psychometric evaluation of the sports inventory for pain · a psychometric evaluation of the sports...
TRANSCRIPT

The Sport Psychologist, 1998,12,29-39 O 1998 Human Kinetics Publishers, Inc
A Psychometric Evaluation of the Sports Inventory for Pain
John B. Bartholomew Britton W. Brewer University of Texas Judy L. Van Raalte
at Austin Springfield College
Danvyn E. Linder Allen E. Cornelius Arizona State University University of Hartford
Shannon M. Bart University of Denver
This investigation was designed to assess the validity of the Sports Inventory for Pain (SIP; Meyers, Bourgeois, Stewart, & LeUnes, 1992). Study 1 used SIP responses to predict three objective measures of pain coping: pain thresh- old, pain tolerance, and the perception of a fixed, submaximal level of painful stimulation. Participants were 70 undergraduate volunteers (35 females, 35 males). Although two SIP subscales (Cognitive and Body Awareness) were related to at least one pain measure, another subscale (Coping) was negatively related to pain tolerance (opposite of predictions), and the composite HURT scores were not related to any of the pain measures. In Study 2,41 participants (31 females, 10 males) completed a wall sit (phantom chair) task and the SIP approximately 1 month after initially filling out the SIP. Test-retest reliabilities of the SIP were acceptable (average r = .75), but responses on the SIP did not predict performance on the painful physical endurance task. In Study 3, 54 participants (17 females, 37 males) completed the SIP approximately 1 month after anterior cruciate ligament reconstruction. SIP scores were not signifi- cantly correlated with measures of rehabilitation adherence and functional
John B. Bartholomew is in the Department of Kinesiology and Health Education at the University of Texas at Austin, 222 Bellmont Hall, Austin, TX 78712. Britton W. Brewer and Judy L. Van Raalte are with the Department of Psychology at Springfield College, 263 Alden Street, Springfield, MA 01109. Darwyn E. Linder is with the Psychology Depart- ment at Arizona State University, Box 871104, Tempe, AZ 85287. Allen E. Cornelius is with the Division of Student Affairs, University of Hartford, 200 Blurnefield Ave., GSU 313, West Hartford, CT 06117. Shannon M. Bart is with the Psychology Department at the University of Denver, 2155 S. Race St., University Park, Denver, CO 80208.

30 BarthoIomao, Brewer, Van Raalte et al.
outcome at approximately 6 months postsurgery. Taken together, these three studies provide marginal support for the validity of the SIP and raise questions about the utility of the SIP as a predictor of participants' ability to function while experiencing pain.
Participation in athletics often carries with it exposure to painful stimuli. The ability to endure pain is an obvious part of many sports (e.g., American foot- ball), and pain accompanies the physical training used to prepare for most sports. Endurance athletes have attributed much of their success to the ability to tolerate high levels of pain (Egan, 1987). It is known that individuals differ in their ability to deal with pain and that differences in pain tolerance have been associated with athletic experience. There is evidence that athletes in contact sports possess a greater ability to tolerate pain than do other athletes (Ryan & Foster, 1967; Ryan & Kovacic, 1966), and that athletes, in general, can tolerate pain better than nonathletes (Jaremko, Silbert, & Mann, 1981; Scott & Gijsbers, 1981; Ryan & Foster, 1967). Despite the role of pain in sport, there is little understanding of individual differ- ences in pain tolerance.
The Sports Inventory for Pain (SIP) was developed in an effort to identify and predict an athlete's ability to cope with pain (Meyers, Bourgeois, Stewart, & LeUnes, 1992). The SIP is a 25-item questionnaire consisting of 5 pain subscales: (a) coping, a measure of direct coping responses; (b) cognitive, a measure of cog- nitive strategies used in the face of pain; (c) avoidance, the tendency to avoid pain- producing responses; (d) catastrophizing, the tendency to be overwhelmed by pain; and (e) body awareness, a measure of response style. The 25 items are scored, from 1 to 5, on a 5-point Likert-type scale, with 1 = strongly disagree and 5 = strongly agree. For example, as a part of the coping subscale, participants are asked if "I see pain as a challenge, and it doesn't bother me," whereas on one of the catastrophizing subscale items they are asked if they "pray for the pain to stop." Scores from individual items are summed to obtain the subscale score. The first four subscales yield a composite score, HURT (Coping + Cognitive - Catastrophizing -Avoidance) that is intended to provide "an overall index of the ability to perform athletically while in pain" (Meyers et al., 1992, p. 254).
