pathology seminar series april 24, 2012 stephanie...
TRANSCRIPT

Pathology Seminar Series April 24, 2012
Stephanie Schutte, MD

Etiology and Pathogenesis
IPF
Radiologic progression
Acute exacerbation
Microscopic pathology
Gross pathology
Risk factors
Epidemiology
Clinical features
Radiologic features
Leslie K. Arch Pathol Lab Med. 2011
Genomic Approach

IPF Review � Unrelenting accumulation
of myofibroblasts and deposition of collagen
� Histology: UIP pattern,
advanced fibrosis with destruction of lung architecture, honeycombing
� The fibroblastic foci is an area of major study � New focus on the epithelial-
mesenchymal border

IPF - Mechanism of injury � A shift:
� From – inflammation invariably leading to fibrosis
� To – repeated epithelial injury and aberrant wound healing leads to fibroblast/myofibroblast accumulation
� Why the change? � Anti-inflammatory and immune modulatory
therapy isn’t working � Both epithelial cells and fibroblasts undergo
distinct phenotypic changes

Normal response to damage � Alveolar epithelial cells: proliferate and
produce inflammatory signals � TGF-β, PDGF, EGF, and FGF-2
� Fibroblasts: respond to epithelial cell signals � Activate and differentiate into myofibroblasts
� Myofibroblasts: secrete collagens and extracellular matrix proteins � A second source of myofibroblasts? EMT
Epithelial-mesenchymal transition (EMT)
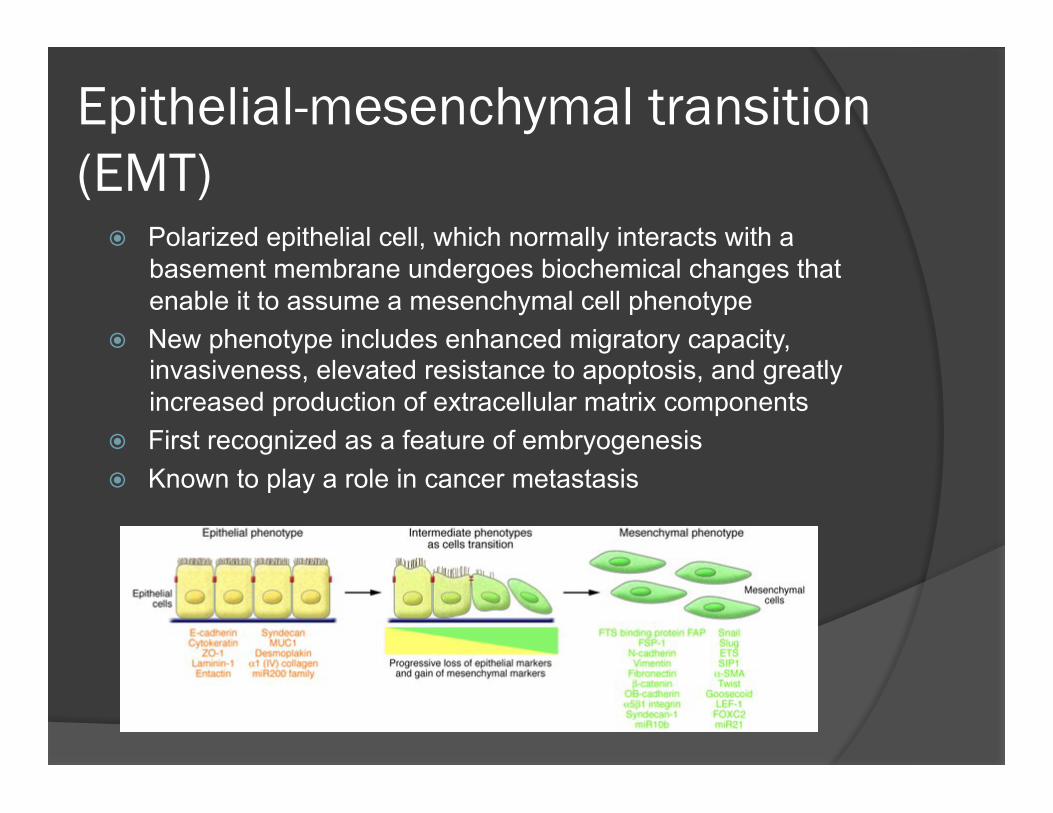
� Polarized epithelial cell, which normally interacts with a basement membrane undergoes biochemical changes that enable it to assume a mesenchymal cell phenotype
� New phenotype includes enhanced migratory capacity, invasiveness, elevated resistance to apoptosis, and greatly increased production of extracellular matrix components
� First recognized as a feature of embryogenesis � Known to play a role in cancer metastasis

