pai m et al. clin. microbiol. rev. 2014;27:3-20
TRANSCRIPT

1
David Koelle, MD
Allergy and Infectious Diseases, Department of Medicine, UW
Thanks to:Anne Cent, Supervisor, UW Clinical Virology Lab
G P L d T h l i t
“Understanding IGRAs”
Greg Pepper, Lead TechnologistRoxanne Porteus, Technical Secretary
Chris McClurkan, Research TechnologistMasae Kawamura, Qiagen
Janene Stageberg, Oxford Immunotec
Presentation contains quality control/quality improvement data. Do not reproduce without permission.
Concept of a TB spectrumnot just
“LTBI” vs. “ATBI”
ATBI
Positive IGRA
MTBdisease
Pai M et al. Clin. Microbiol. Rev. 2014;27:3-20
LTBI or TST
Themes• QFT/IGRA history and technology
• Real life use and results in a complex medical setting
• Grey zones, pain points, and inappropriate uses
– Arghh those *$)@#*@* intedeterminates• Is there ever any useful medical information in an indet result?
– (+) near the cutoff in a low‐risk patient– What patients are inappropriate for QFT?– Conversions and Reversions from QFT (‐) to QFT (+), vice versa– Does a TST prime for a true or false (+) QFT?
– Blood test for tuberculosis disease?

2
How do IGRA work?
Is Interferon Gamma Released? We Assay this.
MTB has 4,000 genes including the RD1 region encoding proteins ESAT6, CFP10
The IGRA TB antigen is peptides from ESAT6, CFP10, ± TB7.7
TB peptides stimulate memory T‐cells in blood that release IFN‐gamma upon exposure to the peptides
FDA approved:Quantiferon Gold or In‐tube (QFT‐IT)T‐SPOT‐TB
IGRA origins lie in veterinary medicine
Randall Reves Univ Colorado
Unique aspects of QuantiFERON‐IT
• Living T‐cells and other cells required
• Advanced collection tubes that are also reaction tubes– Pre bleed
• Specific manufacturing• Shelf life and storage temperature constraints
– Bleed• Shaking requirement “10 karate chops”• No line contaminants from advanced catheters
– After bleed• Time and temperature from bleed to lab• Options to start the lab phase near the bleed site and then transport
Almost every other blood test: lower tech tube, lower stringency at each step

3
MTB GENOME
CFP10 and ESAT6test for immune memoryto these MTB proteins
4 X 106 bp
RD1 = Region of Difference 1 deleted in BCG: fundamental advantage over TST deleted in almost all non‐tuberculous mycobacteria
Strains with RD1 DNA and therefore potentially “false” (+) IGRA:
• MTB complex: • M. bovis, M. africanum, M. microti, M. canetti
• NTM:• M. kansasii, M. szulgai, M. marinum
“Fish Finger Disease” Mycobacterium marinum
Tuberculosis‐like lung disease Mycobacterium kansasii
(+) IGRA in addition to MTB
Likes cooler temperatures (fingers…)Aquarium hobbyistsMarine biologistsFisheries industry
“water bug”2nd commonest NTM to affect lung
(#1 MAC #3 abscessus)Underlying lung disease common

4
Quantiferon workflow in pictures
Draw 3 X 1 ml To lab < 16 hours 37 oC 16‐24 hour Spin save plasma
Do ELISA for interferon‐gamma
~ 2016: Quantiferon workflow in pictures
Draw 4 X 1 ml To lab < 16 hours 37 oC 16‐24 hour Spin save plasma
Do ELISA for interferon‐gamma
Generations of QuantiFERON• 1st 2001 QuantiFERON‐TB (QFT) for humans
– Used PPD as test antigen just like TST– Same BCG pitfall as TST: possible false (+)
• 2nd 2005 QuantiFERON‐Gold– Switched to MTB peptides– Avoids BCG pitfall
• 3rd 2007 QuantiFERON‐TB Gold In‐Tube (QFT‐GIT)3 2007 QuantiFERON TB Gold In Tube (QFT GIT)– Avoids need to purify lymphocytes from blood– Starts with direct whole blood drawn into special tubes– A whole new set of issues....
• 4th ~ 2016 “QFT‐Plus”– MTB antigens different and in 2 tubes
• 4 tubes overall: 4 numbers (let us confuse people even more)– Won’t help “false positive, low MT‐nil, low‐risk person” specificity issue
– May improve detection of ATBI and splitting ATBI from LTBI– 2015 CE‐labeled for Europe; 2016 US FDA submission planned

