physiology and pharmacology of gastric motility and gastric acid production professor john peters...
TRANSCRIPT
Physiology and Pharmacology of Gastric Motility and Gastric Acid production
Professor John PetersE-mail [email protected]
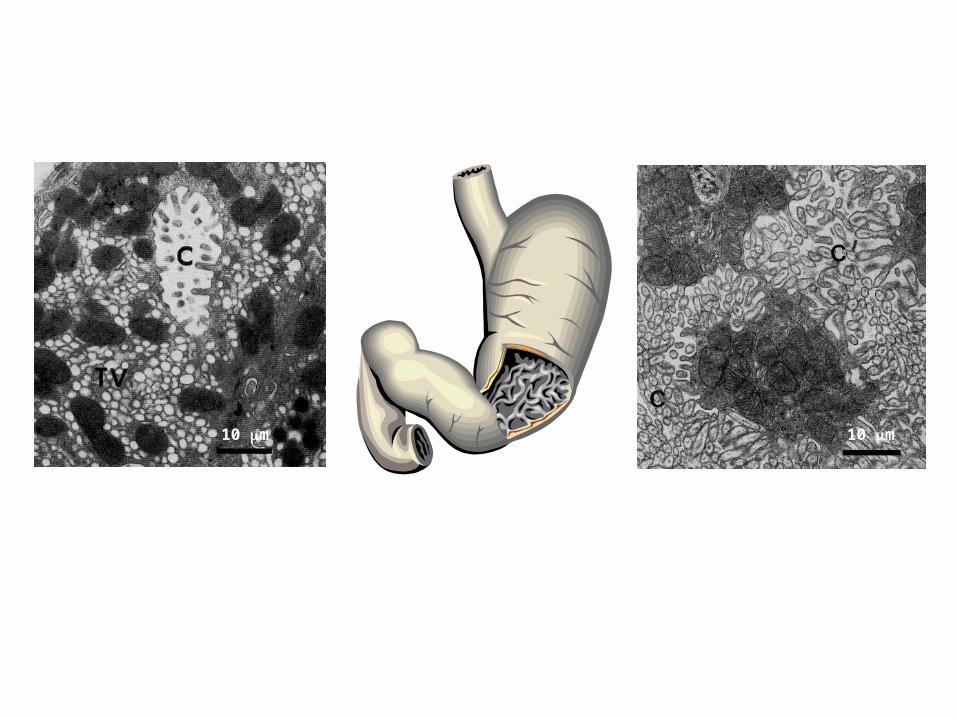
TEMs of resting (left) and stimulated (right) parietal cells from piglet stomach from: Handbook of Physiology – The Gastrointestinal System III (1989). Cell biology of hydrochloric acid secretion. Forte, J.G and Soll, A.
10 m10 m

Learning ObjectivesFollowing this lecture, students should be able to:
Draw a diagram showing how HCl is produced and how this is regulated
List the products of the gastric glands
Describe the 3 phases of gastric secretion and the nature of their controls
Describe the role of peristalsis and the pyloric sphincter in the controlled emptying of the stomach contents
State how emptying is affected by the volume and composition of the food in the stomach Appreciate the overall mechanism by which acetylcholine, histamine and gastrin enhance
the activity of the H+/K+ATPase (‘proton pump’) to promote the secretion of HCl Understand the importance of mucosal-protecting mechanisms in the prevention of ulcer
formation and how such defence may be compromised by NSAIDs and chronic infection of the gastric antrum with H. pylori
Understand how drug treatment aims to promote ulcer healing Appreciate how commonly prescribed drugs that suppress acid secretion [e.g. proton pump
inhibitors (PPIs) and H2 receptor antagonists] exert their actions noting any adverse effects
