operative dentistry motamiz oprd 41 lectures lecture 4 wed
TRANSCRIPT

Operative dentistry
Motamiz OPRD 41 Lectures
lecture 5
WED 15-4-2020

Patient Assessment, Examination,
Diagnosis and Treatment Planning

Examination of non carious lesions
1 Tooth wear
Erosion Attrition Abrasion
2 Developmental enamel hypocalcification
3 Fracture or craze line
Examination of non carious lesions
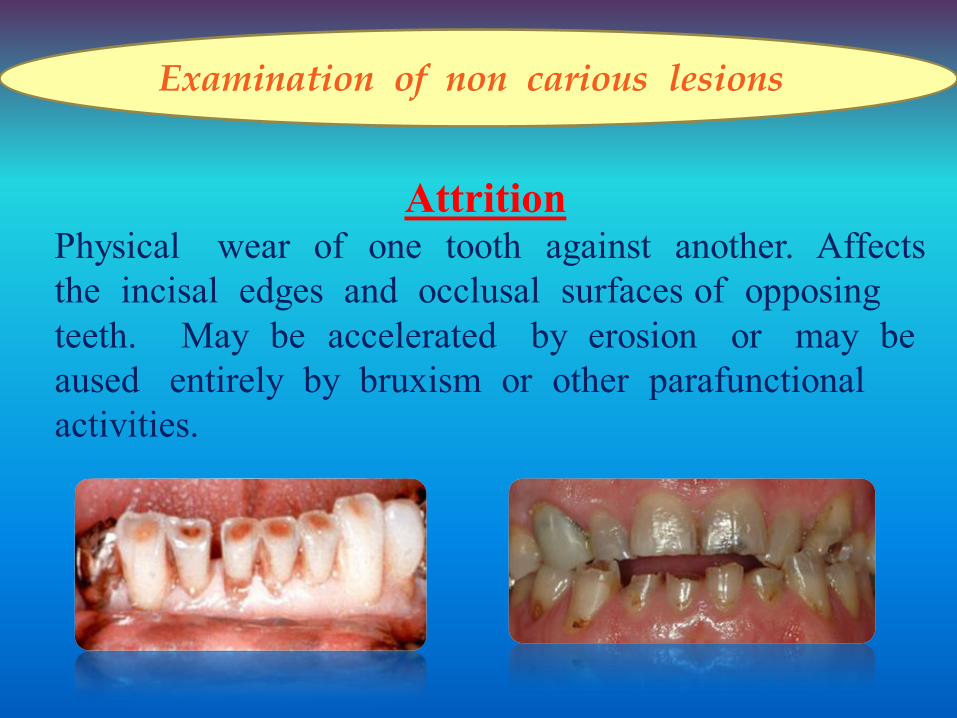
Attrition
Physical wear of one tooth against another. Affects
the incisal edges and occlusal surfaces of opposing
teeth. May be accelerated by erosion or may be
aused entirely by bruxism or other parafunctional
activities.

