pleasing patients through coordination of services
TRANSCRIPT

Pleasing Patients through Coordination of ServicesPresented by:
William Gillespie, VP-CTO WellSpan Health
Frank Poggio, President, The Kelzon Group
KELZON
GROUP
1) Learning - Objectives
2) Introduction: The Care Coordination Challenge
3) WellSpan Health - Background
4) WellSpan Coordinated Services-Scheduling
- Challenges, Accomplishments
- Success Factors, Benefits
- Future Plans
5) ROI Touch Points
6) Larger Challenges and Recap
7) YOUR TURN…...Q&A
Agenda
Learning Objectives
1. Discuss how to improve patient satisfaction by scheduling all medical
and non-medical services for inpatients
2. Identify why coordinating inpatient care has been a challenging task in
most hospitals
3. Discuss the difference between coordinated services and central
scheduling, and why the latter is fraught with organizational difficulties
4. Describe how to avoid the organizational and political battles that come
with improving care coordination, and address the hurdles of
unscheduled emergency services
5. Explain why most hospitals that tried to improve inpatient service flow
have failed, and how they could have succeeded
Introduction: The Care Coordination
Challenge
• Building a Better Delivery System
• Inter-Department Coordination
• Partial-Coordination via HIS/EMR
• Possible Solutions
• Full-Service Coordination
Building a Better Delivery Systemthrough Coordination of Services
Definition: Health care delivery, like other business enterprises, is a
complex socioeconomic system in which multiple agents, often with
very different agendas, interact. As in complex business enterprises,
decisions taken by one party can significantly affect the costs
incurred and the quality of service provided by other parties in the
system. In addition, different entities in the system, so-called agents,
often have different, sometimes conflicting, objectives. The history
of enterprise-management systems has shown that a thorough
understanding of how different agents in the system interact can
yield significant benefits for the entire system.
Building a Better Delivery System, Proctor P. Reid, W. Dale Compton, Jerome H. Grossman, and Gary Fanjiang, Editors, Committee on
Engineering and the Health Care System, Institute of Medicine and National Academy of Engineering, 2005, ISBN:978-0-309-65406-7
Finding 3-1. The health care delivery system functions not as a system, but as a
collection of entities that consider their performance in isolation. Even within a given
organization (e.g., a hospital), individual departments are often isolated and behave as
functional and operational “silos.”
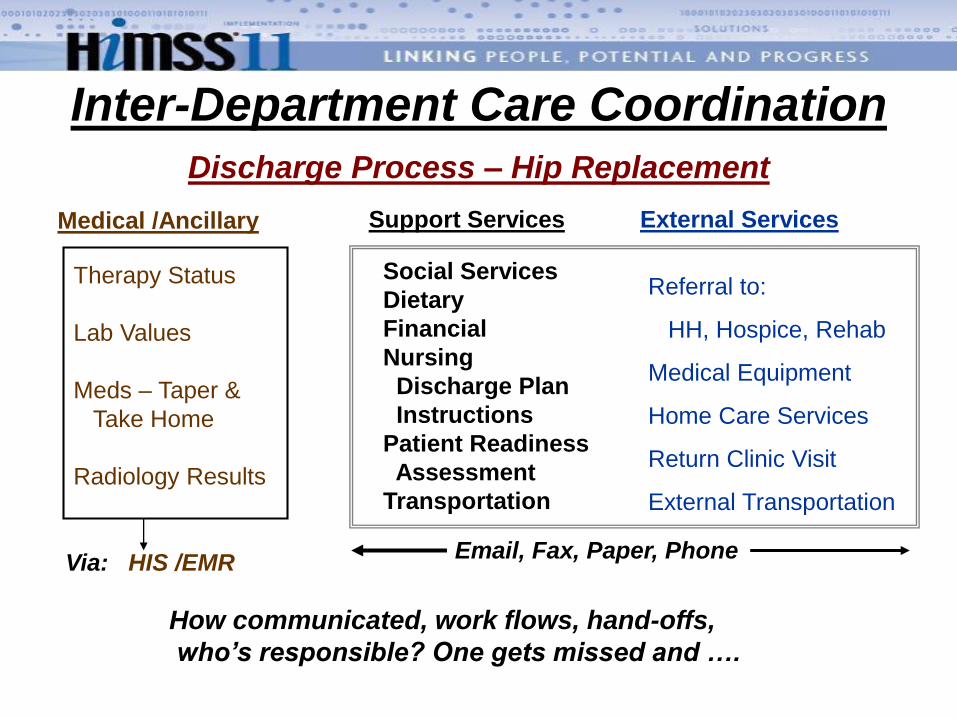
Inter-Department Care Coordination
Discharge Process – Hip Replacement
Medical /Ancillary Support Services External Services
Therapy Status
Lab Values
Meds – Taper &
Take Home
Radiology Results
Social Services
Dietary
Financial
Nursing
Discharge Plan
Instructions
Patient Readiness
Assessment
Transportation
Referral to:
HH, Hospice, Rehab
Medical Equipment
Home Care Services
Return Clinic Visit
External Transportation
How communicated, work flows, hand-offs,
who’s responsible? One gets missed and ….
