precocious puberty - kau puberty dr. abdulmoein eid al-agha consultant, pediatric endocrinologist,...
TRANSCRIPT
Precocious Puberty
Dr. Abdulmoein Eid Al-Agha
Consultant, Pediatric Endocrinologist,
King Abdul Aziz University Hospital, Jeddah, Saudi Arabia

Discussion points
When to say this child is having Precocious puberty (what is the age limits in both sexes)
Types of precocious puberty
Etiology
Biochemical & Radiological investigations
Management
– Who should be treated!
– Treatment options

Puberty
Puberty (Latin pubescere, to be covered with hair)
The stage between the onset of secondary sexual characteristics and the completion of physical maturity
The period in which reproductive capability is attained,manifested by spermatogenesis in males & ovulation in females

Puberty
BRAIN
NEUROTRANSMITTERS
HYPOTHALAMUS
GnRH
PITUITARY GLAND
LH / FSH
GONADS
TESTOSTERONE / E2
ACTIVIN
INHIBIN

Puberty
Normal age
– girls: 9 -13 y (mean age =11 years)
– boys: 11 -15 y (mean age =13 years)
primates
– puberty process happened very quickly within
28 days
Humans
– puberty on hold for a longer period ( 12 y)

Puberty in girls
Psychological / emotional changes
Stages of normal puberty
– Thelarche
– Adrenarche / Pubarche
– Menarche
Pelvic U/S changes of puberty
ovarian volume and follicular size
uterus to cervix ratio
endometrial echo
Skeletal changes in girls
Widening of pelvis and carrying angle
Major increase in BMD
Increased adipose tissue with typical
female distribution
95% of growth happened < menarche
Menarche usually by age 12.5-14.5 yr
Increased in muscle bulk but not to same
extent as males
Puberty
Somatic changes
pubic & axillary hair
acne
perspiration and characteristic body odour
(release of volatile acids= glutaric acid)
oily skin and hair
All these changes happen due to increased
adrenal androgens which are formed equally in
both males and females
– Adrenal androgens
androstenedione, DHEA, DHEAS

Definition of PP
In girls, defined as onset of puberty “breast
enlargement” before age of 8 years
In boys, defined as onset of puberty before
age of 9 years

Definition !!
Recently, many data suggest that girls seen
in sample of pediatric practices from across
the United States are developing pubertal
characteristics at younger ages.
Practitioners may need to revise their
criteria for referral of girls with precocious
puberty, with attention to racial differences !!

Why there is secular trend toward earlier puberty,
especially in girls !!!
Why percentage of girls with
precocious puberty rose from
2.5% in 1969 to 10% in 1990s !!!
1. Increasing % of obesity in girls
2. Environmental estrogen

The Hazards of Environmental Estrogens
World and I magazine; 10/1/2001; Trankina, Michele L.

The Hazards of Environmental Estrogens
Over the past 10 years, many synthetic compounds and plant products present in the environment have been found to affect hormonal functions in various ways
Premature puberty was traced to consumption of beef, and dairy products containing high concentrations of estrogen.
Another study from Puerto Rico revealed higher concentrations of phthalate--a xenoestrogen present in certain plastics--in girls who showed signs of early puberty, compared with controls.
estrogen-like substances in the plastic wrap used on sandwiches for kids' lunches.

It may be that excess of body fat and the exposure
to estrogenic substances operate together to
hasten puberty. Body fat is one site of endogenous
estrogen synthesis. Exposure to environmental
estrogens may add just enough exogenous
hormone to exert the synergistic effect necessary
to bring on puberty, much like the last drop of
water that causes the bucket to overflow !!!!!!!
World and I magazine;
10/1/2001; Trankina, Michele L.

Revised Definitions in girls
USAEurope
< 6 0r 7< 8Precocious
7 - 98 -10Early
> 9> 10Normal
For boys , USA & Europe have same definition !!