Examination of non carious lesions
Abrasion
Commonly affects the neck of the buccal surfaces of both
anterior and posterior teeth. The etiology is not clear, but
some dentists believe that it is caused by physical wear
from external agents such as:
- Abrasive toothpastes and powders.
- Hard toothbrushes or excessive use of other cleaning aids.
Examination of non carious lesions
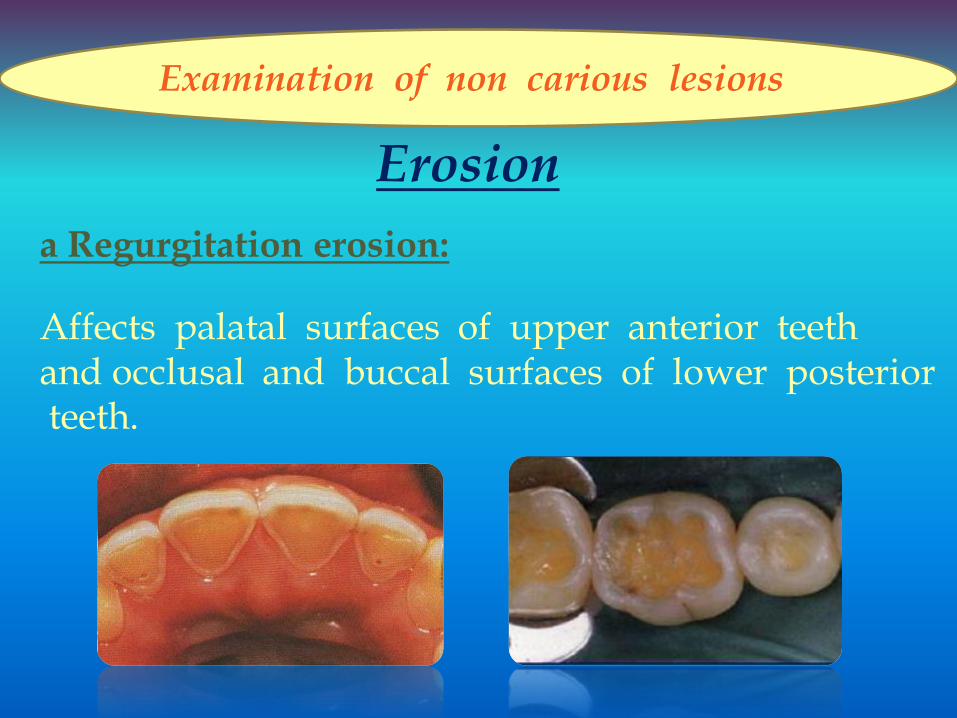
Erosion
a Regurgitation erosion:
Affects palatal surfaces of upper anterior teeth and occlusal and buccal surfaces of lower posterior teeth.

Examination of non carious lesions
Erosion
b Dietary erosion:
Affects the labial surfaces of
upper anterior teeth. Caused
by an excess of food and
drink with a low pH as Citrus
fruits, Pickles and carbonated
drinks.

Examination of non carious lesions
c Industrial erosion: Commonly affects the labial surfaces of the
upper anterior teeth and may cause pitting.
Caused by industrial processes which produce
acid fumes or droplets.
It is a cervical, wedge shaped defect that
is angular. Occur due to heavy force in
eccentric occlusion. It has the same clinical
features as abrasion but mare aggressive form.
Erosion
Abfracion

Examination of non carious lesions
2 Non hereditary developmental enamel
hypocalicification areas
It have man resulted factors
such as childhood fever, trauma
or fluorosis that occurred during
the developmental stages of tooth
formation. It is opaque white and
remain visible regardless if the
tooth is wet or dry.

Examination of non carious lesions
3- Fracture or craze line
It is usually occurs in teeth with extensive restoration,
weakened cusps and deep developmental fissures
across marginal or cusp ridges. It is detected by dye
material, light reflected from a dental mirror or
transillumination.

Examination of existing restorations
I Clinical examination of Amalgam restorations
Amalgam restorations can be examined using:
a Visual observation.
b Tactile sense with the explorer.
c Dental floss
d Radiographs (Bitewing).

Examination of existing restorations
Clinical examination of amalgam restorations may show:
(1) Amalgam blues (2) Proximal overhangs

Examination of existing restorations
(3) Marginal ditching
(4) Voids It occurs at the margins of amalgam restorations. It is
at least 0.3 mm deep. Small voids may be corrected
by recontouring or repairing with a small restoration.
It is the deterioration of the
amalgamtooth interface as a result
of wear, fracture or improper tooth
preparation.