Epithelial-Mesenchymal transition (EMT)
� Three biologic settings in which this occurs: � EMT during implantation, embryogenesis,
and organ development
� EMT associated with cancer progression and metastasis
� EMT associated with tissue regeneration
and organ fibrosis

EMT associated with organ fibrosis
Inflammatory cells and fibroblast generate signalling molecules, which initiate EMT
Induce basement membrane damage, allowing epithelial cells to migrate into the interstitium
Growth factors and other molecules in the interstitium complete the transition

EMT associated with organ fibrosis
Different sources of fibroblasts in organ fibrosis.
• 12% of fibroblasts are from bone marrow • 30% can arise via local EMT involving epithelial cells under inflammatory stress
• 35% are from EndMT
• Proliferation of the resident fibroblasts • Other still unidentified sources.

What goes wrong in IPF? � Normal wound healing – signals are
present that terminate the process � IPF – no termination signals
� Alveolar cells that have undergone EMT do not properly repair alveolar lining
� Fibroblast accumulation and collagen deposition continues
� IPF studies: why does the process fail to
terminate?

Evolving Genomic Approaches to Idiopathic Pulmonary Fibrosis: Moving Beyond Genes.
� Daniel Kass, MD and Naftali Kaminski, MD
� Clin Transl Sci. 2011 October; 4(5): 372-379

Objectives � What are the sources of genomic data in IPF? � Do genomic approaches provide clinically
relevant diagnostic information on IPF? � Do genomic approaches provide clinically
relevant prognostic information on IPF � How has genomic research enhanced our
understanding of the pathogenesis of IPF? � What is the state of “epigenomic” research in
IPF? � What is the future of genomic research in IPF?

Sources of genomic data � Lung tissue from
patients � Biopsy � Explant � Autopsy � “Controls”
� Surrogate tissues � Cultured fibroblasts � Bronchoalveolar lavage � Peripheral blood � Fibrocytes

Lung tissue from patients � Biopsy
� Transbronchial biopsies � Wedge biopsies
� Explants � Numbers?
� Autopsy � Delay to autopsy damages tissue � “warm” or rush autopsies
� “Control” lung tissue for comparison � Normal section from cancer case � Rejected cadaveric donors � Granuloma or scar biopsy

Surrogate tissues
� Cultured fibroblasts � Cells grown under a variety of conditions
and in response to various stimuli
� BAL � gene profile of inflammatory cells
� Peripheral blood – mononuclear cells � Gene expression of mononuclear cells