The original study (Meyers et al., 1992) validated the SIP by correlating responses on the SIP subscales to athletic and injury histories. HURT scores were positively correlated with the number of sports played and the number of injuries endured. On the basis of these data, it has been suggested that the SIP may be a useful clinical tool for sport psychologists, particularly when helping athletes cope with injury rehabilitation (Meyers et al., 1992). For example, results from the SIP could be used to tailor treatment of injured athletes to fit their response style to pain, or the SIP could be used to identify impending psychological dysfunction following an injury (Meyers et al., 1992). Although the initial psychometric data provide some evidence that the SIP is an acceptable measure, further validation is warranted, particularly for an instrument that is designed as a clinical tool. Before it is accepted for assessment purposes', the SIP should be shown to predict performance on a physical task under painful conditions, or, at a minimum, demonstrate the ability to predict responses to objective tests of pain coping, such as pain tolerance and pain perception at a given level of submaximal painful stimulation.

A Psychometric Evaluation 31
A series of three studies was carried out to explore the validity of the SIP. Studies 1 and 2 were designed to assess, respectively, the SIP'S ability to predict performance on objective tests of pain coping and on apainful physical task. Study 3 was designed to assess the ability of the SIP to predict responses to a painful postsurgical rehabilitation program. Across the three studies, it was expected that HURT, Body Awareness, Cognitive, and Coping scores would be positively asso- ciated with successful pain coping and that Avoidance and Catastrophizing scores would be negatively associated with successful pain coping.
Study 1
Method Participants. Participants were 70 undergraduate volunteers (35 males, 35
females) drawn from exercise science classes at a large southwestern university. A university Institutional Review Board-approved informed consent procedure was followed for all participants.
Apparatus. A gross pressure device was used for the pain stimulation (Brewer, Karoly, Linder, & Landers, 1990; Ryan & Kovacic, 1966). The device consisted of a rubber-coated steel football cleat attached to the inside surface of a foam-padded soccer shin guard. The device was fitted to the anterior medial sur- face of the tibia midway between the ankle and the knee of the dominant leg. The sleeve of a standard sphygmomanometer was used to secure the device to the leg. Pain was stimulated by inflating the sleeve, at 5 mmHG every 5 seconds, produc- ing pressure against the tibia. Pain stimulation was quantified as mmHG indicated on the sphygmomanometer. A pain tolerance test-retest reliability coefficient of .95 has been obtained with the gross pressure device (Ryan & Kovacic, 1966), which has been used to induce discernibly different levels of pain in previous studies (Brewer et al., 1990; Brewer, Van Raalte, & Linder, 1990).
Procedure. Upon entering the laboratory, participants completed an in- formed consent form. The gross pressure device was fitted to each participant's dominant leg, and pressure was applied. Pain threshold was operationally defined as the level of pressure at which participants first reported feeling pain. Pain toler- ance was the maximum level of pressure participants could endure. For pain per- ception, the cuff was removed and placed on the opposite leg. Pressure was applied until reaching the level of mmHG that corresponded to 70% of pain tolerance. Participants were then asked to rate the intensity of the pain from 1 to 100, where 1 was equivalent to no pain and 100 was equivalent to their maxi- mum pain tolerance.
