patient-centered medical home improvement dashboard overview and implementation instructions
DESCRIPTION
pcmh overview and instructionsTRANSCRIPT

Patient-Centered Medical Home Improvement Dashboard: Implementation Instructions and Overview
Developed by: Kyrsten Chambers
Access HealthColumbus Staff
Carol Deibel Access HealthColumbus Consultant
For any questions regarding this document please contact:
Jeff Biehl, President, Access HealthColumbus: [email protected] Kyrsten Chambers, Project Coordinator, Access HealthColumbus: [email protected]
2

Patient-Centered Medical Home Dashboard Introduction, Data Collection Instructions, Survey
Administration and Supporting Documents
I. Introduction and Overview The Patient-Centered Medical Home Dashboard is compiled to support improvement, in primary care practices in the following areas:
• Capacity to schedule same day appointments (access) • Continuity of care (patient predominately sees their personal physician) • Consistent screenings among diabetic patients:
o HbA1c o Lipid profile o Nephropathy screening o Foot examination o Eye exam o Smoking status and cessation counseling or treatment
• Management of diabetic testing outcomes (See Attachment A for Diabetes Measurement Descriptions) :
o HdA1c levels o LDL levels o Blood pressure levels
• Utilization metrics for Emergency Department, hospitalization, re-hospitalization, and generic RX use (data collected from participating Health Plans)
• Level of patient activation in their chronic disease self-management (PAM Survey) • Patient experience within their primary care practice (CAHPS Survey) • Provider and staff satisfaction with their job (MBI Survey)
Initial data collection begins when a practice enters a collaborative agreement with Access HealthColumbus and a HIPAA agreement has been executed between Access HealthColumbus and the participating primary care practice (aka Business Associate Agreement). Note: It is the intent of Access HealthColumbus to work with our partners to collect, analyze, and report outcomes in a manner that provides comparisons without identifying individual primary care practices or providers. II. Primary Care Practice Data Submission Instructions
A. Privacy & Security: We intend to transfer and keep this data highly private. We have established a secure FTP server. We will provide your designee with the key and any assistance needed in using it to transfer your files there. Do not use e-mail to send the data or randomization files. B. Randomization and sampling: Randomization is needed for the selection of the diabetes patient sample (clinical data and self-management survey) and the total patient sample (patient experience survey). We would like to support this step, helping to assure consistent methods. Please provide a list file of patients according to the following criteria. We will quickly sample it and return the resulting sample lists to you for use in diabetes data collection and survey names and addresses.

• include patients at or over age 18 • who have had an office visit within the last 12 months • do not exclude patients who have left the practice • ID them irrespective of the reason for the visit or duration of the patient-physician relationship • multiple individuals per household are ok • exclude patients receiving a recent patient experience survey or determined to be receiving
one shortly
The Patient ID list should Include these elements in the file: 1- Patient ID 2- Assigned Physician/Clinician name 3- Patient has diabetes (yes/no) 4- Patient birthday (mmddyyyy) or age C. Format: You may submit the access and clinical (diabetes) data to us in one of three ways:
1- Summary level Excel files for each physician/clinician, as per the second and fifth worksheets in the attached file OR 2- Worksheet level Excel files for each physician/clinician, as per the third, fourth, and last worksheets in the attached file OR 3- CSV or Excel file(s) that you generate for each physician/clinician that contain the same elements specified in the worksheets in the attached file. Provide the field map (or file record layout) for the files.
D. Completeness: We'd like to receive complete files from you all at once, i.e. data that includes all of your physicians/clinicians. The exception to this would be if clinical data that is mined from chart reviews takes longer to complete, then please send the other data as soon as possible so we can begin to compile it. E. Worksheets: If you are unable to collect the same day appointment (access) and continuity of care data electronically, we have provided you with worksheets to collect this information. (Please See Attachment B) For the clinical data collection, we can provide chart review assistance as needed. Updated worksheets are in the attached file. Please upload the information requested below onto the FTP server account provided: 1- File transfer contact name and e-mail or phone number (see A.) 2- Expected date for providing the sampling list (see B.) 3- Expected date for providing the access and clinical (diabetes) data to Access HealthColumbus (see C. D. & E.)
F. Chart Review Assistance: If needed, Access HealthColumbus can provide chart review assistance to aide in the collection of the Patient-Centered Medical Home Improvement Dashboard clinical data. We will provide a nurse consultant to assist in gathering the requested information. If your practice indicates that you will need chart review assistance, we ask that you review the following procedures:
1. Schedule chart review assistance at the appropriate time that your practice will be prepared to start collecting this data
2. Please provide a point of contact for the nurse consultant to contact regarding: a. Scheduling confirmation b. Directions c. Etc.
3. Please provide a workspace for the nurse consultant 4. Pull the 25 charts per physician(same patient sample as the PAM survey) to be reviewed
(electronically or paper file), prior to scheduled arrival 5. Please make sure to schedule a few minutes of your initial meeting with the nurse consultant to
go over your practice patient chart layout or EMR system
III. Survey Samples and Administration Details A. Survey Overview As part of the PCMH Improvement Dashboard, we will be administering three different surveys in the categories of Patient Self-Management, Medical Home Team Satisfaction, and Patient Experience. Each survey has a specific set of instructions. Please see below for an overview of each of the surveys and detailed administration information.
Patient Self-Management Patient self-management will be measured by a survey that assesses the knowledge, skills and confidence integral for patients to manage their health and healthcare. This survey places patients into one of four activation levels. The PAM survey questions are provided at the end of this section. The instrument utilized will be the Patient Activation Measurement (PAM) survey from Insignia Health. The PAM survey will be given to 25 patients per physician that meet the following criteria:
• 18-75 years old • Diabetes (type 1 or 2) • Had at least one visit within the last 12 months
In order to select the sample for this survey, we will use the patient ID list previously requested. Selected patients will receive a survey packet that includes a cover letter from their primary care practice, the PAM survey and a return envelope (postage included). A second mailing will be conducted based on survey return rate. Please see Attachment C to review the draft cover letters. We need you to approve the PAM cover letters and insert them onto your practice letterhead. Please designate a staff member to be the contact person for the PAM survey at your practice. Their contact information should be inserted in the highlighted areas on the PAM cover letters. Please see the attached PAM cover letter sample In addition, completed surveys will be mailed to an Access HealthColumbus P.O. Box. We have created a P.O. Box address specifically for your patients’ survey results. Your P.O. Box address that will be on the sent and return envelope is:
Primary Care Practice Site PAM Survey Results
PO Box 16567 Columbus, Ohio 43216
1

