platelet biology of atrial (af) tailored to the acute ... · 12,562 pts with acs were treated with...
TRANSCRIPT

5/17/2016
1
Classification of Atrial Fibrillation (AF)
2
Recurrent AF*
(≥2 episodes)
Paroxysmal Persistent
Permanent
• Arrhythmia terminates spontaneously
• AF is sustained ≤7 days
• Arrhythmia does not terminate spontaneously
• AF is sustained >7 days
• Both paroxysmal and persistent AF can become permanent
*Termination with pharmacologic therapy or direct-current cardioversion does not change the designation.
Fuster V, et al. Circulation. 2006;114(7):e257-e354.
Platelet Biology
Tailored to the Acute
Coronary Syndrome
No Disclosures
Outline
1. Platelet Biology
1. Drug Therapy
• Aspirin
• Prasugrel
• Ticagrelor
• Cangrelor
• GP 2b/3a inhibitors
2. Preloading
3. Duration of DAPT

5/17/2016
2
Platelet
Thrombus Formation Involves Both Platelet
Activation and Blood Coagulation
INITIATION AMPLIFICATION PROPAGATION
Activated platelet
Fibrinogen (I)
Fibrin
Clot
X Xa
TF-VIIa
TF-VIIa
IX
IXa
Free vWF
VIII/vWF
VIIIa
Prothrombin (II)
Prothrombin
V
Va
XIa Xa Va
XIa
XI
IXa VIIIa
XIIIa
XIII Va
P-selectin
CD40L PAR1;4
Gp IIb/IIIa
P2Y12/ADP
X
TF-expressing cell/ microparticle
Xa
Xa
Thrombin (IIa)
Thrombin (IIa)
De Caterina R et al. Thromb Haemost 2013;109:569–79
No currently approved
antiplatelet agents specifically target
Adhesion
Most approved antiplatelet agents
affect different aspects of platelet
Activation
GP IIb/IIIa inhibitors inhibit the “final
common pathway,” Aggregation
Platelet-Mediated Thrombosis Targets
Meadows et al. Circulation Res. 2007;100:1261-1275
Platelet vWF Receptor (GP1b)
Intact Endothelium
Endothelial Damage
Collagen vWF
(Α2β3 Integrin) Platelet Collagen
Receptor (GPIa)
TXA2
ADP
Aspirin
ticlopidine, clopidogrel, prasugrel,
ticagrelor TXA2
Receptor
ADP (P2Y12)
Receptor
abciximab, eptifibatide,
tirofiban
GP IIb/IIIa
Receptor
GP = glycoprotein; vWF = von Willebrand factor; ADP = adenosine diphosphate; TX = thromboxane.
Desai NR, Bhatt DL. JACC CV int. 2010;3:571-83
Antiplatelet Agents
5/17/2016
3
Outline
1. Platelet Biology
1. Drug Therapy
• Aspirin
• Prasugrel
• Ticagrelor
• Cangrelor
• GP 2b/3a inhibitors
2. Preloading
3. Duration of DAPT
Platelet Inhibition by Low-Dose Aspirin
Patrono et al. JACC 2015 66(1): 74-85
Aspirin is Effective in Acute
Coronary Syndromes NSTE-ACS STEMI
Lancet 1988;2:349-60 Cairns JA et al. NEJM 1985;313:1369-76
Vascu
lar
Death
, n
35
200
300
400
500
100
ASA 461/4295 (10.7%)
SK 448/4300 (10.4%)
Placebo
568/4300 (13.2%)
SK + ASA 343/4292 (8.0%)
7 14 21 28
Days after STEMI
0
20 No aspirin
10
0
MI o
r C
ard
iac D
eath
, %
0 6
Months after NSTEMI
12 18 24
Aspirin
0

5/17/2016
4
PCI Without Aspirin
Kenaan M et al. JACC 2013:on-line
No ASA given w/i 24 hrs prior PCI in 4,640 (7.1%) of 65,175 pts. Propensity-matched in-hospital outcomes in 4,008 pt pairs:
Imbalances
↑ ASA use
• Prior PCI
↑ No ASA use
• Prior GI bleed
• STEMI
• Shock or
post arrest
• Prasugrel or
ticagrelor
Only 10.7%
contraindication
No difference in CIN between the groups (falsification endpoint)
