prenatal and peripartum care for the patient on …€¦ · prenatal and peripartum care for the...
TRANSCRIPT

Prenatal and Peripartum Care for the Patient on Opiate Replacement
C. Luke Peterson, DOAddiction Medicine Fellow
Swedish Addiction Recovery ServicesMarch 10, 2017


Disclosure
• None

Objectives
1. Understand opioid use disorder during pregnancy and dispel misconceptions
2. Learn how opioid use disorder is managed during pregnancy and after delivery
3. Have confidence in counseling patients with opioid use while pregnant

NIH, National InstituteOn Drug Abuse, 2015

Misconception #1Addiction is a character flaw or moral failing
“It’s time to change how we view addiction…Not as a moral failing but as a chronic illness that must be treated with skill, urgency, and compassion. The way we address this crisis is a test for America.”
Vivek Murthy, MDUS Surgeon General
McCarthy M. US must address addiction as an illness, not as a moral failing, Surgeon General says. BMJ. 2016 Nov 22;355:i6265.

Misconception #1Addiction is a character flaw or moral failing
1998 physician surveyIllicit drug use during pregnancy• 52% favor child abuse for
purpose of removing child from maternal custody
• Favor incarceration• Pediatricians 23%• Family 34%• OB 27%
Abel EL, Kruger M. Physician attitudes concerning legal coercion of pregnant alcohol and drug abusers. Am J Obstet Gynecol. 2002 Apr;186(4):768-72.

Misconception #1Addiction is a character flaw or moral failing
2013 physician surveyBeliefs about nature of addiction
Favor disease model• Psychiatrists• Female doctors• Doctors with Asian heritage• Northeastern US• Age 45-53• Less religious
PCP’s Response
MoralModel
PsychModel
Disease model
Not at all 34% 2% 3%
A little 29% 14% 9%
Somewhat 30% 51% 39%
A lot 7% 33% 51%
Lawrence RE, Rasinski KA, Yoon JD, Curlin FA. Physicians' Beliefs about the nature of addiction: a survey of primary care physicians and psychiatrists. Am J Addict. 2013 May-Jun;22(3):255-60Terplan M, Kennedy-Hendricks A, Chisolm MS. Prenatal Substance Use: Exploring Assumptions of Maternal Unfitness. Subst Abuse. 2015 Sep 20;9(Suppl 2):1-4

“In a perfect world…drug use would be recognized as a medical issue, and legal entanglements would not flow from positive toxicology results. Societal resources would be committed to strengthening family bonds and to the well-being of each family member.”
Misconception #2I can tell who and when to screen in pregnancy
Terplan M, Minkoff H. Neonatal Abstinence Syndrome and Ethical Approaches to the Identification of Pregnant Women Who Use Drugs. Obstet Gynecol. 2017 Jan;129(1):164-167.

Examining Bias
Options for screening
• Selective testing
• Universal testing
• Selective screening
• Universal screening
ACOG, AAP, AMA, CDC• Universal Screening• Questionnaires: 4P’s or CRAFT
Terplan M, Minkoff H. Neonatal Abstinence Syndrome and Ethical Approaches to the Identification of Pregnant Women Who Use Drugs. Obstet Gynecol. 2017 Jan;129(1):164-167.

Screening for substance use

Screening for substance use

Misconception #3“Heroin will make my baby messed up”
Dramatic Increase in Maternal Opioid use and Neonatal Abstinence Syndrome, National Institute on Drug Abuse, Advancing Addiction Science, www.drugabuse.gov. Accessed on February 18, 2017.