6

Medical Home Team Satisfaction Employee satisfaction will be measured with a survey that assesses staff feelings of ones’ work.
The survey measures staff’s feelings and emotional response toward recipients of one’s service, care treatment or instruction. Staff’s feelings of competence and successful achievement in their job are also measured. The instrument utilized will be the Maslach Burnout Inventory survey. We are requesting that all practice staff (including physicians, clinicians, nurses, and non-clinical staff) whose job is affected by the practice Patient-Centered Medical Home transformation process, complete this survey. Staff will be asked how they relate to the following statements:
Staff Questions
I feel emotionally drained from my work.
I feel tired when I get up in the morning and have to face another day on the job.
I can effectively solve the problems that arise in my work.
I feel I am making an effective contribution to what this organization does.
I have become less enthusiastic about my work.
I feel exhilarated when I accomplish something at work.
I just want to do my job and not be bothered.
I doubt the significance of my work
I feel used up at the end of the workday.
Working all day is really a strain for me.
I feel burned out from my work.
I have become less interested in my work since I started this job.
In my opinion, I am good at my job.
I have accomplished many worthwhile things in this job.
I have become more cynical about whether my work contributes anything.
At my work, I feel confident I that I am effective at getting things done.
This survey will be administered through an online tool. We have created 27 usernames (email addresses) for your practice, which can be found on the worksheet below: “Staff Survey Worksheet”. Please assign an email address to each staff member, then provide your practice link and email address to them. Please see the worksheet below for your practice’s link to the survey. Staff members will be asked to enter the invited email address when they enter the survey website. Please ask them to use the assigned email address. This worksheet is for you to keep track of which staff members have completed the survey. We encourage your practice to complete this survey as soon as possible. We will be able to track how many of your assigned usernames have completed the survey, and will provide you with an update via email of which usernames have not yet completed the survey.
2
7

Worksheet: Primary Care Practice Site Employee Survey Available Usernames
Please use this worksheet to assign staff members an email address. Please make sure to provide your practice link: http://www.mindgarden.com/rsvp/sample to each staff member. This worksheet is for practice use only.
Username: Assigned: Staff Member: [email protected]
8