Increase in mortality was robust in sensitivity analyses
P=0.0005
P=0.007
Death
No ASA ASA
>>favors ASA
Transfusion
Nephropathy requiring dialysis
CABG
Contrast induced nephropathy
Vascular complication
Stroke/CVA
Repeat PCI (same lesion)
Emergent CABG
0.25
Post procedural MI
<<favors no ASA
1.89 (1.32, 2.71)
1.08 (0.84, 1.39)
0.79 (0.38, 1.64)
1.52 (0.97, 2.40)
1.17 (0.89, 1.54)
0.89 (0.68, 1.17)
4.24 (1.49, 12.11)
1.13 (0.55, 2.34)
0.94 (0.26, 3.43)
1.54 (0.77, 3.05)
2.79%
5.54%
0.60%
1.00%
4.14%
4.07%
0.15%
0.47%
0.20%
0.50%
0.5 1 2 4 8
3.87%
5.71%
0.47%
1.65%
4.37%
3.47%
0.52%
0.50%
0.20%
0.70%
Incidence
Antithrombotic Trialists’ Collaboration. Lancet 2009;373:1849–60
Aspirin in primary and secondary prevention
Aspirin better Aspirin Worse
0.5 0.75 1.0 1.25 1.5 99% CI 95% CI
p<0.00001 0.81 (0.75-0.87) 1801 (8.19) 1505 (6.69) Total
Serious vascular event* (X2 1=0.0; p=1.0)
p=0.04 0.78 (0.61-0.99) 176 (0.77) 140 (0.61) Total
Ischemic stroke (X2 1=0.7; p=0.4)
p<0.00001 0.80 (0.73-0.88) 1214 (5.30) 995 (4.30) Total
Events per year
Major coronary event (X2 1=0.6; p=0.4)
0.81 (0.64-1.02) 314 (7.14) 250 (5.88) Female
0.81 (0.73-0.90) 1487 (8.45) 1255 (6.88) Male
0.73 (0.50-1.06) 123 (0.67) 95 (0.51) Male
0.91 (0.52-1.57) 53 (1.17) 45 (1.04) Female
0.81 (0.72-0.92) 1057 (5.79) 880 (4.70) Male
0.73 (0.51-1.03) 157 (3.36) 115 (2.59) Female
Aspirin Control RR (CI)
Meta-analyses of 16 secondary prevention trials (n=17,000)
Efficacy of Aspirin at Various Doses in Reducing
Vascular Events (Death from Vascular Causes, MI,
or Stroke) in High-risk Patients
Antithrombotic Trialists’ Collaboration, BMJ, 2002;342:71-86.
Aspirin
(mg daily)
No. of
Trials
% Odds
Reduction
Odds Ratio
500-1500
160-325
75-150
<75
Any aspirin
34
19
12
3
65
19
26
32
13
23
Treatment effect
P<0.0001
Aspirin better
0 0.5 1.0 1.5 2.0
Aspirin worse

5/17/2016
5
Yusuf S et al. N Engl J Med. 2001;345:494-502.
ASA Dose Placebo
+ ASA
Clopidogrel
+ ASA
<100 mg 2.0% 2.6%
100 – 200 mg 2.3% 3.5%
>200 mg 4.0% 4.9%
CURE:
Major Bleeding by ASA Dose
The therapeutic target for
thienopyridines and CPTPs is the
platelet P2Y12 receptor
Ticagrelor Prasugrel
Esterification and
2-step oxidation to
active metabolite
1-step oxidation to active metabolite
Active metabolite
P2Y12 Receptor Antagonists
Agent Class
IPA (20 uM ADP)
mean
Time to peak
onset
Reversibility (d/c before
CABG)
Ticlopidine 250 mg bid thienopyridine
(pro-drug) 25% 48 hrs
non reversible
5 days
Clopidogrel 300 mg LD Clopidogrel 600 mg LD
Clopidogrel 75 mg qd
Clopidogrel 150 mg qd
thienopyridine(pro-drug)
30% - 40% 35% - 50%
30% - 35%
45% - 50%
12 hrs 6 hrs
-
-
non reversible 5 days
Prasugrel 60 mg LD* Prasugrel 10 mg qd*
Prasugrel 5 mg qd*
thienopyridine(pro-drug)
80% 60%
40%
1-2 hrs -
-
non reversible 7 days
Ticagrelor 180 mg LD*
Ticagrelor 90 mg bid*
cyclo-pentyl-triazolo-
pyrimidine*
80%
70%
1-2 hrs
-
reversible
2-5 days
*Less affected by genetic polymorphisms and drug interactions (e.g. PPIs)
**not a pro-drug

5/17/2016
6
CURE Trial Investigators. N Engl J Med 2001;345:494–502.
