organic mood disorder and avm
DESCRIPTION
This is real case in UMMC, Malaysia... We've learn a lot by only 1 patient.... It is good if we can elicit the higher function of this patient.TRANSCRIPT
MEDICINEPSYCHOLOGICAL
CONFERENCE
MOHD
HANAFI
NG
BOON KEAT
MR. S
55-year-old | Security Guard
Married | 3 children
Progressively worsened disturbed behaviour for 4 days
HISTORY OF PRESENT ILLNESS• Brought by the son to the accident and
emergency due to bizarre behaviours:– Appeared to be irritable and aggressive– Shouting with vulgar words– No physical damages to self or other
people
• Known case of psychiatric illness, under UMMC follow-up
WITHIN 3 DAYS• Decrease need for sleep • Increase activities
– Wandering around the house non-stop– Pacing faster than normal
• Talkative– Described as talking non-sense
• Impaired functions– Cannot do daily activities properly– Getting complains from working colleagues
• Mood is happy without reason
FURTHER CURRENT HISTORY
• No psychotic symptoms• No depressive symptoms• Clear history of past depressive
episodes
THINK?????
DO YOU
WHAT
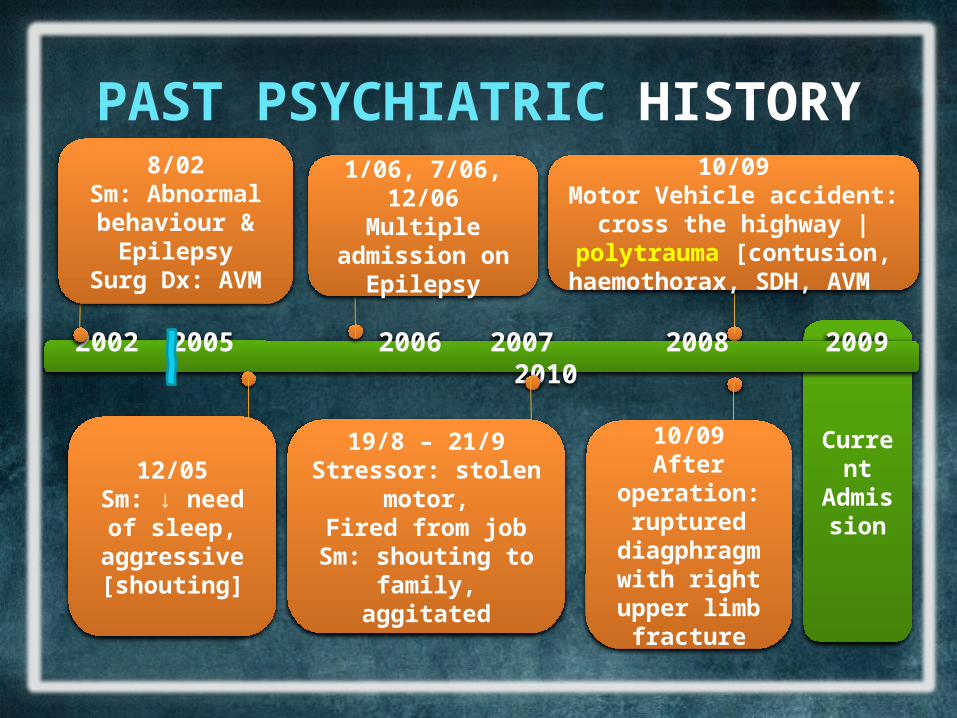
PAST PSYCHIATRIC HISTORY
• Since 2002 Multiple admission due to inappropriate behavior with depression.
• Treated with:– Lorazepam | anxiolytic– Chlopromazine | antipsychotic– Perphenazine | antipsychotic– Carbamazepine | anxiolytic
• Poor compliance to medication
Current Admissi
on
2002 2005 2006 2007 2008 2009 2010
8/02Sm: Abnormal behaviour &
EpilepsySurg Dx: AVM
12/05Sm: ↓ need of
sleep, aggressive [shouting]
1/06, 7/06, 12/06Multiple admission
on Epilepsy
19/8 – 21/9Stressor: stolen motor,
Fired from jobSm: shouting to family,
aggitated
10/09Motor Vehicle accident: cross the highway | polytrauma [contusion,
haemothorax, SDH, AVM
PAST PSYCHIATRIC HISTORY
10/09After operation:
ruptured diagphragm
with right upper limb fracture
PAST MEDICAL HISTORY• Known case of epilepsy since young.• Patient was seeking psychiatric
service in UMMC in 2002 and was referred to surgical team the same year.
• Diagnosed to have arteriovenous malformation.
• Healthy without other medical conditions.• No previous history of ECT:
– AVM– Epilepsy
• Follow-up in neuro-surgical and neuro-medical clinic.