Examination of existing restorations
(5) Fractures
(6) Improper anatomic contours
Proper anatomy Improper anatomy

Examination of existing restorations
(7) Improper proximal contacts
Proper contact
incompatibility ridge ) Marginal8(
caries ) Recurrent9(
Open contact & incompatible marginal ridge height

Examination of existing restorations
Examination of composite restorations
Ideal restoration Recurrent caries
Fractured restoration Marginal discoloration
Examination of existing restorations
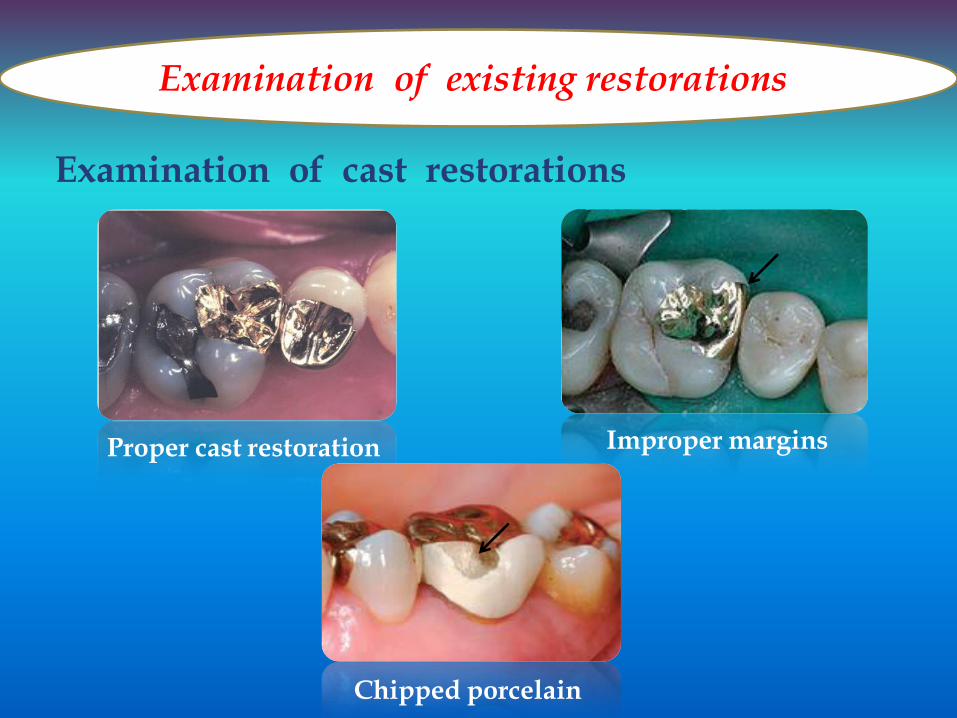
Examination of cast restorations
Proper cast restoration Improper margins
Chipped porcelain

Adjunctive aids for examination
1 Percussion: It is done by gentle tapping of
occlusal or incisal surfaces by the
use of mirror handle.
2 Palpation: It is rubbing the index finger along the facial and
lingual mucosa overlying the apical region to detect
a periapical pathosis in teeth showing tenderness to
Percussion

Adjunctive aids for examination
3 Vitality test •Cold: ethylchloride or
pencil of ice
• Hot: hot gutta percha or instrument
Thermal test
•No response means pulp death
•Tingling sensation means vital pulp.
Electric pulp tester

Adjunctive aids for examination
4 Cavity test: It used round bur without anesthesia, a cavity is made through the restoration into dentin.
5 Anesthetic test: It must be used anesthesia for the suspected tooth and if the symptoms subside, so affected tooth has been identified.
6 Study cast

