precocious puberty - univ-tlse3.fr precoce nejmag carel 2008.pdf · loss due to precocious puberty...
TRANSCRIPT

clinical practice
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 358;22 www.nejm.org may 29, 20082366
Precocious PubertyJean-Claude Carel, M.D., and Juliane Léger, M.D.
From the Department of Pediatric Endo-crinology and Diabetology, INSERM Unité 690, and Centre de Référence des Mala-dies Endocriniennes de la Croissance, Robert Debré Hospital and University of Paris 7 — Denis Diderot, Paris (J.-C.C., J.L.). Address reprint requests to Dr. Carel at Endocrinologie Diabétologie Pédiatrique and INSERM U690, Hôpital Robert Debré, 48, Blvd. Sérurier, 75935 Paris CEDEX 19, France, or at [email protected].
N Engl J Med 2008;358:2366-77.Copyright © 2008 Massachusetts Medical Society.
The parents of a 6-year-old girl bring her to a pediatrician because of breast develop-ment. Her medical history is unremarkable. The parents are of average height, and the mother reports first menstruating when she was 11 years old. At physical exami-nation, the girl is 125 cm tall (in the 97th percentile for her age), weighs 28 kg, and has a body-mass index (the weight in kilograms divided by the square of the height in meters) of 17.9 (90th percentile for her age). Her pubertal development is classified as Tanner stage 3 breast development and Tanner stage 2 pubic hair development. A re-view of her previous growth data indicates that she has grown 8 cm during the past year. How should her condition be evaluated and managed?
The Cl inic a l Problem
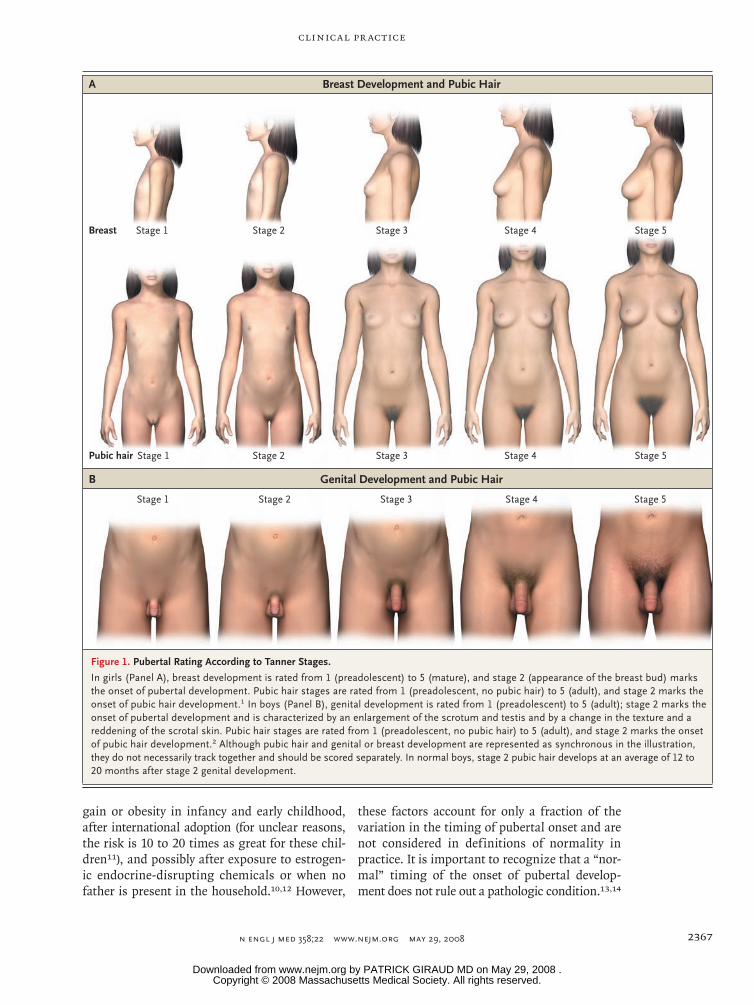
Puberty results when pulsatile secretion of gonadotropin-releasing hormone (GnRH) is initiated and the hypothalamo–pituitary–gonadal axis is activated. Tanner stages (Fig. 1) are used to evaluate pubertal development. The onset of puberty is marked by breast development in girls (Tanner stage 2 breast development, best assessed by both inspection and palpation) and testicular enlargement in boys (Tanner stage 2 genital development, assessed as testicular volume greater than 4 ml or testicular length greater than 25 mm).1,2 Physicians evaluating patients with suspected preco-cious puberty should address several questions: Is pubertal development really oc-curring outside the normal temporal range? What is the underlying mechanism, and is it associated with a risk of a serious condition, such as an intracranial lesion? Is pubertal development likely to progress, and if so, would this impair the child’s normal physical and psychosocial development?
Cross-sectional data obtained in the 1960s led to designation of the normal age range of pubertal onset (the age at which 95% of children attain Tanner stage 2) as between 8 and 13 years in girls and between 9 years 6 months and 13 years 6 months in boys.1,2 More recently, cross-sectional data obtained in the United States indicated that pubertal milestones were being reached earlier than previous-ly thought by black girls and to a lesser extent by Mexican-American and white girls.3-6 These observations led to recommendations to classify pubertal development as precocious when it occurs before the ages of 6 years in black girls and 7 years in all other girls.7 However, the validity of these recommendations has been ques-tioned, and most pediatric endocrinologists in the United States use the traditional threshold of 8 years to define precocious pubertal development in girls.8 Although a similar tendency toward earlier puberty was also noted in Europe, the shift was less marked, and there, the lower end of the normal range for the onset of puberty is also 8 years in girls and 9 years 6 months in boys.9
The onset of puberty is affected by many factors in addition to race10; it occurs earlier in girls with early maternal menarche, low birth weight, or excessive weight
This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines,
when they exist. The article ends with the authors’ clinical recommendations.
Copyright © 2008 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by PATRICK GIRAUD MD on May 29, 2008 .
clinical pr actice
n engl j med 358;22 www.nejm.org may 29, 2008 2367
gain or obesity in infancy and early childhood, after international adoption (for unclear reasons, the risk is 10 to 20 times as great for these chil-dren11), and possibly after exposure to estrogen-ic endocrine-disrupting chemicals or when no father is present in the household.10,12 However,
these factors account for only a fraction of the variation in the timing of pubertal onset and are not considered in definitions of normality in practice. It is important to recognize that a “nor-mal” timing of the onset of pubertal develop-ment does not rule out a pathologic condition.13,14
05/13/08
AUTHOR PLEASE NOTE:Figure has been redrawn and type has been reset
Please check carefully
Author
Fig #Title
ME
DEArtist
Issue date
COLOR FIGURE
Version 4Carel1
LAM
05/29/08
Precocious puberty
CSIK
Genital Development and Pubic Hair
Breast Development and Pubic Hair
Stage 5Stage 4Stage 3Stage 2Stage 1
A
B
Breast
Pubic hair
Stage 1 Stage 2 Stage 3 Stage 4 Stage 5
Stage 1 Stage 2 Stage 3 Stage 4 Stage 5
Figure 1. Pubertal Rating According to Tanner Stages.
In girls (Panel A), breast development is rated from 1 (preadolescent) to 5 (mature), and stage 2 (appearance of the breast bud) marks the onset of pubertal development. Pubic hair stages are rated from 1 (preadolescent, no pubic hair) to 5 (adult), and stage 2 marks the onset of pubic hair development.1 In boys (Panel B), genital development is rated from 1 (preadolescent) to 5 (adult); stage 2 marks the onset of pubertal development and is characterized by an enlargement of the scrotum and testis and by a change in the texture and a reddening of the scrotal skin. Pubic hair stages are rated from 1 (preadolescent, no pubic hair) to 5 (adult), and stage 2 marks the onset of pubic hair development.2 Although pubic hair and genital or breast development are represented as synchronous in the illustration, they do not necessarily track together and should be scored separately. In normal boys, stage 2 pubic hair develops at an average of 12 to 20 months after stage 2 genital development.
Copyright © 2008 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by PATRICK GIRAUD MD on May 29, 2008 .