Types

Types
Central, True, GnRH dependent
– 89-98% of cases (major type)
Periphral, Pseudo, GnRH Independent
– 10 – 15 % of cases (not major type)
Mixed type
– Started with peripheral with 2ry. activation of central
Isolated Forms
– Thelarche
– Adrenarche

Peripheral typeCentral type
suppressedActivated axisH-P-G axis
Pre-pubertalAdult valuesLH & FSH
High High Sex steroids
Small in size (unless
tumor)
Pubertal sizeGonads
Etiology

Central, True, GnRH dependent
Etiology
Idiopathic
– most girls ( 90 %)
Secondary
– most boys ( 70-80%)

Etiology of CPP
CNS disorders
Hypothalamic Hamartoma
Glioma (NF-1)
Astrocytoma
Craniopharyngioma
Ependymoma, germinoma,
CNS radiation therapy
Post trauma (surgery)

Etiology of CPP
Inflammation (Brain abscesses)
Neurological & mental retardation
Hydrocephalus
prolonged sex steroid exposure associated
with peripheral puberty
Prolonged primary hypothyroidism ( -TSH
stimulates FSH, LH, Prl)

Etiology of peripheral type
Gonadial: McCune-Albright, tumour, cyst
Adrenal: Virilising CAH, tumours
Ectopic: hCG secreting tumours
– Germinoma, Hepatoblastoma
Exogenous source of hormone
Familial male dependent (Testotoxicosis)
Chronic primary hypothyroidism (-TSH stimulates testicular enlargement)

Autonomous gonad steroid production
McCune Albright syndrome– germ line activating mutations of the FSH
receptor
Familial male – dependent precocious puberty – activating mutation of the LH receptor
– The mutation is inherited in an autosomaldominant fashion, although sporadic cases can occur.

Examples of some cases

Six year old girl presented with bilateral breast
enlargement & axillary hair for last six
months, progressive in nature.
On examination, she had B2PH3.
Her investigations showed suppressed
LH/FSH with high estardiol level and high
serum inhibin.
What is most likely diagnosis?
What further investigations needed to be
done?

Diagnosis: Granulosa cell ovarian tumor

Three years old young child presented with 2 day history of menstruation with no any other signs of puberty. No previous similar history, no history of medications nor any trauma.
On examination, she was looking well, no systemic findings with weight and height on 10th.percentile and she was having Tanner stage of B2PH1.there was one large Cafe-au-lait macule
What is the most likely diagnosis?
Mention 4 important investigations
Mention 3 modalities of treatment?

McCune - Albright syndrome
Affects both sexes
Gonad autonomy
(Autonomous gonad steroid production)
Happen more commonly in girls
In girls, the presenting feature is often menses with / without Thelarche
Menses usually happen < 2-3 yrs of age
Activating mutation within exon 8 of Gs gene GNAS 1 on 20q13.2,results in increased activity of the Gs protein & cAMP in the affected endocrine tissue

McCune-Albright Syndrome

Abnormalities in McCune-Albright
syndrome
Endocrine problems
Precocious Puberty ++++
Goiter / Hyperthyroidism +++
Acromegaly / Gigantism ++
Cushing’s syndrome +
Hyperprolactinemia +
Hypophosphatemic rickets +

Abnormalities in McCune-Albright syndrome
Non-endocrine
Cafe-au-lait spot ++++
Fibrous dysplasia of bone ++++
Facial asymmetry ++
Elevated hepatic transaminases ++
G.I polyposis +
Cardiomyopathy +
Arrhythmias +
McCune-Albright syndrome
Estradiol level may be normal or high depending on the stage of development of follicular cyst
Menstrual flow represents estrogen withdrawal following regression of large follicular cyst
Basal and stimulated levels of LH / FSH are supressed in early stage
After many cycles of cysts appearance and regression,maturation of Hypothalamic function develop (2ry. central precocious puberty)

Treatment
Sequential removal of ovarian cyst
Complete removal of ovaries
17- Medroxyprogestrone (Provera)
Estrogen antagonists (Tamoxifen)
Aromatase inhibitors
Cyproterone Acetate (Androcur)
LHRH agonist (central stage)
Two years old toddler brought by her
parents, complaining of bilateral breast bud
for the last 2 months with no other relevant
history or examination findings?
What further important history and
examination you need to confirm?
Mention 3 important investigations?
What is the most likely diagnosis?

