optimizing distance image quality of an aspheric multifocal intraocular lens using a comprehensive...
TRANSCRIPT

Optimizing distance image quality of an aspheric multifocal intraocular lens using a
comprehensive statistical design approach
Xin Hong∗ and Xiaoxiao Zhang Alcon Laboratories, Inc. 6201 South Freeway, Fort Worth, Texas 76134, USA
∗Corresponding author: [email protected]
Abstract: The AcrySof ReSTOR intraocular lens (IOL) is a multifocal lens with state-of-the-art apodized diffractive technology, and is indicated for visual correction of aphakia secondary to removal of cataractous lenses in adult patients with/without presbyopia, who desire near, intermediate, and distance vision with increased spectacle independence. The multifocal design results in some optical contrast reduction, which may be improved by reducing spherical aberration. A novel patent-pending approach was undertaken to investigate the optical performance of aspheric lens designs. Simulated eyes using human normal distributions were corrected with different lens designs in a Monte Carlo simulation that allowed for variability in multiple surgical parameters (e.g. positioning error, biometric variation). Monte Carlo optimized results indicated that a lens spherical aberration of –0.10 μm provided optimal distance image quality.
©2008 Optical Society of America
OCIS codes: (220.0220) Optical design and fabrication; (230.0230) Optical devices
References and links
1. C. S. Lee and M. J. Simpson, Diffractive multifocal ophthalmic lens. Alcon Laboratories, Inc. [5699142]. 12-16-0097. US.
2. Alcon Laboratories, Inc. AcrySof ReSTOR apodized diffractive aspheric IOL [package insert]. 1-16. 2007. Fort Worth, TX, USA.
3. G. Smith and C. W. Lu, "The spherical aberration of intra-ocular lenses," Ophthalmic Physiol Opt. 8, 287-294 (1988).
4. J. T. Holladay, P. A. Piers, G. Koranyi, Mooren M. van der, and N. E. Norrby, "A new intraocular lens design to reduce spherical aberration of pseudophakic eyes," J. Refract. Surg. 18, 683-691 (2002).
5. L. Wang and D. D. Koch, "Custom optimization of intraocular lens asphericity," J. Cataract Refract. Surg. 33, 1713-1720 (2007).
6. S. Norrby, "Sources of error in intraocular lens power calculation," J. Cataract Refract. Surg. 34, 368-376 (2008).
7. M. Baumeister, B. Neidhardt, J. Strobel, and T. Kohnen, "Tilt and decentration of three-piece foldable high-refractive silicone and hydrophobic acrylic intraocular lenses with 6-mm optics in an intraindividual comparison," Am. J. Ophthalmol. 140, 1051-1058 (2005).
8. H. H. Dietze and M. J. Cox, "Limitations of correcting spherical aberration with aspheric intraocular lenses," J. Refract. Surg. 21, S541-S546 (2005).
9. L. N. Thibos, A. Bradley, and X. Hong, "A statistical model of the aberration structure of normal, well-corrected eyes," Ophthalmic Physiol Opt. 22, 427-433 (2002).
10. T. Kohnen, "Measuring vision in refractive surgery," Cataract and Refractive Surgery Today 27, 1897-1898 (2001).
11. X. Hong, M. Karakelle, and X. Zhang. Corrections of higher order aberrations in intraocular lenses. Alcon Manufacturing,LTD. [0268453 A1]. 11-22-2007. US.
12. R. P. Lehman, "Clinically Relevant Advantages in the Functional Performance of the AcrySof IQ IOL" (ASCRS, American Society of Cataract and Refractive Surgery Symposium, Chicago, IL, USA 2008).
13. M. Packer, I. H. Fine, R. S. Hoffman, and P. A. Piers, "Prospective randomized trial of an anterior surface modified prolate intraocular lens," J. Refract. Surg. 18, 692-696 (2002).
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20920#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008

14. M. G. Wirtitsch, O. Findl, R. Menapace, K. Kriechbaum, C. Koeppl, W. Buehl, and W. Drexler, "Effect of haptic design on change in axial lens position after cataract surgery," J. Cataract Refract. Surg. 30, 45-51 (2004).
15. P. M. Kiely, G. Smith, and L. G. Carney, "The mean shape of the human cornea," Optica Acta 29, 1027-1040 (1982).
16. M. Guillon, D. P. Lydon, and C. Wilson, "Corneal topography: a clinical model," Ophthalmic Physiol Opt. 6, 47-56 (1986).
17. X. Hong, N. Himebaugh, and L. N. Thibos, "On-eye evaluation of optical performance of rigid and soft contact lenses," Cataract and Refractive Surgery Today 78, 872-880 (2001).
18. M. Simpson. Postoperative intraocular lens location: Technical Report. 013:36830, 1-20. 1998. 19. F. M. Mutlu, A. Bayer, C. Erduman, and M. Z. Bayraktar, "Comparison of tilt and decentration
between phacoemulsification and phacotrabeculectomy," Ophthalmologica 219, 26-29 (2005). 20. K. Hayashi, H. Hayashi, F. Nakao, and F. Hayashi, "Intraocular lens tilt and decentration after
implantation in eyes with glaucoma," J. Cataract Refract. Surg. 25, 1515-1520 (1999). 21. International Organization for Standardization, International Standard IS0 11979-211999 Technical
Corrigendum 1 Ophthalmic implants - Intraocular lenses -Part 2: Optical properties and test methods (=International Organization for Standardization, Geneva, Switzerland 1999).
22. F. W. Campbell and D. G. Green, "Optical and retinal factors affecting visual resolution," J. Physiol 181, 576-593 (1965).
23. X. Hong. Optical aberrations of human eyes and their impact on visual performances. 2001. 24. L. N. Thibos, X. Hong, A. Bradley, and R. A. Applegate, "Accuracy and precision of objective
refraction from wavefront aberrations," Cataract and Refractive Surgery Today 4, 329-351 (2004). 25. L. N. Thibos, "Acuity perimetry and the sampling theory of visual resolution," Optom. Vis. Sci. 75,
399-406 (1998). 26. N. E. Norrby, L. W. Grossman, E. P. Geraghty, C. F. Kreiner, M. Mihori, A. S. Patel, V. Portney,
and D. M. Silberman, "Determining the imaging quality of intraocular lenses," J. Cataract Refract. Surg. 24, 703-714 (1998).
27. I. Escudero-Sanz and R. Navarro, "Off-axis aberrations of a wide-angle schematic eye model," J. Opt. Soc. Am. A Opt. Image Sci. Vis. 16, 1881-1891 (1999).
28. R. Navarro, J. Santamaria, and J. Bescos, "Accommodation-dependent model of the human eye with aspherics," J. Opt. Soc. Am. A 2, 1273-1281 (1985).
29. Zemax Development Corporation. Xemax ray-tracing program. 2001. 30. N. sano-Kato, I. Toda, C. Sakai, Y. Hori-Komai, Y. Takano, M. Dogru, and K. Tsubota, "Pupil
decentration and iris tilting detected by Orbscan: anatomic variations among healthy subjects and influence on outcomes of laser refractive surgeries," J. Cataract Refract. Surg. 31, 1938-1942 (2005).
31. J. T. Holladay, "Standardizing constants for ultrasonic biometry, keratometry, and intraocular lens power calculations," J. Cataract Refract. Surg. 23, 1356-1370 (1997).
32. D. A. Achison, "Design of aspheric intraocular lenses," Ophthalmic and Physiological Optics 11, 137-146 (1991).
33. J. Narvaez, G. Zimmerman, R. D. Stulting, and D. H. Chang, "Accuracy of intraocular lens power prediction using the Hoffer Q, Holladay 1, Holladay 2, and SRK/T formulas," J. Cataract Refract. Surg. 32, 2050-2053 (2006).
