prognostic value of the cardiovascular profile score in fetuses with congestive heart failure
TRANSCRIPT
496 IMMUNOLOGY OF PREGNANCY: CERVICAL INTERLEUKIN-10/INTERLEUKIN-8RATIOS ACROSS GESTATION MYRIAM MONDESTIN1, DAVID SORRENTINO2,JOHN SMULIAN3, ANTHONY VINTZILEOS4, NAZEEH HANNA2, 1University ofMedicine and Denstitry of New Jersey, Jersey Shore University Hospital,Obstetrics Gynecology and Reproductive Sciences, Neptune, New Jersey,2University of Medicine and Dentistry Robert Wood Johnson Medical School,Pediatrics Division of Neonatology, New Brunswick, New Jersey, 3University ofMedicine and Dentistry Robert Wood Johnson Medical School, ObstetricsGynecology and Reproductive Sciences, New Brunswick, New Jersey,4University of Medicine and Dentistry of New Jersey Robert Wood JohnsonMedical School, Obstetrics Gynecology and Reproductive Sciences, NewBrunswick, New Jersey
OBJECTIVE: In the setting of infection mediated preterm labor, IL-8 appearsto play an important role in initiating acute inflammation and subsequentdelivery. In that setting IL-10 has been shown to prevent preterm delivery. Wehave previously shown that cervical IL-10 concentrations fall across gestation.Our goal was to establish cervical IL-8 concentrations and IL-10/IL-8 ratiosacross gestation.
STUDY DESIGN: This was a cohort study of 55 healthy pregnant woman (17first, 27 second and 17 third trimester patients) who presented for routineprenatal care. Specimens were collected from the cervical os using weck-celsponges. IL-8 and IL-10 concentrations (pg/mL) were measured by ELISA.Median (range) IL-8 concentrations were derived for each trimester. Data wasanalyzed using the Kruskall-Wallis test. The mean ratios of IL-10/IL-8 in eachtrimester were compared using ANOVA.
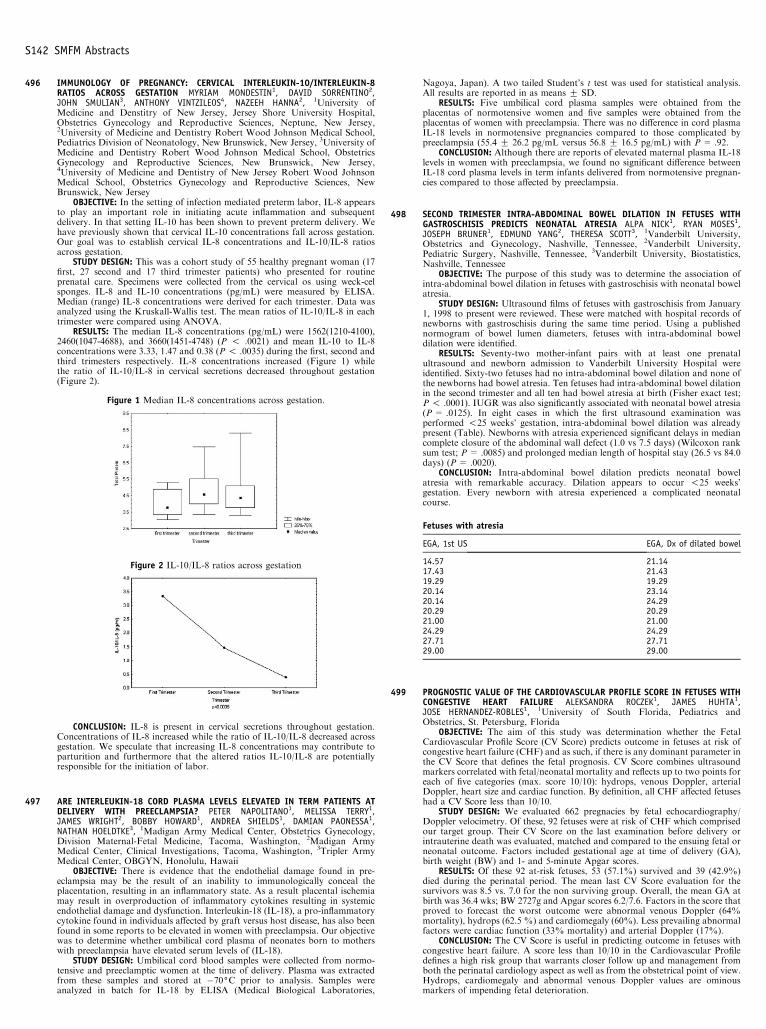
RESULTS: The median IL-8 concentrations (pg/mL) were 1562(1210-4100),2460(1047-4688), and 3660(1451-4748) (P ! .0021) and mean IL-10 to IL-8concentrations were 3.33, 1.47 and 0.38 (P ! .0035) during the first, second andthird trimesters respectively. IL-8 concentrations increased (Figure 1) whilethe ratio of IL-10/IL-8 in cervical secretions decreased throughout gestation(Figure 2).
