immunohematology a student review -...
TRANSCRIPT

5/13/2015
1
ImmunohematologyA Student Review
Scott C. Wise, MS, MT(ASCP)SBB
Associate Professor, Georgia Regents University
American Society for Clinical Laboratory Science – Georgia
2015 Annual Meeting
May 16, 2015
Part I
Blood Group Systems

5/13/2015
2
Genetics
Fig. 3‐2 Difference between phenotype and genotype. The difference between the genotype and phenotype is illustrated
in this diagram of ABO system inheritance patterns.
Inheritance Patterns:
Autosomal Codominant: (most)Autosomal Dominant: A/O, B/ORecessive (silent/amorphic): O/O, dd, Fy, Jk)Suppressor: In(Jk), In(Lu)
Zygosity: homozygous or heterozygous? (e.g., Fy(a‐b+) or Fy(a+b+)
QC ‐ ?Antibody Rule Outs ‐ ?
Chemistry/Antigens (general structures)
Fig. 4‐1 Model of red cell membrane that carries blood group antigens from blood group systems and collections. The red cell antigens are molecules that form part of the red cell membrane's lipid bilayer or extend from the surface of the red cell.
5/13/2015
3
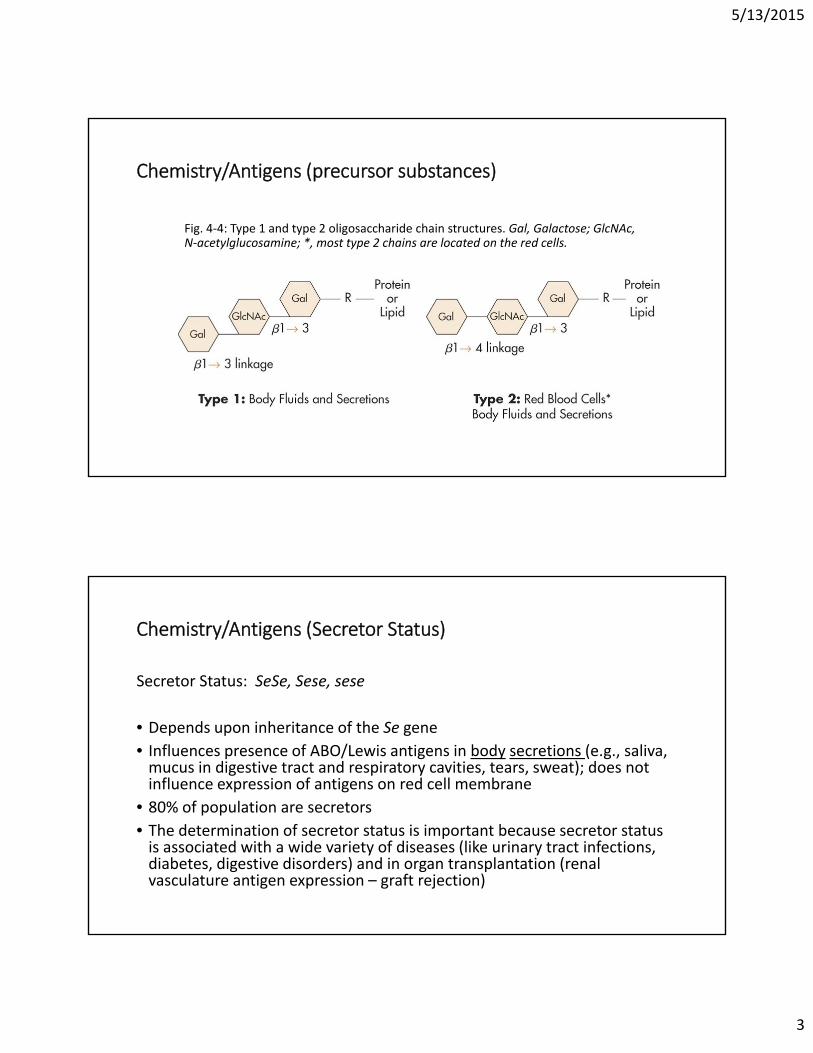
Chemistry/Antigens (precursor substances)
Fig. 4‐4: Type 1 and type 2 oligosaccharide chain structures. Gal, Galactose; GlcNAc, N‐acetylglucosamine; *, most type 2 chains are located on the red cells.
Chemistry/Antigens (Secretor Status)
Secretor Status: SeSe, Sese, sese
• Depends upon inheritance of the Se gene • Influences presence of ABO/Lewis antigens in body secretions (e.g., saliva, mucus in digestive tract and respiratory cavities, tears, sweat); does not influence expression of antigens on red cell membrane
• 80% of population are secretors• The determination of secretor status is important because secretor status is associated with a wide variety of diseases (like urinary tract infections, diabetes, digestive disorders) and in organ transplantation (renal vasculature antigen expression – graft rejection)

5/13/2015
4
Chemistry/Antigens (ABO)
Fig. 4‐5 Biochemical structures of the H, A, and B antigens. Gal, D‐Galactose; GlcNAc, N‐acetylglucosamine; Fuc, L‐fucose; GalNAc, N‐acetylgalactosamine.
Genetics: Expression of A and/or B on RBCs requires the presence of H; no H = ? phenotype
Chemistry/Antigens (H)
Fig. 4‐6 Variation of H‐antigen concentrations in ABO phenotypes. Group O red cells possess the most H antigens; group A1B red cells possess the fewest H antigens.