Opioids and neurocognitive development and birth defects
Neurodevelopmental effects
Animal models note changes in dendritic length, synaptic plasticity, neuronal proliferation, cholinergic function, increase in apoptosis in dopaminergic cell structures in the hippocampus
• Human studies
– Delay in cognitive function
– Lower verbal, reading, arithmetic ability
– Increased ADHD
– Decreased brain volumeBeckwith AM, Burke SA. Identification of early developmental deficits in infants with prenatal heroin, methadone, and other opioid exposure. Clin Pediatr (Phila). 2015 Apr;54(4):3Yuan Q, Rubic M, Seah J, Rae C, Wright IM, Kaltenbach K, Feller JM, Abdel-Latif ME, Chu C, Oei JL; BOB (Brains, Opioids and Babies) Collaborative group.. Do maternal opioids reduce neonatal regional brain volumes? A pilot study. J Perinatol. 2014 Dec;34(12):909-13. 28-35

Opioids and neurocognitive development and birth defects
Neurodevelopmental effects
• Israel Study, N=160 5-12 year olds– Children exposed to heroin in utero
– Controls:
• 2 groups of normally developing children
• Children with fathers using heroin
• Children born to families with socioeconomic depravation
– Highest rates of inattention in socioeconomic depravation group
– Highest rates of inattention, hyperactivity, aggression children born to opioid using parents raised by biologic parents
– Adopted children preformed normally
Ornoy A, Segal J, Bar-Hamburger R, Greenbaum C. Developmental outcome of school-age children born to mothers with heroin dependency: importance of environmental factors. Dev Med Child Neurol. 2001 Oct;43(10):668-75. PubMed PMID 11665823.
Opioids and neurocognitive development and birth defects
Neurodevelopmental effects
• Nygaard et al, 2015
– N=72 children with opioid and polysubstance exposure
– Assessed at 1, 2, 3, 4.5, 8.5 years
– Controlled for socioeconomic status
• Based on parental education
– Exposed group lower cognitive scores
– Boys scored significantly lower than girls
– Did not see cognition catch up over time
Nygaard E, Moe V, Slinning K, Walhovd KB. Longitudinal cognitive development of children born to mothers with opioid and polysubstance use. Pediatr Res. 2015 Sep;78(3):330-5.

Opioids and neurocognitive development and birth defects
Neurodevelopmental effects
“Children of mothers with heroin dependency, if born without significant neurologic damage seem to have normal intellectual potential, as their IQ can be normal if the children are raised in an enviroment without low SES of neglect.” Orney et al, 2001
“Findings indicate continuous negative processes in children born to mothers with opioid and polysubstanceabuse.” Nygaard et al, 2015

Opioids and neurocognitive development and birth defects
Birth defects
• US Collaboration Perinatal Project 1959 – 1965
– Prospective trial
– Overall opioids with no significant cause of birth defects
– Codeine and respiratory defects not statistically sig
– Propoxyphene and club feet not statistically sig
• Michigan Medicate Data 1985 – 1992
– 229,101 pregnancies, 332 had opioid exposure
– No increase in congenital heart diseaseYazdy MM, Desai RJ, Brogly SB. Prescription Opioids in Pregnancy and Birth Outcomes: A Review of the Literature. J Pediatr Genet. 2015 Apr 1;4(2):56-70.

Opioids and neurocognitive development and birth defects
Birth defects• National Birth Defect Prevention Study 1997 – 2005
• 17,499 mothers with cases of birth defects• 2.6% used opioid analgesic use 4-12 weeks • Increased risk of:
– All CHD OR 1.4 (95% CI 1.1-1.7)– Spina bifida OR 2.0 (95% CI 1.3-3.2)– Hydrocephaly OR 2.0 (95% CI 1.0-3.7)
Broussard CS, Rasmussen SA, Reefhuis J, Friedman JM, Jann MW, Riehle-Colarusso T, Honein MA; National Birth Defects Prevention Study.. Maternal treatment with opioid analgesics and risk for birth defects. Am J Obstet Gynecol. 2011 Apr;204(4):314.e1-11.

Opioids and neurocognitive development and birth defects
Neurodevelopmental effects and birth defects
• Carefully consider control groups in these studies
• Environment plays a major role in development
• Women with substance use disorder have increased incidence of other risk factors
• Risk for birth defects remains unclear

Misconception #4“Opioids cause maternal
pregnancy complications”
Pregnancy complications
• Pre-eclampsia
• Premature labor
• Premature preterm rupture of membranes
• Placental insufficiency
• Placental abruption
• Intrauterine growth restriction
• Intrauterine fetal demise
• Low birth weight
• Small head circumference
• Neonatal withdrawal syndrome
Ross EJ, Graham DL, Money KM, Stanwood GD. Developmental consequences of fetal exposure to drugs: what we know and what we still must learn. Neuropsychopharmacology. 2015 Jan;40(1):61-87.