5
Themes• QFT/IGRA history and technology
• Real life use and results in a complex medical setting
• Grey zones, pain points, and inappropriate uses
– Arghh those *$)@#*@* intedeterminates• Is there ever any useful medical information in an indet result?
– (+) near the cutoff in a low‐risk patient– What patients are inappropriate for QFT?– Conversions from QFT (‐) to QFT (+)– Reversions from QFT (+) to QFT (‐)– Does a TST prime for a true or false (+) QFT?– Blood test for tuberculosis disease?
QFT‐Plus• Nil (grey) = as per current product
• TB1 (green) = ESAT‐6 and CFP‐10 CD4 peptides
• TB2 (yellow) = ESAT‐6 and CFP‐10 CD4 and CD8 peptides
• Mitogen (purple) = as per current product
14• In‐lab phase as per current product
QFT‐Plus: potential role for diagnosis of ATBI?
TB2 – TB1 (nil subtracted)Observed ∼0.5 IU/ml difference between TB1 and TB2 in active disease
151. QuantiFERON‐TB Gold Plus Package Insert. October 2014. 1083163EN.
6
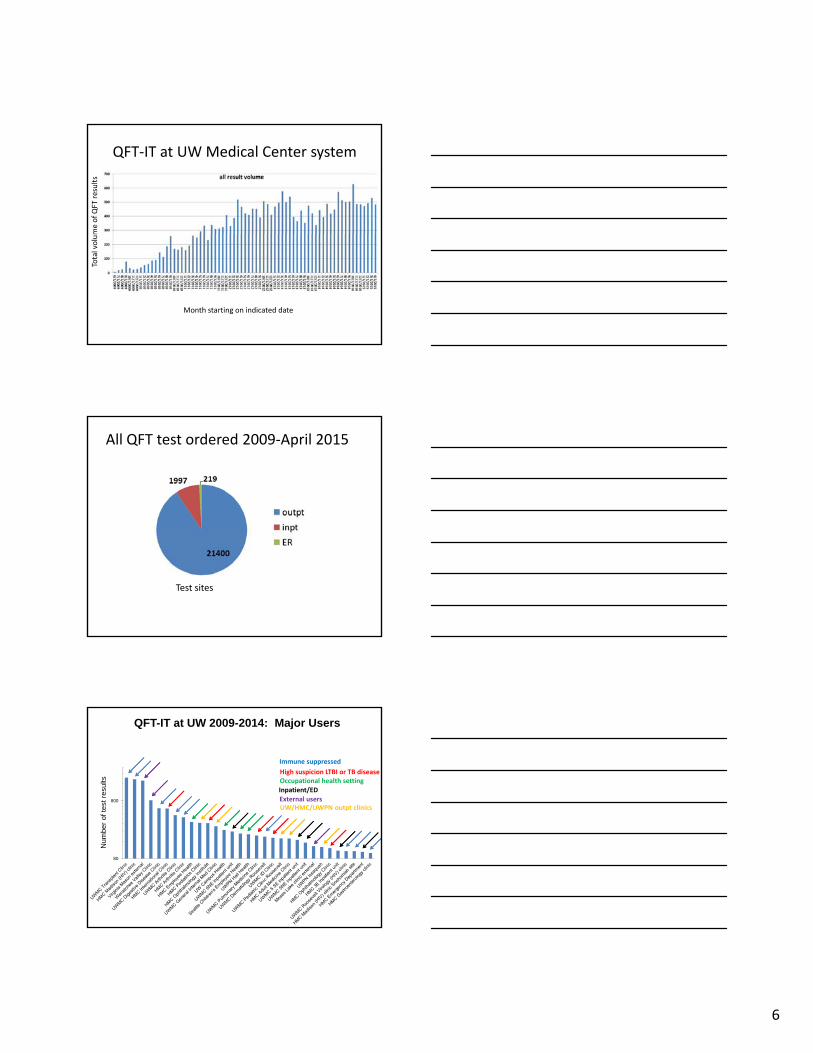
QFT‐IT at UW Medical Center system
me of QFT results
Month starting on indicated date
Total volu
All QFT test ordered 2009‐April 2015
Test sites
800
QFT-IT at UW 2009-2014: Major Users
of te
st re
sults
Immune suppressed High suspicion LTBI or TB diseaseOccupational health settingInpatient/EDExternal usersUW/HMC/UWPN outpt clinics
80
Num
ber o

