old unreduced dislocations
TRANSCRIPT
OLD UNREDUCED DISLOCATIONSCAMPBELL'S OPERATIVE ORTHOPAEDICS 2013
BY: DR HAMID HEJRATI
RESIDENT OF ORTHOPEADIC SURGERY
IRAN, MASHAD UNIVERSITY OF MEDICAL SIENCE
OLD UNREDUCED HIP DISLOCATIONS
Old unreduced dislocations of the hip are relatively uncommon in adults the result of a
motor vehicle accident
also caused head injury, fracture of the ipsilateral femur, or dislocation or fracture of the
opposite hip, which drew attention away from the dislocation.
In developing countries, unreduced traumatic dislocations are seen more frequently. The
various treatment possibilities include closed reduction, open reduction, heavy traction and
abduction, subtrochanteric osteotomy, Girdlestone procedure, arthrodesis, endoprosthetic
replacement, and total hip replacement.
Like acute dislocations, unreduced dislocations can be classified as anterior or posterior.

CHRONIC UNREDUCED (OLD) ANTERIOR DISLOCATIONS
Traumatic anterior dislocation of the hip is a comparatively rare injury.
Trochanteric osteotomy has been reported to correct the deformity and improve body
mechanics and balance. Although trochanteric osteotomy may give a stable hip, long-term
results are not known. Subsequent salvage operations, such as total hip arthroplasty may be
more difficult if the proximal femoral anatomy is distorted.
INTERTROCHANTERIC OSTEOTOMY FOR CHRONIC ANTERIOR
DISLOCATION OF THE HIP
• The Gibson approach is used (see Technique 1-61).
• Divide the femur along the line joining the greater and lesser trochanters. Then adduct,
extend, and internally rotate the limb.
POSTOPERATIVE CARE The patient is kept in skin traction for 6 weeks to prevent recurrence of
the rotational deformity. The patient is allowed to walk with crutches 6 weeks after surgery, and
full weight bearing is allowed in 3 to 4 months. Hamada recommended postoperative
immobilization in a plaster one and one-half spica cast, which includes the normal leg down to
the knee. With intertrochanteric osteotomy, early union usually is complete in 3 to 4 months.

Gibson posterolateralapproach to hip joint. A, Skin incision. B,
Anterior and posterior muscle masses have been retracted to expose greater trochanter and muscles that insert into it. C, Gluteus mediusand minimus have been divided near their insertions into greater trochanter and retracted. Incision in capsule is shown. D, Hip joint has been dislocated by flexing, abducting, and externally rotating thigh.
CHRONIC UNREDUCED (OLD) ANTERIOR DISLOCATIONS
Nagi et al. used a modified Girdlestone arthroplasty in four patients with unreduced anterior hip dislocations. the femoral neck is exposed through an anterior Smith-Petersen approach
or a Watson- Jones anterolateral approach. A subcapital osteotomy is performed, attempting
to leave as much of the femoral neck as possible with the distal fragment. By manipulating the
leg, the cut femoral neck is displaced upward into the acetabulum.
Postoperative skeletal traction of 5 kg is maintained for 6 weeks. Gentle active hip flexion is
started 10 days after surgery, and non-weight bearing with crutches is begun at 6 weeks.
Gradual weight bearing is started at 3 months.

CHRONIC UNREDUCED (OLD) ANTERIOR DISLOCATIONS
These authors believe that preservation of the femoral neck makes subsequent total
hip arthroplasty easier. They recommended this modified subcapital displacement
osteotomy for:
neglected anterior dislocation of the hip treated 6 months or more after dislocation
In young patients to serve as a temporizing procedure until definitive total hip arthroplasty is
performed later.

CHRONIC UNREDUCED (OLD) POSTERIOR DISLOCATIONS
Much more common than the anterior type.
Two factors that have been reported to contribute to poor results in posterior dislocations are:
1. fracture of the femoral head or medial acetabular wall (Epstein types IV and V)
2. osteonecrosis, an unpredictable event that may not become apparent on plain radiographs for many months.
Primary reconstructive procedures have been shown to give the best results. Although the viability of the femoral head in old unreduced posterior dislocations should determine treatment, use of bone scan or MRI to detect the vascularity of the femoral head before beginning treatment is not mentioned in the literature. In young patients, if the femoral head is thought to be viable, an effort should be made to save it.