• Relatively “stable”
FAMILY HISTORY
• No psychiatric, suicide history in the family
• No history of epilepsy, neurological disease in the family.
• Family relationships are good.
d. | unknown cause
70 | housewife | no medical illness
PERSONAL HISTORY: EARLY CHILDHOOD
13/4/1955 | Alor Star
uncomplicated FTSVD | village midwife.
No health problems | No developmental delay
PERSONAL HISTORY: SCHOOL PERFORMANCE
SRK Kancut | SMK Syed Omar– Moderate achievement in primary
school– Drop-out of school after SRP due to
poor performance– No disciplinary problem– Socialize with friends
PERSONAL HISTORY: WORK RECORDS
Move to Kuala Lumpur | 18-year-old
Work | security guard since then.
Never change his job.
Income | around RM1000
PERSONAL HISTORY: SEXUAL ATTITUDE AND PRACTICE
No sexual experience | before marriage
1st intercourse | age of 30
No history of child abuse
PERSONAL HISTORY: MARRIAGE
Arranged by parents
His wife: 53 year old | Freelance teacher | Had been supportive to the husband despite his condition
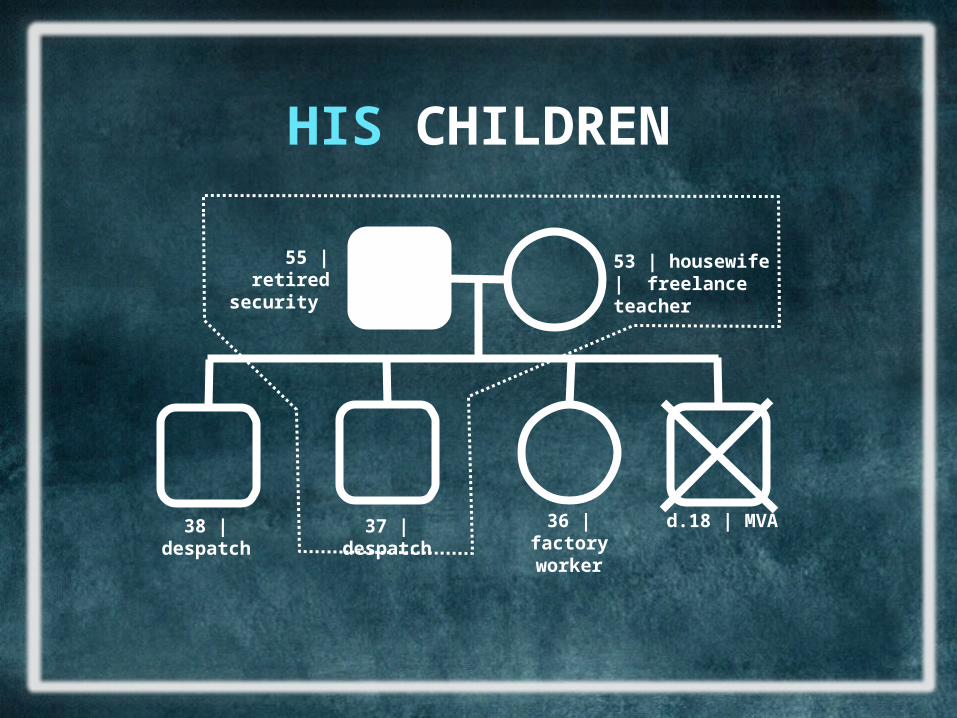
HIS CHILDREN
55 | retired security
53 | housewife | freelance teacher
38 | despatch 37 | despatch 36 | factory worker
d.18 | MVA
PERSONAL HISTORY: SOCIO-CULTURAL BACKGROUND
RM5000 family income per month??
Socialize with friends?
No criminal records
$
PERSONAL HISTORY: SUBSTANCE USE
Smoking | 74 pack years
No alcohol consumption |
No substance abuse
PERSONAL HISTORY: PRE-MORBID PERSONALITY
Proper social | relationships
Stable mood | but depress occasionally
Personality trait??
Weak faith | religion
Favourite past time | sports
Coping skill | sports
MENTAL STATE: GENERAL APPEARANCE
Alert | conscious | cooperative
Easily make rapport | poor eye contact
Hospital attire | unhygienic
Anxious | frowning of the forehead
MENTAL STATE: SPEECH & THOUGHT
↑ amount | ↑ tone | ↑ rate
Pressured speech
Malay-spoken | coherence but irrelevance
thought blocking | flight of ideas
NO
Loose/clang association | circumstantialities | neologism | obsession/phobua | delusions
Suicidal thought
MENTAL STATE: MOOD & PERCEPTION
Sad in mood
Inappropriate affect | incongruent
NO
Hallucinations| Pseudohallucinations |Illusions| Derealization/Depersonalization| Flashback
MENTAL STATE: COGNITIVE FUNCTION
Time, Place, Person | Orientated
Remote, Recent Memory | Good [date of birth & breakfast]
5mins memory test | Remember only 1
Information/knowledge | Appropriate
Proverbs | Can answer [Udang di sebalik batu & sikit-sikit lama-lama jadi bukit]
Similarities | Give 2 [apple & orange: tastes, eaten]
MENTAL STATE: COGNITIVE FUNCTION 2
Attention | Easily distracted
Concentration | Cant do it [serial 7 test, digit span, world backward]
Judgement | Cant assess[patient started irritable and agitated]
Insight | Poor [he and others do not realised his abnormality | not accept and do not need
treatment]

PHYSICAL EXAMINATION
Alert | conscious | not in respiratory distress.