3
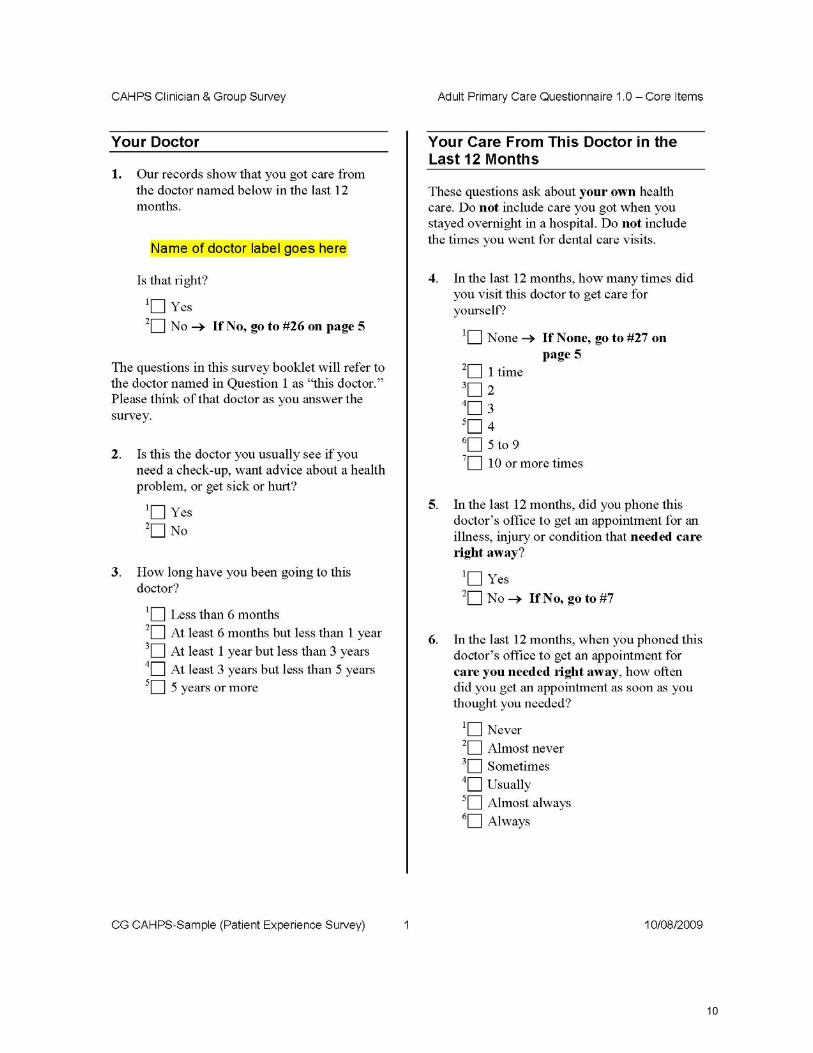
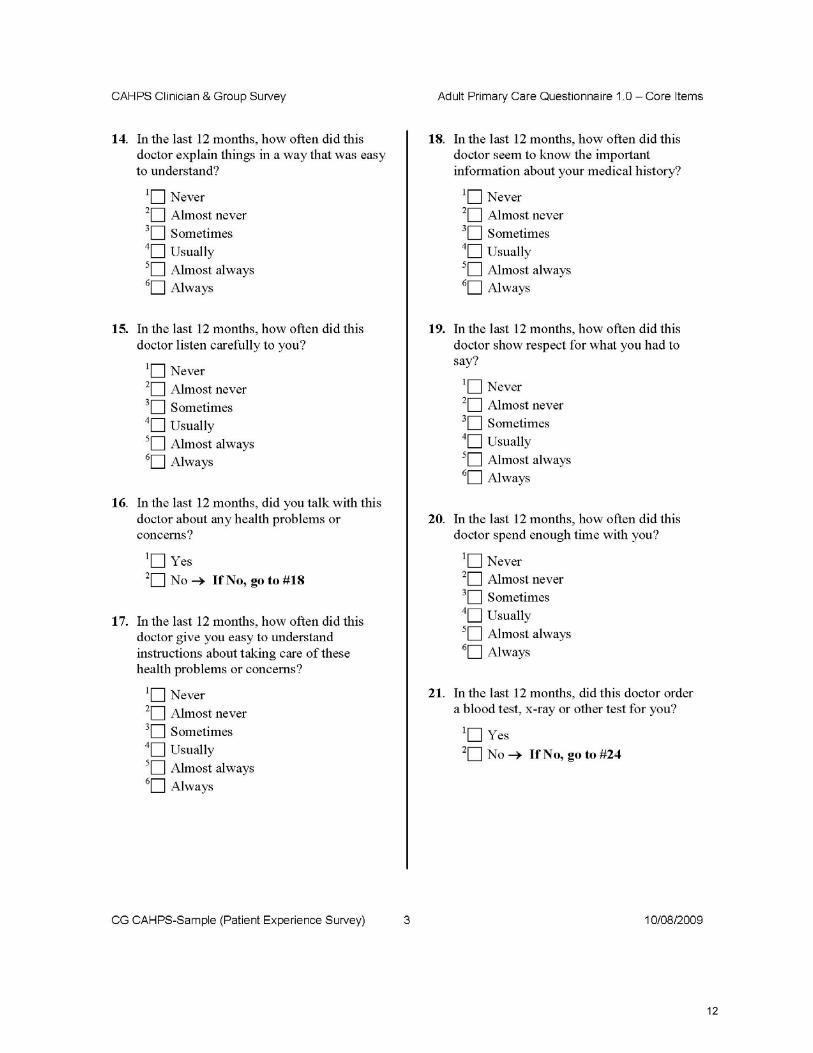
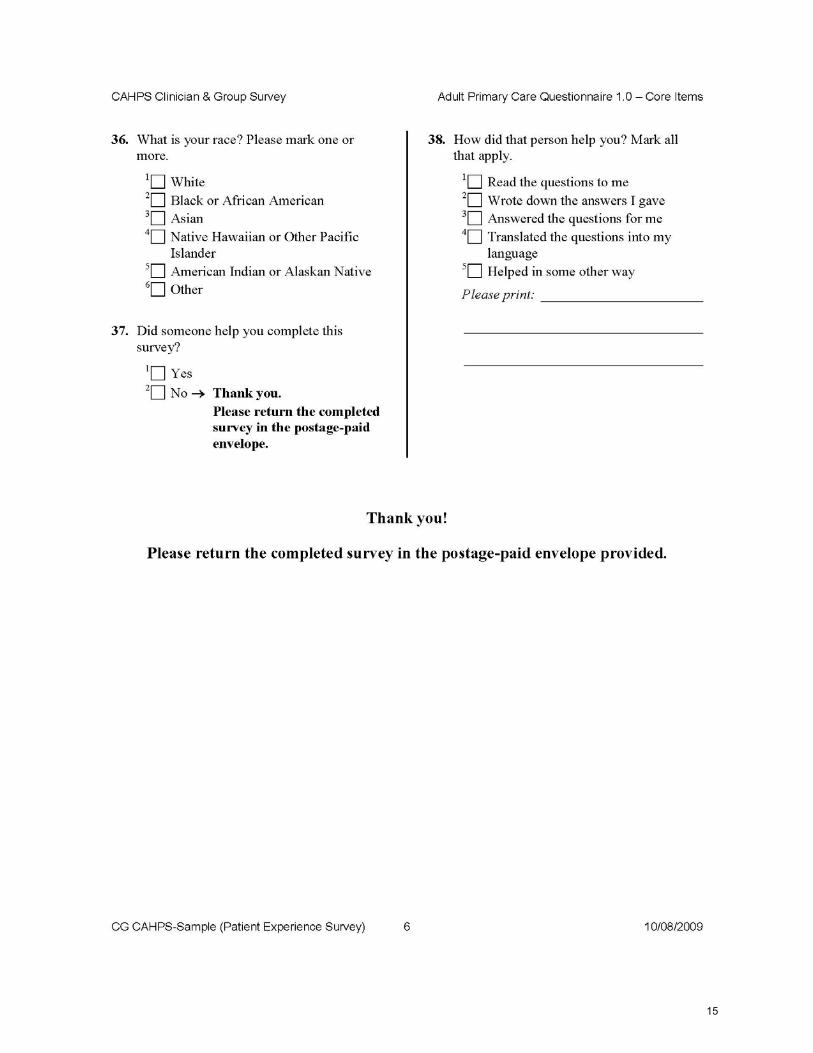
Patient Experience Patient experience improvement will be measured with a survey that assesses patients'
experiences with physicians and their office staff. Provided by the Agency for Healthcare Research and Quality (AHRQ), the survey instrument will be the Clinician & Group Consumer Assessment of Healthcare Providers and Systems (CAHPS). The CAHPS survey questions are provided at the end of this section. In order to meet the survey guidelines, we will need to send this survey to 1, 500 of your patients to ensure we meet the survey guideline of a 300 completion rate. The Patient Experience Survey will be given to a random sample of 1,500 patients who meet the following criteria:
• Age 18 years or older • Had at least one visit within the last 12 months
In order to select the sample for this survey, we will use the patient ID list previously requested. Please proceed with that submission if you have not yet completed it. Selected patients will receive a survey packet that includes a cover letter from their primary care practice, the Patient Experience Survey (CAHPS) and a return envelope (postage included). A second mailing will be conducted based on the survey return rate. Please see Attachment D to review the sample CAHPS cover letter. In addition, completed surveys will be mailed to an Access HealthColumbus P.O. Box. We have created a P.O. Box address specifically for your patients’ survey results. Your P.O. Box address that will be on main and return envelope is:
Primary Care Practice Site
CAHPS Survey Results P.O. Box 16190
Columbus, OH 43934
See below for the CAHPS survey questions:
9
10

