post stroke upper extremity rehabilitation - a clinical perspective
TRANSCRIPT
Post-Stroke Upper Extremity
Rehabilitation –
A Clinical Perspective
Phinoj K. Abraham, MOTh., (Neuro-Occupational Therapist)
NewRo, Bengaluru
Learning Objectives
To share some views and experience of
What to do?
How to do?
in post stroke upper extremity Rehabilitation from
an Occupational Therapy Perspective
2
What to do first?
3
What to do?
‘Diagnosis specific’&
‘Prognosis Oriented’
Evidence basedtreatment planning
4
A) Diagnosis Specificity
• Therapy planning SHOULD be based on the precise diagnosis of Stroke
– Ex:
A 28 year old male civil engineer with left hemiparesis
C/c : Difficulty in eating in ‘buffet’ systemBrunnstrom's recovery Stage for Hand : Stage 6/7
Power : ~ 4+/5
5
Diagnosis Specificity Contd…
• ‘Activity Analysis’ showed– Inability to maintain the plate steadily (horizontally) in his
left hand especially while serving dishes / while talking to others. At the same time he can describe what is the ‘correct’ way of holding
• Why?– Right MCA territory Infarct– Involvement of Rt. Parietal Lobe
‘Perceptual – Motor’ aspect is usually a neglected domain in early post stroke U/E rehab