37.5˚C | 92 beats pm | 20 bpm | 120/80.
Couldn’t assess
1st day | patient irritable and agitated
2nd day | patient physically restrained and chemically sedated
IN SUMMARY
History | irritable, aggressive and shouting for 4 days, with maniac symptoms | no depressive
symptoms within the current period
Previous History | psychiatric illness since 2002 | not complicant with medication | Complicated with
AVM and MVA
Mental State | easily distracted | mostly cannot assess| poor insight
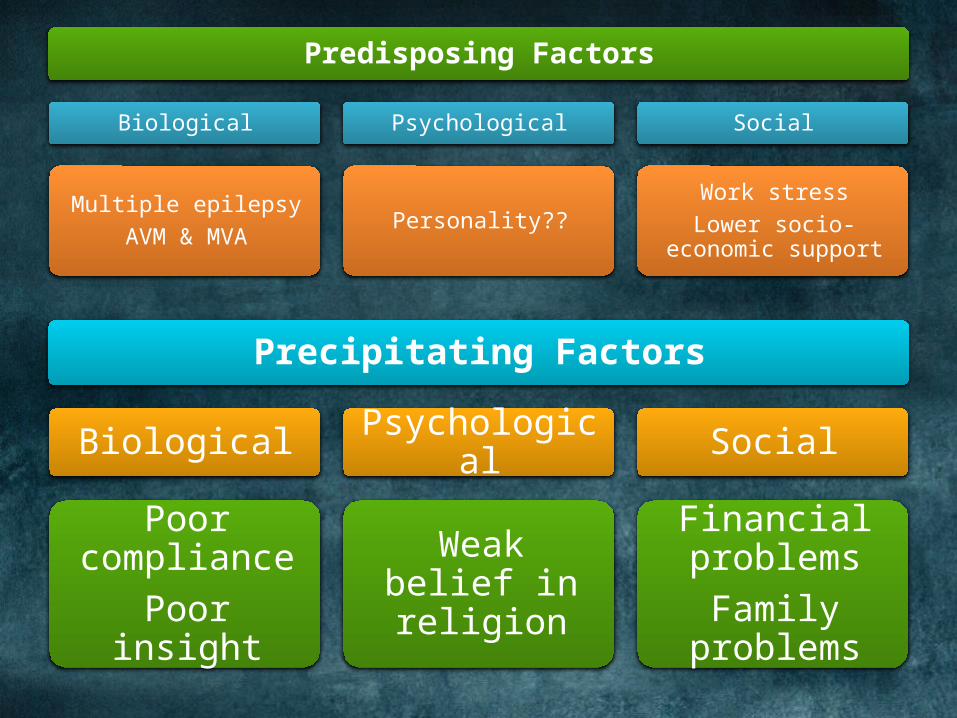
Predisposing Factors
Biological
Multiple epilepsyAVM & MVA
Psychological
Personality??
