public notice regular meeting agenda monday, january …€¦ · city of alameda health care...
TRANSCRIPT

City of Alameda Health Care District – Agenda – January 10, 20111 of 3
PUBLIC NOTICE
CITY OF ALAMEDA HEALTH CARE DISTRICT
BOARD OF DIRECTORS
REGULAR MEETING AGENDA
Monday, January 10, 2011 – 7:30 p.m.
Location: Alameda Hospital (Dal Cielo Conference Room)
2070 Clinton Avenue, Alameda, CA 94501
Office of the Clerk: (510) 814-4001
Members of the public who wish to comment on agenda items will be given an opportunity before or during the consideration of eachagenda item. Those wishing to comment must complete a speaker card indicating the agenda item that they wish to address and presentto the District Clerk. This will ensure your opportunity to speak. Please make your comments clear and concise, limiting your remarks tono more than three (3) minutes.
I. Call to Order (6:00 p.m. – 2 East Board Room) Jordan Battani
II. Roll Call Kristen Thorson
VIII. Closed Session Agenda
A. Call to Order
B. Approval of Closed Session Minutes – November 8, 2010
C. Board Quality Committee Report (BQC) H & S Code Sec. 32155
D. Instructions to Bargaining Representatives Regarding Salaries,Fringe Benefits and Working Conditions
Gov’t Code Sec. 54957.6
E. Consultation with Legal Counsel Regarding Pending Litigation Gov’t Code Sec. 54956.9(a)
F. Discussion of Pooled Insurance Claims Gov’t Code Sec. 54956.95
G. Discussion of Report Involving Trade Secrets
1. Discussion of Hospital Trade Secrets applicable to development ofnew hospital services, programs and facilities. No action will be taken
2. Discussion of Hospital Trade Secrets applicable to development ofnew hospital services, programs and facilities. No action will be taken
3. Discussion of Hospital Trade Secrets applicable to development ofnew hospital services, programs and facilities. No action will be taken
4. Discussion of Hospital Trade Secrets applicable to development ofnew hospital services, programs and facilities. No action will be taken
H & S Code Sec. 32106
H. Adjourn into Open Session
IX. Reconvene to Public Session (Expected to start at 7:30 p.m. – Dal Cielo Conference Room)
A. Announcements from Closed Session Jordan Battani
1

City of Alameda Health Care DistrictAgenda – January 10, 2011
2 of 3
III. Consent Agenda
A. Approval of December 13, 2010 Regular Meeting Minutes ACTION ITEM [enclosure] (PAGES 4-19)
B. Approval of Administrative Policies and Procedures ACTION ITEM [enclosure] (PAGE 20 )
C. Approval of Human Resources Policy – Performance Evaluation ACTION ITEM [enclosure] (PAGES
21-24)
D. Approval of Board Quality Committee Structure and Purpose ACTION ITEM [enclosure] (PAGES 25-
26)
E. Approval Of Union Bank Signing Authorization / Resolution ACTION ITEM [enclosure] (PAGES 27-30)
IV. Regular Agenda
A. Action Items
1) Election of District Officers
ACTION ITEM [ENCLOSURE] (PAGES 31-34)
Kristen Thorson
2) Approval of 2011 District Board Meeting Dates
ACTION ITEM [ENCLOSURE] (PAGES 35-36)
Deborah E. Stebbins
3) 2011 Appointment to Board Committees
ACTION ITEM [ENCLOSURE] (PAGES 37-39)
Jordan Battani
4) Consideration of Primary Stroke Certification
ACTION ITEM
Jordan Battani
B. President’s Report Jordan Battani
1) Update on Compensation Survey Process
INFORMATIONAL [ENCLOSURE] (PAGES 40-48)
2) Use of Electronic Devices During Board Meetings
DISCUSSION
C. Chief Executive Officer’s Report Deborah E. Stebbins
1) Stroke Certification Update
INFORMATIONAL PRESENTATION
2) Monthly Statistics
3) IT Projects Update
4) 401(a) Pension Plan Contributions
INFORMATIONAL [ENCLOSURE] (PAGE 49)
2

City of Alameda Health Care DistrictAgenda – January 10, 2011
3 of 3
D. Facilities Report Kerry Easthope
1) SB 1953 Seismic Compliance Update
INFORMATIONAL PRESENTATION [ENCLOSURE] (PAGES 50-72)
2) Marina Village Space Planning
INFORMATIONAL [ENCLOSURE] (PAGES)
E. Medical Staff President Report
INFORMATIONAL
James Yeh, DO
F. Finance and Management Committee Report
1) Summary of November 2010 Financials
INFORMATIONAL PRESENTATION
Deborah E. Stebbins
X. General Public Comments
XI. Board Comments
XIII. Adjournment
3

D
RA
FT
M
inu
tes
of
the
Bo
ard
of
Dir
ecto
rs
Dec
embe
r 13,
201
0 D
irec
tors
Pre
sent
: M
anag
emen
t Pre
sent
: L
egal
Cou
nsel
Pre
sent
: M
edic
al S
taff
Pres
ent:
E
xcus
ed:
Jord
an B
atta
ni
Rob
ert D
euts
ch, M
D
J. M
icha
el M
cCor
mic
k
Ellio
tt G
orel
ick
Stew
art C
hen,
DC
Deb
orah
E. S
tebb
ins
Ker
ry J.
Eas
thop
e
Dav
id A
. Nea
polit
an
Thom
as D
risco
ll, E
sq.
Alk
a Sh
arm
a, M
D
Subm
itted
by:
Kris
ten
Thor
son
Top
ic
Dis
cuss
ion
Act
ion
/ Fol
low
-Up
I. Sw
earin
g-In
of E
lect
ed B
oard
M
embe
rs
Swea
ring-
In o
f Ele
cted
Boa
rd M
embe
rs b
y th
e H
onor
able
Bev
erly
John
son,
May
or
of th
e C
ity o
f Ala
med
a.
May
or Jo
hnso
n ex
tend
ed h
er w
arm
rega
rds t
o A
lam
eda
Hos
pita
l.
May
or Jo
hnso
n ad
min
ister
ed th
e O
ath
of O
ffice
to th
e ne
wly
ele
cted
Boa
rd
Mem
bers
, Ste
war
t Che
n, D
C, R
ober
t Deu
tsch
, MD
, and
Elli
ott G
orel
ick.
II.
Cal
l to
Ord
er
Jord
an B
atta
ni c
alle
d th
e O
pen
Sess
ion
of th
e B
oard
of D
irect
ors o
f the
City
of
Ala
med
a H
ealth
Car
e D
istric
t to
orde
r at 6
:10
p.m
.
III.
Rol
l Cal
l K
riste
n Th
orso
n ca
lled
roll,
not
ing
that
a q
uoru
m o
f Dire
ctor
s wer
e pr
esen
t.
IV.
Spec
ial R
ecog
nitio
n D
irect
or B
atta
ni g
ave
spec
ial r
ecog
nitio
n to
Rob
Bon
ta, L
eah
Will
iam
s, an
d A
lka
Shar
ma,
MD
for s
ervi
ng o
n th
e B
oard
of D
irect
ors.
Dire
ctor
Sha
rma
exte
nded
her
app
reci
atio
n fo
r the
opp
ortu
nity
to s
erve
as a
re
pres
enta
tive
of th
e M
edic
al S
taff
with
the
Boa
rd o
f Dire
ctor
s.
Rob
Bon
ta th
anke
d th
e B
oard
for t
he p
rivile
ge to
serv
e w
ith e
ach
one
of th
em. H
e re
ferr
ed to
Ala
med
a H
ospi
tal a
s an
amaz
ing
asse
t and
crit
ical
ly im
porta
nt to
the
com
mun
ity.
He
voic
ed th
at it
has
bee
n a
plea
sure
to w
ork
on a
Boa
rd th
at w
orks
to
geth
er so
eff
ectiv
ely
and
that
is th
e B
oard
Mem
bers
dut
y to
face
cha
lleng
es a
nd
help
Ala
med
a H
ospi
tal t
o be
com
e an
d re
mai
n th
e H
ospi
tal t
hat t
he c
omm
unity
vo
ted
to su
ppor
t. M
s. W
illia
ms
was
not
abl
e to
atte
nd th
e m
eetin
g.
4

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
Pu
blic
Com
men
t
Jim
Odd
ie, A
lam
eda
Citi
zen,
spok
e on
beh
alf o
f Cou
ncil
Mem
ber L
ena
Tam
. H
e re
laye
d he
r con
grat
ulat
ions
on
the
elec
tion
to a
ll Bo
ard
Mem
bers
and
to R
ober
t Bo
nta
bein
g el
ecte
d to
the
City
Cou
ncil.
Jim
Odd
ie a
lso
com
men
ted
that
he
help
ed R
ober
t Bon
ta in
his
cam
paig
n an
d w
as
hono
red
to sp
eak
to m
embe
rs o
f the
com
mun
ity. H
e st
ated
that
it w
ould
be
a se
rious
misu
nder
stan
ding
to th
ink
that
the
com
mun
ity w
ould
like
to h
ave
the
Hos
pita
l clo
se it
s doo
rs. H
e fe
els f
rom
per
sona
l exp
erie
nce
that
the
com
mun
ity
supp
orts
the
Hos
pita
l.
V.
Dist
rict B
oard
Orie
ntat
ion
A.
Ove
rvie
w o
f Hos
pita
l – D
ebor
ah S
tebb
ins g
ave
an o
verv
iew
of t
he H
ospi
tal
outli
ning
the
num
ber o
f lic
ense
d be
ds, k
ey s
ervi
ces p
rovi
ded
by th
e H
ospi
tal
and
new
ser
vice
s in
deve
lopm
ent s
uch
as a
wou
nd c
are
prog
ram
and
adv
ance
s in
dia
gnos
tic im
agin
g.
B. H
istor
y of
Hos
pita
l – M
s. St
ebbi
ns re
view
ed th
e hi
stor
y of
the
Hos
pita
l,
notin
g th
e 20
02 E
lect
ion
and
form
atio
n of
the
Dist
rict.
C.
Stru
ctur
e of
Dist
rict /
Ent
ities
– L
egal
Cou
nsel
Tho
mas
Dris
coll
revi
ewed
the
stru
ctur
e of
the
Dist
rict a
nd re
late
d en
titie
s list
ed b
elow
.
1. D
istric
t / H
ospi
tal
2. H
ealth
Car
e C
orpo
ratio
n
3.
CW
&S
Inve
stm
ent C
ompa
ny
4.
Jabe
r Esta
te
D.
Ral
ph M
. Bro
wn
Act
Mr.
Dris
coll
revi
ewed
the
gene
ral p
rovi
sion
s of
the
Ral
ph M
. Bro
wn
Act
st
atin
g th
at it
is th
e la
w th
at g
over
ns p
ublic
mee
tings
and
con
tain
s ex
cept
ions
to
pub
lic d
isclo
sure
such
as p
atie
nt h
ealth
pro
tect
ions
, qua
lity
impr
ovem
ent,
and
med
ical
staf
f cre
dent
ialin
g.
Mr.
Dris
coll
com
men
ted
that
a m
eetin
g is
defin
ed a
s whe
n th
ere
is a
maj
ority
of
Boa
rd o
f Dire
ctor
s dis
cuss
ing
Dist
rict b
usin
ess.
Mos
t mee
tings
, inc
ludi
ng
com
mitt
ee m
eetin
gs, a
re o
pen
to th
e pu
blic
. Th
e D
istric
t pos
ts a
gend
as a
nd
mee
ting
notic
es a
ccor
ding
to th
e Br
own
Act
requ
irem
ents
.
Mr.
Dris
coll
indi
cate
d th
at C
lose
d Se
ssio
n di
scus
sion
s con
tain
item
s suc
h as
5

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
pers
onne
l disc
iplin
ary
actio
ns, p
hysi
cian
cre
dent
ialin
g re
com
men
datio
ns,
med
ical
staf
f con
cern
s, in
stru
ctio
ns to
bar
gain
ing
repr
esen
tativ
es re
gard
ing
sala
ries,
frin
ge b
enef
its a
nd w
orki
ng c
ondi
tions
, cou
nsel
rega
rdin
g lit
igat
ion,
an
d H
ospi
tal t
rade
sec
rets
(i.e
. new
pro
gram
s or
serv
ices
in d
evel
opm
ent).
Mr.
Dris
coll
also
revi
ewed
the
Cal
iforn
ia P
ublic
Rec
ords
Act
, whi
ch a
llow
s pu
blic
acc
ess t
o al
l pap
er re
cord
s or e
lect
roni
c do
cum
ents
unl
ess i
t fol
low
s on
e of
the
exce
ptio
ns, s
uch
as a
Hos
pita
l tra
de se
cret
s or a
ttorn
ey-c
lient
pr
ivile
ged
info
rmat
ion.
E.
Con
fiden
tialit
y
Mr.
Dris
coll
reaf
firm
ed th
at th
e co
nfid
entia
lity
of th
e D
istric
t Clo
sed
Sess
ion
mat
eria
ls an
d di
scus
sion
s are
of a
serio
us n
atur
e an
d ca
n re
sult
in a
crim
inal
vi
olat
ion
if no
t fol
low
ed p
rope
rly. C
onfid
entia
lity
of c
lose
d se
ssio
n m
ater
ials
is to
rem
ain
with
eac
h B
oard
Mem
ber a
nd sh
ould
not
be
shar
ed w
ith a
nyon
e in
clud
ing
spou
se o
r fam
ily. D
istric
t Boa
rd M
embe
rs h
ave
the
priv
ilege
to v
iew
an
y co
nfid
entia
l Hos
pita
l doc
umen
ts. I
f pat
ient
reco
rds
are
requ
este
d by
a
Boar
d M
embe
r, th
ey m
ust f
ollo
w st
rict H
IPPA
gui
delin
es.
Dire
ctor
Che
n as
ked
wha
t the
pro
cedu
re w
as fo
r com
mun
icat
ing
with
Hos
pita
l st
aff a
nd if
it w
as a
ppro
pria
te fo
r Boa
rd M
embe
rs to
con
tact
them
dire
ctly
. M
r. D
risco
ll st
ated
that
the
Boa
rd fu
nctio
ns a
s a w
hole
Boa
rd a
nd in
divi
dual
Bo
ard
Mem
bers
do
not h
ave
the
auth
ority
to a
ct o
n be
half
of th
e D
istric
t. M
r. D
risco
ll an
d M
s. St
ebbi
ns re
com
men
ded
com
mun
icat
ing
thro
ugh
the
CEO
and
th
en b
e fo
rwar
ded
to d
epar
tmen
t man
gers
as a
ppro
pria
te o
r nee
ded.
Ms.
Batta
ni st
ated
that
in v
ery
few
inst
ance
s, ha
s the
boa
rd h
ad to
revi
ew
indi
vidu
al p
atie
nt re
cord
s. Pr
oces
ses h
ave
been
dev
elop
ed to
kee
p pa
tient
na
mes
con
fiden
tial,
by th
e us
e of
med
ical
reco
rd n
umbe
rs o
r oth
er id
entif
iers
w
hen
case
s are
repo
rted
to th
e Bo
ard.
Ms.
Steb
bins
reco
mm
ende
d th
at th
e fir
st
step
for a
ny D
istric
t Boa
rd M
embe
r req
uest
ing
reco
rds
is to
con
tact
the
CEO
an
d in
gen
eral
ther
e m
ust b
e a
real
ly g
ood
reas
on to
requ
est a
pat
ient
spec
ific
reco
rd.
Ms.
Steb
bins
wou
ld li
ke to
stay
as t
rans
pare
nt a
s pos
sible
to in
crea
se
com
mun
icat
ion
with
fello
w B
oard
Mem
bers
.
F.
Rob
erts
Rul
es o
f Ord
er
Mr.
Dris
coll
revi
ewed
Rob
ert’s
Rul
es o
f Ord
er in
dica
ting
that
whe
n th
e D
istric
t was
form
ed, t
he B
oard
ado
pted
to u
se it
as a
val
uabl
e gu
ide
to
cond
uctin
g m
eetin
gs.
The
Rob
ert’s
Rul
es c
onta
in in
form
atio
n re
gard
ing
who
ch
airs
the
mee
ting,
acc
epta
ble
beha
vior
, mak
ing
mot
ions
, etc
.
Dire
ctor
Gor
elic
k st
ated
that
as a
Boa
rd M
embe
r he
unde
rsta
nds t
hat h
e is
6