Clinical examination of non caries lesions:
1- Tooth wear occurs naturally throughout life and so it is common to
find moderate degrees of wear in older people. Tooth wear happened
as a result of: Attrition, Abrasion, abfracture and Erosion.
Attrition:
It loss of hard tooth structure due to physical wear of contacting teeth
due to normal physiologic phenomenon as mastication. It affects incisal
edges and occlusal surfaces of opposing teeth. May be accelerated by
pathologic conditions as bruxism or other parafunctional activities.
Abrasion:
It is loss of hard tooth structure due to use of an external object e.g.
hard tooth brush, whitening tooth paste and smokers tooth powder. Also,
habits such as thread biting and pipe smoking can cause wear in the form
of notches in the incisal edges.
It commonly affects the neck of the buccal surfaces of both anterior
and posterior teeth. The surface of the defect is smooth and varies
according to the causative factor. The most common form of the lesion is
the wedge shaped defect resulting from excessive tooth-brushing.
Erosion:
Erosion is loss of hard tooth structure due to chemical agents as acids.
It is the most common and most damaging cause of tooth loss. There are
different types of erosion as:
a-Regurgitation erosion:
Commonly affects the palatal surfaces of upper anterior teeth and the
occlusal and buccal surfaces of lower posterior teeth. Caused by the
regurgitation of hydrochloric acid from the stomach in patients with:
Various digestive disorders.

Anorexia and bulimia nervosa.
Chronic alcoholism
Morning sickness associated with pregnancy.
Voluntary regurgitation.
b- Dietary erosion:
Commonly affects the labial surfaces of upper anterior teeth. Caused
by using food and drink with a low pH, including:
Citrus fruit and fruit juices (citric acid).
Pickles and other food and drink containing vinegar (acetic acid)
Carbonated drinks.
c- Industrial erosion:
Commonly affects the labial surfaces of the upper anterior teeth and
may cause pitting. Caused by industrial processes which produce acid
fumes or droplets.
Abfraction:
It is a cervical, wedge shaped defect that is angular. It is similar to
abrasion but in a more aggressive form. Occurs due to heavy occlusal
force associated with eccentric occlusion. It is hypothesized that bending
forces produce tension stresses at the neck of the affected teeth. These
stresses cause micro-fractures at the CEJ of the teeth resulted in a wedge
shaped or V shaped defect.
2- Non hereditary developmental enamel hypocalicification areas:
Many factors can resulted in enamel hypocalcification such as
childhood fever, trauma or fluorosis that occurred during the
developmental stages of tooth formation. It is opaque white and remains
visible regardless if the tooth is wet or dry.

3- Fracture or craze line:
Craze lines commonly appear in old age and considered as potential
cleavage planes for possible future fractures e.g. in teeth with extensive
restoration and weakened cusps and deep developmental fissures across
marginal or cusp ridges. It can be diagnosed using dye material or light
reflected from a dental mirror. Minor fractures can be treated by
recontouring but in extensive case the tooth should be restored.
Clinical examination of existing restoration:
I- Clinical examination of Amalgam restorations:
Evaluation of all restorations must be done in a clean, dry, well
lighted field using one of the following methods:
a- Visual observation.
b- Tactile sense with the explorer.
b- Dental floss
d- Interpretation of radiographs
Amalgam restorations may have (10) distinct conditions, when they are
evaluated:
1 - Amalgam blues.
2 - Proximal overhangs.
3 - Marginal ditching.
4 - Voids.
5 - Fracture lines.
6 - Improper anatomic contours.
7 - Marginal ridge incompatibility.
8 - Improper proximal contacts.

9 - Recurrent caries.
10- Improper occlusal contacts.
(1) Amalgam blues:
It is seen through the enamel in teeth that have amalgam
restorations. This bluish discoloration resulted either from leaching of
corrosion products of amalgam into the dentinal tubules or from the color
of underlying amalgam as seen through translucent enamel. The latter
occur when no dentin support such as in undermined cusps, marginal
ridges, and region adjacent to proximal margins.
(2) Marginal ditching:
It is the deterioration of the amalgam-tooth interface as a result of
wear, fracture or improper tooth preparation.It can be diagnosed visually
or tactilely using an explorer. Shallow ditching less than 0.5 deep have no
need for restoration replacement. However if the ditch is too deep, the
restoration should be replaced to avoid secondary caries around the
restoration.
(3) Proximal overhangs:
It is diagnosed visually, tactilely using an explorer,
radiographically or by using dental floss. Overhangs resulted in plaque
accumulation and so it requires restoration replacement.
(4) Voids:
It is occur at the margins of amalgam restorations. It is at least 0.3
mm deep and is located in the gingival third of the tooth crown so it must
be repaired or replaced. Small voids in the marginal area where the
enamel is thicker may be corrected by recontouring or repairing with a
small restoration.

