optimizing the treatment of metastatic merkel cell carcinoma with immune checkpoint inhibitors
TRANSCRIPT

Optimizing the Treatment of Metastatic
Merkel Cell Carcinoma With Immune
Checkpoint Inhibitors
Paul Nghiem, MD, PhD
George F. Odland Endowed Chair in Dermatology
Professor & Head, University of Washington Dermatology
Affiliate Investigator, Fred Hutchinson Cancer Research Center

Disclosures
Dr. Nghiem discloses the following commercial
relationships:Consultant: EMD Serono
Grant/Research Support: Bristol-Myers Squibb
Non-FDA approved use of drugs or products
referenced in this presentation:Pembrolizumab
Nivolumab
Ipilimumab
FDA = Food and Drug Administration.

Learning Objectives
Learning objectives apply to physicians and nurses:
Describe the pathophysiology of MCC and the scientific foundation for immune checkpoint inhibitorsApply emerging data on immune checkpoint inhibitors in treatment planning for patients with metastatic MCCAssess strategies to manage immune-related adverse events associated with immune checkpoint inhibitors
MCC = Merkel cell carcinoma.

Agenda
MCC overview
Pathophysiology
Diagnosis, work-up, and
initial therapy
Immunotherapy for
metastatic MCC
Case discussions

Merkel Cell Carcinoma: Overview
More lethal than melanoma~40% mortality (~15% for
melanoma)
Reported incidence
increasingQuintupled since 1986
Currently ~2,500 new
cases/year in the US
Risk factorsFair skin (98% white), prolonged
sun exposure,
age >50 yr, immune
suppression (HIV, SOTR, CLL)
HIV = human immunodeficiency virus; SOTR = solid organ transplant recipient;
CLL = chronic lymphocytic leukemia.
Paulson et al, 2017; ACS, 2016; Heath et al, 2008; Miller et al, 1999.
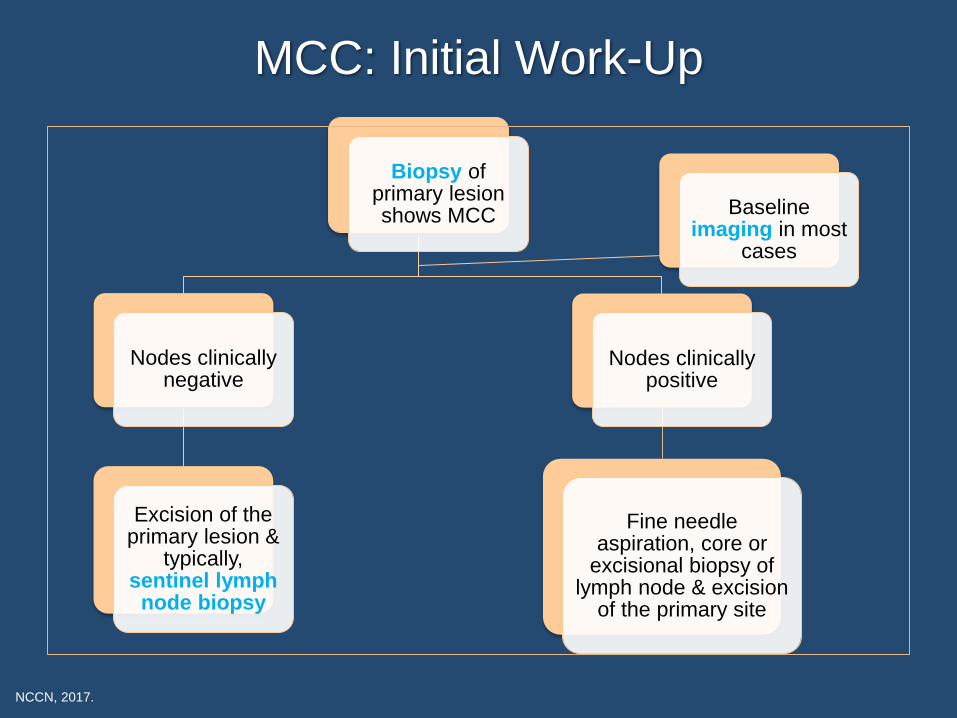
Biopsy of primary lesion shows MCC
Nodes clinicallynegative
Excision of the primary lesion &
typically, sentinel lymph
node biopsy
Nodes clinically positive
Fine needle aspiration, core or
excisional biopsy of lymph node & excision
of the primary site
Baseline imaging in most
cases
MCC: Initial Work-Up
NCCN, 2017.

7th Edition AJCC Staging for MCC
AJCC = American Joint Committee on Cancer.
Edge et al, 2010; Harms et al, 2016.
Disease Extent
(% of initial presentation)Stage
Local (65%)
Stage I: Primary tumor ≤2 cm
Ia: Nodes negative by pathological exam
Ib: Nodes not clinically detectable
Stage II: Primary tumor >2 cm
IIa: Nodes negative by pathological exam
IIb: Nodes not clinically detectable
IIc: Primary tumor invading
bone/muscle/fascia/cartilage
Nodal (26%)
Stage III: Regional nodal disease
IIIa: Nodes positive by pathological exam
and not clinically detectable
IIIb: Nodes clinically detectable; in-transit
metastasis
Distant (8%) Stage IV: Distant metastatic disease

