personality disorders in a hospital setting. personality the totality of emotional and behavioral...
TRANSCRIPT
Personality Disordersin a Hospital Setting

Personality
The totality of emotional and behavioral traits characterizing a person’s day-to-day living.
Relatively stable and predictable under ordinary conditions
Personality Disorders
• Inflexible, maladaptive, exaggerated traits
• Pattern of behavior deeply ingrained and maladaptive in perceiving self, others, environment
DSM-IV-TR
Axis I
Major mental disorder
Axis II
Personality disorders
Cluster A, B, C
Cluster A
• Paranoid
• Schizoid
• Schizotypal
Cluster B
•Antisocial
•Borderline
•Histrionic
•Narcissistic

Cluster C
• Avoidant
• Dependent
• Obsessive-compulsive
• Not Otherwise Specified (NOS)
Personality Disorder Classification Controversial, Problematic
• Diagnostic unreliability• Preferential personality (co-existing conditions?)• Shared characteristics (excessive number of
PDs)• Heterogeneity • Inconsistent, unstable, arbitrary boundaries• Inadequate literature coverage• Too frequent use of NOS category
Proposal 1
Dimensional profile: narrative description of case, not only diagnostic classification, identifying fundamental maladaptive personality traits underlying its functioning
Proposal 2
Integrate the various personality disorders into Axis I diagnostic classification: e.g.,
depressive personality disorder will change to dysthymia, early onset.
Factors in behavior
Genetic, temperamental, biological, psychological factors determine reaction of an individual towards others and environment throughout life and help form a pattern of behaviors typical for the individual.
Defense Mechanisms
Unconscious mental processes that the ego (self) employs to free itself from conscious anxiety generated during interactions with others, its own instincts, reality, conscience
Used to avoid an increase in conscious anxiety and/or depression
Defense Mechanism Types• Fantasy• Dissociation• Denial• Isolation• Projection• Splitting• Passive-Aggressive• Acting out• Projective identification
Fantasy
•Fear of intimacy
•Schizoid behavior
•Aloofness
•Loneliness
•Creating imaginary life, companions
Fears should be recognized in a reassuring, non-confrontational, not insistent manner.
Denial - Dissociation
Unconscious covers-up for anxiety/other unpleasant emotions (e.g., fear) via exhibiting histrionic superficiality.Makes little of problems.May not remember important events of life and medical history.
Caution to not make them more defensiveCaution in not accepting histrionics at face valueAllow to ventilate feelings and anxiety

Isolation
• Obsessive-compulsive• Orderly• Relates well• Tells unnecessary details about self in cool collected manner
Responds well to precise, systematic, rational information.Wants punctuality.Demands interest from physician, others.Often intelligent, able to control own care.
Projection
• Attribution of own feelings to others• Fault-finding• Prejudicial• Hyper-vigilant• Distrustful
Avoid confrontation. Normal but concerned approach. May be useful to establish alliance and expose him/her to interpretations of other reasons for suspiciousness.
Splitting
• Divides people into good and bad
• Some staff members may be idealized
• Some staff members disparaged
• Disruptive behavior
Gentle confrontation – no one is totally good or bad.

Passive-Aggression
• Anger turned against self (masochism)
• Shows as self-demeaning or self-destructive behavior (wrist-cutting)
• Hostility may be part of provocative behavior
• Often viewed as sadistic
Allow ventilation of anger.
Acting Out (I)
• Tantrums• Expression of ambivalent feelings
conscious or unconscious• Assaults without motivation, at times sudden• Different types of abuse (physical, sexual,
adults, children)• At times no apparent guilt feelings• Homicide may take place in uncontrolled
aggression

Acting Out (II)
Interviewer must be calm, good listener. Realize patient lost control and is agitated.
How can I help if you keep screaming or being so upset?
Projective Identification
• Mainly present in Borderline Personality Disorder
Aspect of self projected onto other.
Coercion of the other to identify with the projected aspect.
Projector and recipient feel some kind of union.

