other common causes of painful hindfoot - o'mara for ... · ballet dancers & soccer...
TRANSCRIPT

1
Other Common Causes of Painful HindfootKate O’Mara, DO
April 21, 2015
Financial DisclosuresNothing to disclose.
Objectives
Explore differential diagnosis for hindfoot pain Consider etiologies beyond ligament/tendon injury
Recognize imaging findings typical of impingement syndromes
Heel pain
Other hindfoot pain
Painful Hindfoot
Impingement Syndromes Anterior Anterolateral
Anteromedial Posteromedial
Posterior Talocalcaneal & calcaneofibular
Heel Pain Plantar fasciitis Plantar fibromatosis
Bursitis Haglund deformity/syndrome
Calcaneal stress fracture
Os trigonum Syndrome
Osteochondral Lesions Tarsal Coalition Sinus Tarsi Syndrome Tarsal Tunnel Syndrome Baxter’s neuropathy Synovial Disorders Multifocal bone marrow edema
Ankle Impingement Syndromes
Pathologic conditions resulting in chronic, painful restriction to movement
Secondary to soft-tissue or osseous abnormalities
Typically related to an ankle sprain
Classified according to its anatomic relationship to the tibiotalar joint
Ankle Impingement Syndromes
Anterolateral
Anterior
Anteromedial
Posteromedial
Posterior
Talocalcaneal & Calcaneofibular
Lateral hindfoot

2
Anterior Impingement Syndrome Ballet dancers & soccer players
Progressive symptoms due to impingement of hypertrophied soft tissue & bony spurs Anterior tibiotalar spurs within joint capsule
Repeated dorsiflexion (ballet - plié)
Direct trauma from ball impact (soccer – ball strike)
Microfractured trabecular bone, periosteal hemorrhage, anterior chondral margin trauma result in new bone formation
Effusion
Hypertrophied synovium with impingement, irregular capsular thickening
Marrow edema uncommon
Anterior Impingement Syndrome
Lateral drawing of ankle shows typical location of spur formation (orange) at anterior ankle projecting from anterior tibia and anterior talus. This spur results in decreased angle between tibia and talus, measuring less than 60°.
AJR. 2010;195: 595-604.
Anterior Impingement• 25-year-old man• Opposing tibiotalar
osteophytes • OCD distal tibia &
lateral talar dome
AJR. 2010;195: 595-604.
Anterior Impingement
T1:spurs projecting from dorsal talar neck (arrow) and from anterior distal tibia (arrowhead).
STIR: concavity along dorsal talar neck (arrow) that accommodates tibial osteophyte. Talar neck marrow edema and intraarticular soft-tissue scarring (arrowhead)
Anterolateral Impingement
Typically young athletes with minor trauma (inversion)
Recurrent subclinical instability & microtrauma with hemorrhage, localized reactive synovial hyperplasia, scarring
Eversion & dorsiflexion cause symptoms of impingement
May form reactive hyalinized connective tissue mass: “meniscoid lesion”
May be associated with distal/accessory fascicle of anterior inferior tibiofibular ligament (normal variant)
Treatment: arthroscopic resection of hypertrophic synovium & scar tissue
Anterolateral Impingement
• Typical location ofsynovitis
• Anterolateral recessbetween anteriortibiofibular (arrows) and anterior talofibularligaments (arrowheads)
AJR. 2010;195: 595-604.
3
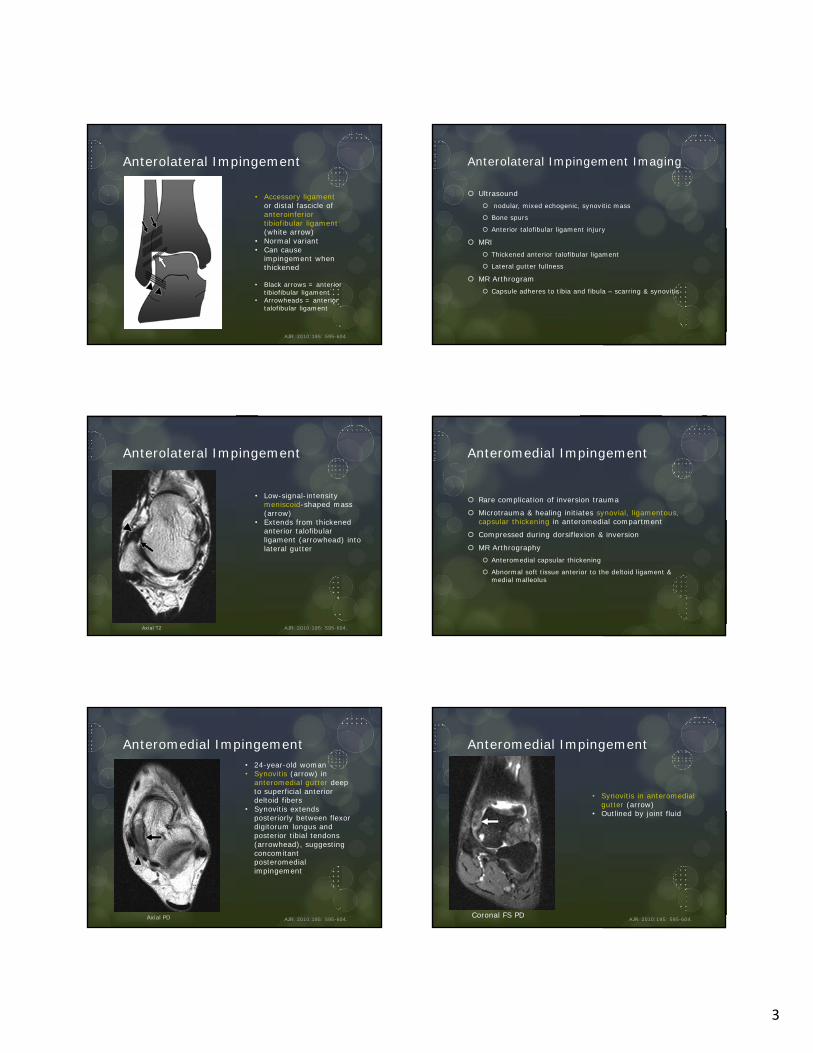
Anterolateral Impingement
• Accessory ligament or distal fascicle of anteroinferior tibiofibular ligament(white arrow)
• Normal variant• Can cause
impingement whenthickened
• Black arrows = anteriortibiofibular ligament
• Arrowheads = anterior talofibular ligament
AJR. 2010;195: 595-604.
Anterolateral Impingement Imaging
Ultrasound nodular, mixed echogenic, synovitic mass
Bone spurs
Anterior talofibular ligament injury
MRI Thickened anterior talofibular ligament
Lateral gutter fullness
MR Arthrogram Capsule adheres to tibia and fibula – scarring & synovitis
Anterolateral Impingement
• Low-signal-intensity meniscoid-shaped mass(arrow)
• Extends from thickenedanterior talofibularligament (arrowhead) intolateral gutter
AJR. 2010;195: 595-604.Axial T2
Anteromedial Impingement
Rare complication of inversion trauma
Microtrauma & healing initiates synovial, ligamentous, capsular thickening in anteromedial compartment
Compressed during dorsiflexion & inversion
MR Arthrography Anteromedial capsular thickening
Abnormal soft tissue anterior to the deltoid ligament & medial malleolus
Anteromedial Impingement• 24-year-old woman• Synovitis (arrow) in
anteromedial gutter deep to superficial anterior deltoid fibers
• Synovitis extendsposteriorly between flexordigitorum longus andposterior tibial tendons(arrowhead), suggestingconcomitant posteromedial impingement
AJR. 2010;195: 595-604.Axial PD
Anteromedial Impingement
• Synovitis in anteromedialgutter (arrow)
• Outlined by joint fluid
AJR. 2010;195: 595-604.Coronal FS PD