Appreciate the role of mucosal strengtheners and antacids in the treatment of peptic ulcer Be aware of combination therapies of antibiotics and PPIs in the treatment of peptic ulcer Give examples of drugs that are used to increase gastric motility and their uses
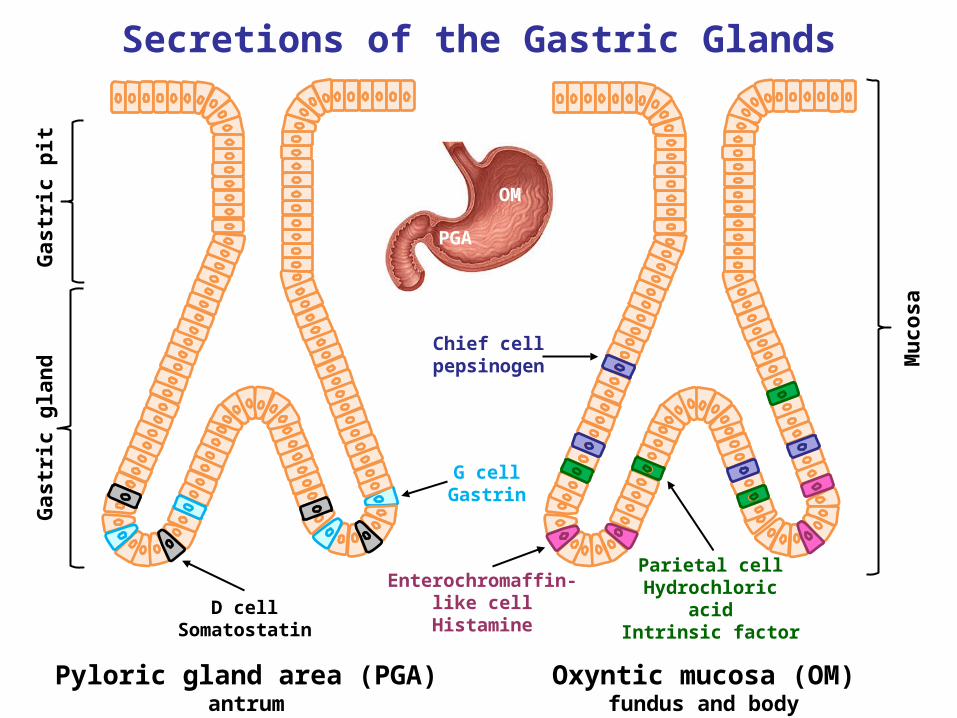
Secretions of the Gastric Glands
Chief cellpepsinogen
Gas
tric
pit
Gas
tric
gla
nd
Mu
cosa
Parietal cellHydrochloric acid
Intrinsic factor
Enterochromaffin-like cell
Histamine
G cellGastrin
D cellSomatostatin
Pyloric gland area (PGA)antrum
Oxyntic mucosa (OM)fundus and body
PGA
OM
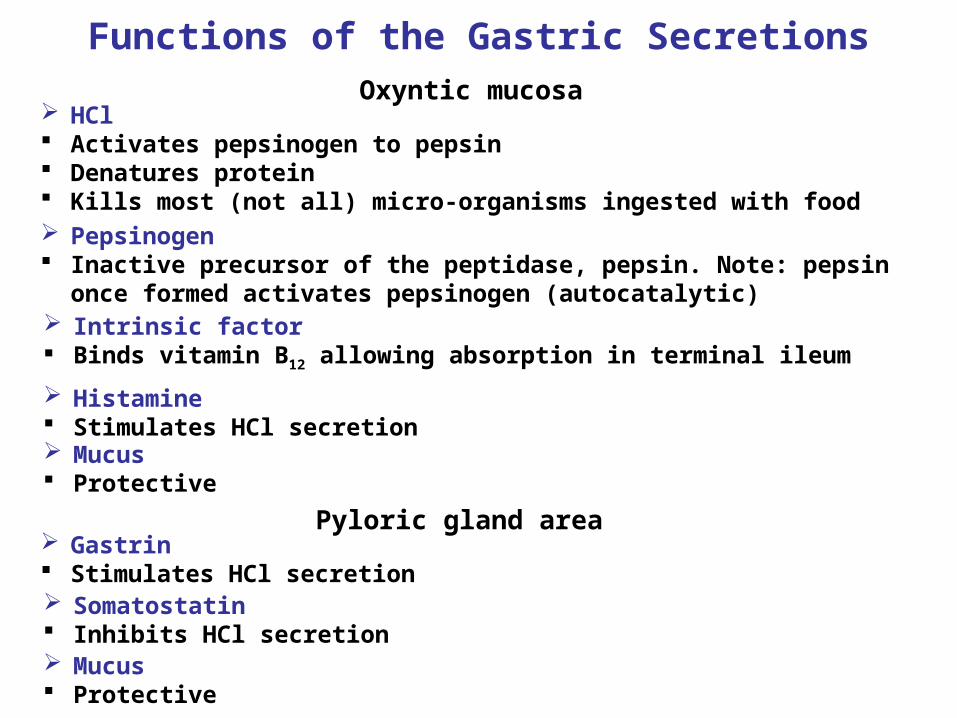
Functions of the Gastric SecretionsOxyntic mucosa
HCl Activates pepsinogen to pepsin Denatures protein Kills most (not all) micro-organisms ingested with food Pepsinogen Inactive precursor of the peptidase, pepsin. Note: pepsin once formed
activates pepsinogen (autocatalytic) Intrinsic factor Binds vitamin B12 allowing absorption in terminal ileum
Histamine Stimulates HCl secretion Mucus Protective
Mucus Protective
Pyloric gland area Gastrin Stimulates HCl secretion Somatostatin Inhibits HCl secretion
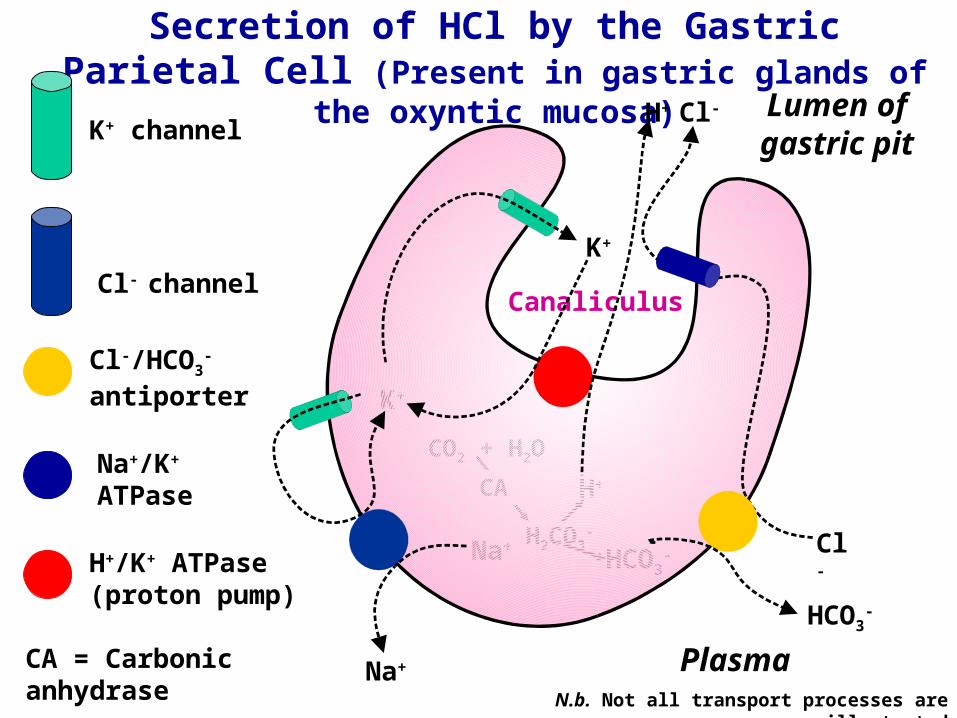
Secretion of HCl by the Gastric Parietal Cell (Present in gastric glands of the oxyntic
mucosa)
K+
K+
CO2 + H2O
HCO3-
H+
H2CO3-
CA
Na+
Na+
HCO3-
Cl-
Cl-H+
Plasma
Lumen of gastric pitK+ channel
Cl- channel
Cl-/HCO3-
antiporter
Na+/K+ ATPase
CA = Carbonic anhydrase
H+/K+ ATPase (proton pump)
N.b. Not all transport processes are illustrated
Canaliculus
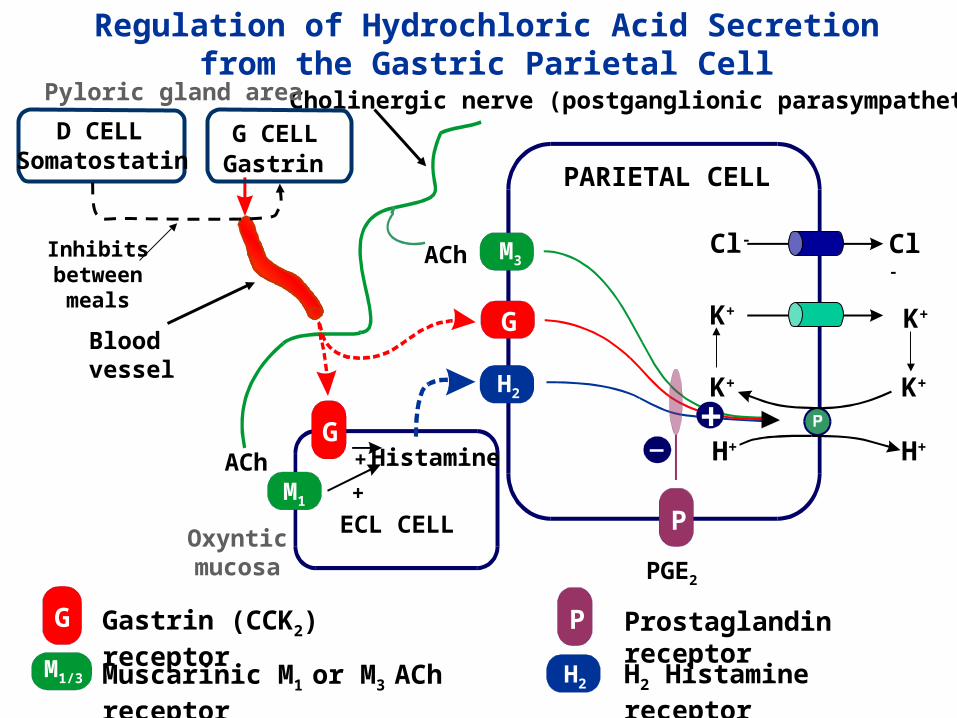
G Gastrin (CCK2) receptor