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
oblig
ated
not
to d
isclo
se a
ny in
form
atio
n th
at is
disc
usse
d in
Clo
sed
Sess
ion.
H
e as
ked
if he
is in
a C
lose
d Se
ssio
n m
eetin
g an
d fe
els
as if
the
item
is n
ot
appr
opria
te fo
r Clo
sed
Sess
ion,
how
he
shou
ld a
ddre
ss th
at.
Mr.
Dris
coll
repl
ied
that
the
Dist
rict B
oard
Pre
side
nt a
nd C
EO w
ith g
uida
nce
by L
egal
C
ouns
el d
eter
min
e w
heth
er th
e na
ture
of t
he su
bjec
t is t
o be
in C
lose
d or
Ope
n Se
ssio
n.
Dire
ctor
Deu
tsch
ask
ed h
ow m
any
Boa
rd M
embe
rs c
an sp
eak
on a
par
ticul
ar
issue
sim
ulta
neou
sly
outs
ide
of a
pub
lic m
eetin
g an
d w
hat t
he g
uide
lines
wer
e fo
r use
of e
mai
l.
Mr.
Dris
coll
repl
ied
that
Boa
rd M
embe
rs, i
n ge
nera
l, sh
ould
not
spea
k to
eac
h ot
her r
egar
ding
Dist
rict b
usin
ess i
n a
setti
ng w
here
the
maj
ority
of t
he
gove
rnin
g bo
dy m
ay b
e in
atte
ndan
ce a
s it i
s the
n co
nsid
ered
a p
ublic
mee
ting.
Bo
ard
Mem
bers
are
also
not
allo
wed
to h
ave
seria
l mee
tings
as o
utlin
ed in
the
Brow
n A
ct.
In te
rms
of e
mai
l, ne
ver u
se th
e “r
eply
all”
as t
his i
ndic
ates
that
de
liber
atio
n is
taki
ng p
lace
.
Mr.
Dris
coll
refe
renc
ed le
gisla
tion
AB
1234
Eth
ics T
rain
ing
that
requ
ires a
ll Bo
ard
Mem
bers
to p
artic
ipat
e in
Eth
ics T
rain
ing,
initi
ally
and
eve
ry tw
o ye
ars
ther
eafte
r.
G.
Boar
d M
embe
r “O
blig
atio
ns”
Ms.
Steb
bins
revi
ewed
gen
eral
obl
igat
ions
of a
Dist
rict B
oard
Mem
ber,
incl
udin
g at
tend
ance
in m
onth
ly B
oard
mee
tings
, atte
ndan
ce a
t Boa
rd
desi
gnat
ed c
omm
ittee
mee
tings
(Fin
ance
and
Man
agem
ent C
omm
ittee
, Boa
rd
Qua
lity
Com
mitt
ee a
nd C
omm
unity
Rel
atio
ns a
nd O
utre
ach
Com
mitt
ee),
parti
cipa
tion
on th
e A
dmin
istra
tive
Pens
ion
Plan
Ove
rsig
ht C
omm
ittee
, pa
rtici
patio
n at
com
mun
ity e
vent
s rep
rese
ntin
g th
e D
istric
t / H
ospi
tal a
nd
supp
ortin
g th
e A
lam
eda
Hos
pita
l Fou
ndat
ion
thro
ugh
thei
r tw
o m
ajor
eve
nts a
ye
ar.
H.
Fina
nce
Dav
id N
eapo
litan
, CFO
pre
sent
ed th
e op
erat
ing
budg
et. T
he p
lann
ing
cycl
e fo
r the
ope
ratin
g bu
dget
beg
ins i
n Fe
brua
ry o
f eac
h ye
ar a
nd e
nds i
n ea
rly
June
, prio
r to
the
begi
nnin
g of
the
fisca
l yea
r. Th
e op
erat
ing
budg
et is
de
velo
ped
taki
ng in
acc
ount
for c
hang
es in
hea
lth la
ws,
strat
egic
pla
nnin
g,
curr
ent a
nd p
ast v
olum
es, i
nflu
ence
s on
reve
nues
and
exp
ense
s, an
d ne
w
prog
ram
nee
ds.
The
oper
atin
g bu
dget
is b
roug
ht to
the
Fina
nce
&
Man
agem
ent C
omm
ittee
for a
ppro
val i
n M
ay b
efor
e it
is a
ppro
ved
by th
e D
istric
t Boa
rd in
June
. Dire
ctor
Gor
elic
k as
ked
if it
is le
gally
requ
ired
for t
he
annu
al o
pera
ting
budg
et to
be
bala
nced
and
how
it w
orks
with
cha
lleng
es. M
r.
7

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
Nea
polit
an re
plie
d th
at th
e m
inim
um g
oal o
f the
bud
get i
s to
reac
h a
zero
ba
lanc
e. T
he e
xecu
tive
man
agem
ent t
eam
, thr
ough
the
budg
et p
roce
ss,
iden
tifie
s act
ions
to k
eep
the
budg
et b
alan
ced
thro
ugho
ut th
e fis
cal y
ear.
Mr.
Nea
polit
an re
porte
d th
e ca
pita
l bud
get i
s dev
elop
ed b
y in
put f
rom
eac
h de
partm
ent.
Con
side
ratio
n of
cap
ital r
eque
sts a
re e
valu
ated
bas
ed o
n sa
fety
re
quire
men
ts, n
ew v
olum
e op
portu
nitie
s, an
d re
plac
emen
t of o
utda
ted
equi
pmen
t.
Mr.
Nea
polit
an a
dvis
ed th
at th
e au
dite
d fin
anci
al st
atem
ents
con
tain
aud
itor
repo
rts, v
olum
es, s
tatis
tics,
reve
nues
, and
exp
ense
s for
the
curr
ent f
iscal
yea
r.
The
Hos
pita
l use
s an
outs
ide
firm
, TC
A P
artn
ers t
o co
nduc
t the
ann
ual a
udit.
Th
e au
dite
d fin
anci
al st
atem
ents
are
bro
ught
to th
e Fi
nanc
e &
Man
agem
ent
Com
mitt
ee in
Oct
ober
for r
evie
w a
nd th
en to
the
Boa
rd o
f Dire
ctor
s for
ac
cept
ance
. M
r. N
eapo
litan
refe
renc
ed th
e m
onth
ly u
naud
ited
gina
ncia
ls w
ere
sim
ilar i
n st
ruct
ure
as th
e an
nual
stat
emen
ts.
Dire
ctor
Bat
tani
men
tione
d th
at th
e ca
pita
l bud
get i
s a re
lativ
ely
new
pro
cess
fo
r the
Dist
rict /
Hos
pita
l and
was
impl
emen
ted
due
to th
e co
nsid
erab
le d
egre
e of
dem
and,
def
erre
d m
aint
enan
ce, a
nd d
efer
red
inve
stm
ent i
n te
chno
logy
. It i
s us
ed a
s a p
lann
ing
and
dire
ctio
nal d
ocum
ent f
or th
e H
ospi
tal.
Dire
ctor
Che
n as
ked
if th
ere
is al
way
s a b
alan
ced
budg
et a
nd h
ow o
ften
the
goal
s of t
he
budg
et a
re m
et. M
r. N
eapo
litan
resp
onde
d th
at it
has
bee
n ba
lanc
ed fo
r the
last
th
ree
year
s. M
s. St
ebbi
ns re
plie
d th
at w
e ha
ve e
xcee
ded
the
budg
et fo
r the
last
th
ree
year
s. W
ith th
e lo
ss o
f the
Kai
ser v
olum
e in
this
last
fisca
l yea
r, w
e ha
d to
look
at n
ew c
ontra
ctua
l rel
atio
nshi
p pr
ogra
ms o
r new
ser
vice
s to
mak
e up
fo
r the
def
icit.
I. M
edic
al S
taff
Dr.
Shar
ma
revi
ewed
the
stru
ctur
e of
the
Med
ical
Sta
ff no
ting
that
ther
e w
ere
3 m
ain
depa
rtmen
ts/c
omm
ittee
s (M
edic
al E
xecu
tive
Com
mitt
ee, M
edic
al
Com
mitt
ee, S
urgi
cal C
omm
ittee
) tha
t mee
t mon
thly
to a
ddre
ss q
ualit
y of
car
e,
med
ical
staf
f mat
ters
and
pro
cess
es.
Ms.
Steb
bins
not
ed th
ere
are
appr
oxim
atel
y ei
ghty
act
ive
Med
ical
Sta
ff, in
w
hich
man
y ar
e do
uble
boa
rd c
ertif
ied.
Mr.
Dris
coll
stat
ed th
e M
edic
al S
taff
is an
inde
pend
ent s
elf-
gove
rnin
g bo
dy in
whi
ch o
pera
tes w
ithin
the
Dist
rict /
H
ospi
tal.
The
resp
onsib
ility
of t
he D
istric
t / H
ospi
tal i
s to
cre
dent
ial t
he
phys
icia
n al
low
ing
them
to tr
eat p
atie
nts w
ithin
our
org
aniz
atio
n.
Dire
ctor
Gor
elic
k ex
tend
ed h
is ap
prec
iatio
n to
Dr.
Shar
ma
for s
ervi
ng a
s the
M
edic
al S
taff
Pres
iden
t with
the
Boa
rd a
nd a
sked
who
her
repl
acem
ent w
ill
be a
nd w
hen
they
will
take
off
ice.
Dr.
Shar
ma
repl
ied
that
Dr.
Jim Y
eh w
ill b
e
8

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
her r
epla
cem
ent b
egin
ning
in Ja
nuar
y 20
11.
Dire
ctor
Gor
elic
k as
ked
Dr.
Sha
rma
the
prim
ary
reas
on fo
r phy
sici
ans
resi
gnin
g fr
om th
e M
edic
al S
taff.
Dire
ctor
Sha
rma
repl
ied
that
a p
hysic
ian
may
cho
ose
to re
tire,
mov
e to
ano
ther
inst
itutio
n, o
r cha
nge
thei
r typ
e of
pr
actic
e.
Dire
ctor
Che
n as
ked
if ph
ysic
ians
are
pai
d st
aff.
Ms.
Steb
bins
repl
ied
that
ac
cord
ing
to th
e St
ate
of C
alifo
rnia
, hos
pita
ls ca
nnot
em
ploy
phy
sici
ans
unle
ss th
ey fa
ll un
der c
erta
in e
xem
ptio
ns su
ch a
s Kai
ser P
erm
anen
te’s
HM
O.
M
r. D
risco
ll no
ted
that
Phy
sici
ans a
re n
ot p
aid
to b
e on
any
Med
ical
Sta
ff.
J. Ph
ysic
al P
lant
Ove
rvie
w
Ker
ry E
asth
ope,
Ass
ocia
te A
dmin
istra
tor s
tate
d th
at th
e H
ospi
tal c
onsi
sts o
f th
e fo
llow
ing
build
ings
: 192
5 Bu
ildin
g, S
teve
ns W
ing,
2nd
floo
r of S
teve
ns
Win
g ad
ded
in 1
950’
s, 3rd
floo
r of t
he S
teve
ns W
ing
was
add
ed in
the
1960
’s,
Wes
t Bui
ldin
g, S
outh
Bui
ldin
g bu
ilt in
198
3, R
adio
logy
& L
abor
ator
y, a
nd
the
Emer
genc
y R
oom
.
Mr.
East
hope
revi
ewed
the
prog
ress
of t
he d
evel
opm
ent o
f a c
ompl
ete
Elec
troni
c H
ealth
Rec
ord
(EH
R) a
nd th
e PA
CS
syst
em th
at w
ill b
e us
ed in
the
Dia
gnos
tic Im
agin
g D
epar
tmen
t. M
r. Ea
stho
pe a
lso d
iscu
ssed
new
pro
gram
de
velo
pmen
t and
off
site
build
ing
spac
e th
at w
ill p
oten
tially
be
used
to h
ouse
th
ese
new
pro
gram
s and
the
expa
nsio
n of
exi
stin
g H
ospi
tal p
rogr
ams.
Mr.
East
hope
stat
ed th
at th
e m
ajor
ity o
f em
ploy
ees a
re re
pres
ente
d by
uni
ons
with
in th
e H
ospi
tal:
SEIU
, Loc
al 2
9, L
ocal
6, a
nd L
ocal
39.
The
re
appr
oxim
atel
y 13
0 em
ploy
ees t
hat a
re n
ot re
pres
ente
d by
a u
nion
. Dire
ctor
C
hen
aske
d ho
w m
any
are
empl
oyed
by
Ala
med
a H
ospi
tal.
Mr.
Easth
ope
stat
ed th
at th
ere
appr
oxim
atel
y 60
0 fu
ll-tim
e an
d pa
rt-tim
e em
ploy
ees.
VI.
Con
sent
Age
nda
1 A
. A
ppro
val o
f Nov
embe
r 8, 2
010
Reg
ular
Mee
ting
Min
utes
. D
irect
or M
cCor
mic
k m
ade
a m
otio
n to
app
rove
the
Reg
ular
M
eetin
g M
inut
es o
f Nov
embe
r 8,
2010
as p
rese
nted
. D
irect
or
Deu
tsch
sec
onde
d th
e m
otio
n.
The
mot
ion
carr
ied.
Dire
ctor
s C
hen
and
Gor
elic
k ab
stai
ned
from
vot
ing
as th
ey w
ere
not
mem
bers
of B
oard
on
Nov
embe
r 8,
201
0.
9