4
Anteromedial Impingement
• 51-year-old man• Remote ankle sprain• Thickening and
ossification of deep (arrows) and superficial (arrowhead) deltoidligament fibers
AJR. 2010;195: 595-604.Coronal FS PD
Posteromedial Impingement
Following severe inversion injury with ATF ligament injury
Allows compression of posteromedial structures between medial wall of talus & medial malleolus Joint capsule
Posterior deltoid ligament
Posteromedial flexor tendons
Forms thickened, disorganized fibrous tissue
Accessory medial talar tubercle may contribute
Treatment Injection: steroid & local anesthetic
Surgical resection
Posteromedial Impingement
MRI Loss of normal fat striations in posterior deltoid ligament
Posteromedial synovitis
Thickening & abnormal signal posteromedial joint capsule May displace/surround adjacent tendons
US Thickening posteromedial capsule
Posteromedial synovial hypertrophy
Displacement/entrapment of adjacent tendons
Posteromedial Impingement• Marked scarring and loss of
normal architecture of deep deltoid ligament (arrows)
• Medial displacement ofposterior tibial tendon (arrowhead)
• Obliteration of fat planesbetween posterior tibial tendon and scarred ligament
• M = medial malleolus.
AJR. 2010;195: 595-604.Axial T2
Posterior impingement
Posterior ankle pain with plantar flexion Compression of talus & soft tissues between posterior tibia
& calcaneus
AKA os trigonum syndrome, talar compression syndrome, posterior block
Os-trigonum most common cause
Posterior impingement
Posterior talar process is bifid Smaller medial process
Groove for flexor hallucis longus tendon
Larger lateral process If elongated: Steida process
Failure of fusion (14-25%): os trigonum (3 articular surfaces)
JAAOS, Oct 2005,vol. 13 no. 6 365-371

5
Posterior impingement
Soft tissue impingement Posterior capsule
Posterior talofibular, posterior intermalleolar & tibiofibular ligaments Posterior intermalleolar ligament
– anatomic variant – extendsobliquely from posterior medial malleolus to posterior margin of fibular malleolar fossa
Radsource.us
Chronic repetitive stress in plantar flexion
Ballet dancers: en pointe
Soccer players: ball strike
Posterior impingement Imaging Lateral x-ray (plantar flexion)
impingement of os trigonum/lateral tubercle between calcaneus & posterior tibia
US Nodular, hypoechoic thickening of posterolateral joint
capsule
MRI Posterolateral capsule thickening & synovitis
Bone marrow edema
Os trigonum/lateral tubercle fragmentation
Fluid along flexor hallucis tendon sheath
Posterior Impingement
• 27-year-old woman• Prominent Stieda process
(black arrow)• Posterior osteophyte (white
arrow) along distal tibia
AJR. 2010;195: 595-604.
Posterior Impingement
Sagittal T1: low-signal-intensity os trigonum (arrow) and adjacent low-signal soft-tissue abnormality (arrowheads)
27-year-old female ballet dancer with posterior impingement and os trigonum.
STIR: opposing talar and os trigonum marrow edema (arrows), adjacent soft-tissue edema, and joint effusion (star)
AJR. 2010;195: 595-604.
Posterior Impingement
Low-signal-intensity soft-tissue scar posterior to talus (arrow)
AJR. 2010;195: 595-604.
T1 STIR
6
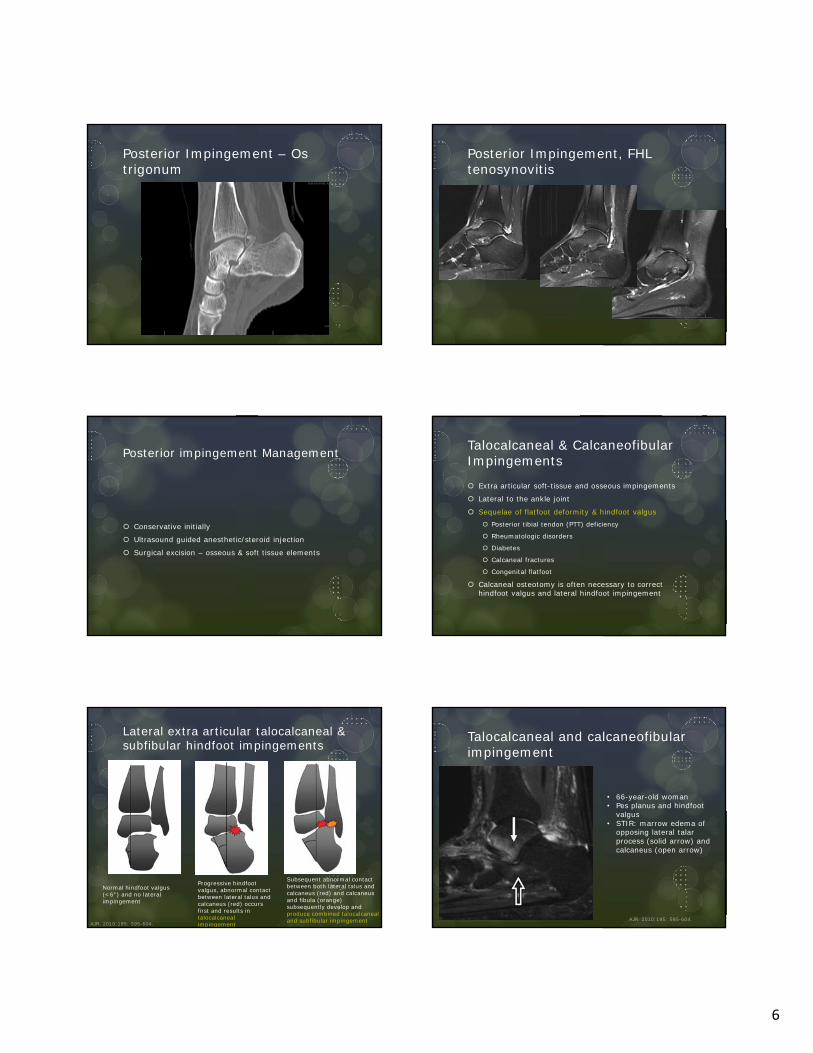
Posterior Impingement – Os trigonum
Posterior Impingement, FHL tenosynovitis
Posterior impingement Management
Conservative initially
Ultrasound guided anesthetic/steroid injection
Surgical excision – osseous & soft tissue elements
Talocalcaneal & Calcaneofibular Impingements
Extra articular soft-tissue and osseous impingements
Lateral to the ankle joint
Sequelae of flatfoot deformity & hindfoot valgus Posterior tibial tendon (PTT) deficiency
Rheumatologic disorders
Diabetes
Calcaneal fractures
Congenital flatfoot
Calcaneal osteotomy is often necessary to correct hindfoot valgus and lateral hindfoot impingement
Lateral extra articular talocalcaneal & subfibular hindfoot impingements
Normal hindfoot valgus (<6°) and no lateral impingement
Progressive hindfoot valgus, abnormal contact between lateral talus and calcaneus (red) occurs first and results in talocalcaneal impingement
Subsequent abnormal contact between both lateral talus and calcaneus (red) and calcaneus and fibula (orange) subsequently develop and produce combined talocalcaneal and subfibular impingementAJR. 2010;195: 595-604.
Talocalcaneal and calcaneofibular impingement
• 66-year-old woman• Pes planus and hindfoot
valgus• STIR: marrow edema of
opposing lateral talarprocess (solid arrow) and calcaneus (open arrow)
AJR. 2010;195: 595-604.
7
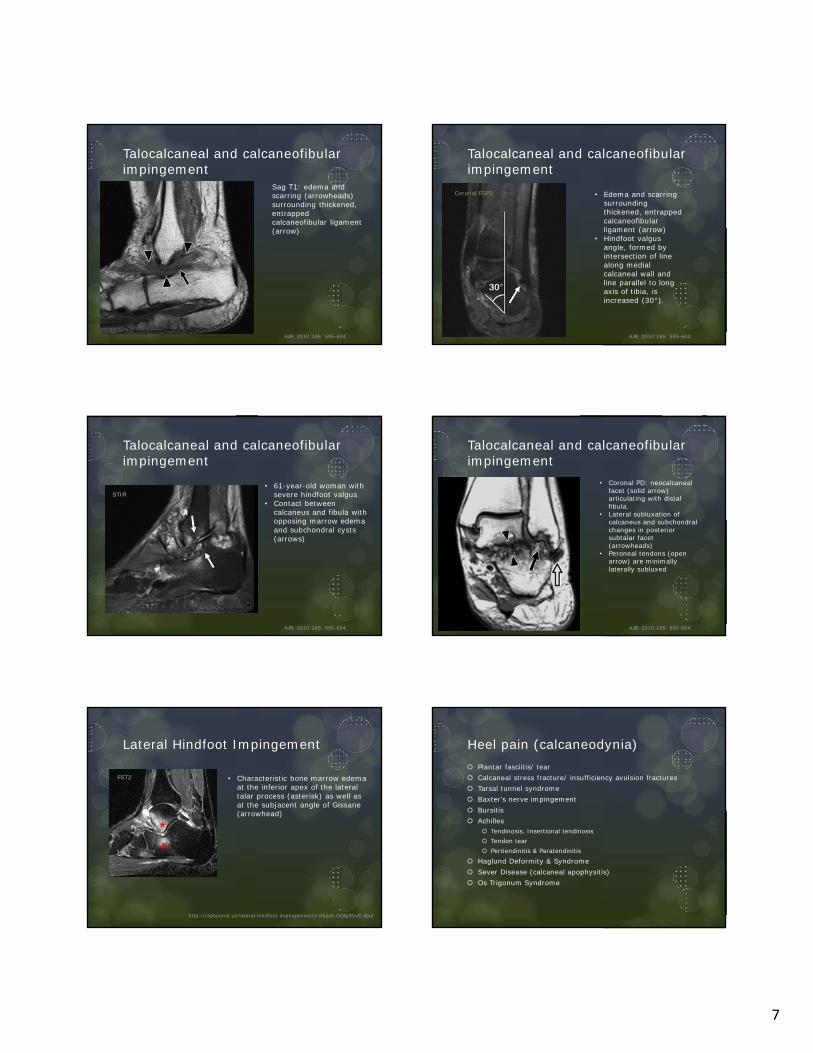
Sag T1: edema and scarring (arrowheads) surrounding thickened, entrapped calcaneofibular ligament (arrow)
Talocalcaneal and calcaneofibular impingement
AJR. 2010;195: 595-604.
• Edema and scarringsurrounding thickened, entrappedcalcaneofibular ligament (arrow)
• Hindfoot valgusangle, formed byintersection of linealong medialcalcaneal wall andline parallel to longaxis of tibia, isincreased (30°).
Talocalcaneal and calcaneofibular impingement
AJR. 2010;195: 595-604.
Coronal FSPD
• 61-year-old woman withsevere hindfoot valgus
• Contact betweencalcaneus and fibula withopposing marrow edemaand subchondral cysts(arrows)
Talocalcaneal and calcaneofibular impingement
AJR. 2010;195: 595-604.
STIR
• Coronal PD: neocalcaneal facet (solid arrow) articulating with distal fibula.
• Lateral subluxation of calcaneus and subchondral changes in posterior subtalar facet (arrowheads)
• Peroneal tendons (open arrow) are minimallylaterally subluxed
Talocalcaneal and calcaneofibular impingement
AJR. 2010;195: 595-604.
Lateral Hindfoot Impingement
• Characteristic bone marrow edemaat the inferior apex of the lateral talar process (asterisk) as well asat the subjacent angle of Gissane(arrowhead)
http://radsource.us/lateral-hindfoot-impingement/#sthash.OQ8j95vE.dpuf
FST2
Heel pain (calcaneodynia) Plantar fasciitis/ tear Calcaneal stress fracture/ insufficiency avulsion fractures Tarsal tunnel syndrome Baxter’s nerve impingement Bursitis Achilles
Tendinosis, Insertional tendinosis Tendon tear Peritendinitis & Paratendinitis
Haglund Deformity & Syndrome Sever Disease (calcaneal apophysitis) Os Trigonum Syndrome