(5) Fracture lines:
Isthmus fracture is the most common fracture line occurs in amalgam
restoration. It indicates replacement of the defective restoration.
(6) Improper anatomic contours:
Inadequate embrasure form or proximal contact which prevents the
use of dental floss, indicates recontouring or replacement of the
restoration.
(7) Marginal ridge incompatibility:
Marginal ridge of amalgam restoration should be compatible with the
adjacent marginal ridge. If marginal ridges are not compatible and are
associated with poor tissue health, food impaction or inability to use
dental floss so restoration should be recontoured or replaced.
(8) Improper proximal contacts:
This leads to poor interproximal tissue health and/or food impaction
so restoration should be replaced.
(9) Recurrent caries:
It is detected visually, tactilely or radiographically. It considered an
indication for repair or replacement.
(10) Improper occlusal contacts:
It cause improper occlusal function which results in inefficient
mastication and/or tooth movement. This condition needs correction or
replacement.
Clinical examination of cast restorations:
It should be evaluated in the same manner as amalgam. In case of
any defect or tissue harm repair replacement of the restoration should be
considered.

Clinical examination of composite restorations:
Tooth colored restorations should be evaluated clinically in the
same manner as amalgam and cast restorations. Corrective procedures
include recontouring, polishing repairing or replacing should be done.
The main concern with anterior teeth is the esthetics. Marginal
discoloration that is non carious may be corrected by a small repair
restoration along the margin. If the stain is superficial it can be removed
by resurfacing. But in deep stains or those involve the bulk of the
restoration, total replacement or veneering would be indicated.
Adjunctive aids for examining teeth and restorations:
1- Percussion:
It is done by gentle tapping the occlusal or incisal surface of the
teeth by the use of mirror handle to determine the presence of tenderness
indicating periapical involvement:
A- Pain on vertical percussion indicating periapical involvement.
B- Pain on lateral percussion indicating periodontal involvement.
C- Sometimes the maxillary teeth exhibit a false pain on percussion in
case of chronic sinusitis.
2- Palpation:
It is done with teeth tender to percussion to determine the presence
of periapical or periodontal abscess. It is performed by rubbing the index
finger along the facial and lingual mucosa overlying the apical region to
detect periapical pathosis.
3- Vitality test:
A- Thermal test:
It is used to detect the pulp vitality, either by cold or hot testing.

- A cotton applicator tip sprayed with a freezing agent
(ethychloride).
- Pencil of ice.
- Hot instrument.
- Hot guttapercha directly to tooth.
B- Electric pulp tester:
It should be placed on the tooth and not on the restoration. It causes
tingling effect when the pulp is vital. In case of no response, this
indicates pulp death. It is important to obtain readings on adjacent and
contra-lateral teeth to evaluate the affected tooth response.
4- Cavity Test:
It is used when there is no other means to diagnose the pulp vitality
or in presence of large restoration in the tooth. Round bur is used without
anesthesia to drill a cavity through the restoration into dentin.
Lack of sensitivity may indicate a non vital pulp. But it give a
false-negative response in case of sclerotic dentin or Multi-rooted teeth.
5- Anesthetic test:
If the patient is not able to localize the affected tooth, anesthesia
test used to determine the suspected tooth. If the symptoms subside, so
the affecting tooth has been identified.
6- Study cast:
The dentist can gain much information through an evaluation of
study cast. In accessible area can be seen:
- Understanding of occlusal relationships such as tilted, rotated or
extruded teeth, cross bite and plunger cusps.
- Development of treatment plan without patient presence which will
be saving time.