5/13/2015
5
Chemistry/Antigens (ABO Phenotyping)
TABLE 4‐6 ABO Phenotype Reactions
Chemistry/Antigens (ABO Discrepancies)
TABLE 4-9 Overviews of ABO Discrepancies

5/13/2015
6
Chemistry/Antigens(ABO Discrepancy Flowchart)
Grouping
Forward
Missing/Weak
A/B Subgroup
Disease (cancer)
Extra
Acquired A/B
B(A) Phenotype
Rouleaux
Mixed Field
O Transfusion
Bone Marrow Transplant
Reverse
Missing/Weak
YoungElderly
Immunocompromised
Extra
Cold Autoantibody
Cold Alloantibody
Rouleaux
Anti-A1
Chemistry/Antigens (ABO Discrepancies – see attachment for possible causes/resolutions)
Discrepancy Anti‐A Anti‐B A1 cells B cells O Cells Autocontrol
1 0 0 0 0 0 0
2* 4+ 0 1+ 4+ 0 0
3 4+ 4+ 2+ 2+ 2+ 2+
4 4+ 4+ 1+ 0 0 0
5* 4+ 0 0 4+ 3+ 0
6 0 0 4+ 4+ 4+ 0
7 0 0 2+ 4+ 0 0
8 4+ 2+ 0 4+ 0 0
9 4+ 4+ 2+ 0 2+ 0
10 0 4+ 4+ 1+ 1+ 1+

5/13/2015
7
Chemistry/Antigens (Methodologies – Traditional Tube/Microwell Testing)
Fig. 2-5 Summary of ABO reagents. Blood banks are using monoclonal antibodies for ABO reagents in routine testing.
Fig. 9-4 Results and interpretation of an ABO/Rh phenotype. In the hemagglutination test, agglutination is a positive result, and no agglutination is a negative result.
Chemistry/Antigens (Methodologies – Solid Phase Red Cell Adherence Assay ‐ SPRCA)Fig. 9-6 Reactions and interpretation of SPRCA.

5/13/2015
8
Chemistry/Antigens (Methodologies – Gel Test)
Fig. 9-14 ID-MTS Gel Test procedure for the detection of A, B, and D antigens.
A Subgroup Resolution
Fig. 4‐8 Comparison of A1 and A2 red cells.
TABLE 4-3 Serologic Characteristics of A3, Ax, and Ael Subgroups
Anti‐A1 Lectin (Dolichos biflorus)Anti‐ H Lectin (Ulex Europeus)

5/13/2015
9
Chemistry/Antigens(Lewis)
Fig. 6‐2 Formation of the Lewis antigens
Chemistry/Antigens (Rh Inheritance)
Fig. 5-1 Comparison of Rh genetic theories. Comparison of three Rh genetic theories that have influenced the nomenclature of the Rh blood group system. Modern molecular techniques have established that the Rh blood group system antigens are determined by two genetic loci.

5/13/2015
10
Chemistry/Antigens (RhoD inheritance)
Rh Inheritance:
Fig. 5‐4 Inheritance of the D antigen. Predicting the probability of D‐positive offspring from a D‐negative mother and a heterozygous (Dd) father. The d gene does not exist and is being used only for illustrative purposes. From this mating, it is shown that 50% of the children could be D‐positive.
Fig. 5‐5 D antigen concentration. The D antigen concentration varies with the antigens inherited at the RHCE gene. The D‐deletion phenotype has the most D antigen sites. The C gene weakens the D antigen expression if inherited on the opposite chromosome. R2R2 cells show a higher D expression than R1R1 cells. If anti‐D was reacted with R2R2 cells, they would typically demonstrate a stronger pattern of agglutination.
Chemistry/Antigens (Rh Phenotype & Conversions)
TABLE 5-2 Wiener Theory: Genes and Antigens TABLE 5-3 Converting Fisher-Race Terminology to Wiener Terminology

5/13/2015
11
Chemistry/Antigens (Weak D)
Fig. 5-7 Weak D caused by Ce inherited in trans. D-antigen expression is weaker when the D and Ce genes are inherited on the opposite chromosome.
TABLE 5-7 Weak D Summary
Chemistry/Antigens (Weak D Testing)
Fig. 5‐6 Weak D test procedure
TABLE 5-6 Weak D Test: Interpretation with Control Results