6
Need of Diagnosis specificity in treatment planning…
• An infarct at ganglio-capsular region usually produce ‘Plastic Rigidity’. (Paul Kaplan,1940) This will be helpful to train the U/E to be a ‘supportive hand’.
• The probability of recovery of isolated UE movement decreases progressively with lesion location as follows: cortex, corona radiata, and Post. Limb of Internal Capsule (Shelton and Reding- 2001)
7
B) Prognosis Oriented
• Why?
“You must always be able to predict what's next
and then have the ‘flexibility to evolve’.”
Marc Benioff
8
B) Prognosis Oriented Contd…
• How? based on • Area and/or type of brain damage 1
» Patients with anterior circulation infarcts, right hemispheric strokes, visual gaze deficits etc… were associated with poor arm function.
• Initial degree of motor Impairment2
» Severe paresis vs. mild paresis» Active finger extension & shoulder abduction
• Other factors» Time of initial ‘Medical Intervention’» Presence / absence of cognitive impairment 1) EBRSR, 2013
2) EBRSR,, 2014,
1) EBRSR, 4,Rehab of hemiplegic U/E, 20142) EBRSR, 10, Upper extremity Interventions, 2013
10
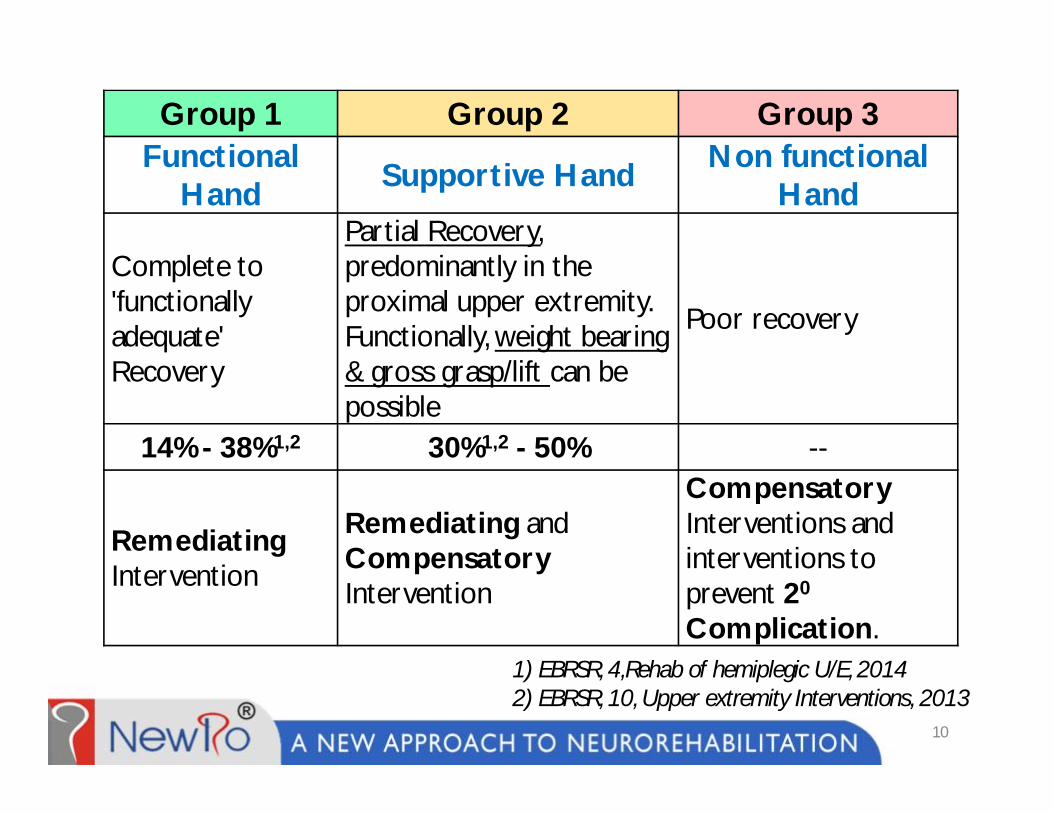