Isolated form of pubertal
development
–Premature Thelarche
– Premature Adrenarche
–Premature Pubarche

Premature Thelarche
Premature breast enlargement with absence of growth spurt
Bone age is not accelerated
Pre pubertal pelvic U/S findings
Onset between 6 m to 4 y of age
Increased sensitivity of the breast tissue to low levels of sex steroids
Benign nature & need no therapy
Eight year old brought by her mother because
of smelly body odor. On examination, she
was having hairy lips, hyperpigmentations,
hoarse voice and acne. Her bone age was
advanced ?
What is the most likely diagnosis?
Mention important 5 investigations?
Mention how to treat this girl?
Premature Adrenarche
Occurs when the adrenal side of puberty is
turned on prematurely in the absence of
gonadal activation
Premature appearance of pubic and axillary
hair, acne, body odor & oily skin
Idiopathic

Premature Adrenarche
Elevated adrenal androgens
Normal LH / FSH & gonadal
steroids
Need to exclude late-onset CAH
Need to exclude adrenal tumours
Need to exclude PCOS

Diagnostic work-up

Evaluation of Precocious Puberty
History
physical examination
Growth percentiles
Calculation of target height
Bone Age assessment
Predicted adult height (PAH)
Basal LH, FSH and sex steroids
GnRH stimulation test
History
Age when secondary sexual development were noted
What features are present ?
Order of appearance of secondary features– Is it usual sequence or not ?
– Virilization symptoms Pubic/ axillary hair
Body odor
– Breast enlargement
– Vaginal discharges & menarche
– Cyclical mood changes

History
Evidence of recent growth acceleration
Family history of early puberty
– Age of parent puberty
Past history of adoption or early weight
gain
History of medications

Examination
Tanner staging
Degree of Virilization
– Clitromegaly in girls indicate abnormal androgen
Visual field assessment & fundoscopy
Abdominal masses
Skin (café-au-lait patches in McCune –Albright
syndrome, NF)
Assessment of height and height velocity

Clinical Measurements
– Standing height (Harpenden stadiometer)
– BMI
– Growth velocity (growth spurt)
– MPH
– Tanner staging of pubertal development
– Bone age (assessed by endocrinologist)
– PAH

Tanner Staging

Laboratory Studies
Sex steroid levels– Basal LH, FSH
GnRH stimulation test– A definitive CPP diagnosis is confirmed by a brisk rise
in LH 20-40 minutes after infusion of GnRH (100 mcg), which is more than the rise in FSH.
– No increase in LH and FSH after infusing GnRHsuggests precocious pseudo-puberty.
– Pre-pubertal girls with premature Thelarche sometimes show an exaggerated rise in FSH after GnRH.
– “FSH predominant response” An FSH rise more than the LH rise does not indicate CPP

hCG
– hepatoblastoma, germinoma
17 OHP &11DOC
– CAH
Thyroid tests are not a routine requirement
Bone Age
A radiograph of the
hand and wrist to
determine bone age
is a quick and useful
means to estimate
the likelihood of
precocious puberty
and its speed of
progression
Imaging Studies
MRI Brain
– Perform an MRI after hormonal studies (GnRHtest) to confirm a CPP diagnosis.
– Ask the radiologist to do a high-resolution study focusing on the hypothalamic-pituitary area.
– The younger girls with CPP, the greater the chance of finding CNS pathology girls younger than 6 y.
For boys younger than 9 years, the incidence of CNS findings is much higher than in girls, and MRI should be part of the evaluation.

In recent years, MRI has become the imaging method of choice in the assessment of CPP
MRI now allows the identification of previously unseen intracranial abnormalities in CPP, thus reducing the number of cases previously considered to be 'idiopathic.'

