obesity and sleep disordered breathing by ahmad younes professor of thoracic medicine mansoura...
TRANSCRIPT

Obesity and Sleep Disordered Breathing
BY
AHMAD YOUNES
Professor of Thoracic Medicine
Mansoura Faculty of Medicine

SLEEP DISORDERED BREATHING
• 1-Obstructive sleep apnea syndrome in which inadequate ventilation occurs despite continued efforts to breath due to upper airway obstruction.
• 2-Central sleep apnea syndrome in which inadequate ventilation occurs resulting from absent or diminished respiratory effort.
• 3-Sleep hypoventilation syndromes > 10 mm Hg increase in PaCO2 during sleep in comparison with an awake supine value.
Sleep related breathing Sleep related breathing disorders defintionsdisorders defintions
•ApneaApnea: : is defined as the drop in peak airflow by >90% of baseline for 10 seconds or longer and at least 90% of the event duration meet the amplitude reduction
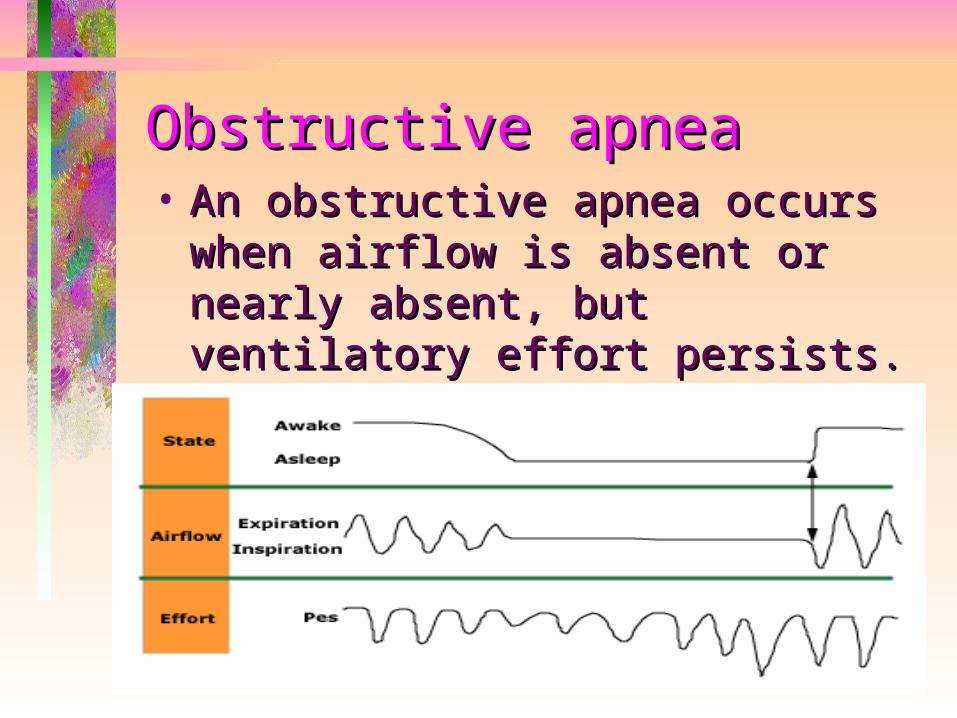
Obstructive apneaObstructive apnea• An obstructive apnea occurs when An obstructive apnea occurs when
airflow is absent or nearly absent, airflow is absent or nearly absent, but ventilatory effort persists. It is but ventilatory effort persists. It is caused by complete, or near caused by complete, or near complete, upper airway complete, upper airway obstruction.obstruction.

Central apneaCentral apnea
• A central apnea occurs when both A central apnea occurs when both airflow and ventilatory effort are airflow and ventilatory effort are absentabsent.

Mixed apneaMixed apnea
• During a mixed apnea, there is an During a mixed apnea, there is an interval during which there is no interval during which there is no respiratory effort (ie, central apnea respiratory effort (ie, central apnea pattern) and an interval during pattern) and an interval during which there are obstructed which there are obstructed respiratory efforts .respiratory efforts .