Surrogate tissues
� Fibrocytes � Identified in 1994, likely bone-marrow derived
collagen-producing cells � Circulate in the peripheral blood � Migrate to sites of injury and differentiate into
fibroblast-like cells � Purified from PB and analyzed � Express collagen-1, CD45, CD34 � TGF-β stimulates them to express α-smooth
muscle actin
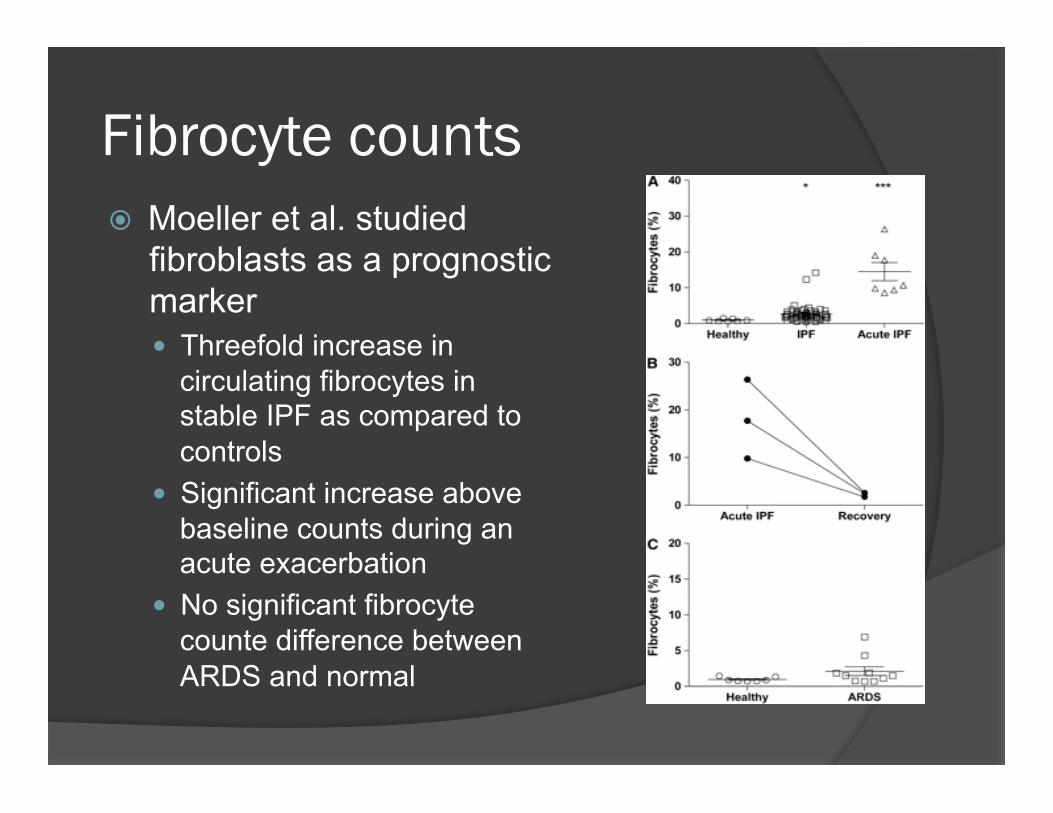
Fibrocyte counts � Moeller et al. studied
fibroblasts as a prognostic marker � Threefold increase in
circulating fibrocytes in stable IPF as compared to controls
� Significant increase above baseline counts during an acute exacerbation
� No significant fibrocyte counte difference between ARDS and normal

Fibrocyte counts � Higher fibrocyte counts
correlated with dramatically decreased survival (7 months v. 27 months)
� Other clinical parameters did not correlate with survival

Objectives � What are the sources of genomic data in IPF? � Do genomic approaches provide clinically
relevant diagnostic information on IPF? � Do genomic approaches provide clinically
relevant prognostic information on IPF � How has genomic research enhanced our
understanding of the pathogenesis of IPF? � What is the state of “epigenomic” research in
IPF? � What is the future of genomic research in IPF?

Genomic Profiling � Genomic profile: Information about all the genes in
an organism, including variations, gene expression, and the way those genes interact with each other and with the environment
� Genotyping & Genomic Profiling Techniques � Single nucleotide polymorphism Genotyping � Copy Number Variation � Array comparative genomic hybridization � Amplified length polymorphism, Restriction fragment length
polymorphism, Single strand confirmation polymorphism � High Resolution Melting (HRM) Analysis � TaqMan® Mutation Detection Assays � Microsatellite Analysis � In Situ Hybridization (ISH)
� 2002 – 1st microarray experiments comparing IPF to uninjured controls were performed
Diagnostic information � How is the diagnosis of IPF made?
� Gold standard: wedge biopsy of lung � Clinical/radiologic correlation is important � Diagnosis of exclusion
� What if histopathology and clinical correlation fails to make the diagnosis? � Consider a genomic approach � Is IPF a unique disease with a unique genomic
profile? Can we then use this profile to make the diagnosis of IPF?