8th Edition AJCC Staging for MCC
Harms et al, 2016.
Stage Primary Tumor Lymph Node Metastasis
0 In situ (within epidermis only) No regional lymph node metastasis No distant metastasis
I Clinical ≤ 2 cm maximum tumor dimensionNodes negative by clinical exam
(no pathological exam performed)No distant metastasis
I Pathological ≤ 2 cm maximum tumor dimension Nodes negative by pathologic exam No distant metastasis
IIA Clinical > 2 cm tumor dimensionNodes negative by clinical exam
(no pathological exam performed)No distant metastasis
IIA Pathological > 2 cm tumor dimension Nodes negative by pathologic exam No distant metastasis
IIB ClinicalPrimary tumor invades
bone, muscle, fascia, or cartilage
Nodes negative by clinical exam
(no pathological exam performed)No distant metastasis
IIB PathologicalPrimary tumor invades
bone, muscle, fascia, or cartilageNodes negative by pathologic exam No distant metastasis
III Clinical Any size / depth tumor Nodes positive by clinical exam
(no pathological exam performed)No distant metastasis
IIIA Pathological
Any size / depth tumor Nodes positive by pathological exam only
(nodal disease not apparent on clinical exam)No distant metastasis
Not detected ("unknown primary")Nodes positive by clinical exam,
and confirmed via pathological examNo distant metastasis
IIIB Pathological Any size / depth tumor Nodes positive by clinical exam, and confirmed via
pathological exam OR in-transit metastasis***No distant metastasis
IV Clinical Any +/- regional nodal involvementDistant metastasis
detected via clinical exam
IV Pathological Any +/- regional nodal involvementDistant metastasis
confirmed via pathological exam
Local (65%)
Nodal (26%)
Distant (8%)
Current Management and Limitations
Local disease:Surgery and radiation○ >95% of patients “free of detectable disease” but nearly half
experience recurrence
Metastatic or locally advanced disease:(Used to be) chemotherapy (“small cell regimen”) ○ Shrinks MCC in most cases, but more than half progress by 3
months
Need more effective therapies
Recent successful trials of PD-1 axis blockade and
FDA approval of avelumab
PD-1 = programmed cell death protein 1.
Iyer et al, 2016; NCCN, 2017.

Immune Suppression and MCC
90% of patients with MCC do not have immune suppression
Early studies in HIV in 2002: 13-fold increased risk of MCC
Immune suppression is a (major) risk factor for MCC
Intensive search for pathogen
Paulson et al, 2013; Heath et al, 2008; Engels et al, 2002.

80% of MCCs Are Associated With
Merkel Cell Polyomavirus
MCC’s similarities to Kaposi’s sarcoma (caused by KSHV) raised
the possibility that MCC may have an infectious origin
MCPyV present in 8/10 MCCs
Validated in dozens of studies
KSHV = Kaposi’s sarcoma-associated herpes virus; MCPyV = Merkel cell polyomavirus.
Feng et al, 2008; Chun et al, 2013; Becker et al, 2009.

Merkel Cell Polyomavirus Genome
Feng et al, 2008.

Virus-Negative Tumors (~20%) Have
High Mutational Burden
NSCLC = non-small cell lung cancer; UV = ultraviolet; TIL = tumor-infiltrating lymphocytes; PD-L1 = programmed-death ligand 1.
Goh et al, 2016; Harms et al, 2015; Wong et al, 2015.
Virus-negative MCC tumors
have more tumor
neoantigens than melanomas
or NSCLC
Characterized by a prominent
UV-signature pattern
Subset of virus-negative
MCC tumors exhibit high TIL
and PD-L1 expression

Genetics of Virus-Positive vs
Virus-Negative MCC
Goh et al, 2015.
“MCC-high”
virus negative
“MCC-low”
virus positive
Exome sequenced tumor mutations
49 MCCs
To make an MCC:
Multiple UV mutations OR polyomavirus
Both “visible” to
immune system!
Seronegative
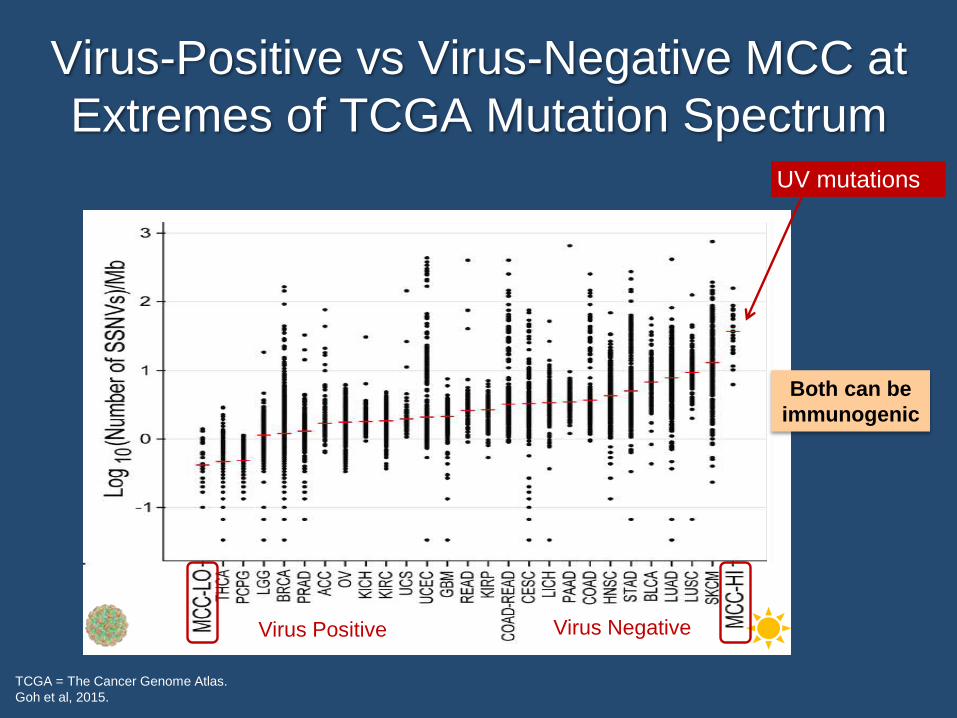
Virus-Positive vs Virus-Negative MCC at
Extremes of TCGA Mutation Spectrum
TCGA = The Cancer Genome Atlas.
Goh et al, 2015.
Both can be
immunogenic
UV mutations
Virus Positive Virus Negative