Results and Discussion To test for main effect differences due to gender, a MANOVA was conducted on HURT scores and pain threshold, tolerance, and perception values. There was no multivariate effect for gender, Wilks lambda = .96, F(4, 65) = .73, p > .lo; nor were there any univariate differences in gender for HURT scores, F(1,68) = .60, p > .lo; pain threshold, F(l, 68) = .26, p > .lo; pain tolerance, F(1,68) = 2.17, p > .lo; or pain perception, F(l, 68) = 1.07, p > .lo. Thus, although males had greater mean values on all variables, those differences were not statistically significant.

32 Bartholomew, Brewer, Van Raalte et al.
Table 1 Correlations Between SIP Subscales and Pain Measures in Study 1
SIP subscale Threshold Tolerance Perception
Body Awareness Avoidance Catastrophizing Coping Cognitive HURT* *
*p i .05 (two-tailed); **HURT = Cognitive + Coping - Avoidance - Catastrophizing.
Pearson product-moment correlations were computed between the SIP subscales and each individual pain measure (see Table 1). HURT scores were not significantly related to any objective measure of pain coping. In accord with the predictions, the Cognitive subscale was positively correlated with pain tolerance and pain perception, and the Body Awareness subscale was positively correlated with pain threshold. Contrary to the hypotheses, neither the composite HURT scale nor the other subscales were positively correlated with any of the objective mea- sures of pain coping, and the Coping subscale was actually negatively correlated with pain tolerance. Cronbach's alpha coefficients were acceptable for the HURT scale and the Coping and Cognitive subscales (see Table 4), but they were unac- ceptable (< .50) for the Body Awareness, Avoidance, and Catastrophizing subscales. In sum, the SIP performed inconsistently in tests of predictive validity using ob- jective measures of pain coping. Results for two of the SIP subscales supported predictions (Cognitive and Body Awareness) and were related to at least one ob- jective measure of pain coping. In contrast, the composite HURT scale and the Avoidance and Catastrophizing subscales were unrelated to the measures of pain coping, and one SIP subscale (Coping) was significantly correlated with pain tolerance in the direction opposite to that hypothesized by Meyers et al. (1992).
These findings do not appear to be due to the method of pain induction. The gross pressure device has been validated as a method to induce a controlled amount of pain (Brewer, Karoly, et al., 1990). It has been successfully used to induce pain to demonstrate differences in the ability to tolerate pain (Ryan & Kovacic, 1966) and to study the effect of pain on the performance of a motor task (Brewer, Van Raalte, & Linder, 1990). Thus, the ability to withstand pain stimulation from the gross pressor device should be an accurate indicator of the general ability to with- stand pain. The ability to withstand pain, however, is not tantamount to the ability to function under pain. Although it may be expected that an athlete's ability to withstand pain would be related to the ability to function with pain, the gross pres- sor device may not be perceived as a true performance situation. Thus, the pain measures used in Study 1 may not be related to a participant's performance on an actual physical task. Therefore, Study 2 was designed to assess both the test-retest reliability of the SIP and the utility of the SIP in predicting performance on an

A Psychometric Evaluation 33
isometric quadriceps task that has been used in previous research as an analogue for athletic pain (Whitmarsh & Alderman, 1993).
Study 2
Method Participants. Participants were 41 undergraduate students (3 1 females, 10
males) enrolled in an abnormal psychology course at a small college. The gender composition was similar to that of the course as a whole. The vast majority of participants (n = 40, 98%) reported having played a sport at the varsity level in high school, and 15 participants (37%) reported having played a sport at the var- sity level in college.
Procedure. Participants completed the pretest, which consisted of a de- mographic questionnaire and the SIP, during a class session. Consistent with Insti- tutional Review Board policy, participants were considered to have given their consent to participate in the pretest by returning the questionnaire. Approximately a month later, participants reported (individually) to the laboratory for a study on "motor endurance performance." After completing an informed consent form, par- ticipants were told that the purpose of the study was to determine how long indi- viduals are able to endure physical discomfort.