34. T. Olsen, "Improved accuracy of intraocular lens power calculation with the Zeiss IOLMaster," Acta Ophthalmol. Scand. 85, 84-87 (2007).
35. International Organization for Standardization. ISO 11979-3:2006 Ophthalmic implants -- Intraocular lenses -- Part 3: Mechanical properties and test methods. 2006.
36. A. J. Lang, V. Lakshminarayanan, and V. Portney, "Phenomenological model for interpreting the clinical significance of the in vitro optical transfer function," J. Opt. Soc. Am. A 10, 1600-1610 (1993).
37. X. Zhang, M. Ye, A. Bradley, and L. Thibos, "Apodization by the Stiles-Crawford effect moderates the visual impact of retinal image defocus," J. Opt. Soc. Am. A Opt. Image Sci. Vis. 16, 812-820 (1999).
38. K. M. Rocha, E. S. Soriano, M. R. Chalita, A. C. Yamada, K. Bottos, J. Bottos, L. Morimoto, and W. Nose, "Wavefront analysis and contrast sensitivity of aspheric and spherical intraocular lenses: a randomized prospective study," Am. J. Ophthalmol. 142, 750-756 (2006).
39. S. Marcos, P. Rosales, L. Llorente, S. Barbero, and I. Jimenez-Alfaro, "Balance of corneal horizontal coma by internal optics in eyes with intraocular artificial lenses: evidence of a passive mechanism," Vision Res. 48, 70-79 (2008).
40. P. Rosales and S. Marcos, "Phakometry and lens tilt and decentration using a custom-developed Purkinje imaging apparatus: validation and measurements," J. Opt. Soc. Am. A Opt. Image Sci. Vis. 23, 509-520 (2006).
41. Castro A. de, P. Rosales, and S. Marcos, "Tilt and decentration of intraocular lenses in vivo from Purkinje and Scheimpflug imaging. Validation study," J. Cataract Refract. Surg. 33, 418-429 (2007).
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20921#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008

42. D. A. Atchison, E. L. Markwell, S. Kasthurirangan, J. M. Pope, G. Smith, and P. G. Swann, "Age-related changes in optical and biometric characteristics of emmetropic eyes," J. Vis. 8, 29-20 (2008).
43. J. Tabernero, A. Benito, E. Alcon, and P. Artal, "Mechanism of compensation of aberrations in the human eye," J. Opt. Soc. Am. A Opt. Image Sci. Vis. 24, 3274-3283 (2007).
44. P. Rosales and S. Marcos, "Customized computer model of eyes with intraocular lenses," Optics Express 15, 2204-2218 (2007).
1. Introduction
Multifocal intraocular lenses (IOLs) provide significant advantages over earlier monofocal designs, incorporating both distance and near-powered optics into one IOL. The AcrySof spherical ReSTOR IOL (Alcon Laboratories, Inc.) is a globally marketed lens with apodized diffractive technology[1] intended for primary implantation for the visual correction of aphakia secondary to removal of a cataractous lens in adult patients with and without presbyopia, who desire near, intermediate, and distance vision with increased spectacle independence.[2] Spherical aberration affects the optical imagery delivered by IOLs. We attempt to find the optimal spherical aberration for multifocal IOLs to further enhance the distance images they can deliver.
In monofocal IOL design, spherical aberration reduction has been proposed[3] by applying asphericity to the IOL[4] to compensate for physiologic corneal spherical aberration.[5] This approach has multiple challenges. Lenses are available only in certain powers. Corneal asphericity varies considerably across the population. At least as importantly, other variables affect overall optical quality, including small refractive errors such as cornea power measurement errors,[6] biometry measurement errors, [6] and final lens position errors such as decentration and tilt due to surgical technique and anatomic variation. [7,8] To include the above variables, statistical modeling may be used; eg, Thibos et al. modeled the wavefront aberration function of normal, well-corrected eye based on normative data from 200 eyes and showed that, apart from spherical aberration, the higher-order aberrations of the human eye tended to be randomly distributed about a mean value of zero. The model was verified by analyzing the statistical properties of 1000 virtual eyes generated by the model.[9]
Beyond improving the optical imagery,, a new aspheric multifocal IOL must satisfy the increasingly higher quality of vision expectations of patients and surgeons.[10] The goal of optimal IOL design is to address optical and surgical variations to provide satisfactory results for every patient, and the greatest benefit to the highest percentage of patients. Accordingly, a novel patent-pending approach[11] in IOL design was undertaken to add the most beneficial amount of spherical aberration to the multifocal ReSTOR parent lens and optimize distance image quality. This approach included Monte Carlo simulation of expected results for a wide variety of eyes, and calculation of the expected modulation transfer function (MTF) for each, with different amounts of spherical aberration.
2. Methods
2.1 Lens design strategy
The benefit of corneal spherical aberration reduction has been demonstrated both optically and clinically. For patients with monofocal IOLs, the reduction of spherical aberration has improved functional visual performance.[12] A clinically significant difference in functional vision corresponds to a 0.15 log unit improvement in contrast sensitivity.[13] This improvement may offset the contrast sensitivity loss for patients with multifocal IOLs.
A simplistic design strategy suggests calculating the appropriate asphericity based on the spherical aberration of the average human eye. However, this approach could not address the biometric and surgical variability inherent in cataract surgery. To treat complex issues such as these, an aberration balancing technique would typically be used by experienced optical designers. In this investigation, the optimal asphericity for a ReSTOR lens was determined using a more comprehensive statistical design approach: a Monte Carlo simulation. Such a
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20922#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008
simulation presumes that if the nature of the variability expected in a particular system can be characterized, multiple outcomes can be calculated as a function of the cumulative probabilities of each contributing random event.
Monte Carlo simulation depends upon knowing the cumulative probability distributions of contributing events. The anatomical variability in the eye, the variability in final lens position, and the resulting residual refractive error can be approximated by normal distributions. For example, studies to date have reported varied measures of corneal radius and asphericity (Table 1). On average, the anterior corneal radius and the anterior corneal asphericity are 7.72 mm ± 0.28 mm and −0.183 ± 0.160 mm, respectively. The standard deviation of anterior chamber depth has been reported as approximately ± 0.30 mm.[14] The mean anterior chamber depth varies for different IOL types.[14] We selected 4.60 ± 0.30 mm as the anterior chamber depth in this investigation. We assumed that these factors were statistically independent and that the joint probability distribution function could be computed as the product of univariate probability distribution functions.
Table 1. Reported values of corneal radius and corneal asphericity
Corneal Radius1 Corneal Asphericity1 References 7.72 mm ± 0.27 mm −0.26 ± 0.18 Kiely et al., 1982[15] 7.79 mm ± 0.26 mm −0.15 ± 0.15 Guillon et al., 1986[16] 7.71 mm ± 0.29 mm −0.24 ± 0.14 Hong et al., 2001[17]
1 Measures pertain to the anterior cornea.
We built a suitable eye model for IOL optics design and testing by searching
ophthalmology and optics science literature and reviewing Alcon proprietary technology. Table 2 lists the variables we considered and associated illustrative values.
Table 2. Selection and definition of variables for a suitable eye model
Variable Case Values Presented in this Paper
Reference
Anterior corneal radius −2 SD (7.16 mm), −1 SD (7.44 mm), 0SD (7.72 mm), +1 SD (8.00 mm) and +2 SD
Average of Published Reported Values[15] [16] [17]
Anterior corneal asphericity -2 SD (-0.503), -1 SD (-0.343), 0 SD (-0.183), +1 SD (-0.023), +2 SD (+0.137)
Average of Published Reported Values[15] [16] [17]
Anterior chamber depth -2 SD (4.0 mm), -1 SD (4.3 mm), 0 SD (4.6 mm), +1 SD (4.9 mm), + 2 SD (5.2 mm)
Average of Published Reported Values[14,18]
Decentration 0.0 mm, 0.25 mm, 0.5 mm [19,20]
Tilt 0°, 2.5°, 5° [19,20]
Sphere 0 D, ± 1/8 D, ± 1/4 D
Cylinder 0 D, ± 1/8 D, ± 1/4 D
Refractive stability across entire IOL power range
bi-convex, symmetric-biconvex, and asymmetric bi-convex platforms
Common lens shape factors in commercialized IOLs
IOL fabrication tolerances Proprietary and more stringent than ISO guidance[21]
ISO 11979-2[21]
IOL = intraocular lens; ISO = International Organization for Standardization
Intraocular lenses are often manufactured in powers from 6 diopters (D) through 34 D. To offer better power predictability across such a large power range, the variability in optical principal plane location was further reduced across this range.