Social
Work stressLower socio-economic
support
Precipitating Factors
Biological
Poor compliancePoor insight
Psychological
Weak belief in religion
Social
Financial problems
Family problems
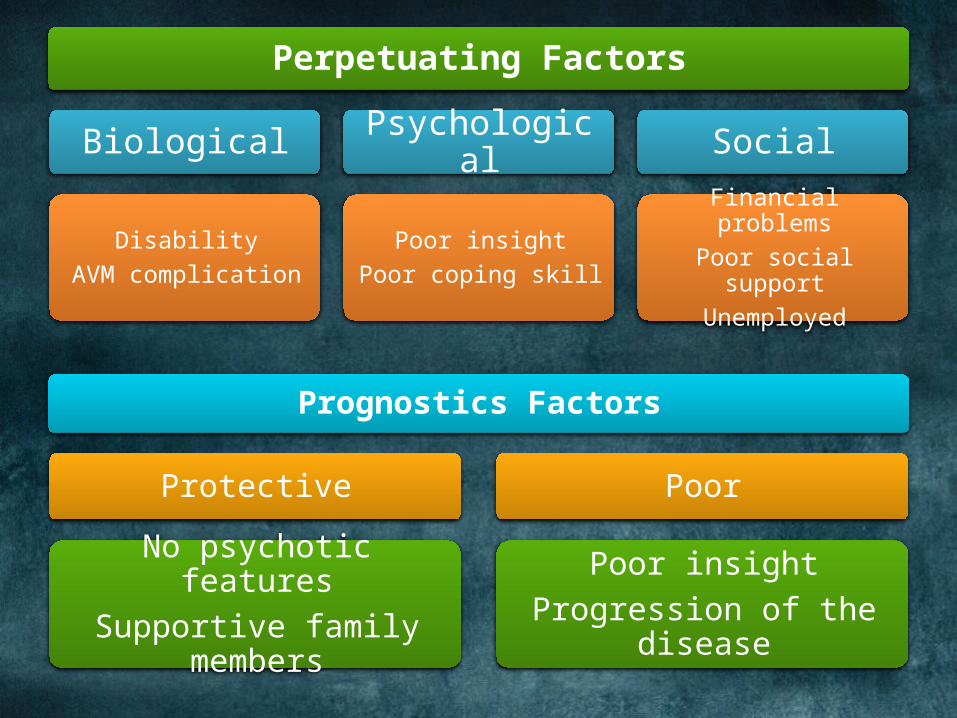
Perpetuating Factors
Biological
DisabilityAVM complication
Psychological
Poor insightPoor coping skill
Social
Financial problemsPoor social support
Unemployed
Prognostics Factors
Protective
No psychotic featuresSupportive family members
Poor
Poor insightProgression of the disease
LIKELYIS THE MOSTWHAT
PROVISIONAL DIAGNOSIS?
PROVISIONAL DIAGNOSIS
• manic episode • The patient has had at
least one previous major depressive episode, manic
episode, or mixed episode
BIPOLAR I DISORDER
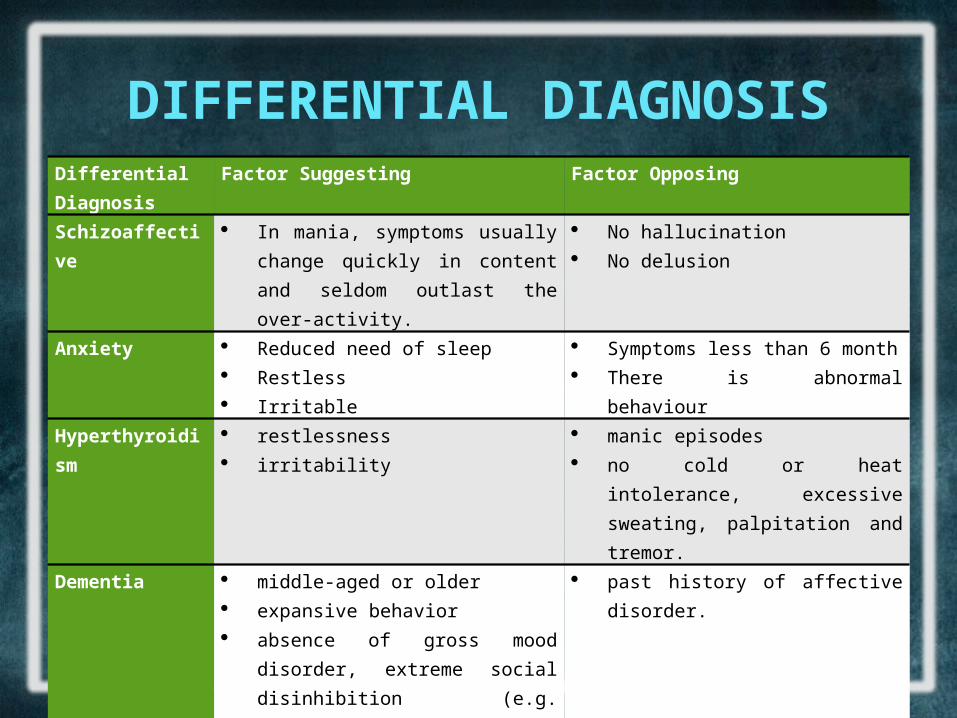
DIFFERENTIAL DIAGNOSISDifferential Diagnosis
Factor Suggesting Factor Opposing
Schizoaffective In mania, symptoms usually change quickly in content and seldom outlast the over-activity.
No hallucination No delusion
Anxiety Reduced need of sleep Restless Irritable
Symptoms less than 6 month There is abnormal behaviour
Hyperthyroidism restlessness irritability
manic episodes no cold or heat intolerance, excessive
sweating, palpitation and tremor. Dementia middle-aged or older
expansive behavior absence of gross mood disorder,
extreme social disinhibition (e.g. urinating in public) strongly suggests frontal lobe pathology.
past history of affective disorder.