7
All QFT results 2009‐end April 2015
T t it R lt ll t tTest sites Results all tests
Results all outpatient tests Results all inpatient tests
All QFT results 2009‐end April 2015
T t it R lt ll t tTest sites Results all tests
Results all outpatient tests Results all inpatient tests
Results trends: all tests
results
Month starting on indicated date
Percen
t of

8
Results trends: all tests
results
Month starting on indicated date
Percen
t of
Indet rate averagingaround 7%: quite highfor a medical test
Results trends: all tests
results
Month starting on indicated date
Percen
t of
high indetIndet rate averagingaround 7%: quite highfor a medical test
Outpatient tests
results
Month starting on indicated date
Percen
t of
high indet

9
Inpatient tests
results
Month starting on indicated date
Percen
t of
high indet
Themes• QFT/IGRA history and technology
• Real life use and results in a complex medical setting
• Grey zones, pain points, and inappropriate uses
– Arghh those *$)@#*@* intedeterminates• Is there ever any useful medical information in an indet result?
– (+) near the cutoff in a low‐risk patient – What patients/uses are inappropriate for QFT?– Conversions from QFT (‐) to QFT (+)– Reversions from QFT (+) to QFT (‐)– Does a TST prime for a true or false (+) QFT?– Blood test for tuberculosis disease?
Sources of variability in the QuantiFERON-TB Gold In-Tube assay.
Pai M et al. Clin. Microbiol. Rev. 2014;27:3-20

10
Sources of variability in the QuantiFERON-TB Gold In-Tube assay.
Pai M et al. Clin. Microbiol. Rev. 2014;27:3-20
!!!!
Issue 1 Endotoxin 2012
Lipopolysaccharide (=endotoxin = LPS) in the TB antigen tube
product recall Sep 27 2012 bad tubes Jan 6‐ Aug 2 2012
also happened with high altitude tubes early 2013
also happened in 2009 in Japan and Europe
LPS acts on TLR4 to activate immunity → high IFN gamma
Uh‐oh clinical impact: potential false (+)
Issue 2: mitogen too weak 2013‐2014 (?)
A mitogen is a substance thatcauses mitosis and also cell
activation, in this case including ll i bl d
Potential clinical impact: too many indeterminate tests
memory T cells in blood

11
• PHA = Phytohemagglutinin a bean protein
– uncooked red kidney beans (highest concentrations)
– white kidney beans (cannellini), green, broad beans
Meet your MIT: PHA
• It is a protein and biologically fragile
• It is multivalent and effects correlate with aggregation
• Agglutinates (cross‐links) “accessory cells” e.g. monocytes to T‐cells
Sources of variability in the QuantiFERON-TB Gold In-Tube assay.
Patientvariables
Pai M et al. Clin. Microbiol. Rev. 2014;27:3-20
n=78 SCCA samples with abs lymph within 5 d of QFT-IT
neg or pos indet
Seattle Cancer Care Alliance QFT data: low lymphocyte counts correlate with indeterminate results
n=65 n=13abs lymph
0 0 10-1000 35 10
1000-2000 22 22000-3000 6 03000-4000 1 0
>4000 1 0

12
Other variables associated with QFT indeterminate results
• HIV (+) CD4 < 200
• Liver failure
• Immune suppressive drugs
Sources of variability in the QuantiFERON-TB Gold In-Tube assay.
PRE‐LAB
Pai M et al. Clin. Microbiol. Rev. 2014;27:3-20
Site of draw is definitely associated with indeterminate rateCombined UWMC/HMC/UWPN/outside user data
Neg
Pos11%
Indet6%
Outpatient
Indet11%
ED/ER
N=14779
N=169
83%
Neg65%Pos
6%
Indet29%
Inpatient Neg70%
Pos19%
11%
N=1528