CHRONIC UNREDUCED (OLD) POSTERIOR DISLOCATIONS
For a type I posterior hip dislocation (no fracture or only a minor fracture of the acetabular rim less than 12weeks from injury), with a viable femoral head, closed reduction under general anesthesia is recommended. After 12 weeks, the acetabulum may fill with fibrous tissue, making a concentric closed reduction impossible. If closed reduction fails, heavy traction and abduction should be considered, as described by Gupta and Shravat. If the type I posterior hip dislocation with a viable femoral head has been present for more than 12 weeks, a concentric reduction most often cannot be obtained with closed reduction or heavy traction and abduction, and open reduction is indicated.

CHRONIC UNREDUCED (OLD) POSTERIOR DISLOCATIONS
The success of the heavy traction technique depends on achieving a concentric reduction. If the reduction is not concentric, an open reduction to debride any interposed soft tissue or bone fragments is necessary.
Type 1 <12 w CR under GA or with heavy traction and abduction
>12 w CR under GA or with heavy traction and abduction may not be successful and open reduction is indicated

TRACTION AND ABDUCTION FOR CHRONIC POSTERIOR HIP
DISLOCATION (GUPTA AND SHRAVAT) • Place a tibial traction pin in the region
of the tibial tubercle and place the patient in 18 kg of skeletal traction. The patient is kept in traction and under sedation and muscle relaxation during this time.
• Obtain radiographs on alternate days. Usually by the fifth day the femoral head should be at or below the level of the acetabulum.
• Gradually abduct the limb and reduce the traction 3.6 kg every fourth day.
• Once the femoral head has been reduced into the acetabulum, maintain 7 kg of traction for the next 2 weeks.
• Remove the traction and begin non-weight-bearing exercises for the next 4 weeks. Weight bearing is not allowed for 3 months.
CHRONIC UNREDUCED (OLD) POSTERIOR DISLOCATIONS
For posterior hip dislocations with a viable femoral head that are type II (large uncomminuted fracture of the posterior acetabular rim) or type III (comminuted fracture of the posterior acetabular rim), open reduction and internal fixation should be considered if the injury is less than 3 months old. If the head of the femur is displaced superiorly, preoperative skeletal traction is necessary. With reduction thus accomplished, it is necessary to fix the bone fragments internally to restore stability.

CHRONIC UNREDUCED (OLD) POSTERIOR DISLOCATIONS
Total hip arthroplasty is recommended for hips with posterior dislocations categorized as type IV (fracture of the acetabular rim and floor) or type V (fracture of the femoral head with or without other fractures) that have been dislocated for more than 3 months. Because of osteonecrosis, poor results have been noted in these types of fracture-dislocations even in some patients who had reduction within 24 hours after injury. If the femoral head is thought to be avascular on MRI or bone scan, a primary reconstructive procedure should be considered rather than open or closed reduction.
CHRONIC UNREDUCED (OLD) POSTERIOR DISLOCATIONS
In young patients, arthrodesis can be considered, although successful fusion may be difficult in
the presence of osteonecrosis. As with any arthrodesis of the hip, the status of the ipsilateral
knee, the contralateral hip, and the lumbar spine must be considered.
Subtrochanteric osteotomy also has been used for late unreduced dislocations of the hip in
areas of the world where arthroplasty or endoprosthetic replacements are not readily
available. This procedure may be indicated for patients who are relatively pain free and have
a reasonable range of hip flexion but have joint contracture or limb-length inequality.
CHRONIC UNREDUCED (OLD) POSTERIOR DISLOCATIONS
The best results in the series by Garrett et al. were obtained after total hip arthroplasty. The
main problem encountered was the creation of adequate acetabular stock when the
posterior acetabular lip was fractured or displaced. This is accomplished by open reduction
and internal fixation of the fracture fragment or by use of the femoral head as a bone graft.
Ilyas and Rabbani reported total hip arthroplasty with bone grafting in 15patients with chronic
(over 6-month history) posterior dislocations. Their short- to mid-term results were quite
satisfactory, especially considering the complex nature of these particular arthroplasties.

OLD UNREDUCED SHOULDER DISLOCATIONS

OLD UNREDUCED SHOULDER DISLOCATIONS
usually occur in patients older than 50 years.
The complaints A. Limitation of motion.
B. Pain which is usually is caused by attempts to move the shoulder beyond its
restricted range.
These old dislocations most often are traumatic but frequently have been produced by a
trivial injury as a result of the patient's increasing age and weakness and degeneration of the
soft tissue around the glenohumeral joint, such as the rotator cuff and subscapularis tendon.