Months
0.00
0.02
0.04
0.06
0.08
0.10
0.12
0.14
CV
Death
, M
I o
r str
oke
3 6 9 0 12
Placebo + Aspirin*
(n = 6303)
11.4%
Clopidogrel + Aspirin*
(n = 6259)
9.3%
P<0.001
20%↓
* In combination with standard therapy
CURE 12,562 pts with NSTE-ACS were treated with aspirin and randomized
to clopidogrel vs. placebo and followed for up to 12 months
Primary endpoint = CV Death, MI, or Stroke
PCI was performed
in 2658 pts (21%): 1 Yr CV Death or MI
A=median time to PCI; B=open label clopidogrel for 30 d after PCI
0.0
0.05
0.10
0.15
0 40 100 200 300 400 10
A B Days following PCI
CV
Death
or
MI
P=0.002 Clopidogrel
Placebo 12.6%
8.8%
31% Relative Risk
Reduction
10 days
Mehta SR et al. Lancet 2001;21:2033–41
CURE 12,562 pts with ACS were treated with aspirin and randomized to
clopidogrel vs. placebo and followed for up to 12 months
ASA + Clopidogrel ASA + Placebo P
CV death, MI, stroke 9.3% 11.4% <0.001
CV death, MI, stroke, refractory ischemia
16.5% 18.8% <0.001
- CV death 5.1% 5.5% NS
- MI 5.2% 6.7% <0.05
- Stroke 1.2% 1.4% NS
- Refractory ischemia 8.7% 9.3% NS
Non CV death 0.7% 0.7% NS
Bleeding events, any 8.5% 5.0% <0.001
- Major 3.7% 2.7% 0.001
- Minor 5.1% 2.4% <0.001
Primary endpoint = CV Death, MI, or Stroke
CURE Trial Investigators. N Engl J Med 2001;345:494–502

5/17/2016
7
Variability in Clopidogrel Response
Serebruany V et al. JACC 2005;45:246-51
Hochholzer W et al. Circ 20051;11:2560-4
0
20
40
60
80
100
120
-20 0 20 40 60 80 100
Nu
mb
er
of
Pati
en
ts
Change in 5 µmol/L ADP-induced
platelet aggregation with
75 mg chronic dosing
N=544
100
0 2 4 6 8 10 0
20
40
60
80
Time from loading dose to cath (h)
Maximal aggregation to
5 µmol/L ADP (%) after
600 mg loading dose
N=1001
Max A
gg
reg
ati
on
(%
)
Hypo
responders
Hyper
responders
ADAPT-DES: Stent thrombosis (definite or
probable) according to post-PCI PRU
HR [95%CI] = 2.54 [1.55, 4.16]
P=0.0001
PRU >208 (n=3610) PRU ≤208 (n=4839)
Ste
nt
thro
mb
osis
(def/p
rob
) (%
)
0
1
2
Months 0 3 6 9 12
3610 3450 3420 3380 3152
4839 4688 4654 4631 4341
Number at risk:
PRU > 208
PRU ≤ 208
1.3%
0.5%
Stone GW et al. Lancet 2013:on-line