HypopneaHypopnea American Academy of Sleep Medicine, recommends American Academy of Sleep Medicine, recommends
that hypopnea be scored when all of the following that hypopnea be scored when all of the following four criteria are met: four criteria are met:
Airflow decreases at least Airflow decreases at least 30 percent30 percent from baseline from baseline There is diminished airflow lasting at least There is diminished airflow lasting at least 10 10
secondsseconds at least at least 4 percent4 percent oxyhemoglobin desaturation oxyhemoglobin desaturation oror
Airflow decreases at least Airflow decreases at least 50 percent50 percent from baseline from baseline There is diminished airflow lasting at least There is diminished airflow lasting at least 10 10
secondsseconds 3 percent3 percent oxyhemoglobin desaturation or oxyhemoglobin desaturation or an arousal an arousal

Respiratory effort related Respiratory effort related arousalsarousals• RERAs exist when there is a sequence of RERAs exist when there is a sequence of
breaths that lasts at least breaths that lasts at least 10 seconds10 seconds, is , is characterized bycharacterized by
• increasing respiratory effortincreasing respiratory effort or or• flattening of the nasal pressure flattening of the nasal pressure
waveformwaveform• leads to an leads to an arousalarousal from sleep from sleep• does not meet the criteria of an apnea does not meet the criteria of an apnea
or hypopnea or hypopnea
HypoventilationHypoventilation • Hypoventilation during sleep is defined Hypoventilation during sleep is defined
as an as an increase increase in in (PaCO2)(PaCO2) of of 10 mm 10 mm HgHg during sleep compared with an during sleep compared with an awake supine value .awake supine value .
• Directly measuring the pCO2 in an Directly measuring the pCO2 in an arterial blood gasarterial blood gas during a sleep study during a sleep study is optimal, but is optimal, but impracticalimpractical. .
• Transcutaneous CO2Transcutaneous CO2 measurements measurements and expired and expired end tidal CO2end tidal CO2 are are alternatives .alternatives .

Polysomnography indicesPolysomnography indices• Apnea-hypopnea indexApnea-hypopnea index (AHI)(AHI) is the is the
total number of total number of apneasapneas and and hypopneas hypopneas per hour of sleep. per hour of sleep.
• Respiratory disturbance index (RDI)Respiratory disturbance index (RDI) is the total number of events (eg, is the total number of events (eg, apneas, hypopneas, apneas, hypopneas, andand RERAs RERAs) per ) per hour of sleep. hour of sleep.

Polysomnography indicesPolysomnography indices• DesaturationDesaturation — — Oxygen desaturation Oxygen desaturation
is a frequent consequence of apnea is a frequent consequence of apnea and hypopnea. and hypopnea.
• Oxygen desaturation index (ODI) Oxygen desaturation index (ODI) This is the number of times that the This is the number of times that the oxygen saturation falls by more than oxygen saturation falls by more than 3 or 4 percent3 or 4 percent per hour of sleep per hour of sleep Minimum levels Minimum levels
• Arousal index (ArI)Arousal index (ArI) is the total is the total number of arousals per hour of sleep.number of arousals per hour of sleep.

•
syndromes of sleep related syndromes of sleep related breathing disordersbreathing disorders• Obstructive sleep apnea syndrome (OSA)Obstructive sleep apnea syndrome (OSA) in in
adults is defined as eitheradults is defined as either
• More than 15 apneas, hypopneas, or RERAs More than 15 apneas, hypopneas, or RERAs per hour of sleep ( per hour of sleep ( AHI or RDI >15 AHI or RDI >15 events/hrevents/hr) in an ) in an asymptomaticasymptomatic patient patient
OR OR • More than 5 apneas, hypopneas, or RERAs More than 5 apneas, hypopneas, or RERAs
per hour of sleep (per hour of sleep (AHI or RDI >5 events per AHI or RDI >5 events per hourhour) in a patient with ) in a patient with symptomssymptoms (eg, (eg, sleepiness, fatigue and inattention) or sleepiness, fatigue and inattention) or signssigns of disturbed sleep (snoring, restless of disturbed sleep (snoring, restless sleep, and respiratory pauses). sleep, and respiratory pauses).

syndromes of sleep related syndromes of sleep related breathing disordersbreathing disorders• Central sleep apnea syndrome (CSAS)Central sleep apnea syndrome (CSAS)
can be:can be:• idiopathic (eg, primary central sleep idiopathic (eg, primary central sleep
apnea)apnea)• secondary. Examples of secondary secondary. Examples of secondary
CSAS include CSAS include Cheyne-Stokes Cheyne-Stokes breathingbreathing, CSA due to , CSA due to high altitude high altitude periodic breathingperiodic breathing, CSA due to a , CSA due to a medical conditionmedical condition, and CSA due to a , and CSA due to a drug or substance. drug or substance.

