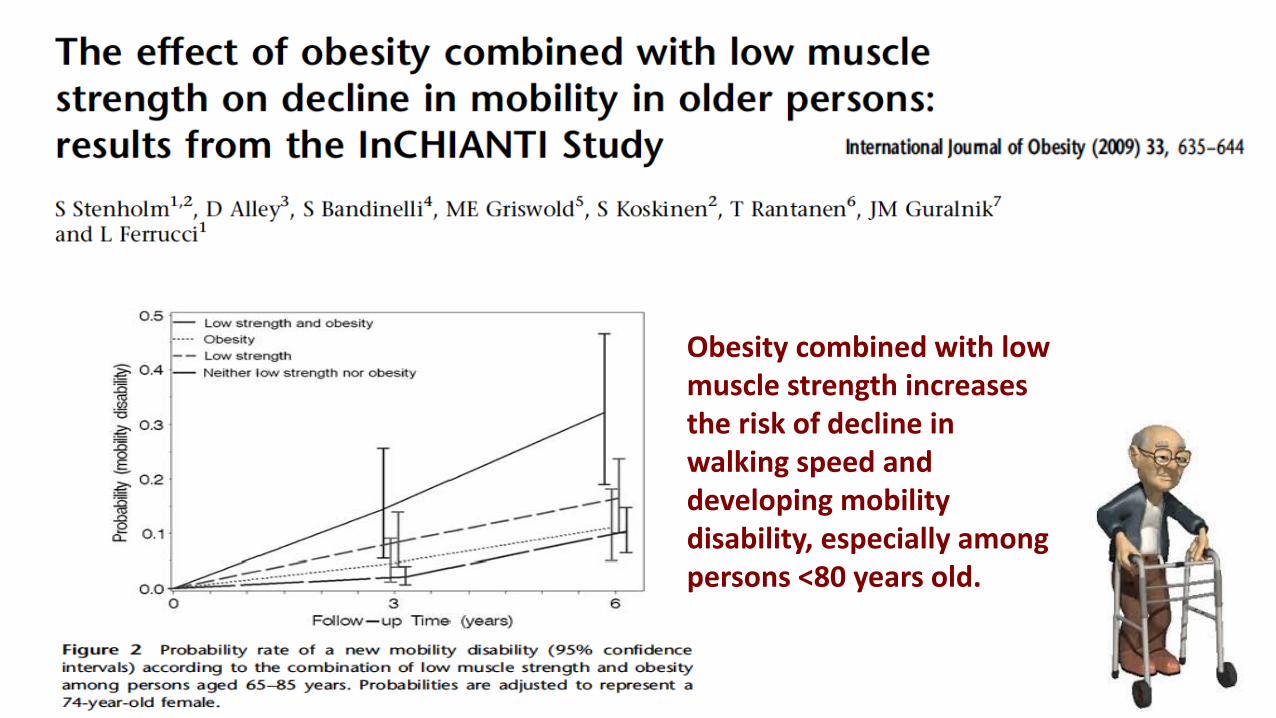
Obesity combined with lowmuscle strength increasesthe risk of decline in walking speed and developing mobilitydisability, especially amongpersons <80 years old.
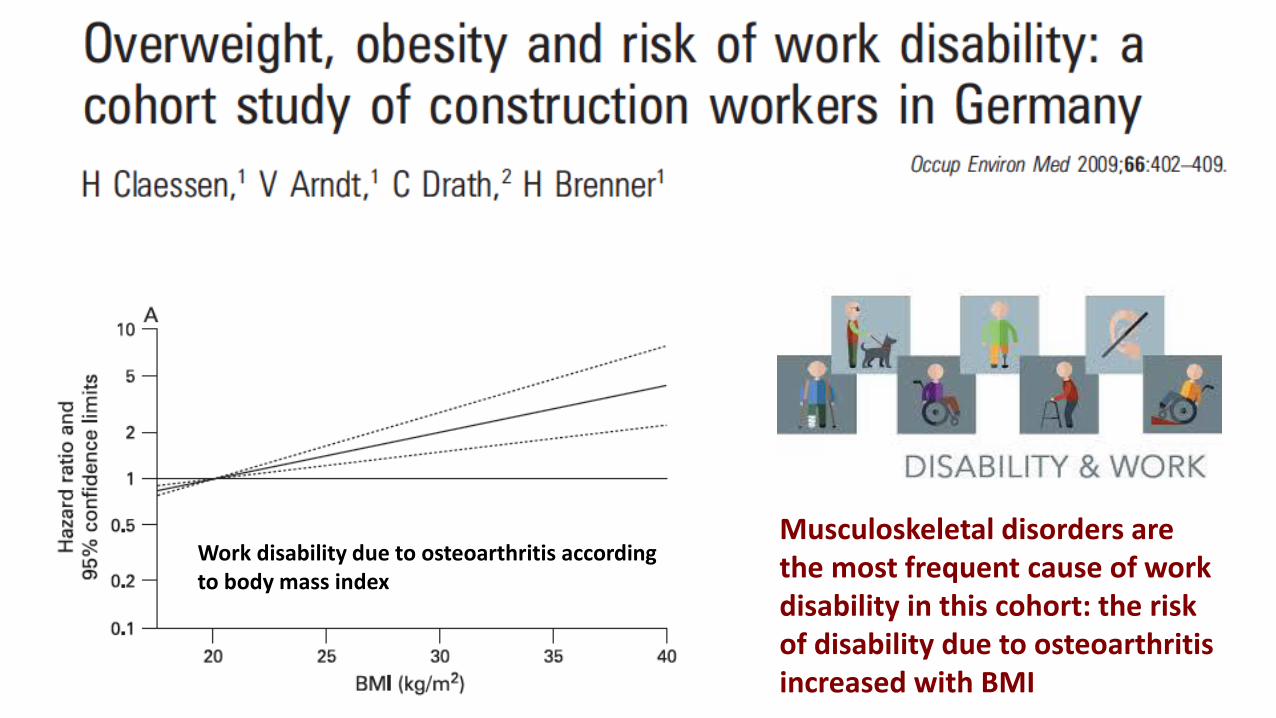
Work disability due to osteoarthritis accordingto body mass index
Musculoskeletal disorders are the most frequent cause of work disability in this cohort: the riskof disability due to osteoarthritisincreased with BMI