Diagnostics – Selman et al. � Study
� Compared lung samples of patients with IPF, hypersensitivity pneumonitis (HP), and nonspecific interstitial pneumonia (NSIP) using custom oligonucleotide microarrays
Results: what genes are expressed?
• IPF – tissue remodeling, epithelial and myofibroblast genes • HP – inflammation, T-cell activation, immune responses • NSIP – most didn’t classify as IPF or HP (has its own distinct gene signature?)

� Conclusions - IPF lungs do not exhibit ‘typical’ inflammatory patterns, instead it is characterized by genes involved in active tissue remodeling
A. Matrix metalloproteinase-1
B. IGFBP-4
C. N-cadherin
Note expression in epithelial cells.

Diagnostics – Hsu et al. � Genomic patterns in IPF and systemic
sclerosis related pulmonary fibrosis (SSc-PF) � Results
� 70% of genes that distinguish IPF and SSc-PF from normal lung are shared
� Conclusions � Clinically unique diseases with similar genomic
profiles � Only a small group of genes differentiates one
from the other

A. Microarray analysis showing genes that are upregulated and downregulated B. Cluster patterns:
1. Genes that are upregulated in both SSc and IPF 2. Genes that are upregulated in both SSC-PF and IPF
3. Genes that are downregulated in both SSc-PF and IPF 4. Genes that are downregulated in both SSc and IPF
C. Venn diagrams showing numbers of unique and shared genes.

Diagnostics – future considerations
� Can a particular gene pattern diagnose UIP or HP or NSIP or SSc when histology and clinical criteria can not?
� Can gene expression identify patients who will respond to immunosuppressive therapy?

Objectives � What are the sources of genomic data in IPF? � Do genomic approaches provide clinically
relevant diagnostic information on IPF? � Do genomic approaches provide clinically
relevant prognostic information on IPF � How has genomic research enhanced our
understanding of the pathogenesis of IPF? � What is the state of “epigenomic” research in
IPF? � What is the future of genomic research in IPF?
Prognostic information
� Clinical predictors of increased mortality � Rate of decline in spirometry � Degree of exercise limitation � Presence of pulmonary hypertension � An acute exacerbation
� Genomic approaches compare those who have increased predictors to those who don’t

Prognostics � Rajkumar et al. – compared patients with
idiopathic pulmonary artery HTN (PAH) to patients with HTN secondary to IPF
� Results
� IPF patients with pulmonary HTN had distinctive gene signatures as compared to patients with PAH and normal subjects
� Genes that function in TGF-β and platelet derived growth factor signaling pathways were enriched in IPF patients with pulmonary HTN

Prognostics � Boon et al. – compared gene expression profiles of
patients with stable disease and rapidly progressing disease � SAGE technique (Serial Analysis of Gene Expression) � Uncovered gene transcripts that distinguished stable
versus progressive IPF ○ 102 up-regulated transcripts (progressive group) ○ 89 down-regulated transcripts (progressive group)
� Plunc (palate, lung and nasal epithelium carcinoma associated protein) ○ Not previously implicated in IPF