Muscarinic M1 or M3 ACh receptor H2 Histamine receptor
P Prostaglandin receptor
M1/3 H2
Regulation of Hydrochloric Acid Secretion from the Gastric Parietal Cell
PARIETAL CELL
ECL CELL
HistamineG
G
+
+
M3
GastrinG CELL
ACh
ACh
+
P
Blood vessel
Cholinergic nerve (postganglionic parasympathetic)
H2
M1
PGE2
Cl-Cl-
K+K+
H+H+
K+K+
Pyloric gland area
Oxyntic mucosa
D CELLSomatostatin
Inhibits between meals
G
M3
H2
G
M3
H2
H+
H+H+
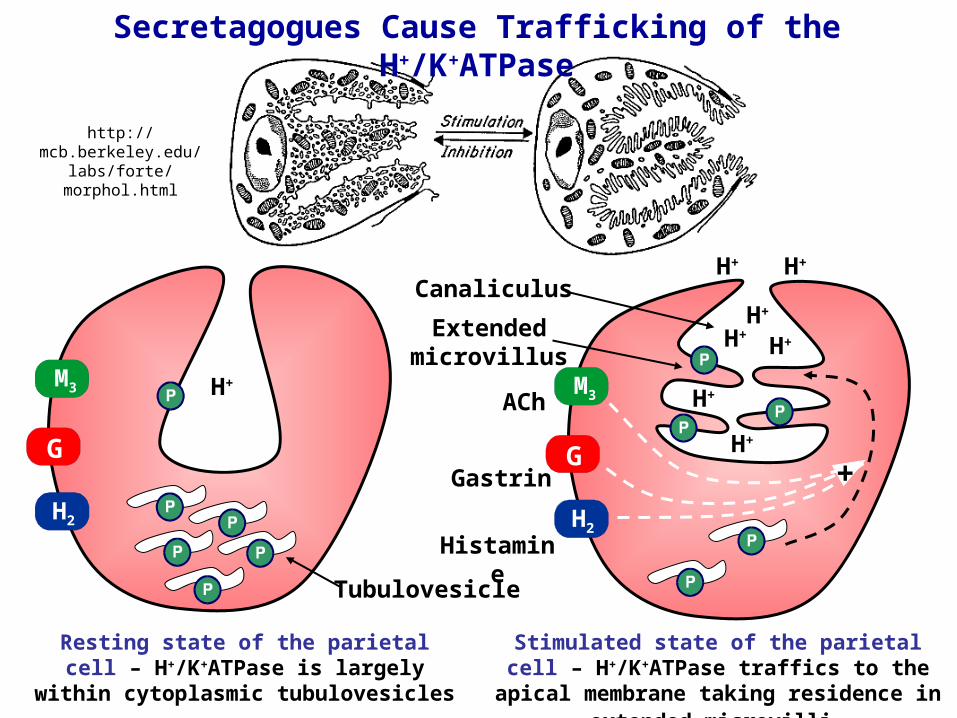
Resting state of the parietal cell – H+/K+ATPase is largely within cytoplasmic
tubulovesicles
Stimulated state of the parietal cell – H+/K+ATPase traffics to the apical membrane
taking residence in extended microvilli
ACh
Gastrin
Histamine
Tubulovesicle
Extended microvillus
+
Secretagogues Cause Trafficking of the H+/K+ATPase
H+
H+
H+H+
Canaliculus
H+
http://mcb.berkeley.edu/labs/
forte/morphol.html
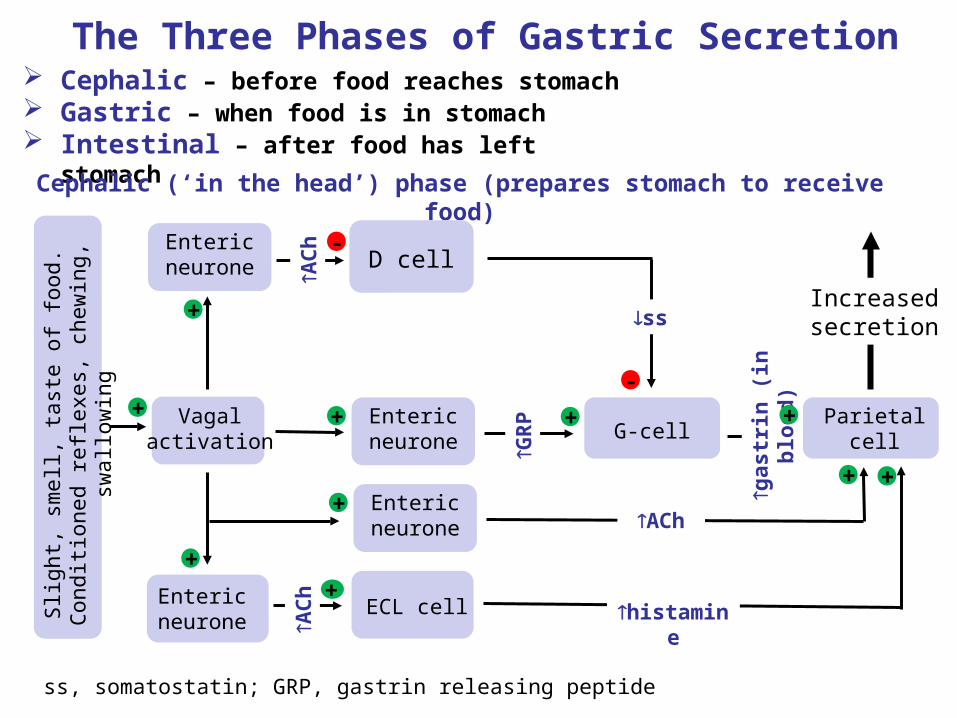
The Three Phases of Gastric Secretion Cephalic – before food reaches stomach Gastric – when food is in stomach Intestinal – after food has left stomach
Cephalic (‘in the head’) phase (prepares stomach to receive food)
Slig
ht, s
mel
l, ta
ste
of fo
od. C
ondi
tione
d re
flexe
s, c
hew
ing,
sw
allo
win
g
ECL cell
G-cell+
GR
P
D cell
AC
h -
-
ss
Parietal cell
+
histamine
+
gas
trin
(in
blo
od
)
+
Increased secretion
Vagal activation
+
Entericneurone
+
Entericneurone
++
Entericneurone
+
AC
h
ss, somatostatin; GRP, gastrin releasing peptide
Entericneurone
+ACh
Slig
ht, s
mel
l, ta
ste
of fo
od. C
ondi
tione
d re
flexe
s, c
hew
ing,
sw
allo
win
g
ECL cell
G-cell+
GR
P
D cell
AC
h -
-
ss
Parietal cell