11
12

13

14
15

Patient-Centered Primary Care Improvement Dashboard -- Diabetes
The current Dashboard example and measure descriptions for the Process & Outcome
Improvements for patients with Diabetes are outlined on the following two pages.
This document also expands on some specifics in support of the sampling process and sourcing of
the data (see last page, added 04/14/2011).
16
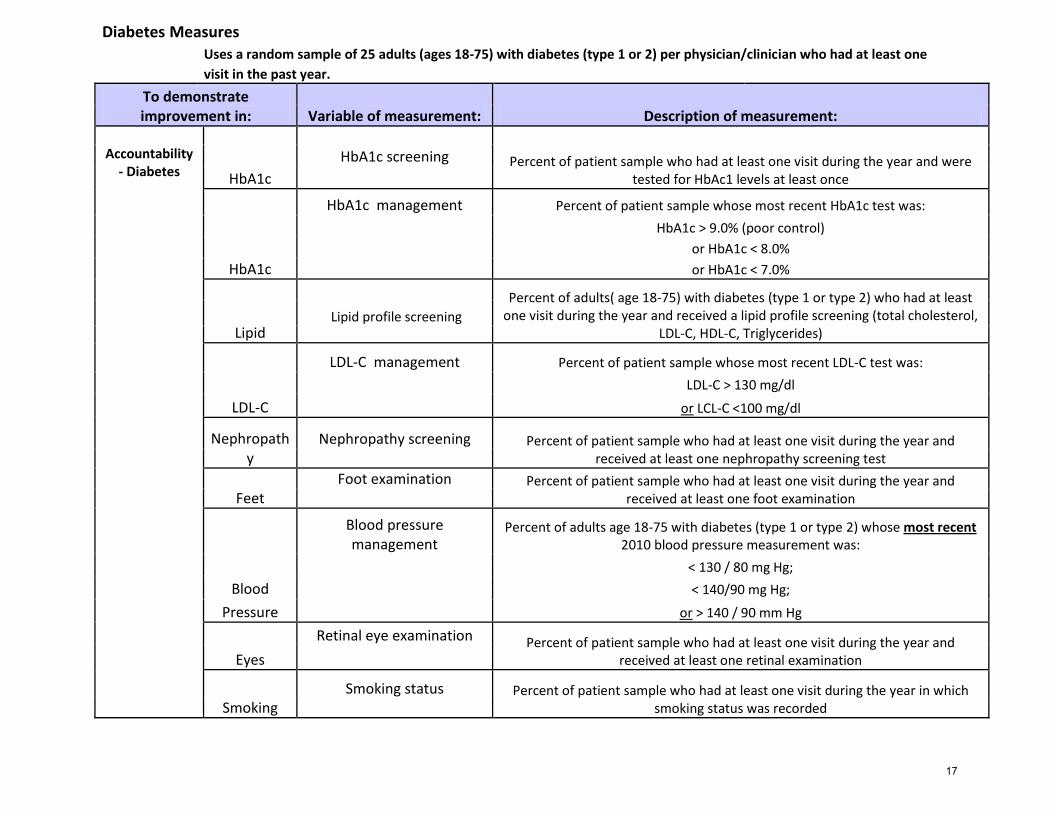
Diabetes Measures
Uses a random sample of 25 adults (ages 18-75) with diabetes (type 1 or 2) per physician/clinician who had at least one
visit in the past year.
To demonstrate improvement in: Variable of measurement: Description of measurement:
Accountability
- Diabetes
Percent of patient sample who had at least one visit during the year and were tested for HbAc1 levels at least once HbA1c
HbA1c screening
HbA1c management Percent of patient sample whose most recent HbA1c test was:
HbA1c > 9.0% (poor control)
or HbA1c < 8.0%
HbA1c or HbA1c < 7.0%
Lipid
Percent of adults( age 18-75) with diabetes (type 1 or type 2) who had at least one visit during the year and received a lipid profile screening (total cholesterol,
LDL-C, HDL-C, Triglycerides) Lipid profile screening
LDL-C management Percent of patient sample whose most recent LDL-C test was:
LDL-C > 130 mg/dl
LDL-C or LCL-C <100 mg/dl
Nephropathy
Nephropathy screening Percent of patient sample who had at least one visit during the year and received at least one nephropathy screening test
Feet Foot examination Percent of patient sample who had at least one visit during the year and
received at least one foot examination
Blood pressure management
Percent of adults age 18-75 with diabetes (type 1 or type 2) whose most recent 2010 blood pressure measurement was:
< 130 / 80 mg Hg;
Blood
< 140/90 mg Hg;
Pressure or > 140 / 90 mm Hg
Eyes
Retinal eye examination Percent of patient sample who had at least one visit during the year and received at least one retinal examination
Smoking Smoking status Percent of patient sample who had at least one visit during the year in which
smoking status was recorded
17

Expanded descriptions, 04/14/2011 Expanded descriptions in support of patient sampling and sourcing of the Diabetes Measures data. Dates of Service The services’ and outcomes’ dates of service should be within the 12 month Patient Visit Period that was used for the Patient ID list that was used for the sampling. Kyrsten Chambers will track and provide that time period for each practice supported by Access HealthColumbus’ chart review. Nephropathy Screening Should include one of three methods: Microalbuminuria test OR Positive urinalysis for protein (microalbuminuria) test OR Medical attention for nephropathy. Foot Examination Foot examination with shoes and socks removed. Retinal Eye Examination Retinal eye examination with documentation of date. If identified with chart review, will identify: yes, with report OR yes, no report OR no
18

Patient Centered Medical Home Improvement DashboardPractice & Patient Sourced ElementsAccess & Surveys
AccessBaseline: 4th quarter 2010 provided by 2/28/2010Ongoing Updates: quarterly, provided 30 days after end of quarter
Personal physician/cli
nician
Visits scheduled with assigned personal physician/clinician
(Continuity of Care)
Percent of appointments in which patients were seen by his/her Physician/Clinician of
Record
Three months' average of percentages from 1 week in each month: ( # patients seen by Physician/Clinician of Record / #
of patients seen)
To demonstrate improvement in: Variable of measurement: Description of measurement: Specifics/Formulas
AccessDaily Access
Capacity to schedule same day appointments
Average percent of appointments available at the beginning of each work day
Three months' average of percentages from 1 week in each month: ( # urgent
(aka blocked) appts beginning of days / # potential appts for the days)
19