Participants were asked to perform a wall sit (or phantom chair) endurance task in which they were requested to sit against a wall with their feet shoulder width apart and one thigh length from the wall, so that their thighs were parallel to the floor (Whitmarsh &Alderman, 1993). To ensure that the task was comparable across participants, a measurement of thigh length (in centimeters) was taken for each and a strip of tape was placed on the floor at a distance corre- sponding to each participant's thigh length away from the wall. Participants were instructed to hold this position as long as possible and to inform the experimenter when they could no longer hold the position. Performance on the wall sit task was assessed with a stopwatch. The total number of seconds that participants main- tained the wall sit position was recorded. Once participants had finished the wall sit task, they were given several minutes to recover. Participants then completed the SIP. This served as the posttest. Finally, participants were debriefed, thanked for their participation, and dismissed.
Results and Discussion As indicated in Table 2, responses on the SIP were stable over the 1-month pretest- posttest interval even though the context of administration (i.e., classroom vs. labo- ratory) differed across the two assessment situations. The average test-retest reli- ability coefficient, calculated as an intraclass correlation, was .75, with the Coping subscale demonstrating the best test-retest reliability, r = 35. As shown in Table 4, acceptable Cronbach's alpha coefficients were obtained only for the HURT scale and Coping subscale.
Pearson product-moment correlations were calculated between SIP subscale scores (at pretest and posttest) and wall sit performance scores. As shown in Table 2, only pretest Catastrophizing was significantly correlated with task performance. It is possible that this single significant relationship may be attributed to the mixed gender sample, as males had significantly higher wall sit performance scores, t (39) = 3.02, p < .01, and significantly lower Catastrophizing scores, t (38) = 2.71, p <

34 Bartholomeu, Brewer, Van Raalte et al.
Table 2 Test-Retest Reliability Coefficients for SIP Subscales and Correlations Between SIP Subscales and Wall Sit Performance in Study 2
SIP subscale Test-retest Pretest Posttest
Body Awareness Avoidance Catastrophizing Cognitive Coping HURT* *
* p < .05 (two-tailed); **HURT = Cognitive + Coping - Avoidance - Catastrophizing.
.05, than female participants. In support of this argument, after controlling for gender, the partial correlation between pretest Catastrophizing and task performance was not statistically significant, r = -.26, p > .lo. No other SIP subscales were significantly correlated with task performance.
Thus, in Study 1 the SIP failed, for the most part, to predict the ability to withstand pain, and in Study 2 the SIP failed to predict performance on a painful task. If these data accurately reflect how an individual would deal with pain, they pose a serious challenge to the validity of the SIP. It has been suggested that par- ticipants deal with pain in a fundamentally different manner in the laboratory than they do when they are forced to endure pain in a true life situation (Pen & Fisher, 1994). A painful stimulus has been theorized to contain both an informational (or sensory) component and an emotional, or fear, component (Melzack & Torgerson, 1971; Leventhal & Everhart, 1979). It may be that being in a controlled laboratory environment reduces the emotional component of the painful stimulus. It is likely that participants realize that no harm will come to them in a laboratory setting, thus there is little to fear from pain stimulation. The SIP subscales may carry the most relevance for the emotional component, that is, in predicting the ability to cope with the fear that accompanies a painful stimulus. A minimal emotional com- ponent, therefore, may diminish the impact of a person's superior ability to deal with pain, thereby confounding a test of the SIP. As a result, Study 3 tested the SIP outside of a laboratory environment, using the SIP to predict the rehabilitation responses (i.e., adherence, outcome, pain) of patients who had recently experi- enced anterior cruciate ligament (ACL) reconstruction. Pain, in this instance, was naturally occurring and was expected to carry a large emotional component. In addition, rehabilitation from major surgery is a performance situation in which the participants would be expected to be fully vested. Thus, there should be little con- cern about the motivational state of the participants.
Study 3
Method Participants. Participants were 54 patients (17 females, 37 males) under-
going rehabilitation at a sports medicine clinic following ACL reconstruction. The

A Psychometric Evaluation 35
mean age of participants was 28.00 (SD = 8.33) years. In terms of sport involve- ment, 28 participants (52%) indicated that they were competitive athletes and 25 (46%) indicated that they were recreational athletes. One participant was self- identified as a nonathlete.