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
VII
. C
onse
nt A
gend
a 2
B.
Acc
epta
nce
of O
ctob
er 2
010
Fina
ncia
l Sta
tem
ents
Dire
ctor
Gor
elic
k as
ked
abou
t the
del
ay o
f pay
men
t fro
m A
lam
eda
Alli
ance
, th
at M
r. N
eapo
litan
repo
rted
on a
t the
last
Boa
rd m
eetin
g an
d w
hen
the
paym
ent w
as re
ceiv
ed.
Mr.
Nea
polit
an st
ated
that
the
dela
y in
pay
men
t was
du
e to
the
lack
of a
Sta
te b
udge
t and
that
pay
men
t was
rece
ived
on
or a
roun
d N
ovem
ber 6
, 201
0.
Dire
ctor
Gor
elic
k ex
pres
sed
conc
ern
rega
rdin
g th
e lo
w le
vels
of c
ash
on h
and
($72
,000
) and
ask
ed if
ther
e is
a tri
age
plan
in p
lace
. Mr.
Nea
polit
an st
ated
th
at th
e H
ospi
tal h
as a
$1,
250,
000
line
of c
redi
t with
the
Bank
of A
lam
eda
but
it ha
s not
bee
n ne
eded
in th
e pa
st.
In a
dditi
on, t
he fi
rst i
nsta
llmen
t of t
he
parc
el ta
x is
due
on D
ecem
ber 1
4, 2
010.
Dire
ctor
Bat
tani
rem
inde
d th
e B
oard
th
at u
se o
f the
line
of c
redi
t req
uire
s Boa
rd a
ppro
val.
Dire
ctor
Deu
tsch
ask
ed
if w
e pa
y pa
rticu
lar a
ttent
ion
to v
endo
rs n
eede
d fo
r crit
ical
ser
vice
s w
hen
cash
is
low
. Ms.
Steb
bins
repl
ied
that
we
pay
vend
ors i
n a
timel
y m
anne
r with
a
spec
ial f
ocus
on
loca
l ven
dors
or s
mal
l bus
ines
s ven
dors
. D
irect
or C
hen
aske
d if
we
have
eve
r nee
ded
to u
se th
e lin
e of
cre
dit.
Dire
ctor
Bat
tani
an
swer
ed th
at is
has
not
bee
n ne
eded
with
the
curr
ent m
anag
emen
t tea
m (i
.e.
CFO
, CEO
). M
s. St
ebbi
ns c
omm
ente
d th
at th
e lin
e of
cre
dit i
s onl
y to
be
used
as
a la
st re
sort.
C.
App
rova
l of 4
03(b
) Tax
Def
erre
d A
nnui
ty R
etire
men
t Pla
n co
mpl
ianc
e A
men
dmen
ts (H
EAR
T an
d EE
SA)
D.
App
rova
l of R
evisi
ons t
o M
edic
al S
taff
By-L
aws,
Podi
atry
Priv
ilege
D
elin
eatio
n
Dire
ctor
Gor
elic
k pu
lled
Con
sent
A
gend
a Ite
m V
II.B
for f
urth
er
disc
ussi
on.
Dire
ctor
Gor
elic
k m
ade
a m
otio
n to
app
rove
the
rem
aind
er o
f the
C
onse
nt A
gend
a, It
ems V
II.C
and
V
II.D
, as p
rese
nted
. D
irect
or
Che
n se
cond
ed th
e m
otio
n. T
he
mot
ion
carr
ied
unan
imou
sly.
With
no
furth
er d
iscus
sion
, D
irect
or D
euts
ch m
ade
a m
otio
n to
acc
ept t
he O
ctob
er 2
010
Fina
ncia
l Sta
tem
ents
. D
irect
or
McC
orm
ick
seco
nded
the
mot
ion.
Th
e m
otio
n ca
rrie
d un
anim
ousl
y.
VII
I. R
egul
ar A
gend
a
A.
Act
ion
Item
s
1.
A
ppro
val o
f Dist
rict R
esol
utio
n N
o. 2
010-
4H –
201
1 St
atem
ent o
f D
irect
or D
utie
s and
Res
pons
ibili
ties
Dire
ctor
Bat
tani
stat
ed th
at th
e A
CH
D d
evel
oped
thes
e st
anda
rds t
o de
mon
stra
te to
the
publ
ic th
at th
e B
oard
und
erst
ands
thei
r re
spon
sibi
litie
s and
dut
ies a
nd st
anda
rds o
f beh
avio
r.
Dire
ctor
Gor
elic
k vo
iced
con
cern
rega
rdin
g th
e la
st p
arag
raph
on
page
46
that
stat
es, “
not l
egal
ly b
indi
ng”.
He
refe
rred
to th
e st
atem
ent a
s a
typi
cally
“go
od fe
elin
g” ty
pe o
f sta
tem
ent a
nd sh
ould
not
be
wha
t we
are
spen
ding
our
tim
e on
. He
men
tione
d th
at th
e re
solu
tion
was
not
ap
prop
riate
giv
en th
e di
vers
ity o
f opi
nion
s of
the
Boa
rd.
Dire
ctor
Deu
tsch
mad
e a
mot
ion
to
appr
ove
the
Dist
rict R
esol
utio
n N
o.
2010
-4H
Sta
tem
ent o
f Dire
ctor
D
utie
s and
Res
pons
ibili
ties.
Dire
ctor
McC
orm
ick
seco
nded
the
mot
ion.
Dire
ctor
Gor
elic
k op
pose
d th
e m
otio
n. T
he m
otio
n pa
ssed
4 to
1.
10

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
Dire
ctor
Che
n st
ated
that
we
are
mem
bers
of t
he A
CH
D. H
e re
ferr
ed to
th
e m
issio
n st
atem
ent a
s a w
ay to
enc
oura
ge th
e B
oard
to b
ehav
e in
such
a
way
. Mr.
Che
n as
ked
if th
ere
is a
pena
lty c
laus
e ex
pelli
ng o
ne fr
om th
e Bo
ard
if th
ey d
o no
t beh
ave
in a
cer
tain
man
ner.
Dire
ctor
Bat
tani
repl
ied
that
ther
e ar
e C
odes
of C
ondu
ct th
at in
clud
e sa
nctio
ns. D
irect
or
McC
orm
ick
aske
d if
it is
poss
ible
to e
xpel
a p
ublic
off
icia
l for
m
isco
nduc
t. M
r. D
risco
ll re
plie
d th
at it
is a
serio
us c
halle
nge
to re
mov
e a
publ
ic o
ffic
ial f
rom
off
ice.
Dire
ctor
McC
orm
ick
advi
sed
ther
e ar
e tw
o co
rrec
tions
on
page
47
in
refe
renc
e to
the
Res
olut
ion.
The
err
ors w
ill b
e co
rrec
ted.
2.
App
rova
l of L
ease
Ter
ms f
or 8
15 A
tlant
ic A
venu
e
Mr.
East
hope
pre
sent
ed th
e Le
ase
Term
s for
815
Atla
ntic
Ave
nue
for
appr
oval
by
the
Boa
rd o
f Dire
ctor
s. H
e sta
ted
that
ther
e is
a la
ck o
f m
edic
al o
ffic
e sp
ace
avai
labl
e w
ithin
Ala
med
a. W
e ha
ve e
ngag
ed a
co
mm
erci
al re
al e
stat
e br
oker
to n
egot
iate
the
term
s of t
he le
ase.
The
lo
catio
n fo
r the
Wou
nd C
are
Cen
ter h
as b
een
revi
ewed
for s
ever
al
mon
ths.
The
adv
anta
ges o
f the
loca
tion
are
that
the
Hos
pita
l will
hav
e a
pres
ence
on
the
wes
t sid
e of
the
isla
nd a
nd th
at th
e hi
gh v
acan
cy ra
te h
as
push
ed re
nt ra
tes d
own.
Mr.
East
hope
stat
ed th
at th
e pr
oper
ty a
t Mar
ina
Vill
age
is zo
ned
for
mix
ed-u
se.
The
term
s of t
he le
ase
incl
udes
a c
laus
e th
at if
we
cann
ot
secu
re fi
nanc
ing
for t
he p
roje
ct, w
e m
ay te
rmin
ate
the
cont
ract
with
no
pena
lty.
Mr.
East
hope
des
crib
ed th
at th
e le
ase
is a
ten
year
leas
e w
ith tw
o, fi
ve
year
term
s. Th
e co
st o
f the
loca
tion
is ap
prox
imat
ely
$0.7
0 pe
r squ
are
foot
com
pare
d to
the
$1.9
0 pe
r squ
are
foot
cos
t at t
he A
lam
eda
Tow
ne
Cen
ter l
ocat
ion.
Mr.
East
hope
disc
usse
d ex
pans
ion
right
s and
subl
et re
spon
sibili
ties.
If A
lam
eda
Hos
pita
l wou
ld li
ke to
exp
and
into
the
rest
of t
he b
uild
ing
with
in o
ne y
ear,
then
the
rent
rate
will
be
asse
ssed
acc
ordi
ng to
our
cu
rren
t con
tract
. If e
xpan
sion
is m
ade
afte
r eig
htee
n m
onth
s, th
en th
e re
nt
will
be
base
d on
cur
rent
mar
ket v
alue
. Sub
letti
ng to
any
affi
liate
of t
he
Hos
pita
l will
be
allo
wed
.
Mr.
East
hope
cla
rifie
d th
at o
nce
the
term
s of t
he L
ette
r of I
nten
t are
ap
prov
ed b
y th
e B
oard
, the
n th
e co
ntra
ct w
ill b
e de
velo
ped
and
subm
itted
to
the
Boa
rd o
f Dire
ctor
s for
fina
l app
rova
l.
Dire
ctor
Bat
tani
mad
e a
mot
ion
to
auth
oriz
e m
anag
emen
t to
mov
e fo
rwar
d on
the
deve
lopm
ent o
f a
non-
bind
ing
agre
emen
t and
use
the
cons
truct
ion
build
out
bud
get
prop
osed
to p
ursu
e fin
anci
ng
optio
ns D
irect
or D
euts
ch m
ade
a m
otio
n to
app
rove
as s
tate
d by
D
irect
or B
atta
ni. D
irect
or
McC
orm
ick
seco
nded
the
mot
ion.
Th
e m
otio
n ca
rrie
d un
anim
ousl
y.
11

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
Dire
ctor
McC
orm
ick
aske
d ab
out p
arki
ng a
vaila
ble.
Mr.
East
hope
repl
ied
that
ther
e ar
e 3.
4 sta
lls p
er 1
,000
squa
re fe
et.
Dire
ctor
McC
orm
ick
aske
d ho
w th
e re
side
ntia
l are
a is
sepa
rate
d fr
om th
e co
mm
erci
al a
rea.
Ms.
Steb
bins
repl
ied
that
ther
e is
a co
ncer
n re
gard
ing
the
view
that
may
be
avai
labl
e fr
om th
e to
p flo
or o
f the
hom
es a
djac
ent t
o th
e pr
oper
ty b
ut th
at th
ere
is a
cem
ent w
all t
hat s
epar
ates
the
resi
dent
ial
prop
ertie
s fro
m th
e co
mm
erci
al p
rope
rty. M
r. Ea
sthop
e su
gges
ted
that
we
may
nee
d an
add
ition
al s
epar
atio
n w
all a
roun
d th
e ox
ygen
tank
. Mr.
East
hope
stat
ed th
e on
e of
the
mos
t diff
icul
t cha
lleng
es w
ill b
e ap
prov
al
for t
he o
xyge
n ta
nk o
n-si
te b
y th
e C
ity a
nd th
e Fi
re M
arsh
all
Dire
ctor
Che
n m
entio
ned
he is
fam
iliar
with
the
area
and
stat
ed th
at th
ere
may
be
a ne
ed fo
r add
ition
al e
veni
ng li
ghtin
g fo
r saf
ety.
Dire
ctor
Gor
elic
k as
ked
if th
e fin
anci
ng is
con
tinge
nt u
pon
the
appr
oval
of
the
leas
e. M
r. Ea
sthop
e re
plie
d th
at o
nce
the
term
s of t
he le
ase
are
appr
oved
, the
con
tract
will
be
deve
lope
d, th
e co
ntra
ct w
ill g
o be
fore
the
Boar
d fo
r app
rova
l and
fina
ncin
g w
ill a
lso b
e re
view
ed fo
r Boa
rd
appr
oval
.
Dire
ctor
Gor
elic
k as
ked
if th
e B
oard
app
rove
s the
Let
ter o
f Int
ent t
onig
ht
and
do n
ot g
o ah
ead
with
the
cont
ract
, will
we
owe
Cus
hman
&
Wak
efie
ld a
fee.
Mr.
East
hope
repl
ied
that
Cus
hman
& W
akef
ield
onl
y ge
t pai
d if
we
ente
r int
o a
cont
ract
and
that
fee
is pa
id b
y th
e la
ndlo
rd o
f th
e pr
oper
ty.
Dire
ctor
Gor
elic
k in
quire
d as
to w
hy th
e de
prec
iatio
n w
as n
ot c
alcu
late
d in
the
finan
cial
pro
form
a. M
r. Ea
stho
pe v
erifi
ed th
e de
prec
iatio
n is
not
incl
uded
in th
e pr
ofor
ma.
Dire
ctor
Gor
elic
k as
ked
abou
t ins
uran
ce c
osts
rela
ted
to th
e on
-site
ox
ygen
tank
. Mr.
East
hope
repl
ied
that
the
Hos
pita
l, as
the
prim
ary
tena
nt, w
ould
be
resp
onsib
le fo
r the
maj
ority
of a
ny in
crea
se in
insu
ranc
e co
sts r
elat
ed to
the
oxyg
en ta
nk.
Ms.
Steb
bins
stat
ed th
at th
e ca
sh c
ontri
butio
n of
the
prog
ram
doe
s not
re
flect
dep
reci
atio
n in
the
initi
al p
rofo
rma.
Dire
ctor
Gor
elic
k di
sagr
eed
with
Ms.
Steb
bins
, sta
ting
that
you
mus
t cal
cula
te th
e up
fron
t cos
t in
the
payb
ack
perio
d to
det
erm
ine
if th
is is
a w
orth
whi
le in
vest
men
t.
Dire
ctor
Bat
tani
ask
ed D
irect
or G
orel
ick
wha
t he
wou
ld su
gges
t as i
t re
late
d to
his
conc
erns
ove
r the
Let
ter o
f Int
ent a
nd fi
nanc
ial p
rofo
rma
pres
ente
d. D
irect
or G
orel
ick
stat
ed th
at h
e w
as u
ncom
forta
ble
mak
ing
a
12

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
deci
sion
on
the
term
s of t
he le
ase
until
mor
e ac
cura
te fi
nanc
ial p
rofo
rmas
ar
e in
pla
ce.
Ms.
Steb
bins
stat
ed th
at M
anag
emen
t was
not
ask
ing
for a
dec
ision
re
gard
ing
the
finan
cial
pro
form
a. B
ut a
skin
g fo
r the
Boa
rd to
app
rove
the
term
s of t
he le
ase
in o
rder
to m
ove
the
cont
ract
pro
cess
forw
ard
to th
e ne
xt st
ep.
Dire
ctor
Deu
tsch
stat
ed th
at it
is im
porta
nt fo
r man
agem
ent t
o ha
ve s
ome
kind
of g
uida
nce
for t
he B
oard
to m
ove
prog
ram
dev
elop
men
t for
war
d.
Dire
ctor
Gor
elic
k ex
pres
sed
his c
once
rn a
bout
the
finan
cial
pro
form
a an
d th
e ov
eral
l fin
anci
ng fo
r the
pro
gram
, but
agr
eed
that
the
term
s of t
he
leas
e w
ere
good
term
s.
Dire
ctor
Bat
tani
mad
e a
mot
ion
to c
ombi
ne a
ctio
n ite
ms A
2 an
d A
3 fo
r vo
ting
purp
oses
.
3.
App
rova
l of W
ound
Car
e C
onst
ruct
ion
Build
-Out
Bud
get
Mr.
East
hope
pre
sent
ed a
reco
mm
enda
tion
to a
ppro
ve th
e W
ound
Car
e C
onst
ruct
ion
Build
-out
bud
get a
s pre
sent
ed.
Mr.
East
hope
stat
ed th
at th
e bu
dget
is o
nly
for t
he W
ound
Car
e sp
ace
(app
roxi
mat
ely
3,80
0 sq
uare
fe
et),
and
not f
or a
ny o
ther
serv
ices
. Tot
al c
ost f
or th
e bu
ild o
ut is
$8
70,6
98.
Dire
ctor
Gor
elic
k as
ked
if th
e H
ospi
tal w
as lo
cked
into
an
agre
emen
t with
A
ccel
ecar
e. D
irect
or B
atta
ni re
plie
d th
at w
e ar
e no
t loc
ked
into
an
agre
emen
t with
Acc
elec
are
and
that
ther
e ar
e te
rms i
n th
e ag
reem
ent w
ith
Acc
elec
are
that
are
con
tinge
nt o
n ob
tain
ing
finan
cing
for t
he o
vera
ll pr
ojec
t. M
r. Ea
stho
pe m
entio
ned
that
the
only
num
bers
that
hav
e be
en
upda
ted
in th
e fin
anci
al p
rofo
rma
wer
e th
e re
nt c
osts
.
Dire
ctor
McC
orm
ick
requ
este
d m
ore
deta
il of
wha
t was
incl
uded
in th
e in
th
e co
nstru
ctio
n co
sts.
Mr.
East
hope
repl
ied
that
the
cons
truct
ion
cost
s are
hi
gher
due
in p
art t
o cu
tting
thro
ugh
cem
ent s
lab
floor
s to
run
plum
bing
, el
ectri
cal w
iring
, H
VA
C sy
stem
s, an
d ru
nnin
g ox
ygen
to th
e hy
perb
aric
ox
ygen
cha
mbe
rs.
Dire
ctor
Gor
elic
k as
ked
if w
e ar
e pr
ohib
ited
to m
ove
the
proj
ect t
o an
off
islan
d sit
e. D
irect
or B
atta
ni re
plie
d th
at w
e ar
e to
ope
rate
all
Dist
rict
proj
ects
with
in th
e bo
unda
ries o
f the
Dist
rict.
Dire
ctor
Gor
elic
k as
ked
if th
e V
.A. w
ould
wor
k w
ith u
s on
a cl
inic
like
this.
Dire
ctor
Bat
tani
stat
ed
her c
once
rn th
at th
e V
.A. h
as n
ot b
roke
n gr
ound
at A
lam
eda
Poin
t and
the
13