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 358;22 www.nejm.org may 29, 20082368
The prevalence of precocious puberty is about 10 times as high in girls as in boys, with an esti-mated prevalence of 0.2% among girls and less than 0.05% among boys in Denmark.15
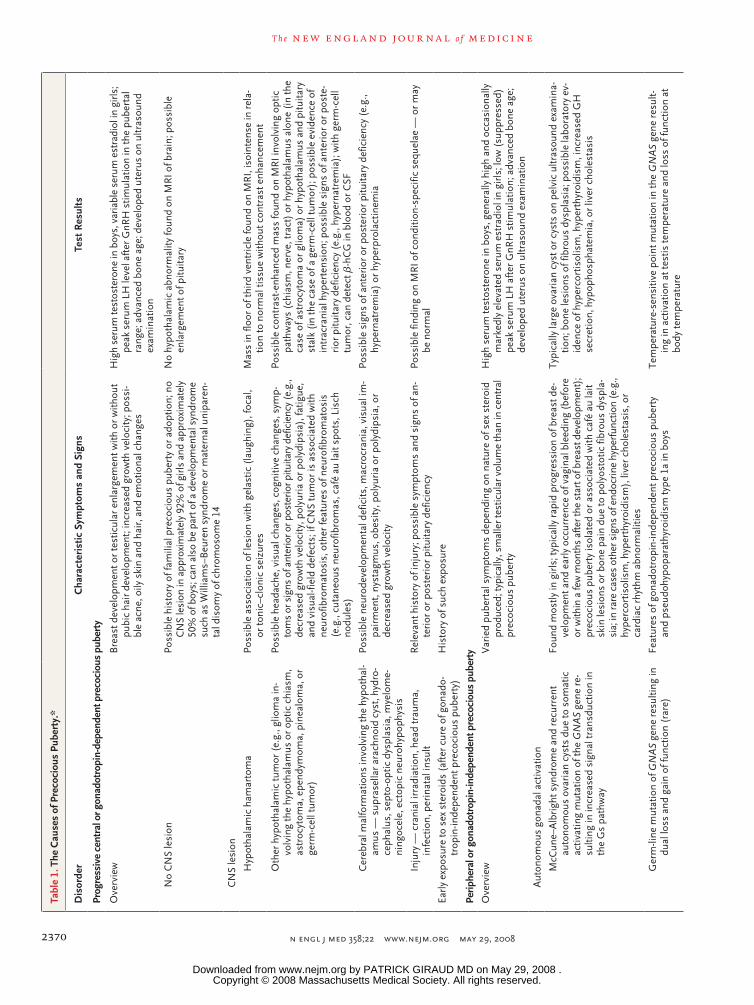
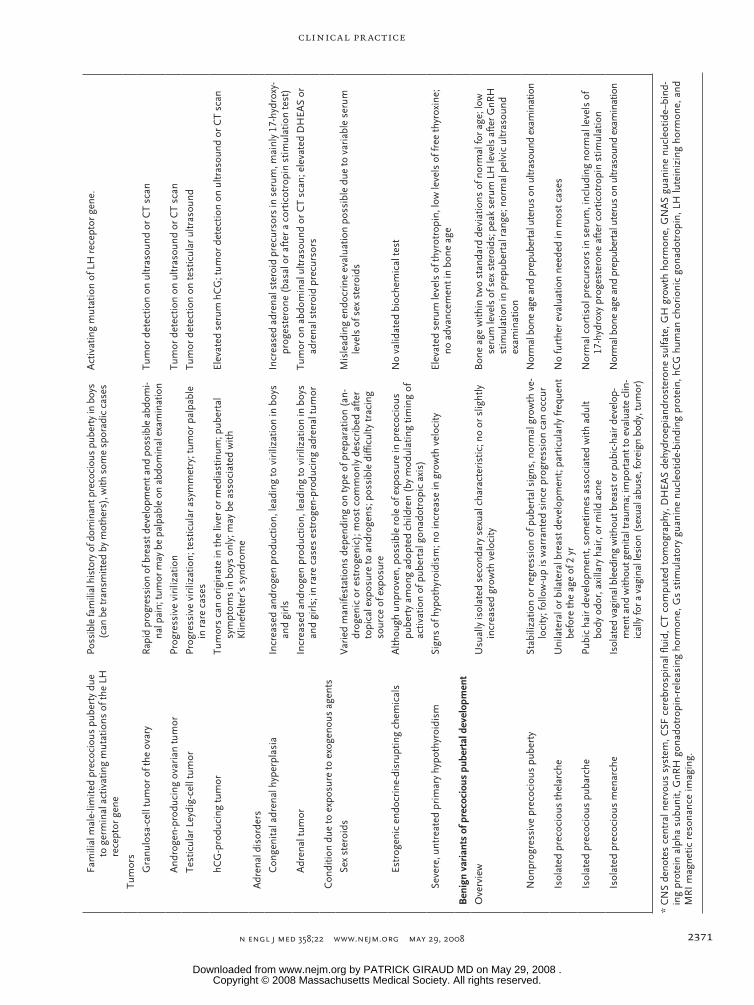
The most common mechanism of progressive precocious puberty is the early activation of pul-satile gonadotropin-releasing hormone (GnRH) secretion (central or gonadotropin-dependent pre-cocious puberty), which may result from hypotha-lamic tumors or lesions but in most cases remains unexplained (Table 1).16 Several causes of periph-eral or gonadotropin-independent puberty are rec-ognized, including gonadal and adrenal tumors and tumors producing human chorionic gonado-tropin, activation of mutations in the gonado-tropic pathway, and exposure to exogenous sex steroids (Table 1). Peripheral precocious puberty can lead to activation of pulsatile GnRH secre-tion and to central precocious puberty.
In at least 50% of cases of precocious pubertal development, pubertal manifestations will regress or stop progressing, and no treatment is neces-sary.17 Although the mechanism underlying these cases of nonprogressive precocious puberty is un-known, the gonadotropic axis is not activated. For cases in which precocious puberty progresses, concerns include early menarche in girls and short adult stature due to early epiphyseal fusion and adverse psychosocial outcomes in both sexes.18 Parents often seek treatment in girls because they fear early menarche,19 but it is difficult to predict the age at which menarche will occur after the onset of puberty. In the general population, the time from breast development to menarche is longer for children with an earlier onset of pu-berty, ranging from a mean of 2.8 years when breast development begins at the age of 9 years to 1.4 years when breast development begins at the age of 12.20
Several studies have assessed adult height in people with a history of precocious puberty. In older published series of untreated patients, mean heights ranged from 151 to 156 cm in boys and from 150 to 154 cm in girls, corresponding to a loss of about 20 cm in boys and 12 cm in girls as compared with normal adult height.21 Height loss due to precocious puberty is inversely corre-lated with the age at the onset of puberty, and today, treated patients tend to have a later onset of puberty than did patients in historical se-ries.21 Adverse psychosocial outcomes are also a concern, but the available data that are specific to patients with precocious puberty have serious
limitations.22 Data from surveys of the general population have indicated that a higher propor-tion of early-maturing adolescents engage in exploratory behaviors (sexual intercourse and legal and illegal substance use), and at an earlier age, than adolescents maturing within the normal age range or later.23,24 However, the relevance of these findings to precocious puberty is unclear, and they should not be used to justify inter-vention.
S tr ategies a nd E v idence
Evaluation
The first step in evaluating a child with preco-cious puberty is to obtain a complete family his-tory (age at onset of puberty in parents and sib-lings) and personal history, including the age at onset of puberty and progression of pubertal manifestations, and any evidence suggesting pos-sible central nervous system dysfunction, such as headache, increased head circumference, visual impairment, or seizures. Growth should be eval-uated, because progressive precocious puberty is almost invariably associated with a high growth velocity; a high growth velocity may also precede the onset of pubertal manifestations.25
The stage of pubertal development should be classified as described by Tanner. Careful assess-ment is needed in obese girls to avoid overesti-mating breast development (Fig. 1). The devel-opment of pubic hair results from the effects of androgens, which may be produced by testes or ovaries in central precocious puberty. In girls, pubic hair in the absence of breast development is suggestive of adrenal disorders, premature pubarche, or exposure to androgens (Table 1). In boys, measurement of testicular volume may sug-gest the cause of puberty; volume increases in central precocious puberty as it does in normal puberty (Fig. 1) and in cases of peripheral preco-cious puberty due to testicular disorders (although generally less so); volume remains prepubertal in adrenal disorders, premature pubarche, and other causes of peripheral precocious puberty. The physical examination should include an as-sessment for signs of specific causes of precocious puberty, such as hyperpigmented skin lesions suggesting neurofibromatosis or the McCune–Albright syndrome (Table 1). Precocious puber-tal changes have been associated with high levels of anxiety in girls,19,23 and psychological evalua-tion may be useful.
Copyright © 2008 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by PATRICK GIRAUD MD on May 29, 2008 .