Complex Sleep Apnea (CompSA)
• CompSA consists of all or predominantly obstructive apneas which convert to all or predominantly central apneas when treated with a CPAP or bilevel devices.
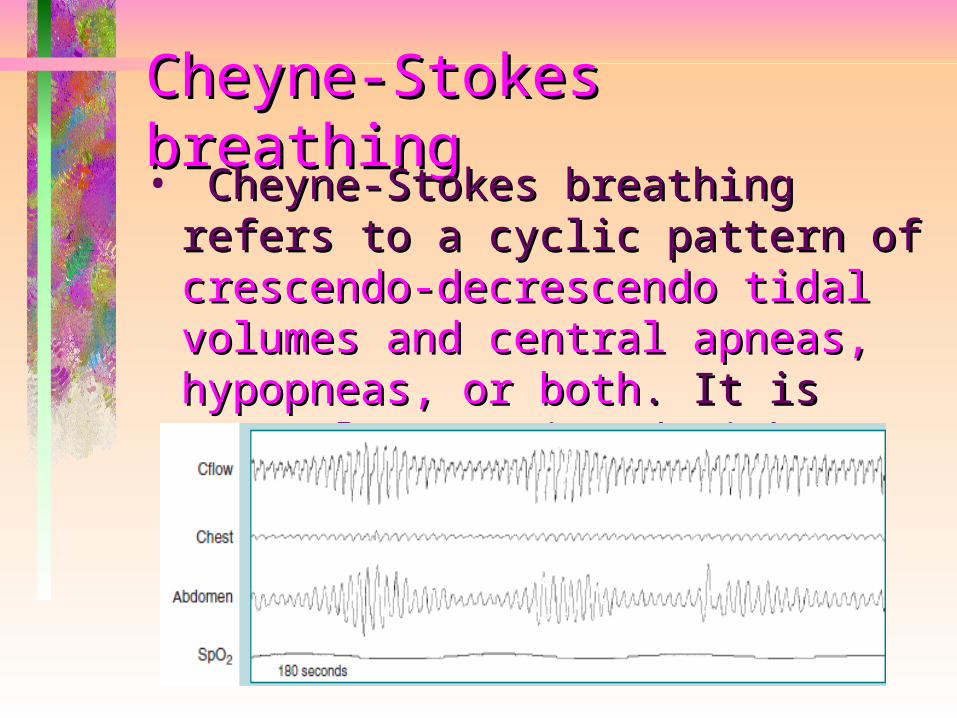
Cheyne-Stokes breathingCheyne-Stokes breathing• Cheyne-Stokes breathing refers to Cheyne-Stokes breathing refers to
a cyclic pattern of a cyclic pattern of crescendo-crescendo-decrescendo tidal volumes and decrescendo tidal volumes and central apneas, hypopneas, or central apneas, hypopneas, or bothboth. It is commonly associated . It is commonly associated with heart failure or stroke. with heart failure or stroke.

Obesity is a BIG problem

Obesity
• Obesity represent a state of excess body fate
• Men Body fat percentage of 15-20%• Women Body fat percentage of 25-
30%• Obesty in men > 25% and 21-25
borderline • Obesty in women > 33% and 31-33
borderline

Potential Consequences of Obesity• Obesity is associated with a rise in many
comorbid conditions, including:– Type 2 Diabetes– Hyperlipidemia– Hypertension– Obstructive Sleep Apnea– Obesity hypoventilation syndrome – Heart Disease– Stroke– Asthma– weight-bearing degenerative problems– Cancer– Depression– AND MORE!
Obesity
• Obesity, a chronic disease that is increasing in prevalence in adults, adolescents, and children, is now considered to be a global epidemic.
• obesity is often assessed by means of indirect estimates of body fat ( anthropometrics) .
• BMI is the accepted standard measure of obesity for children two years of age and older.
• Measures of regional fat distribution (waist circumference and waist-to-hip ratio) .

BMI = body weight (in kg) ÷ height (in meters) squared • Underweight — BMI <18. 5 kg/m2• Normal weight — BMI ≥18.5 to 24.9 kg/m2• Overweight — BMI ≥25.0 to 29.9 kg/m2• Obesity — BMI ≥30 kg/m2 • Obesity Class I — BMI of 30.0 to 34.9 kg/m2• Obesity Class II — BMI of 35.0 to 39.9 kg/m2• Obesity Class III — BMI ≥40 kg/m2. (severe,
extreme, or morbid obesity(.


Body fat pecentage • Body fat pecentage= 1.2(BMI)
+o.23(age)-1o.8(sex)-5.4• Age in years • Sex is 1 for male and o for female

Waist circumference• In addition to measuring body mass index,
waist circumference should be measured to assess abdominal obesity.
• Patients with abdominal obesity (central adiposity, visceral, android, or male-type obesity) are at increased risk for heart disease, diabetes, hypertension, and dys-lipidemia.
• Measurement of the waist-to-hip ratio provides no advantage over waist circumference alone.