Mechanisms of Individual Variability
in Clopidogrel Responsiveness
Angiolillio DJ et al. JACC 2007;49:1505-1516
Cellular Factors
• Accelerated platelet turnover
• Reduced CYP3A metabolic activity
• Increased ADP exposure
• Up-regulation of the P2Y12 pathway
• Up-regulation of the P2Y1 pathway
• Up-regulation of the P2Y–independent pathways (collagen, epinephrine, thomboxane A2, thrombin)
Clinical Factors • Failure to prescribe/poor compliance
• Under-dosing
• Poor absorption
• Drug-drug interactions involving CYP3A4 (?PPIs)
• Acute coronary syndrome
• Diabetes mellitus/insulin resistance
• Elevated body mass index
Suboptimal
Clopidogrel
Response
Genetic Factors
• Polymorphisms of CYP, GPIa, P2Y12, GPIIIa

5/17/2016
8
CYP2C19 Genetic Polymorphisms
and Outcomes With Clopidogrel 9 studies (91% PCI, 55% ACS)
MACE (N=9,684) Risk Ratio
(95% CI) P Value
Carriers vs Noncarriers 1.61 (1.28-2.02) <0.001
Heterozygotes vs Wildtype 1.50 (1.08-2.08) 0.016
Homozygotes vs Wildtype 1.81 (1.21-2.71) 0.004
Stent Thrombosis (N=5,772)
Carriers vs Noncarriers 2.76 (1.77-4.30) <0.001
Heterozygotes vs Wildtype 2.51 (1.59-3.98) <0.001
Homozygotes vs Wildtype 4.78 (2.01-11.39) <0.001
Risk Higher With
CYP2C19 Variant
Risk Lower With
CYP2C19 Variant
0.5 1.0 15.0
Mega JL et al. JAMA 2010; 304:1821-30
Metabolism of P2Y12 Receptor Blockers
Schomig A. NEJM 361;11:1108-11
Ticagrelor
Prasugrel
Clopidogrel
Active compound
Intermediate metabolite
Prodrug
CYP-dependent
oxidation
CYP1A2
CYP2B6
CYP2C19
CYP-dependent
oxidation
CYP2C19
CYP3A4/5
CYP2B6
CYP-
dependent
oxidation
CYP3A4/5
CYP2B6
CYP2C19
CYP2C9
CYP2D6 Hydrolysis
By esterase
Binding
Platelet
P2Y12
No in vivo biotransformation
O
O CI O
N S
F F
N
O Prasugrel Ticagrelor Clopidogrel
O
N
N N
N
F N
S
O
O S
O O
N
Ticagrelor and prasugrel have more rapid and consistently
greater IPA
5/17/2016
9
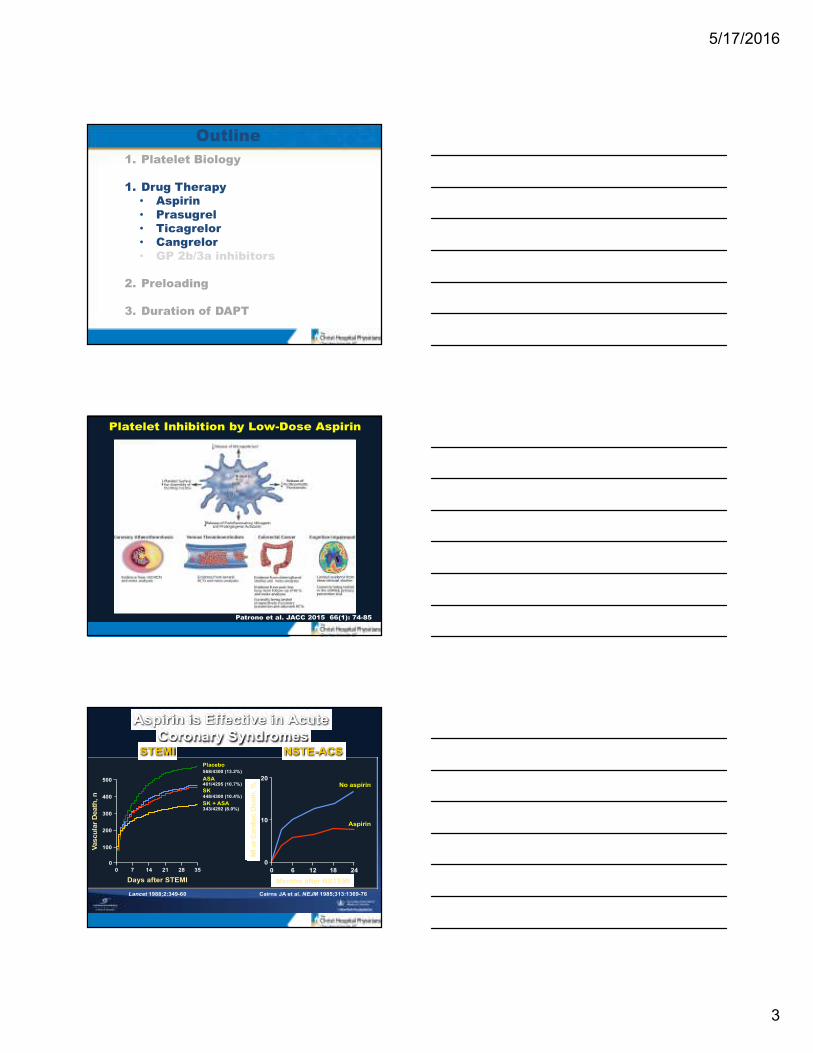
TRITON-TIMI-38 13,608 pts with ACS (unstable angina, NSTEMI, acute STEMI, or recent STEMI) undergoing PCI with known coronary anatomy (except for primary PCI pts) were
treated with aspirin and randomized to clopidogrel 300 mg load + 75 mg qd vs.