clinical pr actice
n engl j med 358;22 www.nejm.org may 29, 2008 2369
Additional Testing
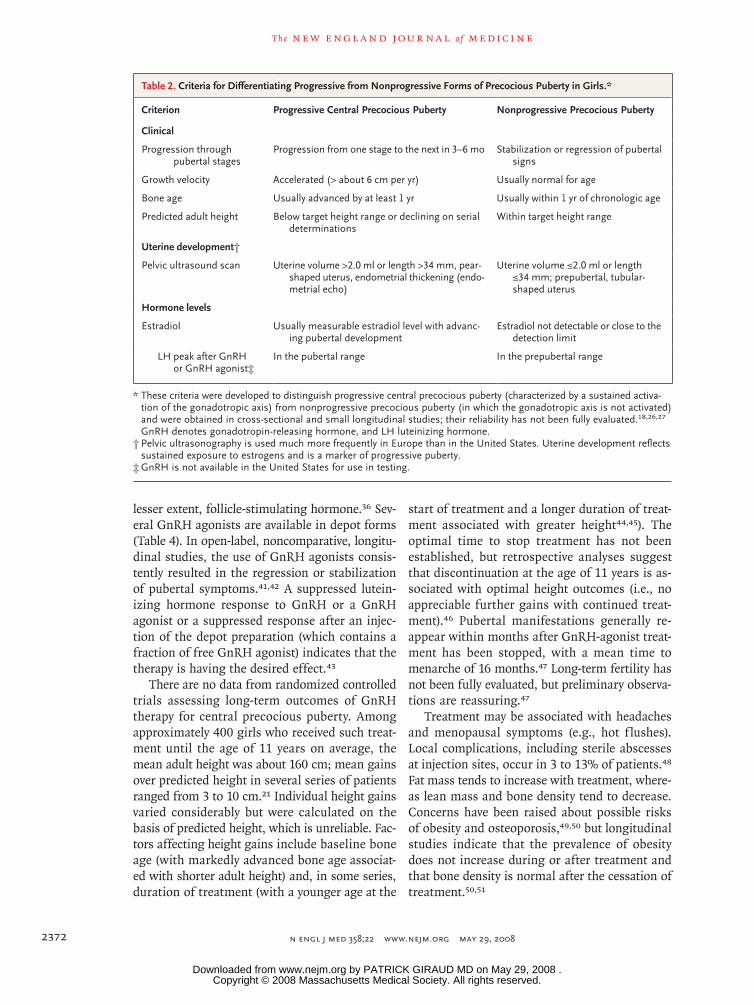
Although no evidence-based algorithm is avail-able to guide testing, evaluation of the mecha-nism and potential for progression of precocious puberty is generally recommended in all boys with precocious pubertal development and in girls who have precocious breast development at stage 3 or higher or at stage 2 with additional criteria such as increased growth velocity or who have symp-toms or signs suggestive of central nervous system dysfunction or of peripheral precocious puberty. Table 2 summarizes the features identified in cross-sectional and small longitudinal studies as potentially useful in distinguishing between pro-gressive and nonprogressive precocious puberty. Particularly when these features are inconsistent, the best policy is to wait a few months and per-form a reassessment in order to avoid unneces-sary treatment.28
Bone AgeA reference atlas such as the one by Greulich and Pyle can be used to evaluate the effect of sex ste-roids on epiphyseal maturation; the bone age of patients with precocious puberty is generally great-er than their chronologic age. Bone age can also be used to predict adult height, although the pre-cision is low (with a 95% confidence interval of about 6 cm below to 6 cm above the predicted value), and predictions tend to overestimate adult height.29
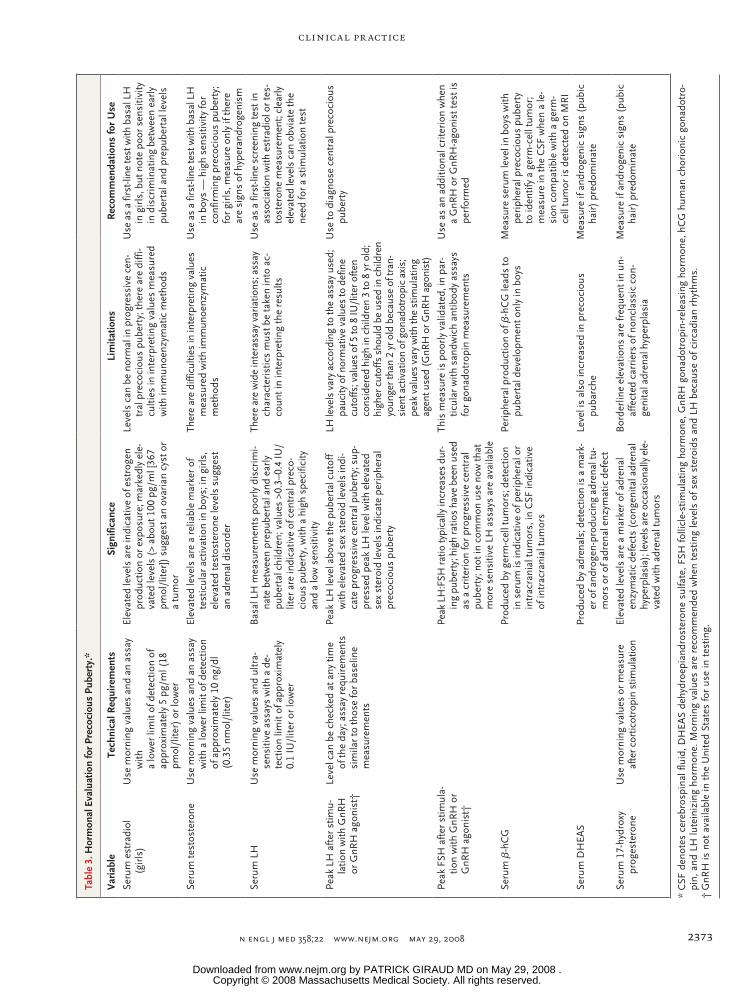
Hormonal MeasurementsLevels of sex steroids should be determined in the morning, with the use of assays that have detection limits adapted to pediatric values (Ta-ble 3). Most boys with precocious puberty have morning plasma testosterone values in the puber-tal range.30 In girls, serum estradiol levels are highly variable and have a low sensitivity for the diagnosis of precocious puberty. Very high estra-diol levels (above 100 pg per milliliter [367 pmol per liter]) generally indicate an ovarian cyst or tumor (Table 1). Gonadotropin determinations (based on ultrasensitive assays) are central to the diagnosis. The gold standard for evaluation is the measurement of gonadotropins after stimulation by GnRH (which is unavailable in the United States) or a GnRH-releasing hormone agonist. Peak luteinizing hormone levels of 5 to 8 IU per liter suggest progressive central precocious puber-ty, but there is an overlap between prepubertal and early pubertal values.31 Random measure-
ments of luteinizing hormone have been proposed as an alternative; in one study, randomly measured values of 0.3 IU per liter and above were reported to be 100% specific for peak values above 5 IU per liter.32 However, unless levels of luteinizing hormone are clearly elevated, it is advisable to con-firm the diagnosis of progressive central preco-cious puberty with a stimulation test before ini-tiating treatment. Caution should be used when interpreting gonadotropin levels in children young-er than 2 or 3 years old, because gonadotropin levels are normally high in this age group. Random measurements of follicle-stimulating hormone are not useful, since they vary little throughout puber-tal development.
Pelvic or Testicular Ultrasound ScansIn girls, pelvic ultrasonography can reveal ovar-ian cysts or tumors. Uterine changes due to estro-gen exposure can be used as an index of progres-sive puberty, but this approach is used much less frequently in the United States than in Europe. A uterine volume greater than 2.0 ml has been reported to have 89% sensitivity and specificity for precocious puberty.26 Testicular ultrasonog-raphy can detect nonpalpable Leydig-cell tumors and should be performed in cases of asymmetric testicular volume or peripheral precocious pu-berty.33
Brain Magnetic Resonance ImagingIn all cases of progressive central precocious pu-berty, magnetic resonance imaging (MRI) of the brain should be performed to determine whether a hypothalamic lesion is present (Table 1).34 The prevalence of such lesions is higher in boys (40 to 90%) than in girls (8 to 33%) presenting with precocious puberty and is much lower when pu-berty starts after the age of 6 years in girls (about 2% in one series).14,35 It has been suggested that an algorithm based on age and estradiol levels may obviate the need for MRI in one third of girls, but this practice has not been extensively vali-dated.14,34
M a nagemen t
Central Precocious Puberty
GnRH agonists are indicated in progressive cen-tral precocious puberty. They work by providing continuous stimulation of the pituitary gonado-trophs, leading to desensitization and decreases in the release of luteinizing hormone and, to a
Copyright © 2008 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by PATRICK GIRAUD MD on May 29, 2008 .
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 358;22 www.nejm.org may 29, 20082370
Tabl
e 1.
The
Cau
ses
of P
reco
ciou
s Pu
bert
y.*
Dis
orde
rC
hara
cter
isti
c Sy
mpt
oms
and
Sign
sTe
st R
esul
ts
Prog
ress
ive
cent
ral o
r gon
adot
ropi
n-de
pend
ent p
reco
ciou
s pu
bert
y
Ove
rvie
wB
reas
t dev
elop
men
t or
test
icul
ar e
nlar
gem
ent w
ith o
r w
ithou
t pu
bic
hair
dev
elop
men
t; in
crea
sed
grow
th v
eloc
ity; p
ossi
-bl
e ac
ne, o
ily s
kin
and
hair
, and
em
otio
nal c
hang
es
Hig
h se
rum
test
oste
rone
in b
oys,
var
iabl
e se
rum
est
radi
ol in
girl
s;
peak
ser
um L
H le
vel a
fter
GnR
H s
timul
atio
n in
the
pube
rtal
ra
nge;
adv
ance
d bo
ne a
ge; d
evel
oped
ute
rus
on u
ltras
ound
ex
amin
atio
n
No
CN
S le
sion
Poss
ible
his
tory
of f
amili
al p
reco
ciou
s pu
bert
y or
ado
ptio
n; n
o C
NS
lesi
on in
app
roxi
mat
ely
92%
of g
irls
and
appr
oxim
atel
y 50
% o
f boy
s; c
an a
lso
be p
art o
f a d
evel
opm
enta
l syn
drom
e su
ch a
s W
illia
ms–
Beu
ren
synd
rom
e or
mat
erna
l uni
pare
n-ta
l dis
omy
of c
hrom
osom
e 14
No
hypo
thal
amic
abn
orm
ality
foun
d on
MR
I of b
rain
; pos
sibl
e en
larg
emen
t of p
ituita
ry
CN
S le
sion
Hyp
otha
lam
ic h
amar
tom
aPo
ssib
le a
ssoc
iatio
n of
lesi
on w
ith g
elas
tic (
laug
hing
), fo
cal,
or
toni
c–cl
onic
sei
zure
sM
ass
in fl
oor
of th
ird
vent
ricl
e fo
und
on M
RI,
isoi
nten
se in
rel
a-tio
n to
nor
mal
tiss
ue w
ithou
t con
tras
t enh
ance
men
t
Oth
er h
ypot
hala
mic
tum
or (
e.g.