OLD UNREDUCED SHOULDER DISLOCATIONS
In younger patients, unreduced dislocations often occur in those with alcoholism, seizures, or
multiple trauma. Many of these dislocations are complicated by fractures of the glenoid
cavity, tuberosities, or other parts of the humerus. More than one third are complicated by
neurological deficits.
Loss of motion is the chief clinical finding; abduction and internal rotation are restricted in old
anterior dislocations, and abduction and external rotation are restricted in old posterior
dislocations.
OLD UNREDUCED SHOULDER DISLOCATIONS
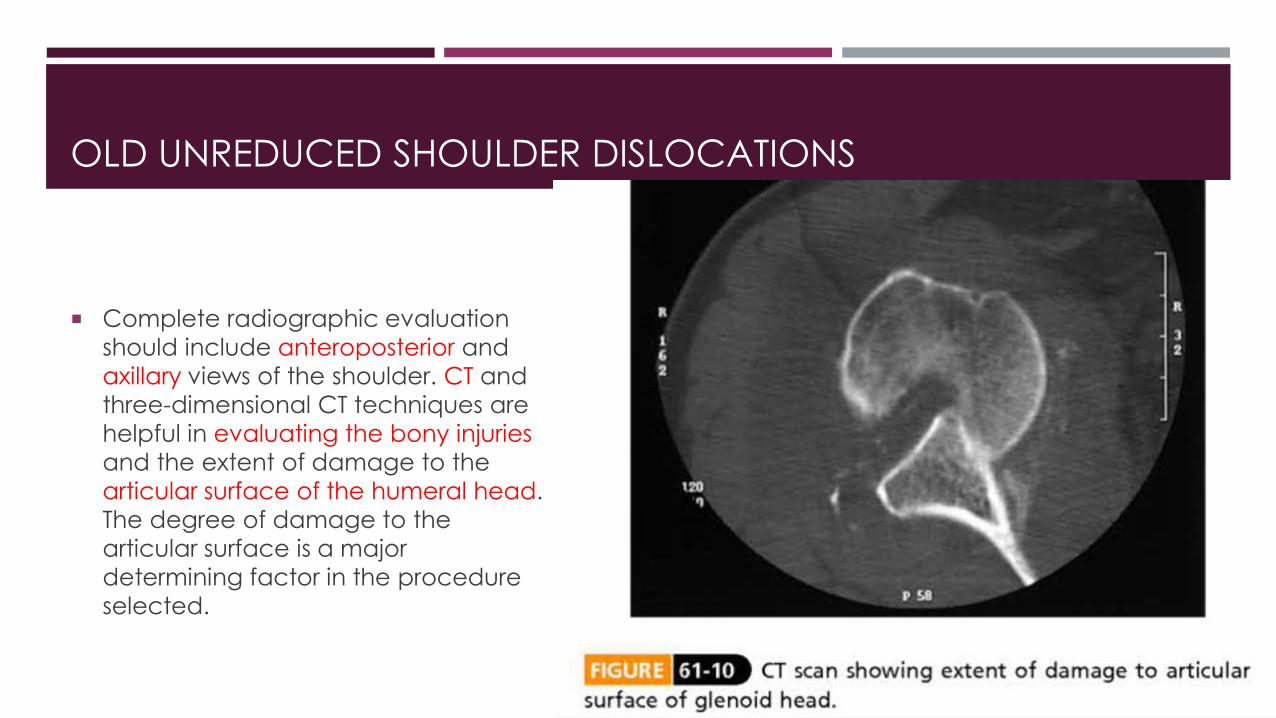
Complete radiographic evaluation
should include anteroposterior and
axillary views of the shoulder. CT and
three-dimensional CT techniques are
helpful in evaluating the bony injuries
and the extent of damage to the
articular surface of the humeral head.
The degree of damage to the
articular surface is a major
determining factor in the procedure
selected.

OLD UNREDUCED SHOULDER DISLOCATIONS
After a few weeks, fibrous and capsular contractures occur across the base of the glenoid. The
rotator cuff muscles also are contracted. The fibrosis can include other structures, such as the
axillary artery and nerve.
The natural anatomy is therefore often markedly distorted. Neviaser has described a capsular
"bowstringing" phenomenon. The capsule itself becomes adherent in the glenoid fossa,
preventing closed reduction.

OLD UNREDUCED SHOULDER DISLOCATIONS
Bony pathological change also is often
seen. In chronic anterior dislocations, a
compression fracture occurs in the
posterolateral aspect of the humeral
head, where it impinges against the
anterior glenoid rim. Because of the
repeated efforts of the patient to achieve
normal motion in the glenohumeral joint,
this lesion often is larger than the usual Hill-
Sachs lesion seen in recurring anterior
dislocations of the shoulder.

OLD UNREDUCED SHOULDER DISLOCATIONS
There are also compression
fractures of the apposing glenoid
rim or sometimes a
pseudoarticulation with the
scapula.