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
leng
th o
f tim
e it
mak
e ta
ke to
initi
ate
the
idea
.
Dire
ctor
Bat
tani
sugg
este
d m
akin
g a
mot
ion
to c
ombi
ne th
e tw
o ac
tion
item
s int
o on
e m
otio
n fo
r app
rova
l. Th
e m
otio
n sh
e su
gges
ted
was
to
auth
oriz
e m
anag
emen
t to
mov
e fo
rwar
d on
the
deve
lopm
ent o
f a n
on-
bind
ing
agre
emen
t and
usi
ng th
e co
nstru
ctio
n bu
ild o
ut b
udge
t pro
pose
d to
pur
sue
finan
cing
opt
ions
and
the
com
plet
e bu
sine
ss c
ase.
B
. Pr
esid
ent’s
Rep
ort
1.
D
istric
t Boa
rd C
omm
ittee
s Bac
kgro
und
Mat
eria
ls
Dire
ctor
Bat
tani
info
rmed
the
Boa
rd th
at c
omm
ittee
ass
ignm
ents
will
ta
ke p
lace
at t
he Ja
nuar
y m
eetin
g. S
he a
sked
the
Boa
rd to
beg
in
thin
king
abo
ut w
hat c
omm
ittee
s the
y w
ould
like
to s
erve
on
and
in w
hat
capa
city
.
2.
D
raft
2011
Dist
rict B
oard
Mee
ting
Dat
es
Dire
ctor
Bat
tani
requ
este
d th
at a
ll Bo
ard
Mem
bers
coo
rdin
ate
with
D
istric
t Cle
rk, K
riste
n Th
orso
n if
ther
e ar
e an
y co
nflic
ts in
thei
r sc
hedu
le th
at w
ill p
reve
nt th
em fr
om a
ttend
ing
a D
istric
t Boa
rd
mee
tings
and
/or b
oard
des
igna
ted
com
mitt
ee m
eetin
gs. F
inal
app
rova
l of
the
2011
sche
dule
will
be
at th
e Ja
nuar
y 10
, 201
1 Bo
ard
mee
ting.
C
. C
hief
Exe
cutiv
e O
ffic
er’s
Rep
ort
1.
M
onth
ly S
tatis
tics
Ms.
Steb
bins
repo
rted
on th
e st
atist
ics f
or th
e m
onth
of N
ovem
ber,
notin
g th
at th
e ce
nsus
was
up
from
prio
r m
onth
s for
acu
te c
are
prog
ram
. Em
erge
ncy
Roo
m v
olum
es w
ere
dow
n 5%
from
the
budg
et, a
nd su
rger
y ca
ses w
ere
also
dow
n fo
r the
mon
th.
N
ovem
ber
Pr
elim
inar
y N
ovem
ber
Bud
get
% ∆
co
mpa
red
to B
udge
t
% ∆
co
mpa
red
to
Nov
embe
r O
ctob
er
Act
ual
Ave
rage
Dai
ly C
ensu
s 85
.7
82.7
3.
7%
7.8%
79
.5
Acu
te
31.6
26
.2
20.5
%
28.6
%
24.5
Su
bacu
te
32.3
33
.5
-3.7
%
-1.0
%
32.6
So
uth
Shor
e 21
.9
23
-4.8
%
-2.2
%
22.4
Pa
tient
Day
s 2,
572
2,48
1 3.
7%
4.3%
2,
465
ER V
isits
1,
397
1,47
0 -5
.0%
7.
0%
1,30
6 O
P Re
gist
ratio
ns
1,92
9 2,
078
-7.2
%
-5.1
%
2,03
2
14

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
Tota
l Sur
gerie
s*
178
182
-2.2
%
-17.
2%
215
Inpa
tient
Sur
gerie
s 38
31
22
.6%
0.
0%
38
Out
patie
nt S
urge
ries
140
151
-7.3
%
-20.
9%
177
2.
St
roke
Cer
tific
atio
n U
pdat
e
Ms.
Steb
bins
upd
ated
the
Boa
rd o
n th
e st
atus
of t
he H
ospi
tal a
chie
ving
st
roke
cer
tific
atio
n th
roug
h th
e Jo
int C
omm
issi
on.
Ms.
Steb
bins
add
ed th
ere
is a
need
for a
Pub
lic A
war
enes
s Cam
paig
n fo
r stro
ke e
duca
tion
and
awar
enes
s and
that
Ala
med
a C
ount
y EM
S ha
s in
dica
ted
that
they
will
ass
ist th
e H
ospi
tal f
inan
cial
ly in
the
impl
emen
tatio
n of
such
a c
ampa
ign.
Dire
ctor
Bat
tani
sugg
este
d th
e ne
ed fo
r pub
lic e
duca
tion
in te
rms
of
reco
gniz
ing
stro
ke s
ympt
oms a
nd in
terv
enin
g ea
rly. D
irect
or B
atta
ni
aske
d w
hat t
he ti
mel
ine
was
for t
he st
art o
f the
of t
he p
ublic
aw
aren
ess
cam
paig
n. M
ary
Bond
, RN
, Exe
cutiv
e D
irect
or o
f Nur
sing
Serv
ices
an
d Lo
uise
Nak
ada,
Dire
ctor
of C
omm
unity
Rel
atio
ns in
dica
ted
that
it
wou
ld st
art i
n Ja
nuar
y/Fe
brua
ry 2
011.
Dire
ctor
Che
n as
ked
how
muc
h re
venu
e is
lost
due
to st
roke
pat
ient
s be
ing
rout
ed o
ff-is
land
. M
s. St
ebbi
ns re
plie
d it
has n
ot b
een
a la
rge
finan
cial
impa
ct o
n th
e H
ospi
tal.
Dire
ctor
Gor
elic
k as
ked
if th
ere
is a
chec
klist
of t
hing
s to
do
in th
e st
roke
cer
tific
atio
n pr
oces
s. M
s. St
ebbi
ns re
plie
d th
at sh
e w
ould
pr
ovid
e th
at in
form
atio
n to
Dire
ctor
Gor
elic
k.
Ms.
Bond
add
ed th
at th
e Jo
int C
omm
issi
on w
ill a
llow
Ala
med
a H
ospi
tal t
o se
e st
roke
pat
ient
s as s
oon
as w
e re
ceiv
e ou
r sur
vey
date
fr
om th
e Jo
int C
omm
issi
on.
Dire
ctor
Bat
tani
add
ed th
e St
roke
Cer
tific
atio
n to
pic
will
be
a sta
ndin
g ite
m o
n th
e ag
enda
for f
utur
e Bo
ard
Mee
tings
.
3.
IT
Pro
ject
s Upd
ate
Ms.
Steb
bins
stat
ed th
at th
e PA
CS
syst
em th
at is
sche
dule
d to
go
live
in e
arly
201
1. M
s. St
ebbi
ns st
ated
that
ther
e ha
ve b
een
rece
nt c
hang
es
in th
e IT
dep
artm
ent l
eade
rshi
p an
d cu
rren
tly th
e IT
Dep
artm
ent
repo
rts d
irect
ly to
her
. Sh
e is
wor
king
with
a c
onsu
lting
firm
to a
sses
s
15

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
the
depa
rtmen
t and
recr
uit a
new
Dire
ctor
.
D
. Fi
nanc
e an
d M
anag
emen
t Com
mitt
ee R
epor
t
1.
C
omm
ittee
Rep
ort –
Nov
embe
r 24,
201
0
Dire
ctor
Bat
tani
stat
ed th
at th
e ef
forts
to im
plem
ent a
new
sys
tem
for
time
and
atte
ndan
ce h
ave
been
aba
ndon
ed. T
he H
ospi
tal i
s ex
plor
ing
new
opt
ions
and
will
see
k so
me
finan
cial
reco
very
for s
oftw
are
and
equi
pmen
t fro
m th
e co
mpa
ny.
Dire
ctor
Bat
tani
stat
ed th
at b
ased
on
initi
al fi
nanc
ial f
easib
ility
resu
lts
that
alte
rnat
e op
tions
for s
eism
ic fi
nanc
ing
will
nee
d to
be
disc
usse
d.
Dire
ctor
Gor
elic
k st
ated
that
he
had
ques
tions
rega
rdin
g re
cent
em
ail
com
mun
icat
ions
bet
wee
n D
irect
or B
atta
ni a
nd M
s. St
ebbi
ns.
His
ques
tion
rela
ted
to e
xten
sion
opt
ions
for s
eism
ic c
ompl
ianc
e ba
sed
on
Med
i-Cal
cas
e m
ix.
Dire
ctor
Bat
tani
mad
e a
reco
mm
enda
tion
that
m
anag
emen
t pro
vide
d an
ove
rvie
w o
f sei
smic
stat
us a
t the
nex
t Boa
rd
mee
ting,
incl
udin
g ex
tens
ion
optio
ns a
vaila
ble
to H
ospi
tals
and
whe
re
the
Hos
pita
l sta
nds a
s it r
elat
es to
seis
mic
com
plia
nce
and
rela
ted
exte
nsio
n op
tions
.
E.
C
omm
unity
Rel
atio
ns a
nd O
utre
ach
Rep
ort
1.
C
omm
ittee
Rep
ort –
Nov
embe
r 16,
201
0
Dire
ctor
McC
orm
ick
reco
gniz
ed D
enni
s Elo
e fo
r his
new
affi
liatio
n w
ith th
e C
ham
ber o
f Com
mer
ce a
s Pre
side
nt a
nd fo
r his
eff
orts
co
nnec
ting
busi
ness
es in
the
com
mun
ity.
Dire
ctor
McC
orm
ick
reco
gniz
ed L
ouis
e N
akad
a fo
r her
ded
icat
ed w
ork
with
the
com
mun
ity, n
ewsl
ette
rs, w
ebsit
e, a
nd o
utre
ach.
Dire
ctor
McC
orm
ick
reco
gniz
ed T
ony
Cor
ica
for h
is in
volv
emen
t with
re
crui
tmen
t of n
ew P
hysi
cian
s.
Dire
ctor
McC
orm
ick
men
tione
d th
e co
ntac
ts th
at h
ave
been
mad
e w
ith
the
Busi
ness
Ass
ocia
tions
and
the
Boy
s and
Girl
s Clu
b.
Loui
se N
akad
a st
ated
that
a la
rge
initi
ativ
e fo
r the
futu
re is
to w
ork
with
A
lam
eda
yout
h an
d ed
ucat
e th
e pu
blic
abo
ut c
hild
hood
obe
sity
.
16
DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
F.
M
edic
al S
taff
Pres
iden
t Rep
ort
Dire
ctor
Sha
rma
invi
ted
all m
embe
rs to
the
post
-hol
iday
eve
nt h
oste
d by
the
Med
ical
Sta
ff on
Janu
ary,
14th
, 201
1.
IX.
Gen
eral
Pub
lic C
omm
ents
Non
e
X.
Boar
d C
omm
ents
M
s. St
ebbi
ns e
xten
ded
her g
ratit
ude
to th
e M
edic
al S
taff
for t
heir
rapi
d ac
tion
in
refe
renc
e to
stro
ke p
roto
cols.
Dire
ctor
Sha
rma
than
ked
the
mem
bers
of t
he B
oard
for t
he o
ppor
tuni
ty to
ser
ve
with
them
.
XI.
Adj
ourn
into
Exe
cutiv
e C
lose
d Se
ssio
n A
mot
ion
was
mad
e to
Adj
ourn
the
mee
ting
into
Exe
cutiv
e C
lose
d Se
ssio
n at
9:4
5 PM
.
XII.
R
egul
ar A
gend
a
B.
Ann
ounc
emen
ts fr
om C
lose
d Se
ssio
n
The
mee
ting
was
reco
nven
ed in
to O
pen
Sess
ion
at 1
0:17
p.m
. D
irect
or
Batta
ni re
porte
d th
at th
e fo
llow
ing
actio
ns w
ere
take
n in
Clo
sed
Sess
ion.
1.
Cl
osed
Ses
sion
Min
utes
– N
ovem
ber 8
, 201
0 (R
egul
ar)
The
Clo
sed
Sess
ion
Min
utes
wer
e ap
prov
ed.
2.
Med
ical
Exe
cutiv
e C
omm
ittee
Rep
ort a
nd A
ppro
val o
f Cre
dent
ialin
g R
ecom
men
datio
ns
The
Med
ical
Exe
cutiv
e C
omm
ittee
R
epor
t and
Cre
dent
ialin
g R
ecom
men
datio
ns w
ere
appr
oved
as
pre
sent
ed b
elow
.
3.
Boar
d Q
ualit
y C
omm
ittee
(BQ
C) R
epor
t – S
epte
mbe
r 201
0
The
BQC
repo
rt w
as a
ccep
ted
as
pres
ente
d.
In
itial
App
oint
men
ts –
Med
ical
Sta
ff
Nam
e Sp
ecia
lty
Aff
iliat
ion
○
Ron
ald
Che
n, M
D
Tele
radi
olog
y Ba
y Im
agin
g C
onsu
ltant
s
○
Roy
ce C
hrys
, MD
Te
lera
diol
ogy
Bay
Imag
ing
Con
sulta
nts
○
Ang
ela
Cru
dale
, MD
Te
lera
diol
ogy
Bay
Imag
ing
Con
sulta
nts
○
Step
hen
Hes
selin
e, M
D
Tele
radi
olog
y Ba
y Im
agin
g C
onsu
ltant
s
○
Will
iam
Hod
dick
, MD
Te
lera
diol
ogy
Bay
Imag
ing
Con
sulta
nts
17

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
○
Dav
id H
owar
d, M
D
Tele
radi
olog
y Ba
y Im
agin
g C
onsu
ltant
s
○
Ron
eesh
a K
nigh
t, M
D
Emer
genc
y M
edic
ine
Emer
genc
y D
epar
tmen
t
○
Baile
y Le
e, M
D
Tele
radi
olog
y Ba
y Im
agin
g C
onsu
ltant
s
○
Sund
eep
Nay
ak, M
D
Tele
radi
olog
y Ba
y Im
agin
g C
onsu
ltant
s
○
Saur
abh
Pate
l, M
D
Tele
radi
olog
y Ba
y Im
agin
g C
onsu
ltant
s
○
Wen
dy P
atto
n, M
D
Tele
radi
olog
y Ba
y Im
agin
g C
onsu
ltant
s
○
Jona
than
Pos
in, M
D
Tele
radi
olog
y Ba
y Im
agin
g C
onsu
ltant
s
○
Ase
em R
awal
, MD
Te
lera
diol
ogy
Bay
Imag
ing
Con
sulta
nts
○
Joan
Rey
nold
s. M
D
Tele
radi
olog
y Ba
y Im
agin
g C
onsu
ltant
s
○
Eric
Sal
ding
er, M
D
Tele
radi
olog
y Ba
y Im
agin
g C
onsu
ltant
s
○
Rob
ert S
chic
k, M
D
Tele
radi
olog
y Ba
y Im
agin
g C
onsu
ltant
s
○
Eric
Tao
, MD
Te
lera
diol
ogy
Bay
Imag
ing
Con
sulta
nts
○
Kei
th T
ao, M
D
Tele
radi
olog
y Ba
y Im
agin
g C
onsu
ltant
s
R
eapp
oint
men
ts –
Med
ical
Sta
ff
Nam
e Sp
ecia
lty
Staf
f Sta
tus
App
oint
men
t Per
iod
○
Has
seeb
Al-M
ufti,
MD
N
ephr
olog
y C
ourte
sy
01/0
1/11
– 1
2/31
/12
○
Jim
my
Car
doza
, MD
R
adio
logy
C
ourte
sy
02/0
1/11
– 0
1/31
/13
○
Edw
ard
Cha
n, M
D
Fam
ily P
ract
ice
Cou
rtesy
02
/01/
11 –
01/
31/1
3
○ K
enne
th C
hang
, MD
G
ener
al S
urge
ry
Cou
rtesy
02
/01/
11 –
01/
31/1
3
○ Ev
an C
uste
r, M
D
Rad
iolo
gy
Cou
rtesy
02
/01/
11 –
01/
31/1
3
○ Jo
anne
DeP
hilli
ps, M
D
Inte
rnal
Med
icin
e A
ctiv
e 01
/01/
11 –
12/
31/1
2
○
Susa
n Ei
senb
erg,
MD
C
ardi
olog
y C
ourte
sy
02/0
1/11
– 0
1/31
/13
○
Yin
g Fu
ng, M
D
Rad
iolo
gy
Cou
rtesy
02
/01/
11 –
01/
31/1
3
○ R
obbi
n G
reen
-Yeh
, DO
In
tern
al M
edic
ine
Cou
rtesy
02
/01/
11 –
01/
31/1
3
○ D
onal
d K
ent,
DD
S D
entis
try
Cou
rtesy
01
/01/
11 –
12/
31/1
2
○ Su
san
Less
in, M
D
Hem
atol
ogy/
Onc
olog
y C
ourte
sy
01/0
1/11
– 1
2/31
/12
○
Scot
t Lip
son,
MD
R
adio
logy
C
ourte
sy
02/0
1/11
– 0
1/31
/13
○
Am
y M
atec
ki, M
D
Inte
rnal
Med
icin
e C
ourte
sy
01/0
1/11
– 1
2/31
/12
○
Cat
herin
e Py
un, D
O
Inte
rnal
Med
icin
e A
ctiv
e 02
/01/
11 –
01/
31/1
3
18