Measures. In addition to the SIP, several other measures were used in this study. A questionnaire was used to obtain demographic and injury-related infor- mation from participants. The questionnaire included items requesting informa- tion on participants' age, gender, date of ACL injury, and level of sport involvement.
Adherence to rehabilitation was measured two ways. First, a ratio of reha- bilitation sessions attended to rehabilitation sessions scheduled was calculated for each participant. Attendance ratios have been used to measure adherence in previ- ous investigations (e.g., Laubach, Brewer, Van Raalte, & Petitpas, 1996; Daly, Brewer, Van Raalte, Petitpas, & Sklar, 1995; Byerly, Worrell, Gahimer, & Domholdt, 1994). Second, at each rehabilitation appointment attended by participants, the physical therapist or athletic trainer responsible for the rehabilitation of each par- ticipant on that day completed the Sport Injury Rehabilitation Adherence Scale (SIRAS). On the three-item SIRAS, practitioners rate participants' intensity of completion of rehabilitation exercises, frequency of following practitioner instruc- tions and advice, and receptivity to changes in the rehabilitation program during that day's appointment on 5-point Likert-type scales. Scale anchors for the three items are "minimum effort"/"maximum effort," "never7'/"always," and "very un- receptive"/"very receptive," respectively. Alpha reliability coefficients of .81 and .82 (Brewer, Van Raalte, Petitpas, Sklar, & Ditmar, 1995; Daly et al., 1995) have been obtained for the SIRAS. A mean SIRAS score was calculated for participants across all rehabilitation sessions attended.
Functional outcome for ACL reconstruction was assessed with the one-leg hop for distance (Daniel, Stone, Riehl, & Moore, 1984), in which participants hopped for distance on one leg, taking off and landing with the same leg. Both legs were tested three times. A mean hop index score was calculated by dividing the mean distance hopped on the involved leg across the three trials by that on the uninvolved leg (Kramer, Nusca, Fowler, & Webster-Bogaert, 1992). Support for the test-retest reliability of the hop index (intraclass correlation coefficient = .8 1) has been obtained (Kramer et al., 1992). This test has been used previously to evaluate the rehabilitation of ACLinjuries (Tegner, Lysholm, Lysholm, & Gillquist, 1986).
Pain was measured with a single item from a Noyes Questionnaire (Noyes & McGinniss, 1985) as modified by Shelbourne, Whitaker, McCarroll, Rettig, and Hirschman (1990). The item is a 6-point Likert-type scale with endpoints of "I experience no pain in my knee. I feel my knee is normal" and "I have pain in my knee at all times even during walking, standing, and at night. The pain is not re- lieved with rest." No psychometric data are available for this scale, although it has been used in ACL outcome research (Noyes & McGinniss, 1985; Shelbourne et al., 1990).
Procedure. Participants completed an informed consent document and the questionnaire with demographic and injury-related items prior to reconstructive surgery as part of a larger study of psychological aspects of ACL rehabilitation. Following reconstructive surgery, measures of adherence to rehabilitation were taken at each scheduled physical therapy appointment.
Approximately 1 month after reconstructive surgery, participants were asked to complete the SIP during a regularly scheduled rehabilitation session. Adherence

36 Bartholomew, Brewer, Van Raalte et al.
measures were taken throughout the rehabilitation period, although only data ob- tained after the 1-month assessment were used in this study to ensure the prospec- tive nature of the investigation. At approximately 6 months postsurgery, the pain item and the one-leg hop for distance were administered to participants.
Results and Discussion Because the distribution for the SIRAS was negatively skewed, a reflection and an inverse transformation were performed on SIRAS data to produce a more normal distribution. Separate one-way MANOVAs were conducted to determine whether there were differences on the predictor variables (i.e., SIP subscales) as a function of gender and level of sport involvement. No significant multivariate effects were found. A comparable pair of one-way MANOVAs performed on the criterion vari- ables (i.e., attendance, SIRAS, pain, one-leg hop for distance) yielded a similar pattern of nonsignificant multivariate effects. Consequently, the data were col- lapsed across genders and levels of sport involvement for subsequent analyses.
