principles of immunohematology prepared by hamad alassaf [email protected]
TRANSCRIPT

ImmunohematologyDefinition•The study of immunologic reactions involving all components of blood deals with antigens, antibodies and antigen-antibody reactions.
Application in ……..•Transfusion of blood and its components.•Diagnosis, prevention and management of Immunization as so with pregnancy.•Leukocyte testing for organ transplantation.•Laboratory resolution of parentage problems.

Introduction•The immune system consists of a cellular component and a humoral component.
•The science of Immunohematology deals with the basic principles of antigen and antibody structure, to understand the principles of compatibility testing and transfusion reactions the basic knowledge of Immunohematology is essential.

Antigen• Antigen is a substance which elicits immune response. The ABH antigens are glycolipids while Rh(D) antigen is a protein.• All the blood group substances are not equally immunogenic. Approximately 50 percent of Rh negative recipients of Rh positive blood are expected to be sensitized to the D antigen. Other Rh antigens like C, E and other blood group systems are much less immunogenic. That is the reason that only D and not other Rh antigens are routinely typed in the Blood Bank.• The numbers of antigen sites on the RBC vary according to specificity. There are approximately 1 million ABH antigen sites and 25000 Rh(D) antigen sites on RBC.• Some of the specificities are poorly developed at the time of birth.
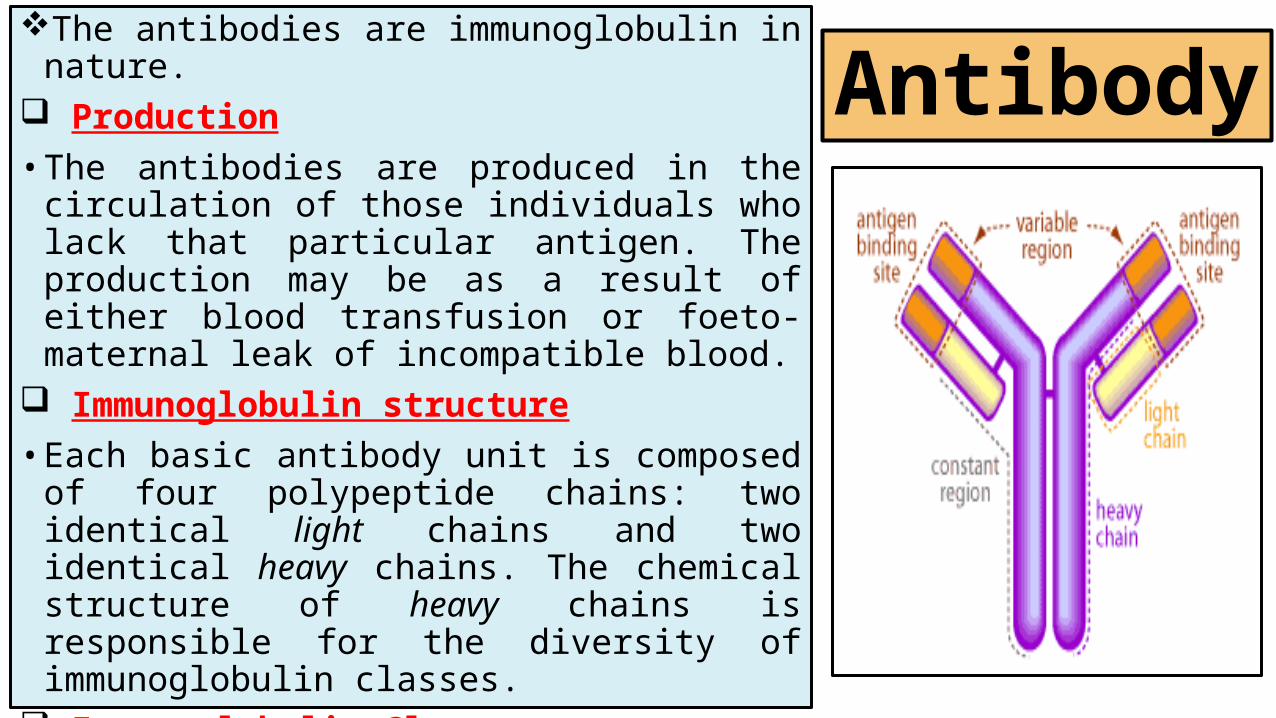
AntibodyThe antibodies are immunoglobulin in
nature. Production• The antibodies are produced in the
circulation of those individuals who lack that particular antigen. The production may be as a result of either blood transfusion or foeto-maternal leak of incompatible blood.
Immunoglobulin structure• Each basic antibody unit is composed of
four polypeptide chains: two identical light chains and two identical heavy chains. The chemical structure of heavy chains is responsible for the diversity of immunoglobulin classes.
Immunoglobulin Classes• The blood antibodies are usually, IgM, IgG
or IgA.• IgG react at 37⁰C and enables to cross the
placental barrier.• IgM react at room temperature (20-25⁰C)
and it does not cross the placental barrier.