prasugrel 60 mg load + 10 mg qd and followed for 6-15 mos (median 12 mos)
Wiviott SD et al. NEJM 2007;357:2001-15
0
5
10
15
0 30 60 90 180 270 360 450
HR 0.81
(0.73-0.90)
P=0.0004
Prasugrel
Days
Pri
mary
En
dp
oin
t
CV
death
, M
I, o
r str
oke (
%)
12.1%
9.9%
Clopidogrel
HR 0.77 P=0.0001
HR 0.80 P=0.0003
7.4%
5.7%
Ste
nt
thro
mb
osis
(%
)
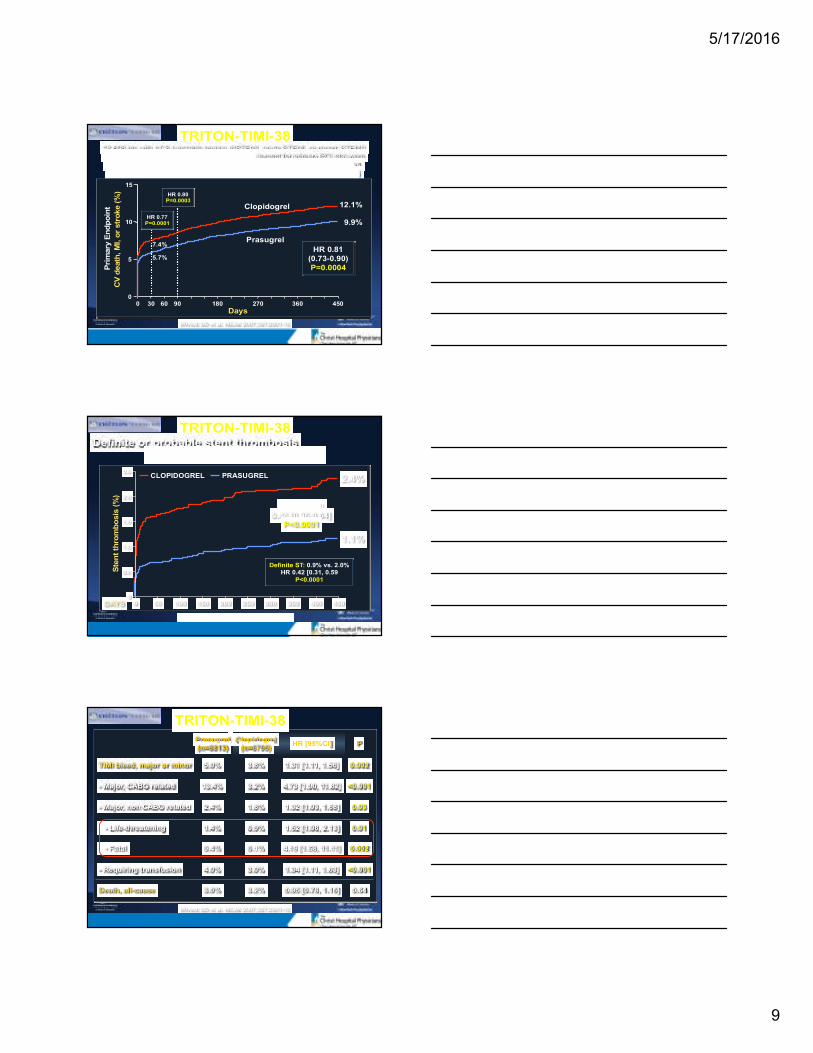
TRITON-TIMI-38 Definite or probable stent thrombosis
in 12,844 pts receiving any stent
0
0.5
1.0
1.5
2.0
2.5
0 50 100 150 200 250 300 350 400 450
HR [95%CI]
0.48 [0.36-0.64]
P<0.0001
2.4%
1.1%
DAYS
Wiviott SD et al. Lancet. 2008;371:1353-63
Definite ST: 0.9% vs. 2.0%
HR 0.42 [0.31, 0.59
P<0.0001
CLOPIDOGREL PRASUGREL
TRITON-TIMI-38
Prasugrel
(n=6813)
Clopidogrel
(n=6795) HR [95%CI] P
TIMI bleed, major or minor 5.0% 3.8% 1.31 [1.11, 1.56] 0.002
- Major, CABG related 13.4% 3.2% 4.73 [1.90, 11.82] <0.001
- Major, non CABG related 2.4% 1.8% 1.32 [1.03, 1.68] 0.03
- Life-threatening 1.4% 0.9% 1.52 [1.08, 2.13] 0.01
- Fatal 0.4% 0.1% 4.19 [1.58, 11.11] 0.002
- Requiring transfusion 4.0% 3.0% 1.34 [1.11, 1.63] <0.001
Death, all-cause 3.0% 3.2% 0.95 [0.78, 1.16] 0.64
Wiviott SD et al. NEJM 2007;357:2001-15

5/17/2016
10
Net Clinical Benefit CV Death / MI / CVA / TIMI Major Bleeding
OVERALL
≥60 kg
<60 kg
<75
≥75