Pelvic ultrasound – Ultrasound is unnecessary for girls with a definite
diagnosis of CPP.
– If performed, however, ultrasound usually shows bilaterally enlarged ovaries, often with multiple small follicular cysts, and an enlarged uterus with an endometrial stripe.
– Pelvic ultrasound is essential when precocious pseudo-puberty is suspected (based on examination or hormone levels) because an ovarian tumor or cyst may be detected.
U/S Testes
Adrenal U/S

Treatment

Why do we need to treat ??
Main problems (Boys)
– eventual short stature
– psychological issues
– aggressiveness
– inappropriate libido
Main problems (Girls)
– eventual short stature
– psychological issues
– inability to cope with menstruation
– risk of child abuse
Goals of treatment
Decrease the progression of pubertal
changes
Decrease bone maturation
Increase the predicted final adult height
Psychosocial and behavioral therapy

Modalities of treatment CPP
Surgical Care– When CPP is caused by a CNS tumor other than a
Hamartoma, perform a resection to the extent possible without impinging on vital structures such as the optic nerves.
Radiation therapy – often is indicated if surgical resection is incomplete.
Unfortunately, removal of the tumor rarely causes regression of precocious puberty.
Medical Care
Gonadotropin-releasing hormone (GnRH) agonists

Do All Idiopathic Central Precocious Puberty
Require Gonadotropin-Releasing Hormone
Agonist Treatment?
Important questions prior starting GnRHa
How early is the onset of puberty?
How much advancement of the bone maturation?
What is the predicted adult height (PAH)?
Comparison of PAH to MPH ?
How fast the progression of physical changes?
GnRH stimulation test ?

Important questions prior starting GnRHa
Is the child also deficient in GH?
Has psychosocial well-being been
compromised?
Is treatment likely to improve the quality of
life?
Are the anticipated gains worth the
potential expense & complications of
therapy?

Very important issue is the distinction
between the non –progressive forms of
CPP with respect to auxological effects
on growth and whether there is need to
start treatment !

GnRH agonists
First reported in 1981
The treatment of choice of CPP
Alteration of peptide sequence of native GnRH with more potency, affinity to the receptors
Acts continuously with down regulation of GnRH receptors


GnRH agonist
Daily S/C preparation
• Desoriline
4-8 ug/kg/d
• Busereline
20-40ug/kg/d
• leuprolide
20-50 ug/kg/day
• Nafarelin(intranasal)
800-1600ug/kg/day
Depot-preparations
• Leuprorelin acetate
(Lupron)
0.3 mg / kg (7.5 mg)
• Tryptorelin
(Decapeptyl)
50-100ug/kg
• Goserelin (Zoladex)

Response to therapy
Suppression of endogenous LH / FSH
should be confirmed by GnRH test after 3m
and then bi-annually
Testosterone and E2 with in 1-2 Wk
Regression of Pubertal changes

Adverse effects
Anaphylactic reactions: angioedema, urticaria
Local skin reactions : redness,swelling, itchiness and sterile abscesses
Flare – up phenomena
– initial activation of HPG axis with worsening of symptoms
Under treatment
Results in stimulation rather suppression of central axis

Final Height After GnRHa Treatment for
Central Precocious Puberty
Bone age (BA) and chronological age (CA) at start of treatment, as well as BA advance at cessation of treatment, were the most important variables influencing height gain in multiple regression analysis.
BA advance at start of treatment was most important in simple correlation.
In girls, GnRHa treatment seems to restore FH into the target range.
A younger age and advanced bone age at start of treatment are associated with more height gain from GnRHa treatment.


Treatment - Conclusion
1) The use of long-acting (GnRH) agonists may not be indicated in slowly progressive variants or borderline early puberty because they do not affect final height.
2) Preservation of height potential is particularly obvious in precocious puberty starting at young ages.
3) In some selected patients, associated growth hormone therapy may increase adult height but
further studies are warranted.

Combined use of GH& GnRHa
It appears that patients with CPP who grow poorly during GnRHa therapy may have alterations in their GH-IGF-I axis.
This may be attributable to an exaggerated and sustained decrease in the secretion of GH with the withdrawal of sex steroids after the GnRHa therapy has been initiated.
Treatment to slow skeletal maturation in the face of suppressed GH secretion will still result in compromised adult height.
This has led some investigators to speculate that at least a subset of patients with CPP would benefit from the addition of GH therapy to the GnRHa treatment.