DIS
TRIC
T BO
AR
D/M
INU
TES/
REG
.12.
13.1
0
○
Jack
Ste
hr, M
D
Orth
oped
ics
Act
ive
02/0
1/11
– 0
1/31
/13
○
Don
ald
Stin
ghen
, MD
G
ener
al S
urge
ry
Act
ive
02/0
1/11
– 0
1/31
/13
○
Nai
lah
Thom
pson
, DO
In
tern
al M
edic
ine
Cou
rtesy
02
/01/
11 –
01/
31/1
3
Initi
al A
ppoi
ntm
ent –
Alli
ed H
ealth
Pro
fess
iona
ls
Nam
e Sp
ecia
lty
○
Emily
Won
g, P
A-C
Ph
ysic
ian
Ass
istan
t
R
eapp
oint
men
t – A
llied
Hea
lth P
rofe
ssio
nal S
tatu
s
Nam
e Sp
ecia
lty
App
oint
men
t Per
iod
○
Rac
hel B
axte
r, PA
-C
Phys
icia
n A
ssist
ant
02/0
1/11
– 0
1/31
/13
○
Ann
Whi
sena
nt, P
A-C
Ph
ysic
ian
Ass
istan
t 01
/01/
11 –
12/
31/1
2
R
esig
natio
ns
Nam
e Sp
ecia
lty
○
Kay
Tra
n, P
A-C
Ph
ysic
ian
Ass
istan
t
XIII
. G
ener
al P
ublic
Com
men
ts
Non
e
XIV
. Bo
ard
Com
men
ts
Non
e
XV
. A
djou
rnm
ent
A m
otio
n w
as m
ade
to a
djou
rn th
e m
eetin
g an
d be
ing
no fu
rther
bus
ines
s, th
e m
eetin
g w
as a
djou
rned
at 1
0:17
p.m
.
Atte
st:
Jord
an B
atta
ni
J.
Mic
hael
McC
orm
ick
Pres
iden
t
Tr
easu
rer
19

Date: January 10, 2011 To: City of Alameda Health Care District Board of Directors From: Deborah E. Stebbins, Chief Executive Officer Subject: Approval of Administrative Policies and Procedures The following Administrative Policies and Procedures have been updated to reflect current practices, regulatory language and information. Policies and Procedures are available for review upon request. Management requests approval of the Administrative Policies and Procedures listed below. Policy # Policy Title & Purpose Statement No. 28
Procedural Sedation REVISION PURPOSE: To outline the management of patients receiving sedation for therapeutic and/or diagnostic procedures.
No. 39
Health Record Content REVISON PURPOSE: To show responsibility for documentation and proper authentication in the medical record.
20

DATE: January 10, 2010 TO: City of Alameda Health Care District, Board of Directors FROM: Phyllis J. Weiss, Director of Human Resources SUBJECT: Approval of Human Resources Policy – Performance Evaluation Recommendation: Modify the current Human Resources policy to reflect an “end of month” due date for Annual Performance Evaluations. Also incorporate into the policy the current practice of how the CEO’s performance evaluation is conducted and filed. Background: Performance Review Timeliness: The current policy requires a Performance Evaluation at two times:
1. A Probationary Performance Evaluation by the end of the first ninety (90) days of employment.
2. An Annual Performance Evaluation with no more than fourteen (14) months between reviews.
With approximately 575 employees, the task of completing each evaluation with thoughtful and meaningful feedback in a timely manner becomes a challenge for those Managers who have a significant number due during the year. HR has developed tracking tools to assist the Managers to remain in compliance, including a “last warning” system in an attempt to avoid delinquencies. In addition to these tools, we feel that moving the evaluation due date to the end of the month in which it is due will relieve the Manager from focusing on a specific date in the month and potentially missing it.
21

2
Documentation of CEO Performance Review process: In the past the CEO’s review has been completed by the Board Chair with input from the Board members and was filed in a confidential envelope in the HR file. In addition, a summary of the review findings (“Meets” or “Exceeds” expectations was incorporated into the open part of the HR file. This will continue to be the practice and will now be documented in this policy. Discussion: Performance Evaluation Timeliness: During our Joint Commission inspection it was found we were not in compliance with Performance Review timeliness. We took several affirmative steps in order to get in compliance and Managers have responded well. One of the steps was to recommend extending the due date until the end of the month in which a review is due. As a result of our efforts, by the end of November, 2010, the Hospital exceeded the 95% goal we established for ourselves and are currently at 99.9% timely submissions. Documentation of CEO Performance Review process: This is only a policy update to reflect our current practice.
22

CITY OF ALAMEDA HEALTH CARE DISTRICT
Human Resources Policy Performance Evaluation
TITLE: Performance Evaluation PURPOSE: To ensure employees are evaluated in writing by the Department
Manager on a regular basis. POLICY: A performance evaluation will be completed for all employees during the first ninety (90) days of employment and annually thereafter, with no more than fourteen (14) months between evaluations. Performance reviews must be submitted by the last day of the month in which they are due in order to be considered to have been submitted in a timely manner. PROCEDURE: Department Managers/Directors are responsible for completing a probationary and an annual, written, performance evaluation on each of the employees reporting to them. Performance evaluations provide the employee with an opportunity to discuss their work based on their specific areas of responsibility. During the evaluation the employee’s competency and accomplishments will be discussed, as well as any areas of deficiency and/or opportunity for development. If the employee feels the performance evaluation does not agree with their perception of their own performance, the employee may request a review by the Human Resources Director. The finalized performance evaluation, together with any comments the employee wishes to submit, will be included in the employee’s personnel file. The completion rate of performance evaluations by Department Directors is reviewed by the CEO at each Department director’s evaluation. The percentage of performance evaluations completed in a timely manner together with their ratings, are reported to the Board of Directors on an annual basis. Employees who do not meet expectations may be placed on a Performance Improvement Plan (PIP) during the probationary period, at the time of their annual evaluation, or anytime during the year the employee is not meeting expectations.
23

This PIP must be reviewed by the Human Resources Director in advance and will include specific areas of non-compliance, expected goals and timelines. The PIP will also invite the employee to identify any areas of training and/or orientation needs in order to meet with success. The Department Director/Manager will hold regular meetings with the employee to provide both oral and written feedback on their progress, or lack thereof, through the PIP review period. Employees who do not successfully complete the PIP goals and timelines may be terminated for lack of performance. This decision must be approved by the Department Administrator in consultation with the Human Resources Director. Performance Review submission for the Chief Executive Officer (CEO): A Performance Evaluation will be completed during the first ninety (90) days of employment for the CEO and annually thereafter, with no more than fourteen (14) months between reviews. A Performance review for the CEO must be conducted no later than last day of the month in which it is due in order to be considered to have been submitted in a timely manner The Performance Evaluation for the CEO will be conducted by the Chair of the Board of Directors with input from the Board members. The review will be filed in the CEO’s personnel file in a confidential envelope to be accessed by the Board Chair only. A summary of the findings (“Meets Expectations” or “Exceeds expectations”) will be filed in the personnel file as a memo to document timely and successful completion of the review period. If the review is rated at the “Does Not Meet” level, either a Performance Improvement Plan will be developed or employment action may be taken in accordance with the employment contract between the CEO and The City of Alameda Health Care District, dba Alameda Hospital. The decision to place the CEO on a PIP or whether to take employment action via the contract will be affirmed by the Chair of the Board of Directors. City of Alameda Health Care District
Performance Evaluation Action: Date: By: Created: 1/7/11 Human Resources Approval: 12/10 Administration
01/11 District Board
24

Date: January 10, 2011 To: City of Alameda Health Care District, Board of Directors From: Robert Deutsch, MD, Chair –Board Quality Committee Deborah Stebbins, CEO Subject: Approval of Board Quality Committee Structure and Purpose Recommendation: We are proposing that the following committee structure be approved by the District Board of Directors. Similar committee structures have been developed for other two board designated committees (Finance and Management Committee and Community Relations and Outreach Committee).
1. Board Quality Committee:
a. Primary Purpose:
i. To review monitoring activity and accept or reject the periodic summary of performance improvement data submitted by the Performance Improvement Committee (PIC).
ii. To assure the measurements, assessments and improvements are consistent with the design of the Performance Improvement Program and the hospital’s mission, vision and values.
b. Committee Composition and Voting Rights: The committee shall
be comprised of the following members:
i. Two members of the City of Alameda Health Care District Board of Directors both of whom shall be voting members of the committee.
ii. The President of the City of Alameda Health Care District Board of Directors shall be an ex-officio, non-noting member, unless the President is serving as a voting member of the committee.
25

2
iii. Up to four members of the Alameda Hospital Medical Staff
(physicians) all of whom shall be voting members of the committee as designated below. In instances where a physician qualifies as one or more of the following designations, an additional physician will not be needed.
1. Medical Staff President 2. Hospitalist Representative 3. Quality Resource Management Medical Director 4. Medical Staff At-Large Representative
iv. The City of Alameda Health Care District Chief Executive
Officer, Chief Financial Officer, Associate Administrator, Director of Quality Resource Management, and Executive Director of Nursing Services, and other hospital management as delegated, who shall not be voting members of the committee.
c. Terms: The committee shall be appointed annually.
d. Meeting Frequency: Committee shall meet monthly.
26

Date: January 10, 2011 To: City of Alameda Health Care District, Board of Directors From: Deborah E. Stebbins, CEO Subject: Approval of Union Bank Signing Authorization / Resolution Recommendation: Management recommends that the City of Alameda Health Care District approve the Certificate of Secretary/partner Corporate, Unincorporated Non-business Association Or Partnership Resolution for the Alameda Hospital Pension Plan and authorize the Secretary of the Board to sign the resolution on behalf of the District. Background: The authorized signers are being amended to add Karen Hopkins, Benefits Manager at Alameda Hospital. Our pension plans require two signatures to release the retirement funds, so this will make the processing of such requests more expedient.
27

28

29

30

DATE: January 10, 2011 TO: City of Alameda Health Care District, Board of Directors FROM: Kristen S. Thorson, District Clerk SUBJECT: Election of District Officers Recommendation: Approve the proposed slate of officers to serve a term of one (1) year or until such time as a successor is elected.
1. President: Jordan Battani
2. First Vice President: Robert Deutsch, MD
3. Second Vice President: Stewart Chen, DC 4. Treasurer: J. Michael McCormick
5. Secretary: Elliott Gorelick
Background: In preparation for the annual election of officers, I have queried each Board Member as to their preference and based upon the responses, the above slate of officers is proposed. Since there are five (5) offices and five (5) Board of Directors, each Board Member will hold an office. Article III, Section 1 of the District Bylaws provides for the election of District officers. Section 1.D. reads: “Officers shall hold their office for terms of one (1) year or until such time as a successor is elected…. Officers may serve consecutive terms.” A copy of the entirety of Article III is attached for your review. The following is a current list of District Officers:
1. President: Jordan Battani
2. First Vice President: Robert Deutsch, MD
3. Second Vice President: Vacant
31
4. Treasurer: J. Michael McCormick
5. Secretary: Vacant
Section 1. C. “Each officer shall be elected upon receiving a majority vote with each member of the Board of Directors having one vote. In the event that there is no majority for a single office, the candidate with the fewest votes shall be eliminated from candidacy and a runoff election with the remaining candidates shall take place. In the event that more than two candidates have an equal number of votes, the office shall be selected by random lot.”
ARTICLE I
OFFICERS
Section 1.
A. The officers of this District shall be President, First Vice-President, Second Vice-President, Secretary, Treasurer, and such other officers as the Board of Directors shall determine are necessary and appropriate.
Officers
B. The offices of President, First Vice-President, Second Vice-President and Secretary shall be filled by election from the membership of the Board of Directors. The office of Treasurer may or may not be filled by a member of the Board of Directors.
C. Each officer shall be elected upon receiving a majority vote with each member of the Board of Directors having one vote. In the event that there is no majority for a single office, the candidate with the fewest votes shall be eliminated from candidacy and a runoff election with the remaining candidates shall take place. In the event that more than two candidates have an equal number of votes, the office shall be selected by random lot.
D. Officers shall be elected at such regular Board meeting as is specified by the Board.
E. Officers shall hold their office for terms of one ( 1 ) year or until such time as a successor is elected. An officer may be removed from office by a majority of the Board of Directors at any time. Officers may serve consecutive terms.
Section 2.
A. The President shall perform the following duties:
President
1. Preside over the meetings of the Board of Directors;
2. Sign and execute jointly with the Secretary, in the name of the District, all contracts and conveyances and all other instruments in writing that have been authorized by the Board of Directors;
32

3. Exercise the power to co-sign, with the Secretary checks drawn on the funds of the District whenever:
a. There is no person authorized by resolution of the Board of Directors to sign checks on behalf of the District regarding a particular matter; or
b. It is appropriate or necessary for the President and Secretary to sign a check drawn on District funds.
4. Have, subject to the advice and control of the Board of Directors, general responsibility for the affairs of the District, and generally discharge all other duties that shall be required of the President by the Bylaws of the District.
B. If at any time, the President is unable to act as President, the Vice Presidents, in the order hereinafter set forth, shall take the President’s place and perform the President’s duties; and if the Vice Presidents are also unable to act, the Board may appoint someone else to do so, in whom shall be vested, temporarily, all the functions and duties of the office of the President.
Section 3.
A. In the absence of the President or given the inability of the President to serve, the First Vice-President, or in the First Vice-President’s absence, the Second Vice-President, shall perform the duties of the President.
Vice-Presidents
B. Perform such reasonable duties as may be required by the members of the Board of Directors or by the President.
Section 4.
The Secretary shall have the following duties:
Secretary
A. To act as Secretary of the District and the Board of Directors.
B. To be responsible for the proper keeping of the records of all actions, proceedings, and minutes of meetings of the Board of Directors.
C. To be responsible for the proper recording, and maintaining in a special book or file for such purpose, all ordinances and resolutions of the Board of Directors (other than amendments to these Bylaws) pertaining to policy or administrative matters of the District and its facilities.
D. To serve, or cause to be served, all notices required either by law or these Bylaws, and in the event of the Secretary’s absence, inability, refusal or neglect to do so, such notices may be served by any person so directed by the President or Board of Directors.
E. To have custody of the seal of this District and the obligation to use it under the direction of the Board of Directors.
33