8
Plantar fasciitis
Most common cause of inferior heel pain Inflammation usually related to repetitive trauma
Microtears near its origin Runners, obese patients
Inflammatory arthropathies (enthesopathy) Reactive arthritis, ankylosing spondylitis, psoriatic arthritis
MRI Intermediate signal (should be low) – intrafascial edema Thickening 6-10mm (normally 2-4mm) – fusiform Marrow edema calcaneal tuberosity Surrounding hyperintense T2 (edema)
Heel spur on X-ray not diagnostic
Plantar fasciitis
AJR 2013;200: 845-855
Plantar Fasciitis Plantar Fascia Tear
Sports related (running, jumping)
Chronic plantar fasciitis after corticosteroid injections
Usually proximal, near calcaneal attachment Associated with tear of flexor digitorum brevis muscle
MRI Partial/complete disruption, edema & hemorrhage
Perifascial fluid
Plantar Fascia Tear Plantar Fascia Tear
9
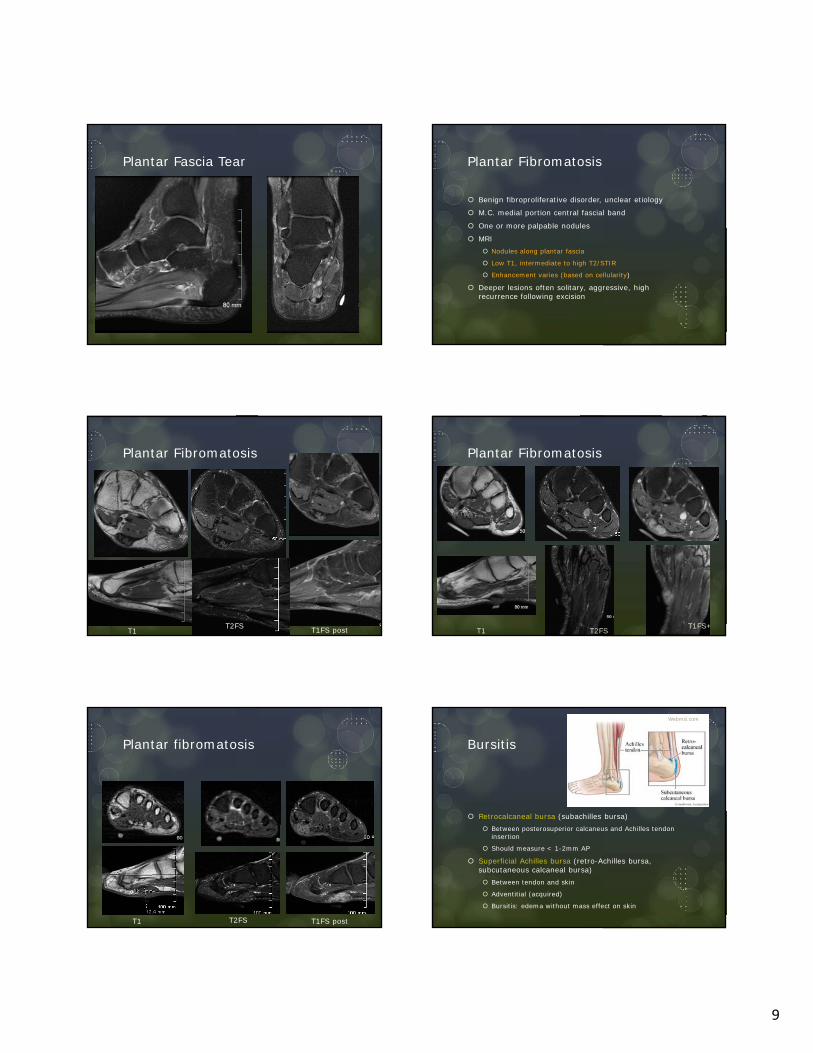
Plantar Fascia Tear Plantar Fibromatosis
Benign fibroproliferative disorder, unclear etiology
M.C. medial portion central fascial band
One or more palpable nodules
MRI Nodules along plantar fascia
Low T1, intermediate to high T2/STIR
Enhancement varies (based on cellularity)
Deeper lesions often solitary, aggressive, high recurrence following excision
Plantar Fibromatosis
T1T2FS T1FS post
Plantar Fibromatosis
T1 T2FS T1FS+
Plantar fibromatosis
T1 T2FS T1FS post
Bursitis
Retrocalcaneal bursa (subachilles bursa) Between posterosuperior calcaneus and Achilles tendon
insertion
Should measure < 1-2mm AP
Superficial Achilles bursa (retro-Achilles bursa, subcutaneous calcaneal bursa) Between tendon and skin
Adventitial (acquired)
Bursitis: edema without mass effect on skin
Webmd.com