How Do CD8 T Cells
Recognize Their Target?
MCPyV-specific T cells
exist in blood & tumors
MCC-specific T cells
often “exhausted”
Target with PD-1 pathway
blockade?
Lyngaa et al, 2014; Iyer et al, 2014; Afanasiev & Nghiem, 2013.
Killer CD8 T cell
MCC cell expressing
MCPyV protein

Why Do Tumors Grow If Patients Have
(Virus-Specific) T Cells?
Photo Credit: Jim Dowdalls/Photo Researchers.
Virus infected cell
CD8
T cell
Are those T cells
dysfunctional?

T-Cell Surface Receptor Phenotype
Reveals Functional Profile
TNF = tumor necrosis factor; PD-L2 =
programmed death ligand 2
Afanasev & Nghiem, 2013.
Activated cells, characterized by expression of:
CD28 Costimulatory receptor (ligand: B7); required for T-cell activation
CD69 Earliest inducible cell surface glycoprotein during T-cell activation;
plays a role in T-cell proliferation
CD137
(4-1BB)
Member of TNF-receptor family; induced by T-cell activation;
important in T-cell proliferation, cytokine secretion, and cytotoxicity
CD38 Cyclic ADP ribose hydrolase; marker of T-cell activation; functions in
cell adhesion, signal transduction, and calcium signaling
HLA-DR MHC class-II surface receptor that is upregulated with T-cell
activation
Recently activated T cells, characterized by expression of:
Combination of activation and inhibition markers via appropriate
immunoregulatory feedback mechanisms
Exhausted T cells, characterized by prolonged expression of:
PD-1
Programmed death 1; inhibitory T-cell receptor (ligands: PD-L1
[B7-H1], PD-L2 [B7-DC]); reduces T-cell proliferation and
effector functions
CTLA-4
(CD152)
Cytotoxic T-lymphocyte antigen 4; inhibitory receptor (ligand: B7);
effectively competes for ligands with CD28 (which has lower avidity
than CTLA-4), preventing T-cell activation
Tim-3T-cell immunoglobulin mucin domain 3; inhibitory T-cell receptor
(ligand: galectin-9); leads to decrease in effector T-cell function
Acute antigen
exposure
T cell
Chronic antigen
exposure

Are the “Brakes” on in MCC-Specific
T Cells (vs Other Viral Responses)?
Tet = tetramer; CMV = cytomegalovirus; EBV = Epstein-Barr virus.
Afanasiev et al, 2013.
Detected “exhausted” PD-1+/Tim-3+ cells
using “tetramers” to isolate specific cells
(Data From 4–7 MCC Patients)
PD
-1+
Tim
-3+
(%
Po
sit
ive
Ce
lls
)
PD-1Tim-3
Target PD-1
and PD-L1?

Brakes and Accelerators of the
T-Cell Response
Drake et al, 2014.
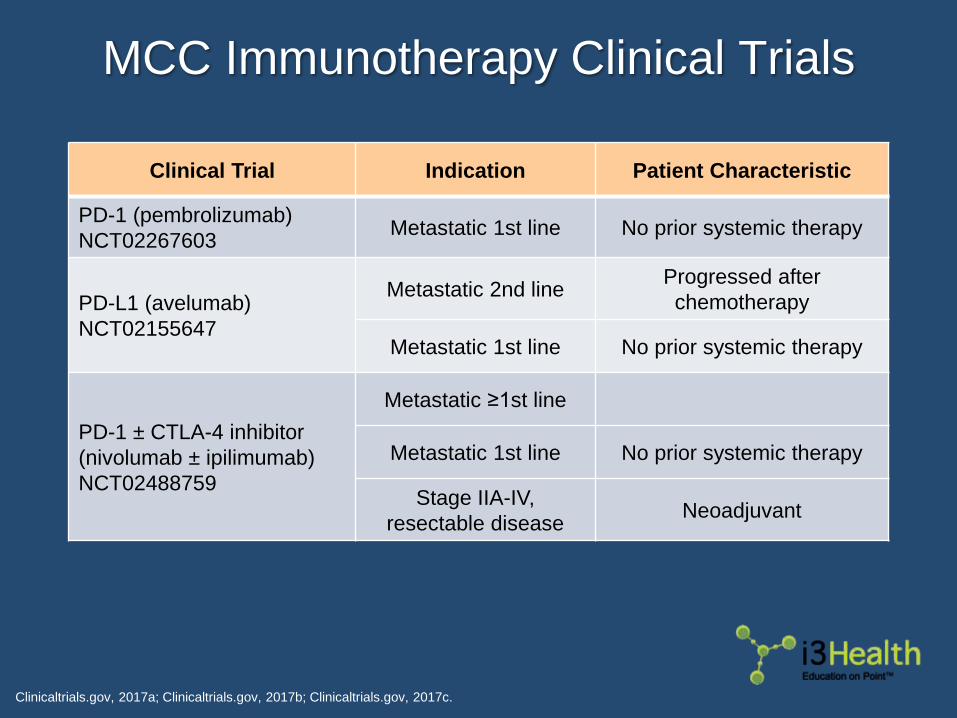
MCC Immunotherapy Clinical Trials
Clinicaltrials.gov, 2017a; Clinicaltrials.gov, 2017b; Clinicaltrials.gov, 2017c.
Clinical Trial Indication Patient Characteristic
PD-1 (pembrolizumab)
NCT02267603Metastatic 1st line No prior systemic therapy
PD-L1 (avelumab)
NCT02155647
Metastatic 2nd line Progressed after
chemotherapy
Metastatic 1st line No prior systemic therapy
PD-1 ± CTLA-4 inhibitor
(nivolumab ± ipilimumab)
NCT02488759
Metastatic ≥1st line
Metastatic 1st line No prior systemic therapy
Stage IIA-IV,
resectable diseaseNeoadjuvant