F. To perform such other duties as pertain to the Secretary’s office and as are prescribed by the Board of Directors.
Section 5.
A. The Board of Directors shall establish its own treasury and shall appoint a Treasurer charged with the safekeeping and disbursal of the funds in the treasury.
Treasurer
B. The Board of Directors shall fix the amount of bond to be given by the Treasurer and shall provide for the payment of the premium therefor.
C. The Treasurer, who may or may not be a member of the Board of Directors, shall be selected by the Board of Directors based upon his or her competence, skill, and expertise.
D. The Treasurer shall be responsible for the general oversight of the financial affairs of the District, including, but not limited to receiving and depositing all funds accruing to the District, coordinating and overseeing the proper levy and collection of the District’s annual parcel tax, performance of all duties incident to the office of Treasurer and such other duties as may be delegated or assigned to him or her by the Board of Directors, provided, however, that the Chief Financial Officer of the District shall implement, and carry out the day to day aspects of the District’s financial affairs.
E. The Treasurer shall maintain active and regular contact with the administrative staff for the purpose of obtaining that information necessary to carry out his or her duties.
34

DATE: January 10, 2011 TO: City of Alameda Health Care District, Board Directors FROM: Deborah E. Stebbins, Chief Executive Officer SUBJECT: 2011 District Board Meeting / Committee Dates Recommendation: Management is recommending approval of the attached schedule for 2011. 2011 District Board & Committee Meeting Dates:
1. District Board meetings will be held the first Monday of the month unless otherwise noted.
2. Finance & Management Committee will meet the last Wednesday of the month at
7:30 a.m.
3. Community Relations and Outreach Committee will meet the fourth Tuesday of the month at 7:30 a.m.
4. Board Quality Committee will meet on the 3rd Wednesday of the month at 7:30
a.m.
35

City
of A
lam
eda
Hea
lth C
are
Dis
trict
20
11 M
eetin
g D
ates
Dis
trict
Boa
rdFi
nanc
e &
Man
agem
ent C
omm
ittee
Com
mun
ity R
elat
ions
Com
mitt
ee
Boa
rd Q
ualit
y C
omm
ittee
Firs
t Mon
day
of th
e M
onth
Last
Wed
nesd
ay o
f the
mon
th4t
h Tu
esda
y of
the
Mon
th3r
d W
edne
sday
of t
he m
onth
Clo
sed
Ses
sion
& O
pen
Ses
sion
Ope
n S
essi
onO
pen
Ses
sion
Clo
sed
Ses
sion
6:00
p.m
. / 7
:30
p.m
.7:
30 a
.m.
7:30
a.m
.7:
30 a
.m.
Dal
Cie
lo R
oom
/ B
oard
Roo
mD
al C
ielo
Roo
mD
al C
ielo
Roo
mB
oard
Roo
m
Jan-
11M
onda
y, J
anua
ry 1
0, 2
011
Wed
nesd
ay, J
anua
ry 2
6, 2
011
Tues
day,
Jan
uary
25,
201
1W
edne
sday
, Jan
uary
19,
201
1
Feb-
11M
onda
y, F
ebru
ary
07, 2
011
Wed
nesd
ay, F
ebru
ary
23, 2
011
Tues
day,
Feb
ruar
y 22
, 201
1W
edne
sday
, Feb
ruar
y 16
, 201
1
Mar
-11
Mon
day,
Mar
ch 0
7, 2
011
Wed
nesd
ay, M
arch
30,
201
1Tu
esda
y, M
arch
22,
201
1W
edne
sday
, Mar
ch 1
6, 2
011
Apr
-11
Mon
day,
Apr
il 04
, 201
1W
edne
sday
, Apr
il 27
, 201
1Tu
esda
y, A
pril
26, 2
011
Wed
nesd
ay, A
pril
20, 2
011
May
-11
Mon
day,
May
02,
201
1W
edne
sday
, May
25,
201
1Tu
esda
y, M
ay 2
4, 2
011
Wed
nesd
ay, M
ay 1
8, 2
011
Jun-
11M
onda
y, J
une
06, 2
011
Wed
nesd
ay, J
une
29, 2
011
Tues
day,
Jun
e 28
, 201
1W
edne
sday
, Jun
e 15
, 201
1
Jul-1
1M
onda
y, J
uly
11, 2
011
Wed
nesd
ay, J
uly
27, 2
011
Tues
day,
Jul
y 26
, 201
1W
edne
sday
, Jul
y 20
, 201
1
Aug
-11
Mon
day,
Aug
ust 0
1, 2
011
Wed
nesd
ay, A
ugus
t 31,
201
1Tu
esda
y, A
ugus
t 23,
201
1W
edne
sday
, Aug
ust 1
7, 2
011
Sep
-11
Mon
day,
Sep
tem
ber 1
2, 2
011
Wed
nesd
ay, S
epte
mbe
r 28,
201
1Tu
esda
y, S
epte
mbe
r 27,
201
1W
edne
sday
, Sep
tem
ber 2
1, 2
011
Oct
-11
Mon
day,
Oct
ober
03,
201
1W
edne
sday
, Oct
ober
26,
201
1Tu
esda
y, O
ctob
er 2
5, 2
011
Wed
nesd
ay, O
ctob
er 1
9, 2
011
Nov
-11
Mon
day,
Nov
embe
r 07,
201
1W
edne
sday
, Nov
embe
r 30,
201
1Tu
esda
y, N
ovem
ber 2
2, 2
011
Wed
nesd
ay, N
ovem
ber 1
6, 2
011
Dec
-11
Mon
day,
Dec
embe
r 05,
201
1N
o M
eetin
gTu
esda
y, D
ecem
ber 2
7, 2
011
Wed
nesd
ay, D
ecem
ber 2
1, 2
011
36

Date: January 10, 2011 To: City of Alameda Health Care District, Board of Directors From: Kristen S. Thorson, District Clerk Subject: 2011 Appointment to Board Committees Recommendation: Approve the proposed Board Committee assignments as outlined below.
Finance and Management Committee
Board Quality Committee
Community Relations and Outreach Committee
Committee Chair Michael McCormick Robert Deutsch, MD Stewart Chen, DC
Voting Member Robert Deutsch, MD Elliott Gorelick Michael McCormick
Ex-Officio Jordan Battani Jordan Battani Jordan Battani
In addition, it is requested that the Board appoint Director Michael McCormick as the Board representative to the Administrative Pension Plan Oversight Committee (APPOC). Background: In preparation for the 2011 appointment to Board Committees, each Board Member was queried as to their preference of committee assignments and based upon the responses, the committee assignments are proposed as outlined above. Board Members are encouraged to attend any committee meeting Each Committee has approved a structure and purpose which designates committee composition including Board Member participation. The current structure as it pertains to the Board of Directors is outlined below. Article V of the Bylaws is also attached for reference.
1. Finance and Management Committee:
Committee Composition and Voting Rights: The committee shall be comprised of the following members:
37

2
Two members of the City of Alameda Health Care District Board of Directors both of whom shall be voting members of the committee. The President of the City of Alameda Health Care District Board of Directors shall be an ex-officio, non-voting member of the committee.
2. Community Relations and Outreach Committee:
Committee Composition and Voting Rights: The committee shall be comprised of the following members:
At least two members of the City of Alameda Health Care District Board of Directors all of whom shall be voting members of the committee. One of these members also shall be appointed to serve as the committee co-chair. The other co-chair will be an at large member from the community.
3. Board Quality Committee:
Committee Composition and Voting Rights: The committee shall be comprised of the following members:
Two members of the City of Alameda Health Care District Board of Directors both of whom shall be voting members of the committee.
The President of the City of Alameda Health Care District Board of Directors shall be an ex-officio, non-noting member, unless the President is serving as a voting member of the committee.
38

3
ARTICLE V
COMMITTEES
Section 1.
A. The Board of Directors may, by resolution, establish one or more committees and delegate to such committees any aspect of the authority of the Board of Directors. Membership and chairmanship of such committees shall be appointed by the Board. The Board of Directors shall have the power to prescribe the manner in which proceedings of any committee shall be conducted. In the absence of any such prescription, such committee shall have the power to prescribe the manner in which its proceedings shall be conducted.
Committees Generally
B. A majority of the members of a committee shall constitute a quorum of such committee and the act of a majority of members present at which a quorum is present shall be the act of the committee.
C. Unless the Board of Directors or the committee shall otherwise provide, the regular and special meetings and other actions of any Committee shall be governed by the same requirements set forth in Article II, Sections 7 and 8 applicable to meetings and actions of the Board of Directors.
39

Your
Tru
sted
Adv
isor
for E
xper
t Res
ults
WH
O W
E A
RE,
GO
VER
NAN
CE
BES
T PR
AC
TIC
ES, &
TOTA
L C
OM
PEN
SATI
ON
REV
IEW
PR
OC
ESS
PR
EP
AR
ED
FO
R
ALA
MED
A H
OSP
ITAL
PR
EP
AR
ED
BY
BIL
L H
OPK
INS,
SEN
IOR
CO
NSU
LTAN
T
JAN
UA
RY 5
, 201
1
40

Inte
grat
ed H
ealth
care
Str
ateg
ies
1
41
Inte
grat
ed H
ealth
care
Str
ateg
ies
-Who
We
Are
2
•Fo
un
de
d in
19
73
•O
ffic
es
in M
inn
eap
olis
an
d K
ansa
s C
ity
•N
ear
ly 2
00
ass
oci
ate
s
•C
lien
ts in
clu
de
ove
r 9
00
maj
or
he
alth
care
pro
vid
ers
•La
rge,
inte
grat
ed p
rovi
der
net
wo
rks
and
sys
tem
s
•A
cad
emic
med
ical
cen
ters
•La
rge,
mu
lti-
spec
ialt
y gr
ou
p p
ract
ices
•C
hild
ren
’s h
osp
ital
s
•N
atio
nal
an
d s
tate
hea
lth
care
ass
oci
atio
ns
The
lead
ing
spec
ialis
t in
hum
an c
apita
l con
sulti
ng
for n
ot-fo
r-pr
ofit
heal
thca
re o
rgan
izat
ions
42

Wha
t We
Do
3
•A
sse
ss a
nd
dev
elo
p t
ota
l co
mp
en
sati
on
pro
gram
s•
Lead
ersh
ip
•St
aff
•P
hys
icia
ns
•P
rovi
de
ind
ep
en
de
nt
advi
sory
se
rvic
es
to b
oar
ds
and
co
mm
itte
es
•G
ove
rnan
ce a
nd
bes
t p
ract
ices
•R
easo
nab
len
ess
op
inio
ns
•Pe
rfo
rman
ce a
pp
rais
al
•D
esi
gn o
f co
mp
en
sati
on
an
d b
en
efit
pla
ns
that
:•
Enh
ance
th
e ab
ility
to
att
ract
an
d r
etai
n q
ual
ity
tale
nt
•A
lign
lead
ersh
ip, s
taff
, an
d p
hys
icia
ns
wit
h t
he
org
aniz
atio
n’s
mis
sio
n a
nd
str
ateg
ic
pri
ori
ties
•H
elp
man
age
per
form
ance
at
all l
evel
s o
f th
e o
rgan
izat
ion
We
prov
ide
a fu
ll su
ite o
f str
ateg
ic h
uman
cap
ital
cons
ultin
g se
rvic
es to
hos
pita
ls a
nd h
ealth
sys
tem
s
43

Who
We
Serv
e
4
IHS
trate
gie
s s
erv
es o
ver
900 lead
ing
healt
hcare
org
an
izati
on
s a
cro
ss t
he c
ou
ntr
y
Hea
dqua
rter
sC
lient
Loc
atio
ns
44
Som
e of
Our
Reg
iona
l Clie
nts
5
El C
amin
o Ho
spita
l M
ount
ain
View
, CA
Was
hing
ton
Hosp
ital H
ealth
care
Sys
tem
Fr
emon
t, CA
Su
tter H
ealth
Sa
cram
ento
, CA
Scrip
ps H
ealth
Sa
n Di
ego,
CA
Adve
ntis
t Hea
lth
Rose
ville
, CA
Hunt
ingt
on M
emor
ial H
ospi
tal
Pasa
dena
, CA
Cotta
ge H
ealth
Sys
tem
Sa
nta
Barb
ara,
CA
Alam
eda
Coun
ty M
edic
al C
ente
r O
akla
nd, C
A Co
mm
unity
Hos
pita
l of t
he M
onte
rey
Peni
nsul
a M
onte
rey,
CA
Kaw
eah
Delta
Hea
lth C
are
Visa
lia, C
A Ei
senh
ower
Med
ical
Cen
ter
Ranc
ho M
irage
, CA
45

Tota
l Com
pens
atio
n R
evie
w P
roce
ss
14
46

Our
Met
hodo
logy
for T
otal
Com
pens
atio
n C
onsu
lting
15
Com
preh
ensi
ve D
ata
Col
lect
ion
Proc
ess
•Fi
nanc
ial a
nd o
rgan
izat
iona
l dat
a re
view
•S
trate
gic
and
oper
atin
g pl
ans
revi
ew•
Job
cont
ent c
alls
•In
cent
ive
plan
revi
ew•
Ben
efit
plan
revi
ew
Focu
sed
Inte
rvie
ws
&
Com
pens
atio
n Ph
iloso
phy
Dev
elop
men
t
•B
oard
inte
rvie
ws
•C
EO
inte
rvie
w•
On-
site
mee
ting
to d
iscu
ss fi
ndin
gs
•Id
entif
y pe
er g
roup
•A
naly
ze s
alar
ies,
ince
ntiv
es a
nd b
enef
its•
Com
pare
tota
l com
pens
atio
n to
pee
r gro
up
•Id
entif
y is
sues
/pro
blem
s ne
edin
g at
tent
ion
Com
petit
ive
Anal
ysis
&D
raft
Rec
omm
enda
tions
Rec
omm
enda
tion
&Fi
nal R
epor
t
•M
eet w
ith B
oard
to p
rese
nt re
port
•D
iscu
ss is
sues
/reco
mm
enda
tions
/opp
ortu
nitie
s•
Hel
p co
mpl
y w
ith b
est p
ract
ices
Ong
oing
Sup
port
•B
oard
sup
port
and
educ
atio
n•
Ann
ual u
pdat
es
Tim
ing
Proc
ess
Step
Activ
ities
Janu
ary
Janu
ary/
Febr
uary
Febr
uary
Mar
ch
As
need
ed
47

Exclusive to Healthcare. Dedicated to People. SM
EXECUTIVE TOTAL COMPENSATION AND GOVERNANCE
MSA EXECUTIVE SEARCH • MSA HR CAPITAL • PHYSICIAN SERVICES
Mr. Hopkins is a Senior Consultant at IHStrategies, specializing in Executive Total
Compensation. Mr. Hopkins works with healthcare organizations providing
executive compensation consulting services, including salary and incentive
compensation analyses, governance compliance audits, total compensation
evaluations, incentive plan design engagements, and formal reasonableness
opinions. Mr. Hopkins routinely works with boards and
compensation committees to help them comply with the
requirements for establishing a rebuttable presumption
of reasonableness, and counsel them regarding the
impact of governance reform initiatives and
regulations.
Mr. Hopkins works with a broad spectrum of healthcare organizations, including
small community hospitals, state hospital associations, quality improvement
organizations, and some of the country’s largest, most prestigious health care
systems.
Mr. Hopkins has been with IHStrategies for six years. Before joining IHStrategies,
Mr. Hopkins practiced as an attorney with a Minneapolis law firm specializing in
collections, clerked for Marshfield Clinic’s general counsel, and worked for the Blue
Cross Blue Shield of Wisconsin’s legal department. Mr. Hopkins received his J.D.
from the Marquette University Law School and his B.S.B. in management and
insurance from the Carlson School of Management at the University of Minnesota.
If you would like to contact Mr. Hopkins, call 1-800-327-9335 or email
BIO
BILL HOPKINS
TITLE:
Senior Consultant
48

Date: January 10, 2011 To: City of Alameda Health Care District, Board of Directors From: Deborah E. Stebbins, CEO Subject: 401(a) Contribution Limits A recent development surrounding my participation in the Alameda Hospital 401(a) Retirement Plan is being reported to the Board for information only. Our Human Resources Department, under guidance from our local pension and TDA Broker, has operated the plan on the assumption of making contributions for eligible employees of 6% of their wages up to the maximum wage limit published for Governmental Plans of $360,000. However, during a recent audit of our employee wages and contribution limits, it was discovered that this limit was only applicable to Governmental plans in existence before July 1, 1993. Our 401(a) Plan was started in 2002 when the District was established. Therefore, although we are treated as a governmental agency, our plan limit on wages that are eligible for contributions is $245,000. This is the maximum for all other nongovernmental organizations and corporations. I am currently the only employee impacted by the clarification of the appropriate maximum contribution. The required correction involves removing the excess contributions, plus earnings (or minus losses) thereon from my account and crediting this sum to the Alameda Hospital Retirement Plan Forfeiture Account. This forfeiture account is used to offset our future contributions to the plan. There are no adverse tax consequences due to this correction as this money is not taxable at this time and there is no action by the Board required. This is being divulged for informational purposes only. While this limit only affected my compensation, procedures have been put in place to prevent excess contributions in the future for all employees. A preliminary estimate of the total amount of the correction is between $20,000 and $24,000.
49