+
histamine
+
gas
trin
(in
blo
od
)
+
Increased secretion
Vagal activation
+
Entericneurone
+
Entericneurone
++
Entericneurone
+
AC
h
ss, somatostatin; GRP, gastrin releasing peptide
Entericneurone+ ACh
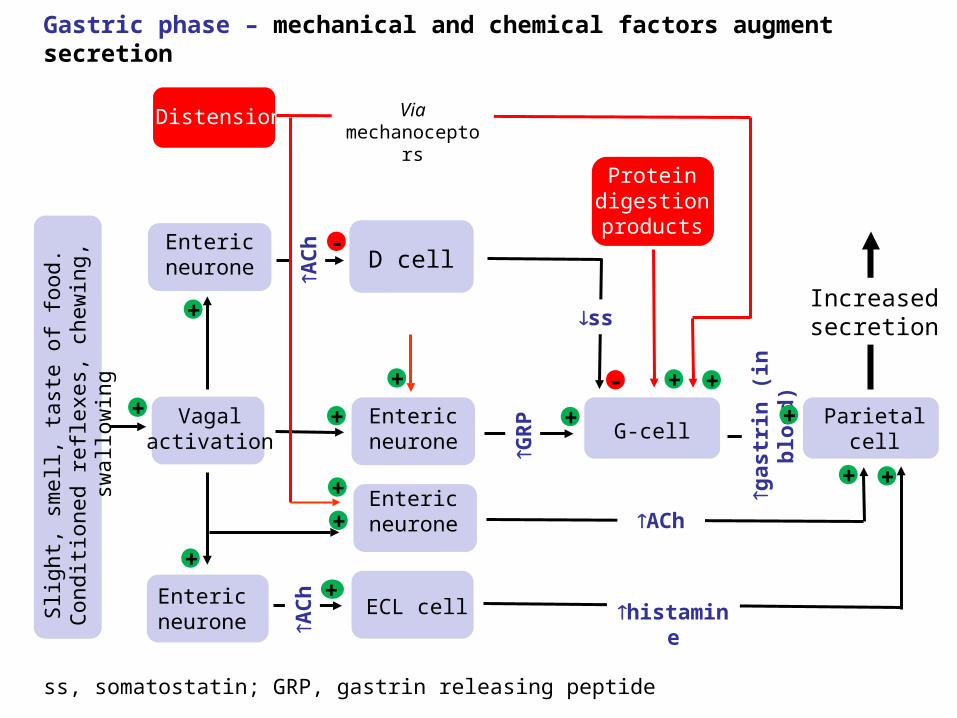
Distension
+ +
Protein digestion products
+
Via mechanoceptors
+
Gastric phase – mechanical and chemical factors augment secretion

Intestinal phase – includes factors originating from the small intestine that switch off acid secretion
The same factors that reduce gastric motility also reduce gastric secretion
As the stomach empties, the stimuli for secretion become less intense
Secretion of somatostatin resumes (low pH in stomach lumen, as occurs between meals, drives secretion)
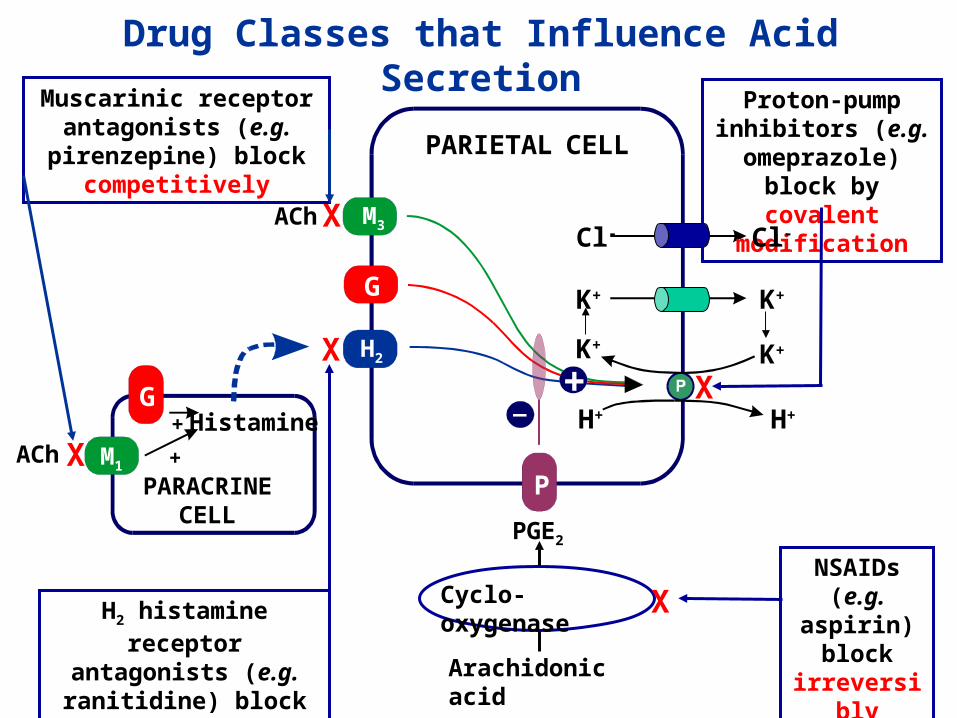
PARIETAL CELL
G
M3ACh
+
P
H2
Arachidonic acid
Cyclo-oxygenaseNSAIDs (e.g. aspirin) block irreversibly
X
X
X
PARACRINE CELL
HistamineG
+
+ACh M1X
Muscarinic receptor antagonists (e.g. pirenzepine)
block competitively
H2 histamine receptor antagonists (e.g. ranitidine)
block competitively
X
Proton-pump inhibitors (e.g. omeprazole) block
by covalent modification
Drug Classes that Influence Acid Secretion
K+ K+
H+ H+
PGE2
Cl-Cl-
K+K+
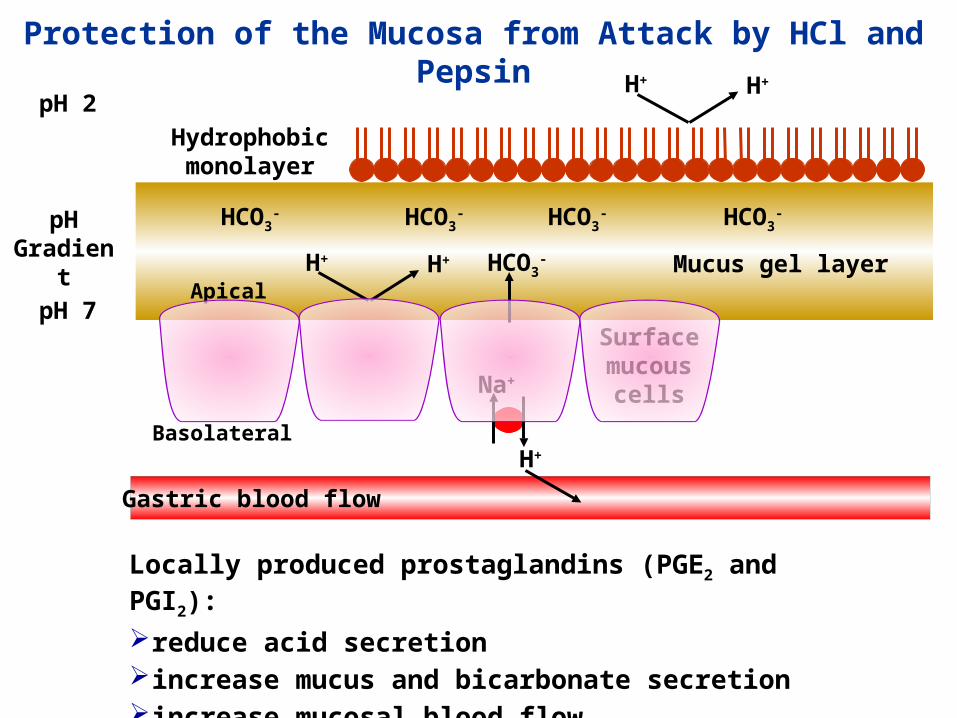
Locally produced prostaglandins (PGE2 and PGI2):
reduce acid secretionincrease mucus and bicarbonate secretionincrease mucosal blood flow
pH Gradient
Protection of the Mucosa from Attack by HCl and Pepsin
H+
Na+
HCO3-
Basolateral
Surface mucous
cells
Mucus gel layer
HCO3- HCO3
- HCO3-HCO3
-
ApicalH+ H+
Hydrophobic monolayer
H+ H+
pH 7
pH 2