Response Rates for Chemotherapy
vs PD-1 Axis Blocking Agents
ORR = overall response rate; NCCN = National Comprehensive Cancer Network.
Iyer et al, 2016; Kaufman et al, 2016; Nghiem et al, 2016; Topalian et al, 2017; NCCN, 2017.
Agents Response Study Status in MCC
Chemotherapy 55% ORR
1st-line treatment,
retrospective study for 62
patients, Iyer et al, 2016
Included in NCCN
guidelines based on
historical/clinical
experiences
Agents Response Study Status in MCC
Chemotherapy 55% ORR
1st-line treatment,
retrospective study for 62
patients, Iyer et al, 2016
Included in NCCN
guidelines based on
historical/clinical
experiences
Avelumab 32% ORR≥2nd-line trial,
Kaufman et al, 2016
FDA-approved: 1st
and ≥ 2nd line, 3/2017
Agents Response Study Status in MCC
Chemotherapy 55% ORR
1st-line treatment,
retrospective study for 62
patients, Iyer et al, 2016
Included in NCCN
guidelines based on
historical/clinical
experiences
Avelumab 32% ORR≥2nd-line trial,
Kaufman et al, 2016
FDA-approved: 1st
and ≥ 2nd line, 3/2017
Pembrolizumab 56% ORR1st-line trial, Nghiem et al,
2016
NCCN guideline for
MCC, 2017
Agents Response Study Status in MCC
Chemotherapy 55% ORR1st-line retrospective study
(N=62), Iyer et al, 2016
Included in NCCN
guidelines based on
historical/clinical
experiences
Avelumab 32% ORR≥2nd-line trial (N=88),
Kaufman et al, 2016
FDA-approved:
1st and ≥2nd line,
3/2017
Pembrolizumab 56% ORR1st-line trial (N=25),
Nghiem et al, 2016
NCCN guideline for
MCC, 2017
Nivolumab 73% ORR
1st- and ≥2nd-line trial
(N=25), Topalian et al,
2017
Public efficacy data
Unclear whether agents differ in response rate.
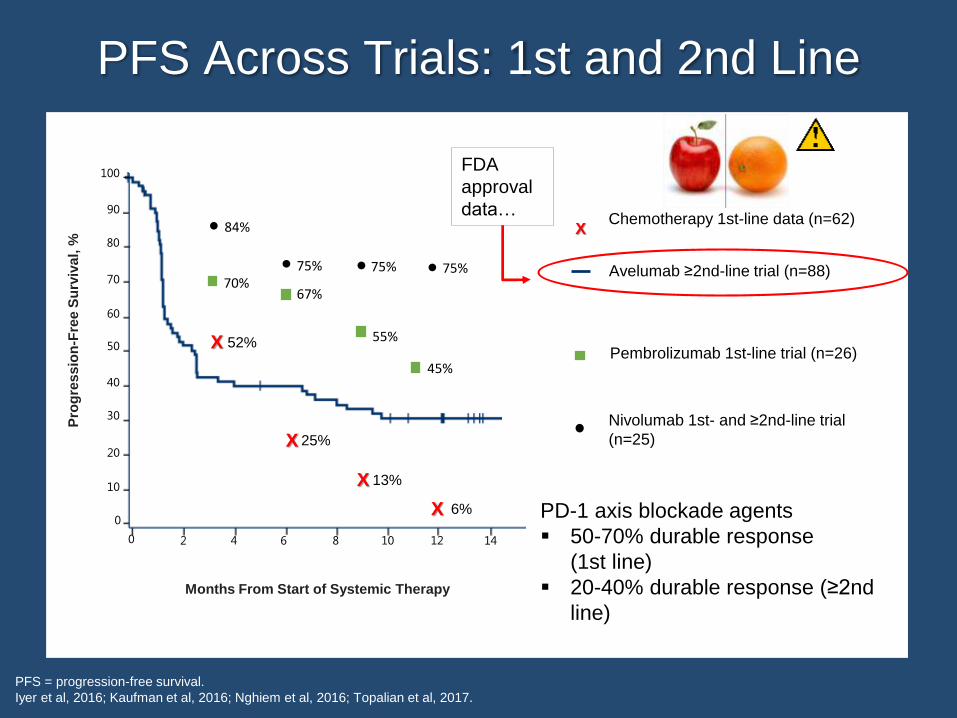
PFS Across Trials: 1st and 2nd Line
PFS = progression-free survival.
Iyer et al, 2016; Kaufman et al, 2016; Nghiem et al, 2016; Topalian et al, 2017.
Pembrolizumab 1st-line trial (n=26)
Avelumab ≥2nd-line trial (n=88)
FDA
approval
data…
Nivolumab 1st- and ≥2nd-line trial
(n=25)
PD-1 axis blockade agents
50-70% durable response
(1st line)
20-40% durable response (≥2nd
line)
45%
70%
55%
67%
84%
75% 75% 75%
52%X
25%X
13%X
6%X
Chemotherapy 1st-line data (n=62)X
100
80
90
70
Pro
gre
ss
ion
-Fre
e S
urv
iva
l, %
Months From Start of Systemic Therapy
60
50
40
30
20
10
0
0 2 4 6 8 10 12 14