DATE: January 10, 2011 TO: City of Alameda Health Care District, Board of Directors FROM: Kerry Easthope, Associate Administrator SUBJECT: SB 1953 Seismic Compliance Update This memo is to serve as a summary of Alameda Hospital’s seismic compliance. I will provide a brief background on what has taken place, where we are today and what are the next planned steps. Note: Only the first six (6) pages are memo narrative. The remainder is supporting documentation and information. Introduction: The California Seismic Compliance Legislation, SB 1953, was put into place to require all acute care hospitals to ensure that the buildings where acute care services are provided will be safe in the event of a major earthquake. The legislation was first passed in 1994 and provides for hospitals to comply with the prescribed seismic standards by either retrofitting non-conforming existing buildings or replacing them with seismically compliant buildings. The legislation provides a phased in approach to compliance with incremental compliance deadlines. In addition, some legislation has been passed subsequent to SB 1953 which allows for extensions to the deadlines, if certain terms and conditions are met. To further complicate the legislation, there are two main components of seismic compliance: Structural Performance Category (SPC) and Non-Structural Performance Category (NPC), each with their own set of requirements measured on a scale from 1 to 5 for each component and compliance time frames. The higher the rating, the more seismically sound a structure is determined to be. (Attachment 1) Background: In summary, the following table shows the eight buildings which comprise Alameda Hospital, the year in which they were built and their SPC & NPC status.
50

Building Year Built NPC
Status SPC Status
1. Original Hospital 1925 1 1 2. Stephens Wing 1955 / 1967 1 1 3. West Building 1967 1 1 4. Compacter Shed 1983 2 4 5. South Wing 1983 1 3 pending testing & review 6. Emergency Room 1986 1 3 pending testing & review 7. Radiology Addition 1989 1 5 pending testing & review 8. Medical Gas Storage 1989 1 3 pending testing & review
Unless an extension is granted through existing legislative extension options, which will be discussed later, all hospital buildings need to be at least NPC 3 and SPC 2 by January 1, 2013. Furthermore, hospital buildings needed to be NPC 2 by January 1, 2002. SPC Status: The attached two letters from the Office of Statewide Health Planning & Development (OSHPD) dated January 13, 2005 (Attachment 2) and March 24, 2006 (Attachment 3), summarize the State’s findings on where each of our buildings are with regards to its SPC rating. It is important to note that additional frame joint testing and review will be required for the South Wing. It is also believed that the Emergency Room may require more testing and the Radiology Wing is still pending final review as of January 2005. This additional testing and verification by OSHPD has not yet occurred. NPC Status: The NPC 2 work which was required by January 2002 includes the following main components, primarily related to anchoring and bracing: bulk medical gas, communications systems, emergency power supply, fire alarm, emergency lights and signs in the means of egress. Although the hospital submitted information to OSHPD indicating OSHPD building projects where each of these items may have been addressed, there was correspondence from OSHPD back in 2002 – 2005, indicating that the documentation is either incomplete or does not completely address the seismic compliance requirement and that additional information and/or work is required. We are meeting with our structural engineer with Thorton Tomassetti to determine what our compliance status is with each of these and what, if any, work is still required to be NPC 2 compliant. In addition, it is required that the Original Hospital (1925), be either delicense or have NPC 2 anchorage work complete. Since the intent for many years has been to eventually delicensed this building, this work has not been done. The OSHPD letter dated April 19, 2005 (Attachment 4) addresses this matter. Furthermore, the Hospital has submitted, and received a building permit for its NPC 3 work. NPC 3 includes bracing of equipment in the laboratory, pharmacy and central / sterile supply. In addition, ceilings, pipes and ductwork must be braced in all areas as well as bracing of walls throughout the surgery area. Mechanical equipment must be
51

braced on the rooftops and in mechanical rooms and elevators also require seismic bracing. Once again, some of the NPC 1 buildings could change to NPC 2 pending our ability to provide documentation addressing all NPC 2 deficiencies. However, some additional work may need to occur in this area and is currently being discussed with our structural engineers. It is my understanding that the follow up and continuation of most seismic testing, plan development and work was interrupted for several years in 2001. The delay was primarily the result of a lack of resources to fund this work given the financial position of the hospital during this time and the need to focus on financial viability. Seismic thinking and planning was not actively discussed again until 2008 at which point, we engaged architects & engineers to help us better understand the scope of our seismic retrofit work and master planning for the January 2013 deadline as well as to understand the associated costs. We are one of the only hospitals that is planning to retrofit existing buildings versus rebuilding in order to minimize the cost of retrofit and allow us to comply with the 2013 standards. Seismic Compliance Extension Options: There are four (4) legislative extension options available to those hospitals that meet the criteria outlined for each. In summary, these options are as follows.
1. HAZUS (Extension to 2030): Key factors: proximity to a major fault line, age of buildings, number of floors, ground composition, building composition, construction specifications and attachment to non-compliant building and the need to relocate essential services. We have applied for HAZUS 10 for the Stephens Wing. At this point, additional documentation and calculations are required from our engineers. (Attachment 5) Note: Representatives from OSHPD has verbally indicated our ability to qualify for reassessment under HAZUS is unlikely due primarily to our proximity to the Hayward fault and the known liquefiable soil identified under the Stephens Wing.
2. SB1661 (Extension to 2015): The focus of this extension is to provide an additional two years for hospitals that are making serious progress towards 2013 compliance but need more time. Hospitals need to have submitted design plans deemed ready by OSHPD for review by January 1, 2009, and requires progressive status reports that must be met in order to maintain compliance with the extension (6/2009 and 6/2011). As previously mentioned, the hospital began active planning for its seismic work in 2008, but were not in a position to meet this deadline.
3. SB 306 (Extension compliance deadline to 2020 if facility meets 2030 standards rather than 2013 by that date). The focus of this extension option was for City and County owned hospitals, safety net hospitals, hospitals that serve a high
52

number of Medi-Cal and uninsured patients, hospitals that meet strict financial hardship and hospitals that if not in operation, would significantly diminish the availability or accessibility of health care services to an underserved community. Alameda Hospital applied for this extension and was denied as indicated in the OSHPD letter dated December 29, 2008 (Attachment 6).
4. SB 499: Like SB 1661, SB 499 which went into effective in February 2010, also provides for up to a 2-year extension option for hospitals that achieve compliance progression benchmarks. The first benchmark is to have SPC-2 building plans submitted to OSHPD by 6/30/10. The second benchmark will be to obtain a building permit by 1/1/2012. The legislation can provide for an extension for NPC-3 compliance to 2030 (then NPC-4 or 5 is required). In addition, the legislation requires annual seismic compliance status reporting to OSHPD beginning November 1, 2010. Lastly, the legislation allows for a new HAZUS 10 reassessment, similar to the previous HAZUS. Alameda Hospital has submitted its plans to OSHPD for structural work on the Stephens Wing as well as relocation of the Kitchen to this building by the required June 30, 2010 date. The plans are still in review and will have a number of back checks and additional data submittal requirements before plans are approved. Through this planning process, we have also obtained reasonable cost estimates for this portion of the work and that budget was submitted to the Board at the October 2010 meeting. We still need to submit plans (a separate project) to decommission the 1925 building as well. The hospital has also applied for the NPC-3 compliance extension, but this request will not be approved until all buildings are verified to be at least NPC-2. We submitted the initial annual seismic compliance status report that was due November 1, 2010, and edits are currently being made as they are reviewed by OSHPD.
Current Status: In summary, the following is the status of our seismic planning and activity.
1. We applied for an extension under SB 306 and have been denied.
2. We submitted a seismic compliance status report, as required under SB 1661 in June 2009. This report indicates that we would be compliant by 2013, with the comment that our ability to comply is heavily contingent upon our ability to obtain the financing required to pay for this unfunded mandate (Attachment 7).
3. We submitted our annual seismic compliance status report prior to November 1,
2010 as required by SB 499. OSHPD is currently reviewing these reports as they are much more comprehensive than the SB 1661 status report. We have edited our report to indicate that we would not be compliant until January 2016.
53

The report was accompanied by a letter describing the hospital’s current situation and intent and that is part of our file at OSHPD.
4. We have submitted plans for NPC 3 work and currently have a building permit
that is valid until April 2011. At that point, it will expire and will need to be re-approved.
5. We have submitted plans for our structural work in the Stephens and West Wings,
including plans to relocate the kitchen to the Stephens Wing. These plans are currently under review and back-check with OSHPD. Our architects and engineers will be responding to their comments.
a) Additional soil testing was required as part of this plan review and this has
recently been complete. Although not definitive yet, the soil testing results may indicate that the West Wing will have its rating upgraded to SPC 2. (There is a meeting with the A&E team this week to discuss).
b) We have informed the architect and engineers of our immediate challenge in obtaining the necessary financing to put this project out to bid. However, it is our intent to continue with the plan review and approval process with the goal of obtaining an approved building permit.
c) OSHPD has been delayed in reviewing any plans for two months while
engaged in the SB499 report review. OSHPD is required to report to the state legislature in February 2011 regarding the seismic status of California’s hospitals.
6. HAZUS 10 reassessment is still pending due to additional structural data to
complete the review. This may cost more money if additional testing is required to gather the needed data. We are not sure if this will affect or change our ability to be compliant given the connection to and services provided in the 1925 building.
7. We have taken steps to obtain capital financing through Cal-Mortgage. We met with representatives from Cal-Mortgage and discussed our seismic needs as well as other potential capital projects. We subsequently engaged financial consultants to prepare the necessary financial feasibility studies for this loan request. Given the current year financial performance, it is felt that we do not demonstrate the ability to assume this amount of new debt service at this time, especially for a something that does not have a return on investment such as seismic.
Next Steps: The following are the next steps to address our seismic challenges.
1. Complete the review to ascertain what is needed to achieve NPC 2 status on all buildings except the Original Hospital.
54

2. Determine what is necessary to complete testing and verification of other SPC 3 – SPC 5 buildings in order to remove contingency.
3. Complete the plan review process for the structural and kitchen relocation project currently under review with OSHPD.
4. Continue to pursue new revenue generating business ventures and/or partnerships
that will enable the hospital to have the financial stability required obtain the capital financing required to complete this work.
5. Given that we have indicated to OSHPD that we will not be compliant by January
2013, wait for the statewide status report that should be forthcoming. Given the number of other hospitals in our situation, there may be additional legislation introduced on a broader level that will provide the legislative assistance that we need.
6. Continue our dialogue with our local state legislators to discuss our situation and
actions taken to date. Ensure that we have their support; including possible introduction off special legislation, if necessary, granting an extension specifically to Alameda Hospital, do to our financial constraints.
55
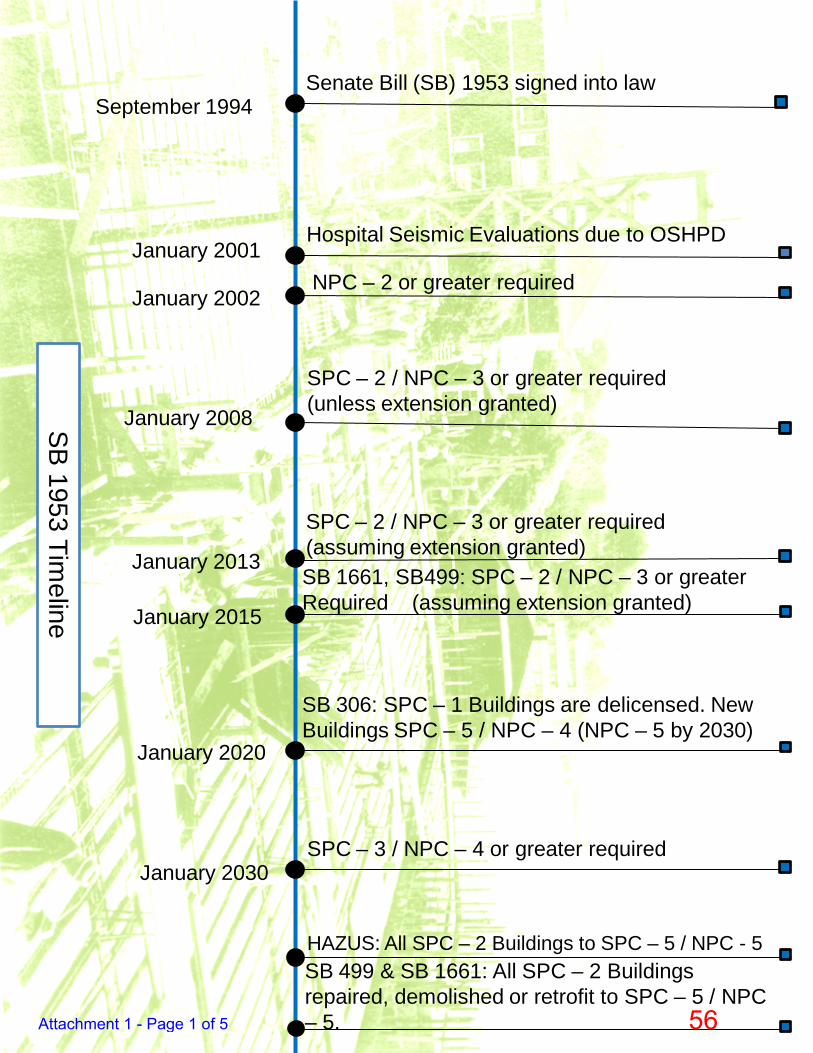
September 1994
January 2001
January 2002
January 2008
January 2013
January 2030
Senate Bill (SB) 1953 signed into law
Hospital Seismic Evaluations due to OSHPD
NPC – 2 or greater required
SPC – 2 / NPC – 3 or greater required(unless extension granted)
SPC – 2 / NPC – 3 or greater required(assuming extension granted)
SPC – 3 / NPC – 4 or greater required
HAZUS: All SPC – 2 Buildings to SPC – 5 / NPC - 5
SB 1661, SB499: SPC – 2 / NPC – 3 or greater Required (assuming extension granted)
January 2015
January 2020
SB 306: SPC – 1 Buildings are delicensed. New Buildings SPC – 5 / NPC – 4 (NPC – 5 by 2030)
SB 499 & SB 1661: All SPC – 2 Buildings repaired, demolished or retrofit to SPC – 5 / NPC – 5.
SB 1953 Timeline
Attachment 1 - Page 1 of 5 56

Attachment 1 - Page 2 of 5 57

Attachment 1 - Page 3 of 5 58

Key to the Summary of Hospital Seismic Safety RatingsApril 2001Page 1
KEY TO THE SUMMARY OF HOSPITAL SEISMICPERFORMANCE RATINGS
California state law requires hospitals to evaluate their facilities, develop plans tomeet seismic standards and ensure that their buildings are seismically sound byspecified deadlines. The state’s original seismic safety law – the Alfred E. AlquistFacility Seismic Safety Act of 1973 (Alquist Act) – was passed in 1973.Significant amendments to the original law were passed in 1994.
Under these latest amendments to the Alquist Act, California’s general acutecare hospitals were required by law to evaluate and rate their hospital buildingsfor seismic performance and to submit these ratings to the California Office ofStatewide Health Planning and Development (OHSPD) no later than January 1,2001.
Hospitals evaluated and rated their buildings according to how they wouldperform in a strong earthquake. The ratings are defined as follows:
Structural ratings: These are ratings of the actual building’s structure (StructuralPerformance Category—SPC)
SPC-0 The hospital evaluated this building but did not provide any rating in itsreport to OSHPD.
SPC-1 These buildings pose a significant risk of collapse and a danger to thepublic after a strong earthquake. These buildings must be retrofitted,replaced or removed from acute care service by January 1, 2008.
SPC-2 These are buildings in compliance with the pre-1973 California BuildingStandards Code or other applicable standards, but are not in compliancewith the structural provisions of the Alquist Hospital Facilities SeismicSafety Act. These buildings do not significantly jeopardize life, but maynot be repairable or functional following strong ground motion. Thesebuildings must be brought into compliance with the Alquist Act by January1, 2030 or be removed from acute care service.
SPC-3 These buildings are in compliance with the structural provisions of theAlquist Hospital Facilities Seismic Safety Act. In a strong earthquake, theymay experience structural damage that does not significantly jeopardizelife, but may not be repairable or functional following strong groundmotion. Buildings in this category will have been constructed orreconstructed under a building permit obtained through OSHPD. They canbe used to 2030 and beyond.
Attachment 1 - Page 4 of 5 59