Relative risk ratiosdemonstrating the cross-sectionalrelationshipbetween obesity and total hip and kneearthroplasty.

Obesity had a negative influenceon outcome aftertotal kneearthroplasty.

Presurgical obesity is
associated with worse clinical
outcomes of hip or knee
arthroplasty in terms of pain,
disability and complications in
patients with osteoarthritis.
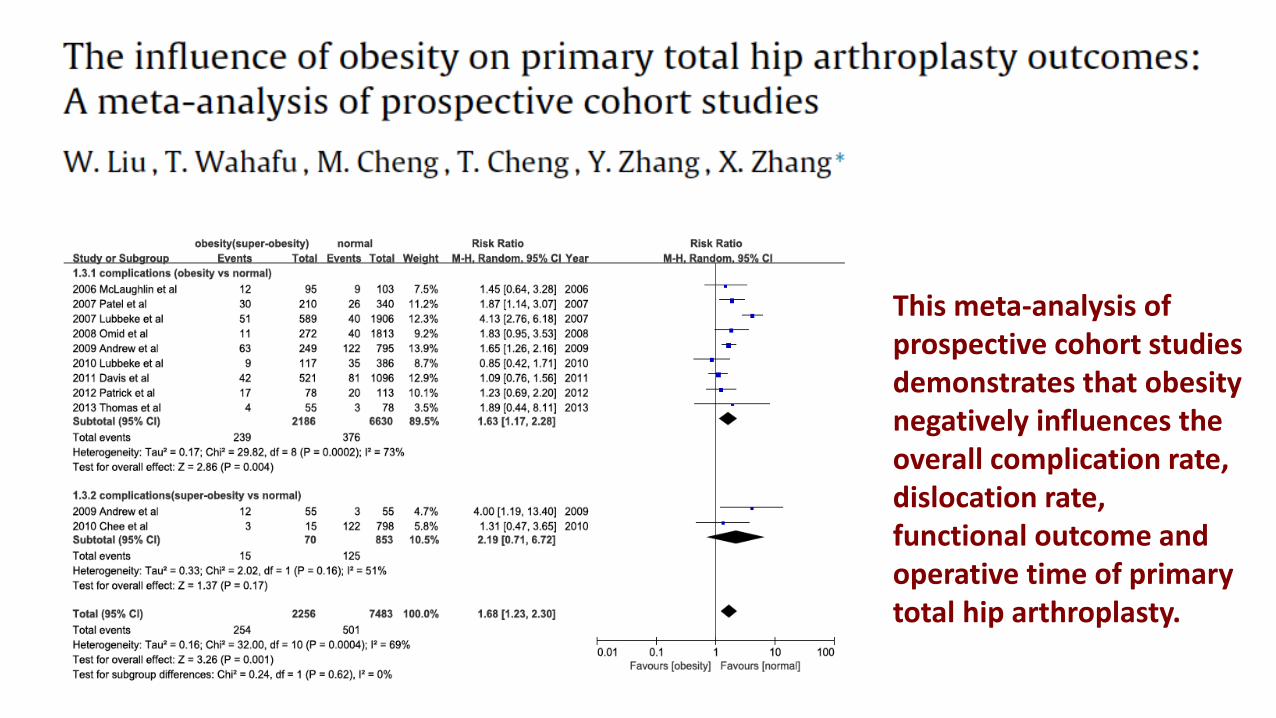
