private insurance plans - do they have a future in canada?
TRANSCRIPT

Private drug insurance plans:Do they have a future in Canada?
Louise BinderJune 16, 2016

Agenda 1. Background of drug payment systems in Canada
2. Role of public versus private drug insurance
3. Pricing for private plans
4. Recent cost constraint policies and their implications
5. Next steps and proposed solutions
6. Recommendations for involvement

3
In 2014, Canadians spent an estimated $28.8 billion on prescribed drugs
Total Health Expenditure, by Use of Funds, Canada, 2014f

4
Innovative medicines make up just over 6% of healthcare spending in Canada
Source: Canadian Health Policy Institute, Spending on Patented Drugs in Canada 1990-2014, February 23, 2016

Who Pays for Pharmaceuticals in Canada?Total 2013 Rx Meds Expenditure
$29.3 B*; 100%
Private Sector Share
$17.1 B; 58.4% of total
Public Sector Share
$12.2 B; 41.6% of total
Other Publicly Funded Drug Expenditure; 1.1 B; 3.8% of total; 9.0% of public share
Federal Drug Benefit Plan; 0.6 B; 2.0% of total; 4.9% of public share
Provincial Drug Benefit Plan; 10.5 B; 35.8% of total; 86.1% of
public share
Out-of-Pocket Contributions;
7.0 B; 23.9% of total;
40.9% of private share
Private Insurers; 10.1 B; 34.5% of total; 59.1% of private share
* Not including medicines dispensed in hospitals
Source: Prescribed Drug Spending in Canada 2012 Report, CIHI

Patented Medicine Prices Review Board
• Federal agency
• Determines if the price set by the manufacturer is “excessive”
• Compares the price to the median price set in 7 countries including the U.S.
• Recently proposed changes to this basket of countries
• These prices are “retail” price and are paid generally by private payers and people paying out of pocket

What are the factors considered in public drug funding?

• Patient Workshop: Fall 2015
Economic Evaluations in The Public System
Advisory expert panels review evidence + some non-evidentiary factors, and make recommendations: • CADTH’s CDR (CDEC), pCODR (pERC)• Quebec’s, INESSS
Payers (provinces, PP, hospitals) make decisions. • expert panel recommendations • other non-evidentiary factors• product listing agreements.

Common Drug Review (CDR) program for non-cancer drugs:• considers patient input, clinical, and economic evidence
pan-Canadian Oncology Review (pCODR) program for oncology drugs:• considers clinical, economic, patient input and ease of implementation
“equally” as its deliberative framework BOTH CDR and pCODR:• each decides the “value” of the drug relative to others available and relative
to opportunity costs of funding this drug versus other drugs• recommends a yes, a yes with conditions – usually a pricing reduction – or
no to provincial funding bodies in health ministries
INESSS in Quebec (Separate process specific to Quebec)*

Pan-Canadian Pharmaceutical Alliance
• Provincial/territorial/federal coalition • Negotiates behind close doors with the manufacturers to
find an acceptable price• Claims to have saved an estimated $490 million in savings
on 63 completed submissions as of March 31, 2015 • Problems:
– no one gets access to the drug while negotiations are ongoing unless the companies do so voluntarily
– there is no time limit for negotiations – provinces may still decide they cannot afford to pay for the
drug through the drug budget now or at all

What are the factors considered when designing private benefit plans?
https://www.telushealth.co/item/finding-right-balance-benefit-plan-costs-employee-health/

How “Private” Are Private Benefit Plans Really?
• Private benefit plans were developed to be part of a competitive compensation plan
• They attract and retain the level of employee an employer wants relative to competitors for staff
• They have been shifting over time to be more flexible, recognizing varying employee needs
• They rely on an internal committee to determine which drugs and biologics to cover, not CADTH
• Plans have been quite open until recently
What has been put on Watch and Wait to date?
• We understand that 6 drugs and biologics are on Watch and Wait
> 2 oncology drugs > 2 hypertension medications > 1 CF drug > 1 in rheumatoid arthritis medication
Confidential | Panel Discussion 1 – Immuno-Oncology Trends
Public versus Private Plans
*Source: 1. http://www.canadianhealthpolicy.com/news/news-release---study-compares-private-versus-public-drug-coverage-in-canada.html
• For the new drugs approved for sale by Health Canada in 2012 that were eventually covered under at least one private plan and at least one public plan, private drug plans took 143 days on average to approve coverage compared to 316 days for public drug plans