Waist circumference• The waist circumference is measured with a
flexible tape placed on a horizontal plane at the level of the iliac crest as seen from the anterior view .
• In adults with a BMI of 25 to 34.9 kg/m2, a waist circumference greater than 102 cm for men and 88 cm for women is associated with a greater risk of hypertension, type 2 diabetes, and dys-lipidemia, and IHD .
• In patients with a BMI ≥ 35 kg/m2, measurement of waist circumference is less helpful since it adds little to the predictive power of the disease risk classification of BMI; almost all individuals with this BMI also have an abnormal waist circumference.

Determine etiology
• Most cases of obesity are related to non-medical disorders such as a sedentary lifestyle and increased caloric intake.
• Medications are a common cause of weight gain and obesity, in particular corticosteroid , insulin, sulfonylureas, and antipsychotics.
• Smoking cessation is also associated with weight gain
• Although uncommon, some obese patients have an endocrine disorder such as Cushing's syndrome , hypo-thyroidism .

Effect of obesity on sleep architecture in the absence of SDB• The excessive daytime sleepiness in the
severely obese without OSA could be due to a disruption of sleep homeostasis due to obesity per se which occurs as a consequence of poor sleep quality.
• Proinflammatory somnogenic cytokines released by the adipose tissue such as Il-6 and TNF-alpha have been hypothesized to cause daytime sleepiness and fatigue in obese subjects who do not suffer from OSA .
• Lighter and more fragmented sleep, longer sleep latency and less rapid eye movement sleep. with markedly reduced amounts of the deepest non-REM sleep compared to lean controls

Impact of obesity on sleep-disordered breathing• The most common type of sleep-disordered
breathing (SDB) is OSA.• These obstructive respiratory events are associated
with cortical arousals and oxygen desaturation leading to sleep fragmentation, chronic sleep loss, and increased sympathetic neural activity.
• Clinical symptoms suggestive of OSA include loud snoring, breathing pauses witnessed by a bed-partner, choking or gasping during sleep, morning headaches, insomnia, and daytime sleepiness.
• A number of health related conditions have been associated with OSA including diminished neurocognitive function, increased risk of motor vehicle accidents, reduced quality of life, hypertension, insulin resistance, and cardiovascular diseases.

Epidemiology of OSA• High prevalence rates of OSA and OSA syndrome
in various geographic regions and amongst a range of ethnic groups This “epidemic” of OSA is closely related to the obesity epidemic.
• Up to 80% of cases of moderate or severe OSA have gone undiagnosed despite adequate access to health care
• The prevalence of OSA (AHI >5) in middle-aged adults between 30 and 60 years of age was 9% for women and 24% for men. The OSA syndrome, characterized by both an AHI>5 along with EDS was present in 2% of women and 4% of men.

Obesity as a risk factor for OSA• The strongest risk factor is obesity reflected
by several markers including BMI, neck circumference, and waist-to-hip ratio. more than
half of the prevalence of OSA is attributable to excess body weight .
• Other risk factors include aging , male gender, menopause, craniofacial abnormalities, upper airway anatomy, smoking, alcohol, and genetic predisposition.

What is the most appropriate treatment? • Treatments for obesity either decrease
energy intake or increase energy expenditure.
• Behavior therapy (modifying food intake, physical activity, and controlling stimuli in the environment that trigger eating ) is one cornerstone in the treatment for obesity. These are conducted by psychologists .
• Drug therapy (Orlistat , Lipase Inhibitor ,120 mg 3 times/day with each main meal containing fat ) .
• While the medical management of obesity is relatively ineffective, bariatric surgery is the most successful method for sustained weight loss and markedly reduces obesity-related morbidity and mortality.
National Institutes of Health guidelines for surgery
• Be well-informed and motivated• Have a BMI ≥40 kg/m2• Have acceptable risk for surgery• Have failed previous non-surgical weight
loss• BMI ≥35 kg/m2 who have serious co-
morbidities such as severe diabetes, sleep apnea, or joint disease may also be candidates.

Liposuction • Removal of fat by aspiration after
injection of physiologic saline has been used to remove and contour subcutaneous fat.
• While this can result in a significant reduction in fat mass and weight, it does not appear to improve insulin sensitivity or risk factors for coronary heart disease.