5/13/2015
12
Chemistry/Antigens (HLA – Antigens and Significance)
Fig. 1-16 Major histocompatibility complex (MHC). Transfusion:
Platelet refractoriness –↓post 1 hour count; HLA matched or crossmatched platelets (50/50)
Transplantation:
Graft survival – depends on number of Class I & Class II mismatches; HPC ‐ GVHD
Diagnosis:
Disease markers – B27 (Ankylosing Spondylitis), DQ2 (Celiac disease) Location: most nucleated cells (leukocytes), tissues, platelets, weak
expression on red cells (Bga, Bgb, Bgc)
Sensitizing Events ‐ Pregnancy, Blood Transfusion, Prior Transplant
Chemistry/Antigens (HLA ‐ Testing)
Fig. 1-18 Lymphocytotoxicity test for identification of HLA antigens. Complement and a dye are used to determine whether there is antigen-antibody recognition. Complement-mediated cell membrane damage occurs if the antigen and antibody form a complex. The damaged membrane becomes permeable to the dye, which enters the cell, allowing a positive reaction to be observed. Dye exclusion is a negative reaction.
Other: Flow Cytometry, Luminex, DNA testing (SSO, SSP)
5/13/2015
13
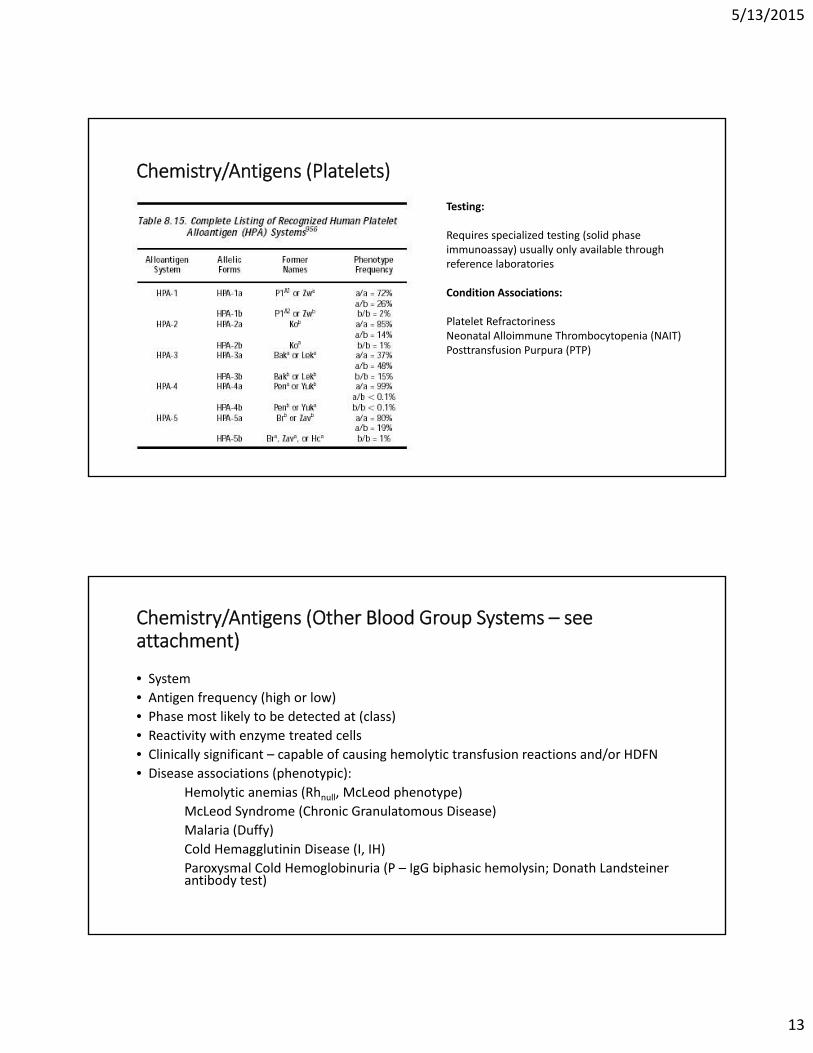
Chemistry/Antigens (Platelets)
Testing:
Requires specialized testing (solid phase immunoassay) usually only available through reference laboratories
Condition Associations:
Platelet RefractorinessNeonatal Alloimmune Thrombocytopenia (NAIT)Posttransfusion Purpura (PTP)
Chemistry/Antigens (Other Blood Group Systems – see attachment)
• System
• Antigen frequency (high or low)
• Phase most likely to be detected at (class)
• Reactivity with enzyme treated cells
• Clinically significant – capable of causing hemolytic transfusion reactions and/or HDFN
• Disease associations (phenotypic):
Hemolytic anemias (Rhnull, McLeod phenotype)
McLeod Syndrome (Chronic Granulatomous Disease)
Malaria (Duffy)
Cold Hemagglutinin Disease (I, IH)
Paroxysmal Cold Hemoglobinuria (P – IgG biphasic hemolysin; Donath Landsteiner antibody test)

5/13/2015
14
Part II
Antibody Screening and Identification
Immunogenecity & Antigen Frequency
• Immunogenicity:
Definition?
Factors?
What is the most immunogenic blood group antigen? 2nd?
• Antigen Frequency (%):
ABO (O = ? A = ? B = ? AB = ?)
Other (low? high?)

5/13/2015
15
Immune System (B & T Cell Interactions)
Immune Response (Macrophages)
Fig. 1‐4 Antibody attaches to the Fc receptor on a macrophage to signal clearance. The variable portion of the immunoglobulin attaches to the antigen on the red cell, while the macrophage attaches to the Fc portion. The red cell is transported to the spleen and liver for clearance.