Greenshield Policy
• Will only pay for Subsequent entry Biologics even if originator biologic will cost the plan the same amount
Manulife and Desjardins Policies of Watch and Wait
• Opt out programs only for insured companies
• Those that opt out pay more to be insured
• Plan sponsors generally do not know the implications of this policy until a plan member is impacted
Watch and WaitA critical eye on emerging drugs – Payer stays on top of newly-approved medications and newly-approved uses by Health Canada. Drugs expected to impose a considerable financial cost on drug plans will be placed On Watch and subjected to further review before they can be considered for addition to your clients’ plans
A reliable, third-party review – Payer will determine the value of new drugs coming to market based in part on the publicly available information from the Canadian Agency for Drugs and Technologies in Health (CADTH). CADTH reviews drugs and makes reimbursement recommendations to Canada's federal, provincial and territorial public drug plans, with the exception of Quebec, to guide their drug funding decisions.
A rigorous process to help ensure new drugs can be offered efficiently and at the right value for the money. Informed by CADTH recommendations, payer will work with pharmaceutical manufacturers to seek the best possible drug prices and determine if an effective delivery program, such as an adherence plan or an exclusive distribution arrangement, can help provide additional value. .

What's New in Manulife's Plan Sponsor Contracts? Of interest to manufacturers, the new contract language covers: Manulife Policy March 2016 Drugs subject to prior authorization will be based on predefined
clinical criteria and a pharmacoeconomic evaluation. Manulife's new ability to put drugs on the Manulife DrugWatch ™
list while they undergo assessment and to "not list" drugs on Manulife drug plans if they are determined not to provide value relative to the health outcomes achieved.
All Extended Health Care Benefits are paid as if the covered person were eligible under the Provincial Plan. In the event that a Provincial Plan changes funding, the Manulife plan will not automatically assume coverage of the charges.
(Cont’d) What's New in Manulife's Plan Sponsor Contracts? • Integration with patient assistance programs to ensure plan
members have access to all the health and financial resources available to them. Specifically, Manulife reserves the right to reduce the amount of a covered expense by the amount of financial assistance the covered person is entitled to receive under the Patient Assistance Program
• Use of lower cost alternatives when there are two or more therapeutically equal alternatives (could include subsequent entry biologics when/if regulation comes into effect that allows them to be interchangeable) or restricting the maximum amount covered to the price of the Lower Cost Alternative
21
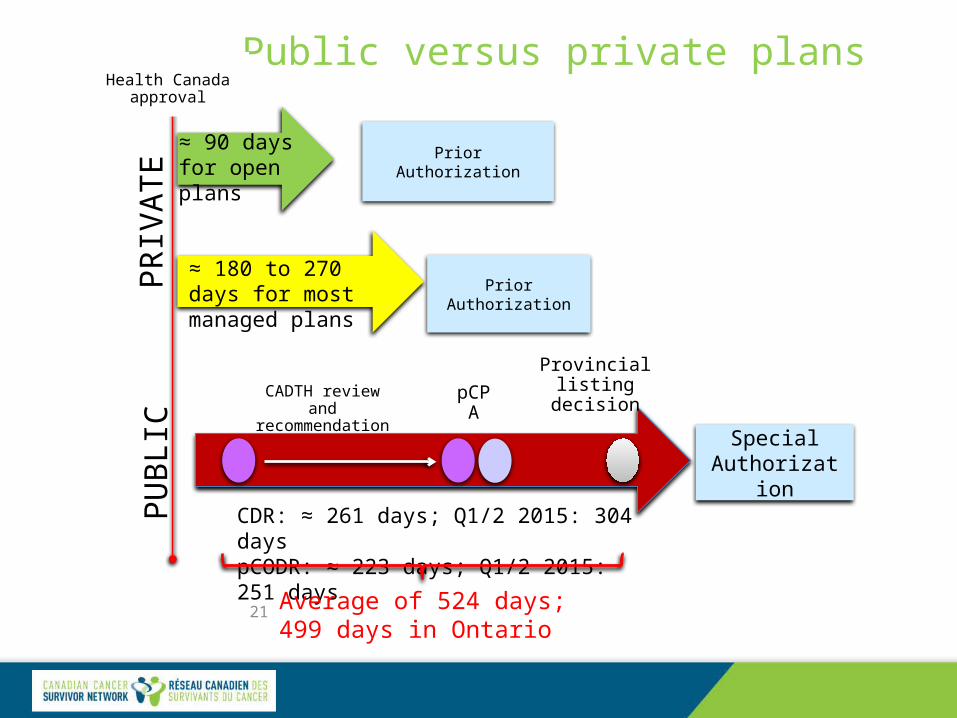
Public versus private plans Health Canada
approval
PRIV
ATE
PUBL
IC
Prior Authorization≈ 90 days for open plans
≈ 180 to 270 days for most managed plans Prior Authorization
Special Authorization
pCPA Provincial listing decision
CDR: ≈ 261 days; Q1/2 2015: 304 dayspCODR: ≈ 223 days; Q1/2 2015: 251 days
Average of 524 days; 499 days in Ontario
CADTH review and recommendation