Gastric blood flow

Non-Steroidal Anti-inflammatory Drugs and Peptic Ulcer
Non-steroidal anti-inflammatory drugs (NSAIDs; e.g. aspirin) reduce prostaglandin formation (COX 1 inhibition) and may trigger:gastric ulcerationBleedingNote: COX2-selective inhibitors may avoid this problem but are associated with increased risk of myocardial infarction and stroke – several withdrawn
Gastric damage due to long-term NSAID treatment can be prevented with a stable PGE1 analogue (i.e. misoprostol)
inhibits basal and and food-stimulated gastric acid formationmaintains (or increases) secretion and mucus and bicarbonate
Peptic ulcer refers to any ulcer in an area where the mucosa is exposed to hydrochloric acid and pepsin (stomach, duodenum)
Development of peptic ulcer is associated with a shift in the balance between mucosal-damaging and mucosal-protecting mechanisms Stomach ulcer
Drug treatment of peptic ulcer aims to promote ulcer healing by:reducing acid secretionincreasing mucosal resistanceEradicating H. pylori (see next slide)
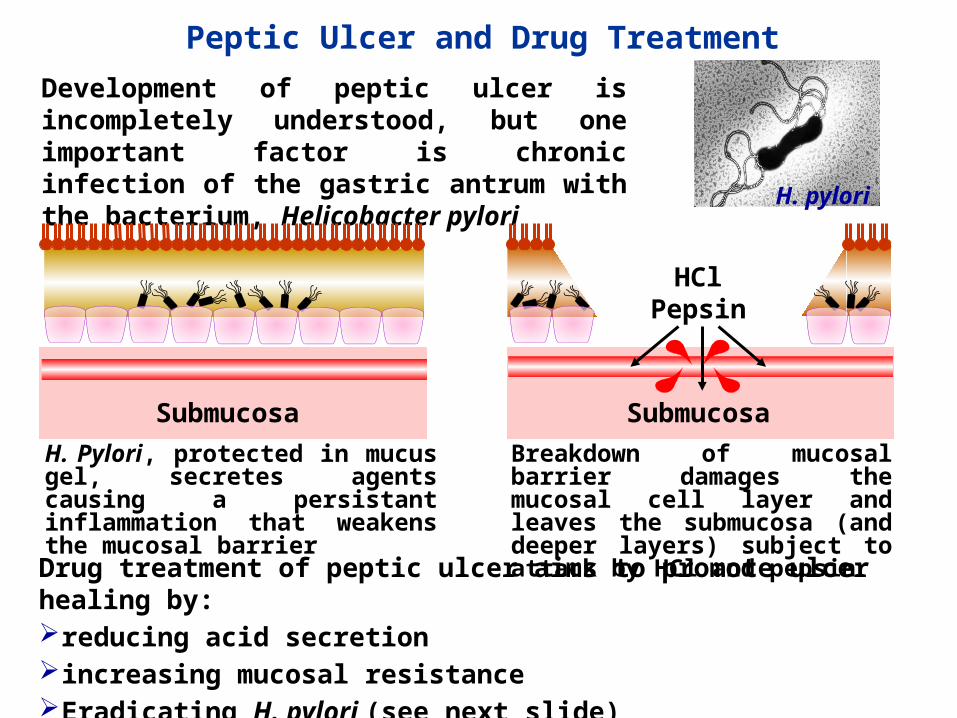
Peptic Ulcer and Drug Treatment
H. pylori
Development of peptic ulcer is incompletely understood, but one important factor is chronic infection of the gastric antrum with the bacterium, Helicobacter pylori
H. Pylori, protected in mucus gel, secretes agents causing a persistant inflammation that weakens the mucosal barrier
Submucosa Submucosa
Breakdown of mucosal barrier damages the mucosal cell layer and leaves the submucosa (and deeper layers) subject to attack by HCl and pepsin
HCl Pepsin