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20923#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008

2.2 Methods for lens testing and the Monte Carlo simulation
The quality of an optical system is accurately and conveniently evaluated by measurement of its modulation transfer function (MTF).[21] Typically a high spatial frequency (i.e., 100 line pairs/millimeter [lp/mm]) has been used to gauge the optical fidelity of a monofocal IOL. The MTF is linearly related to the contrast sensitivity function,[22-24] which justifies the use of MTF performance for the prediction of visual performance. The human visual system utilizes the spatial frequencies that are resolvable by retinal neural sampling.[25] Low and mid-range spatial frequencies contribute to face recognition and daily tasks and are typically measured with contrast sensitivity testing. High spatial frequencies contribute to detail identification tasks and are often measured with visual acuity testing. Another commonly used unit to represent the MTF of human eye is cycles per degree. Our optical modeling showed that for the typical human eye, 10 lines/mm corresponds to 3 cpd and 100 lines/mm corresponds to 30 cpd. Accordingly, our approach used a MTF range from low to high spatial frequencies at 10 lp/mm intervals, from 10 lp/mm to 100 lp/mm, which are the dominant frequency ranges that approximately correspond to visual acuity ranging from 20/200 to 20/20, respectively.[26] The FFT algorithm in the Zemax ray-tracing program was used to calculate the MTF. The MTF values were computed for monochromatic light; wavelength was 550 nm. Based on a proprietary study collaboration between Alcon Laboratories, Inc. and Indiana University, the diffractive design at wavelength of 550 nm supported consideration of polychromatic performance. The refractive indices were identical to those used by Escuderio-Sanz and Navarro[27] and Navarro et al. [27,28]
Continuous MTF data may be plotted on a curve across the spatial frequency range tested (10 lp/mm to 100 lp/mm). Because low, mid-range, and high spatial frequencies each contribute to different tasks, we decided to average the MTF results with equal weighting to evaluate the overall optical performance of the human eye with an IOL. This average value was implemented as the merit function in the Zemax ray-tracing program [29] and was utilized to find the best focal plane to maximize overall MTF performance and reported optical quality of a particular hypothetical eye in the Monte Carlo simulation.
Five suitable spherical aberration correction options for lens designs were selected for evaluation. Each had an aspheric ReSTOR diffractive IOL design and a symmetric-biconvex lens style. Design options included lenses with a range of lens spherical aberration values (as root mean square [RMS] for a 6 mm entrance pupil): (1) 0 μm, (2) –0.05 μm, (3) –0.10 μm, (4) –0.15μm, and (5) –0.20 μm. In addition, a control case was investigated consisting of a ReSTOR lens design with a lens spherical aberration value of +0.05 µm. This was selected as the control because it has the spherical aberration value of the spherical ReSTOR IOL and was referred to as lens design (6) or the control.
To create different spherical aberration levels, we applied different degrees of asphericity to the base curve of the anterior lens surface on which the diffractive multifocal element is overlaid.
Each of the 5 lens designs affects the overall spherical aberration of the eye, given a corneal spherical aberration of 0.28 microns (Fig. 1). Greater spherical aberration in the IOL reduces the overall spherical aberration in the eye, as the negative IOL spherical aberration compensates for the positive spherical aberration of the cornea. The lens spherical aberration change was realized by adjusting the conic constant Q (cc) of the anterior lens surface.
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20924#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008

Fig. 1. Five lens designs with increasingly negative spherical aberration correction values (right) and corresponding average total eye spherical aberration values (left) (as root mean square [RMS] for a 6 mm entrance pupil).
These lens designs were evaluated with a Monte Carlo simulation. Cumulative distribution
functions for axial length, anterior chamber depth, corneal radius and corneal asphericity were used to generate a population of 200 hypothetical eyes. Each lens design was positioned in the resulting eye models with randomly-generated tilt and decentration consistent with observed surgical variability. The MTFs of the resultant eye/IOL combinations were calculated, based on optimizing the merit function previously described. The MTF values for each eye were aggregated into statistical descriptors (e.g., mean, standard deviation, 10th percentile, 50th percentile and 90th percentile).
In addition, individual variables were investigated to understand their internal contributions. Power prediction, or refractive stability across the entire IOL power range, was investigated with 2nd principal plane calculation method for IOLs with bi-convex, symmetric-biconvex, and asymmetric bi-convex platforms. Pupil decentration and its variability in the population were not included as a variable because investigation of the Navarro wide angle schematic eye indicates that pupil decentration has a small effect on the monochromatic MTF.[30]
3. Results
3.1. Effects of individual variables
3.1.1. Corneal radius
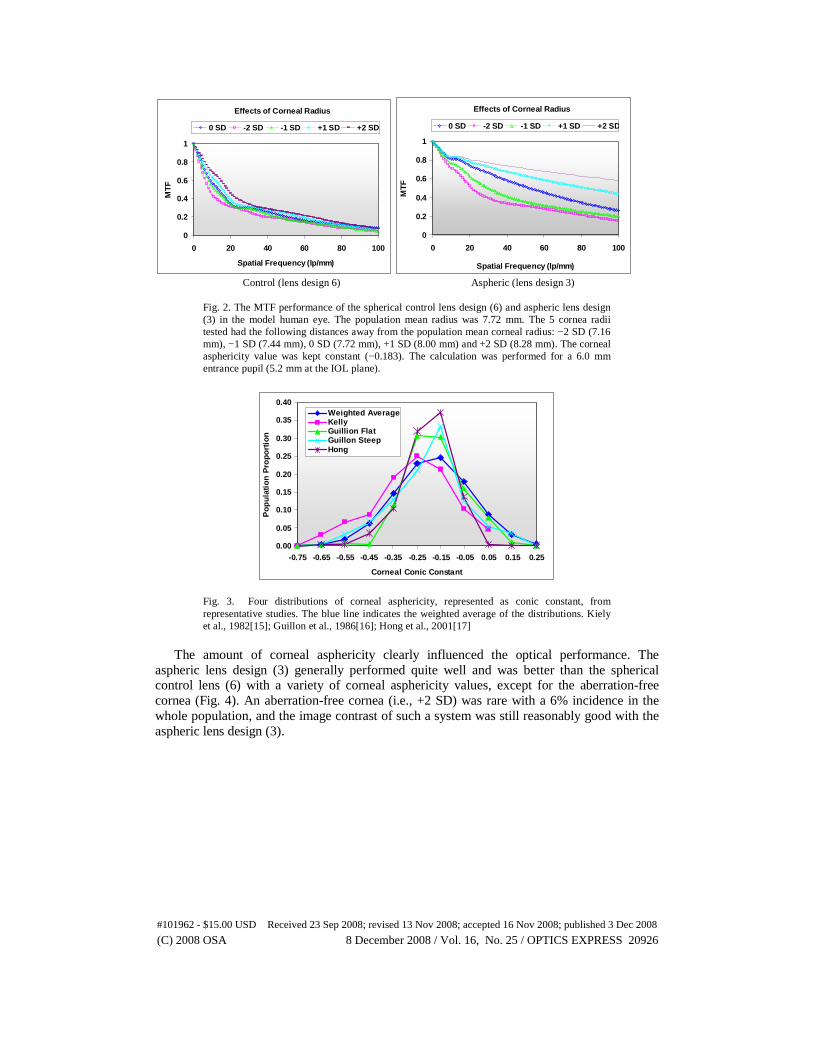
The effect of variation in anterior corneal radius size was investigated by testing the MTF through model eyes with 5 different corneal radii. Results for lens designs (6) and (3) are shown in Fig. 2. The flat cornea had less positive spherical aberration and better MTF results with both lens designs. Corneal radius change influenced the MTF of the aspheric lens design (3), but had little effect on the MTF of the spherical control lens design (6).