Via: HIS /EMREmail, Fax, Paper, Phone
Radio
logy
Surg
ery
Thera
pie
s
Fin
ance
Card
iolo
gy
Pharm
acy
Labora
tory
Housekeep
Tra
nspor-
tation
Nurs
ing-
Routine
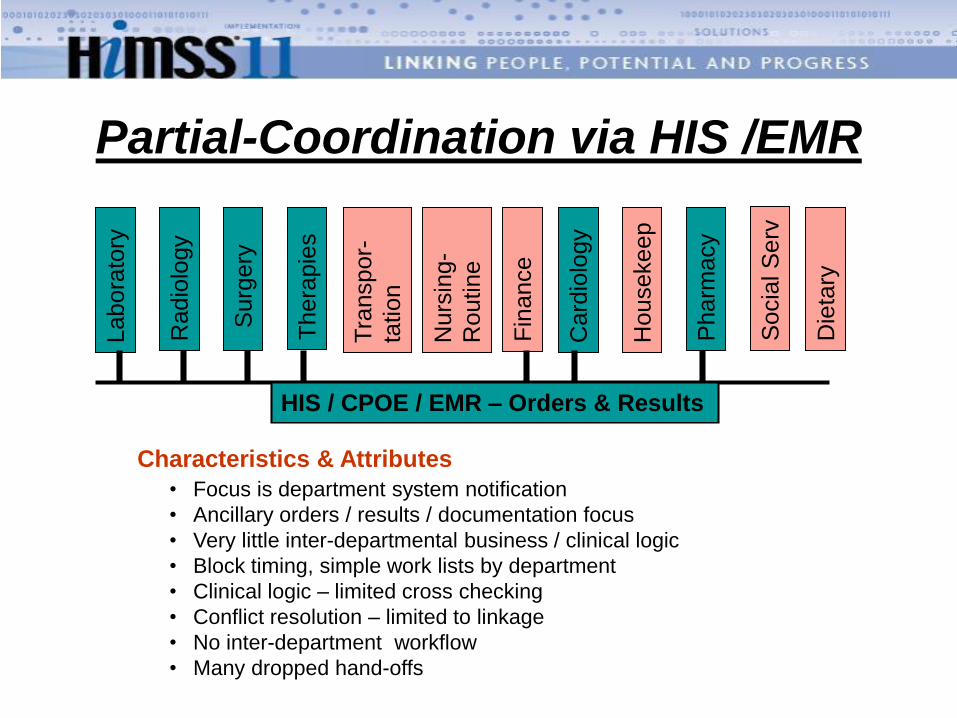
• Focus is department system notification
• Ancillary orders / results / documentation focus
• Very little inter-departmental business / clinical logic
• Block timing, simple work lists by department
• Clinical logic – limited cross checking
• Conflict resolution – limited to linkage
• No inter-department workflow
• Many dropped hand-offs
Characteristics & Attributes
HIS / CPOE / EMR – Orders & Results
Socia
l S
erv
Partial-Coordination via HIS /EMR
Die
tary
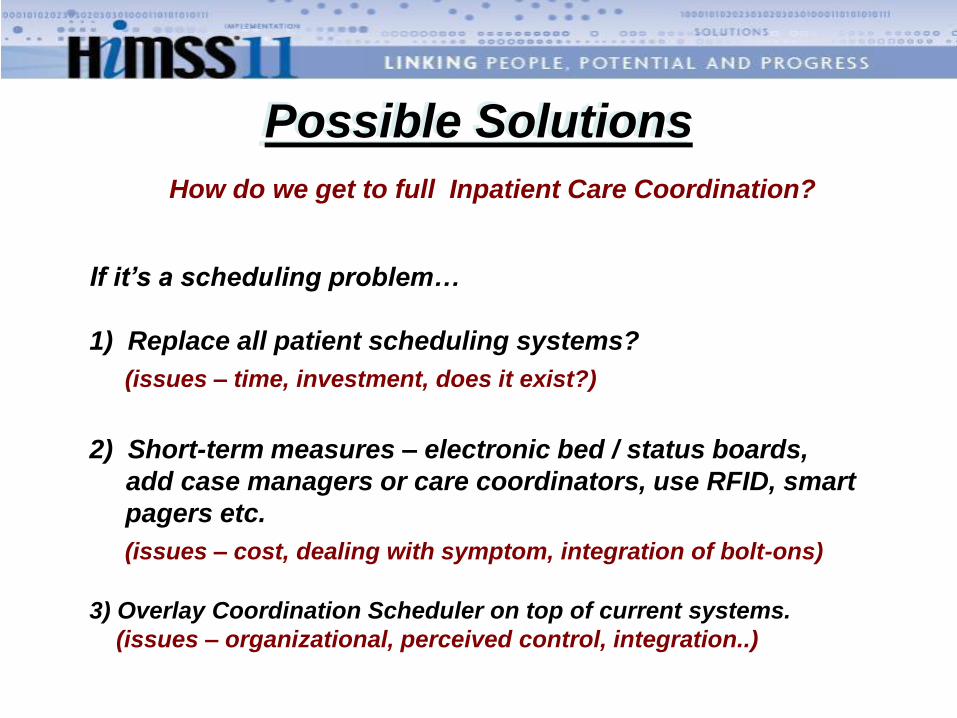
Possible Solutions
If it’s a scheduling problem…
1) Replace all patient scheduling systems?