The results of such treatment first were reported in 1991 by Oostdijk et al in a study of 3 girls with growth velocities less than the 25th percentile for chronologic age after 3 years of treatment with deslorelin.
Treatment with GH was then started, and after 18 months of combination therapy, all the girls' predicted adult heights had improved (statistical analysis not published).
Since then, additional studies have addressed the question of whether combination therapy improves the predicted adult height in children with idiopathic CPP.
Pediatrics;1999; Pescovitz, Ora Hirsch

Effects of combined Gonadotropin-releasing
hormone agonist and growth hormone therapy on
adult height in precocious puberty
Pucarelli I ,et.al J Pediatr Endocrinol Metab. 2003
Sep;16(7):1005-10.

Combined use of GH& GnRHa
CONCLUSIONS
The primary goal of GnRHa therapy in CPP is to maintain normal height potential,
It is disturbing that not all patients attain adult heights that are within their genetic target ranges.
The effect of GnRHa therapy on the growth axis still is not completely clear, but it is apparent that some children have significant deceleration of their growth velocity, sometimes in association with decreases in GH and IGF-I levels, during treatment.
In fact, decreased secretion of IGF-I may even occur in treated patients with normal growth.

The published studies do suggest a real benefit from adding GH to GnRHa therapy in children with suboptimal growth during GnRHa therapy.
However, the studies have been small and have not all included control groups, and that the sole study that followed the subjects to adult heights found only a modest improvement.
Studies in short normal children and GH-deficient children who are treated with a combination of GH and GnRHa to improve adult heights have yielded encouraging, yet somewhat limited, results as well
Combination therapy could be a viable treatment option in some children with CPP, but additional studies are needed before widespread clinical use outside of a research setting can be recommended.
Conclusions

GnRH antagonist
act by competitive binding to the pituitary GnRH
receptors, thereby preventing the action of
endogenous GnRH - theoretically offering a more
direct and dose-dependent treatment
The antagonist available today in Germany is a
concomitant in assisted reproduction with only 1 -
3 days duration.
long-acting depot preparations of other GnRH
antagonists are in developing phase