3.1.2. Corneal asphericity
Anterior corneal asphericity (usually expressed as conic constant [cc]) varies in human eyes. The corneal asphericity distributions from several representative studies are plotted in Fig. 3; distributions are relatively normal. Most distributions center around the population means and have a small aberration-free portion (~ cc = –0.5) and a small spherical portion (~ cc = 0.0). Most anterior corneas have positive spherical aberrations; the associated anterior corneal conic constant has a mean of –0.183 ± 0.160.
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20925#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008
Effects of Corneal Radius
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100
Spatial Frequency (lp/mm)
MT
F
0 SD -2 SD -1 SD +1 SD +2 SD
Effects of Corneal Radius
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100
Spatial Frequency (lp/mm)
MT
F
0 SD -2 SD -1 SD +1 SD +2 SD
Control (lens design 6) Aspheric (lens design 3)
Fig. 2. The MTF performance of the spherical control lens design (6) and aspheric lens design (3) in the model human eye. The population mean radius was 7.72 mm. The 5 cornea radii tested had the following distances away from the population mean corneal radius: −2 SD (7.16 mm), −1 SD (7.44 mm), 0 SD (7.72 mm), +1 SD (8.00 mm) and +2 SD (8.28 mm). The corneal asphericity value was kept constant (−0.183). The calculation was performed for a 6.0 mm entrance pupil (5.2 mm at the IOL plane).
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
-0.75 -0.65 -0.55 -0.45 -0.35 -0.25 -0.15 -0.05 0.05 0.15 0.25
Corneal Conic Constant
Po
pu
lati
on
Pro
po
rtio
n
Weighted AverageKellyGuillion FlatGuillon SteepHong
Fig. 3. Four distributions of corneal asphericity, represented as conic constant, from representative studies. The blue line indicates the weighted average of the distributions. Kiely et al., 1982[15]; Guillon et al., 1986[16]; Hong et al., 2001[17]
The amount of corneal asphericity clearly influenced the optical performance. The
aspheric lens design (3) generally performed quite well and was better than the spherical control lens (6) with a variety of corneal asphericity values, except for the aberration-free cornea (Fig. 4). An aberration-free cornea (i.e., +2 SD) was rare with a 6% incidence in the whole population, and the image contrast of such a system was still reasonably good with the aspheric lens design (3).
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20926#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008

Effects of Corneal Asphericity
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100
Spatial Frequency (lp/mm)
MT
F0SD -2SD -1SD +1SD +2SD
Effects of Corneal Asphericity
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100
Spatial Frequency (lp/mm)
MT
F
0 SD -2 SD -1 SD +1 SD +2 SD
Control (lens design 6) Aspheric (lens design 3)
Fig. 4. The MTF performance of the spherical control lens design (6) and aspheric lens design (3) in the model human eye. The population mean asphericity was −0.183. The 5 corneal asphericity values tested had the following distances away from the population mean corneal asphericity: −2 SD (−0.503), −1 SD (−0.343), 0 SD (−0.183), +1 SD (−0.023) and +2 SD (+0.137). The corneal radius was kept constant at 7.72 mm. The calculation was performed for a 6.0 mm entrance pupil (5.2 mm at the IOL plane).
3.1.3. Anterior chamber depth/effective lens position
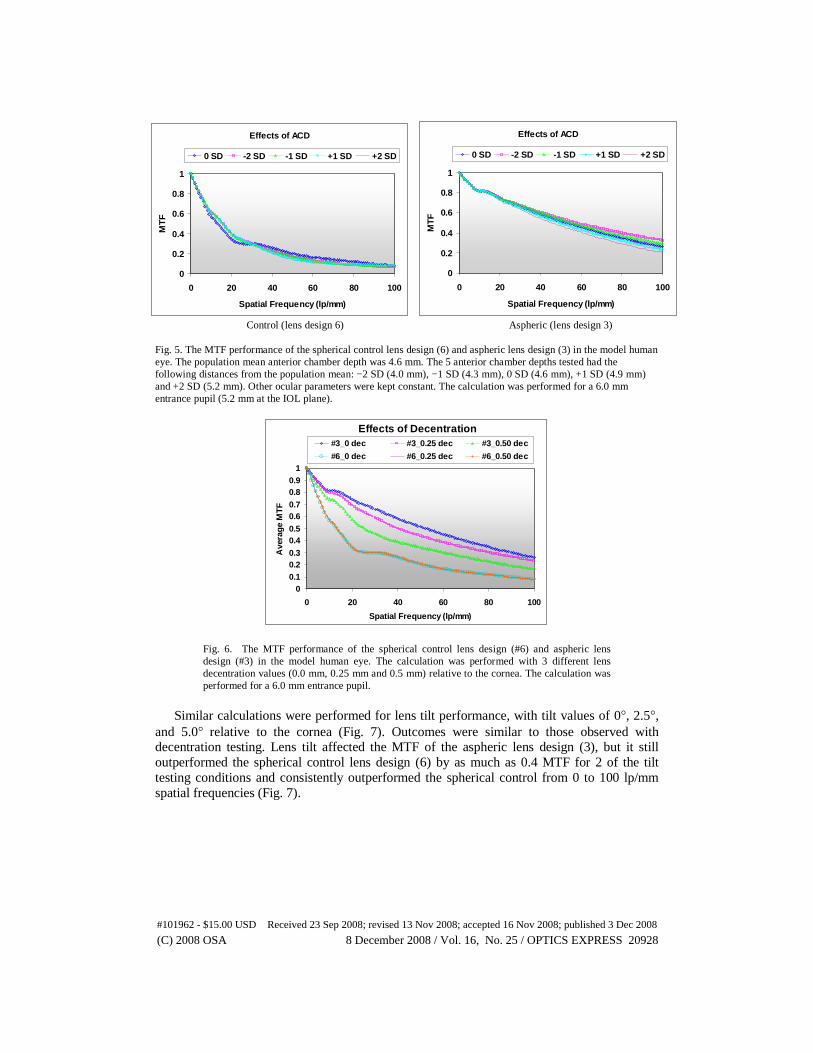
The anterior chamber depth is the distance between the anterior corneal surface and the anterior lens surface and is known to affect the refractive power of the whole eye.[31] With an implanted IOL, the anterior chamber depth corresponds to the effective lens position. The optical effects of varied anterior chamber depths were quite limited. MTF results were consistent within each lens design, from spatial frequencies of 0 to 100 lp/mm, despite varied anterior chamber depth/effective lens position values (Fig. 5) The modulation contrast results for both the spherical control (6) and the aspheric lens design (3) did not vary as dramatically as those observed with variations in corneal radius (Fig. 2) and corneal asphericity values (Fig. 4). This is not surprising, as the merit function was designed to take into consideration an adjustment of defocus to optimize the MTF.