(issues – time, investment, does it exist?)
2) Short-term measures – electronic bed / status boards,
add case managers or care coordinators, use RFID, smart
pagers etc.
(issues – cost, dealing with symptom, integration of bolt-ons)
3) Overlay Coordination Scheduler on top of current systems.
(issues – organizational, perceived control, integration..)
How do we get to full Inpatient Care Coordination?
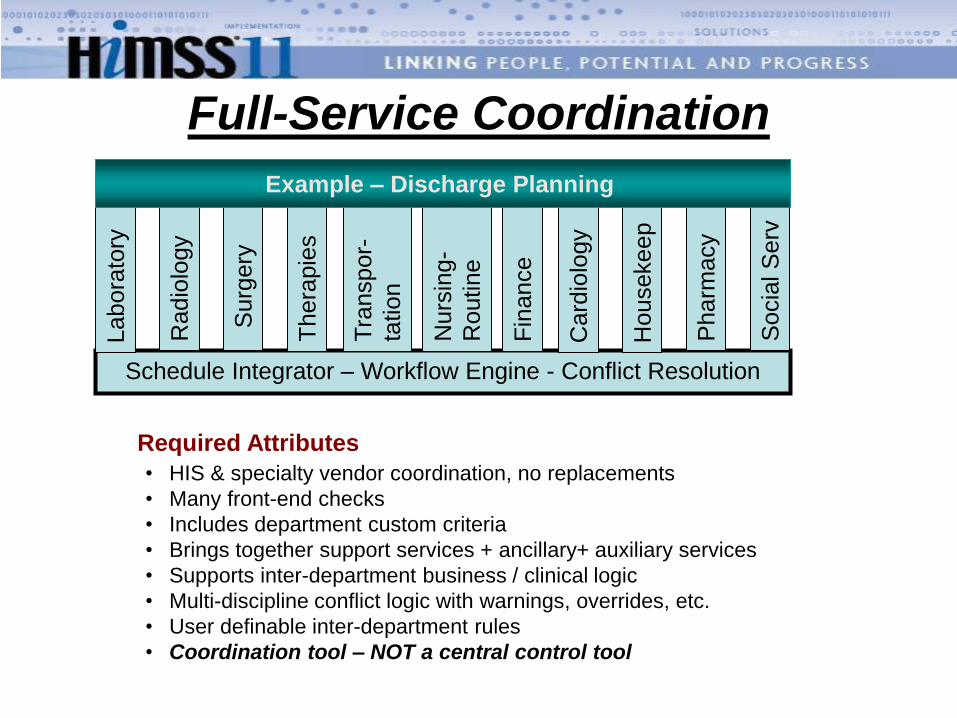
Required Attributes
Schedule Integrator – Workflow Engine - Conflict Resolution
Radio
logy
Surg
ery
Thera
pie
s
Fin
ance
Card
iolo
gy
Pharm
acy
Socia
l S
erv
Labora
tory
Housekeep
Tra
nspor-
tation
Nurs
ing-
Routine
• HIS & specialty vendor coordination, no replacements
• Many front-end checks
• Includes department custom criteria
• Brings together support services + ancillary+ auxiliary services
• Supports inter-department business / clinical logic
• Multi-discipline conflict logic with warnings, overrides, etc.
• User definable inter-department rules
• Coordination tool – NOT a central control tool
Full-Service Coordination
Example – Discharge Planning
WellSpan Health System –
Background
WellSpan Health System
• Geography
• Facilities
• Staff
• Patient Experience
WellSpan Health System
Who are we?