5/13/2015
16
Immune Response (Primary vs Secondary)
Fig. 1‐6 Primary and secondary immune responses. The initial exposure to an antigen elicits the formation of IgM, followed by IgG antibodies and memory B cells. The second response to the same antigen causes much greater production of IgG antibodies and less IgM antibody secretion.
Immunoglobulin Structure
TABLE 1-2 Comparison of IgM and IgG

5/13/2015
17
Immunoglobulin Structure
Complement
Serum proteins that assist with the clearance of antibody‐coated red cells. Biologic functions include:
Opsonization – enhancing phagocytosis of antigensChemotaxis – attracting macrophages and neutrophilsCell Lysis – rupturing membranes of foreign cellsAgglutination – clustering and binding of pathogens together (sticking)
5/13/2015
18
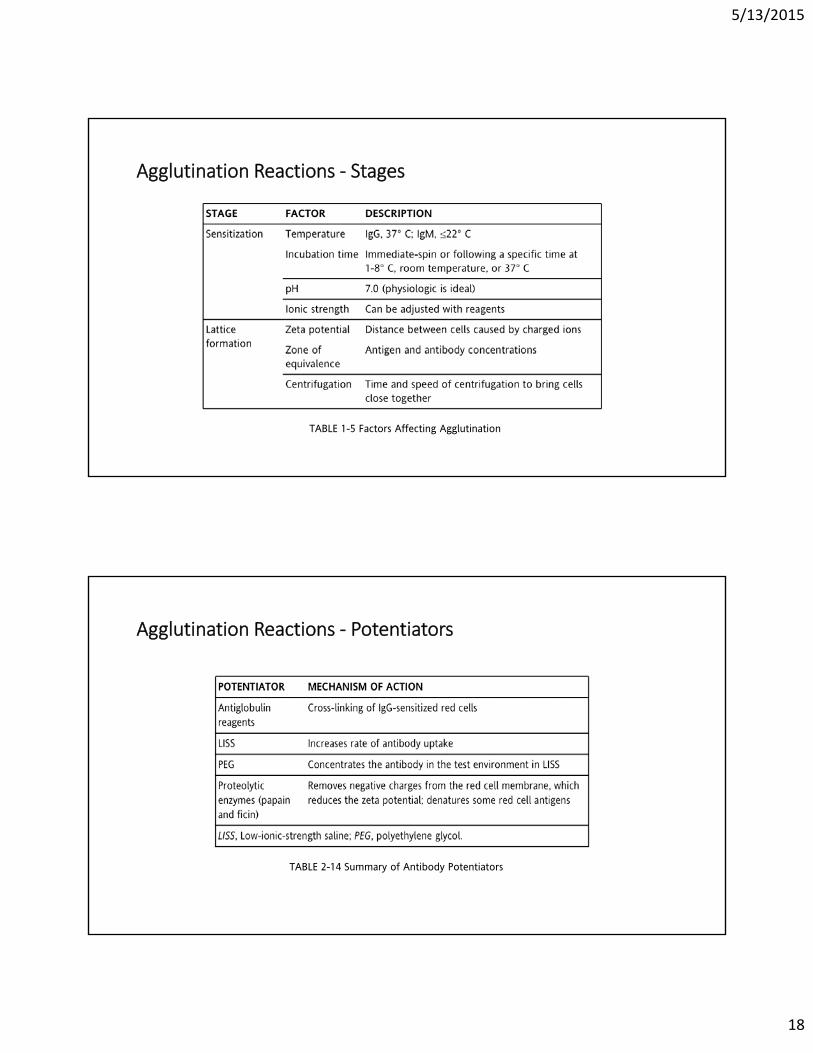
Agglutination Reactions ‐ Stages
TABLE 1-5 Factors Affecting Agglutination
Agglutination Reactions ‐ Potentiators
TABLE 2-14 Summary of Antibody Potentiators

5/13/2015
19
Direct and Indirect Antiglobulin Tests
TABLE 2‐10 Comparison of Direct Antiglobulin Test and Indirect Antiglobulin Test
Sources of Error in Antiglobulin Testing
TABLE 2-11 Common Sources of False-PositiveError in Antiglobulin Testing
TABLE 2-12 Common Sources of False-Negative Error in Antiglobulin Testing

5/13/2015
20
Applications of DAT and IAT
TABLE 2-9 Applications of Indirect Antiglobulin Test in the Immunohematology Laboratory
TABLE 2-8 Clinical Examples Causing a Positive Direct Antiglobulin Test
Antibody Screening
• Methodology (Tube, Gel, Solid Phase)
Fig. 7-1 Screening cell antigram.