10
Retrocalcaneal bursitis
With or without Achilles tendinosis
Repetitive trauma (runners)
Conservative treatment, sometimes corticosteroids
X-ray: obliteration of normal retrocalcaneal fat pad
MRI: enlarged bursa >7mm long, 11mm trans, 1mm AP considered abnormal
Retrocalcaneal bursitis
Radiology blogspot
Haglund Deformity & Syndrome
Deformity: prominent bony projection of calcaneus Superior, posterior aspect of calcaneal tuberosity
Associated with wearing low-back shoes
Syndrome: mechanically induced inflammation Inflammation of superficial bursa
Achilles tendinosis
Retrocalcaneal bursitis
Bony prominence
Haglund Deformity - XR
Enlarged calcaneal tuberosity Draw parallel pitch lines
along superior & inferior calcaneus
Calcaneal tuberosity enlarged if extends above superior pitch line
Syndrome: loss of radiolucent retrocalcaneal recess (indicates bursitis)
AJR. 2013;200: 845-855.
Radiopaedia
Haglund Syndrome
Bony prominence (T1)
Excessive fluid retrocalcaneal bursa
Fluid in retro-Achilles bursa
Bone marrow edema in calcaneal tuberosity
Achilles insertional tendinosis
AJR. 2013;200: 845-855.
Calcaneal stress fracture 2nd most common site of fatigue stress fracture (after
metatarsals) Insufficiency fractures (RA, neurologic disorders, DM) Repetitive trauma (jumping) Posterosuperior or posterior calcaneus
Oriented vertically (perpendicular to long axis of calcaneus)
X-ray: variable sclerotic band MRI:
band-like low T1, high T2 in intramedullary space, extends to cortex
Extensive surrounding edema, hemorrhage
Periosteal callus – hypointense line parallel to cortex

11
Calcaneal stress fracture
• 24 year old militaryrecruit
• Fracture line (arrow) and intense surrounding marrow edema
• Associated retrocalcaneal bursitis(arrowhead)
radsource.us/plantar-fasciitis/#sthash.1gxQs12n.dpuf
T2 fat sat
Calcaneal Stress Fracture
• 43-year-old woman
• Vertical fracture line outlined by bone marrow edema
American Journal of Roentgenology. 2011;197: W720-W729.
STIR
Sever Disease (calcaneal apophysitis)
Skeletally immature
Traction: at site of Achilles tendon insertion
X-ray nonspecific Increased density, fragmentation of apophysis (also seen in
healthy kids)
MRI Edema in calcaneal apophysis, may extend to calcaneal
tuberosity
Sever Disease (calcaneal apophysitis)
Orthocarolina.comMypacs.net/case 154930
Calcaneal Insufficiency Avulsion (CIA) Fractures
Avulsion fracture involving posterior 1/3 of calcaneus
Same plane as fatigue type calcaneal fracture
No significant force
Displaced 10-30 mm, often rotated
Mean time from diagnosis of diabetes mellitus to CIA fracture: 20 years

12
Calcaneal tuberosity avulsion fracture. Weerakkody et al. Radiopaedia
Calcaneal Insufficiency Avulsion (CIA) Fractures
Calcaneal Insufficiency Avulsion (CIA) Fractures Osteochondral Lesions (OCL)
Post-traumatic injury of articular (hyaline) cartilage and underlying subchondral bone
Common locations (in order of frequency) Femoral condyles
Capitellum of elbow
Talar dome
Patella
Talar dome OCL Medial more common than lateral
Deeper
Greater surface area
Radiopaedia
Small OCD talar dome OCD talus

13
OCD Talus OCD Talus
Stable v Unstable OCL
Unstable Hyperintense T2 signal (equal to joint fluid) between
detached osteochondral fragment and parent bone
Cystic change at donor site
Extensive bone marrow edema
Collapse of articular surface
Arthrogram may help delineate, if necessary
Treatment
Stable Nonweightbearing cast immobilization
Progressive weightbearing over 3-4 months
Unstable Surgery: remove subchondral fragment & Debris
Microfracture of remnant bone to promote growth of new fibrocartilage
Internal fixation (fragment > 7.5mm)
Osteochondral allografts or autografts
OATS (osteochondral autograft transfer system)
Heal with type II collagen instead of fibrocartilage
OCL Differential Diagnosis
AVN – Avascular Necrosis Significant bone marrow edema
Spares articular surface
End stage OCL and AVN can result in collapse of articular surface
OA – Osteoarthritis Changes involve both sides of joint
Eburnation
Osteophytes
OCL may result in OA
AVN Talar dome
Radiopaedia.

14
Osteoid Osteoma Talus Tarsal Coalition
Congenital connection between 2 or more bones Bony, cartilaginous, or fibrous
Prevent normal joint motion
Subtalar coalition
Calcaneonavicular coalition
Coalitions cause abnormal bone overgrowth Osseous coalition: continuous bony bar
Nonosseous coalition: bony overgrowth with irregular cleft
Tarsal Coalition –Radiographic features Subtalar coalition (best seen on Harris view)
C-sign (lateral) – continuity of inferomedial talus and ST Also seen in flat foot deformity
Dysmorphic Sustentaculum Tali – inferior border rounded, enlarged
Talar beak – articular surface flares superiorly to accommodate increased motion at talonavicular joint Talar osteophyte – proximal to joint and arcs over joint Talar ridge – normal attachment ankle joint capsule, proximal
Absent Middle Facet sign
Calcaneonavicular coalition Anteater sign (lateral) – Elongated anterior process of calcaneus Elongated Navicular sign (AP) – Reverse anteater – elongated
lateral navicular
C-sign, talar beak
Subtalar coalition: CT/MRI
Osseous: bony continuity across middle subtalar facet
Nonosseous: fibrous or cartilaginous coalition Narrow, obliquely oriented, undulating contour
Subchondral cysts
Bone marrow edema
Enlarged ST, rounded contour inferiorly
Peroneal or flexor tendon tenosynovitis
Subtalar (talocalcaneal) coalition