● Integrated health system located in south-central PA
● Top 100 – Integrated Health Systems
● York Hospital – “Top 100” Hospital with Thomson Reuters – 7 years
● Gettysburg Hospital – “Top 100” Performance Improvement Leader
2 hospitals (630 beds)
65 sites in 3 counties; 2 states serving a population of 500,000, 60% overall market share
8,000 staff, physicians, volunteers
7 residency programs, 250 students and a research center
6 retail pharmacy sites
450-member multi-specialty medical group
1 home health organization
PPO serving 50,000+ covered lives
WellSpan Health System
● 36,000 IN-PAT DISCHARGES
● 1.1 million OUT-PAT ENCOUNTERS
- 95,000+ ED visits
- 74,000 Clinic visits
- Lab-specimens and nursing home labs
● $1.2 billion annual gross revenue
● 1.2 annual medical group physician visits
Wellspan Health Statistics
WHY

Every week, a significant percentage of the Adams-York population experiences care from a WellSpan Service
14,133 patients visit a
WSH physician practice
8,708 patients fill a
prescription at a WSH
outpatient pharmacy
1,918 patients receive
a VNA home visit
685 patients are admitted
to a WSH hospital
17,575 patients undergo a
test, procedure or treatment
in a WSH ambulatory facility
1,678 patients visit a WSH
emergency department
Community Health
Improvement
Patient Experience
Health System Design
Financial Performance
Physician Partnerships
Human Resources
WellSpan Strategic Goals
WellSpan Health
Patient Experience - Goal
To provide an exceptional
care experience—safe,
timely, effective, equitable,
efficient and patient-
centered—to each and every
patient, each and every
time, every day.