, glio
ma
in-
volv
ing
the
hypo
thal
amus
or
optic
chi
asm
, as
troc
ytom
a, e
pend
ymom
a, p
inea
lom
a, o
r ge
rm-c
ell t
umor
)
Poss
ible
hea
dach
e, v
isua
l cha
nges
, cog
nitiv
e ch
ange
s, s
ymp-
tom
s or
sig
ns o
f ant
erio
r or p
oste
rior p
ituita
ry d
efic
ienc
y (e
.g.,
decr
ease
d gr
owth
vel
ocity
, pol
yuri
a or
pol
ydip
sia)
, fat
igue
, an
d vi
sual
-fiel
d de
fect
s; if
CN
S tu
mor
is a
ssoc
iate
d w
ith
neur
ofib
rom
atos
is, o
ther
feat
ures
of n
euro
fibro
mat
osis
(e
.g.,
cuta
neou
s ne
urof
ibro
mas
, caf
é au
lait
spot
s, L
isch
no
dule
s)
Poss
ible
con
tras
t-en
hanc
ed m
ass
foun
d on
MR
I inv
olvi
ng o
ptic
pa
thw
ays
(chi
asm
, ner
ve, t
ract
) or
hyp
otha
lam
us a
lone
(in
the
case
of a
stro
cyto
ma
or g
liom
a) o
r hy
poth
alam
us a
nd p
ituita
ry
stal
k (i
n th
e ca
se o
f a g
erm
-cel
l tum
or);
pos
sibl
e ev
iden
ce o
f in
trac
rani
al h
yper
tens
ion;
pos
sibl
e si
gns
of a
nter
ior
or p
oste
-ri
or p
ituita
ry d
efic
ienc
y (e
.g.,
hype
rnat
rem
ia);
with
ger
m-c
ell
tum
or, c
an d
etec
t β-h
CG
in b
lood
or
CSF
Cer
ebra
l mal
form
atio
ns in
volv
ing
the
hypo
thal
-am
us —
sup
rase
llar
arac
hnoi
d cy
st, h
ydro
-ce
phal
us, s
epto
-opt
ic d
yspl
asia
, mye
lom
e-ni
ngoc
ele,
ect
opic
neu
rohy
poph
ysis
Poss
ible
neu
rode
velo
pmen
tal d
efic
its, m
acro
cran
ia, v
isua
l im
-pa
irm
ent,
nyst
agm
us, o
besi
ty, p
olyu
ria
or p
olyd
ipsi
a, o
r de
crea
sed
grow
th v
eloc
ity
Poss
ible
sig
ns o
f ant
erio
r or
pos
teri
or p
ituita
ry d
efic
ienc
y (e
.g.,
hype
rnat
rem
ia)
or h
yper
prol
actin
emia
Inju
ry —
cra
nial
irra
diat
ion,
hea
d tr
aum
a,
infe
ctio
n, p
erin
atal
insu
ltR
elev
ant h
isto
ry o
f inj
ury;
pos
sibl
e sy
mpt
oms
and
sign
s of
an-
teri
or o
r po
ster
ior
pitu
itary
def
icie
ncy
Poss
ible
find
ing
on M
RI o
f con
ditio
n-sp
ecifi
c se
quel
ae —
or
may
be
nor
mal
Earl
y ex
posu
re to
sex
ste
roid
s (a
fter
cur
e of
gon
ado-
trop
in-in
depe
nden
t pre
coci
ous
pube
rty)
His
tory
of s
uch
expo
sure
Perip
hera
l or g
onad
otro
pin-
inde
pend
ent p
reco
ciou
s pu
bert
y
Ove
rvie
wV
arie
d pu
bert
al s
ympt
oms
depe
ndin
g on
nat
ure
of s
ex s
tero
id
prod
uced
; typ
ical
ly, s
mal
ler t
estic
ular
vol
ume
than
in c
entr
al
prec
ocio
us p
uber
ty
Hig
h se
rum
test
oste
rone
in b
oys,
gen
eral
ly h
igh
and
occa
sion
ally
m
arke
dly
elev
ated
ser
um e
stra
diol
in g
irls
; low
(su
ppre
ssed
) pe
ak s
erum
LH
aft
er G
nRH
stim
ulat
ion;
adv
ance
d bo
ne a
ge;
deve
lope
d ut
erus
on
ultr
asou
nd e
xam
inat
ion
Aut
onom
ous
gona
dal a
ctiv
atio
n
McC
une–
Alb
righ
t syn
drom
e an
d re
curr
ent
auto
nom
ous
ovar
ian
cyst
s du
e to
som
atic
ac
tivat
ing
mut
atio
n of
the
GN
AS
gene
re-
sulti
ng in
incr
ease
d si
gnal
tran
sduc
tion
in
the
Gs
path
way
Foun
d m
ostly
in g
irls
; typ
ical
ly r
apid
pro
gres
sion
of b
reas
t de-
velo
pmen
t and
ear
ly o
ccur
renc
e of
vag
inal
ble
edin
g (b
efor
e or
with
in a
few
mon
ths
afte
r the
sta
rt o
f bre
ast d
evel
opm
ent)
; pr
ecoc
ious
pub
erty
isol
ated
or
asso
ciat
ed w
ith c
afé
au la
it sk
in le
sion
s or
bon
e pa
in d
ue to
pol
yost
otic
fibr
ous
dysp
la-
sia;
in ra
re c
ases
oth
er s
igns
of e
ndoc
rine
hype
rfun
ctio
n (e
.g.,
hype
rcor
tisol
ism
, hyp
erth
yroi
dism
), li
ver
chol
esta
sis,
or
card
iac
rhyt
hm a
bnor
mal
ities
Typi
cally
larg
e ov
aria
n cy
st o
r cy
sts
on p
elvi
c ul
tras
ound
exa
min
a-tio
n; b
one
lesi
ons
of fi
brou
s dy
spla
sia;
pos
sibl
e la
bora
tory
ev-
iden
ce o
f hyp
erco
rtis
olis
m, h
yper
thyr
oidi
sm, i
ncre
ased
GH
se
cret
ion,
hyp
opho
spha
tem
ia, o
r liv
er c
hole
stas
is
Ger
m-li
ne m
utat
ion
of G
NA
S ge
ne r
esul
ting
in
dual
loss
and
gai
n of
func
tion
(rar
e)Fe
atur
es o
f gon
adot
ropi
n-in
depe
nden
t pre
coci
ous
pube
rty
an
d ps
eudo
hypo
para
thyr
oidi
sm ty
pe 1
a in
boy
sTe
mpe
ratu
re-s
ensi
tive
poin
t mut
atio
n in
the
GN
AS
gene
res
ult-
ing
in a
ctiv
atio
n at
test
is te
mpe
ratu
re a
nd lo
ss o
f fun
ctio
n at
bo
dy te
mpe
ratu
re
Copyright © 2008 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by PATRICK GIRAUD MD on May 29, 2008 .
clinical pr actice
n engl j med 358;22 www.nejm.org may 29, 2008 2371
Fam
ilial
mal
e-lim
ited
prec
ocio
us p
uber
ty d
ue
to g
erm
inal
act
ivat
ing
mut
atio
ns o
f the
LH
re
cept
or g
ene
Poss
ible
fam
ilial
his
tory
of d
omin
ant p
reco
ciou
s pu
bert
y in
boy
s (c
an b
e tr
ansm
itted
by
mot
hers
), w
ith s
ome
spor
adic
cas
esA
ctiv
atin
g m
utat
ion
of L
H r
ecep
tor
gene
.
Tum
ors
Gra
nulo
sa-c
ell t
umor
of t
he o
vary
Rap
id p
rogr
essi
on o
f bre
ast d
evel
opm
ent a
nd p
ossi
ble
abdo
mi-
nal p
ain;
tum
or m
ay b
e pa
lpab
le o
n ab
dom
inal
exa
min
atio
nTu
mor
det
ectio
n on
ultr
asou
nd o
r C
T sc
an
And
roge
n-pr
oduc
ing
ovar
ian
tum
orPr
ogre
ssiv
e vi
riliz
atio
nTu
mor
det
ectio
n on
ultr
asou
nd o
r C
T sc
an
Test
icul
ar L
eydi
g-ce
ll tu
mor
Prog
ress
ive
viri
lizat
ion;
test
icul
ar a
sym
met
ry; t
umor
pal
pabl
e in
rar
e ca
ses
Tum
or d
etec
tion
on te
stic
ular
ultr
asou
nd
hCG
-pro
duci
ng tu
mor
Tum
ors
can
orig
inat
e in
the
liver
or
med
iast
inum
; pub
erta
l sy
mpt
oms
in b
oys
only
; may
be
asso
ciat
ed w
ith
Klin
efel
ter’
s sy
ndro
me
Elev
ated
ser
um h
CG
; tum
or d
etec
tion
on u
ltras
ound
or
CT
scan
Adr
enal
dis
orde
rs
Con
geni
tal a
dren
al h
yper
plas
iaIn
crea
sed
andr
ogen
pro
duct
ion,
lead
ing
to v
irili
zatio
n in
boy
s an
d gi
rls
Incr
ease
d ad
rena
l ste
roid
pre
curs
ors
in s
erum
, mai
nly
17-h
ydro
xy-
prog
este
rone
(ba
sal o
r af
ter
a co
rtic
otro
pin
stim
ulat
ion
test
)
Adr
enal
tum
orIn
crea
sed
andr
ogen
pro
duct
ion,
lead
ing
to v
irili
zatio
n in
boy
s an
d gi
rls;
in r
are
case
s es
trog
en-p
rodu
cing
adr
enal
tum
orTu
mor
on
abdo
min
al u
ltras
ound
or
CT
scan
; ele
vate
d D
HEA
S or
ad
rena
l ste
roid
pre
curs
ors
Con
ditio
n du
e to
exp
osur
e to
exo
geno
us a
gent
s
Sex
ster
oids
Var
ied
man
ifest
atio
ns d
epen
ding
on
type
of p
repa
ratio
n (a
n-dr
ogen
ic o
r es
trog
enic
); m
ost c
omm
only
des
crib
ed a
fter
to
pica
l exp
osur
e to
and
roge
ns; p
ossi
ble
diffi
culty
trac
ing
sour
ce o
f exp
osur
e
Mis
lead
ing
endo
crin
e ev
alua
tion
poss
ible
due
to v
aria
ble
seru
m
leve
ls o
f sex
ste
roid
s
Estr
ogen
ic e
ndoc
rine
-dis
rupt
ing
chem
ical
sA
lthou
gh u
npro
ven,
pos
sibl
e ro
le o
f exp
osur
e in
pre
coci
ous
pube
rty
amon
g ad
opte
d ch
ildre
n (b
y m
odul
atin
g tim
ing
of
activ
atio
n of
pub
erta
l gon
adot
ropi
c ax
is)
No
valid
ated
bio
chem
ical
test
Seve
re, u
ntre
ated
pri
mar
y hy