No
Yes
0.5 1 2
Prior
Stroke / TIA
Age (years)
Weight
Risk (%)
+37
-16
-1
-16
+3
-14
-13
Prasugrel Better Clopidogrel Better HR
Pint = 0.006
Pint = 0.18
Pint = 0.36
Post-hoc analysis
Wiviott SD et al. NEJM 2007;357:2001-15
Prasugrel – FDA Label “Boxed Warning”
TRILOGY ACS: Study Design Medically managed UA or NSTEMI (68%)
(n=9,326)
Clopidogrel*
75 mg MD
Prasugrel*
5 or 10 mg MD
Minimum Rx Duration: 6 months; Maximum Rx Duration: 30 months
Primary Efficacy Endpoint: CV Death, MI, Stroke
Randomization stratified by:
age, country, prior clopidogrel treatment
(Primary analysis cohort — Age <75 years; n=7,243)
Clopidogrel* 300 mg LD
+ 75 mg MD
Prasugrel*
30 mg LD +
5 or 10 mg MD
Medical Management Decision ≤72 hrs (No prior clopidogrel given) — 4% of total
Medical Management Decision ≤ 10 days (Clopidogrel started ≤ 72 hrs in-hospital OR
on chronic clopidogrel) — 96% of total
*All patients were on aspirin and low-dose aspirin (< 100 mg) was strongly recommended. For patients <60 kg or ≥75 years, 5 mg MD of prasugrel was given.
Among pts <75 years, 7.9% underwent revascularization (median 113 [40-334] days)
Median time from presentation to
enrollment = 4.5 days
With (42%) or w/o prior angiography;
if with, required CAD
with DS ≥30%
Adapted from Chin CT et al. Am Heart J 2010;160:16-22.