3.1.4. Misalignment effects of decentration and tilt
Any IOL implanted in the human eye is subject to various misalignment errors such as IOL decentration and tilt. Because of its aspheric shape, decentration and tilt may be more important for an aspheric IOL than a spherical one.[32] Slight deviations from the optical axis such as decentration and tilt might affect the outcome in aspheric or multifocal IOLs.[7,8]
The MTF values were calculated for spherical and aspheric designs at on-axis (0 decentration relative to the corneal optical axis) and two decentration conditions (0.25 mm and 0.50 mm decentration relative to the corneal optical axis) (Fig. 6). While decentration of the aspheric lens (3) decreased its MTF values considerably, it outperformed the spherical lens design (6), even with a 0.50 mm decentration. The spherical (control) lens design (6) was less sensitive to decentration but its MTF was consistently lower across spatial frequencies from 0 to 100 lp/mm.
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20927#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008
Effects of ACD
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100
Spatial Frequency (lp/mm)
MT
F0 SD -2 SD -1 SD +1 SD +2 SD
Effects of ACD
0
0.2
0.4
0.6
0.8
1
0 20 40 60 80 100
Spatial Frequency (lp/mm)
MT
F
0 SD -2 SD -1 SD +1 SD +2 SD
Control (lens design 6) Aspheric (lens design 3) Fig. 5. The MTF performance of the spherical control lens design (6) and aspheric lens design (3) in the model human eye. The population mean anterior chamber depth was 4.6 mm. The 5 anterior chamber depths tested had the following distances from the population mean: −2 SD (4.0 mm), −1 SD (4.3 mm), 0 SD (4.6 mm), +1 SD (4.9 mm) and +2 SD (5.2 mm). Other ocular parameters were kept constant. The calculation was performed for a 6.0 mm entrance pupil (5.2 mm at the IOL plane).
Effects of Decentration
00.10.20.30.40.50.60.70.80.9
1
0 20 40 60 80 100
Spatial Frequency (lp/mm)
Ave
rag
e M
TF
#3_0 dec #3_0.25 dec #3_0.50 dec
#6_0 dec #6_0.25 dec #6_0.50 dec
Fig. 6. The MTF performance of the spherical control lens design (#6) and aspheric lens design (#3) in the model human eye. The calculation was performed with 3 different lens decentration values (0.0 mm, 0.25 mm and 0.5 mm) relative to the cornea. The calculation was performed for a 6.0 mm entrance pupil.
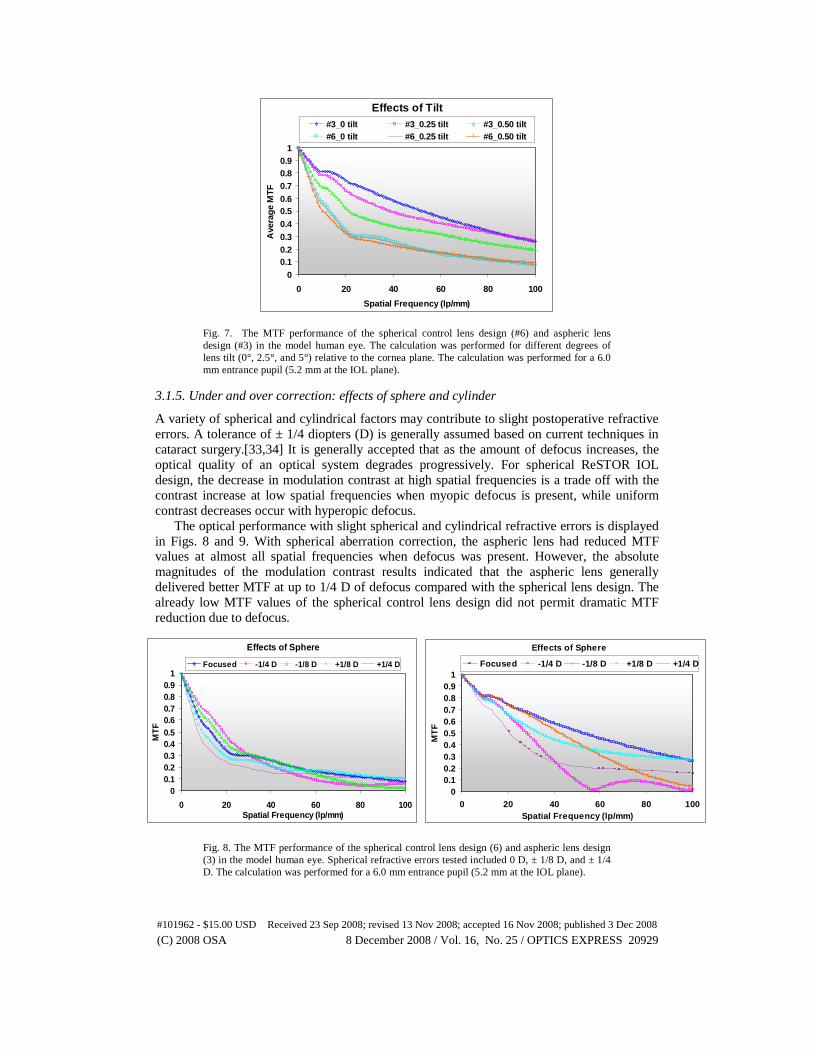
Similar calculations were performed for lens tilt performance, with tilt values of 0°, 2.5°,
and 5.0° relative to the cornea (Fig. 7). Outcomes were similar to those observed with decentration testing. Lens tilt affected the MTF of the aspheric lens design (3), but it still outperformed the spherical control lens design (6) by as much as 0.4 MTF for 2 of the tilt testing conditions and consistently outperformed the spherical control from 0 to 100 lp/mm spatial frequencies (Fig. 7).
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20928#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008
Effects of Sphere
00.10.20.30.40.50.60.70.80.9
1
0 20 40 60 80 100Spatial Frequency (lp/mm)
MT
F
Focused -1/4 D -1/8 D +1/8 D +1/4 D
Effects of Tilt
00.10.20.30.40.50.60.70.80.9
1
0 20 40 60 80 100
Spatial Frequency (lp/mm)
Ave
rag
e M
TF
#3_0 tilt #3_0.25 tilt #3_0.50 tilt#6_0 tilt #6_0.25 tilt #6_0.50 tilt
Fig. 7. The MTF performance of the spherical control lens design (#6) and aspheric lens design (#3) in the model human eye. The calculation was performed for different degrees of lens tilt (0°, 2.5°, and 5°) relative to the cornea plane. The calculation was performed for a 6.0 mm entrance pupil (5.2 mm at the IOL plane).
3.1.5. Under and over correction: effects of sphere and cylinder
A variety of spherical and cylindrical factors may contribute to slight postoperative refractive errors. A tolerance of ± 1/4 diopters (D) is generally assumed based on current techniques in cataract surgery.[33,34] It is generally accepted that as the amount of defocus increases, the optical quality of an optical system degrades progressively. For spherical ReSTOR IOL design, the decrease in modulation contrast at high spatial frequencies is a trade off with the contrast increase at low spatial frequencies when myopic defocus is present, while uniform contrast decreases occur with hyperopic defocus.
The optical performance with slight spherical and cylindrical refractive errors is displayed in Figs. 8 and 9. With spherical aberration correction, the aspheric lens had reduced MTF values at almost all spatial frequencies when defocus was present. However, the absolute magnitudes of the modulation contrast results indicated that the aspheric lens generally delivered better MTF at up to 1/4 D of defocus compared with the spherical lens design. The already low MTF values of the spherical control lens design did not permit dramatic MTF reduction due to defocus.
Control (lens design 6) Aspheric (lens design 3)
Fig. 8. The MTF performance of the spherical control lens design (6) and aspheric lens design (3) in the model human eye. Spherical refractive errors tested included 0 D, ± 1/8 D, and ± 1/4 D. The calculation was performed for a 6.0 mm entrance pupil (5.2 mm at the IOL plane).
