potent clinical and radiological response to larotrectinib ... · potent clinical and radiological...
TRANSCRIPT
Potent clinical and radiological response to larotrectinib in first case of TRK fusion high grade gliomaZiegler DS,1,2 Tsoli M,2 Tyrell V,2 Cohn RJ,1 Lau LMS,1 Cox MC,3 Cowley MJ,2,4,5 Ekert PG,6 Marshall GM,1,2 Haber M2
1Kids Cancer Centre, Sydney Children’s Hospital, Randwick, NSW, Australia; 2Children’s Cancer Institute, UNSW, Sydney, Australia; 3Clinical Development, Loxo Oncology, Inc. South San Francisco, CA, USA; 4Kinghorn Centre for Clinical Genomics, Garvan Institute, Sydney, Australia; 5St Vincent’s Clinical School, UNSW Sydney, Sydney, Australia;
6Murdoch Children’s Research Institute, Royal Children’s Hospital, Melbourne, Australia Abstract EAPH-09
n Somatic oncogenic fusions involving the NTRK1, NTRK2, and NTRK3genes (NTRK gene fusions), which encode the TRKA, TRKB and TRKCreceptor tyrosine kinases, occur in a broad range of solid tumors.
n Beyond embryogenesis, TRK proteins are primarily expressed in thenervous system.1
n The 3 neurotrophin receptors regulate specific normal functions:2-6
– NTRK1 encodes TRKA → Pain, thermoregulation
– NTRK2 encodes TRKB → Movement, memory, mood, appetite, body weight
– NTRK3 encodes TRKC → Proprioception
n NTRK gene fusions are generally rare, but are recurrent oncogenicdrivers.
n NTRK gene fusions are found at high frequencies in certain rare tumortypes and may be oncogenic drivers in up to 1% of all solid tumors.
n In children with non-brainstem high grade gliomas who were less than3 years of age, NTRK gene fusions were identified in 40% of tumors.7
n Larotrectinib is a highly potent small-molecule inhibitor of TRKA, TRKB, andTRKC (5–11 nM IC50 in cellular assays).
n It is highly selective, with little or nointeraction with other kinase and non-kinase targets.8
n Liquid formulation allows dosing ofchildren as young as 1 month of age anddelivers equivalent pharmacokinetics tocapsules.9
n Larotrectinib is highly active in childrenand adults with TRK fusion solid tumors,eliciting durable responses in both.8,9
n Larotrectinib is the first selective TRK inhibitor in clinical development:
– An overall response rate of 80% has been reported in a series of pediatric and adult patients with TRK fusion cancer8
– However, no patients in this cohort had a TRK fusion high grade glioma
n Patient is a 3-year-old girl who was diagnosed with a brain tumor at5 months of age.
n Presented initially with vomiting and seizures; MRI showed aheterogeneous mass measuring 6 x 3 x 2 cm in the right lateralventricle.
n Following gross total resection, pathology showed a high gradeglioma and she was treated with 20 cycles of chemotherapy.
n 4 months after completing treatment, she had disease progression inthe tumor bed with multiple nodules in the lateral and third ventricles.Further tumor debulking confirmed recurrent disease.
n After 6 months, a new mass in the tumor bed was subtotally resected;patient received focal radiotherapy of 54 Gy to the tumor bed. Inparallel, the resected tumor underwent molecular testing on a pilotpersonalized medicine study, to inform therapeutic options forpotential future disease progression:
– Whole genome sequencing of tumor DNA revealed a somatic ETV6-NTRK3 gene fusion (Figure 1); RNA sequencing showed that the ETV6-NTRK3 fusion was robustly expressed.