Misconception #5“All I need to do is detox from everything”
Opioid detoxification during pregnancy
Stewart et al, 2013
– N=95 pregnant women detoxed with methadone• 53% patients successfully completed detox
• 32% left the study
Jones et al, 2017– Reviewed 500 documented cases of opioid detox– Opioid detoxification associated with:
• Less time in treatment, fewer prenatal care visits, less likely to deliver at study hospital
– No fetal losses attributed to medically assisted withdrawal
– Relapse 17-96% (average 48%)Stewart RD, Nelson DB, Adhikari EH, McIntire DD, Roberts SW, Dashe JS, Sheffield JS. The obstetrical and neonatal impact of maternal opioid detoxification in pregnancy. Am J Obstet Gynecol. 2013 Sep;209(3):267.e1-5.Jones HE, Terplan M, Meyer M. Medically Assisted Withdrawal (Detoxification): Considering the Mother-Infant Dyad. J Addict Med. 2017 Jan 11

Misconception #5“All I need to do is detox from everything”
Opioid detoxification during pregnancy
• Detoxification not recommended due to:– Decreased neonatal birth weight
– Decreased prenatal care
– Illicit drug relapse
– Resumption of high risk behaviors (IVDU, prostitution, criminal activity)
Medication assisted treatment (MAT)
• Reported success rates 63-82%
Krans EE, Patrick SW. Opioid Use Disorder in Pregnancy: Health Policy and Practice in the M idst of an Epidemic. Obstet Gynecol. 2016 Jul;128(1):4-10. doi
Misconception #6“Opioids will make my baby small”

Misconception #6“Opioids will make my baby small”
MJ Cocaine OpioidsSmoking+10/day
Heavy drinking
Unadjusted -250 -475 -462 -543 -438
Adjusted* -24 -142 -85 -158 -30
*Adjusted for social, psychosocial, behavioral, and biomedical factorsSchemph and Strobino, 2008
Opioid use and decreases in birth weight (grams)
Schempf AH, Strobino DM. Illicit drug use and adverse birth outcomes: is it drugs or context? J Urban Health. 2008 Nov;85(6):858-73.

Misconception #6“Opioids will make my baby small”
Norgaard et al, 2015• Danish retrospective study• N=564 compared to general population
• Low birth weight (LBW) <2,500 grams• Small for gestational age (SGA) <2x SD• Prevalence risk for opioid exposed (95% CI)
Opioid v.General population
Opioid + smoking vGen pop + smoking
LBW 4.3 (3.0-6.1) 2.7 (1.9-3.9)
SGA 2.7 (1.8-4.1) 1.5 (1.0-2.4)
Nørgaard M, Nielsson MS, Heide-Jørgensen U. Birth and Neonatal Outcomes Following Opioid Use in Pregnancy: A Danish Population-Based Study. Subst Abuse. 2015 Oct 9;9(Suppl 2):5-11

Misconception #7“Methadone or buprenorphine is trading one
addiction for another”

Substance use disorder v Physical dependence
• Opioid use disorder (DSM V)
– Problematic pattern of use leading to clinically significant impairment or distress (in past 12 mo)
1. Taken in larger amounts or longer duration
2. Desire to cut back or unsuccessful efforts to cut back
3. Great deal of time obtaining, using, or recovering
4. Craving, strong desire, urge
5. Recurrent use resulting in failure to fulfill obligations
6. Continued use despite persistent or recurrent social or intrapersonal problems

Substance use disorder v Physical dependence
• Opioid use disorder (DSM V)
– Problematic pattern of use leading to clinically significant impairment or distress (in past 12 mo)
7. Give up important social, occupational, recreational activities
8. Recurrent use in physically hazardous situations
9. Continued use despite knowing physical or psychological problems
10. Tolerance*
11. Withdrawal*

Substance use disorder v Physical dependence
• Physical dependence
– Tolerance: loss of effect after repeated use, leading to need for higher doses to achieve desired effect
– Withdrawal: constellation of unpleasant symptoms that occur after abstinence to a substance