Substance Abuse state of excitement. Cannot elicit usage of drugs [amphetamine]
WARD: Investigation done
Full Blood Count | Liver Function Test | Glucose Level | Renal Profile
Normal
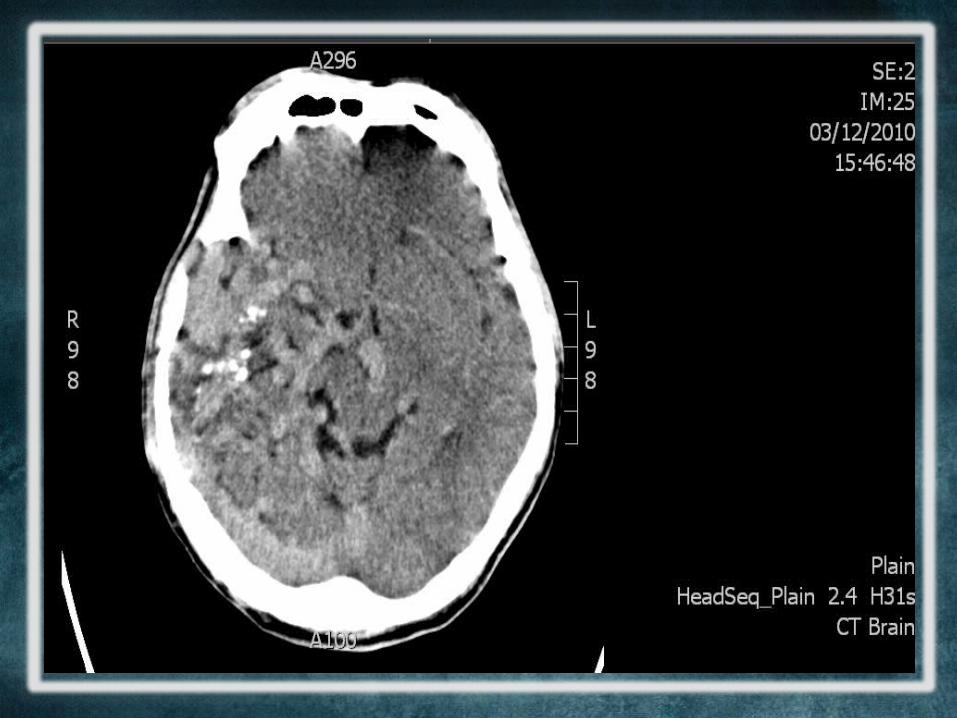
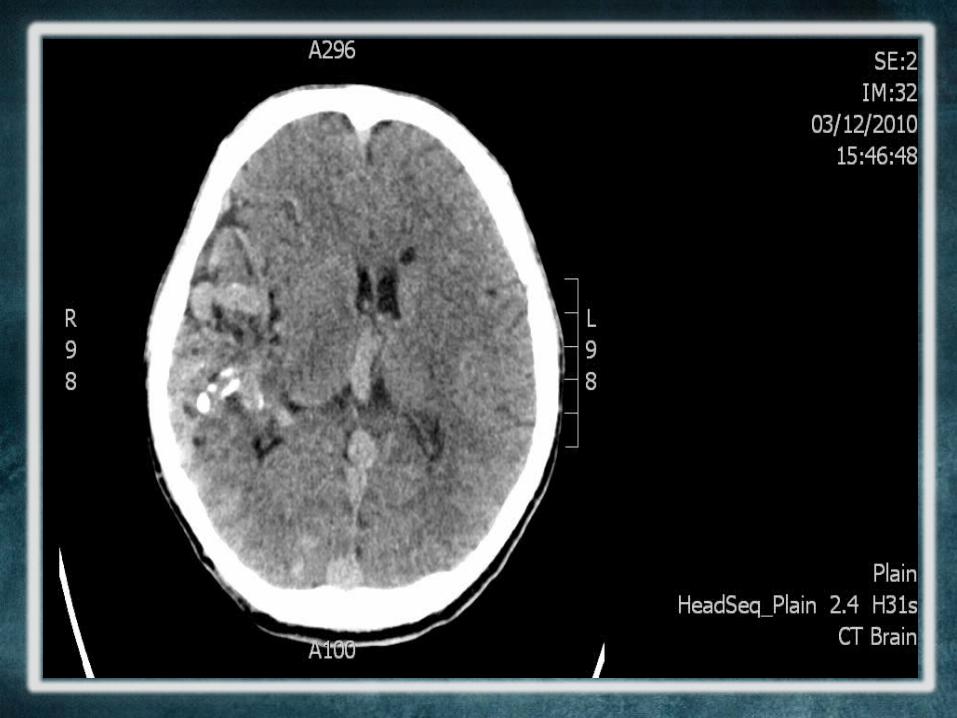
CT Brain was ordered…..