1. A consistently great patient experience is a matter
of design
2. We are not Disney. Satisfaction is less about making
people happy and more about reducing anxiety
3. Caring and communicating caring are two different
things
4. Patients want care to feel personal. We can
standardize personalization
5. Ineffective accountability is evidence that we are not
serious.
WellSpan Health
Patient Experience - Guiding Principles
WellSpan Coordination of Services –
Scheduling
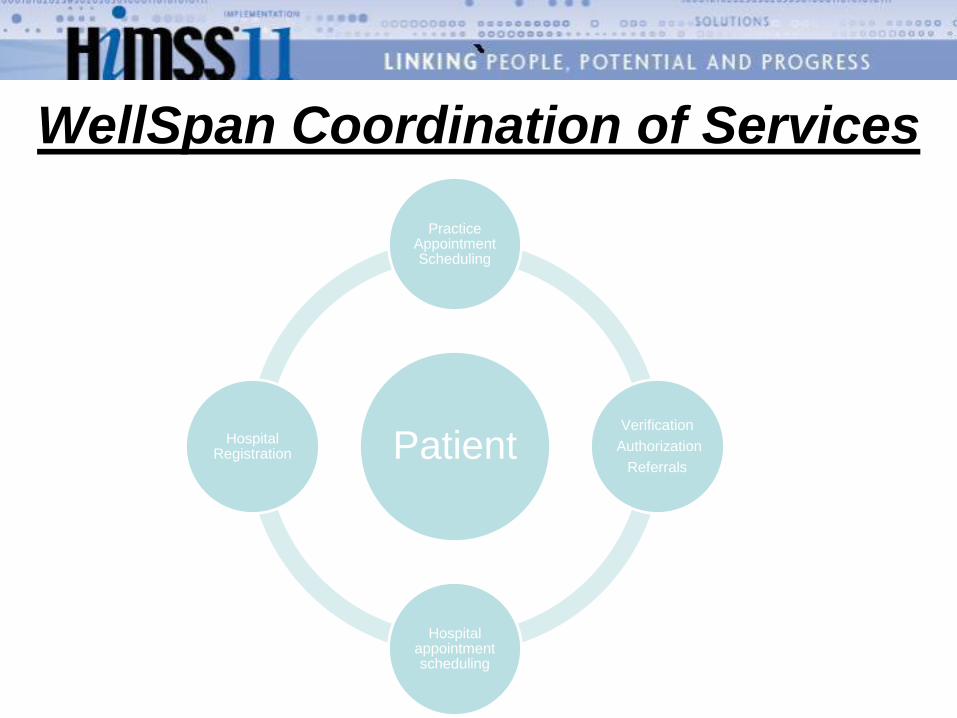
WellSpan Coordination of Services
Patient
Practice Appointment Scheduling
Verification
Authorization
Referrals
Hospital appointment scheduling
Hospital Registration
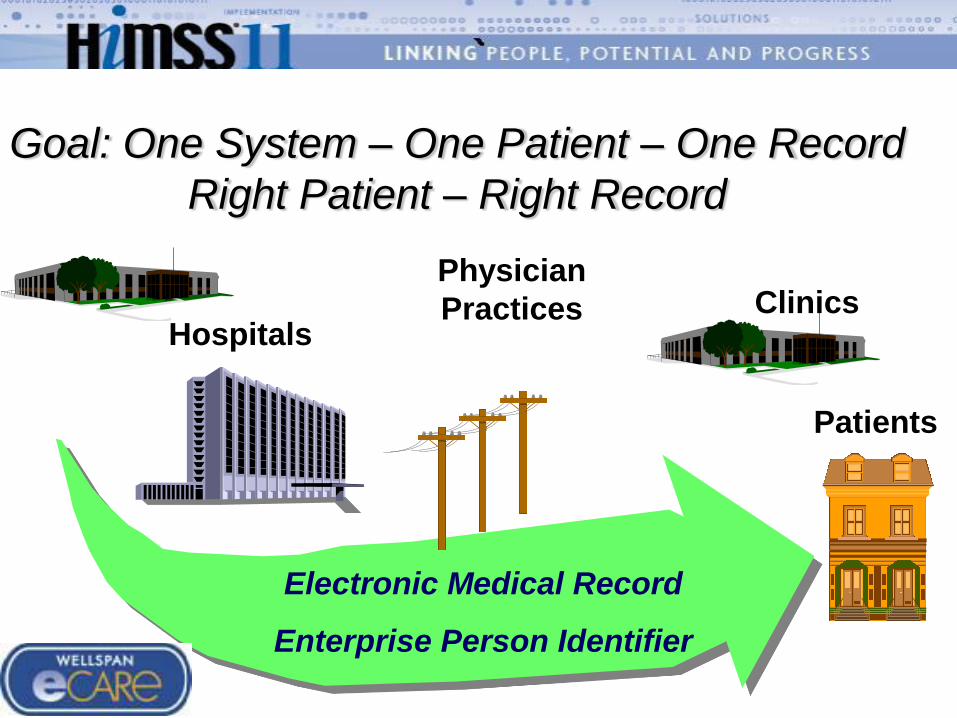
Hospitals
Physician
Practices Clinics
Patients
Electronic Medical Record
Enterprise Person Identifier
Goal: One System – One Patient – One Record
Right Patient – Right Record
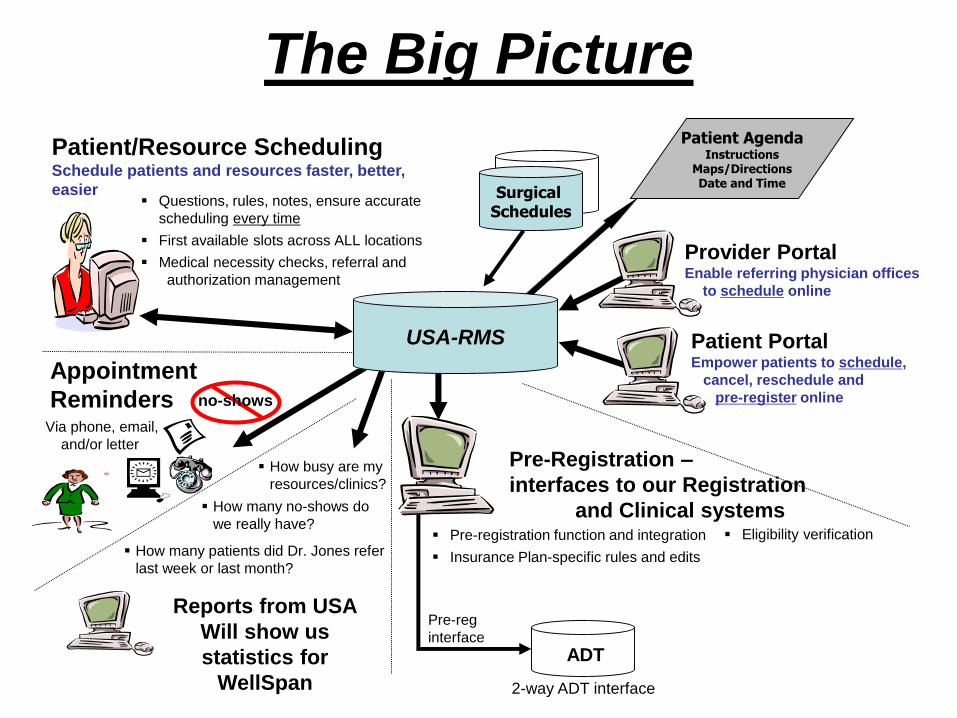
The Big Picture
Provider PortalEnable referring physician offices
to schedule online
Patient PortalEmpower patients to schedule,
cancel, reschedule and
pre-register online
Pre-Registration –
interfaces to our Registration
and Clinical systems Pre-registration function and integration
Insurance Plan-specific rules and edits
Eligibility verification
ADT
2-way ADT interface
Pre-reg
interface
Surgical Schedules
Patient AgendaInstructions
Maps/DirectionsDate and Time
Patient/Resource SchedulingSchedule patients and resources faster, better,
easier Questions, rules, notes, ensure accurate
scheduling every time
First available slots across ALL locations
Medical necessity checks, referral and
authorization management
How busy are my
resources/clinics?