Pearson product-moment correlations were computed between the SIP subscales and the rehabilitation response measures. As shown in Table 3, no statis- tically significant (p < .05) correlations were obtained. One factor that may have contributed to the SIP'S inability to predict rehabilitation behaviors and outcomes is the low internal consistency of several subscales. As can be seen in Table 4, although the Cronbach's alpha coefficients were acceptable or marginally accept- able for the HURT composite and the Coping and Catastrophizing subscales, the internal consistency coefficients for the Cognitive, Avoidance, and Body Aware- ness subscales were clearly inadequate. This lack of internal consistency mirrors that found in Study 1 and Study 2, and it may have attenuated associations be- tween SIP scores and rehabilitation responses.
General Discussion When taken together, the three studies furnish little support for the validity of the SIP. The subscales were only weakly associated with the behaviors that they are intended to predict (i.e., dealing with pain). These data are particularly challenging
Table 3 Correlations Between SIP Subscales and Rehabilitation Response Measures in Study 3
SIP subscale Attendance SIRAS Pain HOP
Body Awareness Avoidance Catastrophizing Coping Cognitive HURT**
*p <.05 (two-tailed); **HURT = Cognitive + Coping - Avoidance - Catastrophizing.
A Psychometric Evaluation 37
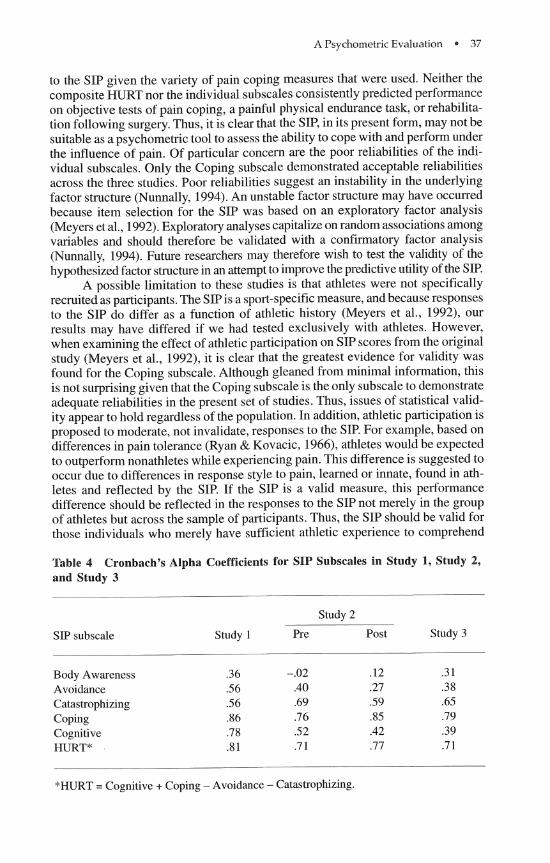
to the SIP given the variety of pain coping measures that were used. Neither the composite HURT nor the individual subscales consistently predicted performance on objective tests of pain coping, a painful physical endurance task, or rehabilita- tion following surgery. Thus, it is clear that the SIP, in its present form, may not be suitable as a psychometric tool to assess the ability to cope with and perform under the influence of pain. Of particular concern are the poor reliabilities of the indi- vidual subscales. Only the Coping subscale demonstrated acceptable reliabilities across the three studies. Poor reliabilities suggest an instability in the underlying factor structure (Nunnally, 1994). An unstable factor structure may have occurred because item selection for the SIP was based on an exploratory factor analysis (Meyers et al., 1992). Exploratory analyses capitalize on random associations among variables and should therefore be validated with a confirmatory factor analysis (Nunnally, 1994). Future researchers may therefore wish to test the validity of the hypothesized factor structure in an attempt to improve the predictive utility of the SIP.