Effects of Sphere
00.10.20.30.40.50.60.70.80.9
1
0 20 40 60 80 100Spatial Frequency (lp/mm)
MT
F
Focused -1/4 D -1/8 D +1/8 D +1/4 D
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20929#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008
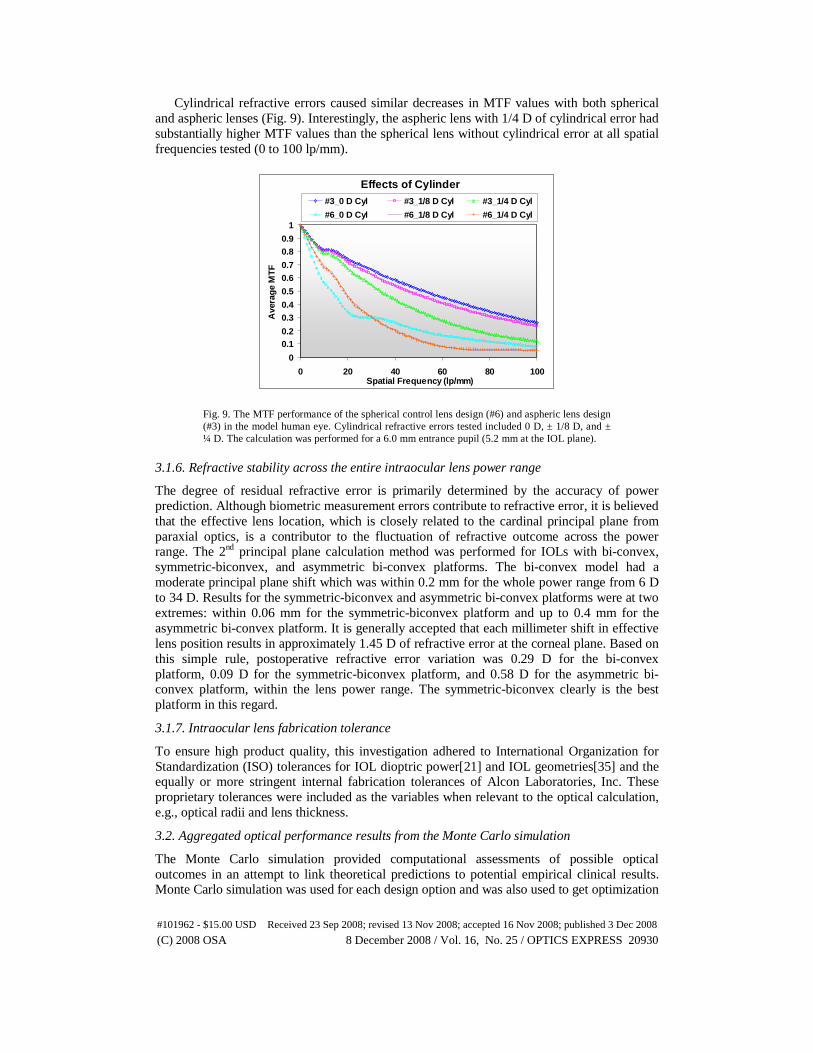
Cylindrical refractive errors caused similar decreases in MTF values with both spherical and aspheric lenses (Fig. 9). Interestingly, the aspheric lens with 1/4 D of cylindrical error had substantially higher MTF values than the spherical lens without cylindrical error at all spatial frequencies tested (0 to 100 lp/mm).
Effects of Cylinder
0
0.10.2
0.30.4
0.5
0.60.7
0.80.9
1
0 20 40 60 80 100Spatial Frequency (lp/mm)
Ave
rag
e M
TF
#3_0 D Cyl #3_1/8 D Cyl #3_1/4 D Cyl
#6_0 D Cyl #6_1/8 D Cyl #6_1/4 D Cyl
Fig. 9. The MTF performance of the spherical control lens design (#6) and aspheric lens design (#3) in the model human eye. Cylindrical refractive errors tested included 0 D, ± 1/8 D, and ± ¼ D. The calculation was performed for a 6.0 mm entrance pupil (5.2 mm at the IOL plane).
3.1.6. Refractive stability across the entire intraocular lens power range
The degree of residual refractive error is primarily determined by the accuracy of power prediction. Although biometric measurement errors contribute to refractive error, it is believed that the effective lens location, which is closely related to the cardinal principal plane from paraxial optics, is a contributor to the fluctuation of refractive outcome across the power range. The 2nd principal plane calculation method was performed for IOLs with bi-convex, symmetric-biconvex, and asymmetric bi-convex platforms. The bi-convex model had a moderate principal plane shift which was within 0.2 mm for the whole power range from 6 D to 34 D. Results for the symmetric-biconvex and asymmetric bi-convex platforms were at two extremes: within 0.06 mm for the symmetric-biconvex platform and up to 0.4 mm for the asymmetric bi-convex platform. It is generally accepted that each millimeter shift in effective lens position results in approximately 1.45 D of refractive error at the corneal plane. Based on this simple rule, postoperative refractive error variation was 0.29 D for the bi-convex platform, 0.09 D for the symmetric-biconvex platform, and 0.58 D for the asymmetric bi-convex platform, within the lens power range. The symmetric-biconvex clearly is the best platform in this regard.
3.1.7. Intraocular lens fabrication tolerance
To ensure high product quality, this investigation adhered to International Organization for Standardization (ISO) tolerances for IOL dioptric power[21] and IOL geometries[35] and the equally or more stringent internal fabrication tolerances of Alcon Laboratories, Inc. These proprietary tolerances were included as the variables when relevant to the optical calculation, e.g., optical radii and lens thickness.
3.2. Aggregated optical performance results from the Monte Carlo simulation
The Monte Carlo simulation provided computational assessments of possible optical outcomes in an attempt to link theoretical predictions to potential empirical clinical results. Monte Carlo simulation was used for each design option and was also used to get optimization
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20930#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008
from the design options. All of the aforementioned factors (biometry, misalignment and refractive error) were treated as independent, uncorrelated variables in a joint probability distribution. Each of the 200 simulated pseudophakic model eyes, including an IOL, was modeled in optical ray-tracing software for calculating the optical performance. The process was repeated for the five 200-eye cohorts, one for each lens design, and the control. Each individual eye was modeled, and the MTF was calculated and displayed as 1 data point. Pupil size (6 mm), lens power (21.00 D), and toricity (1.50 D) were kept consistent among all lens designs.