This meta-analysis of prospective cohort studies demonstrates that obesity negatively influences the overall complication rate, dislocation rate, functional outcome and operative time of primary total hip arthroplasty.
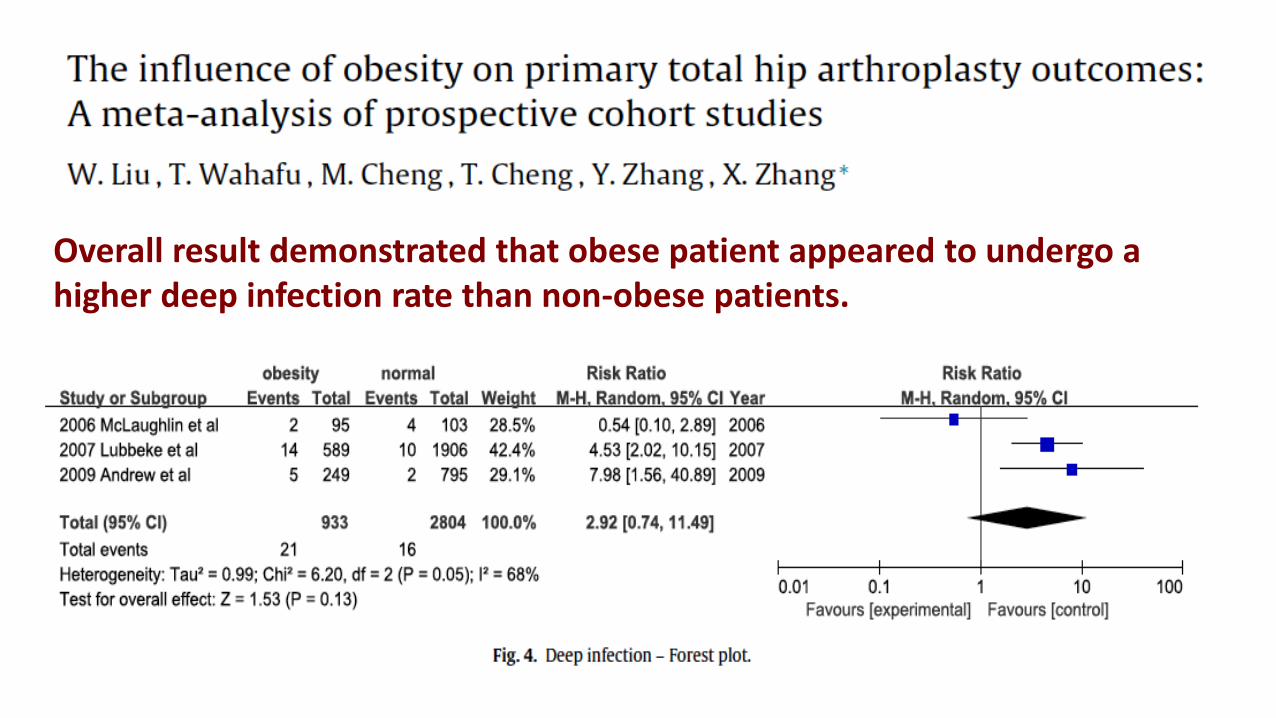
Overall result demonstrated that obese patient appeared to undergo a higher deep infection rate than non-obese patients.