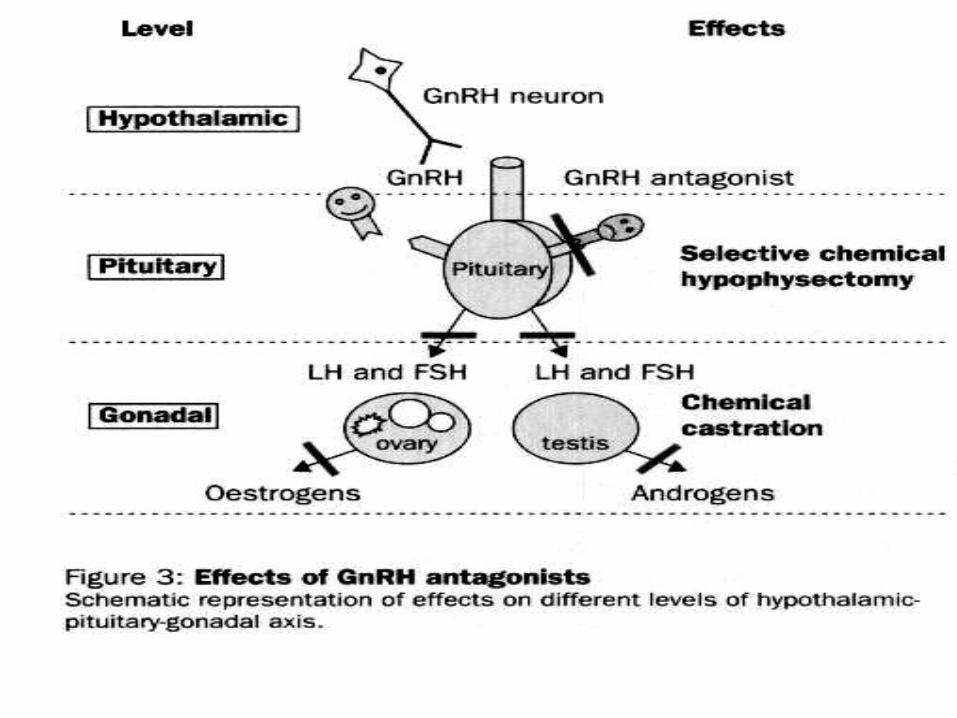

GnRH antagonist
Antagonists such as Abarelix-Depot bind to GnRH
receptors and turn them off, causing an immediate
and complete decline in sex hormones production
to the level of medical castration.
The immediate suppression of the pituitary
achieved by GnRH antagonists without an
initial stimulatory effect is the main advantage
of these compounds over the agonists.
The main disadvantages of the antagonists
are that they are expensive

Other Medications !!

Cyproterone Acetate (Androcur)® in the
Treatment of Precocious Puberty
CPA was found effective in persistently suppressing pituitary gonadotropic secretion when administered orally at a dose of 50 mg bid.
After the introduction of gonadotropic analogues (GnRHa) for treatment of central precocious puberty, short term use of CPA was found useful to counteract the initial initial'flare-up' of the pituitary-gonadal axis, followed by a reduced luteinising hormone secretion by desensitization of pituitary GnRH receptors
Other indications for CPA treatment during childhood and adolescence,– congenital adrenal hyperplasia
– Acne
– Hirsuitism

Treatment of peripheral type
Medical therapy
Medroxyprogestrone acetate (Provera)
Ketoconazole
Aromatase enzyme inhibitors (testolctone)
Androgen antagonists
Surgical treatment of underlying pathology if present

Medroxyprogestrone acetate (Provera)
Before availability of GnRH agonists, this category was the mainstay of therapy.
Progestin work by providing feedback suppression of pituitary Gonadotropin secretion.
They lack significant androgenic or estrogenic activity.
Not expensive treatment
Can stop menstruations, but has no much role in improvement of PAH
Can be a good choice to those who present late

Medroxyprogestrone acetate (Provera)
Structurally similar to glucocorticoid
Progestational agent which suppresses gonadotrophin
Useful in the treatment of both types
Effective in halting the advancement of secondary characters in both sexes
Effective in preventing menstruation
No effects on bone maturation
Dose : 100-200 mg/m2 IM q2wk

ketoconazole
Anti-fungal with side effect of the inhibition of both steroidogenesis and testosterone synthesis at 17,20 Lyasestep
Dose 400-600 mg/day
Suppression happen with in 48 h
Potential hepatotoxic

Aromatase Inhibitors Aromatase enzyme converts
– Androstedione to estrone
– Testosterone to estradiol
Decreasing level of estradiol and receptor affinity has major rule in decreasing bone maturation and give more chance of delayed epiphysis closure in both sexes
Many researches going on currently, to use of this category in those with advanced bone age and short stature to improve PAH, especially those with verilizing CAH, who present late with precocious puberty & advanced bone age

Aromatase Inhibitors
First generation
– Testolactone
Second generation
– Formastine, Plomestane, Atamestane,
Minamestane, Exemastane
Third generation
– Anastrazole (Arimidex)
– Letrazole (Femara)

Aromatase Inhibitors
Testolactone (Teslac) is a competitive
steroidal aromatase inhibitors
Combined with Spirinolactone is useful in
treatment of familial Testotoxicosis
Dose 20 mg/kg/day initially then 40
mg/kg/day divided into 4 doses

Anti - Androgens
1. Intra – Adrenal blockage of androgen production
– Ketoconazole
– Blocks adrenal steroid production at several
enzymatic steps
– Considered to be “ reversible medical adrenalectomy”
2. Peripheral blockage of androgen action
– Anti- Androgens:
Spirinolactone (aldactone)
Cyproterone acetate (Androcur)®
Finasteride = 5 - reductase enzyme inhibitor
– Androgen receptor-blockers:
Flutamide