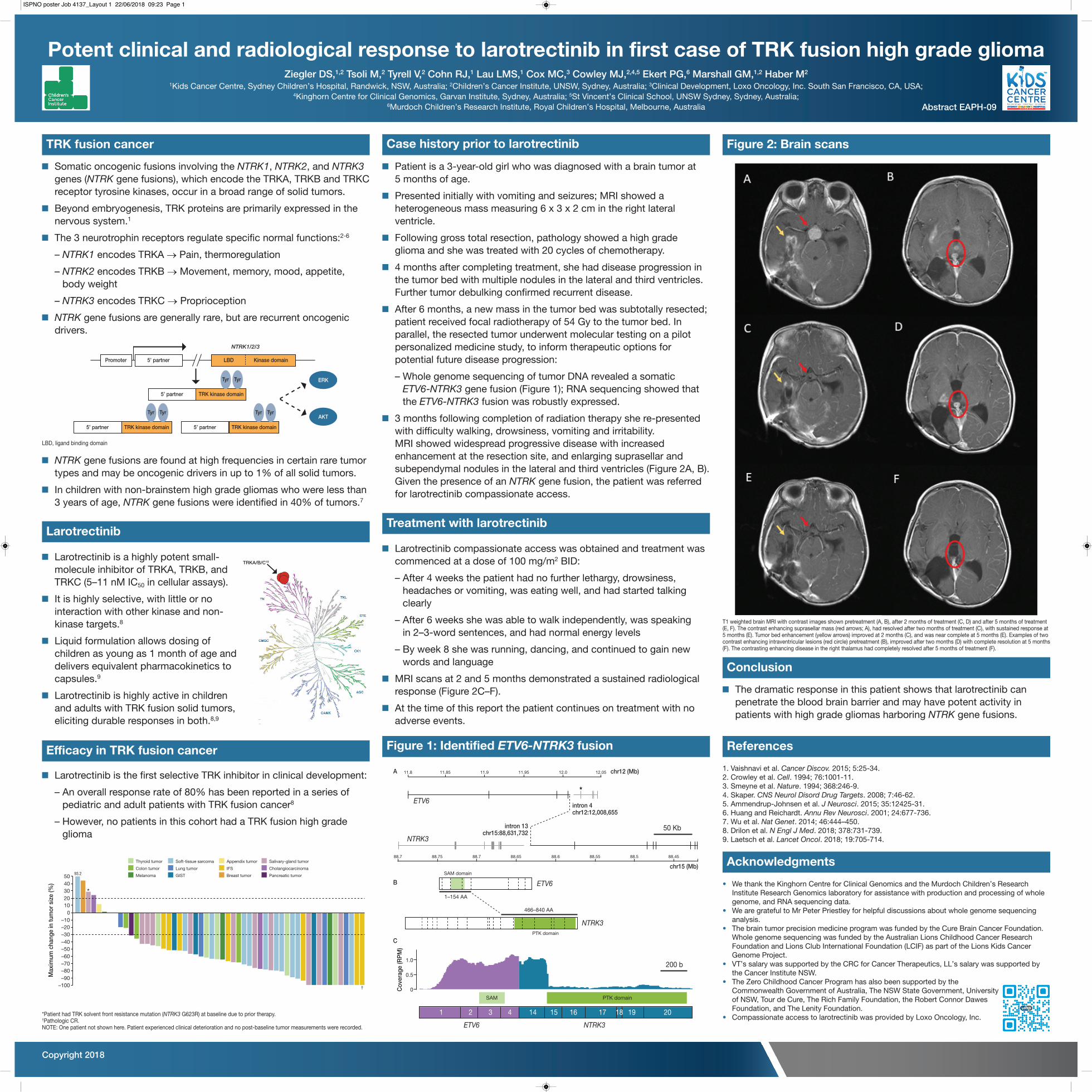
n 3 months following completion of radiation therapy she re-presentedwith difficulty walking, drowsiness, vomiting and irritability.MRI showed widespread progressive disease with increasedenhancement at the resection site, and enlarging suprasellar andsubependymal nodules in the lateral and third ventricles (Figure 2A, B).Given the presence of an NTRK gene fusion, the patient was referredfor larotrectinib compassionate access.
n Larotrectinib compassionate access was obtained and treatment wascommenced at a dose of 100 mg/m2 BID:
– After 4 weeks the patient had no further lethargy, drowsiness, headaches or vomiting, was eating well, and had started talking clearly
– After 6 weeks she was able to walk independently, was speaking in 2–3-word sentences, and had normal energy levels
– By week 8 she was running, dancing, and continued to gain new words and language
n MRI scans at 2 and 5 months demonstrated a sustained radiologicalresponse (Figure 2C–F).
n At the time of this report the patient continues on treatment with noadverse events.
n The dramatic response in this patient shows that larotrectinib canpenetrate the blood brain barrier and may have potent activity inpatients with high grade gliomas harboring NTRK gene fusions.