poth
yroi
dism
Sign
s of
hyp
othy
roid
ism
; no
incr
ease
in g
row
th v
eloc
ityEl
evat
ed s
erum
leve
ls o
f thy
rotr
opin
, low
leve
ls o
f fre
e th
yrox
ine;
no
adv
ance
men
t in
bone
age
Ben
ign
vari
ants
of p
reco
ciou
s pu
bert
al d
evel
opm
ent
Ove
rvie
wU
sual
ly is
olat
ed s
econ
dary
sex
ual c
hara
cter
istic
; no
or s
light
ly
incr
ease
d gr
owth
vel
ocity
Bon
e ag
e w
ithin
two
stan
dard
dev
iatio
ns o
f nor
mal
for
age;
low
se
rum
leve
ls o
f sex
ste
roid
s; p
eak
seru
m L
H le
vels
aft
er G
nRH
st
imul
atio
n in
pre
pube
rtal
ran
ge; n
orm
al p
elvi
c ul
tras
ound
ex
amin
atio
n
Non
prog
ress
ive
prec
ocio
us p
uber
tySt
abili
zatio
n or
reg
ress
ion
of p
uber
tal s
igns
, nor
mal
gro
wth
ve-
loci
ty; f
ollo
w-u
p is
war
rant
ed s
ince
pro
gres
sion
can
occ
urN
orm
al b
one
age
and
prep
uber
tal u
teru
s on
ultr
asou
nd e
xam
inat
ion
Isol
ated
pre
coci
ous
thel
arch
eU
nila
tera
l or
bila
tera
l bre
ast d
evel
opm
ent;
part
icul
arly
freq
uent
be
fore
the
age
of 2
yr
No
furt
her
eval
uatio
n ne
eded
in m
ost c
ases
Isol
ated
pre
coci
ous
puba
rche
Pubi
c ha
ir d
evel
opm
ent,
som
etim
es a
ssoc
iate
d w
ith a
dult
body
odo
r, a
xilla
ry h
air,
or
mild
acn
e N
orm
al c
ortis
ol p
recu
rsor
s in
ser
um, i
nclu
ding
nor
mal
leve
ls o
f 17
-hyd
roxy
pro
gest
eron
e af
ter
cort
icot
ropi
n st
imul
atio
n
Isol
ated
pre
coci
ous
men
arch
eIs
olat
ed v
agin
al b
leed
ing
with
out b
reas
t or p
ubic
-hai
r dev
elop
-m
ent a
nd w
ithou
t gen
ital t
raum
a; im
port
ant t
o ev
alua
te c
lin-
ical
ly fo
r a v
agin
al le
sion
(se
xual
abu
se, f
orei
gn b
ody,
tum
or)
Nor
mal
bon
e ag
e an
d pr
epub
erta
l ute
rus
on u
ltras
ound
exa
min
atio
n
* C
NS
deno
tes
cent
ral n
ervo
us s
yste
m, C
SF c
ereb
rosp
inal
flui
d, C
T co
mpu
ted
tom
ogra
phy,
DH
EAS
dehy
droe
pian
dros
tero
ne s
ulfa
te, G
H g
row
th h
orm
one,
GN
AS
guan
ine
nucl
eotid
e–bi
nd-
ing
prot
ein
alph
a su
buni
t, G
nRH
gon
adot
ropi
n-re
leas
ing
horm
one,
Gs
stim
ulat
ory
guan
ine
nucl
eotid
e-bi
ndin
g pr
otei
n, h
CG
hum
an c
hori
onic
gon
adot
ropi
n, L
H lu
tein
izin
g ho
rmon
e, a
nd
MR
I m
agne
tic r
eson
ance
imag
ing.
Copyright © 2008 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by PATRICK GIRAUD MD on May 29, 2008 .
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 358;22 www.nejm.org may 29, 20082372
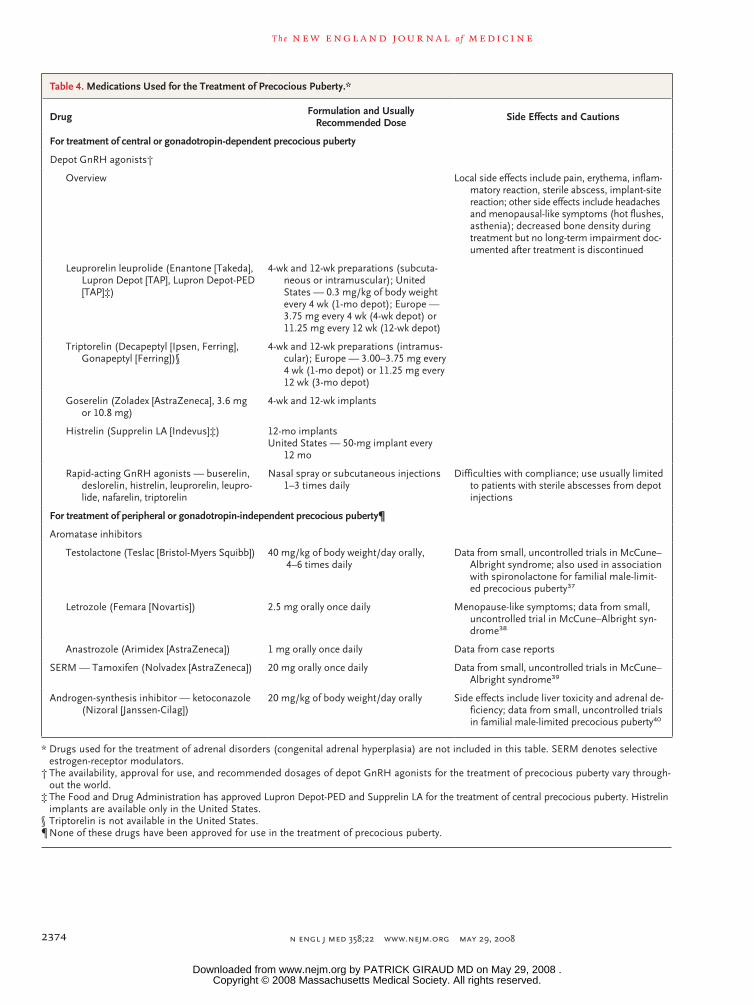
lesser extent, follicle-stimulating hormone.36 Sev-eral GnRH agonists are available in depot forms (Table 4). In open-label, noncomparative, longitu-dinal studies, the use of GnRH agonists consis-tently resulted in the regression or stabilization of pubertal symptoms.41,42 A suppressed lutein-izing hormone response to GnRH or a GnRH agonist or a suppressed response after an injec-tion of the depot preparation (which contains a fraction of free GnRH agonist) indicates that the therapy is having the desired effect.43
There are no data from randomized controlled trials assessing long-term outcomes of GnRH therapy for central precocious puberty. Among approximately 400 girls who received such treat-ment until the age of 11 years on average, the mean adult height was about 160 cm; mean gains over predicted height in several series of patients ranged from 3 to 10 cm.21 Individual height gains varied considerably but were calculated on the basis of predicted height, which is unreliable. Fac-tors affecting height gains include baseline bone age (with markedly advanced bone age associat-ed with shorter adult height) and, in some series, duration of treatment (with a younger age at the
start of treatment and a longer duration of treat-ment associated with greater height44,45). The optimal time to stop treatment has not been established, but retrospective analyses suggest that discontinuation at the age of 11 years is as-sociated with optimal height outcomes (i.e., no appreciable further gains with continued treat-ment).46 Pubertal manifestations generally re-appear within months after GnRH-agonist treat-ment has been stopped, with a mean time to menarche of 16 months.47 Long-term fertility has not been fully evaluated, but preliminary observa-tions are reassuring.47
Treatment may be associated with headaches and menopausal symptoms (e.g., hot f lushes). Local complications, including sterile abscesses at injection sites, occur in 3 to 13% of patients.48 Fat mass tends to increase with treatment, where-as lean mass and bone density tend to decrease. Concerns have been raised about possible risks of obesity and osteoporosis,49,50 but longitudinal studies indicate that the prevalence of obesity does not increase during or after treatment and that bone density is normal after the cessation of treatment.50,51
Table 2. Criteria for Differentiating Progressive from Nonprogressive Forms of Precocious Puberty in Girls.*
Criterion Progressive Central Precocious Puberty Nonprogressive Precocious Puberty
Clinical
Progression through pubertal stages
Progression from one stage to the next in 3–6 mo Stabilization or regression of pubertal signs
Growth velocity Accelerated (> about 6 cm per yr) Usually normal for age
Bone age Usually advanced by at least 1 yr Usually within 1 yr of chronologic age
Predicted adult height Below target height range or declining on serial determinations
Within target height range
Uterine development†
Pelvic ultrasound scan Uterine volume >2.0 ml or length >34 mm, pear-shaped uterus, endometrial thickening (endo-metrial echo)
Uterine volume ≤2.0 ml or length ≤34 mm; prepubertal, tubular-shaped uterus
Hormone levels
Estradiol Usually measurable estradiol level with advanc-ing pubertal development
Estradiol not detectable or close to the detection limit
LH peak after GnRH or GnRH agonist‡
In the pubertal range In the prepubertal range
* These criteria were developed to distinguish progressive central precocious puberty (characterized by a sustained activa-tion of the gonadotropic axis) from nonprogressive precocious puberty (in which the gonadotropic axis is not activated) and were obtained in cross-sectional and small longitudinal studies; their reliability has not been fully evaluated.18,26,27 GnRH denotes gonadotropin-releasing hormone, and LH luteinizing hormone.
† Pelvic ultrasonography is used much more frequently in Europe than in the United States. Uterine development reflects sustained exposure to estrogens and is a marker of progressive puberty.
‡ GnRH is not available in the United States for use in testing.