Medication Assisted Treatment
Methadone
• Full opioid agonist
• T1/2= 36-48 hours
• Dosed at certified opioid treatment program
Buprenorphine
• Partial opioid agonist
• T1/2: 36 hours
• Physicians & PA and ARNP*
• Combination naloxone to prevent diversion

Misconception #8“Buprenorphine is better than methadone”
MethadonePros:• Daily observed dose• Less risk for diversion• Full opioid agonist
– No precipitated withdrawal
• Ancillary services at methadone clinic
• Better retentionCons:• Daily observed dose• QTc prolongation• Medication interaction• Prolonged induction• More stigma• Less available in rural area
BuprenorphinePros:• Office based treatment • Less stigma• Less overdose risk• Induction fasterCons:• Withdrawal to start• Partial opioid agonist
– Risk of precipitated withdrawal
• Higher diversion risk• Ceiling effect for high
equivalence doses• Fewer prescribers

Misconception #9“I don’t want my baby born addicted”
“I don’t want my baby to go through withdrawal”
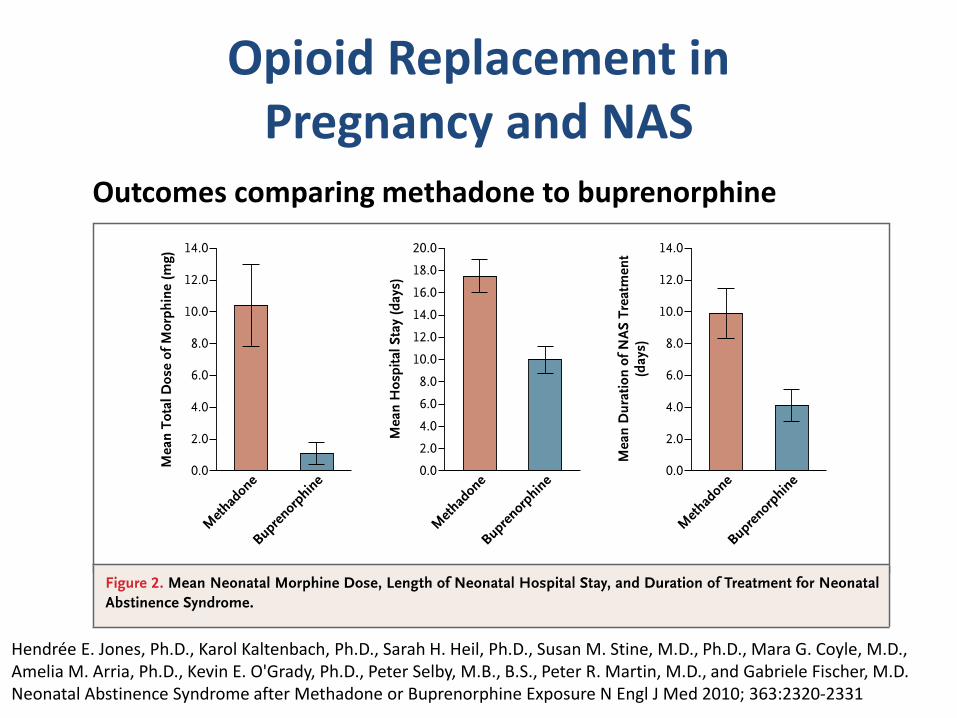
Opioid Replacement in Pregnancy and NAS
Outcomes comparing methadone to buprenorphine
Hendrée E. Jones, Ph.D., Karol Kaltenbach, Ph.D., Sarah H. Heil, Ph.D., Susan M. Stine, M.D., Ph.D., Mara G. Coyle, M.D., Amelia M. Arria, Ph.D., Kevin E. O'Grady, Ph.D., Peter Selby, M.B., B.S., Peter R. Martin, M.D., and Gabriele Fischer, M.D. Neonatal Abstinence Syndrome after Methadone or Buprenorphine Exposure N Engl J Med 2010; 363:2320-2331