Group 1 Group 2 Group 3Functional
Hand Supportive Hand Non functional Hand
Complete to 'functionally adequate' Recovery
Partial Recovery, predominantly in the proximal upper extremity. Functionally, weight bearing & gross grasp/lift can be possible
Poor recovery
14% - 38%1,2 30%1,2 - 50% --
RemediatingIntervention
Remediating and Compensatory Intervention
Compensatory Interventions and interventions to prevent 20
Complication.
How to do it?
11
Overview
• Interventions for Group 1
• Interventions for Group 2
• Interventions for Group 3
12

Intervention for Group 1
• It’s a continuous process with considerable
overlap between each step
13
1111 2222 3333 4444 5555 66aa66aa 66bb66bb 66cc66ccStep
Intervention For Group 1
–
• Deficits like,
– Diplopia, Photosensitivity, hemianopia etc…
– Neglect, Visual Inattention etc…
– Emotional Lability, attention deficits etc…
Step – 1 : Understand / Management of 'Key' Visual, Perceptual and cognitive Deficits to make the patient 'Ready' for rehabilitation
14
Intervention For Group 1 Contd…
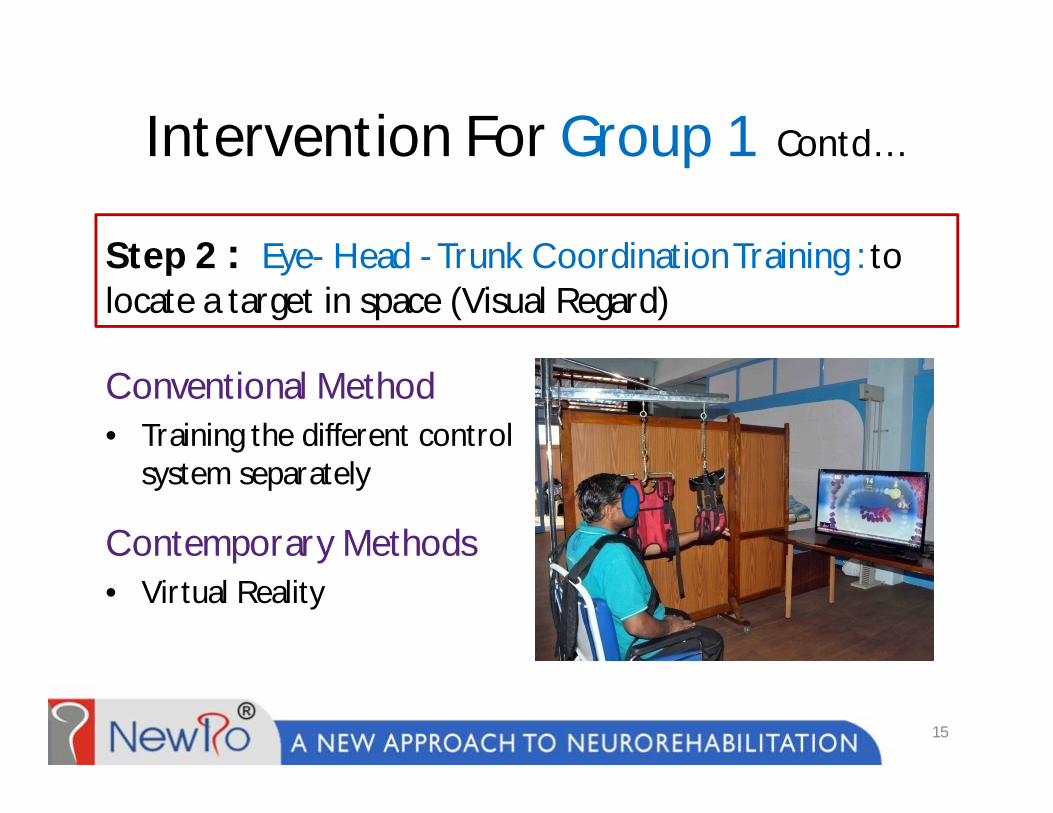
Step 2 : Eye- Head - Trunk Coordination Training : to locate a target in space (Visual Regard)