5/13/2015
21
Antibody Screening
Fig. 7-2 Screen interpretations. Tentative interpretations that can be made after testing of the antibody screen and direct antiglobulin test. IS, Immediate-spin; 37° C, 37° C incubation; AHG, antihuman globulin; CC, check cells; ✓, check cells agglutinate; NT, not tested; Poly, polyspecific antiglobulin reagent; C3, anticomplement reagent.
Antibody Identification
TABLE 7‐3 Guidelines for Interpretation of a Panel

5/13/2015
22
Antibody Identification
Antibody Identification

5/13/2015
23
Antibody Identification
Antibody identification

5/13/2015
24
Antibody Identification
Antibody Identification
Fig. 7-4 Mini-cold panel.

5/13/2015
25
Antibody Identification
Antibody Identification
*Never assume that the antibody in the serum is the same as the antibody coating the red cells.
Fig. 7-6 Principle of the elution technique.

5/13/2015
26
Antibody Identification – Special Procedures/Reagents
Neutralization – good for Lewis (Lewis Substance); P1 antibodies (hydatid cyst fluid), anti‐Sda (fresh urine) Ch and Rg (plasma).
Adsorptions:
Autologous – can only be performed if patient has not been recently transfused or unless cell separation procedure is performed. If DAT is positive, antibody must be removed before procedure can be performed.
Allogeneic – use R1R1, R2R2 and rr cells. Must be careful during interpretation as clinically significant antibodies can be excluded.
Commercially available W.A.R.M and RESt kits are available.
RBC Phenotyping – DAT must be negative. If DAT is positive and patient has not been recently transfused, Chlorquin Diphosphate can be used to remove IgG from patient’s red cells. Recent transfusion requires cell separation procedure to be performed prior to phenotyping.
Antibody Identification – Special Procedures/Reagents
• 2‐ME (2‐Mercaptoethanol) and DTT (Dithiothreitol) – cleaves disulfide bonds of IgM antibody molecules. Helps distinguish between IgM and IgG.
• AET (2‐aminoethylisothiouronium bromide) – creates red cells that lack Kell antigens
• ZZAP (DTT + papain) –used to remove immunoglobulins and complement from the surface of red blood cells, commonly when evaluating a potential autoantibody. ZZAP also deactivates a multitude of red cell antigens on the red cell surface.

5/13/2015
27
Antibody Identification
Fig. 7-5 Prewarm technique.
Antibody Identification
Fig. 7‐3 Strategies for the weak antibody or one that does not fit a pattern.

5/13/2015
28
Antibody Identification
Fig. 4-10 Saline replacement technique. Rouleaux causing false-positive reactions can be distinguished from agglutination through the use of this simple technique.
Part III
Crossmatch and Special Tests

5/13/2015
29
Compatibility Testing
Fig. 8-1 Process of compatibility testing. The process begins at the recipient and ends with a safe transfusion into the recipient.
Fig. 8-5 Recipient sample labeling.
Compatibility Testing
Fig. 8-4 Comparison of immediate-spin, computer, and antiglobulin crossmatch requirements. XM, Crossmatch.

5/13/2015
30
Compatibility Testing
TABLE 8-3 Unexpected Incompatibilities in Immediate-Spin Crossmatch
Compatibility Testing
Antibodies can be missed in compatibility testing if:
• The corresponding antigen is absent from screening cells
• The antibody is so weak that it detects only homozygous expressions of the antigen (dosage effect)
• The antibody is detectable only by a method not routinely employed (e.g., in the presence of a particular enhancement medium)
• Antibody history is unknown

5/13/2015
31
Compatibility Testing
TABLE 8-5 ABO Compatibility for Whole Blood, Red Blood Cells, and Plasma Transfusions
Compatibility Testing - Incorrect ABO Grouping
Resolution:
• Check all tube labeling against positive ID of donor and patient
• Repeat ABO/Rh of patient and donor
• Request new sample if necessary
IS 37oC AHG CC
Patient serum
+
Donor cells
4+
Crossmatch:

5/13/2015
32
Compatibility Testing - Rh Incompatibility
• will not be detected unless prior sensitization has occurred
IS 37oC AHG CC
Patient serum
+
Donor cells
0 0 0 2+
Crossmatch:
Compatibility Testing - Alloantibodies in patient serum reacting with Donor RBC
• Check reaction(s) of screening cells
• Perform antibody panel
• Phenotype patient* and donor units
*if not transfused within last 3 months
IS 37oC AHG CC
I 0 0 2+ NT
II 0 0 0 2+
III 0 0 0 2+
AC 0 0 0 2+
Dr1 0 0 0 2+
Dr2 0 0 2+ NT

5/13/2015
33
Compatibility Testing - Autoantibodies in patient serum reacting with Donor RBC
• Check reaction(s) of screening cells• Check autocontrol• Perform antibody panel • Adsorb out autoantibody• Run same panel on adsorbed serum• If underlying alloantibodies,
phenotype donor units• Remove IgG from patient cells
before phenotyping (if not recently transfused)
IS 37oC AHG CC
I 0 0 2+ NT
II 0 0 2+ NT
III 0 0 2+ NT
AC 0 0 2+ NT
Dr1 0 0 2+ NT
Dr2 0 0 2+ NT
Compatibility Testing – Antibodies to low incidence antigens
• Panel studies usually not helpful
• Specific antiserum sometimes not available
• Easy to find compatible blood
• May have to rely on reference lab for ID
IS 37oC AHG CC
I 0 0 0 2+
II 0 0 0 2+
III 0 0 0 2+
AC 0 0 0 2+
Dr1 0 0 0 2+
Dr2 0 0 0 2+
Dr3 0 0 0 2+
Dr4 0 0 1+ 2+