Complete and Incomplete Antibodies
The antibodies which are produced without any antigenic stimulus are known as complete antibodies. Most IgM class antibodies fall in this category. They are capable of agglutinating red cells suspended in normal saline at 20-25⁰C. Most of the ABH antibodies are IgM in nature, and they are called natural or complete antibodies.
The antibodies which require a bridge like the Coomb’s sera for binding to the antigenic site are called incomplete antibodies. Most IgG antibodies are incomplete antibodies. They react at 37⁰C. The Rh(CDE) are incomplete or Acquired antibodies.

Monoclonal and Polyclonal antibodies
The antibodies which are derived from multiple ancestral clones of antibody producing cells and which carry both kappa and lambda light chains are termed as polyclonal antibodies. In contrast some of the antibodies contain exclusively kappa or lambda light chains are known as monoclonal antibodies. Because monoclonal antisera have the ability to recognize single antigenic epitopes, this provides greater diagnostic precision than polyclonal antisera.

Antigen Antibody Ratio
The speed by which antigen and antibody bind, is dependent on number of antibody molecules in the medium and the antigen sites available on the cell. By raising the serum to cell ratio the number of molecules are increased. If 2 drops of cell suspension is added to 4 drops of serum, it increases the sensitivity of the test. The other factors affecting the binding of antigen antibody are pH, temperature and incubation period.

Complement•The complements are serum proteins which interact with bound antibodies resulting in cell lysis and enhanced phagocytosis. •The nine components of complements are designated C1 to C9. •The complements are destroyed when heated with anticoagulants to 56⁰C for 30minutes.

Sensitization• The sensitization is defined as binding of antigen and antibody, in vitro or in vivo with or without agglutination.