Paranoid Personality Disorder (I)
• Frequency – 0.5-2.5%• Referrals from spouse, family, employer• More frequent in men• Higher in immigrants• Higher in deaf• Appears serious, humorless, suspicious • Speech logical but with false premises• Prejudice, projection, ideas of reference
Paranoid Personality Disorder (II)
• Fear of exploitation• Jealous• Disdains weak and impaired• Businesslike, efficient• Questions trustworthiness of friends
A chronic condition that poses difficulty in living with spouse, friends, co-workers.
Schizoid Personality Disorder (I)
About 7.5% of populationSocial withdrawalDiscomfort in relating to peopleIntroversionConstricted affectIsolatedLonelyPrefers solitary job, also at night
Schizoid Personality Disorder (II)
• Avoids eye contact• Fearful• Short answers• Minimal spontaneous speech• Flattened affect• Unable to relate• Lives in fantasy world• Repressed intimacy and sexuality
Schizoid Personality Disorder (III)
• Unable to express anger• Pseudo-philosophizes• Excessive day-dreaming
Good patients in hospital who, absorbed in self, need protection from other patients (dyscontrolled or paranoid). If staff is able to establish rapport, they will uncover a plethora of day-dreaming.

Schizotypal Personality Disorder
• 3% of general population
• Odd, strange magical thinking
• Ideas of reference
• Illusions
• Peculiarity of thinking, behavior, appearance
• 10% commit suicide
Antisocial Personality Disorder (I)
• 3% male – 1 % female• Nonconforming• Antisocial• Criminal behavior• Callous• Remorseless• Prone to lying, irritability, rage• Conduct disorder in childhood
Antisocial Personality Disorder (II)
• May have a veneer of normality, seductiveness
Must be dealt with firmness and by establishing clear staff-patient rapport.

Borderline Personality Disorder (I)
• Previously called Ambulatory Schizophrenia, Psychotic Character, or Pseudoneurotic Schizophrenia
• 1-2% of general population
• More common in women
• Unable to establish lasting relationships
• Love-hate tendencies
• Fluctuation of mood
Borderline Personality Disorder (II)
• Proclivity to move into psychosis under intense stress
• Always in a state of crisis
• Argumentative, depressed
• No feelings
• Micropsychotic episodes
• Unpredictable Behavior

Borderline Personality Disorder (III)
• Repetitive self-destructive acts
• Self-mutilation- expresses anger
Do well in hospital setting because of attention received, avoiding intrafamilial problems. Limits posed to behavior (self-destructive acts) in a supervised protected environment. Suicide attempts frequent.
Histrionic Personality Disorder (I)
• 2-3% of general population• More frequent in women• Found especially in mental institutional settings• Colorful• Extroverted• Dramatic behavior• Excitable• Flamboyant
Histrionic Personality Disorder (II)
• Attention-seeking• Frequently somatize • Use drugs/alcohol• Gesturing• Eager to express and communicate in
colorful way• Some tangentiality and forgetfulness• Magnify importance of events
Histrionic Personality Disorder (III)
• Mood swings and tears to make point
• Seductive, flirtatious, inconsistent
• Sensation seeking
• May get into trouble with law
Narcissistic Personality Disorder (I)
• 1% of general population• Larger number in clinical setting• Exaggerated sense of self-importance• Enraged by criticism or completely ignores
it• Ambitious• Continuous search for recognition• Needs reassurance

Narcissistic Personality Disorder (II)
• Superficial relationships• No empathy• Cunning and exploitative• Fragile self-esteem• May become depressed• Often rejected because of behavior
Need structured firmness, clear understanding of procedures.
Avoidant Personality Disorder (I)
• 1-2% of general population• Sensitive to rejection• Lonely• Very timid• Inferiority feelings• Anxious/tense• Need acceptance• Vulnerable to comments about self
Avoidant Personality Disorder (II)
• Misperceives interviewing statements
• Needs and wants companionship
• May express fears of rejection
• Phobic avoidance
Should be approached with friendly acceptance, made to feel wanted and appreciated.
Dependent Personality Disorder (I)
• Lack of self-confidence• Relies on others• Does not assume responsibility• Passive, pessimistic, suggestible• Lack emotional endurance• Submissive• Fear of expressing sexual/aggressive
feelings
Dependent Personality Disorder (II)
• Unable to make decisions on their own
• Subject to abuse by others
Patient should be told what has to be done. Should undergo behavior and assertiveness therapy/training.
Obsessive-Compulsive Personality Disorder (I)
• Perfectionist• Obsessed with orderliness• Obsessive thoughts• Affect constricted• Stiff, formal, rigid, stubborn• Anal stage of development• Want to be in control• Detailed answers when interviewed
Obsessive-Compulsive Personality Disorder (II)
• Rationalization
• Intellectualizations
• Doing-undoing/ritualistic behavior
Should be dealt with in matter-of-fact, rigid routine and a formal relationship.