Checkpoint Inhibitors: A New Standard
of Care for Advanced MCC?
October 2016: Anti–PD-1 (pembrolizumab) listed in
NCCN guidelines for MCC
March 2017: Anti–PD-L1 (avelumab) FDA approved for
MCC
“Taken together, these reports strongly suggest
that checkpoint blockade is the best option to treat
patients with advanced Merkel cell carcinoma…”
– Axel Hauschild & Dirk Schadendorf
Hauschild & Schadendorf, 2016; NCCN, 2017.
PD-1 Axis Blockade for MCC
Metastatic MCC
Most responses by 8‐12 weeks
Optimal duration of therapy is not known1-2 years after best response?
Restarting PD-1 blocking agents for progression after treatment
completed
Kaufman et al, 2016.

Case 1: PD-1 Axis Blockade for MCC
55-year-old woman
History:5/2014 – Patient noticed a 1-cm growing nodule on the
left chest skin
7/2014 – Skin biopsy showed MCC
8/2014 – PET/CT showed FDG-avid liver lesions
8/2014 – Liver biopsy showed metastatic MCC
Diagnosis: Stage IV metastatic MCC involving liver
(2 x 11 cm) and left chest
PET/CT = positron emission tomography/computed tomography; FDG = fluorodeoxyglucose.
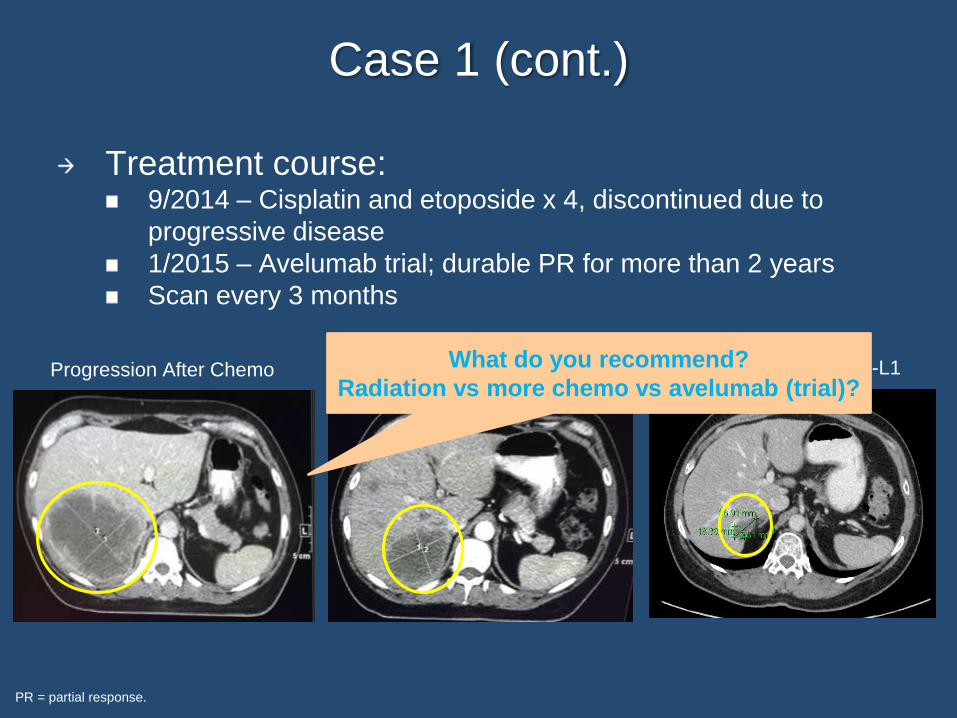
Case 1 (cont.)
Treatment course:9/2014 – Cisplatin and etoposide x 4, discontinued due to
progressive disease
1/2015 – Avelumab trial; durable PR for more than 2 years
Scan every 3 months
PR = partial response.
After 4 Weeks (2 Doses) of PD-L1 After 20 Months of PD-L1What do you recommend?
Radiation vs more chemo vs avelumab (trial)?Progression After Chemo
Case 2: PD-1 Axis Blockade Combined
With Pain Management
56-year-old woman
History:9/2013 – Stage IB MCC of the right calf with clinically negative
LN, s/p WLE
11/2016 – Metastatic MCC of the right kidney, s/p right
nephrectomy
1/2017 – Patient developed worsening right-sided abdominal
pain
2/2017 – PET/CT showed enlarged retroperitoneal LN adjacent
to the nephrectomy bed
3/2017 – Biopsy of the LN showed MCC
Diagnosis: Metastatic MCC involving retroperitoneal LN
LN = lymph node; s/p = status post; WLE = wide local excision.