Prognostics � Plunc staining in IPF (bronchial columnar
cells in areas of honeycombing) as compared to normal control (no Plunc expression)
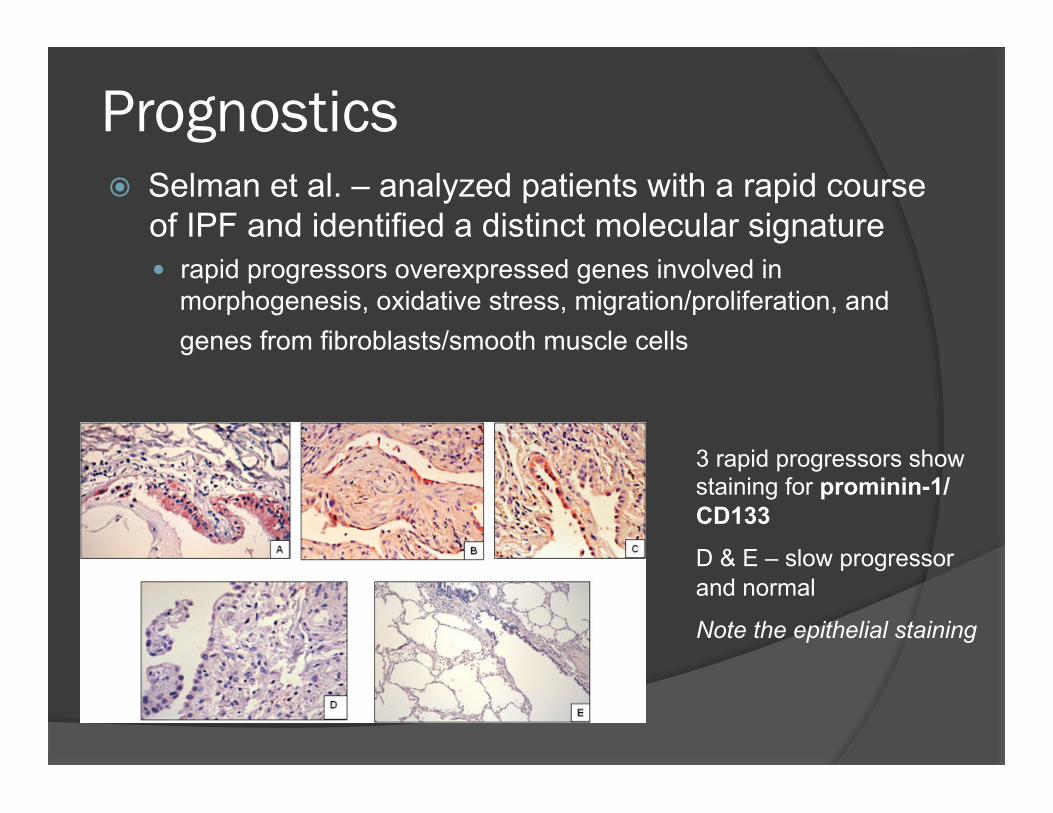
Prognostics � Selman et al. – analyzed patients with a rapid course
of IPF and identified a distinct molecular signature � rapid progressors overexpressed genes involved in
morphogenesis, oxidative stress, migration/proliferation, and genes from fibroblasts/smooth muscle cells
3 rapid progressors show staining for prominin-1/CD133
D & E – slow progressor and normal
Note the epithelial staining

Objectives � What are the sources of genomic data in IPF? � Do genomic approaches provide clinically
relevant diagnostic information on IPF? � Do genomic approaches provide clinically
relevant prognostic information on IPF � How has genomic research enhanced our
understanding of the pathogenesis of IPF? � What is the state of “epigenomic” research in
IPF? � What is the future of genomic research in IPF?

Pathogenesis
� Most IPF studies have focused on single genes to determine their relevance to IPF
� Looking to identify potential drug targets � Identify factors that promote fibroblast
accumulation in the lung � Why do they have increased proliferation and
decreased apoptosis?

Pathogensis � Matrilysin (matrix metalloproteinase 7, MMP-7)
� Early IPF studies using gene expression profiling (Zuo et al.) � Enriched expression of MMP-7 � MMP-7 -/- mice were protected from bleomycin induced PF � Mechanism? A possible biomarker?
� Twist1 � Plays a role in tumor metastasis and epithelial-mesenchymal
transition � Necessary for fibroblast survival in vitro � Mediator of EMT in pulmonary fibrosis

Pathogenesis � Osteopontin
� Increases proliferation and migration in human lung fibroblasts and Type II alveolar epithelial cells
� Increased gene expression has been confirmed by real-time PCR in patients with UIP (as has increased MMP7)
� Pigment epithelium-derived factor � Present in fibroblastic foci of IPF � Induced by TGF-β1
Pathogenesis – cell biology
� IPF fibroblasts have pro-proliferative and anti-apoptotic properties
� Why?
� Increased Wnt5a expression, acts as a pro-proliferative and anti-apoptotic signal in human lung fibroblasts
� React differently than normal lung fibroblasts to TGF-β1 stimulation

Pathogenesis – global gene expression patterns
� Significantly increased expression (in IPF) of genes that are associated with lung development � Wnt and TGF-β signalling pathways � A pathologic ‘repetition’ of embryonic
development?