Obesity was associated with
worse RA disease outcomes
and a higher prevalence of
comorbidities. Body
measurements are
recommended to improve
prediction of the disease
course.

it has been described that abdominal obesity is
associated with high disease activity, high
disability, physical inactivity and poor mental
health in a cohort of RA patients.
Evidence clarified that adipose tissue is a dynamic endocrine
organ that releases several bioactive substances including some
pro-inflammatory cytokines like TNF-α and IL-6, and specific
cytokines, termed adipokines, that may have a key role in RA
pathogenesis.

BMI is linked to both axial
and peripheral new bone
formation and entheseal
inflammation by imaging,
as supported by the limited
number of studies in the
literature
The association between obesity
and new bone formation highlights
the importance of biomechanical
factors in patients with SpA.
Biomechanical factors can be
considered the trigger of an
inflammatory process, so the
response of healing at these sites
can be associated with
new bone formation

Obesity was related significantly to
greater pain sensitivity to TP
palpation particularly in the lower
body areas, reduced physical
strength and lower-body flexibility,
shorter sleep duration, and greater
restlessness during sleep.
Obesity is a common co-
morbidity that may complicate
the clinical picture of FMS.
We found that obesity is
common in FMS. Approximately
a half of our patients were obese
and additional 30% were
overweight

Obesità e malattie reumatiche: elementi fisiopatologici e potenziali biomarkers
Obesità e rischio di insorgenza della malattia reumatica: profilo epidemiologico e predittori
Obesità ed impatto sull’attività e severità dellamalattia reumatica
Obesità e risposta al trattamento con farmacibiologici
Obesità ed approccio terapeutico integrato
OBESITA’ & MALATTIE REUMATICHE
4

The results of our meta-analysis
suggest that obesity and overweight
reduce the chances to achieve
minimal disease activity (MDA) in
patients with rheumatic diseases
receiving treatment with traditional
or biologic disease-modifying
antirheumatic drugs.
Forest plot of minimal disease activity achievement in obese patients versus normal-
weight patients with rheumatic diseases

Obese patients were
shown to have a poorer
response rate to
treatment in all outcome
measures in comparison
to the overweight and the
normal-weight RA
patients.

Obesity represents a risk
factor for a poor
remission rate in patients
with longstanding RA
treated with
anti-TNF agents.
Percentage of Disease
Activity Score in 28 joints
(DAS28) remission in
obese and nonobese
rheumatoid arthritis
patients treated with
adalimumab (ADA),
etanercept (ETA), and
infliximab (IFX). None of
the obese patients
responded to IFX.

…..RA and PsApatients with obesityhave a poor responseto biological anti-TNF drugs….

Data suggest that being female,
overweight and mostly obese is
associated with a lower rate of
success in obtaining response
status in axial SpA patients treated
with anti-TNF drugs. Body weight
could represent a modifiable factor
to reach the best outcome in axial
SpA patients treated with TNF
blockers

Obesity is associated with significantly lower response rates to TNFi in patients with axSpA.
While being overweight decreased
the odds of achieving an ASAS40
response upon TNF inhibition by
about 30%, the odds were decreased
by 70% in obese patients.