In chronic posterior dislocations, a bony
lesion similar to the Hill-Sachs lesion of
recurring anterior dislocations is found.
This is a compression fracture caused by
impingement of the posterior rim of the
glenoid on the anteromedial aspect of
the humeral head. These lesions also
are usually large because of the
patient's continual attempts to increase
the range of motion of the affected
joint.

TREATMENT
The treatment options for an old unreduced dislocation of the shoulder no treatment,
closed reduction (arthroscopic assisted), open reduction, hemiarthroplasty, and total shoulder
replacement.
Not all patients with old unreduced dislocations of the shoulder require treatment. In some
patients, although motion is limited and slightly uncomfortable, the upper extremity remains
functional. Also, if a patient is inactive and a poor risk for surgery, the option of no surgical
treatment should be considered.
TREATMENT
Patients with posterior dislocations who were not treated have been shown to have better
results than those with untreated anterior dislocations.
In unreduced posterior dislocations, the arm rests at the side in internal rotation, allowing the
patient to reach the face, head, and rear of the body.
The arm of a patient with an unreduced anterior dislocation is held away from the body in
external rotation, making it difficult to reach the face and impossible to reach the back.

CLOSE REDUCTION
As emphasized by many authors, manipulative reduction should not be undertaken before the
patient's age, the degree of osteoporosis of the humerus, the vascular status, and the duration
of the dislocation are all carefully considered. The size of the humeral depression defect also
should be taken into account.
A few cases of closed reduction of shoulders that have been dislocated for more than 4 weeks
have been reported in the literature. After this time, the soft tissue contractures, the fibrous
tissue within the glenoid cavity, and the retracted rotator cuff muscles usually make closed
reduction impossible.
CLOSE REDUCTION In general, it may be unwise to attempt closed reduction for a shoulder with an impression
defect involving more than 20% of the articular surface of the humeral head or for a shoulder
that has been dislocated for more than 3 to 4 weeks.
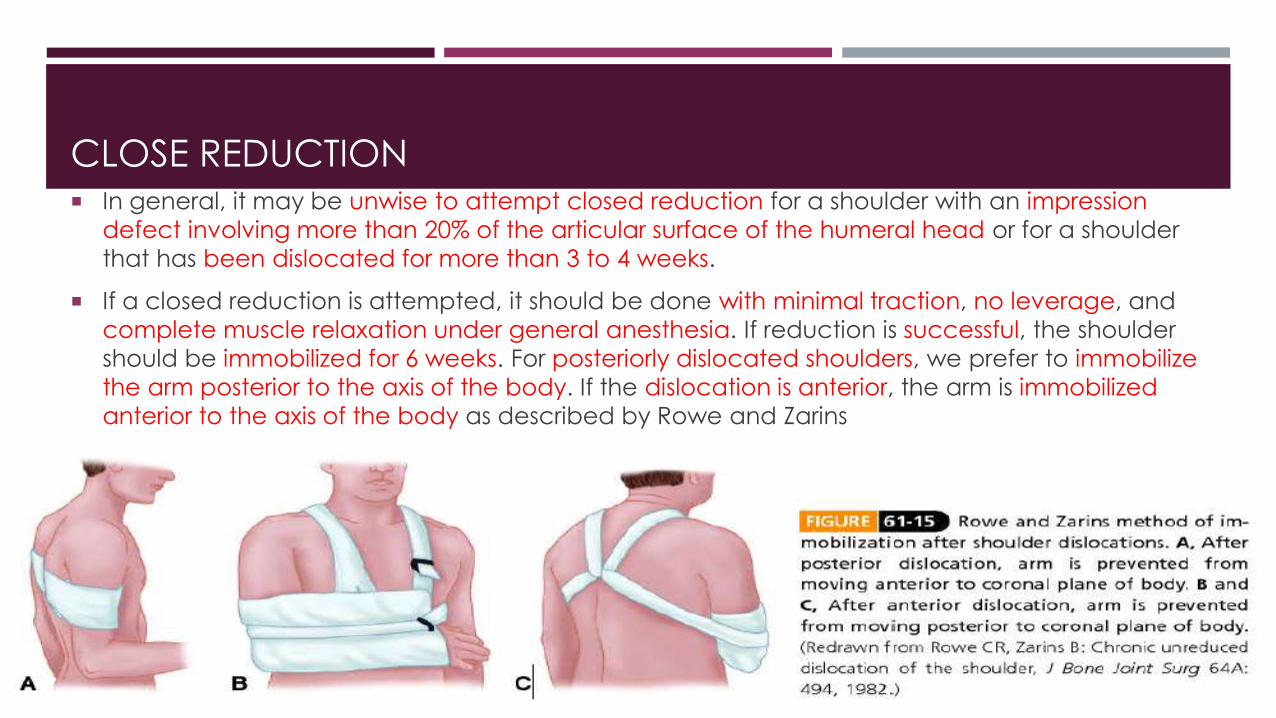
If a closed reduction is attempted, it should be done with minimal traction, no leverage, and
complete muscle relaxation under general anesthesia. If reduction is successful, the shoulder
should be immobilized for 6 weeks. For posteriorly dislocated shoulders, we prefer to immobilize
the arm posterior to the axis of the body. If the dislocation is anterior, the arm is immobilized
anterior to the axis of the body as described by Rowe and Zarins
OPEN REDUCTION
Two obstacles generally are encountered with open reduction. The first is difficulty in replacing
the humeral head because of fibrosis, shortening of the muscle, contracture, bowstringing of
the capsule across the glenoid cavity, defect of the articular surface in the humeral head at
the point of impingement at the glenoid, and scar tissue in the glenoid fossa. The second
obstacle is difficulty maintaining reduction because of instability.