5/17/2016
11
Primary Efficacy: CV death,
MI, or stroke (Age < 75 years)
HR (95% CI):
0.91 (0.79, 1.05)
P = 0.21
Roe MT et al. NEJM 2012:on-line
Median FU 17 months
Ticagrelor (AZD 6140): an Oral Reversible P2Y12 Antagonist
Ticagrelor is a cyclo-pentyl-triazolo-pyrimidine (CPTP)
O H
O H
O
O H
N
F
S
N
H
N N
N
N
F
• Direct acting
� Not a prodrug; does not require metabolic activation
� Rapid onset of inhibitory effect on the P2Y12 receptor
� Greater inhibition of platelet aggregation than clopidogrel
• Reversibly bound
� Degree of inhibition reflects plasma concentration
� Faster offset of effect than clopidogrel
� Functional recovery of all circulating platelets
� Off-target effects
� Blocks red blood cell adenosine re-uptake
Clopidogrel vs. Ticagrelor ONSET/OFFSET Study
Hours
0
20
40
60
80
100
0 4 8 12 16 20 24
Clopidogrel 600 mg
Ticagrelor 180mg
IPA
(%
; 20 m
M A
DP, F
inal)
.5
*
* * * *
Loading Maintenance and Offset
Ticagrelor vs clopidogrel.
* P<0.0001; † P<0.005; ‡, P<0.05
Gurbel PA et al. Circulation. 2009;120:2577-85.
Time (hours)
Offset Maintenance
Ticagrelor (n=54) Clopidogrel (n=50)
IPA
% (
20µM
AD
P –
Fin
al E
xte
nt)
100
80
70
50
10
0
6 weeks 24
‡
†
20
30
40
60
90
0 2 4 8 24 48 72 120 168 240
*
* *
* †
5/17/2016
12
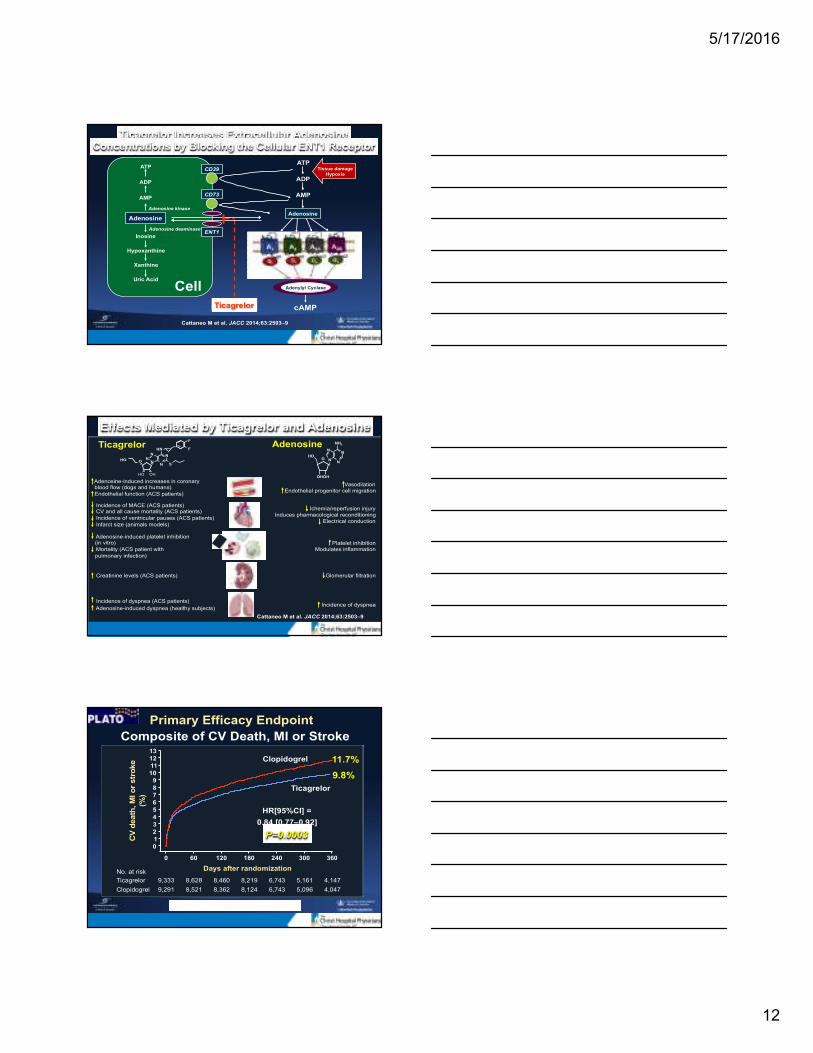
Ticagrelor Increases Extracellular Adenosine
Concentrations by Blocking the Cellular ENT1 Receptor
ATP
ADP
AMP
Adenosine
Inosine
Hypoxanthine
Xanthine
Uric Acid
Cell
Adenosine kinase
Adenosine deaminase
Ticagrelor cAMP
Tissue damage
Hypoxia
ATP
ADP
AMP CD73
CD39
Adenylyl Cyclase
Cattaneo M et al. JACC 2014;63:2503–9
ENT1
Adenosine
Effects Mediated by Ticagrelor and Adenosine
Cattaneo M et al. JACC 2014;63:2503–9
Ticagrelor Adenosine
Adenosine-induced increases in coronary blood flow (dogs and humans)
Endothelial function (ACS patients)
Incidence of MACE (ACS patients) CV and all cause mortality (ACS patients)
Incidence of ventricular pauses (ACS patients)
Infarct size (animals models)
Adenosine-induced platelet inhibition (in vitro)
Mortality (ACS patient with
pulmonary infection)