Case 2 (cont.)
Treatment course:3/2017 – Single fraction radiation treatment (8 Gy) to
symptomatic lesion
3/2017 – Pembrolizumab with CR on 6/2017 scan
Scan every 3 months
CR = complete response.
Iyer et al, 2015.
Iyer and colleagues (2015): Single-fraction
radiation therapy in patients with
metastatic Merkel cell carcinoma.
Challenges:
1. Acute severe pain due to a small
metastasis
2. Uncertainty whether PD-1 alone
will work
3. High risk of metastasis to other
sites
Our decision through
multidisciplinary discussion…
3/2017 – Painful Metastasis
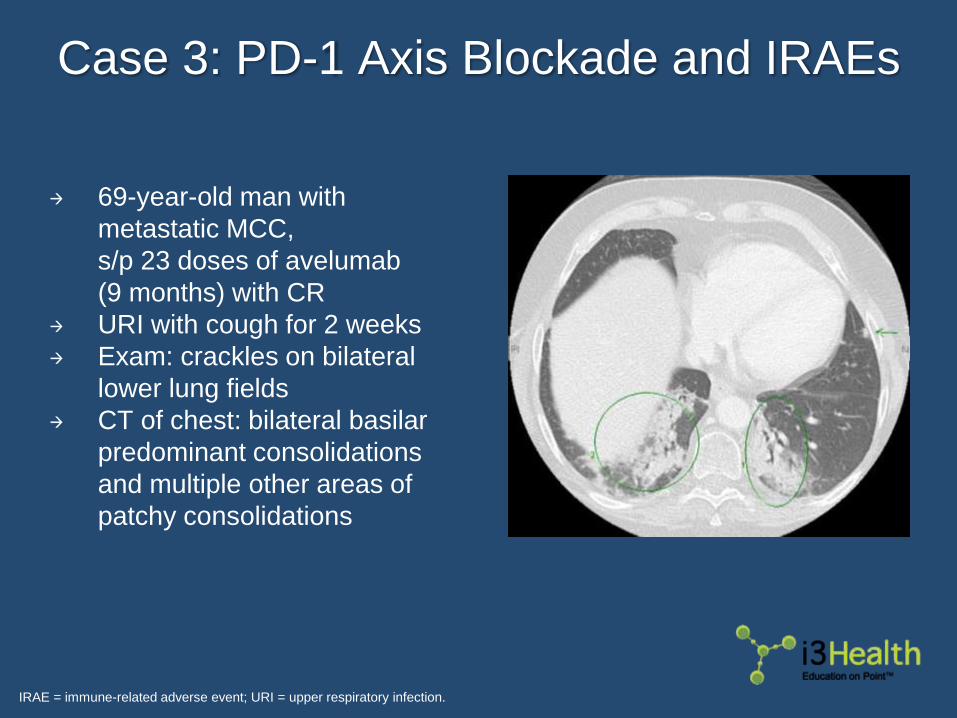
Case 3: PD-1 Axis Blockade and IRAEs
69-year-old man with
metastatic MCC,
s/p 23 doses of avelumab
(9 months) with CR
URI with cough for 2 weeks
Exam: crackles on bilateral
lower lung fields
CT of chest: bilateral basilar
predominant consolidations
and multiple other areas of
patchy consolidations
IRAE = immune-related adverse event; URI = upper respiratory infection.

Case 3 (cont.)
Function deteriorated despite empiric antibiotics for
presumed aspiration pneumonia (dyspnea, unable
to walk through grocery store)
TreatmentHold avelumab
Admission, high-dose systemic steroids and empiric antibiotics
Bronchoscopy with lavage and tissue biopsies
Patient subsequently improved; presumed pneumonitis
Pneumonia vs Pneumonitis

Adverse Events Can Be Significant
Common:Fatigue (50%)
Musculoskeletal pain (32%)
Diarrhea (23%)
Infusion-related reactions (22%)
Rash (22%)
Abnormal CBC (~49%), LFT (~34%)
CBC = complete blood count; LFT = liver function test.
Bavencio® prescribing information, 2017.

IRAEs Can Affect Any Organ System
Hypophysitis
Thyroiditis
Adrenal insufficiency
Diabetes mellitus
Enterocolitis
Dermatitis
Arthritis
Pneumonitis
Hepatitis/
pancreatitis
Nephritis
Neuropathies
And many
more…

Laboratory Monitoring
Prior to each dose:Careful clinical evaluation – Assess for immune-mediated
adverse events
CBC with differential, CMP, TFTs, cortisol, lipase
Cannot predict who will experience IRAEs
Radiologic assessment prior to start of therapy and:As needed to evaluate for IRAEs (eg, pneumonitis)
Approximately every 8-12 weeks thereafter
CMP = comprehensive metabolic panel; TFT = thyroid function test.