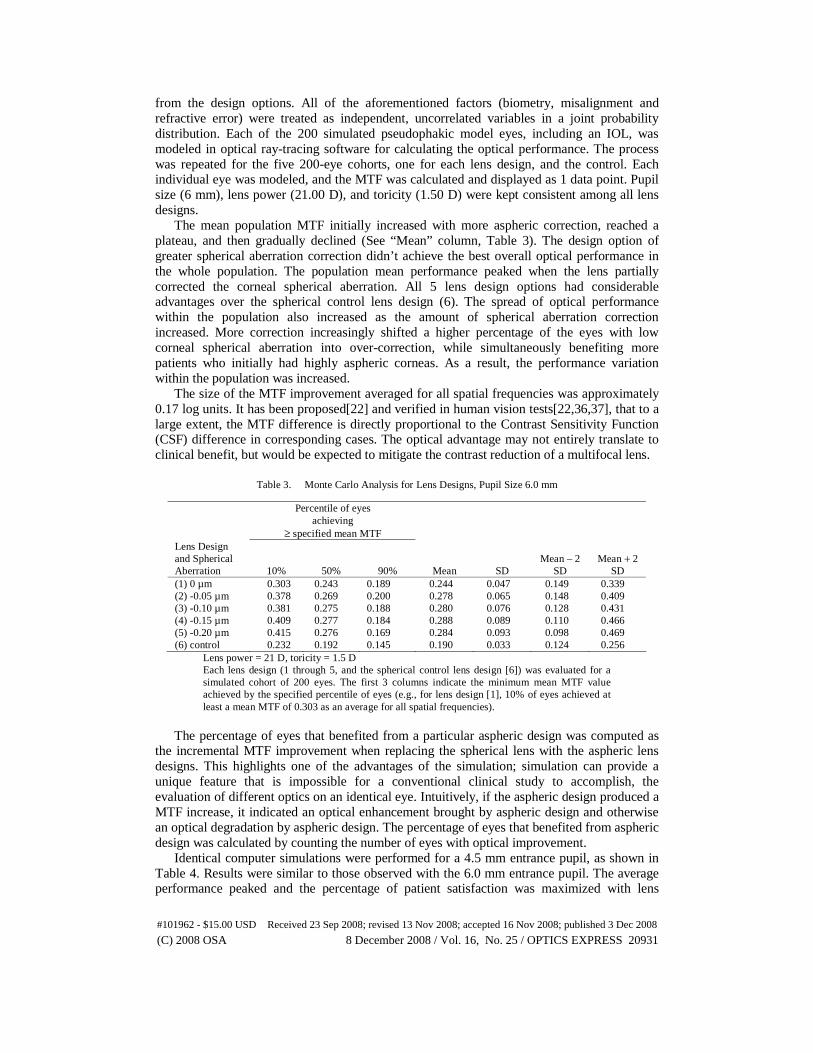
The mean population MTF initially increased with more aspheric correction, reached a plateau, and then gradually declined (See “Mean” column, Table 3). The design option of greater spherical aberration correction didn’t achieve the best overall optical performance in the whole population. The population mean performance peaked when the lens partially corrected the corneal spherical aberration. All 5 lens design options had considerable advantages over the spherical control lens design (6). The spread of optical performance within the population also increased as the amount of spherical aberration correction increased. More correction increasingly shifted a higher percentage of the eyes with low corneal spherical aberration into over-correction, while simultaneously benefiting more patients who initially had highly aspheric corneas. As a result, the performance variation within the population was increased.
The size of the MTF improvement averaged for all spatial frequencies was approximately 0.17 log units. It has been proposed[22] and verified in human vision tests[22,36,37], that to a large extent, the MTF difference is directly proportional to the Contrast Sensitivity Function (CSF) difference in corresponding cases. The optical advantage may not entirely translate to clinical benefit, but would be expected to mitigate the contrast reduction of a multifocal lens.
Table 3. Monte Carlo Analysis for Lens Designs, Pupil Size 6.0 mm
Percentile of eyes achieving
≥ specified mean MTF Lens Design and Spherical Aberration 10% 50% 90% Mean SD
Mean – 2 SD
Mean + 2 SD
(1) 0 µm 0.303 0.243 0.189 0.244 0.047 0.149 0.339 (2) -0.05 µm 0.378 0.269 0.200 0.278 0.065 0.148 0.409 (3) -0.10 µm 0.381 0.275 0.188 0.280 0.076 0.128 0.431 (4) -0.15 µm 0.409 0.277 0.184 0.288 0.089 0.110 0.466 (5) -0.20 µm 0.415 0.276 0.169 0.284 0.093 0.098 0.469 (6) control 0.232 0.192 0.145 0.190 0.033 0.124 0.256
Lens power = 21 D, toricity = 1.5 D Each lens design (1 through 5, and the spherical control lens design [6]) was evaluated for a simulated cohort of 200 eyes. The first 3 columns indicate the minimum mean MTF value achieved by the specified percentile of eyes (e.g., for lens design [1], 10% of eyes achieved at least a mean MTF of 0.303 as an average for all spatial frequencies).
The percentage of eyes that benefited from a particular aspheric design was computed as
the incremental MTF improvement when replacing the spherical lens with the aspheric lens designs. This highlights one of the advantages of the simulation; simulation can provide a unique feature that is impossible for a conventional clinical study to accomplish, the evaluation of different optics on an identical eye. Intuitively, if the aspheric design produced a MTF increase, it indicated an optical enhancement brought by aspheric design and otherwise an optical degradation by aspheric design. The percentage of eyes that benefited from aspheric design was calculated by counting the number of eyes with optical improvement.
Identical computer simulations were performed for a 4.5 mm entrance pupil, as shown in Table 4. Results were similar to those observed with the 6.0 mm entrance pupil. The average performance peaked and the percentage of patient satisfaction was maximized with lens
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20931#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008
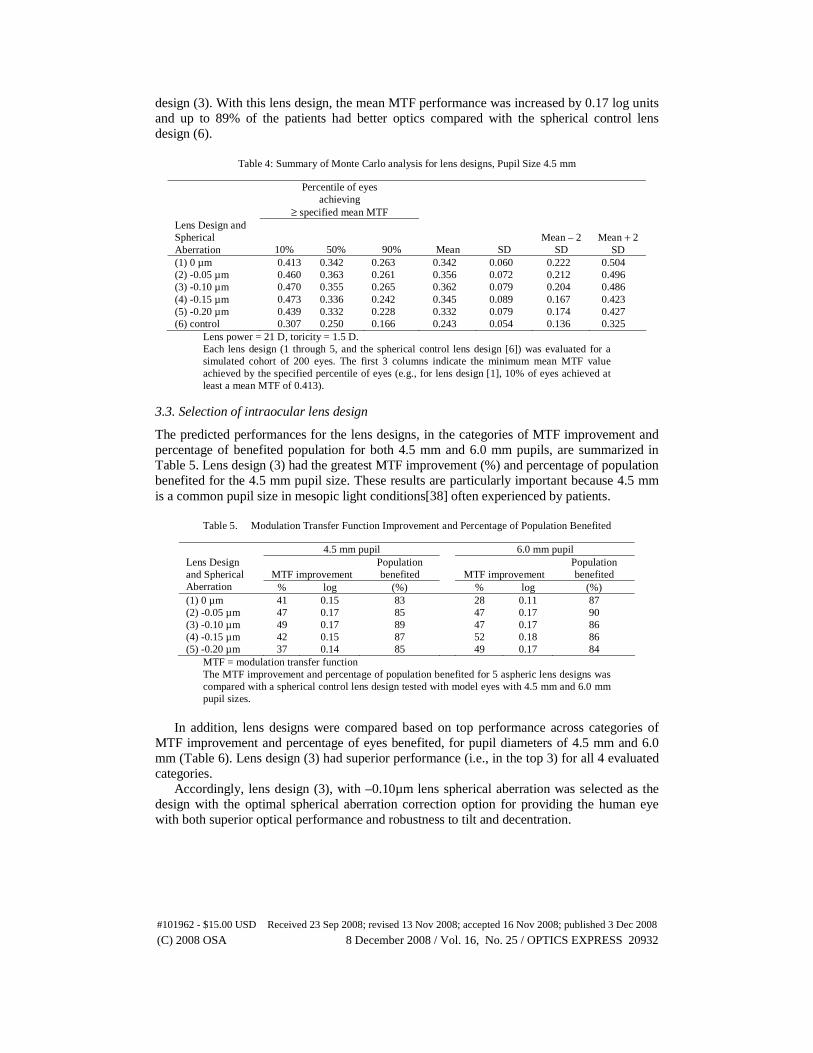
design (3). With this lens design, the mean MTF performance was increased by 0.17 log units and up to 89% of the patients had better optics compared with the spherical control lens design (6).
Table 4: Summary of Monte Carlo analysis for lens designs, Pupil Size 4.5 mm
Percentile of eyes achieving
≥ specified mean MTF Lens Design and Spherical Aberration 10% 50% 90% Mean SD
Mean – 2 SD
Mean + 2 SD
(1) 0 µm 0.413 0.342 0.263 0.342 0.060 0.222 0.504 (2) -0.05 µm 0.460 0.363 0.261 0.356 0.072 0.212 0.496 (3) -0.10 µm 0.470 0.355 0.265 0.362 0.079 0.204 0.486 (4) -0.15 µm 0.473 0.336 0.242 0.345 0.089 0.167 0.423 (5) -0.20 µm 0.439 0.332 0.228 0.332 0.079 0.174 0.427 (6) control 0.307 0.250 0.166 0.243 0.054 0.136 0.325
Lens power = 21 D, toricity = 1.5 D. Each lens design (1 through 5, and the spherical control lens design [6]) was evaluated for a simulated cohort of 200 eyes. The first 3 columns indicate the minimum mean MTF value achieved by the specified percentile of eyes (e.g., for lens design [1], 10% of eyes achieved at least a mean MTF of 0.413).