Creatinine levels (ACS patients)
Vasodilation Endothelial progenitor cell migration
Ichemia/reperfusion injury Induces pharmacological reconditioning
Electrical conduction
Platelet inhibition Modulates inflammation
Glomerular filtration
Incidence of dyspnea
HO OH
HO O N N
N
N N
S
F
F HN
OH
O
OH
HO N
N
N
NH2
N
Incidence of dyspnea (ACS patients)
Adenosine-induced dyspnea (healthy subjects)
Primary Efficacy Endpoint
Composite of CV Death, MI or Stroke
No. at risk
Clopidogrel
Ticagrelor
9,291
9,333
8,521
8,628
8,362
8,460
8,124
Days after randomization
6,743
6,743
5,096
5,161
4,047
4,147
0 60 120 180 240 300 360
12
11
10
9
8
7
6
5
4
3
2
1
0
13
CV
death
, M
I o
r str
oke
(%)
9.8%
11.7%
8,219
HR[95%CI] =
0.84 [0.77–0.92]
P=0.0003
Clopidogrel
Ticagrelor
Wallentin L et al. NEJM 2009;361:1045-57

5/17/2016
13
PLATO
Stent Thrombosis
1.9
2.8
3.6
1.3
2.1
2.8
0
1
2
3
4
5
Definite Denite or probable Definite, probable
or possible
12 M
on
th E
ven
tRate
(%
)
Clopidogrel (n=5,649) Ticagrelor (n=5,640)
HR(95%CI) = 0.67 (0.50–0.91)
P=0.009
HR(95%CI) = 0.77 (0.62–0.95)
P=0.01
HR(95%CI) = 0.75 (0.59–0.95)
P=0.02
Wallentin L et al. NEJM 2009;361:1045-57
PLATO
Primary and Secondary Endpoint Events
11.7
5.1
6.9
1.3
5.9
9.8
4.0
5.8
1.5
4.5
0
5
10
15
CV death,
MI, stroke
CV death MI Stroke All death
12 M
on
th E
ven
t R
ate
(%
)
Clopidogrel (n=9,291) Ticagrelor (n=9,333)
HR(95%CI) = 0.84 (0.77–0.92)
P<0.001
HR(95%CI) = 0.84 (0.75–0.95)
P=0.005
HR(95%CI) = 0.78 (0.69–0.89))
P<0.001
HR(95%CI) = 0.79 (0.69–0.91)
P=0.001
HR(95%CI) = 1.17 (0.91–1.52)
P=0.22
Wallentin L et al. NEJM 2009;361:1045-57
PLATO: Non-CABG and
CABG-related Major Bleeding
P=0.026
P=0.025
P=0.32 9
Non-CABG
PLATO major
bleeding
8
7
6
5
4
3
2
1
0 Non-CABG
TIMI major
bleeding
CABG
PLATO major
bleeding
CABG
TIMI major
bleeding
4.5
3.8
2.8 2.2
7.4 7.9
5.3
5.8
P=0.32
Ad
vers
e e
ven
t ra
te (
%)
Clopidogrel (n=9,291)
Ticagrelor (n=9,333)
Wallentin L et al. NEJM 2009;361:1045-57

5/17/2016
14
Percentage of Patients With High On-
Treatment Platelet Reactivity:
Ticagrelor vs. Clopidogrel
Angiolillo, et al. JACC 2016;67:603-13