15
Talocalcaneal coalition Talocalcaneal coalition (fibrocartilagenous)
Calcaneonavicular Coalition –CT/MRI
Sagittal: elongated anterior calcaneal process with blunted tip
Axial: Abnormal shape anterior calcaneus and lateral navicular
Subchondral cysts & bone marrow edema anterior calcaneus
Calcaneonavicular Coalition
• T1: elongated & broadened anterior process of calcaneus (arrowhead)
• Irregular articulation(arrow) with the navicular: "anteater's nose".
• STIR: bony hypertrophy& subarticular marrow edema (asterisks) at the abnormalcalcaneonavicular articulation
T1: slightly widened mediolateral dimension of the navicular (black arrow)• tapers laterally and
articulates (white arrow) with the enlarged anterior process of the calcaneus (arrowhead)
http://radsource.us/tarsal-coalition
Calcaneonavicular coalition Calcaneonavicular coalition
16
Sinus Tarsi Syndrome
Lateral pain, perceived hindfoot instability
Subtalar region, anterior to posterior subtalar joint
Normally fat-filled
Talocalcaneal (Interosseous) Ligament Cervical ligament: anterior
Best seen on Coronal: vertical course
Interosseous talocalcaneal ligament: posterior & medial Coronal: oblique orientation inferior talus to superior calcaneus
Inferior extensor retinaculum (superficial)
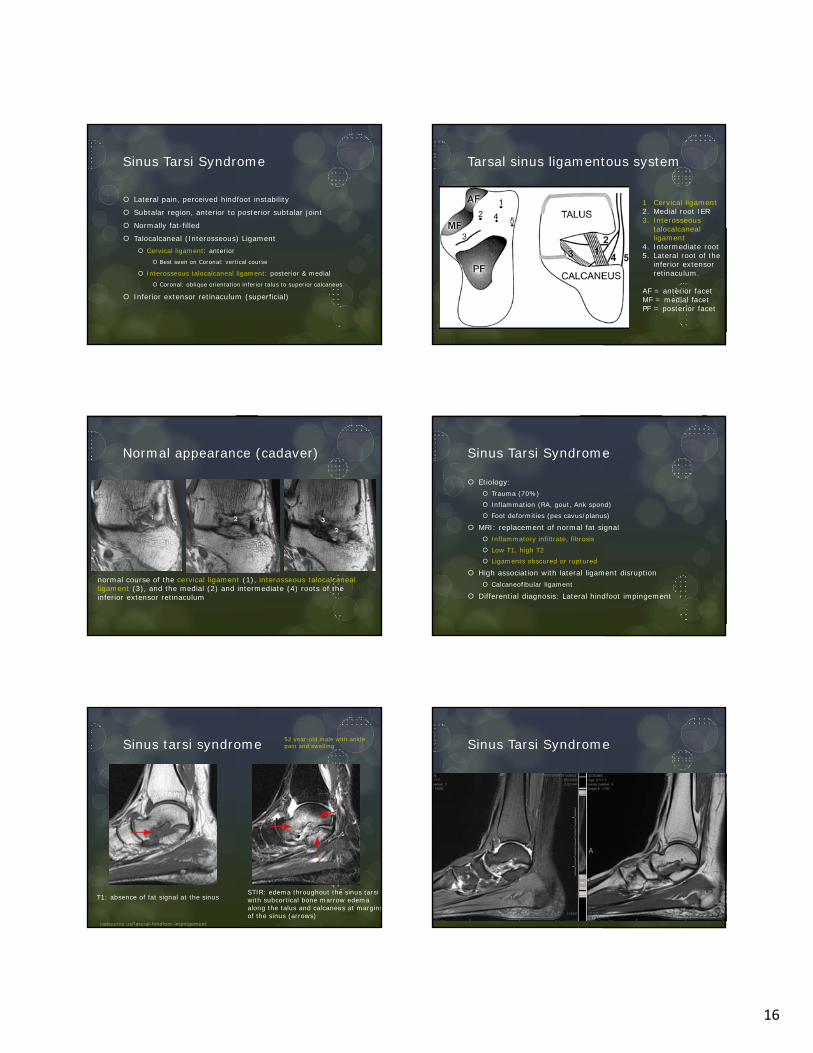
Tarsal sinus ligamentous system
1. Cervical ligament2. Medial root IER3. Interosseous
talocalcaneal ligament
4. Intermediate root5. Lateral root of the
inferior extensorretinaculum.
AF = anterior facetMF = medial facetPF = posterior facet
Normal appearance (cadaver)
normal course of the cervical ligament (1), interosseous talocalcaneal ligament (3), and the medial (2) and intermediate (4) roots of the inferior extensor retinaculum
Sinus Tarsi Syndrome
Etiology: Trauma (70%)
Inflammation (RA, gout, Ank spond)
Foot deformities (pes cavus/planus)
MRI: replacement of normal fat signal Inflammatory infiltrate, fibrosis
Low T1, high T2
Ligaments obscured or ruptured
High association with lateral ligament disruption Calcaneofibular ligament
Differential diagnosis: Lateral hindfoot impingement
Sinus tarsi syndrome
T1: absence of fat signal at the sinus
radsource.us/lateral-hindfoot-impingement
52 year-old male with ankle pain and swelling
STIR: edema throughout the sinus tarsi with subcortical bone marrow edema along the talus and calcaneus at marginsof the sinus (arrows)
Sinus Tarsi Syndrome
17
Tarsal tunnel syndrome
Entrapment neuropathy of posterior tibial nerve or of its branches within the tarsal tunnel Usually unilateral
Clinical presentation Pain & paresthesia in the toes, sole, or heel
Physical exam: Tinel sign (distal paresthesias produced by percussion over the affected portion of nerve)
Electromyography and nerve conduction studies are useful in confirming the diagnosis
Tarsal tunnel anatomy Fibro-osseous canal , medial ankle
Boundaries
Roof: flexor retinaculum
Floor - medial surfaces of talus & calcaneus
Contents (from anterior to posterior)
Tibialis posterior tendon
Flexor digitorum longus tendon
Neurovascular bundle
Posterior tibial artery & vein
Posterior tibial nerve
Flexor hallucis longus tendon
A mnemonic to remember the order is: Tom, Dick and Very Nervous Harry
Divided by fibrous septae joining the retinaculum to calcaneus, forming four separate compartments - one for each of the tendons and one for the neurovascular bundle
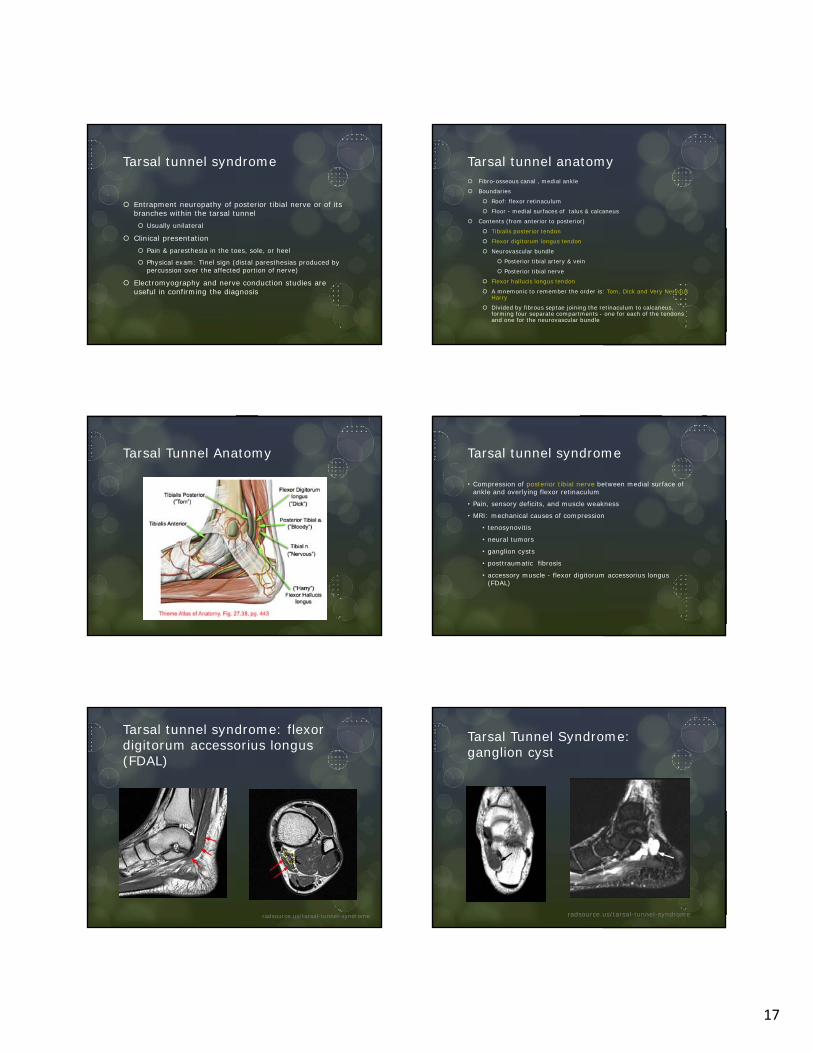
Tarsal Tunnel Anatomy Tarsal tunnel syndrome
• Compression of posterior tibial nerve between medial surface of ankle and overlying flexor retinaculum
• Pain, sensory deficits, and muscle weakness
• MRI: mechanical causes of compression
• tenosynovitis
• neural tumors
• ganglion cysts
• posttraumatic fibrosis
• accessory muscle - flexor digitorum accessorius longus (FDAL)
Tarsal tunnel syndrome: flexor digitorum accessorius longus (FDAL)
radsource.us/tarsal-tunnel-syndrome
Tarsal Tunnel Syndrome: ganglion cyst
radsource.us/tarsal-tunnel-syndrome
18
Tarsal tunnel syndrome: Schwannoma
radsource.us/tarsal-tunnel-syndrome
Tarsal tunnel syndrome: Varicosities
radsource.us/tarsal-tunnel-syndrome
Baxter's neuropathy
Nerve entrapment syndrome : compression of the inferior calcaneal nerve 1st branch of the lateral plantar nerve - courses through
tarsal tunnel
Clinical presentation heel pain (plantar medial foot and anterior/medial
calcaneus)
paresthesia with motor weakness of the abductor digiti minimi muscle
no associated cutaneous sensory deficit
Baxter’s neuropathy - MRI
Acute phase of muscle denervation Decreased T1, increased T2FS signal intensity
Increased extracellular water content
Decreased muscle fiber volumes
Chronic phase of muscle denervation Amyotrophy or fatty degeneration
Abductor digiti minimi muscle
Less commonly: flexor digitorum brevis & quadratus plantae muscles
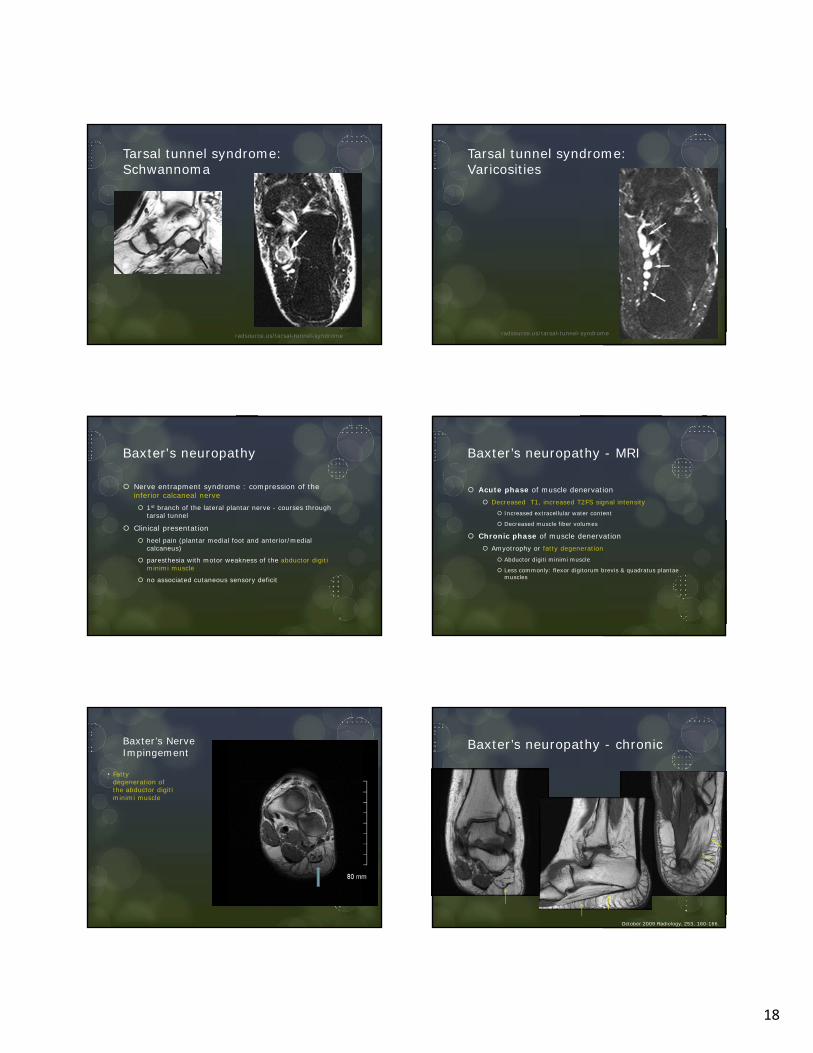
Baxter’s Nerve Impingement
• Fattydegeneration of the abductor digiti minimi muscle
Baxter’s neuropathy - chronic
October 2009 Radiology, 253, 160-166.