Canadian Life and Health Insurance Association Position on Drug Pricing
• PMPRB rules should be changed• Private insurers should pay the same prices as public payers• Private insurers want to join the pCPA and let provinces and
territories negotiate for them• Private insurers have not determined how to deal with the
issue that private plans cover drugs that public plans do not and those drug prices will need to be negotiated
• Private payors cannot negotiate as a group due to anti-competition legislation

Pharmaceutical Industry Position
• Private plan prices subsidize the lower prices paid in the public system
• If private plan prices go down, public plan prices go up
• Savings from private plan negotiations are not used to reduce plan costs or to increase plan coverage

Government Stance
• Public payers only negotiate for public plans
• They are not in a position, nor do the have the mandate or resources, to negotiate for private payers

Plan Sponsors and Members
• Sponsors (employers) rely on the insurance companies, benefits consultants and Human Resources departments to manage plans effectively and ensure competitiveness
• Plan members needs are different depending on demographics including age, marital status, health status
• Small and medium size plan sponsors can afford much less generally than large employers
The Future• Private payers will become much like public payers,
limiting access, moving as much onto public plans as possible and negotiating pricing with public plans
• Public plans will have more pressure placed on them as private plans divest
• Public plans will be less sustainable, cover fewer treatments, place more restrictions on coverage
• Drugs may well take longer to get through pCPA • Individuals will get less overall coverage and will have
to pay more out of pocket

Why?• Manulife and Desjardins have already moved to “Watch and Wait”
reliance on CADTH recommendations for new high cost drugs• Manulife is now postponing drug coverage for any plan members
who have access to industry patient special access programs• Greenshield SEB policy• Private plans are becoming more “managed” with annual and/or
lifetime caps on coverage, mandatory generic substitution, preferred prescriber networks, cuts to coverage
• Canadian Health and Life Insurance Association (CHLIA) advocates for changes to PMPRB and private/public plan negotiations
• PMPRB 2015-2018 Strategic Plan recommends wholesale changes to its role

What can we do?
1. Educate insurance companies and offer to join in developing solutions that are more constructive and provide access to those most in need of expensive drugs
2. Educate benefits consultants and offer to assist in developing constructive solutions
3. Educate plan sponsors and offer to assist developing constructive plan designs and to educate employees

What can we do?
4 .Advise provincial and territorial politicians and bureaucrats about our views
5. Contact and advise CHLIA about our views
6. Respond to PMPRB consultation on pricing
7. Come to the Fall all patient education and awareness summit about drug pricing
Canadian Cancer Survivor Network Contact Info
Canadian Cancer Survivor Network1750 Courtwood Crescent, Suite 210Ottawa, ON K2C 2B5Telephone / Téléphone : 613-898-1871E-mail [email protected] or [email protected] site www.survivornet.caBlog: http://jackiemanthornescancerblog.blogspot.com/Twitter: @survivornetcaFacebook: www.facebook.com/CanadianSurvivorNet Pinterest: http://pinterest.com/survivornetwork/

Questions?