How many no-shows do
we really have?
Appointment
RemindersVia phone, email,
and/or letter
no-shows
Reports from USA
Will show us
statistics for
WellSpan
How many patients did Dr. Jones refer
last week or last month?
USA-RMS
WellSpan Coordinated Services
1.From the top – Executive Champion
2.Primary Objectives: Streamline services,
pursue patient itinerary
3.Project led by: Peter Ivers, Director of Product Knowledge Office, and
Amy Repman, Director of Patient Access
4.Start in Imaging
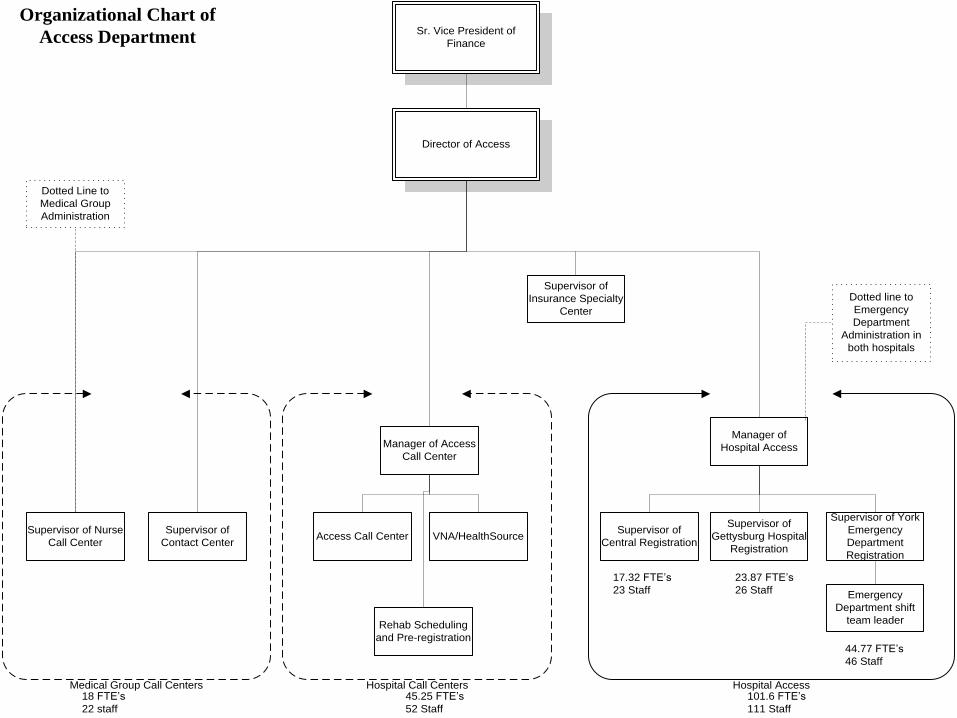
Director of Access
Manager of Access
Call Center
Manager of
Hospital Access
Access Call CenterSupervisor of
Central Registration
Supervisor of York
Emergency
Department
Registration
Supervisor of
Gettysburg Hospital
Registration
Supervisor of Nurse
Call Center
Emergency
Department shift
team leader
Sr. Vice President of
Finance
Dotted Line to
Medical Group
Administration
Hospital Call Centers Hospital Access
17.32 FTE’s
23 Staff
23.87 FTE’s
26 Staff
44.77 FTE’s
46 Staff
45.25 FTE’s
52 Staff
101.6 FTE’s
111 Staff
Dotted line to
Emergency
Department
Administration in
both hospitals
Organizational Chart of
Access Department
Supervisor of
Contact Center
Supervisor of
Insurance Specialty
Center
Medical Group Call Centers
VNA/HealthSource
Rehab Scheduling
and Pre-registration
18 FTE’s
22 staff
WellSpan Coordinated Services
• Improving the patient experience with complete view of department and patient availability and appointment history
• Integrating pre-registration and registration information
• Providing preparatory instructions and details to reduce anxiety due to the “unknown”
• Integrating appointment location with driving directions and on-site directions and details
• Rehabilitation Medicine
• Imaging
• Cardiology
• Maternal Fetal Medicine
• Pulmonary and Sleep
• Specialty Clinics
WellSpan Coordinated Services -Scheduling
Initial project focus – All Imaging services
Started - March 2007
Go live at Gettysburg facility - December 2007
WellSpan Coordinated Services -Scheduling
WellSpan
Coordinated Services -SchedulingChallenges:1. Eleven different scheduling systems
across just all imaging services,
2. Different patient priorities for each,
3. Different clinical and operational rules,
4. Different code tables, mpi, little or no
communication between them,
5. Organizational issue;
centralization=loss of control?