PROVISIONAL DIAGNOSIS
ORGANIC MOOD DISORDER

FINAL DIAGNOSIS: AXIS
Axis Multi-axial Classification
Diagnosis
Axis I Clinical Disorder 293.83: Mood disorder due to a general medical condition
Axis II Personality Disorder/Mental R.
nil
Axis III General Medical Condition
Arterio-venous Malformation [Diseases of the vascular]
Axis IV Psychosocial & Environment
Economic problems
Axis V Global Assessment of Functioning
50 [Some Serious Symptoms or Serious Impairment in Functioning]
MANAGEMENT IN THE WARD
| Psychiatric View | • Psychotic medication not aim to
cure the organic condition• ECT cancelled
• Given Rozidal, Carbamazepine, Lorazepam, Chlorphomazine
MANAGEMENT IN THE WARD
| Neurosurgical View | • CT Brain done Cerebral oedema and complex AVM
• No surgical management available (grade 5 AVM)

NEURO-
PSYCHOLO
GICAL
CORRELATIO
NSDISSCUSIO
N
FROM THE NEUROLOGICAL ASPECT
• AVM• Mania and
frontal lobe
MANIA AND FRONTAL LOBE• Secondary mania can be resulted from frontal
lobe lesion• Multiple case studies reported that most mania
symptoms occurs in RIGHT frontal lobe lesion.• Can occur immediately or later in life after injury.
PATHOPHYSIOLOGY• No clear mechanism
– Postulation: • 1. Brain asymmetry causing dis-inhibition
syndrome.• 2. Limbic system damage.
» Psychosomatics 48:433-435, September-October 2007 doi: 10.1176/appi.psy.48.5.433
AVM: SHORT OVERVIEW• Patient has a right extensive fronto-
temporo-occipital AVM• Not curable in this case• Causing the mood symptoms and
epilepsy
AVM: DEFINITION–Lesions of the cerebral vasculature–Blood flows from arterial to venous
system–Without capillary system–Shunt