19
Synovial Disorders
PVNS – Pigmented Villonodular Synovitis
Synovial chondromatosis
Synovitis
PVNS
Proliferative disorder of synovium
Joints, tendon sheaths, bursae
Hemorrhage results in hemosiderin deposition
MRI variable: intermediate/low T1, low and high T2, blooming artifact GRE
Diffuse form involves joints (knee > hip > ankle)
Focal form: tendon sheath (GCTTS giant cell tumor of tendon sheath)
PVNS Ankle FHL Giant Cell Tumor Tendon Sheath
FHL GCTTS post Gad Synovial chondromatosis
Synovial metaplasia
Benign, monoarticular
Lining cells produce cartilage nodules
May or may not ossify
Treatment: synovectomy
20
Synovial chondromatosis
T1 T2FS
Mass-like signal distending ankle joint
MyPACS.net: Radiology Teaching Files > Case 8494317
Synovial chondromatosis
Multifocal Bone Marrow Edema
High turnover - children <15 years Multiple foci of high T2 signal in several ankle/foot bones
Asymptomatic, self limiting
Altered gait Strenuous exercise Bone impaction/bone contusions
Trabecular microfractures, edema, hemorrhage
Immobilization – patchy, subcortical, subchondral CRPS – Complex Regional Pain Syndrome
Skin edema & thickening
Patchy, subcortical edema pattern
High Turnover
• 12-year-old girl
• Sagittal STIR image shows multiple foci ofincreased bone marrow signal
• Associated withincreased sports-related activity
AJR. 2011;197: W720-W729.
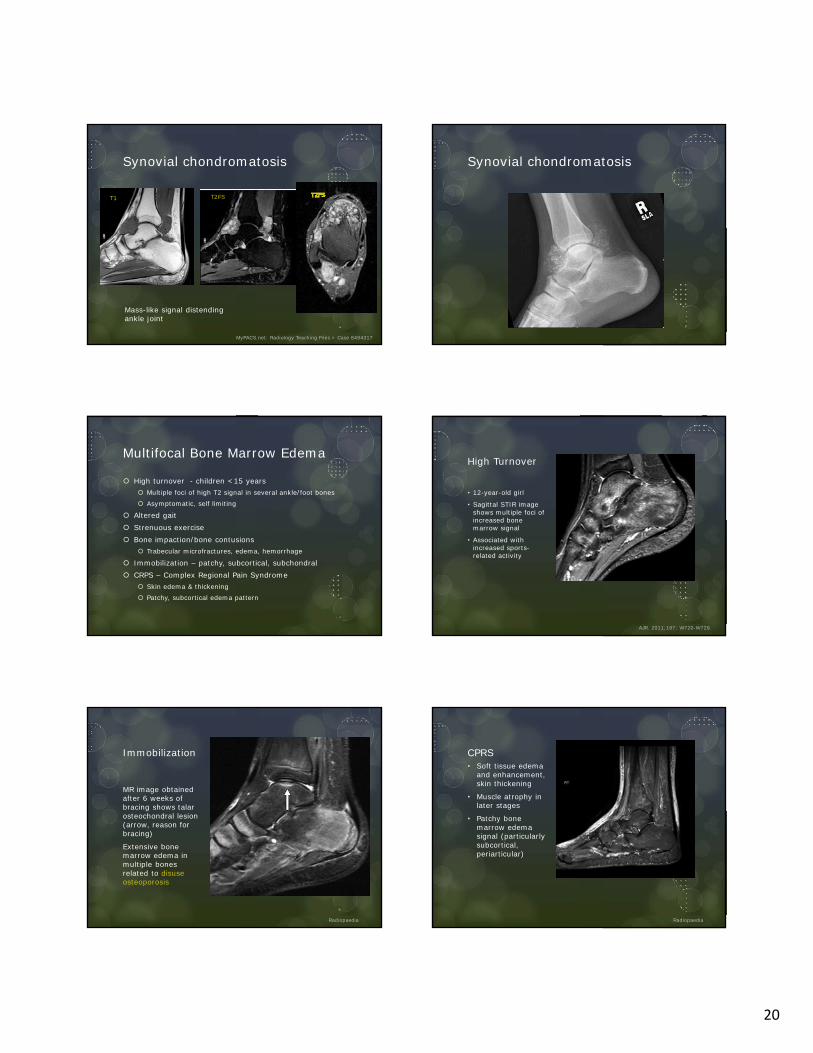
Immobilization
MR image obtained after 6 weeks of bracing shows talar osteochondral lesion (arrow, reason for bracing)
Extensive bone marrow edema in multiple bones related to disuse osteoporosis
Radiopaedia
CPRS• Soft tissue edema
and enhancement, skin thickening
• Muscle atrophy inlater stages
• Patchy bonemarrow edemasignal (particularlysubcortical, periarticular)
Radiopaedia