Obesità e malattie reumatiche: elementi fisiopatologici e potenziali biomarkers
Obesità e rischio di insorgenza della malattia reumatica: profilo epidemiologico e predittori
Obesità ed impatto sull’attività e severità dellamalattia reumatica
Obesità e risposta al trattamento con farmacibiologici
Obesità ed approccio terapeutico integrato
OBESITA’ & MALATTIE REUMATICHE
5


Obesity is a major risk factor for OA, and weight loss is effectiveat reducing the risk of OA, butadherence to interventions is
poor and should be addressed by personalized strategies
A conceptual model of OA

Obesity is a risk factor for manyconditions, including knee OA. The benefit of modifying thisrisk factor may cause significantrisk reduction of knee OA in the general population.

The meta-analysis
indicated that knee OA
risk increased almost
exponentially according
with the increase of body
mass index. Knee OA
prevention will benefit
from weight control

Meta regression analysis
indicated that physical
disability of patients
with knee OA and
overweight diminished
after a moderate
weight reduction regime.
Pain
Disability

The main factors associated with
onset of knee pain were being
overweight (pooled OR 1.98, 95%
confidence intervals (CI) 1.57 e
2.20), obesity (pooled OR 2.66
95% CI 2.15 - 3.28), female gender
(pooled OR 1.68, 95% CI 1.37 e
2.07), previous knee injury
(pooled OR 2.83, 95% CI 1.91 e
4.19).
Obesity in particular needs to
be a major target for prevention
of development of knee pain.

Overweight and obese patients areat >40% and 100% increased risk of kneereplacement surgery, respectively, compared to patients with normal weight.
Weight reduction strategies couldpotentially reduce the need for kneereplacement surgery by 31% amongpatients with knee OA.

The results should
encourage clinicians to
consider exercise therapy
as a treatment option for
patients with knee
osteoarthritis, even in the
presence of severe
comorbidity.

For knee OA, primary prevention includes the prevention of knee injury. Secondary preventionincludes dietary intervention and exercise in individualswho are overweight, have impaired muscle function or prior joint injury, whereas tertiary prevention involvesearly treatment of OA to prevent progression of the disease. The OA continuum

Overweight patients were 25% less
likely, and obese patients were 47% less
likely, to achieve sREM in the first 3 years,
despite similar initial disease-modifying
antirheumatic drug treatment and
subsequent biologic use. This is the largest
study demonstrating the negative impact of
excess weight on RA disease activity and
supports a call to action to better identify
and address this risk in RA patients
Weight may be a
potentially modifiable risk
factor to consider in
overweight and obese
early RA patients who
demonstrate an
inadequate response to
therapy.

Short-term weight loss
treatment was associated with
significant positive effects on
disease activity in joints,
entheses and skin in patients
with PsA and obesity.
The study supports the
hypothesis of obesity as a
promotor of disease activity in
PsA.
The percentage of patients reaching American College of Rheumatology (ACR) 20, ACR 50 and ACR 70
response criteria, Psoriatic Arthritis Response Criteria (PsARC) and Minimal Disease Activity (MDA). BL,
baseline; M6, 6 months visit

Patients in the higher BMI categories
were less likely to achieve sustained
MDA compared those in the lowest
BMI category (overweight: OR 0.66
p=0.003; obese: OR 0.53 p<0.0001)
after adjusting for potential
confounding variables.
Overweight and obese patients
with PsA are less likely to achieve
sustained MDA compared to
those of normal weight.
Weight loss may improve the long-
term outcome and overall health of
the patients and increase their
chances of achieving disease
remission

Evidence strongly suggests that
comorbid obesity is common in chronic
pain conditions, and pain complaints are
common in obese individuals.
Based upon the existing research, we
present several potential mechanisms that
may link the two phenomena, including
mechanical/structural factors, chemical
mediators, depression, sleep, and lifestyle
Weight loss/exercise
therapy for obese pain
patients appears to be an
important aspect of
overall pain rehabilitation

Classifica degli sport più
praticati al mare:
1) Corsa
2) Beach volley
3) Racchettoni
4) Nuoto
5) Apnea per tenere in dentro la pancia