Figure 1 Median IL-8 concentrations across gestation.
Figure 2 IL-10/IL-8 ratios across gestation
CONCLUSION: IL-8 is present in cervical secretions throughout gestation.Concentrations of IL-8 increased while the ratio of IL-10/IL-8 decreased acrossgestation. We speculate that increasing IL-8 concentrations may contribute toparturition and furthermore that the altered ratios IL-10/IL-8 are potentiallyresponsible for the initiation of labor.
497 ARE INTERLEUKIN-18 CORD PLASMA LEVELS ELEVATED IN TERM PATIENTS ATDELIVERY WITH PREECLAMPSIA? PETER NAPOLITANO1, MELISSA TERRY1,JAMES WRIGHT2, BOBBY HOWARD1, ANDREA SHIELDS1, DAMIAN PAONESSA1,NATHAN HOELDTKE3, 1Madigan Army Medical Center, Obstetrics Gynecology,Division Maternal-Fetal Medicine, Tacoma, Washington, 2Madigan ArmyMedical Center, Clinical Investigations, Tacoma, Washington, 3Tripler ArmyMedical Center, OBGYN, Honolulu, Hawaii
OBJECTIVE: There is evidence that the endothelial damage found in pre-eclampsia may be the result of an inability to immunologically conceal theplacentation, resulting in an inflammatory state. As a result placental ischemiamay result in overproduction of inflammatory cytokines resulting in systemicendothelial damage and dysfunction. Interleukin-18 (IL-18), a pro-inflammatorycytokine found in individuals affected by graft versus host disease, has also beenfound in some reports to be elevated in women with preeclampsia. Our objectivewas to determine whether umbilical cord plasma of neonates born to motherswith preeclampsia have elevated serum levels of (IL-18).
STUDY DESIGN: Umbilical cord blood samples were collected from normo-tensive and preeclamptic women at the time of delivery. Plasma was extractedfrom these samples and stored at �70(C prior to analysis. Samples wereanalyzed in batch for IL-18 by ELISA (Medical Biological Laboratories,
Nagoya, Japan). A two tailed Student’s t test was used for statistical analysis.All results are reported in as means G SD.
RESULTS: Five umbilical cord plasma samples were obtained from theplacentas of normotensive women and five samples were obtained from theplacentas of women with preeclampsia. There was no difference in cord plasmaIL-18 levels in normotensive pregnancies compared to those complicated bypreeclampsia (55.4 G 26.2 pg/mL versus 56.8 G 16.5 pg/mL) with P = .92.
CONCLUSION: Although there are reports of elevated maternal plasma IL-18levels in women with preeclampsia, we found no significant difference betweenIL-18 cord plasma levels in term infants delivered from normotensive pregnan-cies compared to those affected by preeclampsia.
498 SECOND TRIMESTER INTRA-ABDOMINAL BOWEL DILATION IN FETUSES WITHGASTROSCHISIS PREDICTS NEONATAL ATRESIA ALPA NICK1, RYAN MOSES1,JOSEPH BRUNER1, EDMUND YANG2, THERESA SCOTT3, 1Vanderbilt University,Obstetrics and Gynecology, Nashville, Tennessee, 2Vanderbilt University,Pediatric Surgery, Nashville, Tennessee, 3Vanderbilt University, Biostatistics,Nashville, Tennessee
OBJECTIVE: The purpose of this study was to determine the association ofintra-abdominal bowel dilation in fetuses with gastroschisis with neonatal bowelatresia.