Neonatal Abstinence Syndrome
• Pearls:• Explain ORT as a healthy treatment in pregnancy and
treatment as NAS as part of it• Prepare and set expectations • Compare to glucose in neonates of GDM• Encourage mother to be mother• NAS improved with rooming in and skin to skin• NAS improved with breastfeeding
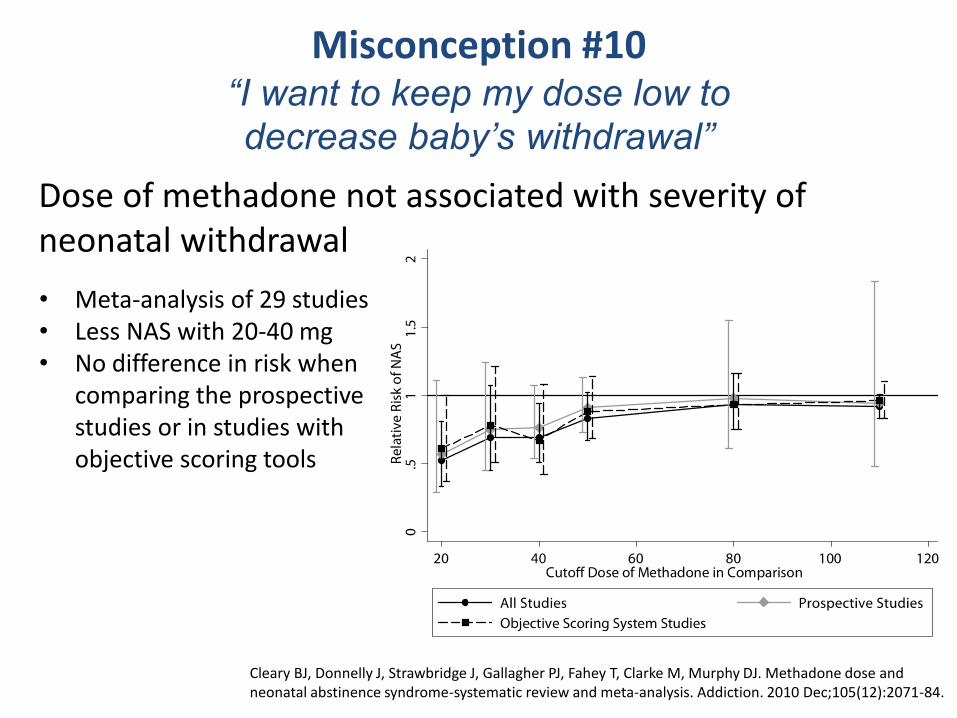
Misconception #10“I want to keep my dose low to
decrease baby’s withdrawal”
Dose of methadone not associated with severity of neonatal withdrawal
• Meta-analysis of 29 studies• Less NAS with 20-40 mg• No difference in risk when
comparing the prospective studies or in studies with objective scoring tools
Cleary BJ, Donnelly J, Strawbridge J, Gallagher PJ, Fahey T, Clarke M, Murphy DJ. Methadone dose and neonatal abstinence syndrome-systematic review and meta-analysis. Addiction. 2010 Dec;105(12):2071-84.
Misconception #11“I’ll have to be on methadone the rest of my life”
“I’ll taper off after I deliver”
Wilder C, Lewis D, Winhusen T. Medication assisted treatment discontinuation in pregnant and postpartum women with opioid use disorder. Drug Alcohol Depend. 2015 Apr 1;149:225-31.
Discontinuation rates:• Prenatal: 0-33%• Postpartum: 26-64%• 50% will be off
methadone by 6 months
Encourage treatment as long as it is working• At least 1 year

Misconception #14“ORT is adequate for acute pain”
“You can’t have adequate pain relief on ORT”
“Prescribing opioids for pain will cause relapse”