Bariatric surgical procedures• Restrictive, in which the gastric
volume is reduced to decrease energy intake.
• Malabsorptive, in which portions of the small intestine are bypassed to reduce energy absorption.
• Combined restrictive and mal-absorptive.

Laparoscopic Sleeve gastrectomy


Gastric Banding
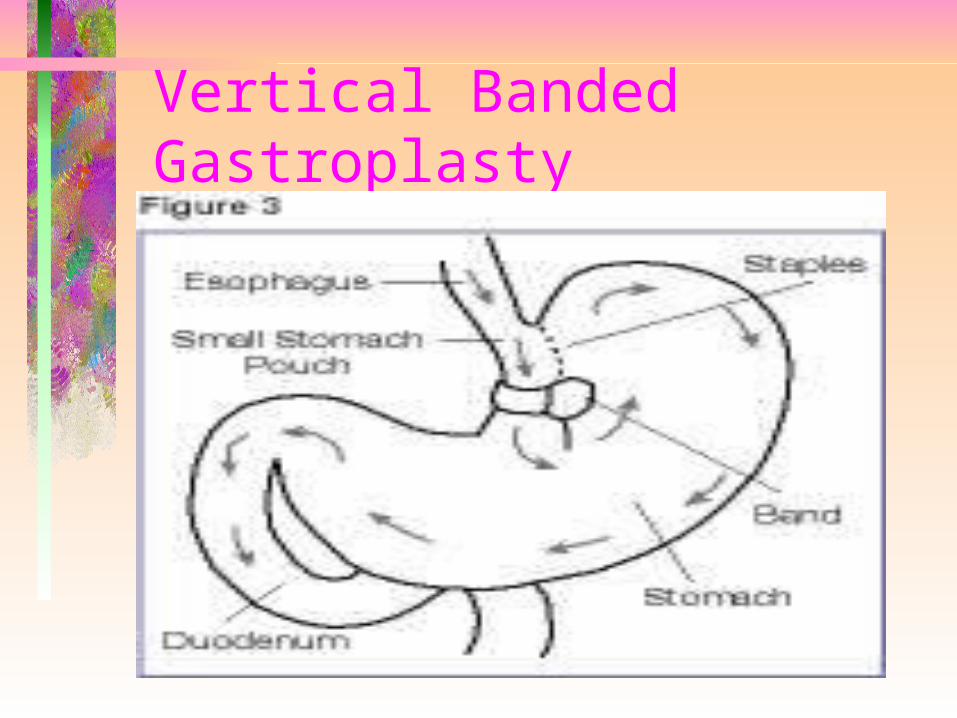
Vertical Banded Gastroplasty

Roux-en-Y Gastric Bypass

Bariatric surgical Benfits• Gastric banding and gastroplasty
("stomach stapling") are restrictive procedures that decrease the stomach size from about six cups to one.
• Malabsorptive procedures, which block food absorption, include gastric bypass.
• "Roux-en-Y" gastric bypass combines both approaches and is the most common weight loss surgery in the U.S. It reduces the size of the stomach and prevents the absorption of calories in the small intestine.
Impact of surgical weight loss on the sleep architecture• Significant improvement in sleep
efficiency and latency to REM sleep.• Increase in the duration of stage 3 and
4 of non-REM sleep • Increased in REM sleep.Impact of non-surgical weight loss on OSA• lifestyle modifications leading to
significant weight loss can be an effective intervention in patients with mild to moderate OSA.

Impact of surgical weight loss on OSA symptoms• The significant weight loss seen in these
patients led to dramatic improvements in self-reporting of frequent apneas, snoring, and EDS .
• The degree of improvement in sleep apnea symptoms was related to the degree of weight loss achieved.
• Despite the dramatic weight loss and improvement in symptoms, a proportion of patients remained symptomatic.
• Such a high cure rate based on subjective symptom improvement is unreliable since there is a poor correlation between symptoms of OSA and severity of the disease based on the AHI.

Impact of surgical weight loss on polysomnographic measures of OSA• Only 38% achieved cure defined as AHI <5/h.• 62% of patients had residual disease with
the mean residual AHI of 16 events per hour. • some patients still have moderate OSA after
maximum weight loss and could therefore benefit from CPAP therapy.
• Recommendation of formal reevaluation of OSA severity with polysomnography after maximum weight loss.
• The pressure requirements decrease with significant weight loss


Obesity hypoventilation syndrome• Alveolar hypoventilation and daytime respiratory
failure (awake PaCO2> 45 mmHg) in patients with a BMI> 30 kg/m2 and sleep disordered breathing .
• This disorder is diagnosed after other possible causes of hypoventilation such as lung, neuromuscular or chest wall deformities have been excluded.
• The incidence of OHS rises significantly as obesity increases, with a reported prevalence of around 10-20% in outpatients presenting to sleep clinics, to almost 50% of hospitalised patients with a BMI > 50 kg/m2.
• Unfortunately it is also one that is frequently overlooked, despite the significant co-morbidities and higher hospitalization rates these individuals experience.