STUDY DESIGN: Ultrasound films of fetuses with gastroschisis from January1, 1998 to present were reviewed. These were matched with hospital records ofnewborns with gastroschisis during the same time period. Using a publishednormogram of bowel lumen diameters, fetuses with intra-abdominal boweldilation were identified.
RESULTS: Seventy-two mother-infant pairs with at least one prenatalultrasound and newborn admission to Vanderbilt University Hospital wereidentified. Sixty-two fetuses had no intra-abdominal bowel dilation and none ofthe newborns had bowel atresia. Ten fetuses had intra-abdominal bowel dilationin the second trimester and all ten had bowel atresia at birth (Fisher exact test;P ! .0001). IUGR was also significantly associated with neonatal bowel atresia(P = .0125). In eight cases in which the first ultrasound examination wasperformed !25 weeks’ gestation, intra-abdominal bowel dilation was alreadypresent (Table). Newborns with atresia experienced significant delays in mediancomplete closure of the abdominal wall defect (1.0 vs 7.5 days) (Wilcoxon ranksum test; P = .0085) and prolonged median length of hospital stay (26.5 vs 84.0days) (P= .0020).
CONCLUSION: Intra-abdominal bowel dilation predicts neonatal bowelatresia with remarkable accuracy. Dilation appears to occur !25 weeks’gestation. Every newborn with atresia experienced a complicated neonatalcourse.
Fetuses with atresia
EGA, 1st US EGA, Dx of dilated bowel
14.57 21.1417.43 21.4319.29 19.2920.14 23.1420.14 24.2920.29 20.2921.00 21.0024.29 24.2927.71 27.7129.00 29.00
S142 SMFM Abstracts
499 PROGNOSTIC VALUE OF THE CARDIOVASCULAR PROFILE SCORE IN FETUSES WITHCONGESTIVE HEART FAILURE ALEKSANDRA ROCZEK1, JAMES HUHTA1,JOSE HERNANDEZ-ROBLES1, 1University of South Florida, Pediatrics andObstetrics, St. Petersburg, Florida
OBJECTIVE: The aim of this study was determination whether the FetalCardiovascular Profile Score (CV Score) predicts outcome in fetuses at risk ofcongestive heart failure (CHF) and as such, if there is any dominant parameter inthe CV Score that defines the fetal prognosis. CV Score combines ultrasoundmarkers correlated with fetal/neonatal mortality and reflects up to two points foreach of five categories (max. score 10/10): hydrops, venous Doppler, arterialDoppler, heart size and cardiac function. By definition, all CHF affected fetuseshad a CV Score less than 10/10.
STUDY DESIGN: We evaluated 662 pregnacies by fetal echocardiography/Doppler velocimetry. Of these, 92 fetuses were at risk of CHF which comprisedour target group. Their CV Score on the last examination before delivery orintrauterine death was evaluated, matched and compared to the ensuing fetal orneonatal outcome. Factors included gestational age at time of delivery (GA),birth weight (BW) and 1- and 5-minute Apgar scores.
RESULTS: Of these 92 at-risk fetuses, 53 (57.1%) survived and 39 (42.9%)died during the perinatal period. The mean last CV Score evaluation for thesurvivors was 8.5 vs. 7.0 for the non surviving group. Overall, the mean GA atbirth was 36.4 wks; BW 2727g and Apgar scores 6.2/7.6. Factors in the score thatproved to forecast the worst outcome were abnormal venous Doppler (64%mortality), hydrops (62.5 %) and cardiomegaly (60%). Less prevailing abnormalfactors were cardiac function (33% mortality) and arterial Doppler (17%).
CONCLUSION: The CV Score is useful in predicting outcome in fetuses withcongestive heart failure. A score less than 10/10 in the Cardiovascular Profiledefines a high risk group that warrants closer follow up and management fromboth the perinatal cardiology aspect as well as from the obstetrical point of view.Hydrops, cardiomegaly and abnormal venous Doppler values are ominousmarkers of impending fetal deterioration.