Patient Centered Medical Home Improvement DashboardPractice & Patient Sourced ElementsData Summary Example -- 4q10 Physician/Clinician: John Jones, M.D.
Access# Description Format Example
1 Week beginning 2nd Monday of the month YYYYMMDD 20101011
2 # urgent appointments beginning of the days of the week Number 30
3 Potential appointments for the week Number 300
4 Week beginning 2nd Monday of the month YYYYMMDD 20101108
5 # urgent appointments beginning of the days of the week Number 33
6 Potential appointments for the week Number 350
7 Week beginning 2nd Monday of the month YYYYMMDD 20101213
8 # urgent appointments beginning of the days of the week Number 34
9 Potential appointments for the week Number 323
10 Week beginning 2nd Monday of the month YYYYMMDD 20101011
11 # patients seen by Physician of Record Number 150
12 # patients seen by the practice Number 290
13 Week beginning 2nd Monday of the month YYYYMMDD 20101108
14 # patients seen by Physician of Record Number 168
15 # patients seen by the practice Number 325
16 Week beginning 2nd Monday of the month YYYYMMDD 20101213
17 # patients seen by Physician of Record Number 179
18 # patients seen by the practice Number 318
Capacity to schedule same day appointments
Visits scheduled with assigned physician (Continuity of Care)
20
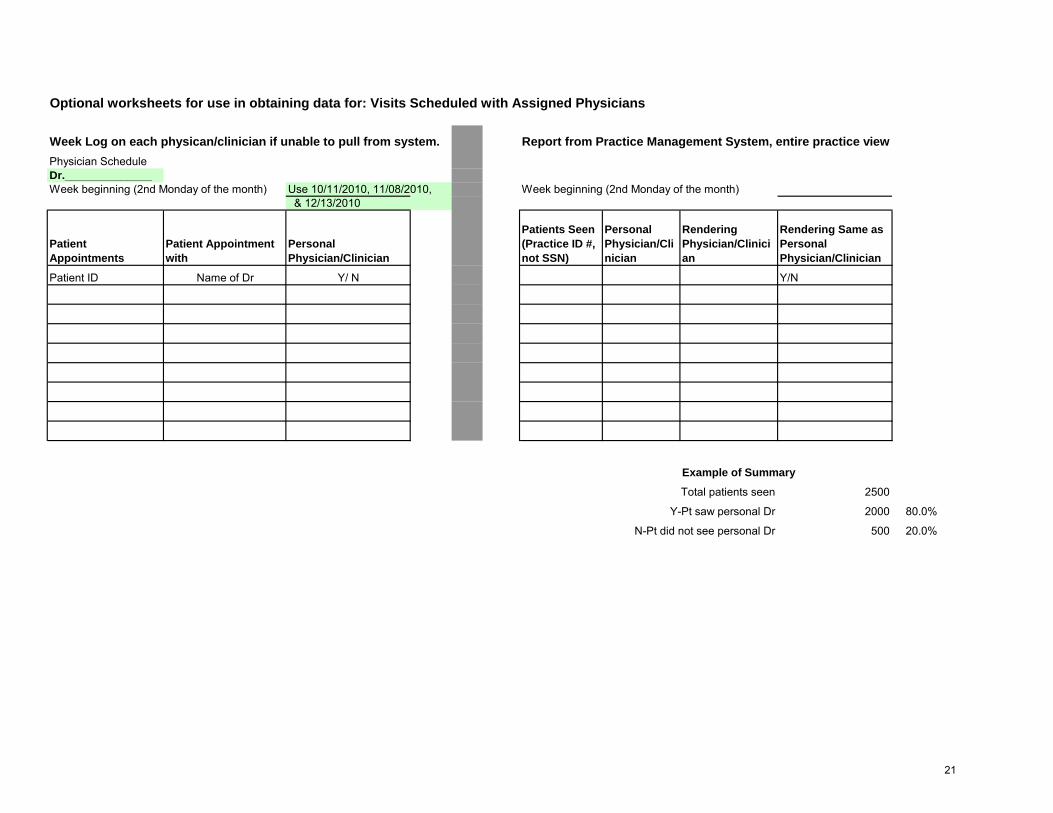
Optional worksheets for use in obtaining data for: Visits Scheduled with Assigned Physicians
Week Log on each physican/clinician if unable to pull from system. Report from Practice Management System, entire practice viewPhysician ScheduleDr.______________Week beginning (2nd Monday of the month) Use 10/11/2010, 11/08/2010, Week beginning (2nd Monday of the month)
& 12/13/2010
Patient Appointments
Patient Appointment with
Personal Physician/Clinician
Patients Seen (Practice ID #, not SSN)
Personal Physician/Clinician
Rendering Physician/Clinician
Rendering Same as Personal Physician/Clinician
Patient ID Name of Dr Y/ N Y/N
Example of Summary
Total patients seen 2500
Y-Pt saw personal Dr 2000 80.0%
N-Pt did not see personal Dr 500 20.0%
21