Conventional Method• Training the different control
system separately
Contemporary Methods• Virtual Reality
15
Intervention For Group 1 Contd…
Two key challenges at this phase are
– Effect of Gravity– Weight of the upper extremity on relatively
unstable shoulder joint
Step-3 : Training for Reach
16
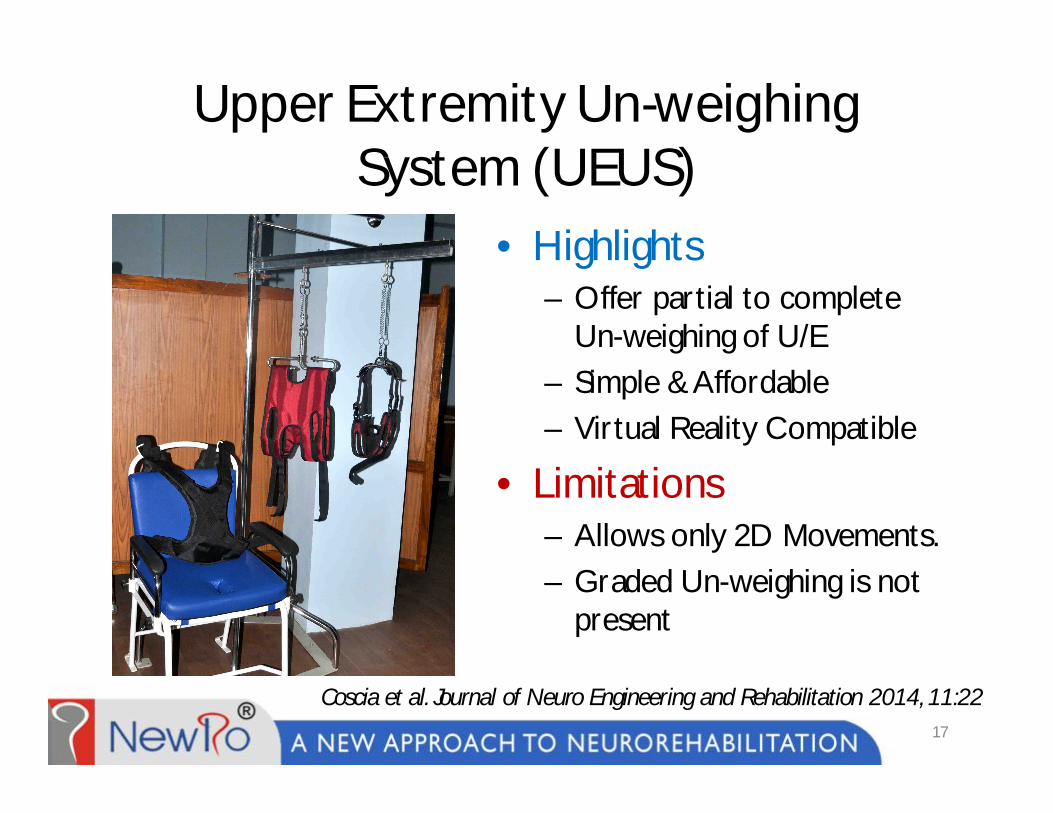
Upper Extremity Un-weighing System (UEUS)
• Highlights– Offer partial to complete
Un-weighing of U/E– Simple & Affordable– Virtual Reality Compatible
• Limitations– Allows only 2D Movements.– Graded Un-weighing is not
present
17
Coscia et al. Journal of Neuro Engineering and Rehabilitation 2014, 11:22
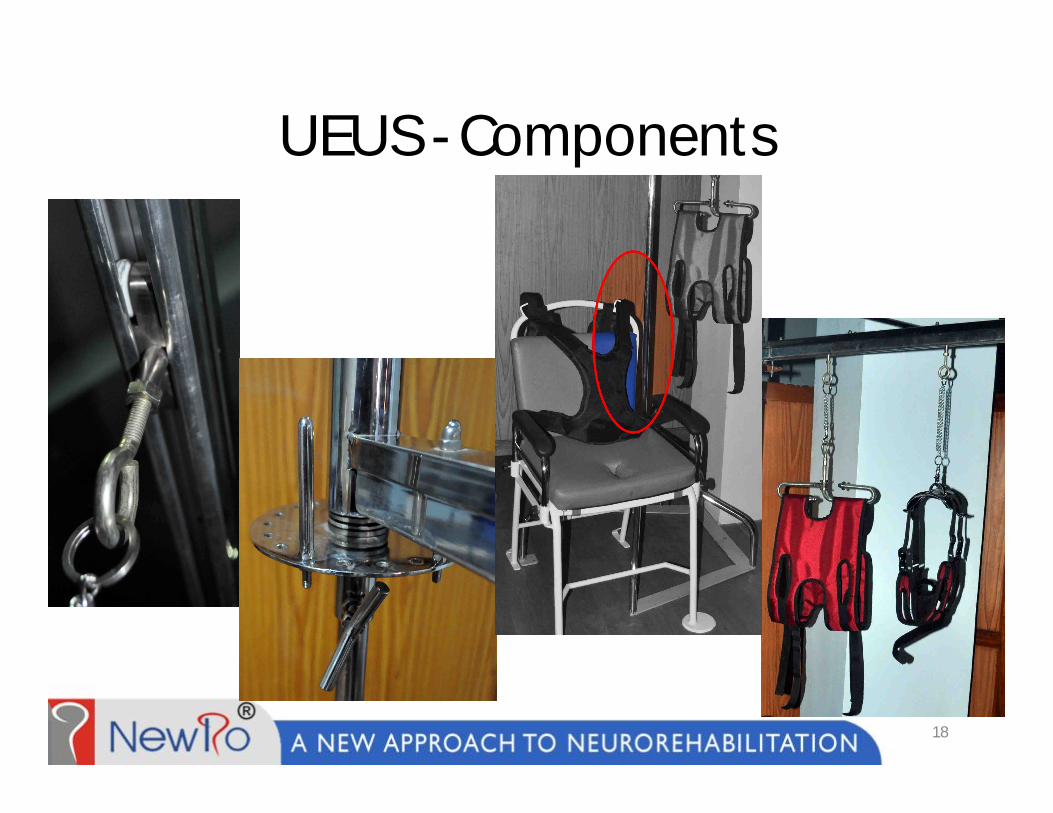
UEUS - Components
18
UEUS & Virtual Reality - Video
19

Step 3 Contd…
Reach against gravity
Key Challenge here is the smooth, graded transition
of reach movement from eliminated gravity to
against gravity
20
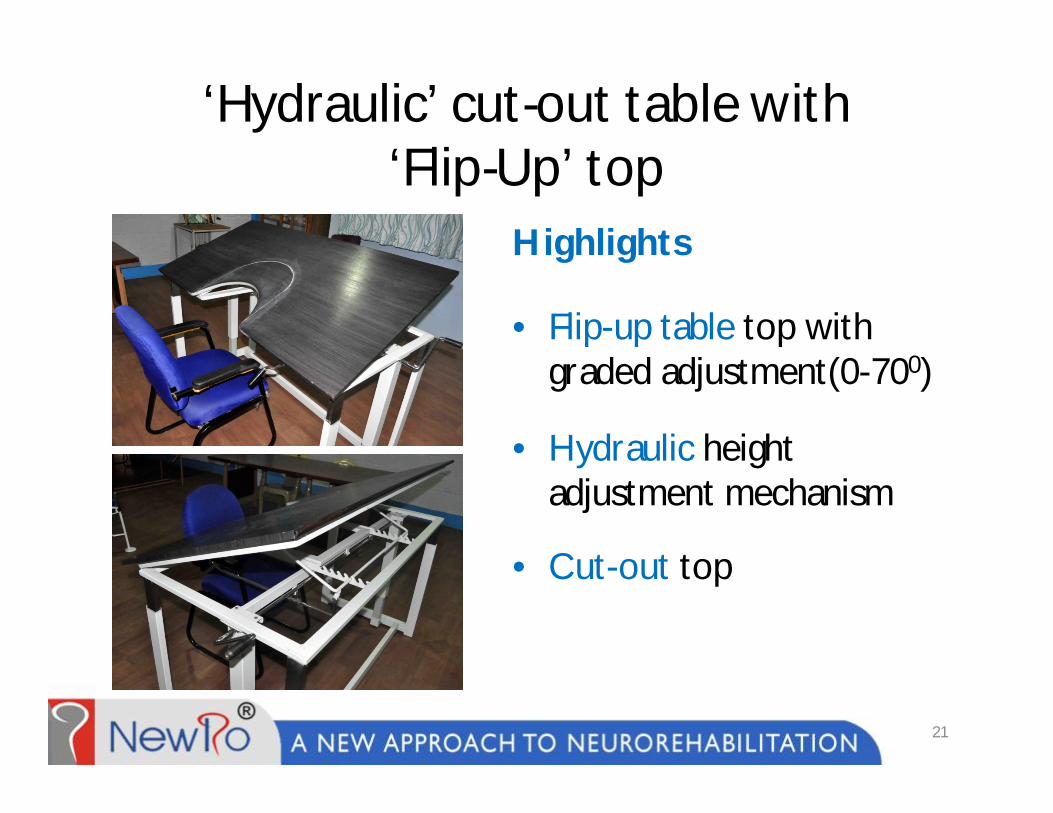
‘Hydraulic’ cut-out table with ‘Flip-Up’ top
Highlights
• Flip-up table top with graded adjustment(0-700)
• Hydraulic height adjustment mechanism
• Cut-out top
21

How does it work?
22
Intervention For Group 1 Contd…