Drugs that Reduce Acid SecretionDrugs that reduce gastric acid secretion are used in the treatment of:
4) antagonism of gastrin receptors (not utilized clinically)
Acid hypersecretion [e.g. Zollinger-Ellison syndrome (a rare, gastrin-producing, tumour); Cushing’s ulcers (heightened vagal tone)]
gastro-oesophageal reflux disease (GORD; inappropriate relaxation of lower oesophageal sphincter allowing reflux of acid gastric contents into the oesophagus and subsequent tissue damage – oesophagitis)
peptic ulcer
Mechanisms of anti-secretory activity include:
1) inhibition of the proton-pump
2) competitive antagonism of histamine H2 receptors
3) competitive antagonism of muscarinic M1 and M3 ACh receptors

Proton-pump inhibitors (PPIs); e.g. omeprazole
inhibit the active (i.e. membrane inserted) H+/K+-dependent ATPase (proton-pump) – note pumps in tubulovesicles are not inhibited
are basic prodrugs that are inactive at neutral pH, but which change conformation in a strongly acidic environment (i.e. the canaliculus)
are absorbed from the GI tract and delivered via the systemic circulation to the secretory canaliculi of the stomach where accumulation, activation (to a sulfenamide) and covalent modification of lumenal sulphydryl groups of the membrane inserted proton-pump occurs
Systemic circulation Plasma
• Concentration (1000-fold)
• Two step activation involving protonation
• Cys-modification
• Inactivation of all available pumps
are used in treatment of peptic ulcer (particularly when associated with H. pylori), GORD and are the drugs of choice in Zollinger-Ellison syndrome