AVM: CLINICAL PRESENTATION• Clinical presentations:
– Haemorrhage(41-79%)– Seizure(11-33%)– Heache
• Prognosis– Average rate of haemorrhage – 2.8-4.6%
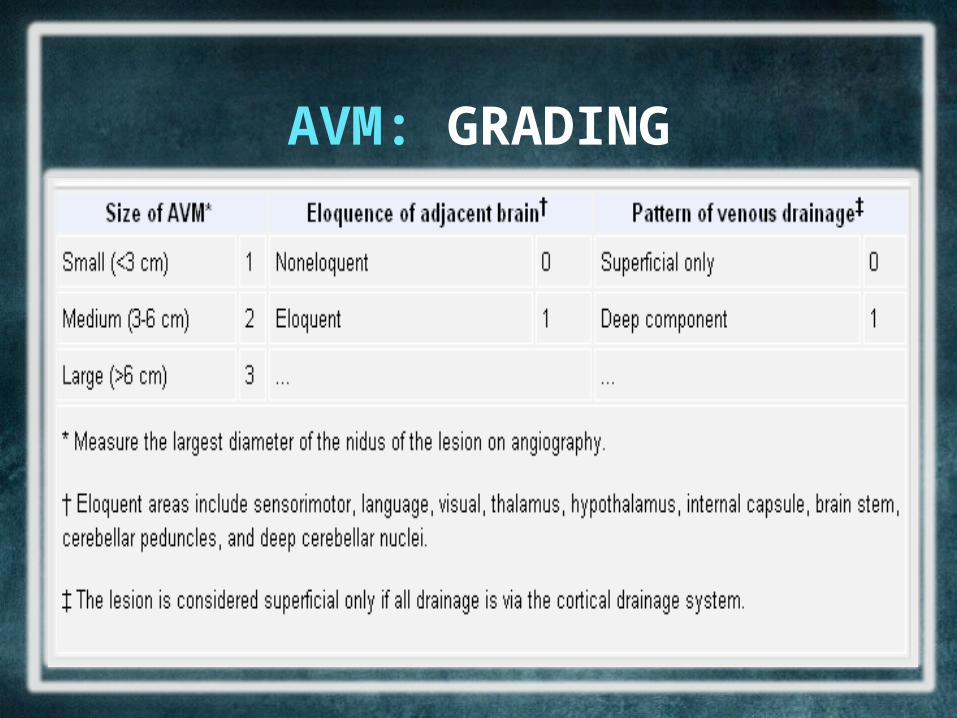
AVM: GRADING
AVM: TREATMENT
– Surgery not a chance– Vascular surgery not a
chance– Radiosurgery only chance
for the patient(do in stages)
DSM-IV criteria for mood disorder resulting from medical or neurologic condition, manic type (secondary
mania)• Elation or irritability • Four of the following:
– inflated self-esteem or grandiosity– decreased need for sleep– pressured speech– flight of ideas– Distractibility– increased goal-directed activity or psychomotor
agitation– excessive involvement in pleasurable activities
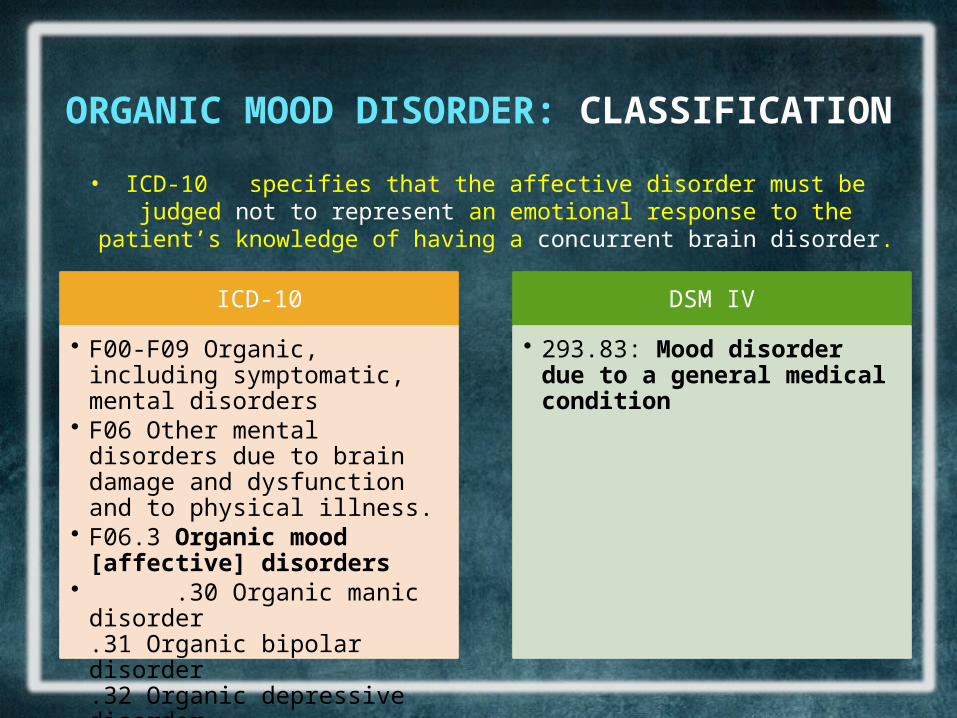
ORGANIC MOOD DISORDER: CLASSIFICATION
• ICD-10 specifies that the affective disorder must be judged not to represent an emotional response to the patient’s knowledge of having a
concurrent brain disorder.
ICD-10
• F00-F09 Organic, including symptomatic, mental disorders
• F06 Other mental disorders due to brain damage and dysfunction and to physical illness.
• F06.3 Organic mood [affective] disorders
• .30 Organic manic disorder.31 Organic bipolar disorder.32 Organic depressive disorder.33 Organic mixed affective disorder
DSM IV
• 293.83: Mood disorder due to a general medical condition
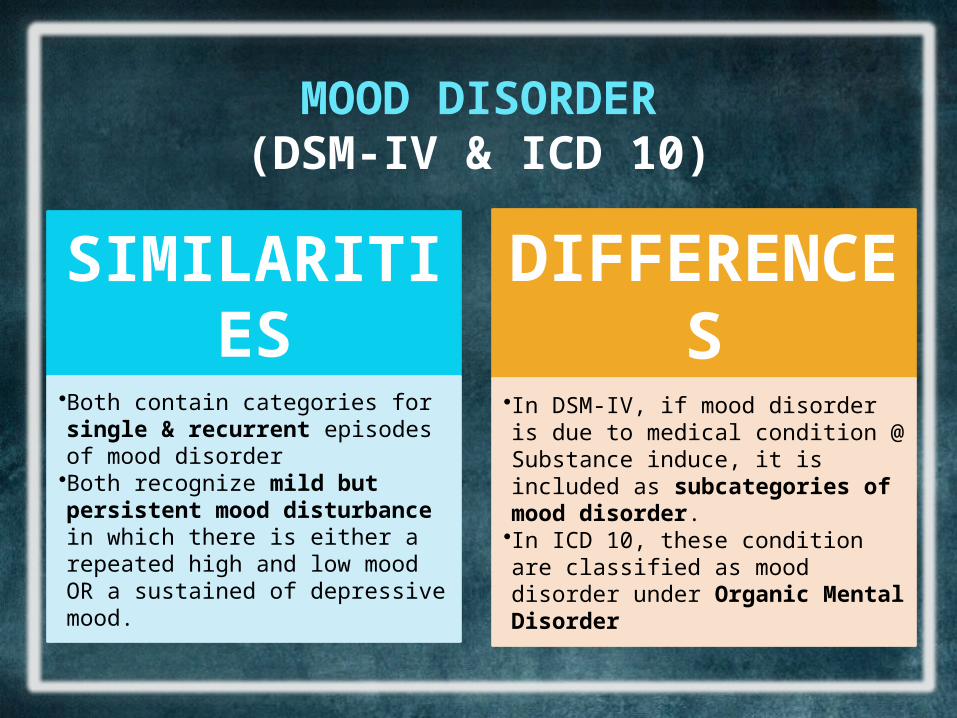
MOOD DISORDER(DSM-IV & ICD 10)
SIMILARITIES•Both contain categories for single & recurrent episodes of mood disorder•Both recognize mild but persistent mood disturbance in which there is either a repeated high and low mood OR a sustained of depressive mood.