Agglutination •Whenever the sensitized cells come into contact of each other the end result is clumping of red cells known as agglutination.
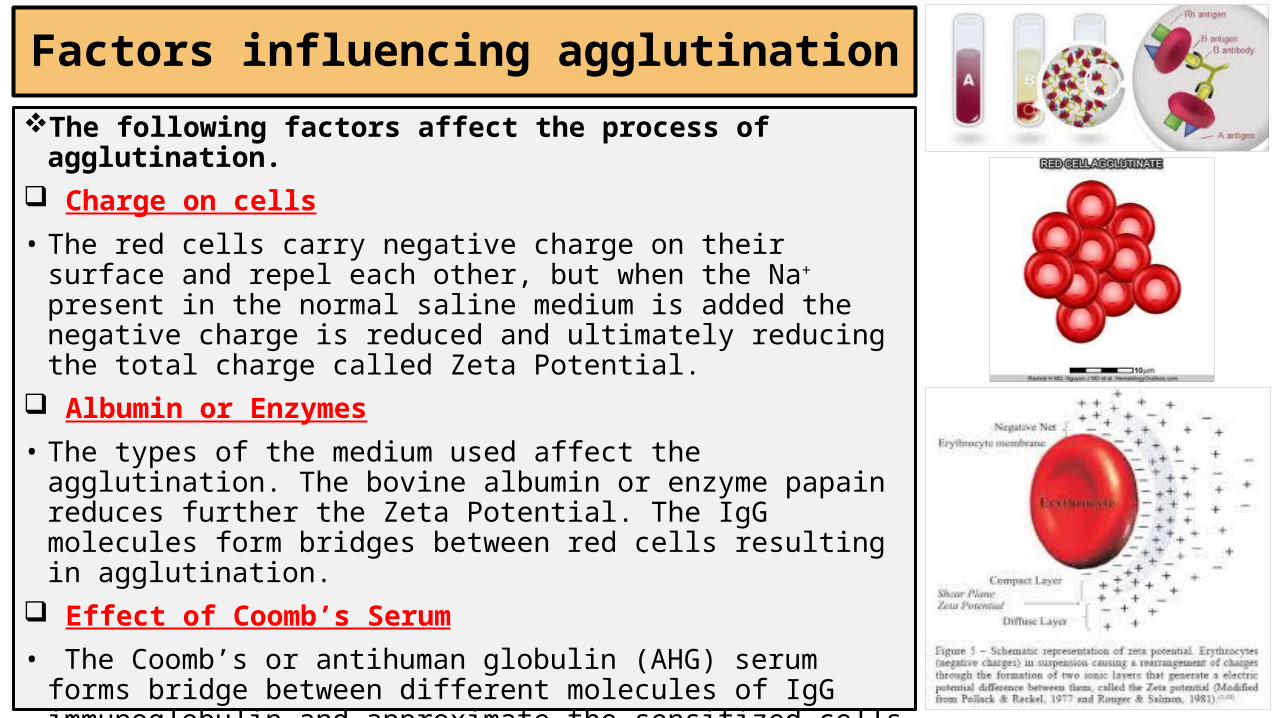
Factors influencing agglutinationThe following factors affect the process of
agglutination. Charge on cells
• The red cells carry negative charge on their surface and repel each other, but when the Na+ present in the normal saline medium is added the negative charge is reduced and ultimately reducing the total charge called Zeta Potential.
Albumin or Enzymes
• The types of the medium used affect the agglutination. The bovine albumin or enzyme papain reduces further the Zeta Potential. The IgG molecules form bridges between red cells resulting in agglutination.
Effect of Coomb’s Serum
• The Coomb’s or antihuman globulin (AHG) serum forms bridge between different molecules of IgG immunoglobulin and approximate the sensitized cells bringing about agglutination.
Hemolysis
• The antigen and antibody reaction where complement is activated and leads to breakdown of red cells and release of hemoglobin is called hemolysis.