are effective orally once daily (q.d.) (as a capsule containing enteric-coated granules). However, not all pumps are inactivated and nocturnal acid breakthrough (NAB) may occur
unwanted effects are uncommon but concerns have been raised regarding long term treatment
Proton-pump inhibitors (PPIs); e.g. omeprazole (continued)
inhibition of acid secretion (typically 10-14 hr duration after a single dose before breakfast) greatly exceeds plasma half-life [for most PPIs e.g. lansoprazole, pantoprazole, rabeprazole 1 to 1.5 hr – tenatoprazole is an exception].
full effect is only achieved after repeated dosing
timing of dosing is important – drug must be present in plasma at an effective concentration whilst proton pumps are active

are used in the treatment of peptic ulcer and reflux oesophagitis
Muscarinic ACh receptor antagonists; e.g. pirenzepineHave been used for the treatment of peptic ulcer in the past but are now obsolete
Gastrin receptor antagonists; e.g. proglumideAre useful experimental tools, but have no clinical uses
completely block the histamine-mediated component of acid secretion and reduce secretion evoked by gastrin and ACh
Histamine H2 receptor antagonists; e.g. ranitidine and cimetidine
act as competitive (reversible) antagonists of H2 receptors
are effective against basal and stimulated gastric acid production
are effective once/twice daily by oral administration
unwanted effects (of ranitidine) are rare
Mucosal Strengtheners
Sucralfate – a complex of aluminium hydroxide and sulphated sucroserequires an acid environment for activation – releases aluminium to