WellSpan
Coordinated Services -Scheduling1.Specialized systems not replaced, eg. Radiation
Oncology, linked into new coordinated scheduling system.
2.New coordinated scheduler from outside firm.
3.Tied together all manual and automated existing
systems.
4.Service requests can originate in new system or
in any of the eleven systems and are
coordinated for conflicts.
WellSpan
Coordinated Services -Scheduling
Typical conflict /coordination problem:. A patient is scheduled for a series of radiology exams all of which could
conflict with each other if not done in the proper sequence.
Specifically, a physician places an order for a CT with contrast on
Monday, and on Tuesday orders a multi-day Nuclear Medicine exam that
can only be done 24 hours after the Monday contrast procedure. In this
example, we have to do a conflict check on a prior scheduled procedure,
then schedule the Nuclear Medicine exam with enough elapsed time for
the contrast to dissipate.
In the past this was done manually referencing a set of three inch binder
rule books. A time consuming and error prone process.
WellSpan Coordinated Services
Imaging services hurdles:
• Standardizing terminology across all
locations
• Identify champions in each area
• Disparate coding systems in each area (insurance, payer, service codes, etc.)
• How to handle random ER requests?
• Link 7 different imaging systems
• Allow routine imaging requests to be made
real time in physician offices
WellSpan Coordinated ServicesAccomplishments:
Radiology procedures can be scheduled from any
site in less than 10 minutes
• Inpatient and outpatient services are coordinated,
conflicts resolved quickly
• Physicians can schedule Images from their
offices before the patient leaves,
• Critical demographic and insurance info is
captured long before the patient comes to the
ancillary department.
• Itineraries for multi service visits are available
WellSpan Coordinated Services
Handling ER requests and interruptions:
In the past: Inpatient requests were back fill for
large ER unused open blocks.
Current: All IP requests scheduled, system
manages flexible smaller open block times for
ER cases.
Results: ED support can be accommodated
without using inpatients as back fill.
Future: Experienced based predictive models
could eliminate ER open blocks
WellSpan Coordinated Services
Success Factors:1. Executive leadership needed to drive such an undertaking across
multiple departments
2. Keep the focus on patient satisfaction.
3. Openness and willingness of the Imaging staff to adopt standards
and coordination of schedules.
4. The technical integration ability of WellSpan’s IT staff in
implementing linkages across the multiple systems.
5. Software flexibility of purchased system, and vendor’s open
approach to work with other systems.
WellSpan Coordinated Services
Benefits:1. Significantly improve patient satisfaction by eliminating or
greatly reducing wait times (for both IP and OP) at the
ancillary departments and quicker turnaround for service
schedule requests.
2. Increase revenue by increasing department capacity without
increases in capital investment.
3. Avoid financial losses due to longer than allowed stays under
DRG or managed care contracts.