ABO Blood Group System
Introduction• Karl Landsteiner opened the doors of Blood Banking with his discovery of first Blood Group System, ABO, in the year 1901. The blood groups were divided in A, B and O. A year later, in 1902 the AB Blood Group was discovered by Von Decastello.• The nomenclature of different blood groups is based on the presence or absence of particular antigens on the surface of red cells.
•Genotype - the genetic constitution of the organism•Phenotype - the observable expression of genotype
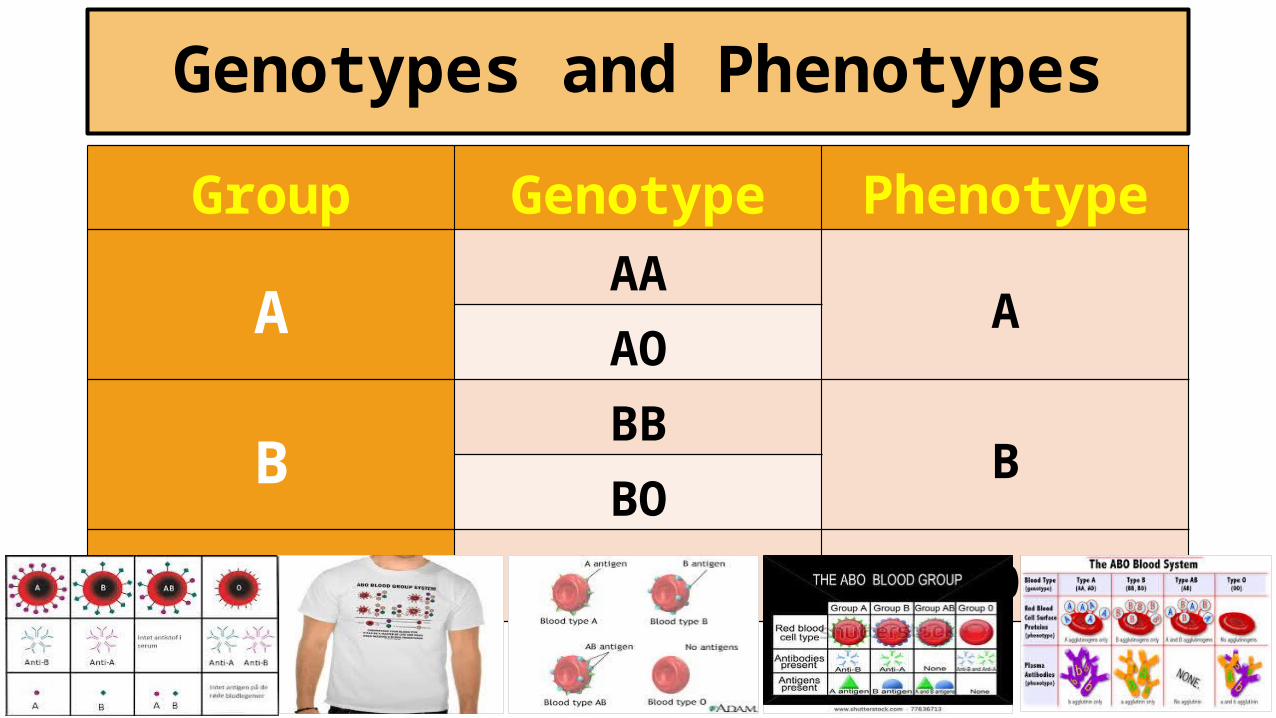
Genotypes and PhenotypesGroup Genotype Phenotype
AAA
AAO
BBB
BBO
O OO O

Antigen and Antibodies of ABO Group
• The Anti-AB present in group “O” individuals carries a higher titer than Anti-A or Anti-B.• The Anti-A and Anti-B present in “O” blood group are more often IgG in nature.• The IgM anti-A and Anti-B in neonates are not produced up to the age of 3 to 6 months. Whatever antibodies are present in a newborn are of maternal origin.
Group Antigens AntibodiesA A & H Anti-B
B B & H Anti-A
AB A, B & H None
O H Anti-A , Anti-B & Anti-AB

Bombay Blood Group
• The “O” blood group individuals normally do not carry either A or B antigen but maximum amount of H antigen. Some individuals are lack even H antigen along with A and B. these individuals are Oh phenotype. Since there is no H antigen on the surface of red cells of Oh, the anti-H antibody develops in their serum, along with all the other antibodies found in any “O” blood group. This Anti-H of Oh is clinically significant, warm antibody reactive at 37⁰C. • This blood group was first discovered in Bombay, Hence its name, by Bhende et al in the year 1952.• The Bombay blood group is not compatible with any “O” blood group, and the only choice of blood for these individuals remains only Bombay itself.
ABO Subgrouping
• The clinically significant subgroups which are detected in the Blood Bank are A1, A2, A1B and A2B.• In 1–8 % of cases of A2 group Anti-A1 is also present beside Anti-B.• The cells of approximately 80% of “A” blood group individuals are A1 while the remaining 20% are A2.• Approximately 22-35% of A2B individuals produce Anti-A1. • The Anti-A1 present in A2 or A2B individuals is usually a cold reactive clinically insignificant antibody, unless it reacts at 37⁰C.