acquire a strong negative charge
Bismuth chealate
has mucosal strengthening actions similar to sucralfate
administered orally
increases mucosal blood flow, mucus, bicarbonate and prostaglandin production
binds to the ulcer base (positively charged proteins) and forms complex gels with mucus – provides a mucosal barrier against acid and pepsin
administered orally (in combination with ranitidine)
is toxic towards H. pylori - used in combination with antibiotics and histamine H2 antagonists (ranitidine) to promote eradication of the bacterium and ulcer healing
AntacidsAct to neutralize gastric acid and inhibit peptic activity, e.g.
Aluminium hydroxide – forms AlCl3 in the stomach
Aluminium salts cause constipation
Magnesium hydroxide – forms MgCl2 in the stomach
Magnesium trisilicate - forms MgCl2 and colloidal silica (which binds pepsin) in the stomach
Magnesium salts cause diarrhoea
Antacids are used in the symptomatic relief of peptic ulcer and in dyspepsia
Combination Therapies in the Treatment of Peptic Ulcer
Aim to promote ulcer healing and prevent relapse by the eradication of H. pylori
Numerous combinations exist, examples include:
• Omeprazole + clarithromycin + amoxycillin
• Omeprazole + clarithromycin + metronidazole
Drugs That Increase Motility
Domperidone – increases tone of the lower oesophageal sphincter, increases gastric emptying and enhances duodenal peristalsis
Used in GORD and disorders of gastric emptying (e.g. gastroparesis associated with diabetic neuropathy)
Metoclopramide – greatly increases the rate of gastric
Used in GORD and disorders of gastric emptying