TGF-β and PTEN � TGF-β: controls cell
growth, cell proliferation, cell differentiation and apoptosis
� PTEN inhibits cell migration, promotes cellular apoptosis , and inhibits cell growth
� Fibroblasts of IPF patients have been shown to diminished PTEN expression

PTEN & PS6 expression � Evaluate PTEN & PS6 expression in IPF lungs vs.
lungs with non-progressive fibrosis vs. normal
Image 1 – Normal lung: H&E, PS6, PTEN, and SMA (left to right). Normal airway shows positivity for SMA (smooth muscle), PTEN (epithelium), and PS6 (epithelium).

PTEN & PS6 expression
� Subpleural fibrosis (non-progressive)
Image 2 – Reactive pleuritis with fibrosis: H&E, PS6, PTEN, and SMA (left to right). In these areas of subpleural fibrosis, SMA, PTEN, and PS6 expression is strong and coexpressed. In the normal pleura there is no SMA or PTEN staining.

PTEN & PS6 expression
� Fibroblastic foci of IPF
Image 3- Idiopathic pulmonary fibrosis: H&E, PS6, PTEN, and SMA (left to right). The fibroblastic foci (arrows) shows SMA positivity and loss of PTEN/PS6. The normal epithelium (lower aspect) maintains PTEN/PS6 expression.

Results � In the non-progressive fibrosis cases, SMA, PTEN
and PS6 expression were all strongly positive in subpleural areas of fibrosis and also areas of organization.
� In the IPF cases, SMA showed strong positivity in
fibroblastic foci and honeycomb areas while PTEN and PS6 expression were decreased.
� Interestingly, the epithelium overlying the fibroblastic foci was greatly attenuated with decrease in PTEN and PS6 expression.

TGF-β and PTEN � TGF-β: controls cell
growth, cell proliferation, cell differentiation and apoptosis
� PTEN inhibits cell migration, promotes cellular apoptosis , and inhibits cell growth
� Fibroblasts of IPF patients have been shown to diminished PTEN expression
Conclusions � In IPF, in areas of fibroblastic foci and honeycombing , SMA
expression increases while PTEN and PS6 decrease.
� In reactive pleuritis with fibrosis, SMA, PTEN and PS6 are strongly coexpressed.
� PTEN repression contributes to myofibroblastic differentiation, proliferation and continued matrix deposition in IPF and may be a factor in the progression of the disease.
� Because non-progressive scarring can show variable PTEN expression, other pathways may also be active in the progressive injury of IPF.

Objectives � What are the sources of genomic data in IPF? � Do genomic approaches provide clinically
relevant diagnostic information on IPF? � Do genomic approaches provide clinically
relevant prognostic information on IPF � How has genomic research enhanced our
understanding of the pathogenesis of IPF? � What is the state of “epigenomic” research in
IPF? � What is the future of genomic research in IPF?

Epigenomic research � Epigenetics –regulation of phenotype or gene
expression by changes independent of the underlying DNA sequence
� Uses many of the same techniques as genomic studies
� Methylation � Early studies: changes in global methylation
patterns in IPF tissue and fibroblasts
� MicroRNA recruitment

Epigenomics - microRNA � microRNA let7d
� Decreased in IPF � Binds to a TGF-β intermediate � Inhibition of let7d increased collagen gene
expression and EMT in mice
� microRNA 21 � Increased in IPF and 1 ̊ lung fibroblasts
stimulated with TGF-β � Suppression of miR-21 attenuated bleomycin-
induced lung injury in mice

Objectives � What are the sources of genomic data in IPF? � Do genomic approaches provide clinically
relevant diagnostic information on IPF? � Do genomic approaches provide clinically
relevant prognostic information on IPF � How has genomic research enhanced our
understanding of the pathogenesis of IPF? � What is the state of “epigenomic” research in
IPF? � What is the future of genomic research in IPF?