The sources of respiratory abnormality in OHS1-Alterations in pulmonary function2-Changes in ventilatory control3-Sleep breathing abnormalities.• The majority of morbidly obese individuals
are able to compensate for the abnormalities imposed by their excessive weight, maintaining daytime eucapnia.
• OHS emerges only when compensatory mechanisms fail or become overwhelmed.
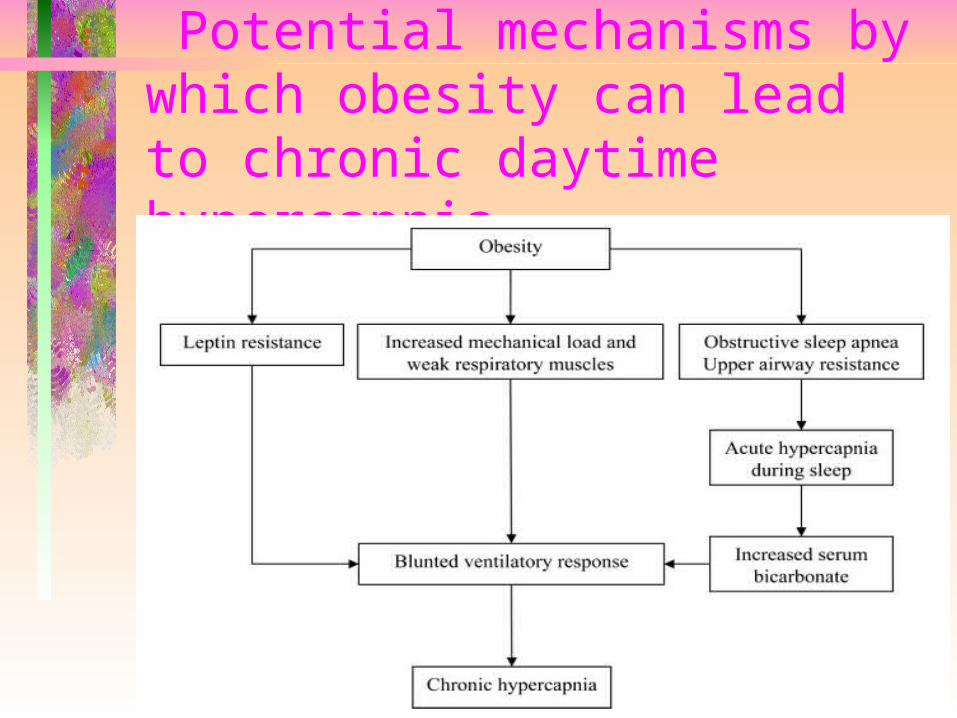
Potential mechanisms by which obesity can lead to chronic daytime hypercapnia.

Alterations in pulmonary function• Fat accumulation around the abdomen and
chest wall imposes a significant load on the respiratory system such that lung volumes are reduced, while marked changes in respiratory system compliance and airway resistance contribute to a high work of breathing.
• TLC ,ERV and FRC are all reduced, and these changes are more evident in OHS than eucapnic patients even at similar levels of BMI.
• A central pattern of obesity is associated with more severely compromised lung volumes than obese patients with a lower body obesity pattern.
• Individuals with OHS have larger neck circumferences and higher waist: hip ratios than those with eucapnic obesity or OSA, reflecting greater degrees of central obesity.

Alterations in pulmonary function• Breathing at low lung volumes significantly
reduce both chest wall and lung compliance, while increasing airway resistance.
• By breathing at low lung volumes, small airway closure during exhalation is more likely, creating expiratory flow limitation and intrinsic positive end expiratory pressure (PEEPi). This in turn increases the work of breathing by imposing a threshold load on the inspiratory muscles.
• Low ERV worsen ventilation-perfusion matching particularly in the supine position.