13
0
100
200
300
400
500
600
no of results
minutes between blood draw and temp upshift
negative
100
120
140
Indeterminate
Delay between blood draw and incubation @ 37 oCseems not to account for IND issue at UW
minutes between blood draw and temp upshift
0
5
10
15
20
25
30
35
40
45
no of results
minutes between blood draw and temp upshift
Positive
0
20
40
60
80
no of results
minutes between blood draw and temp upshiftTime between blood draw and 37 oC, min
Time between blood draw and 37 oC, min
Sources of variability in the QuantiFERON-TB Gold In-Tube assay.
Pai M et al. Clin. Microbiol. Rev. 2014;27:3-20
in‐LAB
Those )%*#) intedeterminates
• Optimally, an indeterminate result tells you that MTB infection data cannot be obtained from the QFT‐IT test– Low lymphocyte count– Low lymphocyte count
– Low lymphocyte activation potential
• Optimally, an improvement over the current TST in which “anergy” cannot be diagnosed

14
Results from UWMC pre‐transplant outpatient clinic
PHA problem summer 2013
Pre‐transplant getting a little better….
The other IGRA
T‐SPOT‐TB

15
Plusses and minuses of T‐SPOT‐TB• Plusses
– Compensates for lymphopenia (low lymphocytes per ml in patient blood sample as in some immune suppressed persons)
– Separates lymphocytes from liver/kidney toxins: might help
– Interpretive criteria recognizes “gray zone” reality • Four “results”: pos borderline=equivocal neg (plus• Four results : pos, borderline=equivocal, neg (plus indeterminate=invalid)
– Interpretive criteria recognize reality that pre‐test LTBI probability influences the positivity cutoff (Bayesian probability)
• Developing world: high pre‐test probability: high likelihood that a few spots are a true positive: fewer spots needed to call positive
• Developed world: low pre‐test probability: low likelihood that a few spots are a true positive: more spots needed to call positive
Plusses and minuses of T‐SPOT‐TB• Minuses and miscellany
– Still requires living lymphocytes: same issues as QFT– Definition of a “spot” is subjective– Expensive in‐lab phase
• Specialized equipment and staff/training• Seldom implemented in local/regional labs
– 8 results! • developed world origin (+) (-) borderline invalid
• developing world origin (+) (-) borderline invalid
• New central lab near Fedex headquarters one‐stop operation– Our cutoff time is 2 PM for draw at UWMC
• QFT‐IT and T‐SPOT TB each FDA approved/CDC recommended
Themes• QFT/IGRA history and technology
• Real life use and results in a complex medical setting
• Grey zones, pain points, and inappropriate uses
– Arghh those *$)@#*@* intedeterminates• Is there ever any useful medical information in an indet result?
– (+) near the cutoff in a low‐risk patient – What patients/uses are inappropriate for QFT?– Conversions from QFT (‐) to QFT (+)– Reversions from QFT (+) to QFT (‐)– Does a TST prime for a true or false (+) QFT?– Blood test for tuberculosis disease?

16
500
600
700
y
TB‐ nil, Pos samples
How positive is a positive? UW experience 2009‐2014
0
100
200
300
400
< 0.35 0.35 ‐ 1 1 ‐ 2 2 ‐ 3 3 ‐ 4 4 ‐ 5 5 ‐ 6 6 ‐ 7 7 ‐ 8 8 ‐ 9 > 9
Freq
uency
Frequency
Arguable low pos/borderlineClinical significance requires context
Unequivocally positive
Does IGRA (+) predict progression to tuberculosis disease in mid‐high incidence countries: NO
Unadjusted incidence rates for development of tuberculosis disease in the short term (median f/u 3 years), stratified by IGRA result. Rate estimates on X axis are per
1,000 person years of follow up. Pai M et al. Clin. Microbiol. Rev. 2014;27:3-20
Themes• QFT/IGRA history and technology
• Real life use and results in a complex medical setting
• Grey zones, pain points, and inappropriate uses
– Arghh those *$)@#*@* intedeterminates• Is there ever any useful medical information in an indet result?
– (+) near the cutoff in a low‐risk patient – What patients/uses are inappropriate for QFT?– Conversions from QFT (‐) to QFT (+)– Reversions from QFT (+) to QFT (‐)– Does a TST prime for a true or false (+) QFT?– Blood test for tuberculosis disease?