Optional worksheet for use in obtaining data for: Capacity to schedule same day appointments
Physician# Total Appt
# Urgent Appts
Blocked Physician# Total Appt
# Urgent Appts
Blocked Physician# Total Appt
# Urgent Appts
Blocked Physician# Total Appt
# Urgent Appts
Blocked Physician# Total Appt
# Urgent Appts
Blocked Physician# Total Appt
# Urgent Appts
Blocked
Dr A 24 20 Dr A 24 0 Dr A 24 0 Dr A 24 0 Dr A 24 0 Dr A 120 20 17%
Dr B 24 0 Dr B 24 20 Dr B 24 0 Dr B 24 0 Dr B 24 0 Dr B 120 20 17%
Dr C 24 0 Dr C 24 0 Dr C 24 20 Dr C 24 0 Dr C 24 0 Dr C 120 20 17%
Dr D 12 0 Dr D 12 0 Dr D 12 0 Dr D 12 10 Dr D 12 10 Dr D 60 20 33%
Dr E 12 0 Dr E 12 0 Dr E 12 0 Dr E 12 10 Dr E 12 10 Dr E 60 20 33%
Total Phys = 5 96 20
Total Phys = 5 96 20
Total Phys = 5 96 20
Total Phys = 5 96 20
Total Phys = 5 96 20
Total Phys = 5 480 100
21% 21% 21% 21% 21% 21%
480 Total number of appointments for the week
100 Total Number of Appointments Blocked for the week
21% % Capacity --Access for patient to be seen the same day
Total
Accessibility
% Available AppointmentsWeek beginning (2nd Monday of the month) xx/xx/xxxx (Use 10/06/2010, 11/08/2010, & 12/06/2010)
Monday Tuesday Wednesday Thursday Friday
Example - urgent doc floats Results are based upon the physicians who are scheduled in the office each day.
22
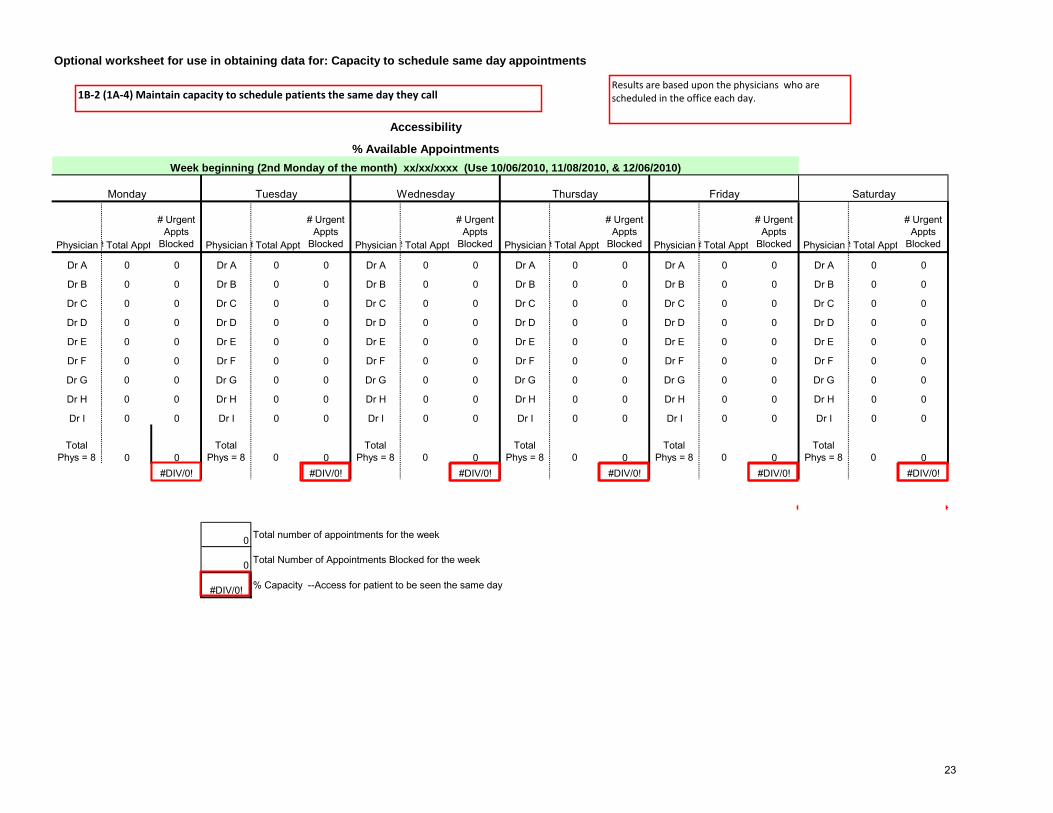
Optional worksheet for use in obtaining data for: Capacity to schedule same day appointments
Physician# Total Appt
# Urgent Appts
Blocked Physician# Total Appt
# Urgent Appts
Blocked Physician# Total Appt
# Urgent Appts
Blocked Physician# Total Appt
# Urgent Appts
Blocked Physician# Total Appt
# Urgent Appts
Blocked Physician# Total Appt
# Urgent Appts
Blocked
Dr A 0 0 Dr A 0 0 Dr A 0 0 Dr A 0 0 Dr A 0 0 Dr A 0 0
Dr B 0 0 Dr B 0 0 Dr B 0 0 Dr B 0 0 Dr B 0 0 Dr B 0 0
Dr C 0 0 Dr C 0 0 Dr C 0 0 Dr C 0 0 Dr C 0 0 Dr C 0 0
Dr D 0 0 Dr D 0 0 Dr D 0 0 Dr D 0 0 Dr D 0 0 Dr D 0 0
Dr E 0 0 Dr E 0 0 Dr E 0 0 Dr E 0 0 Dr E 0 0 Dr E 0 0
Dr F 0 0 Dr F 0 0 Dr F 0 0 Dr F 0 0 Dr F 0 0 Dr F 0 0
Dr G 0 0 Dr G 0 0 Dr G 0 0 Dr G 0 0 Dr G 0 0 Dr G 0 0
Dr H 0 0 Dr H 0 0 Dr H 0 0 Dr H 0 0 Dr H 0 0 Dr H 0 0
Dr I 0 0 Dr I 0 0 Dr I 0 0 Dr I 0 0 Dr I 0 0 Dr I 0 0
Total Phys = 8 0 0
Total Phys = 8 0 0
Total Phys = 8 0 0
Total Phys = 8 0 0
Total Phys = 8 0 0
Total Phys = 8 0 0
#DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0!
0 Total number of appointments for the week
0 Total Number of Appointments Blocked for the week
#DIV/0! % Capacity --Access for patient to be seen the same day
Saturday
Accessibility
% Available AppointmentsWeek beginning (2nd Monday of the month) xx/xx/xxxx (Use 10/06/2010, 11/08/2010, & 12/06/2010)
Monday Tuesday Wednesday Thursday Friday
1B-2 (1A-4) Maintain capacity to schedule patients the same day they call Results are based upon the physicians who are scheduled in the office each day.
23