Personality Disorder NOS
• Passive-aggressive
• Depressive
• Sado-masochistic
• Sadistic
Personality Changes due to a General Medical Condition
Significant changes of habitual pattern of premorbid behavior
ICD-10 Personality and Behavioral Disease due to:
Brain diseaseBrain damageBrain dysfunctionPost-encephalopathy SyndromePost-concussion Syndrome
Personality Changes due to a Medical Condition (I)
• Head trauma
• Cerebrovascular disease
• Cerebral tumor
• Epilepsy (partial complex epilepsy)
• Huntington’s Disease
• Multiple Sclerosis
• Endocrine disorders

Personality Changes due to a Medical Condition (II)
• Heavy metal poisoning (manganese, mercury)
• Neurosyphillis
• Acquired Immune Deficiency Syndrome (AIDS)
Organic Personality DisorderDiagnostic Criteria (I)
• Alteration of habitual pattern of behavior
• Emotions, impulses and needs are affected
• Defective cognitive function
consequences of actions/planning
Organic Personality DisorderDiagnostic Criteria (II)
• Perseverance in goal-directed activity reduced
• Unable to postpone gratification
• Emotional lability
• Euphoria, inappropriate jocularity
• Sudden shift from cheerfulness to irritability
• Outbursts of anger and aggression
Organic Personality DisorderDiagnostic Criteria (III)
• Apathy
• Impulsive actions w/ caring for consequences (stealing, sexual exposure/ advances, etc.)
• Suspiciousness
• Paranoid ideation, preoccupation (extreme) with religious or abstract themes
• Circumstantiality, viscosity
Organic Personality DisorderDiagnostic Criteria (IV)
• Alters sexual behavior
• Possibly violent behaviors, especially if intoxicated
Anabolic steroids (used to maximize muscle strength) may cause a persistent alteration of personality and behavior.

In dementia there is a global deterioration in intellectual and behavioral capacities.
Personality changes in brain tumor, multiple sclerosis, Huntington’s Disease may evolve into dementia.

In general medical conditions personality changes show with:
• Cognitive disorder with significant memory loss, confusion, at times eventuating in dementia.
• Changes persist if cause persists.• Trauma followed by coma.• Delirium due to vascular accident
Personality changes in chronic intoxication, medical illness, drug therapy (levodopa for Parkinson’s Disease) may be reversed if cause is eliminated.
Some patients need custodial care.
Caution! Behavioral Dyscontrol