Acute pain management while on buprenorphine or methadone
• Home dose not enough for acute severe pain • Possible to have adequate pain control after delivery
– Consider high affinity opioid mu receptor agonists• 2-4 times the normal dose • Hydromorphone PCA• Hydromorphone (Dilaudid) approx 3-6 mg q3h
– Morphine (Duromorph) spinal (18hrs)– Utilize non-opioid medications like APAP & NSAIDs– Mildfulness, stress reduction
• No studies show that prescribing opioids for acute pain will cause relapse
Alford DP, Compton P, Samet JH. Acute pain management for patients receiving maintenance methadone or buprenorphine therapy. Ann Intern Med. 2006 Jan 17;144(2):127-34. Review. Erratum in: Ann Intern Med. 2006 Mar 21;144(6):460. Meyer M, Wagner K, Benvenuto A, Plante D, Howard D. Intrapartum and postpartum analgesia for women maintained on methadone during pregnancy. Obstet Gynecol. 2007 Aug;110(2 Pt 1):261-6.

Conclusions
• Opioid use disorder is a complex neurobiological, psychosocial disease

Conclusions
• Universally screen all pregnant women for substance use with 4Ps or CRAFT

Conclusions
• Opioid exposure in utero may be linked with neurocognitive deficits in children which may be overcome by environmental stability

Conclusions
• Lack of adequate control in studies and complicated confounders makes it difficult to ascertain if in utero exposure of opioids causes birth defects
Conclusions
• Opioid use during pregnancy is associated with poorer obstetrical outcomes
Conclusions
• Medication assisted treatment with methadone or buprenorphine is the standard of care for opioid use during pregnancy

Conclusions
• Methadone dose does not equate to severity of NAS

Conclusions
• NAS less incidence, severity, duration with buprenorphine compared with methadone

Conclusions
• Adequate pain control possible with on opioid replacement therapy

Work cited
• Krans EE, Patrick SW. Opioid Use Disorder in Pregnancy: Health Policy and Practice in the M idst of an Epidemic. Obstet Gynecol. 2016 Jul;128(1):4-10.
• Stoklosa H, MacGibbon M, Stoklosa J. Human Trafficking, Mental Illness, and Addiction: Avoiding Diagnostic Overshadowing. AMA J Ethics. 2017 Jan 1;19(1):23-34.
• Ross EJ, Graham DL, Money KM, Stanwood GD. Developmental consequences of fetal exposure to drugs: what we know and what we still must learn. Neuropsychopharmacology. 2015 Jan;40(1):61-87.
• Dramatic Increase in Maternal Opioid use and Neonatal Abstinence Syndrome, National Institute on Drug Abuse, Advancing Addiction Science, www.drugabuse.gov. Accessed on Februrary 18, 2017. https://www.drugabuse.gov/related-topics/trends-statistics/infographics/dramatic-increases-in-maternal-opioid-use-neonatal-abstinence-syndrome
• Terplan M, Minkoff H. Neonatal Abstinence Syndrome and Ethical Approaches to the Identification of Pregnant Women Who Use Drugs. Obstet Gynecol. 2017 Jan;129(1):164-167.
• Abel EL, Kruger M. Physician attitudes concerning legal coercion of pregnant alcohol and drug abusers. Am J Obstet Gynecol. 2002 Apr;186(4):768-72.
Work cited
• Yazdy MM, Desai RJ, Brogly SB. Prescription Opioids in Pregnancy and Birth Outcomes: A Review of the Literature. J Pediatr Genet. 2015 Apr 1;4(2):56-70
• Beckwith AM, Burke SA. Identification of early developmental deficits in infants with prenatal heroin, methadone, and other opioid exposure. Clin Pediatr (Phila). 2015 Apr;54(4):328-35.
• Yuan Q, Rubic M, Seah J, Rae C, Wright IM, Kaltenbach K, Feller JM, Abdel-Latif ME, Chu C, Oei JL; BOB (Brains, Opioids and Babies) Collaborative group.. Do maternal opioids reduce neonatal regional brain volumes? A pilot study. J Perinatol. 2014 Dec;34(12):909-13.
• Nygaard E, Moe V, Slinning K, Walhovd KB. Longitudinal cognitive development of children born to mothers with opioid and polysubstance use. Pediatr Res. 2015 Sep;78(3):330-5
• Nørgaard M, Nielsson MS, Heide-Jørgensen U. Birth and Neonatal Outcomes Following Opioid Use in Pregnancy: A Danish Population-Based Study. Subst Abuse. 2015 Oct 9;9(Suppl2):5-11.
• Ornoy A, Segal J, Bar-Hamburger R, Greenbaum C. Developmental outcome of school-age children born to mothers with heroin dependency: importance of environmental factors. DevMed Child Neurol. 2001 Oct;43(10):668-75.
• Stewart RD, Nelson DB, Adhikari EH, McIntire DD, Roberts SW, Dashe JS, Sheffield JS. The obstetrical and neonatal impact of maternal opioid detoxification in pregnancy. Am J ObstetGynecol. 2013 Sep;209(3):267.e1-5.