Approach to Potentially
Immune-Mediated Symptoms
Drug-induced until proven otherwise; often
diagnosed by exclusionOther causes must be ruled out (infections, reactions to
other medications, metabolic causes, neoplasm)
Educate the entire team!Any organ system can be affected
Early recognition, evaluation, and treatment are critical
for patient safety
IRAEs can occur ~2 years even after the
discontinuation of medication

General Toxicity Management
Discontinuation favored over dose reduction
Steroids often indicated and do not reverse antitumor effects in most
patients
Min et al, 2015; Abdel-Wahab et al, 2016.
Grade Recommendation
1 (mild) Supportive care; may or may not withhold therapy
2 (moderate) Withhold therapy; may consider restarting therapy in future
if resolves to grade ≤ 1
Low-dose corticosteroids (prednisone 0.5 mg/kg/d or
equivalent) given if symptoms do not resolve in 1 wk
3/4 (severe)
Discontinue therapy, consider permanent discontinuation
Use high-dose corticosteroids (prednisone 1-2 mg/kg/d or
equivalent) tapered SLOWLY over ≥1 mo once toxicity
resolves to grade ≤1
Grade Recommendation
1 (mild) Supportive care; may or may not withhold therapy
2 (moderate)
Withhold therapy; may consider restarting therapy in future
if resolves to grade ≤1
Low-dose corticosteroids (prednisone 0.5 mg/kg/d or
equivalent) given if symptoms do not resolve in 1 wk
Grade Recommendation
1 (mild) Supportive care; may or may not withhold therapy

IRAEs Associated With Avelumab
PFT = pulmonary function test; Cr = creatinine; CCr = creatinine clearance rate; DM = diabetes mellitus; DKA =
diabetic ketoacidosis.
Bavencio® prescribing information, 2017.
IRAE Freq. Detection Onset (mo)Duration
(median)Note
Thyroid
disorders6% Exam, TFT
2.3
(2 wk – 13 mo)
Often
permanent
Colitis 1.5%Exam,
colonoscopy
2.1
(2 d - 11 mo)6 wk
Pneumonitis 1.2% Exam, CT, PFT2.5
(3 d - 11 mo)7 wk
Hepatitis 0.9% Exam, LFT3.2
(1 wk - 15 mo)2.5 mo
Adrenal
insufficiency0.5% Exam, cortisol
2.5
(1 d - 8 mo)n/a
Nephritis 0.1% Exam, Cr, CCr n/a n/a
Type 1 DM 0.1% Exam, blood n/a n/aPossible
DKA

Controversies Surrounding
PD-1 Blockade in MCC
How long to treat?6-12 months after complete/deep-stable disease response?
Until IRAE develops?
Refractory disease…Combination therapies?
Follow-up?

Follow-Up
No data to guide recommendations for surveillance in
patients with recurrence/metastasis
Follow-up as high-risk patients?
NCCN, 2017.

Future Directions
Combinations with anti–PD-1 therapy under
investigation:CTLA-4 blockade (ipilimumab)
MCPyV-specific T cells○ Transgenic T-cell receptors
Natural killer cells with IL-15
T-VEC
CD47
Many more
Adjuvant immunotherapy?Avelumab (US trial)
Ipilimumab (EU trial)
IL-15 = interleukin-15; T-VEC = talimogene laherparepvec; CD47 = cluster of differentiation 47.

Key Takeaways
PD-1 pathway blockade preferred over
chemotherapy in 1st line for MCC due to improved
chance for durable response
Avelumab is approved based on ≥2nd-line data
Publicly available data support the use of
pembrolizumab and nivolumab
A multidisciplinary approach is essential for
optimal MCC management
Careful monitoring for adverse events is critical

Questions?

References
Abdel-Wahab N, Shah M & Suarez-Almazor ME (2016). Adverse events associated with immune checkpoint blockade in patients with cancer: a
systematic review of case reports. PLoS One, 11(7):e0160221. DOI:10.1371/journal.pone.0160221
Afanasiev O & Nghiem P (2013). Track and attack: emerging prognostic and therapeutic approaches. Merkel Cell Carcinoma. 1st edition.
Springer:180.
Afanasiev OK, Yelistratova L, Miller N, et al (2013). Merkel polyomavirus-specific T cells fluctuate with Merkel cell carcinoma burden and
express therapeutically targetable PD-1 and Tim-3 exhaustion markers. Clin Cancer Res, 19(19):5351-5360. DOI:10.1158/1078-
0432.ccr-13-0035
American Cancer Society (2016). Key statistics for Merkel cell carcinoma. Available at: http://www.cancer.org
Bavencio (avelumab) prescribing information (2017). EMD Serono. Available at:
https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/761049s000lbl.pdf
Becker JC, Houben R, Ugurel S, et al (2009). MC polyomavirus is frequently present in Merkel cell carcinoma of European patients. J Invest
Dermatol, 129(1):248-250. DOI:10.1038/jid.2008.198
Chun SM, Yun SJ, Lee SC, et al (2013). Merkel cell polyomavirus is frequently detected in Korean patients with Merkel cell carcinoma. Ann
Dermatol, 25(2):203-207. DOI:10.5021/AD.2013.25.2.203
Clinicaltrials.gov (2017a). Pembrolizumab in treating patients with advanced Merkel cell cancer. Available at: http://clinicaltrials.gov. NLM
identifier: NCT02267603
Clinicaltrials.gov (2017b). Avelumab in subjects with merkel cell carcinoma (JAVELIN Merkel 200). Available at: http://clinicaltrials.gov. NLM
identifier: NCT02155647
Clinicaltrials.gov (2017c). An investigational immuno-therapy stiudy to investigate the safety and effectiveness of nivolumab, and nivolumab
conbination therapy in virus-associated tumors (CheckMate358). Available at: http://clinicaltrials.gov. NLM identifier: NCT02488759
Drake CG, Lipson EJ & Brahmer JR (2014). Breathing new life into immunotherapy: review of melanoma, lung and kidney cancer. Nat Rev Clin
Oncol, 11(1):24-37. DOI:10.1038/nrclinonc.2013.208