5/13/2015
34
Compatibility Testing – Antibodies to high-incidence antigens
• Panel studies usually not able to resolve
• Specific antiserum sometimes not available
• Hard to find compatible blood
• May have to rely on reference lab for ID and to find compatible blood
IS 37oC AHG CC
I 0 0 2+
II 0 0 2+
III 0 0 2+
AC 0 0 0 2+
Dr1 0 0 2+
Dr2 0 0 2+
Dr3 0 0 2+
Dr4 0 0 2+
Serological Steps to Resolution of Incompatibility
• Verify integrity of specimen (patient identification, labeling)
• Check patient history (diagnosis, medications)
• Perform antibody ID
• If panel results are inconclusive (or cannot rule out all possibilities) must run selected cells, special techniques (neutralizations, absorption, elution, enzymes, etc.)
• Type antibody-producer for corresponding antigen (if not transfused within last 3 months)
• Screen for antigen negative (ABO/Rh) compatible units

5/13/2015
35
Part IV
Blood Donation, Transfusion Therapy
Transfusion Reactions, and Hemolytic Disease of Fetus and Newborn
Donor Selection
• Registration (positive identification)
• Educational Materials
• Screening (Health History Interview – see attachment)
• Physical Examination
• Informed consent
• Self‐exclusion

5/13/2015
36
Donor Collection
• 0.7% aqueous scrub solution of iodophor compound to remove surface dirt and bacteria and begin germicidal action
• 10% povidone‐iodine is applied beginning at the intended venipuncture site and continuing outward in a concentric spiral.
• The area is allowed to air dry for 30 seconds before being covered with sterile gauze
• For donors sensitive to these solutions, another method should be designated by the blood bank physician, such as chlorhexidine (ChloraPrep 2%) and 70% isopropyl alcohol
• ABBB standards require the use of collection containers that divert the first 10 to 20 mL of blood into a “diversion pouch” when platelet products are to be prepared from whole blood donation
• Primary bag used for blood collection, all attached satellite bags, sample tubes, and the donor registration form must be labeled with a unique identification number.
Physical Examination
TABLE 12-6 Physical Examination Requirements

5/13/2015
37
Donor Deferrals (see attachments)
• Temporary
• Permanent
• Indefinite
Donor Adverse Reactions
TABLE 12-7 Adverse Donor Reactions and Appropriate Treatment

5/13/2015
38
Special Donations
Autologous :
• Doctor’s prescription
• No age limit
• Lower hemoglobin (11.0 g/dL)
• Cannot donate within 72 hours of surgery
• Abbreviated testing per AABB standards
Directed/Desginated:
• A patient must give consent and have his/her physician submit a written request for the Red Cross to collect blood from the selected donors.
• No evidence that patients can select safer donors than a volunteer blood system provides.
• All donated blood products are tested with the same tests for HIV and other infectious diseases, which further enhances the safety of the blood supply.
• Social pressure associated with directed donations may compromise the reliability of the donor’s answers to health‐history questions.
Donor Processing
FDA Regulations:
• Blood is classified as a drug under the Federal Food, Drug and Cosmetic Act and is therefore subject to strict regulatory requirements during the manufacturing process as well as subsequent handling by transfusion facilities including labeling. It may only be dispensed with a prescription from a physician.
• Any equipment used in the manufacturing of blood products is also regulated under Medical Devices by the FDA (e.g., blood collection scales, apheresis machines, computer hardware/software).
• Any adverse reactions during donation or during subsequent transfusion must be reported to FDA (Biological Product Deviation Reporting)
• Fatalities attributable to blood component transfusion must be reported verbally to FDA within 24 hours and a written report filed within 7 days.
5/13/2015
39
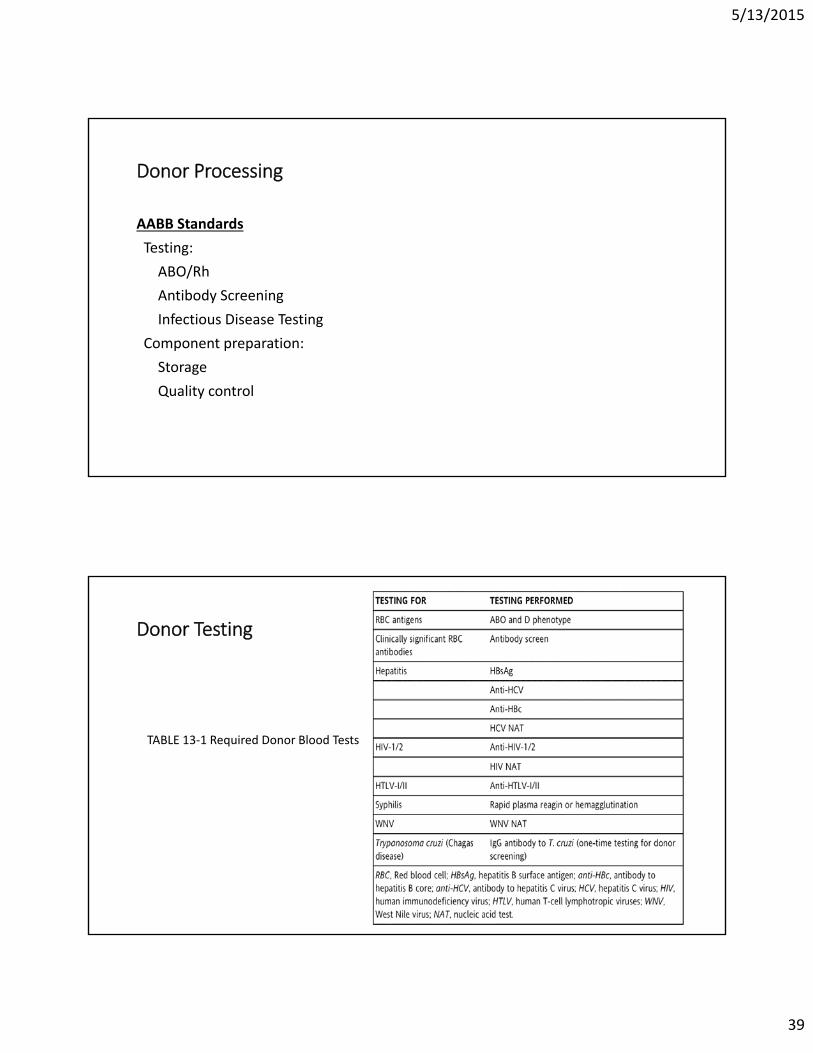
Donor Processing
AABB Standards
Testing:
ABO/Rh
Antibody Screening
Infectious Disease Testing
Component preparation:
Storage
Quality control
Donor Testing
TABLE 13‐1 Required Donor Blood Tests