• Synergy patterns can be reversed if movement
takes place in the weaker synergy first
Ref: Chedoke McMaster Stroke Impairment Inventory : Stage 4
Step 4 : Training for Grasp Release (Extension of fingers and thumb)
23
Intervention For Group 1 Contd…
• Initially starts with Gross grasp
• Incorporated with ‘Meaningful activities’
• In a meaningful ‘Context’ (i.e.,Task Oriented)
– Eg: holding a glass of water
Step 5 : Training for Grasp (Flexion of fingers and thumb)
24
Intervention For Group 1 Contd…
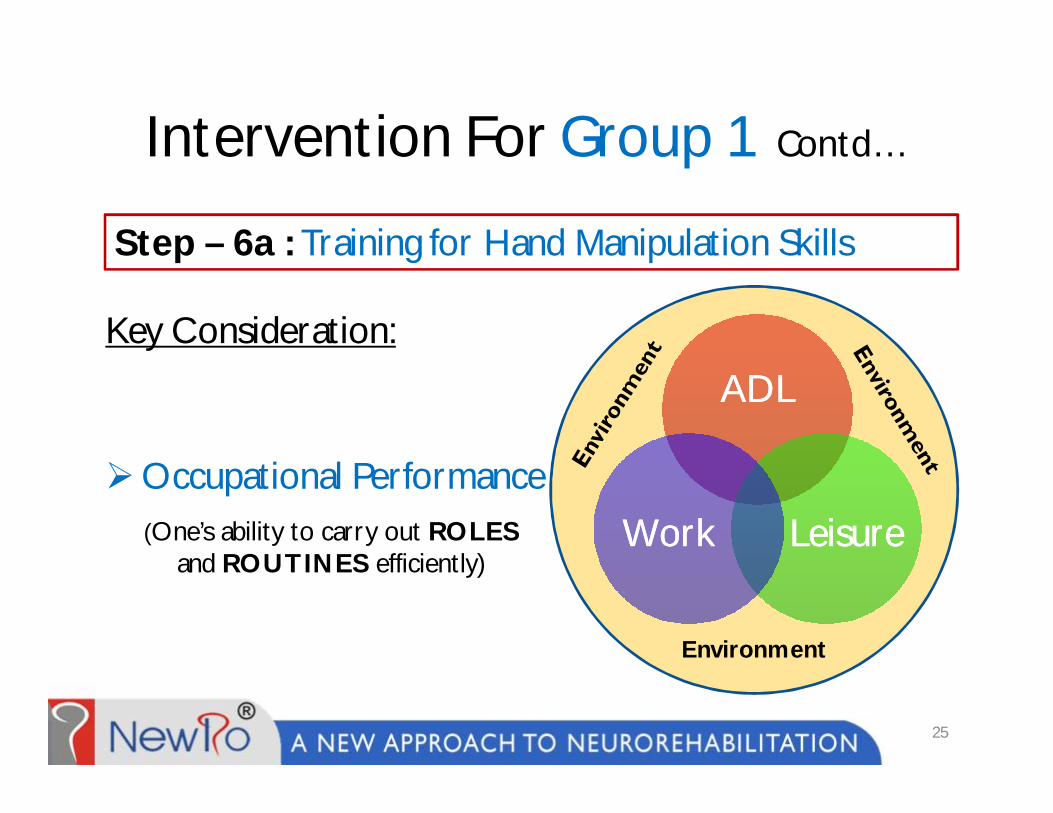
Key Consideration:
Occupational Performance
Step – 6a : Training for Hand Manipulation Skills
ADLADL
LeisureLeisureWorkWork
Environment
25
(One’s ability to carry out ROLESand ROUTINES efficiently)

Therapy through ‘Occupation’
Job specific training (Work) Task specific training (ADL)
26

Therapy through ‘Occupation’
Leisure Diagnosis Specific
Prevocational Training
27
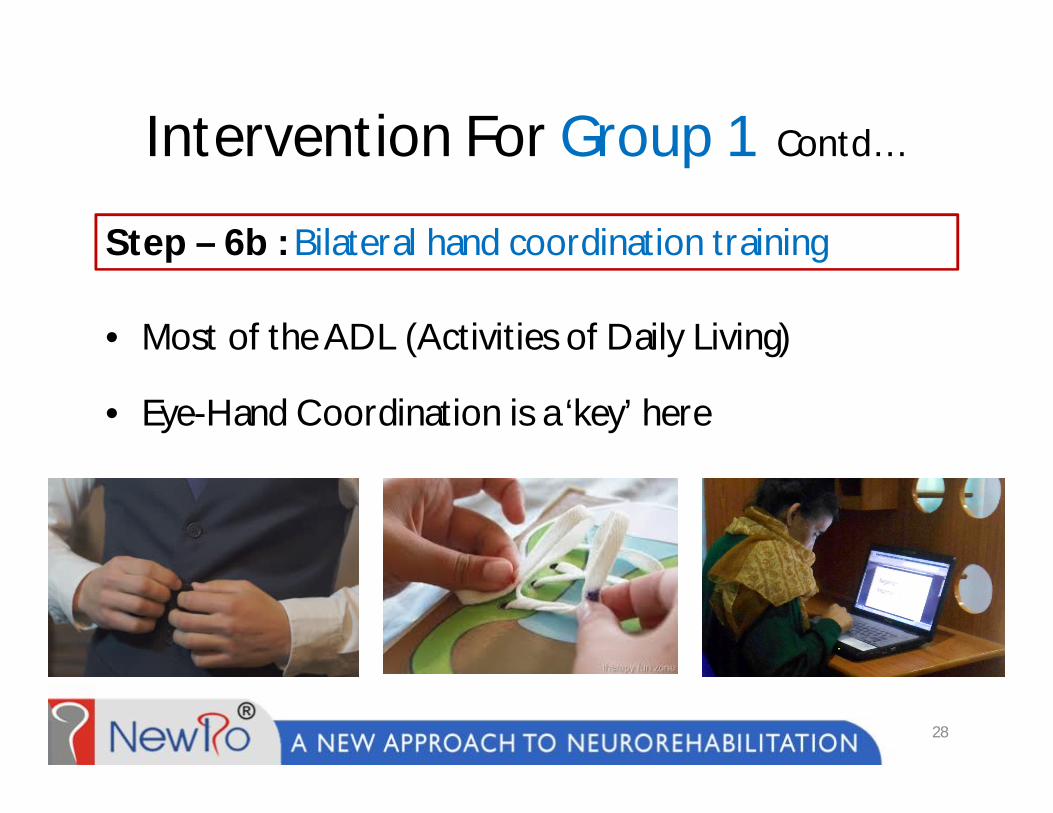
Intervention For Group 1 Contd…
• Most of the ADL (Activities of Daily Living)
• Eye-Hand Coordination is a ‘key’ here
Step – 6b : Bilateral hand coordination training
28
Intervention For Group 1 Contd…