17
Seroconversions / seroreversions
T‐cell conversions / T‐cell reversions
463 unique persons had > 1 test
563 unique within‐person comparisons
386 persons had 2 tests58 persons had 3 tests16 persons had 4 tests2 persons had 5 tests1 person had 6 tests
Time between tests mean/median 287/258 days
200
time elapsed between QFT‐IT re‐tests 2009‐2014
173
84
47
120
59
2418 20
11 8 5 1 0 0 10
20
40
60
80
100
120
140
160
180
200
numbe
r of paired tests
days between tests
IRA Conversions and Reversions are a real problem in low risk HCW
Results of paired QFT‐IT tests UWMC/HMC 2009‐present
308
200
250
300
350
‐person test pairs
2336
55 61
2
40
1
45
0
50
100
150
neg toneg
neg topos
neg toind
pos toneg
pos topos
pos toind
ind toneg
ind topos
ind toind
Num
ber of with
in

18
Red countries where BCG vaccine is given after infancy or multiple times (at present or in past)
IGRA maybe better
Pai M et al. Clin. Microbiol. Rev. 2014;27:3-20
TST: less of a problem still fine in persons from yellow countries
Themes• QFT/IGRA history and technology
• Real life use and results in a complex medical setting
• Grey zones, pain points, and inappropriate uses
– Arghh those *$)@#*@* intedeterminates• Is there ever any useful medical information in an indet result?
– (+) near the cutoff in a low‐risk patient– What patients are inappropriate for QFT?– Conversions from QFT (‐) to QFT (+)– Reversions from QFT (+) to QFT (‐)– Does a TST prime for a true or false (+) QFT?– Blood test for tuberculosis disease or risk of tuberculosis disease?
“YES”
Themes• QFT/IGRA history and technology
• Real life use and results in a complex medical setting
• Grey zones, pain points, and inappropriate uses
– Arghh those *$)@#*@* intedeterminates• Is there ever any useful medical information in an indet result?
– (+) near the cutoff in a low‐risk patient– What patients are inappropriate for QFT?– Conversions from QFT (‐) to QFT (+)– Reversions from QFT (+) to QFT (‐)– Does a TST prime for a true or false (+) QFT?– Blood test for tuberculosis disease or risk of tuberculosis disease?
NO!

19
Case 1• 68 yr old man Haitian, in US 24 years, with cough and fever. Community clinic does CXR (abnormal) and refers. You admit, isolate, collect sputum (AFB smear pending) and treat for community acquired pneumonia. Will a QFT be useful and why/why not?
1) useful: if (+) he has TB disease and needs empiric RIPE– 1) useful: if (+) he has TB disease and needs empiric RIPE– 2) useful: if (+) he has LTBI and needs Rx at some point– 3) useful: if (+) must screen family & contacts– 4) useful: if (‐) he does not have TB disease, d/c isolation– 5) useless: high pre‐test probability of TB immune memory; IGRA cannot distinguish LTBI from TB disease; cost‐benefit of LTBI therapy may be low
Case 2– 26 year old nurse starting at the hospital. No int’l travel or known TB exposure and always had (‐) TST, last one year ago. Rubella, VZV, HBV immune. QFT shows
• Nil 0.06• MTB 0.46• Mit >10
D– Do you– 1) perform TST now– 2) repeat QFT now– 3) CXR and history to r/o TB disease, if normal, LTBI Rx– 4) perform T‐SPOT‐TB now– 5) no more testing, allow to begin duty, re‐test later
OUR CASE
Nil 0.06 nil is <8 so far so goodMTB 0.46 TB minus nil is 0.4, which is > 0.35 and > 25% of nilMit >10 mitogen minus nil > 0.5, mit result does not change interp

20
Conclusions: IGRA• Ask for the numbers and not just the “interpretation”
• LTBI testing most appropriate in med‐high pre‐test probability of LTBI• IGRA preferred if h/o multiple or post‐infancy BCG• IGRA equivalent to TST if no BCG• TST perhaps fine if one infancy BCG
– Will person benefit from Rx of LTBI if diagnosed?• Lower pre‐test probability but irreversible/severe immune suppression coming upWill R f LTBI if di d?• Will you Rx for LTBI if diagnosed?
• ED/ER and much inpatient use may not be appropriate
• High‐tech pre‐analytical phase: challenges, product defects
• HCW screening plagued by high “low (+)” rate, and high conversion and reversion
– Possible higher cutoffs may be appropriate– ?confirm with TST or repeat IGRA: CDC suggestion– Must place in context of pre‐test probability of MTB infection