Grouping of Newborn or Cord Blood
•The ABH antigens are not fully developed on the cells of a newborn. The naturally occurring complete antibodies are also not present. So, the reverse grouping is not recommended on newborn’s blood.•The cord blood contains Wharton’s jelly which may lead to error unless the cord cells are thoroughly washed 3-4 times in saline.
The Rh Blood Group System
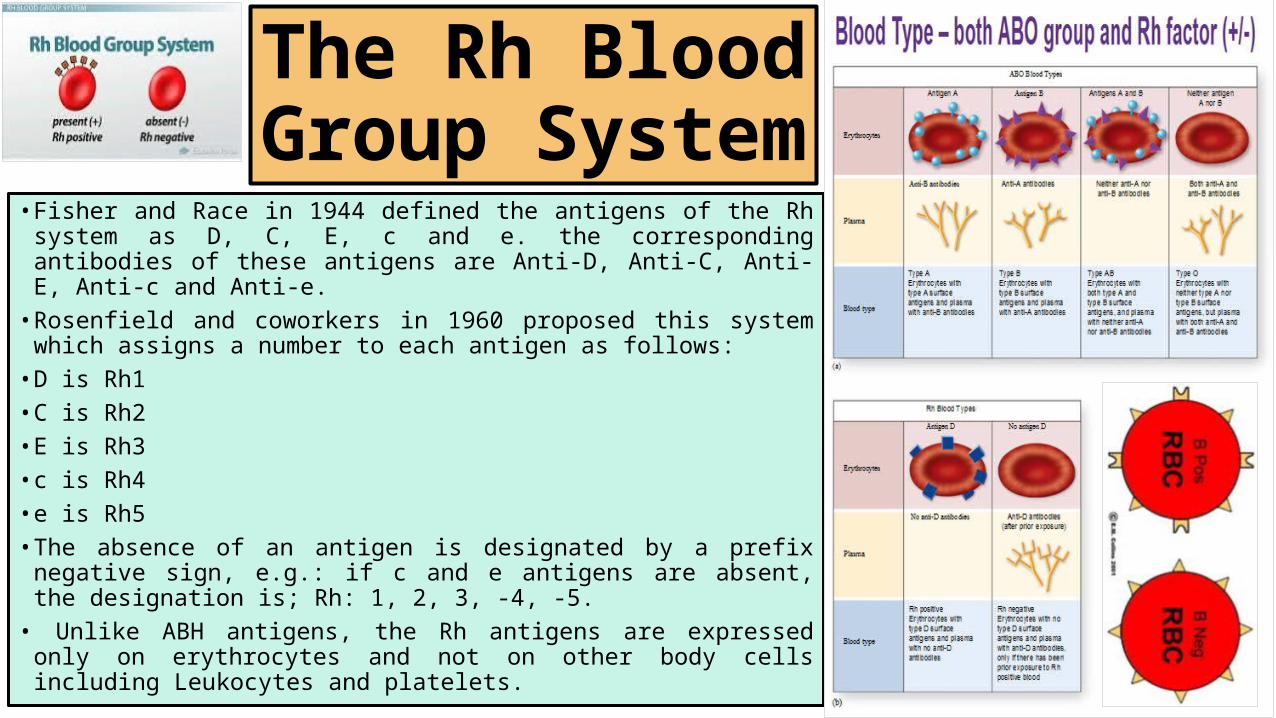
• Fisher and Race in 1944 defined the antigens of the Rh system as D, C, E, c and e. the corresponding antibodies of these antigens are Anti-D, Anti-C, Anti-E, Anti-c and Anti-e.
• Rosenfield and coworkers in 1960 proposed this system which assigns a number to each antigen as follows:
• D is Rh1• C is Rh2• E is Rh3• c is Rh4• e is Rh5• The absence of an antigen is designated by a prefix
negative sign, e.g.: if c and e antigens are absent, the designation is; Rh: 1, 2, 3, -4, -5.
• Unlike ABH antigens, the Rh antigens are expressed only on erythrocytes and not on other body cells including Leukocytes and platelets.



The Rh Blood Group System; Clinical
Significance
•The D antigen is as significant in transfusion practice as A and B antigens. The Anti-D is not found in all D negative individuals. The formation of the Anti-D is always after exposure of a D negative person to D positive blood either through transfusion or pregnancy. More than 80% of D negative persons develop Anti-D after transfusion of a single unit of D positive blood.