A possible limitation to these studies is that athletes were not specifically recruited as participants. The SIP is a sport-specific measure, and because responses to the SIP do differ as a function of athletic history (Meyers et al., 1992), our results may have differed if we had tested exclusively with athletes. However, when examining the effect of athletic participation on SIP scores from the original study (Meyers et al., 1992), it is clear that the greatest evidence for validity was found for the Coping subscale. Although gleaned from minimal information, this is not surprising given that the Coping subscale is the only subscale to demonstrate adequate reliabilities in the present set of studies. Thus, issues of statistical valid- ity appear to hold regardless of the population. In addition, athletic participation is proposed to moderate, not invalidate, responses to the SIP. For example, based on differences in pain tolerance (Ryan & Kovacic, 1966), athletes would be expected to outperform nonathletes while experiencing pain. This difference is suggested to occur due to differences in response style to pain, learned or innate, found in ath- letes and reflected by the SIP. If the SIP is a valid measure, this performance difference should be reflected in the responses to the SIP not merely in the group of athletes but across the sample of participants. Thus, the SIP should be valid for those individuals who merely have sufficient athletic experience to comprehend
Table 4 Cronbach's Alpha Coefficients for SIP Subscales in Study 1, Study 2, and Study 3
Study 2
SIP subscale Study 1 Pre Post Study 3
Body Awareness Avoidance Catastrophizing Coping Cognitive HURT*
"HURT = Cognitive + Coping - Avoidance - Catastrophizing.

38 Bartholornew, Brmer, Van Raalte et al.
the items. Because the majority of participants in the present studies reported at least some athletic experience, this population should provide a fair test of the SIP.
Despite the limitations of the SIP, it remains clear that athletes differ in their ability to tolerate pain (Ryan & Kovacic, 1966). Therefore, the development of a sport-specific measure of pain coping is a worthy endeavor. Further research, how- ever, must first determine the factors that underlie the differences among athletes in pain tolerance. Are pain coping abilities learned, such that participation in a contact sport fosters these abilities? If so, then one might expect athletes to differ in their choice of learned coping responses and cognitive strategies that are ap- plied under painful conditions. Or, is high pain tolerance instead inherent in some individuals who then self-select into contact sports? If so, then the assessment of learned strategies would be of little help. It appears that prior to the development of a useful scale for assessing the ability to cope with pain in sport, we must first better understand the manner in which athletes experience pain, both across sports and over time.
References Brewer, B .W., Karoly, P., Linder, D.E., & Landers, D.M. (1990). Validation of a procedure
to induce pain of varied intensities. Research Quarterly for Exercise and Sport, 61, 268-27 1.
Brewer, B.W., Van Raalte, J.L., & Linder, D.E. (1990). Effects of pain on motor perfor- mance. Journal of Sport & Exercise Psychology, 12, 353-365.
Brewer, B.W., Van Raalte, J.L., Petitpas, A.J., Sklar, J.H., & Ditmar, T.D. (1995). A brief measure of adherence during sport injury rehabilitation sessions [Abstract]. Journal of Applied Sport Psychology, 7, S44.
Byerly, P.N., Worrell, T., Gahimer, J., & Domholdt, E. (1994). Rehabilitation compliance in an athletic training environment. Journal of Athletic Training, 29, 352-355.
Daly, J.M., Brewer, B.W., Van Raalte, J.L., Petitpas, A.J., & Sklar, J.H. (1995). Cognitive appraisal, emotional adjustment, and adherence to rehabilitation following knee sur- gery. Journal of Sport Rehabilitation, 4, 23-30.
Daniel, D.M., Stone, M.L., Riehl, B., & Moore, M.R. (1984). Ameasurement of lower limb function. The one leg hop for distance. American Journal of Knee Surgery, 4, 212- 214.
Egan, S. (1987). Acute pain tolerance among athletes. Canadian Journal of Sport Sciences, 12, 175-178.