Neuroimaging Studies
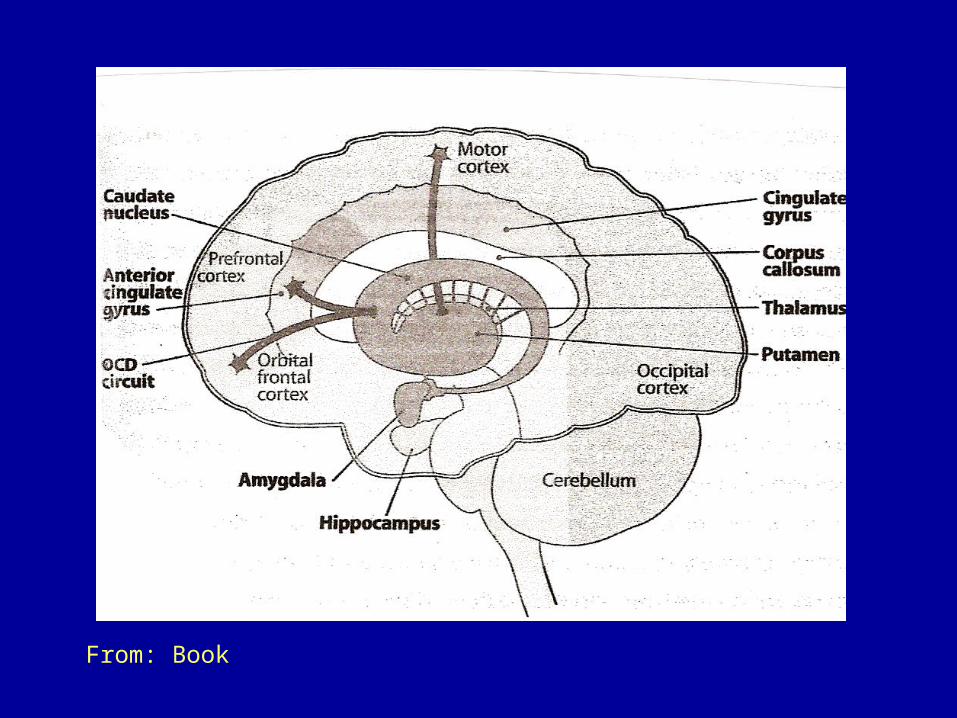
From: Book
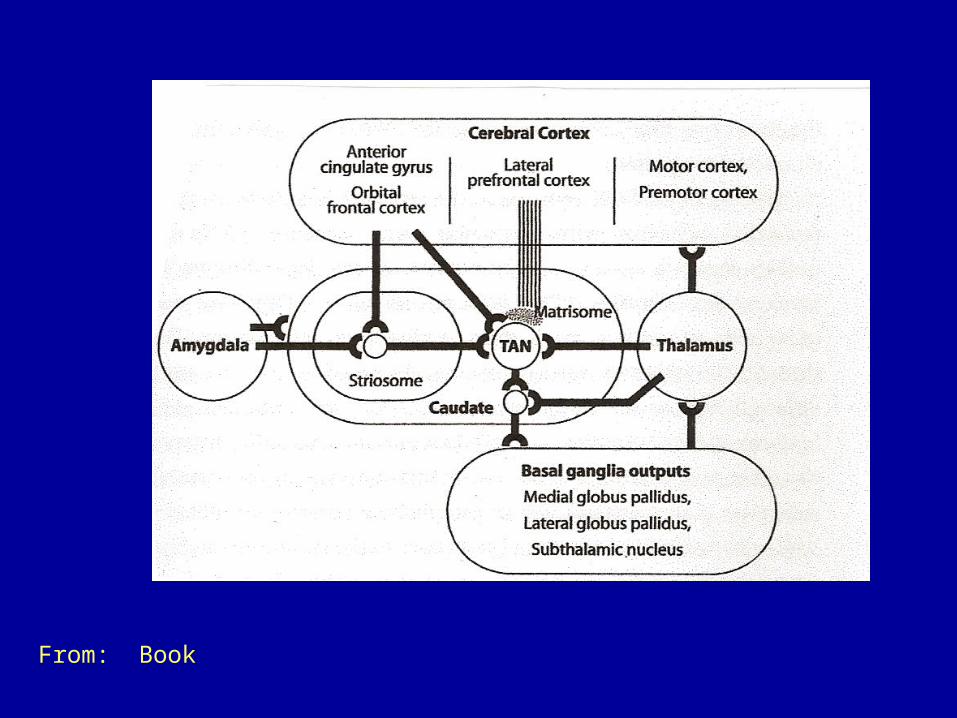
From: Book

Neuroimaging Studies• MRI
• CT scans
• PET-SPECT
Minimal cortical atrophy, dilatation of lateral ventricles, hypermetabolism of basal ganglia
Schizotypal Personality DisorderCluster A
• Larger ventricles (lateral)
• Smaller caudate and left hippocampus
• Larger hippocampus (R)
• Reduced prefrontal regions
• Decrease perfusion basal ganglia and thalamus
Borderline Personality Disorder (BPD)
Cluster B
Disinhibited aggression and affective instability associated with deficient top-down control of negative emotions

BPD: Impulsive aggression due to high level of anger
ASPD: Aggressive behavior associated with less anger-stimulation and/or gain

Emotional Modulation Circuit (I)
• ACC (anterior cingulate cortex)
• OFC (orbital frontal cortex)
• VMC (ventromedial prefrontal cortex)
• DLPFC (dorso-lateral prefrontal cortex)
Emotional Modulation Circuit (II)
OFC (orbital frontal cortex)
ACC ( anterior cingulate cortex)
OFC and ACC interact to modulate response of amygdala

BPDStructural and Functional Studies
• Smaller total frontal lobe volumes
• Reduction in gray matter volume
• Reduction in neural density (reduction of acetylaspartate in DLPFC [dorsolateral prefrontal cortex])
• Questionable volume reduction of amygdala
• Decrease in volume of ACC and hippocampus
• Hyperactive amygdala?
• 5-HT diminished in aggressive impulsivityy

ASPD
• 20% may be psychopaths• Frontal regions in emotional tasks may
function insufficiently (relatively speaking), even though there is increased activation
• Questionable volume of amygdala• Affective memory tasks slow• Decreased activity in amygdala,
hippocampus, parahippocampus, ventral striatum, anterior-posterior cingulate gyrus
Fear-AnxietyCluster C
• Top-down control of subcortical network responding to fear and connected with memory
• Larger ACC ↔ higher score of Harm-Avoidance (HC)