Sleep disordered breathing
• In the majority of individuals with OHS, upper airway obstruction during sleep will be present.
• In 10-15% the primary abnormality will be purely sleep hypoventilation characterised by sustained periods of low saturation and increased CO2 without obvious apneic or hypopneic events

Ventilatory control• Respiratory drive is significantly increased in
morbidly obese individuals who maintain eucapnia .Neural drives in morbidly obese individuals that were two to three times greater than those measured in non-obese controls.
• Patients with OHS fail to augment drive to compensate for the added load created by excess weight, permitting a gradual rise in CO2 to occur.
• Ventilatory responsiveness to both hypoxia and hypercapnia are attenuated in OHS patients compared to normal weight subjects and eucapnic obese patients with or without OSA.
• The increased bicarbonate seen in patients with OHS would blunt ventilatory responsiveness to CO2.

Leptin and OHS• In severely obese individuals, higher
concentrations of serum leptin are associated with a reduced respiratory drive and a reduced hypercapnic response.
• The stimulatory effects of leptin on ventilation are reduced in some individuals, which would predispose them to the development of hypercapnia.
• leptin “resistance” may contribute to the more severe alterations in pulmonary mechanics seen in patients with OHS compared to those with eucapnic obesity.
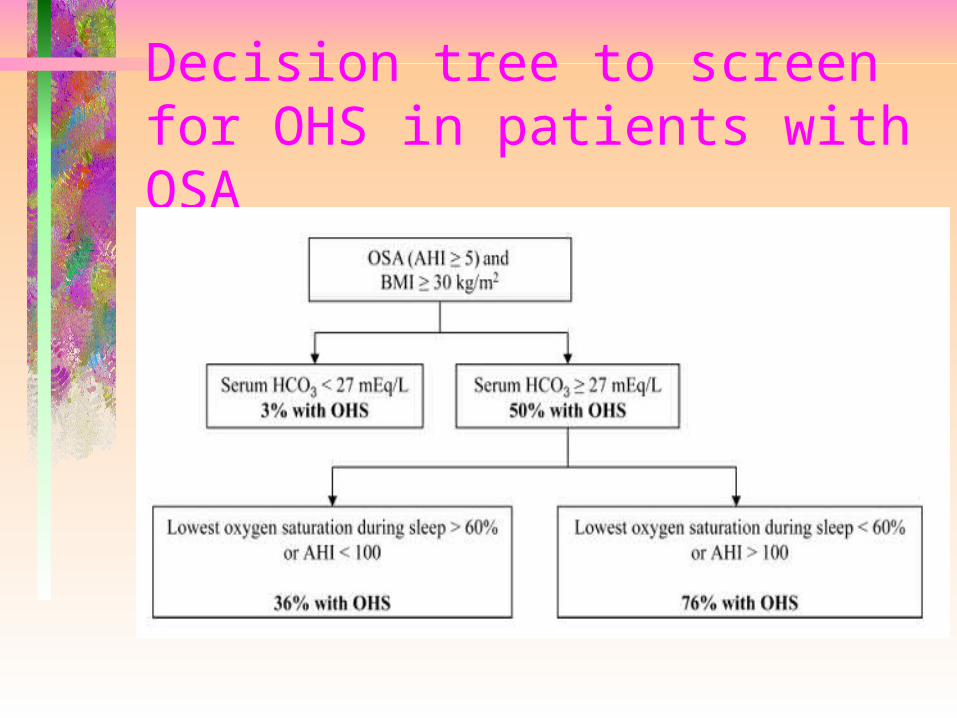
Decision tree to screen for OHS in patients with OSA

Comorbidities Reported in Patients With OHS•Hypertension•Heart failure•Pulmonary hypertension•Type 2 diabetes mellitus•Asthma•Erythrocytosis
Impact of surgical weight loss on OHS• Only one study has examined the
impact of bariatric surgery in patients with the obesity hypoventilation syndrome .
• In 31 patients, preoperative (PaO2) increased from 53 to 73 mmHg one year after surgery, and (PaCO2) decreased from 53 to 44 mm Hg.

Surgical weight loss and impact on Type 2 diabetes mellitus• Diabetes resolution, (ability to maintain
euglycemia after discontinuing all diabetes–related medications), was achieved in more than 75% of the patients across all procedures, while up to 85% of patients experienced demonstrable improvement..
• Restrictive bariatric surgeries induce an improvement of diabetes diabetes that is proportional to the degree of weight loss
• Improvement of diabetes occurs early after mala-bsorptive bariatric procedures, before any significant weight loss has occurred.
Practice points• Bariatric surgery is the most effective
treatment for obesity• Despite improvement of subjective OSA
symptoms, some degree of OSA persists even after maximal surgical weight loss and therefore patients should be retested for OSA once their weight has stabilized after bariatric surgery.
• Obesity may affect sleep even in the absence of clinically significant OSA.
• Most of the improvement of the metabolic syndrome (glucose homeostasis ,dyslipedemia and blood pressure) may occur shortly after the surgical procedure,