Jaremko, M.E., Silbert, L., & Mann, T. (1981). The differential ability of athletes and nonathletes to cope with two types of pain: Aradical behavioral model. The Psycho- logical Record, 31, 265-275.
Kramer, J.E, Nusca, D., Fowler, P., & Webster-Bogaert, S. (1992). Test-retest reliability of the one-leg hop test following ACL reconstruction. Clinical Journal of Sport Medi- cine, 2, 240-243.
Laubach, W.J., Brewer, B. W., Van Raalte, J.L., & Petitpas, A. J. (1996). Attributions for recovery and adherence to sport injury rehabilitation. Australian Journal of Science and Medicine in Sport, 28, 30-34.
Leventhal, H., & Everhart, D. (1979). Emotion, pain, and physical illness. In C . E. Izard (Ed.), Emotions in personality andpsychopathology (pp. 263-299). New York: Plenum Press.
Melzack, R., & Torgerson, W.S. (1971). On the language of pain. Anethesiology, 34, 50-59.

A Psychometric Evaluation 39
Meyers, M.C., Bourgeois, A.E., Stewart, S. & LeUnes, A. (1992). Predicting pain response in athletes: Development and assessment of the Sports Inventory for Pain. Journal of Sport & Exercise Psychology, 14, 249-261.
Noyes, F.R., & McGinniss, G.H. (1985). Controversy about treatment of the knee with anterior cruciate laxity. Clinical Orthopedics and Related Research, 198, 61-76.
Nunnally, J.C. (1994). Psychometric theory (3rd ed.). New York: McGraw Hill. Pen, L.J., & Fisher, C.A. (1994). Athletes and pain tolerance. Sports Medicine, 18, 3 19-329. Ryan, E.D., & Kovacic, C.R. (1966). Pain tolerance and athletic participation. Perceptual
and Motor Skills, 22, 383-390. Ryan, E.D., & Foster, R. (1967). Athletic participation and perceptual augmentation and
reduction. Journal of Personality and Social Psychology, 6, 472-476. Scott, V. & Gijsbers, K. (1981). Pain perception in competitive swimmers. British Medical
Journal, 283,91-93. Shelbourne, K.D., Whitaker, H.J., McCarroll, J.R., Rettig, A.C., & Hirschrnan, L.D. (1990).
Anterior cruciate ligament injury: Evaluation of intraarticular reconstruction of acute tears without repair. l%o to seven year followup of 155 athletes. American Journal of Sports Medicine, 18, 484-489.
Tegner, Y., Lysholm, J., Lysholm, M., & Gillquist, J. (1986). A performance test to monitor rehabilitation and evaluate anterior cruciate ligament injuries. American Journal of Sports Medicine, 14, 156-159.
Whitmarsh, B.G., & Alderman, R.B. (1993). Role of psychological skills training in in- creasing athletic pain tolerance. The Sport Psychologist, 7, 388-399.
Note
This article was supported in part by grant number R15 AR42087-01 from the Na- tional Institute of Arthritis and Musculoskeletal and Skin Diseases. Its contents are solely the responsibility of the authors and do not represent the official views of the National Institute of Arthritis and Musculoskeletal and Skin Diseases. We thank Alan Bachrnan, John Brickner, Chris Buntrock, Wally Bzdell, Terry Ditmar, Ron Hokanson, Chris Izzo, Kelly Kane, Greg Kelleter, Dave LaLiberty, Jeff Laubach, Randy Masciana, Julie O'Brien, Trina Runge, Darrell Sikes, and John Sullivan for their assistance in data collection and gratefully acknowledge the cooperation of NovaCare Outpatient Rehabilitation and Drs. Albert Petitpas, Joseph SMar, Mark Pohlman, and Robert Krushell in conducting Study 3. Data from Study 2 were presented at the annual meeting of the American Psychological Association in New York in August 1996.
Manuscript submitted: February 27, 1997 Revision received: August 20, 1997