21
Calcaneal Vascular Grooves
• At critical angle of Gissane
• Common • May be quite extensive
American Journal of Roentgenology. 2011;197: W720-W729.
STIR
Painful Hindfoot
Impingement Syndromes Anterior Anterolateral
Anteromedial Posteromedial
Posterior Talocalcaneal & calcaneofibular
Heel Pain Plantar fasciitis Plantar fibromatosis
Bursitis Haglund deformity/syndrome
Calcaneal stress fracture
Os trigonum Syndrome
Osteochondral Lesions Tarsal Coalition Sinus Tarsi Syndrome Tarsal Tunnel Syndrome Baxter’s neuropathy Synovial Disorders Multifocal bone marrow edema
Objectives
Explore differential diagnosis for hindfoot pain Consider etiologies beyond ligament/tendon injury
Recognize imaging findings typical of impingement syndromes
Heel pain
Other hindfoot pain
References
Current Concepts in Imaging Diabetic Pedal Osteomyelitis. Donovan. Radiol Clin N Am 46 (2008) 1105-1124.
Osteochondral Lesions About the Ankle. Naran. Radiol Clin N Am 46 (2008) 995-1002
Ankle Impingement Syndromes. Hopper. Radiol Clin N Am 46(2008) 957-971
Imaging of Tarsal Coalition. Crim. Radiol Clin N Am 46(2008) 1017-1026
Imaging of Soft Tissue Lesions of the Foot & Ankle. Bancroft. Radiol Clin N Am 46(2008) 1093-1104
Current Concepts in Imaging Diabetic Pedal Osteomyelitis. Donovan. Radiol Clin N Am 46(2008) 1105-1124
References
Sinus Tarsi Syndrome. MRI Clin No Amer. Vol 2, Num 1 (1994) 59-66.
Tarsal Tunnel Syndrome. MRI Clin No Amer. Vol 2, Num 1 (1994) 67-78
MRI of Plantar Fasciitis & Other Causes of Heel Pain. MRI Clin No Amer. Vol 2, Num 1 (1994) 97-108
Tumors of the Ankle & Foot. MRI Clin No Amer. Vol 2, Num 1 (1994) 139-154
Sonography & MRI of Selected Benign Masses in the Foot & Ankle. Pham. AJR 2003;180:99-107
MRI of Ankle and Lateral Hindfoot Impingement Syndromes. AJR 2010; 195:595-604
Bone Marrow Edema Patterns in Ankle & Hindfoot: Distinguishing MRI Features. Rios. AJR 2011;197:W720-W729

22
References
Calcaneal insufficiency avulsion fractures in patients with diabetes mellitus. Radiology 1991 Sep;180(3):725-9.
MRI of Heel Pain. AJR 2013; 200:845-855
MR imaging of the tarsal tunnel and related spaces: normal and abnormal findings with anatomic correlation. AJR. 1990;155: 323-328.
Avascular Necrosis of the Talus: A Pictorial Essay. RSNA. 2005;25:399-410.
Diabetic Foot & Ankle 2012, 3: 18754 -http://dx.doi.org/10.3402/dfa.v3i0.18754
Imaging of the Foot & Ankle. 3rd Ed. Berquist. LWW. 2011.
Diabetes
Pedal osteomyelitis
Charcot joint
Calcaneal insufficiency avulsion fractures
Skin Callus
Develop at pressure points Normal: 1st/5th metatarsal head, heel
Hallux valgus: medial to 1st metatarsal
Rocker-bottom: beneath cuboid
MRI: focal prominence in subcutaneous fat Low T1, low to intermediate T2
May enhance
Adjacent fat normal (helps distinguish from infection)
Adventitial bursa Thin, flat fluid collection
Adjacent to callus
Skin Callus
• Focal hypointense area in subcutaneous fat in the midfoot in both sequences (arrows) • No accompanying soft tissue changes, consistent with callus• Subchondral marrow edema at intertarsal joints is a result of neuroarthropathy
T1 T2FS
Diabetic Foot & Ankle 2012, 3: 18754 - http://dx.doi.org/10.3402/dfa.v3i0.18754
Ulceration & Sinus Tract
Callus breakdown
Focal skin interruption, “heaped up” margins, soft tissue defect
T2 bright, intense peripheral enhancement (granulation tissue)
Sinus tract (“tram track” enhancement) leads to bony prominence
Plantar ulcer with cuboid osteomyelitis
Radiology Assistant/Diabetic Foot MRI

23
Sinus tract – no osteo
Radiology Assistant/Diabetic Foot MRI
Soft tissue swelling, cellulitis, abscess
Edema & cellulitis: fat reticulation with intermediate T1 & high T2 signal Cellulitis enhances, edema does not
Phlegmon: ill-defined low T1, intermediate to high T2 (not as bright as fluid) Vague enhancement
Abscess: fluid signal collection Peripheral rim enhancement
Cellulitis, fistula and associated osteomyelitis and septic arthritis
T1 T2FS
T1+G
T1+G
• High T2 signal and significant skin enhancement = cellulitis (arrowheads).• Deep ulcer in the medial portion of the first toe • Fistula (white arrow) traversing the distal phalanx• Abnormal signal of the proximal and distal phalanges due to osteomyelitis & septic arthritis (black arrow)
Diabetic Foot & Ankle 2012, 3: 18754 - http://dx.doi.org/10.3402/dfa.v3i0.18754
Gangrene
Clinical diagnosis – imaging usually unnecessary
Dry – noninfected, devitalized tissue
Wet – superimposed infection
MRI – delineate areas of soft tissue devascularization Nonenhancing area
Sharp demarcation from viable tissue
Reactive hyperemia/enhancement of periphery
Wet gangrene – look for soft tissue gas GRE most sensitive - blooming
Gas gangrene
• Widespread low-signal-intensity foci demonstrating blooming artifact (arrowheads) alongthe dorsum of the foot indicating soft-tissue gas
• Fluid collections (white arrows), with peripheral enhancement (black arrows) • Subcutaneous tissue, fascial and muscular enhancement (asterisk) are present
T1 T2FS
T1+G T1+G
Diabetic Foot & Ankle 2012, 3: 18754 - http://dx.doi.org/10.3402/dfa.v3i0.18754
Osteomyelitis
Confluent low T1 signal, high T2
High T2 signal without low T1 – reactive edema (may enhance)
Periosteal reaction: circumferential high T2, enhances
Adjacent soft tissue findings (ulcer, sinus tract, cellulitis, abscess, foreign body)