The future of genomic research
� Obstacles to overcome � Limited availability of tissues � Data sharing across centers � Must replicate observations independently � Training for new genomic researches
� NIH funded studies � Created a repository of lung tissue, blood, imaging and
clinical data of IPF patients � Multidisciplinary teams are assembling databases of
genomic data on IPF � Ensure adequate funding for training of new researches

The future of genomic research
� Paradigm shift from single-gene approach to a global genome approach � Provides more insight in the complex pathogenesis of IPF � Provide a better working model of how abnormal organ
phenotypes are maintained over time, years after the inciting injury
� Impact for patients � A few clinical trials involving newer molecular
targets, including TGF-β � No trials yet involving MMP-7, Twist1, IGFBP,
and microRNA

Conclusion
� Genomic research has had an impact on our understanding of IPF
� Genomic profiling has identified several new molecules involved in the mechanism of IPF
� Genomic profiling has demonstrated that gene signatures may be able to predict the rate of IPF progression
References Dr. Jagirdar Leslie K. Idiopathic Pulmonary Fibrosis May Be a Disease of Recurrent, Tractional Injury to the Periphery of the Aging Lung. A Unifying Hypothesis Regarding Etiology and Pathologenesis. Arch Pathol Lab Med. October 2011. Kass D, Kaminski N. Evolving Genomic Approaches to Idiopathic Pulmonary Fibrosis: Moving Beyond Genes. Coin Transl Sci. 2011 October; 4(5):372-379. Maher TM, Wells AU, Laurent GJ. Idiopathic pulmonary fibrosis: multiple causes and multiple mechanisms? Eur Respir J. 2007; 30:835-839 Moeller A, Gilpin SD, Ask K, Cox G, Cook D, Gauldie J, Margetts PJ, Farkas L, Dobranowski J, Boylan C, et al. Circulating fibrocyes are an indicator of poor prognosis in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2009; 179:588-594. Selman M, Pardo A, Barrera L, Es-trada A, Watson S, Wilson K, Aziz N, Kaminski N, Zlotnik A. Gene Expresion Profiles Distinguish Idiopathic Pulmonary Fibrosis from Hypersentsitivity Pneumonitis. Am J Respir Crit Care Med. 2006; 173: 188-198. Boon K, Bailey N, Yang J, Steel M, Groshong S, Kervitsky D, Brown K, Schwarz M, Schwartz D. Molecular Phenotypes Distinguish Patients with Relatively Stable from Progressive Idiopathic Pulmonary Fibrosis. PLoS One. 2009; 4:e5134. Hsu E, Shi H, Jordan RM, Lyons-Weiler J, Pilewski JM, Feghali-Bostwick CA. Lung tissues in patients with systemic sclerosis have gene expression patterns unique to pulmonary fibrosis and pulmonary hypertension. Arthritis Rheum. 2011 March;63(3):783-94. Rajkumar R, Knoishi K, Richards TJ, Ishizawar DC, Wiechert AC, Kaminski N, Ahmad F. Genomewide RNA expression profiling in lung identifies distinct signatures in idiopathic pulmonary arterial hypertension and secondary pulmonary hyptertension. Am J physiol Heart Circ Physiol. 2012 April;298(4):H1235-48. Kalluri R, Wienberg R. The basics of epithelial-mesenchymal transition. J Clin Invest. 2009;119(6):1420–1428. http://www.invitrogen.com/site/us/en/home/Products-and-Services/Applications/Gene-Expression-Analysis-Genotyping/Genotyping-Genomic-Profiling.htm White E, Atrasz R, Hu B, Phan S, Stamblic V, Mak T, Hogaboam C, Flaherty K, Martinez F, Kontos C, Toews G. Negative Regulation of Myofibroblast Differentiation by PTEN (Phosphatase and Tensin Homolog Deleted on Chromosome 10) . Am J Respir Crit Care Med. Vol 173. pp 112-121. 2006. Sawyers C. The Cancer Biomarker Problem. Nature 452, 548-552(3 April 2008)