4. Improve physician relations from remote office scheduling.
WellSpan Coordinated IP Services
Future Plans:
1) Expand Vendor system to more
ancillary areas
2) Create the complete patient
itinerary in Vendor system
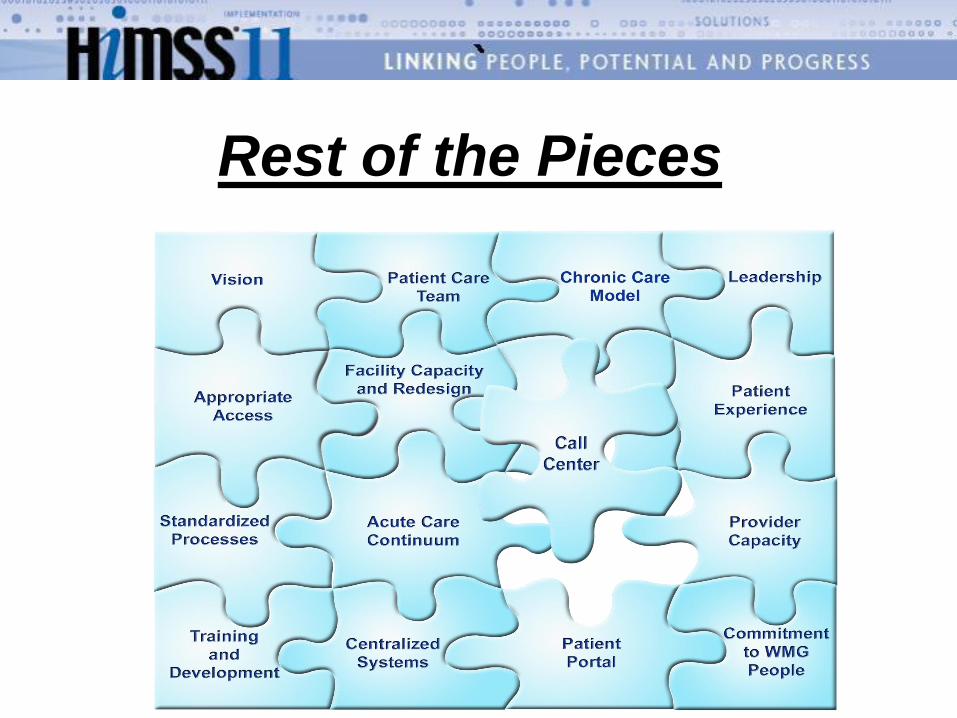
Rest of the Pieces
Rarely done in Hospitals because:
- Requires Significant Department Coordination
- Rethink transportation management and other support services
- Complex inter-department process re-engineering (LEAN+)
- Requires sophisticated work flow tools
- Many political / organizational hurdles
- ‘Centralization’ not an accepted clinical approach…’coordination’
But can have significant benefits & ROI:
Inpatient Care Coordination
The 800 pound gorilla !
- MANDATORY: Active Executive Support !!
Today…
Coordinated IP Services
• Improve Patient Flow
• Start point for ACO
• Improve Patient Satisfaction – Patient Itinerary - P4P Impact
• Increase Revenues from Increases in Capacity
• Improve Physician Satisfaction = Increase Revenues
• Facilitate ‘Health Support Models’ = Improve Revenues
• Reduce DRG / Managed Care Losses for Extra Stays
• Reduce / eliminate/ avoid Capital Investments:
ED, Surgery, Beds, Ancillary service equipment, etc.
• Labor / Supply Reductions, Increase Department Efficiency
ROI Touch Points
YOUR TURN….
Have you identified this as a major issue?
How do you deal with it now?
Who in your organization is the lead?
Other suggestions / observations?
Questions?
Thank YouGroup
Kelzon
Improving Care Coordination
Frank L. Poggio
Frank L. Poggio has over thirty-five years of experience in health care systems. He has served as a
hospital administrator/CFO, software entrepreneur, and industry consultant. He has completed
consulting engagements for both large and small hospitals and clinics, and major vendors of health
information systems. He is President of The Kelzon Group, a firm that focuses on health systems
issues. Previously, he was General Manager of Mediware, Inc., a clinical software and publicly held
company. He served as President of Citation Computer Systems, Inc., a St. Louis based clinical
software company acquired by Cerner ,Inc. In 1980, Mr. Poggio founded Health Micro Data Systems
(HMDS), a firm specializing in client server based systems for health care organizations. HMDS’
clinical and financial software was installed in over 120 hospitals and other health facilities around the
country.
In 1971 he started his health care career as a project engineer for the Hospital Association of NY where
he completed many operational reviews for patient flow and operational efficiency. He was VP and
Associate Administrator, CFO and CIO at the University of Wisconsin Hospital and Clinics and was
Senior Consultant with KPMG for health information systems. He is a frequent invited speaker for the
Healthcare Financial Management Association, and the HIMSS. He served as a faculty member of the
University of Wisconsin Graduate School of Business, Health Care Fiscal Management Program for 13
years. Mr. Poggio has published over forty articles in various professional health journals on health
information systems, finance and related topics.
Mr. Poggio can be contacted at [email protected], or http://KelzonGroup.com
KELZON
GROUPGroup
Kelzon
William ‘Buddy’ Gillespie
Mr. Gillespie is Vice President, Chief Technology Officer and CIO
Emeritus at WellSpan Health, an integrated delivery system based in
York, Pennsylvania. WellSpan has been named a Top 100 Most Wired
and a Top 25 Best Connected health system four-years running.
Gillespie joined WellSpan Health in 1996 after serving as vice president
of information services at Allegheny General Hospital in Pittsburgh. As
WellSpan's CTO, he is responsible for the strategic planning and
implementation of information technology to support integrated
applications consisting of financial, clinical and administrative
systems. Mr. Gillespie holds degrees in physics and mathematics from
Athens University. He has been active in healthcare informatics for more
than 25 years in both the development and implementation of technology
solutions He also serves on the PAeHI Board where he is Chair of the
Health Information Exchange Committee.
Mr. Gillespie can be contacted at: [email protected]