OPEN REDUCTION
When an open reduction is performed, it often is necessary to prevent recurrent dislocations
caused by the humeral head defect. This problem generally is encountered more often in old
unreduced posterior dislocations than in anterior dislocations. McLaughlin recommended filling
the defect in the anterior part of the humeral head with the subscapularis tendon (A and B).
Neer described the technique of transplanting the subscapularis tendon with the lesser
tuberosity attached(C).

OPEN REDUCTION Rockwood recommended a posterior approach for old unreduced posterior dislocations of
the shoulder if the anteromedial humeral head defect is less than 15%. If the head defect is greater than 15%, an anterior reconstruction through an anterior approach is recommended. Superior and anteromedial approaches for open reduction of these posterior dislocations also have been advocated.
Elshewy et al. treated chronic posterior dislocations (with head defect less than 25%) by reduction, and then posterior capsular shift as described by Neer, with good pain relief and reasonable functional improvement.

OPEN REDUCTION
A humeral rotational osteotomy has
been described for patients who have
locked posterior shoulder dislocations
and meet the following criteria: (1)
healthy articular cartilage, (2) humeral
head defect involving less than 40% of
the articular surface, and (3) ability to
participate in an active rehabilitation
program.

OPEN REDUCTION
Internal fixation may be a helpful (or necessary) adjunct to open reduction. A Swiss screw or
crossed Kirschner wires through the acromion into the humeral head have been described.
OPEN REDUCTION
Goga used Kirschner wire fixation in anterior dislocations but also transferred the coracoid to
the glenoid.
Rowe and Zarins found it unnecessary to transfix the shoulder joint at all; they recommended
simply supporting the arm at the side in a position anterior to the coronal plane of the body for
anterior dislocations and posterior to the coronal plane for posterior dislocations.

OPEN REDUCTION
Full function of the shoulder rarely is regained after this operation. Motion is often limited,
especially in abduction and external rotation. The patient therefore should not expect full
recovery, but some improvement in shoulder function should be expected.
OPEN REDUCTION
Approaches and techniques for open reduction in Campbell
A. OPEN REDUCTION OF ANTERIOR SHOULDER DISLOCATIONS
B. OPEN REDUCTION OF POSTERIOR SHOULDER DISLOCATION FROM A SUPERIOR APPROACH
C. OPEN REDUCTION OF POSTERIOR SHOULDER DISLOCATION THROUGH AN ANTEROMEDIAL APPROACH
D. DELTOPECTORAL APPROACH FOR POSTERIOR SHOULDER DISLOCATION

HEMIARTHROPLASTY
For very old (longer than 6 months) dislocations or for large head defects (larger than 45% to
50%), most authors suggest proceeding directly to arthroplasty, using hemiarthroplasty if the
glenoid is normal and if the dislocation is more than 6months old or the defect involves more
than 45% of the articular surface as seen on the axillary radiograph or CT scan.
For a posterior shoulder dislocation that has been present for more than 6 months, the humeral
component is placed in approximately neutral version.
For a posterior shoulder dislocation that has been present for less than 6 months, the
component is placed in approximately 20 degrees of retroversion.

TOTAL SHOULDER ARTHROPLASTY
Total shoulder replacement is recommended if the glenoid has been destroyed and the
dislocation is more than 6 months old or the defect involves more than 45% of the articular
surface.
The longer the dislocation has been present, the more retroversion must be
reduced. The correct amount of version can be determined by inserting trial components
and testing the stability of the shoulder at the time of surgery, making adjustments if required.