Copyright © 2008 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by PATRICK GIRAUD MD on May 29, 2008 .
clinical pr actice
n engl j med 358;22 www.nejm.org may 29, 2008 2373
Tabl
e 3.
Hor
mon
al E
valu
atio
n fo
r Pr
ecoc
ious
Pub
erty
.*
Var
iabl
eTe
chni
cal R
equi
rem
ents
Sign
ifica
nce
Lim
itatio
nsR
ecom
men
datio
ns fo
r U
se
Seru
m e
stra
diol
(g
irls
)U
se m
orni
ng v
alue
s an
d an
ass
ay
with
a
low
er li
mit
of d
etec
tion
of
appr
oxim
atel
y 5
pg/m
l (18
pm
ol/l
iter)
or
low
er
Elev
ated
leve
ls a
re in
dica
tive
of e
stro
gen
prod
uctio
n or
exp
osur
e; m
arke
dly
ele-
vate
d le
vels
(>
abou
t 100
pg/
ml [
367
pmol
/lite
r])
sugg
est a
n ov
aria
n cy
st o
r a
tum
or
Leve
ls c
an b
e no
rmal
in p
rogr
essi
ve c
en-
tral
pre
coci
ous
pube
rty;
ther
e ar
e di
ffi-
culti
es in
inte
rpre
ting
valu
es m
easu
red
with
imm
unoe
nzym
atic
met
hods
Use
as
a fir
st-li
ne te
st w
ith b
asal
LH
in
gir
ls, b
ut n
ote
poor
sen
sitiv
ity
in d
iscr
imin
atin
g be
twee
n ea
rly
pube
rtal
and
pre
pube
rtal
leve
ls
Seru
m te
stos
tero
neU
se m
orni
ng v
alue
s an
d an
ass
ay
with
a lo
wer
lim
it of
det
ectio
n
of a
ppro
xim
atel
y 10
ng/
dl
(0.3
5 nm
ol/l
iter)
Elev
ated
leve
ls a
re a
rel
iabl
e m
arke
r of
te
stic
ular
act
ivat
ion
in b
oys;
in g
irls
,
elev
ated
test
oste
rone
leve
ls s
ugge
st
an a
dren
al d
isor
der
Ther
e ar
e di
fficu
lties
in in
terp
retin
g va
lues
m
easu
red
with
imm
unoe
nzym
atic
m
etho
ds
Use
as
a fir
st-li
ne te
st w
ith b
asal
LH
in
boy
s —
hig
h se
nsiti
vity
for
conf
irm
ing
prec
ocio
us p
uber
ty;
for
girl
s, m
easu
re o
nly
if th
ere
are
sign
s of
hyp
eran
drog
enis
m
Seru
m L
HU
se m
orni
ng v
alue
s an
d ul
tra-
sens
itive
ass
ays
with
a d
e-
tect
ion
limit
of a
ppro
xim
atel
y 0.
1 IU
/lite
r or
low
er
Bas
al L
H m
easu
rem
ents
poo
rly
disc
rim
i-na
te b
etw
een
prep
uber
tal a
nd e
arly
pu
bert
al c
hild
ren;
val
ues
>0.3
–0.4
IU/
liter
are
indi
cativ
e of
cen
tral
pre
co-
ciou
s pu
bert
y, w
ith a
hig
h sp
ecifi
city
an
d a
low
sen
sitiv
ity
Ther
e ar
e w
ide
inte
rass
ay v
aria
tions
; ass
ay
char
acte
rist
ics
mus
t be
take
n in
to a
c-co
unt i
n in
terp
retin
g th
e re
sults
Use
as
a fir
st-li
ne s
cree
ning
test
in
asso
ciat
ion
with
est
radi
ol o
r te
s-to
ster
one
mea
sure
men
t; cl
early
el
evat
ed le
vels
can
obv
iate
the
need
for
a st
imul
atio
n te
st
Peak
LH
aft
er s
timu-
latio
n w
ith G
nRH
or
GnR
H a
goni
st†
Leve
l can
be
chec
ked
at a
ny ti
me
of
the
day;
ass
ay r
equi
rem
ents
si
mila
r to
thos
e fo
r ba
selin
e m
easu
rem
ents
Peak
LH
leve
l abo
ve th
e pu
bert
al c
utof
f w
ith e
leva
ted
sex
ster
oid
leve
ls in
di-
cate
pro
gres
sive
cen
tral
pub
erty
; sup
-pr
esse
d pe
ak L
H le
vel w
ith e
leva
ted
sex
ster
oid
leve
ls in
dica
te p
erip
hera
l pr
ecoc
ious
pub
erty
LH le
vels
var
y ac
cord
ing
to th
e as
say
used
; pa
ucity
of n
orm
ativ
e va
lues
to d
efin
e cu
toffs
; val
ues
of 5
to 8
IU/l
iter o
ften
co
nsid
ered
hig
h in
chi
ldre
n 3
to 8
yr o
ld;
high
er c
utof
fs s
houl
d be
use
d in
chi
ldre
n yo
unge
r tha
n 2
yr o
ld b
ecau
se o
f tra
n-si
ent a
ctiv
atio
n of
gon
adot
ropi
c ax
is;
peak
val
ues
vary
with
the
stim
ulat
ing
agen
t use
d (G
nRH
or G
nRH
ago
nist
)
Use
to d
iagn
ose
cent
ral p
reco
ciou
s pu
bert
y
Peak
FSH
aft
er s
timul
a-tio
n w
ith G
nRH
or
GnR
H a
goni
st†
Peak
LH
:FSH
ratio
typi
cally
incr
ease
s du
r-in
g pu
bert
y; h
igh
ratio
s ha
ve b
een
used
as
a c
rite
rion
for
prog
ress
ive
cent
ral
pube
rty;
not
in c
omm
on u
se n
ow th
at
mor
e se
nsiti
ve L
H a
ssay
s ar
e av
aila
ble
This
mea
sure
is p
oorl
y va
lidat
ed, i
n pa
r-tic
ular
with
san
dwic
h an
tibod
y as
says
fo
r go
nado
trop
in m
easu
rem
ents
Use
as
an a
dditi
onal
cri
teri
on w
hen
a G
nRH
or
GnR
H-a
goni
st te
st is
pe
rfor
med
Seru
m β
-hC
GPr
oduc
ed b
y ge
rm-c
ell t
umor
s; d
etec
tion
in s
erum
is in
dica
tive
of p
erip
hera
l or
intr
acra
nial
tum
ors,
in C
SF in
dica
tive
of in
trac
rani
al tu
mor
s
Peri
pher
al p
rodu
ctio
n of
β-h
CG
lead
s to
pu
bert
al d
evel
opm
ent o
nly
in b
oys
Mea
sure
ser
um le
vel i
n bo
ys w
ith
peri
pher
al p
reco
ciou
s pu
bert
y to
iden
tify
a ge
rm-c
ell t
umor
; m
easu
re in
the
CSF
whe
n a
le-
sion
com
patib
le w
ith a
ger
m-
cell
tum
or is
det
ecte
d on
MR
I
Seru
m D
HEA
SPr
oduc
ed b
y ad
rena
ls; d
etec
tion
is a
mar
k-er
of a
ndro
gen-
prod
ucin
g ad
rena
l tu-
mor
s or
of a
dren
al e
nzym
atic
def
ect
Leve
l is
also
incr
ease
d in
pre
coci
ous
puba
rche
Mea
sure
if a
ndro
geni
c si
gns
(pub
ic
hair
) pr
edom
inat
e
Seru
m 1
7-hy
drox
y pr
oges
tero
neU
se m
orni
ng v
alue
s or
mea
sure
af
ter c
ortic
otro
pin
stim
ulat
ion
Elev
ated
leve
ls a
re a
mar
ker
of a
dren
al
enzy
mat
ic d
efec
ts (
cong
enita
l adr
enal
hy
perp
lasi
a); l
evel
s ar
e oc
casi
onal
ly e
le-
vate
d w
ith a
dren
al tu
mor
s
Bor
derl
ine
elev
atio
ns a
re fr
eque
nt in
un-
affe
cted
car
rier
s of
non
clas
sic
con-
geni
tal a
dren
al h
yper
plas
ia
Mea
sure
if a
ndro
geni
c si
gns
(pub
ic
hair
) pr
edom
inat
e
* C
SF d
enot
es c
ereb
rosp
inal
flui
d, D
HEA
S de
hydr
oepi
andr
oste
rone
sul
fate
, FSH
folli
cle-
stim
ulat
ing
horm
one,
GnR
H g
onad
otro
pin-
rele
asin
g ho
rmon
e, h
CG
hum
an c
hori
onic
gon
adot
ro-
pin,
and
LH
lute
iniz
ing
horm
one.
Mor
ning
val
ues
are
reco
mm
ende
d w
hen
test
ing
leve
ls o
f sex
ste
roid
s an
d LH
bec
ause
of c
irca
dian
rhy
thm
s.†
GnR
H is
not
ava
ilabl
e in
the
Uni
ted
Stat
es fo
r us
e in
tes
ting.
Copyright © 2008 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by PATRICK GIRAUD MD on May 29, 2008 .