5/13/2015
40
Storage of Blood Components
Fig. 14‐3 Storage lesion
Donor Labeling

5/13/2015
41
Transfusion Therapy ‐Summary
Transfusion Therapy – Expected Increments with Component Transfusions
In a 70‐kg adult (per unit):
• Whole Blood and RBCs: Hgb 1 g/dL, Hematocrit 3%
• Random Donor Platelets: 5‐10K per unit
• Apheresis Platelets: 30‐60K per unit• Fresh Frozen Plasma (FFP)* – coagulation factors 20% (3‐6 units)
• Cryoprecipitate (CRYO)*: fibrinogen 5‐10 mg/dL
*FFP and CRYO should only be given in the event that there are no suitable coagulation factor concentrates that are available.

5/13/2015
42
Transfusion Therapy ‐ Neonatal
<4 months of age do not have to repeat compatibility testing if initial screen and DAT are negative
Fresh blood < 7 days
CMV seronegative
Leukoreduced
Irradiated
Hgb S negative
Transfusion Therapy ‐ Emergency
• RBCs ‐ Group O (Rh positive or Rh negative selection may be sex dependent in some facilities)
• Plasma – Group AB
• Uncrossmatched – no sample or not enough time to complete testing; donor blood must be conspicuously labeled and segments pulled for later compatibility testing (when sample received and testing completed)
5/13/2015
43
Transfusion Therapy – Massive Transfusion
• Massive transfusion defined as the replacement of one or more blood volumes within a 24 hour period.
• Adult EBV 5000 mL (about 10 units whole blood)
• Will also develop deficiencies of clotting factors and platelets so these will need to be replaced as well
• Switching blood types may be necessary to avoid depleting blood supply of a particular type (e.g. A+ to O+). Care must be taken when switching back to original type. Why?
Transfusion Therapy – Sickle Cell Patients
• Sickle cell patients tend to make antibodies more readily than do other patients. This is due to the fact that Sickle Cell disease is a disease that occurs in the black population who share antigenic similarities. The majority of the donor population is white with antigenic dissimilarities. This fact alone contributes to the increased immunogenicity of donor blood antigens in Sickle Cell patients.
• Sickle cell patients should be given blood that is ABO/Rh compatible and negative for C, E, and K antigens. Blood must also be Hgb S negative.