1. Vaishnavi et al. Cancer Discov. 2015; 5:25-34.2. Crowley et al. Cell. 1994; 76:1001-11.3. Smeyne et al. Nature. 1994; 368:246-9.4. Skaper. CNS Neurol Disord Drug Targets. 2008; 7:46-62.5. Ammendrup-Johnsen et al. J Neurosci. 2015; 35:12425-31.6. Huang and Reichardt. Annu Rev Neurosci. 2001; 24:677-736.7. Wu et al. Nat Genet. 2014; 46:444–450.8. Drilon et al. N Engl J Med. 2018; 378:731-739.9. Laetsch et al. Lancet Oncol. 2018; 19:705-714.
• We thank the Kinghorn Centre for Clinical Genomics and the Murdoch Children’s ResearchInstitute Research Genomics laboratory for assistance with production and processing of wholegenome, and RNA sequencing data.
• We are grateful to Mr Peter Priestley for helpful discussions about whole genome sequencinganalysis.
• The brain tumor precision medicine program was funded by the Cure Brain Cancer Foundation.Whole genome sequencing was funded by the Australian Lions Childhood Cancer ResearchFoundation and Lions Club International Foundation (LCIF) as part of the Lions Kids CancerGenome Project.
• VT’s salary was supported by the CRC for Cancer Therapeutics, LL’s salary was supported bythe Cancer Institute NSW.
• The Zero Childhood Cancer Program has also been supported by theCommonwealth Government of Australia, The NSW State Government, Universityof NSW, Tour de Cure, The Rich Family Foundation, the Robert Connor DawesFoundation, and The Lenity Foundation.
• Compassionate access to larotrectinib was provided by Loxo Oncology, Inc.
TRK fusion cancer
Larotrectinib
Efficacy in TRK fusion cancer
Case history prior to larotrectinib
Figure 1: Identified ETV6-NTRK3 fusion
Treatment with larotrectinib
Figure 2: Brain scans
Conclusion
References
Acknowledgments
Promoter LBD
NTRK1/2/3
Kinase domain5’ partner
5’ partner TRK kinase domain
5’ partner TRK kinase domain 5’ partner TRK kinase domain
Tyr Tyr
Tyr Tyr Tyr Tyr
ERK
AKT
LBD, ligand binding domain
304050
93.2
20*
†
100
Max
imum
cha
nge
in tu
mor
siz
e (%
)
–10–20–30–40–50
Thyroid tumor
–60–70–80–90
–100
Colon tumor
Melanoma
Soft-tissue sarcoma
Lung tumor
GIST
Appendix tumor
IFS
Breast tumor
Salivary-gland tumor
Cholangiocarcinoma
Pancreatic tumor
*Patient had TRK solvent front resistance mutation (NTRK3 G623R) at baseline due to prior therapy.†Pathologic CR.NOTE: One patient not shown here. Patient experienced clinical deterioration and no post-baseline tumor measurements were recorded.
A
B
C
ETV6
ETV6
ETV6 NTRK3
NTRK3
50 Kb
200 b
chr12 (Mb)
chr15 (Mb)
intron 4chr12:12,008,655
intron 13chr15:88,631,732
Cov
erag
e (R
PM
)
★
12.0 12.0511.9511.85
SAM domain
PTK domain
1–154 AA
0
466–840 AA
11.911.8
88.7
0.5
1.0
88.75 88.7 88.65 88.6 88.55 88.5 88.45
NTRK3
SAM PTK domain
1 2 3 4 14 15 16 17 18 19 20
T1 weighted brain MRI with contrast images shown pretreatment (A, B), after 2 months of treatment (C, D) and after 5 months of treatment(E, F). The contrast enhancing suprasellar mass (red arrows; A), had resolved after two months of treatment (C), with sustained response at5 months (E). Tumor bed enhancement (yellow arrows) improved at 2 months (C), and was near complete at 5 months (E). Examples of twocontrast enhancing intraventricular lesions (red circle) pretreatment (B), improved after two months (D) with complete resolution at 5 months(F). The contrasting enhancing disease in the right thalamus had completely resolved after 5 months of treatment (F).
Copyright 2018
TRKA/B/C19
ISPNO poster Job 4137_Layout 1 22/06/2018 09:23 Page 1