24
Osteomyelitis3 phase bone scan• Increased activity blood
flow, blood pool, delayed phases distal 1st MT
• Consistent withosteomyelitis.
MRI• Confluent hypointense
T1, hyperintense T2 • Indicate presence of
osteomyelitis in the first metatarsal head (white arrows)
Diabetic Foot & Ankle 2012, 3: 18754 - http://dx.doi.org/10.3402/dfa.v3i0.18754
Septic arthritis
Contiguous spread from adjacent soft tissue infection Ankle & subtalar joints in hindfoot related to ulceration at
malleoli or calcaneus
Complex joint effusion, thick synovial enhancement
Soft tissue & subchondral marrow edema, marginal erosions
Confluent low T1 - osteomyelitis
Septic Arthritis
• XR: focal soft tissue swelling, demineralization (arrows) inperiarticular region in distalinterphalangeal joint of the first toe.
• T2FS: ulcer and sinus tract (thinwhite arrow) extending to the joint space.
• T1, T1+G: synovial enhancement(arrowhead) and abnormal intramedullary signal (thick whitearrow) that is extending from thejoint surface, consistent with septicarthritis and accompanyingosteomyelitis
Diabetic Foot & Ankle 2012, 3: 18754 - http://dx.doi.org/10.3402/dfa.v3i0.18754
Septic tenosynovitis
Spread from adjacent ulceration Peroneals – lateral malleolus ulcer
Achilles (peritenonitis) – calcaneal ulcer
Tiny fluid collection around the posterior tibial tendon that demonstrates contrast enhancement (arrows). The tendon is closely related with to the deep ulcer in subcutaneous tissue (arrowheads).
T2T1+G
Septic tenosynovitis
Diabetic Foot & Ankle 2012, 3: 18754 - http://dx.doi.org/10.3402/dfa.v3i0.18754
Neuropathic arthropathy
Acute stage may mimic osteomyelitis MRI: soft tissue edema, fluid collections, effusions, marrow
changes, enhancement
Subacute stage (coalescense): bone resorption
Chronic, consolidation stage: debris, destruction, dislocation, density (x-ray) MR: deformity, osseous fragmentation, joint effusions
25
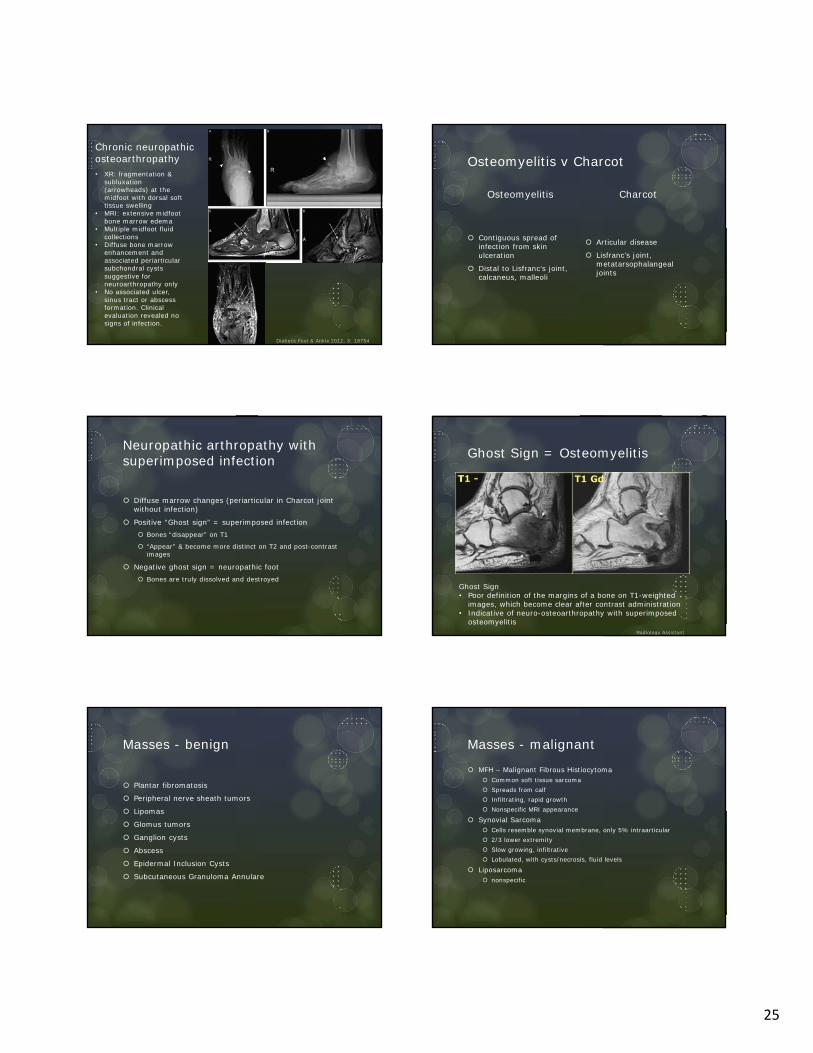
Chronic neuropathic osteoarthropathy• XR: fragmentation &
subluxation (arrowheads) at the midfoot with dorsal soft tissue swelling
• MRI: extensive midfoot bone marrow edema
• Multiple midfoot fluid collections
• Diffuse bone marrow enhancement and associated periarticular subchondral cysts suggestive for neuroarthropathy only
• No associated ulcer,sinus tract or abscess formation. Clinical evaluation revealed no signs of infection.
Diabetic Foot & Ankle 2012, 3: 18754
Osteomyelitis v Charcot
Osteomyelitis
Contiguous spread of infection from skin ulceration
Distal to Lisfranc’s joint, calcaneus, malleoli
Charcot
Articular disease
Lisfranc’s joint, metatarsophalangeal joints
Neuropathic arthropathy with superimposed infection
Diffuse marrow changes (periarticular in Charcot joint without infection)
Positive “Ghost sign” = superimposed infection Bones “disappear” on T1
“Appear” & become more distinct on T2 and post-contrast images
Negative ghost sign = neuropathic foot Bones are truly dissolved and destroyed
Ghost Sign = Osteomyelitis
Ghost Sign• Poor definition of the margins of a bone on T1-weighted
images, which become clear after contrast administration• Indicative of neuro-osteoarthropathy with superimposed
osteomyelitisRadiology Assistant
Masses - benign
Plantar fibromatosis
Peripheral nerve sheath tumors
Lipomas
Glomus tumors
Ganglion cysts
Abscess
Epidermal Inclusion Cysts
Subcutaneous Granuloma Annulare
Masses - malignant
MFH – Malignant Fibrous Histiocytoma Common soft tissue sarcoma Spreads from calf Infiltrating, rapid growth Nonspecific MRI appearance
Synovial Sarcoma Cells resemble synovial membrane, only 5% intraarticular 2/3 lower extremity Slow growing, infiltrative Lobulated, with cysts/necrosis, fluid levels
Liposarcoma nonspecific

26
MFH
Radiopaedia.org
Synovial sarcoma