5/13/2015
44
Transfusion Therapy ‐ Summary
Adverse Complications of Transfusion ‐ Instructions
Fig. 10‐5 Instructions to medical staff when a transfusion reaction is suspected.
5/13/2015
45
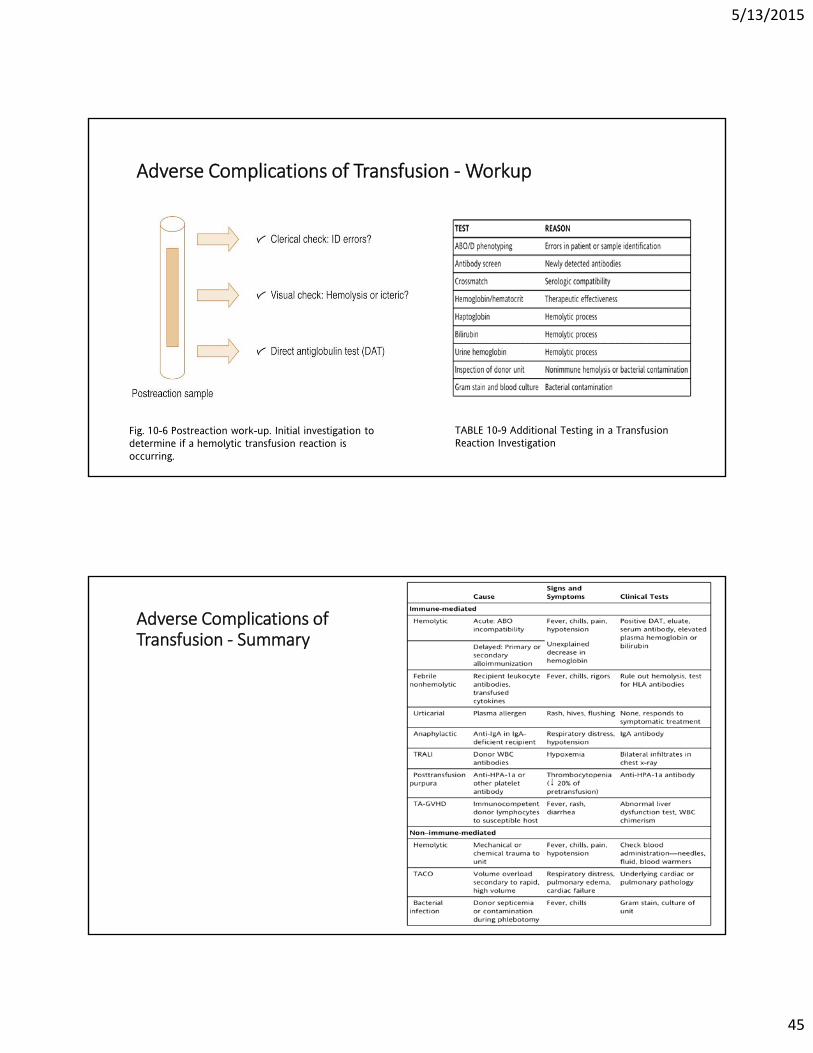
Adverse Complications of Transfusion ‐Workup
Fig. 10-6 Postreaction work-up. Initial investigation to determine if a hemolytic transfusion reaction is occurring.
TABLE 10-9 Additional Testing in a Transfusion Reaction Investigation
Adverse Complications of Transfusion ‐ Summary

5/13/2015
46
Hemolytic Disease of Fetus and Newborn (HDFN)
Fig. 11-1 Metabolism of bilirubin. A, Before delivery, fetal bilirubin produced by the breakdown of sensitized red cells in the fetal spleen is safely metabolized by the maternal liver. B, After delivery, the newborn's liver does not produce glucuronyl transferase and cannot convert bilirubin to an excretable form. As a result, it collects in tissues and causes brain damage.
HDFN
TABLE 11-2 Prenatal Testing: Tests to Identify Women at Risk of Hemolytic Disease of the Fetus and Newborn
Fig. 11-2 Twofold serial dilutions of the serum containing the antibody are prepared with saline as the diluent. Saline is first added to tubes 1:2→1:256. Serum is then added to tube 1 and 1:2. The serum is transferred from 1 to 1:2 and then to 1:4 continuing to the last tube, changing pipette tips to prevent carryover. The red cell selected for testing is usually homozygous and tested by the antiglobulin technique using anti-IgG. The titer is reported as the reciprocal of the highest dilution that gives a 1+ reaction.

5/13/2015
47
HDFN
TABLE 11-3 Testing at Delivery (Postpartum Testing)
HDFN
Fig. 11-5 Liley graph and Queenan et al modification. A, Liley graph for evaluating data from spectrophotometric analysis of amniotic fluid. The change in optical density at 450 (∆OD 450) and weeks of gestation are plotted to estimate the severity of HDFN. A reading of 0.206 at 35 weeks correlates with severe HDFN, which may necessitate immediate delivery. B, Modification by Queenan et al. of the Liley graph to include four zones beginning at 14 weeks of gestation.

5/13/2015
48
HDFN ‐ RhIGTABLE 11-4 Decisions for Rh Immune Globulin Administration
HDFN
Fig. 11-6 Rosette test for detection of fetomaternal hemorrhage. RhIG, Rh immune globulin; lpf, low power field.
Fig. 11-7 Acid elution test for determination of hemoglobin F. After staining, fetal red cells appear dark pink, and adult cells appear as pale ghost cells. Fetal hemoglobin resists acid elution and remains intact, whereas the adult cells lose the hemoglobin and do not take up the stain.

5/13/2015
49
HDFNFig. 11-8 Calculating the dosage of RhIG
The End.
REVIEW BOC STUDY GUIDE QUESTIONS
Good Luck on the Certification Exam!
References (tables and figures):
Blaney, Kathy, Paula Howard. Basic & Applied Concepts of Blood Banking and Transfusion Practices, 3rd Edition. Mosby, 2013.