Treatment OF OHS• Improvement in chronic daytime hypercapnia
and hypoxia with PAP therapy (CPAP or bilevel PAP).
• Approximately half of patients with OHS require oxygen therapy in addition to PAP therapy upon initiation of treatment.
• Autoadjusting PAP technology can be used in patients with simple OSA to bypass laboratory-based titration studies, this technology cannot be recommended in patients with OHS because it does not have the ability to recognize hypoventilation and hypoxemia. As a result, patients with OHS require a laboratory-based PAP therapy and oxygen titration.

CPAP Therapy: Given that the majority of patientswith OHS have concomitant severe OSA, treatmentwith CPAP seems reasonable.
• The improvement in hypercapnia and hypoxia is directly related to the daily dose of PAP therapy, and maximum improvement in blood gas levels is achieved as early as 1 month after the start of therapy.
• In a study of 75 ambulatory patients with OHS, 17 Paco2 decreased by 1.8 mm Hg and Pao2 increased by 3 mm Hg per hour of daily CPAP or bilevel PAP use.
• up to 25% of patients who are adherent to PAP therapy do not become eucapnic .


Bilevel PAP therapy• Should be considered if during PAP titration
the oxygen saturation remains persistently below 90% after the resolution of apneas, hypopneas, and flow limitation with CPAP therapy , if the Paco2 does not normalize after 1 to 2 months of therapy with CPAP
• If the oxygen saturation remains persistently below 90% after the resolution of apneas, hypopneas, and flow limitation, IPAP should be added to the final EPAP to improve ventilation.
• In patients with OHS who do not have OSA, EPAP can be set at 5cmH2O and IPAP can be titrated to improve ventilation.
• Many patients with OHS who initially require bilevel PAP therapy can be switched to CPAP therapy after the resolution of hypercapnia.
• Bilevel PAP therapy might prevent endotracheal intubation and invasive mechanical ventilation in patients with OHS during acute-on-chronic respiratory failure.

Reasons for Lack of Improvement ofHypercapnia With PAP Therapy in Patients With OHS
• Inadequate adherence with PAP therapy• Inadequate PAP titration• Sleep-disordered breathing other than
OSA (central hypoventilation)• Unidentified respiratory disease (ie,
COPD and interstitial lung disease)• Unidentified hypothyroidism or
neuromuscular disease• Metabolic alkalosis (ie, due to high
doses of loop diuretics)

Average Volume-Assured Pressure Support (AVAPS)• AVAPS, a hybrid mode that delivers a more
consistent tidal volume with the comfort of pressure support ventilation, has been compared to bilevel PAP in a randomized crossover trial, was more successful than bilevel PAP therapy in improving nocturnal and daytime ventilation (mean transcutaneous CO2 during sleep, 45 vs52 mm Hg, respectively; mean daytime Paco2,42 vs46 mm Hg, respectively.

Oxygen Therapy• Approximately half of patients with
OHS require supplemental nocturnal oxygen in addition to PAP therapy.
• The need for nocturnal and daytime oxygen therapy decreases significantly in patients who are adherent to PAP therapy.
• Supplemental oxygen without PAP therapy is inadequate and does not improve hypoventilation.

Summary • CPAP therapy is effective in the majority
of stable patients with OHS, particularly in the subgroup of patients who have severe OSA.
• Bilevel PAP therapy should be strongly considered in patients who do not respond to CPAP therapy, patients with OHS who experience acute-on-chronic respiratory failure, and in patients who have OHS without OSA.
• Whether AVAPS therapy has long-term benefits over bilevel PAP therapy remains uncertain.
• The treatment of OHS with PAP improves blood gas levels, morning headaches, excessive daytime sleepiness and vigilance, dyspnea, pulmonary hypertension, and leg edema.

Summary• Improvements in symptoms and blood gas
levels are directly related to adherence with therapy ,and maximum improvement in blood gas levels can be achieved as early as after 2 to 4 weeks of therapy.
• Early follow-up should include repeat measurement of arterial blood gases and objective assessment of adherence with PAP therapy as patients frequently overestimate adherence.
• Changes in serum bicarbonate level and pulse oximetry could be used as a less invasive measure of ventilation.
• Changing bilevel PAP to CPAP therapy and discontinuing oxygen therapy when no longer indicated can decrease the cost of therapy in patients with OHS.