DIFFERENCES•In DSM-IV, if mood disorder is due to medical condition @ Substance induce, it is included as subcategories of mood disorder.•In ICD 10, these condition are classified as mood disorder under Organic Mental Disorder
ORGANIC MOOD DISORDER: EPIDEMIOLOGY
• Depression in the medically ill appears to be equally prevalent by sex, or possibly slightly
higher in men (Caine and Lyness, 2000).
• Patients with secondary mania are more likely to have negative family and personal
histories of mood disorder (Evans et al., 1995)
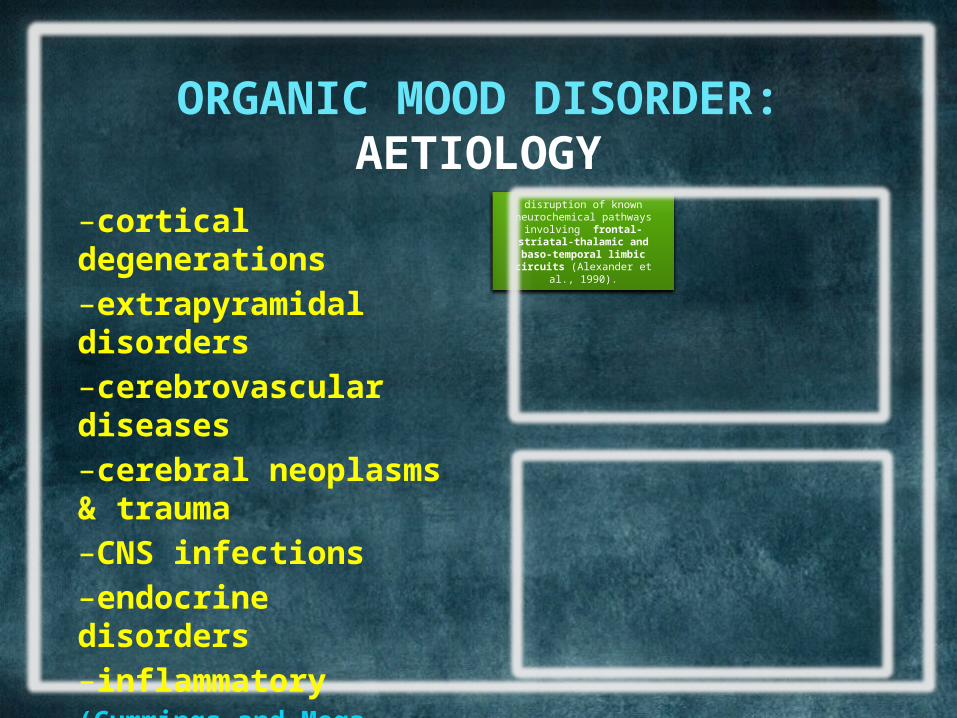
ORGANIC MOOD DISORDER: AETIOLOGY
–cortical degenerations–extrapyramidal disorders–cerebrovascular diseases–cerebral neoplasms & trauma–CNS infections –endocrine disorders–inflammatory (Cummings and Mega, 2003).
Lesion-deficit and functional imaging frontal and temporal cortices and striatum
(Mayberg et al., 2002).
disruption of known neurochemical pathways involving frontal-striatal-
thalamic and baso-temporal limbic circuits (Alexander et al.,
1990).
ORGANIC MOOD DISORDER: MANAGEMENT
• Poststroke Depression Nortriptyline and trazodone. (Lipsey et al., 1984; Reding et al., 1986).
• Traumatic Brain Injury Depression Desipramine and sertraline
(Wroblewski et al., 1996; Fann et al., 2000).
• Manic Lithium (Evans et al., 1995).
• Secondary Mania Clonidine, valproate, carbamazepine and antipsychotics
(Bakchine et al., 1989; Starkstein et al., 1991)