References
Edge SB, Byrd DR, Compton CC, et al (2010). AJCC Cancer Staging Manual. 7th edition. Springer:315-324.
Engels EA, Frisch M, Goedert JJ, et al (2002). Merkel cell carcinoma and HIV infection. Lancet, 359(9305):497-498. DOI:10.1016/s0140-
6736(02)07668-7
Feng H, Shuda M, Chang Y & Moore PS (2008). Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science,
319(5866):1096-1100. DOI: 10.1126/science.1152586
Goh G, Walradt T, Markarov V, et al (2016). Mutational landscape of MCPyV-positive and MCPyV-negative Merkel cell carcinomas with
implications for immunotherapy. Oncotarget, 7(3):3403-3415. DOI:10.18632/oncotarget.6494
Harms KL, Healy MA, Nghiem P, et al (2016). Analysis of prognostic factors from 9387 Merkel cell carcinoma cases forms the basis for the new
8th edition AJCC staging system. Ann Surg Oncol, 23(11):3564-3571.
Harms PW, Vats P, Verhaegen ME, et al (2015). The distinctive mutational spectra of polyomavirus-negative Merkel cell carcinoma. Cancer
Res, 75(18):3720-3727. DOI:10.1158/0008-5472.can-15-0702
Hauschild A & Schadendorf D (2016). Checkpoint inhibitors: a new standard of care for advanced Merkel cell carcinoma? Lancet Oncol,
17(10):1337-1339. DOI:10.1016/s1470-2045(16)30441-7
Heath M, Jaimes N, Lemos B, et al (2008). Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J
Am Acad Dermatol, 58(3):375-381. DOI:10.1016/j.jaad.2007.11.020
Ilcus C, Bagacean C, Tempescul A, et al (2017). Immune checkpoint blockade: the role of PD-1-PD-L axis in lymphoid malignancies. Onco
Targets Ther, 10:2349-2363. DOI:10.2147/ott.s133385
Iyer JG, Blom A, Doumani R, et al (2016). Response rates and durability of chemotherapy among 62 patients with metastatic Merkel cell
carcinoma. Cancer Med, 5(9):2294-2301. DOI:10.1002/cam4.815
Iyer JG, Parvathaneni U, Gooley T, et al (2015). Single-fraction radiation therapy in patients with metastatic Merkel cell carcinoma. Cancer Med,
4(8):1161-1170. DOI:10.1002/cam4.458
Kaufman HL, Russell J, Hamid O, et al (2016). Avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma: a
multicentre, single-group, open-label, phase 2 trial. Lancet Oncol, 17(10):1374-1385. DOI:10.1016/s1470-2045(16)30364-3
References
Lyngaa R, Pedersen NW, Schrama D, et al (2014). T-cell responses to oncogenic Merkel cell polyomavirus proteins distinguish patients with
Merkel cell carcinoma from healthy donors. Clin Cancer Res, 20(7):1768-1778. DOI:10.1158/1078-0432.ccr-13-2697
Menzies AM, Johnson DB, Ramanujam S, et al (2017). Anti-PD-1 therapy in patients with advanced melanoma and preexisting autoimmune
disorders or major toxicity with ipilimumab. Ann Onc, 28(2):368-376. DOI:10.1093/annonc/mdw443
Miller RW & Rabkin CS (1999). Merkel cell carcinoma and melanoma: etiological similarities and differences. Cancer Epidemiol Biomarkers
Prev, 8(2):153-158.
Min L, Holdi FS & Kaiser UB (2015). Corticosteroids and immune checkpoint blockade. Aging, 7(8):521-522. DOI:10.18632/aging.100797
National Comprehensive Cancer Network (2017). NCCN Clinical Practice Guidelines in Oncology: Merkel cell carcinoma. Version 1.2018.
Available at: http://www.nccn.org
Nghiem PT, Bhatia S, Lipson EJ, et al (2016). PD-1 blockade with pembrolizumab in advanced Merkel-cell carcinoma. N Engl J Med,
374(26):2542-2552. DOI:10.1056/NEJMoa1603702
Ong M, Ibrahim AM, Bourassa-Blanchette S, et al (2016). Antitumor activity of nivolumab on hemodialysis after renal allograft rejection. J
Immunother Cancer, 4(64). DOI:10.1186/s40425-016-0171-8
Paulson KG, Iyer JG, Blom A, et al (2013). Systemic immune suppression predicts diminished Merkel cell carcinoma—specific survival
independent of stage. J Invest Dermatol, 133(3):642-646. DOI:10.1038/jid.2012.388
Paulson KG, Park SY, Vandeven NA, et al (2017). Merkel cell carcinoma: current United States incidence and projected increases based on
changing demographics. J Amer Acad Dermatol. [Epub ahead of print] DOI:10.1016/i.jaad.2017.10.028
Topalian SL, Bhatia S, Hollebecque A, et al (2017). Non-comparative, open-label, multiple cohort, phase 1/2 study to evaluate nivolumab
(NIVO) in patients with virus-associated tumors (CheckMate 358): efficacy and safety in Merkel cell carcinoma. Proc Am Assoc Cancer
Res, 77(13). Abstract CT074. DOI:0.1158/1538-7445.AM2017-CT074
Wong SQ, Waldeck K, Vergara IA, et al (2015). UV-associated mutations underlie the etiology of MCV-negative Merkel cell carcinomas. Cancer
Res, 75(24):5228-5234. DOI:10.1158/0008-5472.can-15-1877