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 358;22 www.nejm.org may 29, 20082374
Table 4. Medications Used for the Treatment of Precocious Puberty.*
Drug Formulation and Usually Recommended Dose Side Effects and Cautions
For treatment of central or gonadotropin-dependent precocious puberty
Depot GnRH agonists†
Overview Local side effects include pain, erythema, inflam-matory reaction, sterile abscess, implant-site reaction; other side effects include headaches and menopausal-like symptoms (hot flushes, asthenia); decreased bone density during treatment but no long-term impairment doc-umented after treatment is discontinued
Leuprorelin leuprolide (Enantone [Takeda], Lupron Depot [TAP], Lupron Depot-PED [TAP]‡)
4-wk and 12-wk preparations (subcuta-neous or intramuscular); United States — 0.3 mg/kg of body weight every 4 wk (1-mo depot); Europe — 3.75 mg every 4 wk (4-wk depot) or 11.25 mg every 12 wk (12-wk depot)
Triptorelin (Decapeptyl [Ipsen, Ferring], Gonapeptyl [Ferring])§
4-wk and 12-wk preparations (intramus-cular); Europe — 3.00–3.75 mg every 4 wk (1-mo depot) or 11.25 mg every 12 wk (3-mo depot)
Goserelin (Zoladex [AstraZeneca], 3.6 mg or 10.8 mg)
4-wk and 12-wk implants
Histrelin (Supprelin LA [Indevus]‡) 12-mo implantsUnited States — 50-mg implant every
12 mo
Rapid-acting GnRH agonists — buserelin, deslorelin, histrelin, leuprorelin, leupro-lide, nafarelin, triptorelin
Nasal spray or subcutaneous injections 1–3 times daily
Difficulties with compliance; use usually limited to patients with sterile abscesses from depot injections
For treatment of peripheral or gonadotropin-independent precocious puberty¶
Aromatase inhibitors
Testolactone (Teslac [Bristol-Myers Squibb]) 40 mg/kg of body weight/day orally, 4–6 times daily
Data from small, uncontrolled trials in McCune–Albright syndrome; also used in association with spironolactone for familial male-limit-ed precocious puberty37
Letrozole (Femara [Novartis]) 2.5 mg orally once daily Menopause-like symptoms; data from small, uncontrolled trial in McCune–Albright syn-drome38
Anastrozole (Arimidex [AstraZeneca]) 1 mg orally once daily Data from case reports
SERM — Tamoxifen (Nolvadex [AstraZeneca]) 20 mg orally once daily Data from small, uncontrolled trials in McCune–Albright syndrome39
Androgen-synthesis inhibitor — ketoconazole (Nizoral [Janssen-Cilag])
20 mg/kg of body weight/day orally Side effects include liver toxicity and adrenal de-ficiency; data from small, uncontrolled trials in familial male-limited precocious puberty40
* Drugs used for the treatment of adrenal disorders (congenital adrenal hyperplasia) are not included in this table. SERM denotes selective estrogen-receptor modulators.
† The availability, approval for use, and recommended dosages of depot GnRH agonists for the treatment of precocious puberty vary through-out the world.
‡ The Food and Drug Administration has approved Lupron Depot-PED and Supprelin LA for the treatment of central precocious puberty. Histrelin implants are available only in the United States.
§ Triptorelin is not available in the United States.¶ None of these drugs have been approved for use in the treatment of precocious puberty.
Copyright © 2008 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by PATRICK GIRAUD MD on May 29, 2008 .

clinical pr actice
n engl j med 358;22 www.nejm.org may 29, 2008 2375
For cases in which precocious puberty is caused by a central lesion (e.g., a mass or malfor-mation), management of the causal lesion gener-ally has no effect on the course of pubertal de-velopment. Hypothalamic hamartomas should not be removed surgically for the purpose of manag-ing precocious puberty. When precocious puberty is associated with the presence of a hypothalamic lesion, there may be progression to gonadotro-pin deficiency.
Peripheral Precocious Puberty
Surgery is indicated for gonadal tumors. The roles of postoperative chemotherapy and radiotherapy in granulosa-cell tumors of the ovary at stage I or after complete resection have not been defined.52 For large ovarian cysts (those that are greater than 20 ml in volume [3.4 cm in diameter] and particularly those that are more than 75 ml in volume [5.2 cm in diameter]), puncture should be considered because of the risk of adnexal tor-sion.53 If there is exposure to exogenous sex ste-roids, it should be withdrawn.
Aromatase inhibitors38 have been used to in-hibit the production of estrogens, and selective estrogen-receptor modulators39 have been used to interfere with the action of estrogens in the McCune–Albright syndrome. Limited data from uncontrolled studies suggest that these strategies have been effective in some cases.
A r e a s of Uncerta in t y
The appropriate age threshold for the definition of precocious puberty remains controversial; well-performed longitudinal assessments of normally developing children are needed to inform these criteria. The best approach for differentiating pro-gressive from nonprogressive forms of precocious puberty remains unclear. The decision about whether to provide treatment is therefore often difficult, particularly for girls with an onset of puberty between the ages of 6 and 8 years. The most appropriate age for stopping treatment also remains uncertain. The addition of growth hor-mone54 or oxandrolone55 has been proposed when growth velocity decreases or if the prognosis for adult height appears to be unsatisfactory, but data are limited on the efficacy and safety of these
drugs in children with precocious puberty. Causal mechanisms underlying idiopathic precocious pu-berty also remain uncertain.16
Guidel ines
A consensus statement on the use of GnRH ago-nists in children is currently being prepared by the European Society for Paediatric Endocrinology and its American counterpart, the Lawson Wilkins Pediatric Endocrine Society.
Conclusions a nd R ecommendations
In the case described in the vignette, advanced breast development (Tanner stage 3), pubic hair development, higher-than-expected height given parental height, and increased growth velocity at 6 years of age suggest progressive precocious pu-berty. Evidence of possible causes of precocious puberty should be sought by means of a thor-ough history taking and careful examination, but this search is often unrevealing. Further eval-uation should include measurements of bone age (which would probably be advanced) and levels of estradiol and luteinizing hormone. If a randomly measured level of luteinizing hormone is in the pubertal range, an MRI scan of the brain should be obtained, and it would be useful to perform a GnRH-agonist stimulation test to confirm pro-gressive central precocious puberty before con-sidering treatment with a GnRH agonist. If the randomly measured level of luteinizing hormone is in the prepubertal range, a pelvic ultrasound scan is needed to rule out an ovarian tumor or cyst, particularly if the estradiol level is elevated. If randomly measured levels of both estradiol and luteinizing hormone are in the prepubertal range, we recommend performing a GnRH or GnRH-agonist stimulation test to further evalu-ate the activation of the gonadotropic axis and the potential for progression of puberty. If the results suggest nonprogressive precocious pu-berty, we recommend follow-up every 3 to 6 months between the ages of 6 and 7 years to as-sess the child clinically for progression. If pro-gressive central precocious puberty is confirmed, treatment with a depot GnRH agonist is recom-
Copyright © 2008 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by PATRICK GIRAUD MD on May 29, 2008 .

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 358;22 www.nejm.org may 29, 20082376
mended and is generally continued until the child is 11 years old, although the optimal duration of therapy is uncertain. [Educational information for families can be found at http://eurospe.org/patient/English/index.html or at www.hormone.org/Public/factsheets.cfm.]
Dr. Carel reports receiving grant funding from Ipsen and
Takeda; having been part of the organizing committee of a pediatric endocrinology consensus meeting supported in part by Indevus, Ipsen, Ferring, and TAP; and receiving lecture fees from Ferring. No other potential conflict of interest relevant to this article was reported.
We thank Drs. Jean-Louis Chaussain, Najiba Lahlou, and Marc Roger for their longstanding contributions to the field of preco-cious puberty.An audio version of this article is available at www.nejm.org.
References
Marshall WA, Tanner JM. Variations in the pattern of pubertal changes in boys. Arch Dis Child 1970;45:13-24.
Idem. Variations in the pattern of pu-bertal changes in girls. Arch Dis Child 1969;44:291-303.
Herman-Giddens ME, Slora EJ, Wasser-man RC, et al. Secondary sexual charac-teristics and menses in young girls seen in office practice: a study from the Pediat-ric Research in Office Settings Network. Pediatrics 1997;99:505-12.
Herman-Giddens ME, Kaplowitz PB, Wasserman R. Navigating the recent arti-cles on girls’ puberty in Pediatrics: what do we know and where do we go from here? Pediatrics 2004;113:911-7.
Wu T, Mendola P, Buck GM. Ethnic differences in the presence of secondary sex characteristics and menarche among US girls: the Third National Health and Nutrition Examination Survey, 1988-1994. Pediatrics 2002;110:752-7.
Sun SS, Schubert CM, Chumlea WC, et al. National estimates of the timing of sexual maturation and racial differences among US children. Pediatrics 2002;110: 911-9.
Kaplowitz PB, Oberfield SE. Reexami-nation of the age limit for defining when puberty is precocious in girls in the United States: implications for evaluation and treatment. Pediatrics 1999;104:936-41.
Rosenfield RL, Bachrach LK, Chernau-sek SD, et al. Current age of onset of pu-berty. Pediatrics 2000;106:622-3.
Mul D, Fredriks AM, van Buuren S, Oostdijk W, Verloove-Vanhorick SP, Wit JM. Pubertal development in the Nether-lands 1965-1997. Pediatr Res 2001;50:479-86.
Parent AS, Teilmann G, Juul A, Skak-kebaek NE, Toppari J, Bourguignon JP. The timing of normal puberty and the age limits of sexual precocity: variations around the world, secular trends, and changes after migration. Endocr Rev 2003; 24:668-93.
Teilmann G, Pedersen CB, Skakke-baek NE, Jensen TK. Increased risk of pre-cocious puberty in internationally adopt-ed children in Denmark. Pediatrics 2006; 118(2):e391-e399.
Matchock RL, Susman EJ. Family com-position and menarcheal age: anti-inbreed-ing strategies. Am J Hum Biol 2006;18: 481-91.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
Midyett LK, Moore WV, Jacobson JD. Are pubertal changes in girls before age 8 benign? Pediatrics 2003;111:47-51.
Chalumeau M, Hadjiathanasiou CG, Ng SM, et al. Selecting girls with preco-cious puberty for brain imaging: valida-tion of European evidence-based diagno-sis rule. J Pediatr 2003;143:445-50.
Teilmann G, Pedersen CB, Jensen TK, Skakkebaek NE, Juul A. Prevalence and incidence of precocious pubertal develop-ment in Denmark: an epidemiologic study based on national registries. Pediatrics 2005;116:1323-8.