The fruitfulness of rehabilitation lies when the learning at ‘ideal’ environment transforms to the ‘real’ environment
Transfer of Learning– To ADL– To Work– To Lesiure
Step – 6c : Transfer of learning
29

Intervention For Group 1 Contd…
Prevocational Training Unit
30

Intervention For Group 1 Contd…
Kitchen & Homemaking skills Simulation Unit
31
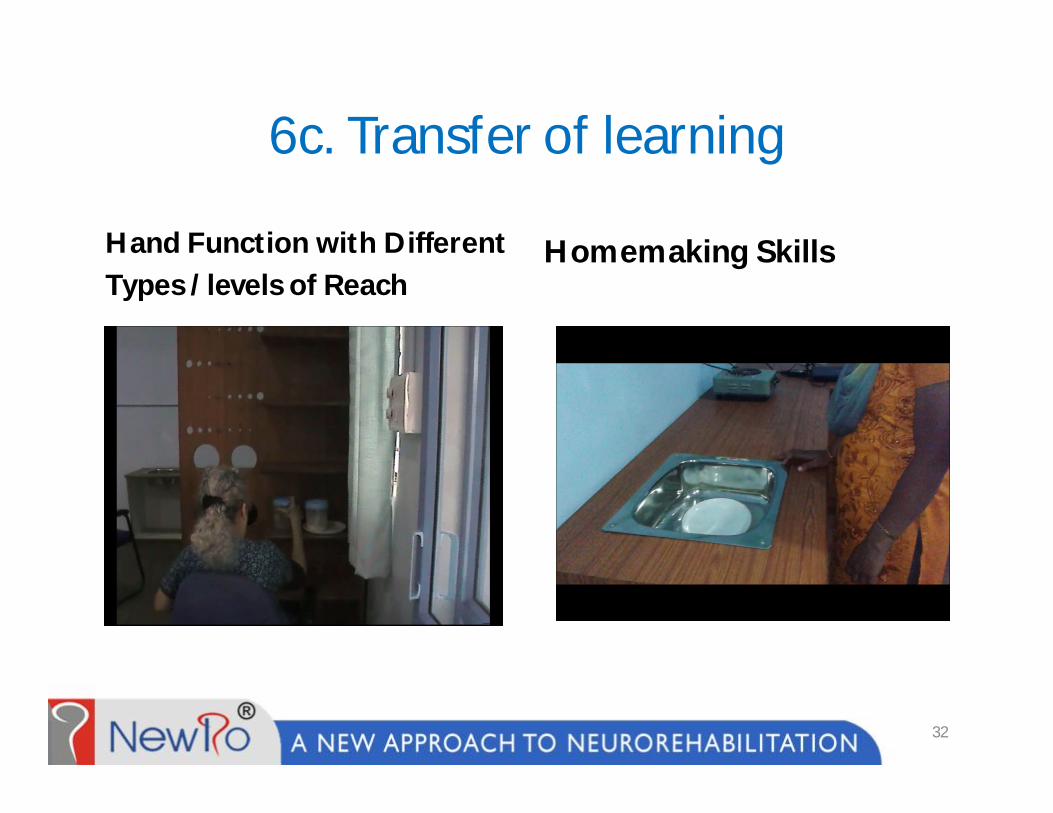
6c. Transfer of learning
Hand Function with Different Types / levels of Reach
Homemaking Skills
32
Overview
• Interventions for Group 1
• Interventions for Group 2
• Interventions for Group 3
33
Interventions for Group 2• For the Affected Hand
– Step 1-3 are same– Training for sustained gross grasp (at least ½
range of digit flexion)– Independent weight bearing on affected hand– Technology /equipments like SaeboFlex™
• For the Un-affected Hand– Compensatory strategy training like ‘one handed
techniques for dressing’
34
Overview
• Interventions for Group 1
• Interventions for Group 2
• Interventions for Group 3
35
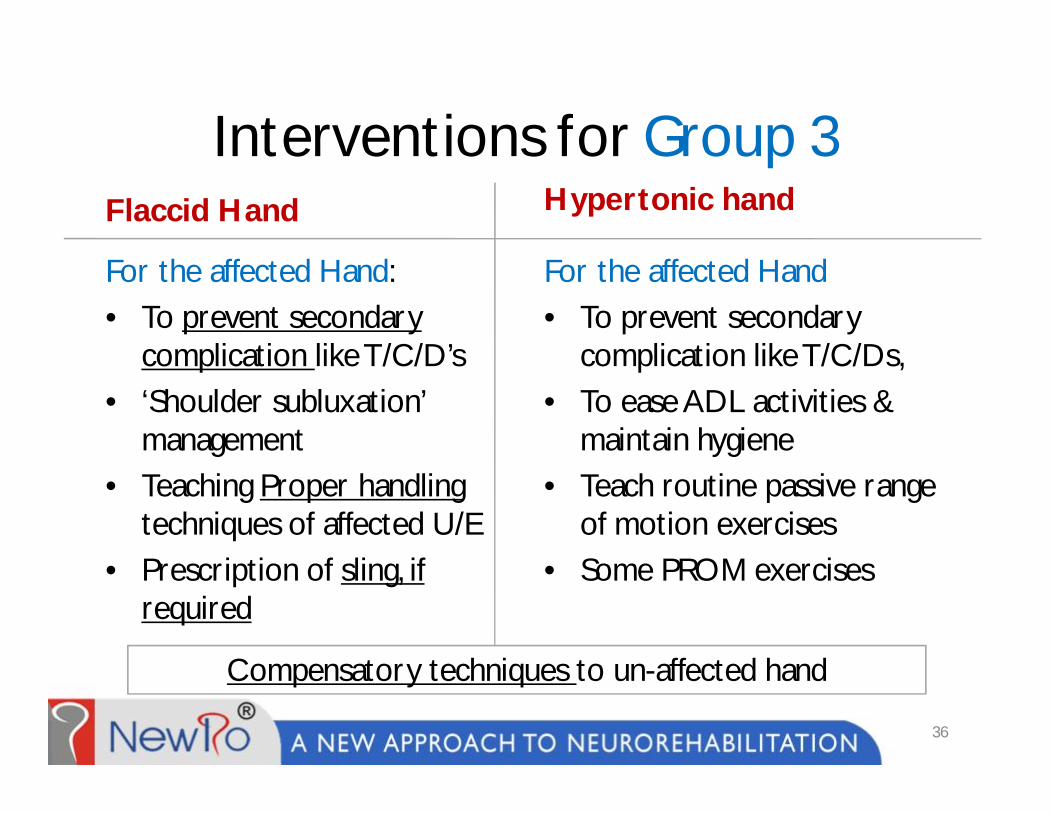
Interventions for Group 3Flaccid Hand
For the affected Hand: • To prevent secondary
complication like T/C/D’s• ‘Shoulder subluxation’