The Du (weak D)
• It has been observed that certain D positive red cells are not agglutinated by all anti-D sera, but require AHG (Coomb’s) sera and ICT to show agglutination. This phenomenon is nothing but a weak expression of the antigen. This particular D phenotype is called Du. so; Du is not a different antigen but a differing expression of D antigen. • All Du donor units are considered Rh(D) positive and transfused only to Rh(D)positive recipients. Du patient if recipient considered to receive Rh(D) negative units only. • If the mother carries Anti-D antibody then Du infant is likely to suffer from HDN.

Rh Antibodies
•The Rh antibodies are clinically significant and capable of causing hemolytic transfusion reaction. Except for Anti-C and Anti-E that occur without known stimulus, most of the Rh antibodies result from immunization by transfusion or pregnancy. The Rh antibodies are mostly IgG, and react best in enzyme or antiglobulin medium, but some like Anti-C have been detected is saline test indicating their IgM nature. In general Rh antibodies do not bind complement. Though the ABO-HDN is more common but the Rh antibodies lead to more serious forms of hemolytic disease of Newborn (HDN).

Other Blood Group System
•Beside ABO and Rh there are other blood group systems, but are of less clinical significance. There testing is not carried out as a routine but antibodies of this system have also been found causing hemolytic transfusion reaction (HTR) and hemolytic disease of newborn (HDN).

Some of the other blood group systems are given below:
LEWIS BLOOD GROUP SYSTEM- Lewis antigens are Lea and Leb.- Lewis Antibodies are cold reacting IgM antibodies which bind
complement. They are Anti-Lea and Anti-Leb. Lewis antibodies do not cause HDN. Also, Anti-Leb does not cause HTR.
MNS BLOOD GROUP SYSTEM- MNS antigens are M, N, and S- Antibodies of MNS systemAnti-M: IgM & IgG can cause HDNAnti-N: IgM does not cause HTR & HDN.Anti-S & Anti-s: warm antibodies reacting most by ICT. Can
cause HTR & HDN.

P BLOOD GROUP SYSTEM- The main antigens are P1 & P.
- Antibodies are: Anti-P1: IgM, clinically insignificant antibody. Anti-P : IgG, may cause HTR. li BLOOD GROUP SYSTEM- antigens : I & i- Antibodies are: Anti-I : IgM, rare causes HTR. Anti-i : this is a cold reactive auto-agglutinin. It has been detected in the
sera of patients of infectious mononucleosis. Clinically insignificant. KELL BLOOD GROUP SYSTEM- Antigens are K & k and infrequently Kpa & Kpb.- Antibodies are Anti-K, Anti-k, Anti-Kpa & Anti-Kpb. These antibodies react
mostly in ICT. They may cause HTR & mild degree of HDN.

KIDD BLOOD GROUP SYSTEM- Antigens are JKa & JKb.- Antibodies: Anti-JKa & JKb are IgG antibodies detected by ICT only. The
antibodies cause mild HDN and delayed HTR.
DUFFY BLOOD GROUP SYSTEM- Antigens: are Fya & Fyb.- Antibodies: Anti-Fya & Anti-Fyb are warm antibodies, detected by ICT. Can
cause HTR & HDN.
LUTHERAN BLOOD GROUP SYSTEM- Antigens: are Lua & Lub.- Antibodies: Anti-Lua: react at room temperature. It dose not cause HTR but may lead
to mild HDN. Anti-Lub: This reacts in ICT and may cause HTR and Mild HDN.

CrossMatching (Compatibility Testing)
• The compatibility testing includes, ABO and Rh typing on the donor and recipient blood samples screening of donor’s and patient’s sera for unexpected alloantibody detection and finally a cross match.
• The crossmatching is two types: Major cross match & Minor crossmatch.•Major Crossmatch: Donor’s cells + Patient’s serum.•Minor Crossmatch: Donor’s serum + Patient’s cells.
References 1. Technical Manual of the American Association of Blood Banks. Bethesda, MD: American Association of Blood Banks.2. Standards for Blood Banks and Transfusion Services. Bethesda, MD: American Association of Blood Banks.3. Essential of Blood Banking. SR Mehdi MD Reader/Associate Professor. JN Medical College, AMU, Aligarh, India.