Work cited
• Schempf AH, Strobino DM. Illicit drug use and adverse birth outcomes: is it drugs or context? J Urban Health. 2008 Nov;85(6):858-73.
• Hendrée E. Jones, Ph.D., Karol Kaltenbach, Ph.D., Sarah H. Heil, Ph.D., Susan M. Stine, M.D., Ph.D., Mara G. Coyle, M.D., Amelia M. Arria, Ph.D., Kevin E. O'Grady, Ph.D., Peter Selby, M.B., B.S., Peter R. Martin, M.D., and Gabriele Fischer, M.D. Neonatal Abstinence Syndrome after Methadone or Buprenorphine Exposure N Engl J Med 2010; 363:2320-2331
• Gaalema DE, Scott TL, Heil SH, Coyle MG, Kaltenbach K, Badger GJ, Arria AM, Stine SM, Martin PR, Jones HE. Differences in the profile of neonatal abstinence syndrome signs in methadone- versus buprenorphine-exposed neonates. Addiction. 2012 Nov;107 Suppl 1:53-62.

end


Opioid Replacement in Pregnancy and NAS
NAS - methadone compared to buprenorphine
Gaalema DE, Scott TL, Heil SH, Coyle MG, Kaltenbach K, Badger GJ, Arria AM, Stine SM, Martin PR, Jones HE. Differences in the profile of neonatal abstinence syndrome signs in methadone- versus buprenorphine-exposed neonates. Addiction. 2012 Nov;107 Suppl 1:53-62.

Side effects of MAT
• Feb 2017
– N=49 Buprenorphine maintained pregnant women
• Monitored 60 min peak and trough @ 24, 28, 32, 36 wk
• Decrease in peak and trough fetal HR by 2-5 bpm
• Decreased activity
• Does not effect accelerations

Diagnostic Overshadowing
“Diagnostic overshadowing refers to a well-described clinically and ethically problematic phenomenon in which clinicians ignore patients’ general health concerns because of that patient’s mental illness… such that legitimate general health problems are misattributed as originating from a patient’s mental illness “
Artist Kumi Yamashita
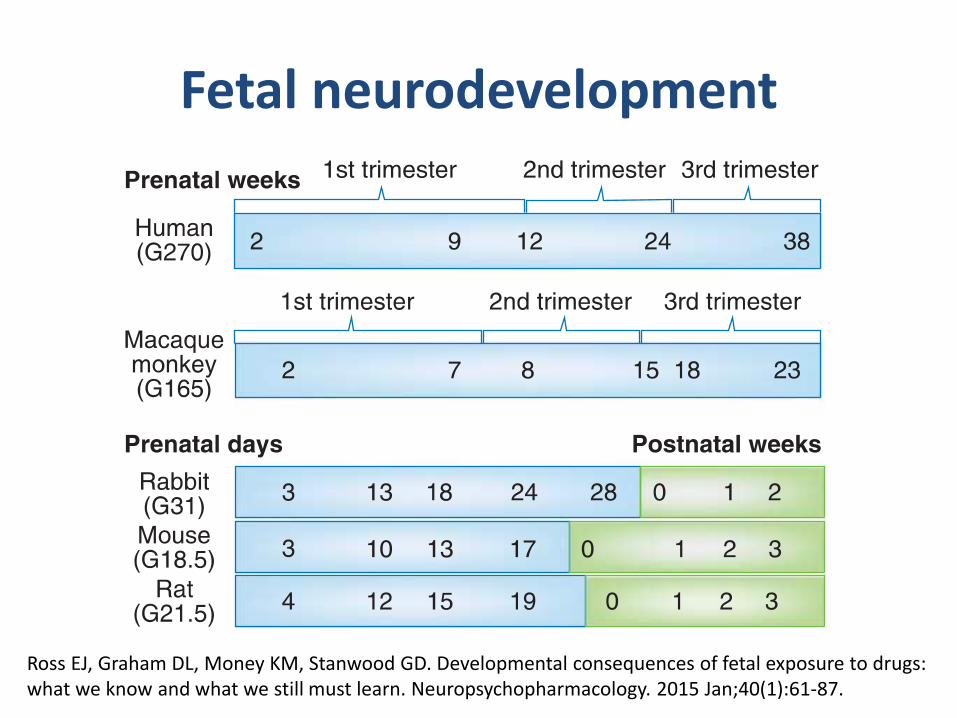
Fetal neurodevelopment
Ross EJ, Graham DL, Money KM, Stanwood GD. Developmental consequences of fetal exposure to drugs: what we know and what we still must learn. Neuropsychopharmacology. 2015 Jan;40(1):61-87.