management• Teaching Proper handling
techniques of affected U/E• Prescription of sling, if
required
Hypertonic hand
For the affected Hand• To prevent secondary
complication like T/C/Ds, • To ease ADL activities &
maintain hygiene• Teach routine passive range
of motion exercises• Some PROM exercises
36
Compensatory techniques to un-affected hand

Take Home Message
• Post-stroke U/E rehabilitation should be based on
diagnosis specific and prognostic oriented treatment
planning
• The focus of the therapy SHOULD be on functional
Independence NOT confined to reach, grasp release
37
Key References• Stroke Rehabilitation Clinician Handbook 2014; Chapter 4. Motor
Rehabilitation; Section 4b. Rehab of Hemiplegic Upper Extremity Post Stroke by Robert Teasell and Norhayati Hussein | www.ebrsr.com
• EBRSR (Evidence-Based Review of Stroke Rehabilitation) 2013, Module10, Upper Extremity Interventions by Norine Foley et al | www.ebrsr.com
• ‘Rehabilitation of stroke’ by Paul E Kaplan and Rene Cailliet- Butterworth Heinemann publication
• Effect of Lesion Location on Upper Limb Motor Recovery After Stroke by Fátima de N.A.P. Shelton, MD; Michael J. Reding, MD (Stroke. 2001;32:107-112.) http://stroke.ahajo1u0r7nals.org
• The effect of arm weight support on upper limb muscle synergies during reaching movements by Coscia et al. Journal of NeuroEngineering and Rehabilitation 2014, 11:22 http://www.jneuroengrehab.com/content/11/1/22
38
Acknowledgement
My sincere gratitude to the directors of NewRo,®
my colleagues and friends for their support
39

The Art & Science of Empowering Lives…
40
About the Speaker• Mr. Phinoj K. Abraham has done his Bachelor of occupational
therapy from KMCH college of Occupational Therapy, Coimbatore and his Master of Occupational Therapy (MOTh) in Neurosciences from ‘All India Institute of Physical Medicine and Rehabilitation’ (AIIPMR), Mumbai
• He is currently working as Chief Neuro Occupational Therapist at atNewRo, Bengaluru, India.
• He was working as Asst. Professor in Occupational Therapy at SRMCollege of Occupational Therapy, Chennai.
• He has designed several therapy gadgets and devices like Upper Extremity Un-weighing System (UEUS), Hemiplegic Upper Extremity Orthosis (HUEO), Hydraulic cut-out table with flip up top, prevocational evaluation and workstation etc..
• Contact Email: [email protected]
41