3.3. Selection of intraocular lens design
The predicted performances for the lens designs, in the categories of MTF improvement and percentage of benefited population for both 4.5 mm and 6.0 mm pupils, are summarized in Table 5. Lens design (3) had the greatest MTF improvement (%) and percentage of population benefited for the 4.5 mm pupil size. These results are particularly important because 4.5 mm is a common pupil size in mesopic light conditions[38] often experienced by patients.
Table 5. Modulation Transfer Function Improvement and Percentage of Population Benefited
4.5 mm pupil 6.0 mm pupil
MTF improvement Population benefited MTF improvement
Population benefited
Lens Design and Spherical Aberration % log (%) % log (%) (1) 0 µm 41 0.15 83 28 0.11 87 (2) -0.05 µm 47 0.17 85 47 0.17 90 (3) -0.10 µm 49 0.17 89 47 0.17 86 (4) -0.15 µm 42 0.15 87 52 0.18 86 (5) -0.20 µm 37 0.14 85 49 0.17 84
MTF = modulation transfer function The MTF improvement and percentage of population benefited for 5 aspheric lens designs was compared with a spherical control lens design tested with model eyes with 4.5 mm and 6.0 mm pupil sizes.
In addition, lens designs were compared based on top performance across categories of
MTF improvement and percentage of eyes benefited, for pupil diameters of 4.5 mm and 6.0 mm (Table 6). Lens design (3) had superior performance (i.e., in the top 3) for all 4 evaluated categories.
Accordingly, lens design (3), with –0.10µm lens spherical aberration was selected as the design with the optimal spherical aberration correction option for providing the human eye with both superior optical performance and robustness to tilt and decentration.
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20932#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008

Table 6. Rank Ordering of Lens Designs
Greatest MTF Improvement
Greatest % of Population Benefited
4.5 mm pupil Lens Designs and their
Spherical Aberration
(3) -0.10 µm (2) -0.05 µm (4) -0.15 µm
(3) -0.10 µm (4) -0.15 µm (5) -0.20 µ m
6.0 mm pupil Lens Designs and their
Spherical Aberration
(4) -0.15 µm (5) -0.20 µm (3) -0.10 µm
(2) -0.05 µm (1) 0 µm
(3) -0.10 µm MTF = modulation transfer function The top 3 lens designs achieving the greatest MTF improvement and benefiting the greatest percentage of population were rank ordered for 4.5 mm or 6.0 mm pupil sizes.
4. Discussion
Table 6 data have suggested a peak MTF performance with –0.10 µm lens spherical aberration. Combining this with Fig. 1, one could envision that deviation from this value in both less and more lens spherical aberration directions could cause MTF performance drop. If one could make extrapolation into the lens spherical aberration regions outside of Fig. 1 range, one might see further performance reduction. Further study is being considered to test this extrapolation.
The challenge of improving the ReSTOR IOL by including an aspheric component required more than merely adopting the spherical aberration correction of the parent monofocal aspheric lens. Rather, a comprehensive approach considered multiple variables and measured the expected MTF values for a simulated population. Through an evaluation of the improvements in MTF with both 4.5 mm and 6.0 mm pupils, the lens design that benefited the greatest percentage of the population was determined.
The Monte Carlo simulation revealed a tradeoff between the maximum achievable optical performance and the percentage of patients benefiting from aspheric correction. Considering the balance between optical superiority and correction robustness, lens design (3) was the aspheric lens design which provided optimal performance for both 4.5 mm and 6.0 mm pupils. Lens design (3), with –0.1 μm spherical aberration, is expected to achieve a 0.17 log unit MTF improvement, to benefit 86% to 89% of patients, and to lead to more reproducible optical performance from patient to patient. Lens design (3) was the best option based on optical performance superiority and robustness to tilt and decentration. The selected design will perform best when implanted within tolerance to tilt and decentration as reported in Section 3.1.4.
Study findings revealed a difference in desired IOL spherical aberration between the parent monofocal (–0.2 µm) and this apodized multifocal design (–0.1 µm), supporting the contention that existing optical models may be improved, especially for multifocal optics. Higher levels of spherical aberration correction were associated with increased variability of optical performance within the population, primarily due to decentration and tilt considerations. These effects would not have been demonstrated with a model that used only an average human eye to characterize IOL performance.
Other approaches to spherical aberration correction in monofocal lens design have been described in ophthalmic and optical science literature. These approaches were based on theoretical predictions and addressed the spherical aberration of the average human cornea alone. These approaches may be inadequate to characterize lens performance in a population because of the inherent variability in the human eye. We submit that the approach we
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20933#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008

identified reflects a more realistic expectation considering the wide biometric variation of human eyes and different surgical and refractive outcomes.
Alternative approaches and considerations are of interest for future study. In our study, eyes were simulated with realistic values taken from the literature of anterior corneal radius and asphericity, anterior chamber depth, tilt, decentration, refractive errors, as well as fabrication tolerances. We did not include the angle lamda as a variable. Based on recent publications,[39] the angle lamda is a relevant aspect to consider in future studies. We simulated eyes with tilt and decentration values that were consistent with the literature; however, recent validated advances in imaging methodology such as Purkinje or Scheimpflug imaging[40,41] may be incorporated to further future research. Our future approach could be expanded to consider the wide biometric variation of human eyes and different surgical and refractive outcomes that may be associated with age or gender.[42] In our study, variables were appropriately assumed independent; we required confirmed evidence to support optimization of intraocular lenses for production. Emerging evidence suggests potential associations among the variables. Given further solidification of the evidence, such associations could be incorporated in future studies.
Our approach included Monte Carlo simulation which was suitable for optimization of intraocular lenses that are manufactured in large volumes. Recent research has utilized customized eye models that truly represent individual eyes and accurately predict experimental measurements of higher order aberrations in the same eyes. These models could reliably be used for future custom applications.[43,44] Future approaches to lens design may achieve even better refractive optimization through customization.[5] More precise diagnostic methods, more precise positioning of the IOL, and improved refraction targeting may contribute to advances in IOL success. Other potential applications of our strategy could include computer simulation of individual variation in aberration structure, retinal image quality, visual performance, novel ophthalmic lens designs, or refractive surgery outcomes. Given the state of the art in IOL surgery; however, results of this investigation indicate that the degree of spherical aberration adopted for the ReSTOR aspheric multifocal IOL will provide the greatest benefit to the widest population.
Acknowledgments
The authors thank Jeanette Tomanka for scientific writing, editing, and oversight of manuscript development. The authors are grateful to Mutlu Karakelle and Paul Soye for critical discussion about the design of the experiment and Monte Carlo simulation methods, to Diane Houtman for contributing to scientific and clinical aspects of the manuscript, and to reviewers Tim Adkins, Diane Houtman, Mutlu Karakelle, Armando Pastrana, Rick Potvin, Kathie Schoepf, Paul Soye, and Steve VanNoy for critical reading of this manuscript. The authors thank the peer reviewers for their comments which helped to improve the quality of the manuscript.
(C) 2008 OSA 8 December 2008 / Vol. 16, No. 25 / OPTICS EXPRESS 20934#101962 - $15.00 USD Received 23 Sep 2008; revised 13 Nov 2008; accepted 16 Nov 2008; published 3 Dec 2008