Nathan BM, Palmert MR. Regulation and disorders of pubertal timing. Endo-crinol Metab Clin North Am 2005;34: 617-41.
Kaplowitz P. Clinical characteristics of 104 children referred for evaluation of precocious puberty. J Clin Endocrinol Metab 2004;89:3644-50.
Klein KO. Precocious puberty: who has it? Who should be treated? J Clin Endocri-nol Metab 1999;84:411-4.
Xhrouet-Heinrichs D, Lagrou K, Hein-richs C, et al. Longitudinal study of be-havioral and affective patterns in girls with central precocious puberty during long-acting triptorelin therapy. Acta Paediatr 1997;86:808-15.
Marti-Henneberg C, Vizmanos B. The duration of puberty in girls is related to the timing of its onset. J Pediatr 1997;131: 618-21.
Carel JC, Lahlou N, Roger M, Chaus-sain JL. Precocious puberty and statural growth. Hum Reprod Update 2004;10: 135-47.
Dorn LD. Psychological and social problems in children with premature adrenarche and precocious puberty. In: Pescovitz OH, Walvoord EC, eds. When puberty is precocious: scientific and clini-cal aspects. Totowa, NJ: Humana Press, 2007:309-27.
Tremblay L, Frigon JY. Precocious pu-berty in adolescent girls: a biomarker of later psychosocial adjustment problems. Child Psychiatry Hum Dev 2005;36:73-94.
Michaud PA, Suris JC, Deppen A. Gen-der-related psychological and behavioural correlates of pubertal timing in a national sample of Swiss adolescents. Mol Cell En-docrinol 2006;254-255:172-8.
Papadimitriou A, Beri D, Tsialla A,
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
Fretzayas A, Psychou F, Nicolaidou P. Early growth acceleration in girls with idiopathic precocious puberty. J Pediatr 2006;149:43-6.
de Vries L, Horev G, Schwartz M, Phillip M. Ultrasonographic and clinical parameters for early differentiation be-tween precocious puberty and premature thelarche. Eur J Endocrinol 2006;154: 891-8.
Palmert MR, Malin HV, Boepple PA. Unsustained or slowly progressive puber-ty in young girls: initial presentation and long-term follow-up of 20 untreated pa-tients. J Clin Endocrinol Metab 1999;84: 415-23.
Léger J, Reynaud R, Czernichow P. Do all girls with apparent idiopathic pre-cocious puberty require gonadotropin- releasing hormone agonist treatment? J Pediatr 2000;137:819-25.
Bar A, Linder B, Sobel EH, Saenger P, DiMartino-Nardi J. Bayley-Pinneau meth-od of height prediction in girls with cen-tral precocious puberty: correlation with adult height. J Pediatr 1995;126:955-8.
Roger M, Lahlou N, Chaussain JL. Go-nadotropin-releasing hormone testing in pediatrics. In: Ranke MB, ed. Diagnostics of endocrine function in children and adolescents. Heidelberg, Germany: Johann Ambrosius Barth Verlag, 1996:346-69.
Resende EA, Lara BH, Reis JD, Fer-reira BP, Pereira GA, Borges MF. Assess-ment of basal and gonadotropin-releasing hormone-stimulated gonadotropins by im-munochemiluminometric and immuno-fluorometric assays in normal children. J Clin Endocrinol Metab 2007;92:1424-9.
Neely EK, Wilson DM, Lee PA, Stene M, Hintz RL. Spontaneous serum gonad-otropin concentrations in the evaluation of precocious puberty. J Pediatr 1995;127: 47-52.
Liu G, Duranteau L, Carel J-C, Monroe J, Doyle DA, Shenker A. Leydig-cell tumors caused by an activating mutation of the gene encoding the luteinizing hormone receptor. N Engl J Med 1999;341:1731-6.
Stanhope R. Gonadotrophin-depen-dent precocious puberty and occult intra-cranial tumors: which girls should have neuro-imaging? J Pediatr 2003;143:426-7.
De Sanctis V, Corrias A, Rizzo V, et al. Etiology of central precocious puberty in males: the results of the Italian Study Group for Physiopathology of Puberty.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
Copyright © 2008 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by PATRICK GIRAUD MD on May 29, 2008 .

clinical pr actice
n engl j med 358;22 www.nejm.org may 29, 2008 2377
J Pediatr Endocrinol Metab 2000;13: Suppl 1:687-93.
Lahlou N, Carel JC, Chaussain JL, Roger M. Pharmacokinetics and pharma-codynamics of GnRH agonists: clinical implications in pediatrics. J Pediatr Endo-crinol Metab 2000;13:Suppl 1:723-37.
Leschek EW, Jones J, Barnes KM, Hill SC, Cutler GB Jr. Six-year results of spi-ronolactone and testolactone treatment of familial male-limited precocious puberty with addition of deslorelin after central puberty onset. J Clin Endocrinol Metab 1999;84:175-8.
Feuillan P, Calis K, Hill S, Shawker T, Robey PG, Collins MT. Letrozole treat-ment of precocious puberty in girls with the McCune-Albright syndrome: a pilot study. J Clin Endocrinol Metab 2007;92: 2100-6.
Eugster EA, Rubin SD, Reiter EO, Plourde P, Jou HC, Pescovitz OH. Tamoxi-fen treatment for precocious puberty in McCune-Albright syndrome: a multicenter trial. J Pediatr 2003;143:60-6.
Soriano-Guillén L, Lahlou N, Chauvet G, Roger M, Chaussain JL, Carel JC. Adult height after ketoconazole treatment in patients with familial male-limited pre-cocious puberty. J Clin Endocrinol Metab 2005;90:147-51.
Neely EK, Hintz RL, Parker B, et al. Two-year results of treatment with depot leuprolide acetate for central precocious puberty. J Pediatr 1992;121:634-40.
Carel JC, Blumberg J, Seymour C, Ad-amsbaum C, Lahlou N. Three-month sus-tained-release triptorelin (11.25 mg) in the treatment of central precocious puberty. Eur J Endocrinol 2006;154:119-24.
36.
37.
38.
39.
40.
41.
42.
Bhatia S, Neely EK, Wilson DM. Se-rum luteinizing hormone rises within minutes after depot leuprolide injection: implications for monitoring therapy. Pedi-atrics 2002;109(2):E30.
Klein KO, Barnes KM, Jones JV, Feuil-lan PP, Cutler GB Jr. Increased final height in precocious puberty after long-term treat-ment with LHRH agonists: the National Institutes of Health experience. J Clin En-docrinol Metab 2001;86:4711-6.
Paul DL, Conte FA, Grumbach MM, Kaplan SL. Long-term effect of gonado-tropin-releasing hormone agonist therapy on final and near-final height in 26 chil-dren with true precocious puberty treated at a median age of less than 5 years. J Clin Endocrinol Metab 1995;80:546-51.
Carel JC, Roger M, Ispas S, et al. Final height after long-term treatment with trip-torelin slow release for central precocious puberty: importance of statural growth after interruption of treatment. J Clin En-docrinol Metab 1999;84:1973-8.
Heger S, Muller M, Ranke M, et al. Long-term GnRH agonist treatment for female central precocious puberty does not impair reproductive function. Mol Cell Endocrinol 2006;254-255:217-20.
Carel JC, Lahlou N, Jaramillo O, et al. Treatment of central precocious puberty by subcutaneous injections of leuprorelin 3-month depot (11.25 mg). J Clin Endocri-nol Metab 2002;87:4111-6.
Boot AM, de Muinck Keizer-Schrama S, Pols HA, Krenning EP, Drop SL. Bone mineral density and body composition be-fore and during treatment with gonado-tropin-releasing hormone agonist in chil-dren with central precocious and early
43.
44.
45.
46.
47.
48.
49.
puberty. J Clin Endocrinol Metab 1998;83: 370-3.
Palmert MR, Mansfield MJ, Crowley WF Jr, Crigler JF Jr, Crawford JD, Boepple PA. Is obesity an outcome of gonadotro-pin-releasing hormone agonist adminis-tration? Analysis of growth and body composition in 110 patients with central precocious puberty. J Clin Endocrinol Metab 1999;84:4480-8.
Bertelloni S, Baroncelli GI, Sorrentino MC, Perri G, Saggese G. Effect of central precocious puberty and gonadotropin- releasing hormone analogue treatment on peak bone mass and final height in fe-males. Eur J Pediatr 1998;157:363-7.
Pectasides D, Pectasides E, Psyrri A. Granulosa cell tumor of the ovary. Cancer Treat Rev 2008;34:1-12.
Linam LE, Darolia R, Naffaa LN, et al. US findings of adnexal torsion in children and adolescents: size really does matter. Pediatr Radiol 2007;37:1013-9.
Pasquino AM, Pucarelli I, Segni M, Matrunola M, Cerroni F, Cerrone F. Adult height in girls with central precocious pu-berty treated with gonadotropin-releasing hormone analogues and growth hormone. J Clin Endocrinol Metab 1999;84:449-52. [Erratum, J Clin Endocrinol Metab 1999; 84:1978.]
Vottero A, Pedori S, Verna M, et al. Final height in girls with central idiopath-ic precocious puberty treated with gonad-otropin-releasing hormone analog and oxandrolone. J Clin Endocrinol Metab 2006;91:1284-7.Copyright © 2008 Massachusetts Medical Society.
50.
51.
52.
53.
54.
55.
collections of articles on the journal’s web site
The Journal’s Web site (www.nejm.org) sorts published articles into more than 50 distinct clinical collections, which can be used as convenient
entry points to clinical content. In each collection, articles are cited in reverse chronologic order, with the most recent first.
Copyright © 2008 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org by PATRICK GIRAUD MD on May 29, 2008 .