Misconception #5“All I need to do is detox from everything”
Opioid detoxification during pregnancy
Luty et al, 2003
– No clear evidence of safety for detoxification
– 101 pregnant women underwent 21 day detox
– One first trimester SAB, 1 premature delivery
Jones et al, 2008– Methadone assisted withdrawal during pregnancy
• Less time in treatment, fewer prenatal care visits, less likely to deliver at study hospital
Luty J, Nikolaou V, Bearn J. Is opiate detoxification unsafe in pregnancy? JSubst Abuse Treat. 2003 Jun;24(4):363-7. Jones HE, Terplan M, Meyer M. Medically Assisted Withdrawal (Detoxification): Considering the Mother-Infant Dyad. J Addict Med. 2017 Jan 11

Figure 4. Forest plot of comparison: 1 Flexible dose buprenorphine versus flexible dose methadone,
outcome: 1.1 Retention in treatment.
Comparison 02: Low-dosebuprenorphine versuslow-dose
methadone:
The comparison indicated that low-dose methadone was more
likely to retain participants than low-dose buprenorphine; RR
0.67; 95% CI 0.52 to 0.87; three studies, 253 participants
(Ahmadi 2003a; Kosten 1993; Schottenfeld 1997). See Analysis
2.1.
Comparison 03: Medium-dose buprenorphineversus
medium-dose methadone:
There was no difference between medium-dose buprenorphine
and medium-dosemethadonein theability to retain participants
in treatment, RR 0.87; 95% CI 0.69 to 1.10; seven studies, 780
participants (Johnson 1992; Kamien 2008; Ling 1996; Oliveto
1999; Pani 2000; Schottenfeld 1997; Schottenfeld 2005). See
Analysis3.1.
Comparison 04: High-dose buprenorphineversushigh-dose
methadone:
Therewereno differencesbetween high-dosebuprenorphineand
high-dosemethadonein retention: RR0.79;95% CI 0.20to3.16;
onestudy, 134 participants(Kamien 2008). SeeAnalysis4.1
Comparison 05: Low-dosebuprenorphine maintenance
versusplacebo:
The results showed a benefit for low-dose buprenorphine over
placebo in termsof retaining participants in treatment: RR 1.50;
95% CI 1.19 to 1.88); five studies, 1131 participants (Ahmadi
2002a; Ahmadi 2003a; Ahmadi 2004; Johnson 1995a; Ling
1998). SeeAnalysis5.1.
Comparison 06: Medium-dose buprenorphinemaintenance
versusplacebo:
Theresultsshowedabenefit for medium-dosebuprenorphineover
placebo in termsof retaining participants in treatment: RR 1.74;
95% CI 1.06 to 2.87; four studies, 887 participants (Ahmadi
2003a; Ahmadi 2004; Johnson 1995a; Ling 1998). SeeAnalysis
6.1.
13Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence (Review)
Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Mattick RP, Kimber J, Breen C, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2004;(3):CD002207. Review. Update in: Cochrane Database Syst Rev.2008;(2):CD002207.