Note: Your Privacy is Protected. All information that would let someone identify you or your family will be kept private. Your responses
to this survey are also completely confidential. Your Participation is Voluntary. You may choose to answer this survey or not. If
you choose not to, this will not affect the health care you get.
[Insert PO Box Practice Name Here]
PAM Survey Results
P.O. Box 16897
Columbus, OH 43216
Dear Valued Patient: We at [PRACTICE NAME] would like to learn more about how our patients feel about managing their own health care. Our records indicate that you have visited us in the last 12 months, and you have been randomly selected to complete a brief survey. This survey will only take 3-4 minutes to complete. The survey includes questions that ask you what you think and feel when dealing with your health. Often people are tempted to answer these questions in a way that they think will please the nurses and doctors. Please do not do this. We need to know how you honestly think and feel when dealing with your health. This information will help us understand if we are providing care that enhances our patients’ confidence in managing their health. Enclosed in this packet you will find a Patient Activation Measure (PAM) survey. The information that you provide will be kept completely private and confidential. Your individual answers will never be seen by your doctor or anyone else involved with your care.
Please return the completed survey in the enclosed postage-paid envelope by [2 weeks from sent date]. We hope you will participate in our survey!
If you have any questions about this survey, please call [CONTACT NAME] at (XXX) [XXX-XXXX].
Sincerely,
[Insert ALL practice provider names here]
24

Note: Your Privacy is Protected. All information that would let someone identify you or your family will be kept private. Your responses
to this survey are also completely confidential. You may notice a number on the cover of the survey. This number is used only to let us
know if you returned your survey so we don’t have to send you reminders. Your Participation is Voluntary. You may choose to
answer this survey or not. If you choose not to, this will not affect the health care you get.
[Insert PO Box Practice Name Here]
CAHPS Survey Results
P.O. Box 16896
Columbus, OH 43216
Dear Valued Patient: We at [PRACTICE NAME] need your help! Our records indicate that you have visited us in the last 12 months, and we would like you to tell us about your experiences over the last year. We are committed to providing you with the best quality health care available, and your input will help us to achieve this goal.
Enclosed this packet you will find a Patient Experience Survey. This survey should only take about 10 minutes or less of your time. The information that you provide will be kept completely private and confidential. Your individual answers will never be seen by your doctor or anyone else involved with your care.
We hope you will take this chance to tell us about your experiences with our practice. Please return the completed survey in the enclosed postage-paid envelope by [2 weeks from sent date].
If you have any questions about this survey, please call [CONTACT NAME] at (XXX) [XXX-XXXX]. Thank you for helping to make health care at [PRACTICE NAME] better for everyone!
Sincerely,
[Insert ALL providers names here]
25