Key to the Summary of Hospital Seismic Safety RatingsApril 2001Page 2
SPC-4 These are buildings in compliance with the structural provisions of theAlquist Hospital Facilities Seismic Safety Act that may experiencestructural damage which could inhibit the building’s availability following astrong earthquake. Buildings in this category will have been constructedor reconstructed under a building permit obtained through OSHPD. Theymay be used to 2030 and beyond.
SPC-5 These buildings are in compliance with the structural provisions of theAlquist Hospital Facilities Seismic Safety Act, and are reasonably capableof providing services to the public following strong ground motion.Buildings in this category will have been constructed or reconstructedunder a building permit obtained through OSHPD. They may be usedwithout restriction to 2030 and beyond.
Non-structural ratings. These ratings cover a building’s non-structuralsystems including communications, emergency power supplies, bulkmedical gas, fire alarms and emergency lighting. Hospitals must anchorand brace these systems by January 1, 2002.
NPC-0 The hospital evaluated the building’s non-structural components but didnot report any rating.
NPC-1 In these buildings, the basic systems essential to life safety and patientcare are inadequately anchored to resist earthquake forces. Hospitalsmust brace the communications, emergency power, bulk medical gas andfire alarm systems in these buildings by January 1, 2002.
NPC-2 In these buildings, essential systems vital to the safe evacuation of thebuilding are adequately braced. The building is expected to suffersignificant nonstructural damage in a strong earthquake.
NPC-3 In these buildings, nonstructural systems are adequately braced in criticalareas of the hospital. If the building structure is not badly damaged, thehospital should be able to provide basic emergency medical carefollowing the earthquake.
NPC-4 In these buildings, the contents are braced in accordance with currentcode. If the building structure is not badly damaged, the hospital buildingshould be able to function, although interruption of the municipal watersupply or sewer system may impede operations.
NPC-5 These buildings meet all the above criteria and have water andwastewater holding tanks—sufficient for 72 hours of emergencyoperations—integrated into the plumbing systems. They also contain anon-site emergency system and are able to provide radiological serviceand an onsite fuel supply for 72 hours of acute care operation.
Attachment 1 - Page 5 of 5 60

Attachment 2 - Page 1 of 1 61

Attachment 3 - Page 1 of 2 62

Attachment 3 - Page 2 of 2 63

Attachment 4 - 1 of 2 64

Attachment 4 - 2 of 2 65

Attachment 5 - Page 1 of 2 66

Attachment 5 - Page 2 of 2 67

Attachment 6 - Page 1 of 3 68

Attachment 6 - Page 2 of 3 69

Attachment 6 - Page 3 of 3 70

Attachment 7 - Page 1 of 2 71

Attachment 7 - Page 2 of 2 72

1
DATE: January 10, 2011 TO: City of Alameda Health Care District, Board of Directors FROM: Kerry Easthope, Associate Administrator SUBJECT: Marina Village Space Planning As a follow up to the presentation and discussion at the December 13, 2010 Board meeting regarding our recommendation to enter into a lease agreement for medical office space at 815 Atlantic Avenue in Alameda, it was recognized that more information needs to be presented with regards to our plans for that building. Background: An important aspect of the hospital’s strategic plan is growth and the development of new programs and services that will allow us to better serve the medical needs of those in our community while providing a positive contribution to the hospitals financial strength. A second aspect of our strategic plan is to develop a more comprehensive medical staff base that will support the primary care physician needs in the community but also support the growth and medical strength of the acute care hospital. As we look at new programs and services, especially outpatient programs, adequate medical office / clinical space have been an ongoing challenge. In addition, the future need for better and additional physician office space has been identified. The hospital currently leases approximately 8,400 sq. ft. of space at Alameda Towne Center. In that space, we have 12 physicians practicing, many of which are part of the hospitals 1206(b) clinic. We also operate a lab draw station at that location to make it more accessible to patients who require this diagnostic testing. The lease at Alameda Towne Center has a term date of April 30, 2012, with two 1-year renewal options at the hospital’s discretion. The landlord has not been willing to provide extension options beyond that date and there have been discussion of possible alternative uses for this building space in the long term. Space within the hospital available for outpatient services is very limited and very costly to renovate and bring up to current OSHPD building code if we were to convert space for alternative uses. Utilizing our current licensed inpatient space for inpatient services is a better and more cost effective use of these spaces once suitable services are identified.
73

2
Given the aforementioned, management has been directed to pursue other potential space within the district boundaries that can be utilized to serve the needs of our local physicians as well as enhance and/or expand our outpatient service capabilities. Discussion: There is very limited functional space available within Alameda for physician office and clinical services use. However, we have identified a building located at 815 Atlantic Avenue, part of the Marina Village business park, that would be suitable to help us accomplish our strategic plans. The entire building is just less than 25,000 sq. ft. It is the first building you come to when accessing the business park off of Constitution Way or Webster Street and is therefore very accessible, not only to those residents living on the West end of Alameda, but to patients who would utilize the services provided at this location who live in Oakland. Initial Leased Space (Suite 100): The initial recommendation, presented last board meeting, was to enter into a lease for 10,612 sq. ft. We would have expansion rights for the remaining empty suite (Suite 105) which is 11,640 sq. ft., as well as two other smaller suites of 1,122 and 1,492 sq. ft. respectively, which are currently under lease with other tenants. The plan for the initial leased space (Suite 100) is to open a Wound Care Center as previously discussed. This program would be operated in conjunction with Accelecare Wound Centers Inc., who is experienced in managing this type of service. Our preliminary schematic plan indicates that the Wound Care program would take about 3,800 sq. ft. of direct clinical space plus share up to a 400 sq. ft. waiting room area. We are prepared to move forward with implementation of this program once our lease agreement is finalized and we secure financing for the required tenant improvements. The remaining space in Suite 100 (approx 6,400 sq. ft.) would be used for Rehabilitation Services (outpatient physical therapy, speech therapy, occupational therapy, sports medicine, and potentially cardio fit services). Our current rehab services space here at the hospital is only about 1,400 sq. ft. and has limited treatment space. In addition, because of the lack of space, we do not have the desired equipment, machines and apparatuses that would provide for improved therapy and recovery for a broader spectrum of patients. There is currently a consistent back-log to schedule an initial assessment for outpatient therapy, do in part, to our limited clinical space. We are currently engaged in discussions with a contract rehabilitation services management company who would assist us in designing, implementing and managing expanded service. We will explore having this management company provide upfront capital to assist with the build out of the center and acquisition of equipment.
74

3
Expanding and enhancing our outpatient rehabilitation services program is particularly important as we become a Stroke Certified hospital. Post discharge, many of these patients will require extensive outpatient therapy for full recovery. In addition, there is an ongoing initiative to increase our orthopedic surgery practice here at Alameda. A comprehensive and well managed rehabilitation service is very important to this patient population as well. Expansion Space: Within the first year after executing the initial lease, it would be our goal to exercise our expansion right into Suite 105. This space would be designed and built out for physician office space and would allow us to vacate the space at Alameda Towne Center and even relocate some of the physicians currently located in the 1925 building. In addition to physician office space, the plan would be to have a Lab draw station, basic radiology and ultrasound. This would provide a comprehensive one-stop for primary care and diagnostic services. Once we are able to exercise expansion rights into the smaller two suites that are currently occupied, we are contemplating adding an urgent care or possibly expanding and/or relocating other hospital based outpatient services to this building. Summary: In order to achieve our strategic plans of growth, physician recruitment and enhancing the types and quality of services that we provide to the community, securing the physical space where these activities can occur is an important first step. Given the terms and conditions that we have negotiated and that will become part of our long term lease, we will have space not only to implement new services and expand existing services in the immediate future, but we will have the necessary space to meet our longer term expansion / relocation needs. Furthermore, the location at Marina Village is very attractive because of its location on the west end of Alameda. Our ability to have a primary care and medical presence on the west end of Alameda will be of benefit to the residents who live or work in that area, but will also service the Oakland / China Town population. We feel that this is a good opportunity and will accomplish many of our short and long term objectives.
75

Alameda HospitalPrimary Stroke CenterCertification Update
Presented By:
Deborah E. Stebbins, CEO
January 10, 2011

Every 45 seconds someone has a stroke.Overall in Alameda County: Stroke is the 3rd Leading Cause of Death

Primary Stroke CenterDemographic Context – City of Alameda *
2nd oldest median age in Alameda County: 40.8 years (Countyaverage = 37.0 years)
27.5 % of population over 55 years
2.4% of population over 85 years (patients > 85 havedramatically higher stroke related mortality)
650 residents of skilled nursing facilities in City of Alameda
Age-adjusted stroke mortality in City of Alameda is 38.7%,lower than County-wide average of 40.7%
Stroke Mortality Rates for all racial and ethnic groups in theCounty have declined in recent years
* Alameda County Public Health Department: Health of Alameda County City and Places, 2010

11 Elements of an Primary Stroke Center*1. Acute stroke team available 24 hours a day2. Written care protocols to ensure rapid recognition, diagnosis,
and treatment3. Emergency medical services integrated into the primary stroke
team operations4. Emergency Department integrated into the primary stroke team5. Stroke unit6. Neurosurgical services available within 2 hours7. Commitment from the institution8. Neuroimaging performed and interpreted within 45 minutes of
patient arrival9. Laboratory services with rapid turn around of tests10. Quality improvement program including a database or registry11. Continuing education program
*Brain Attack Coalition

A Stroke Center… Improves outcomes
• Optimizes chance of recovery
• Minimizes complications
• Decreases length of hospital stay
Provides ongoing monitoring
• Neurologic deterioration (4-8% seizure)
• Cardiac dysrhythmias (Cardiac etiology in 14% of post stroke deaths)
• Decreases incidence of complications such as PE, pneumonia (30%of stroke deaths)
Facilitates thorough, consistent diagnostic work-up
Ensures early rehabilitation, patient and family education
Promotes optimal recovery of function

Letter from County EMSInterim Medical DirectorNovember 25, 2010
“ Alameda Hospital has both verbally and in written fashion
committed to work toward accreditation status as a JointCommission Primary Stroke Center. We recognize the significantprogress made thus far, and believe that many essential buildingblocks for that accreditation are in process at the facility. We willwelcome Alameda Hospital’s inclusion into the Alameda CountyStroke Systems once the requirements are met. As we did withEden, we will be willing to designate Alameda Hospital as a StrokeCenter for our EMS system when the Joint Commission hasapproved all required documentation and has scheduled the facilityfor a site visit. “
Joe Barger, MD
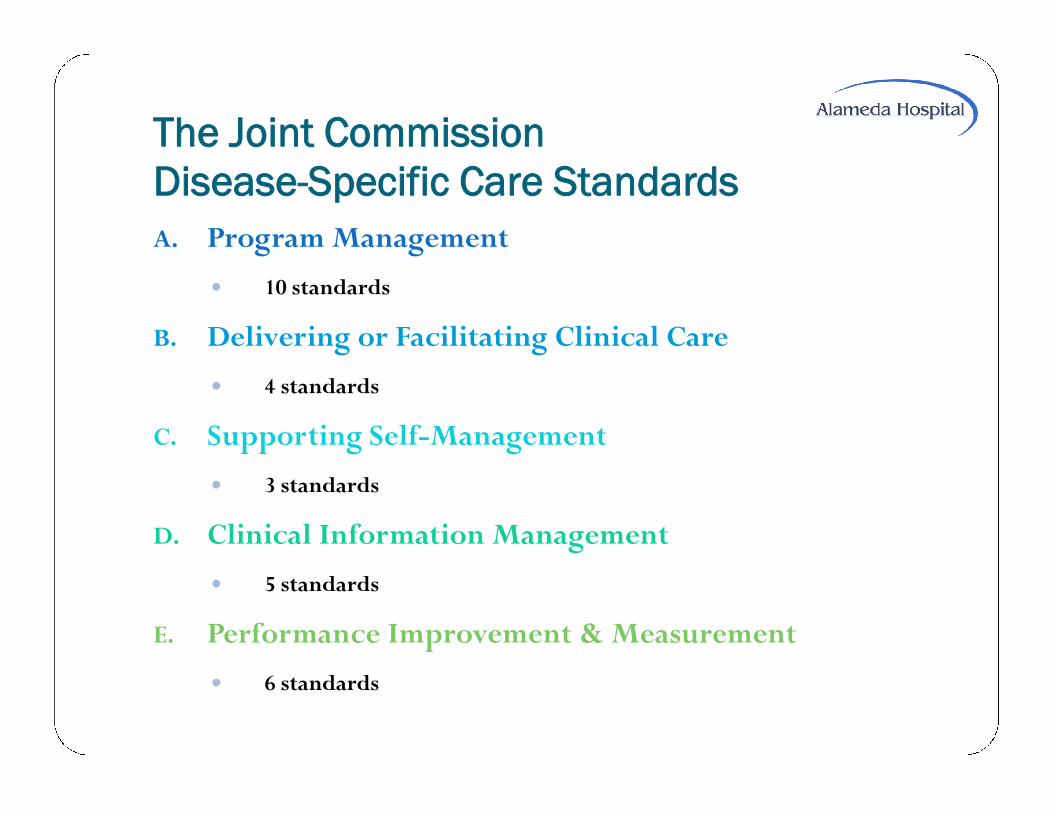
The Joint CommissionDisease-Specific Care StandardsA. Program Management
10 standards
B. Delivering or Facilitating Clinical Care
4 standards
C. Supporting Self-Management
3 standards
D. Clinical Information Management
5 standards
E. Performance Improvement & Measurement
6 standards

Disease-Specific Care StandardsA. Program Management
Leadership Roles
o Delineated Director & Coordinator
o Defined roles, relationships, & responsibilities
o Performance improvement plan formalized & accepted, 2-4 wks
o Expectations for performance improvement finalized, 2-4 wks
Collaborative Design-Stroke Committee formed & active
o Complete
Target population & needs identified
o Complete
Program follows a code of ethics
o Complete
Program complies with applicable laws and regulations
o Complete

Disease-Specific Care StandardsProgram Management (continued)
Current Reference & Patient Resource Materials
o Reference materials easily accessible—printing approx 4 wks
o Reference materials authoritative & current
Facilities Are Safe & Physically Available
o Complete
Scope, Level of Care,Treatment, & Services Communicated toParticipants
o 4 of 5 standards complete
o Information on access, treatment & services—website, printedmaterial, educational programs in process—approx. 1-2 months
Scope & Level of Care Same for All Participants
o Complete
Eligible Patients Have Access to the Program
o EMS County approval to change EMS routing protocols uponapproval byTJC of all documentation and site visit scheduled

Disease-Specific Care Standards
B. Delivering or Facilitating Clinical Care
Practitioners are Qualified and Competent
o StrokeTeam 8-hour Education—January 2011
o Nursing Education—January 2011
o Licensing andVerification for Staff Complete
o Mechanisms toVerify Licensing, Competence, etc. in Place
o Orientation Program in Place
Clinical Practice Guidelines Are Established, Reviewed, Up-to-Date,Relevant with Evidence-Based Practice
o Complete
Program is Designed to Meet the Participant’s Needs
o Complete
Program Manages and Coordinates ConditionsThat May Occur inConjunction with Stroke
o Complete
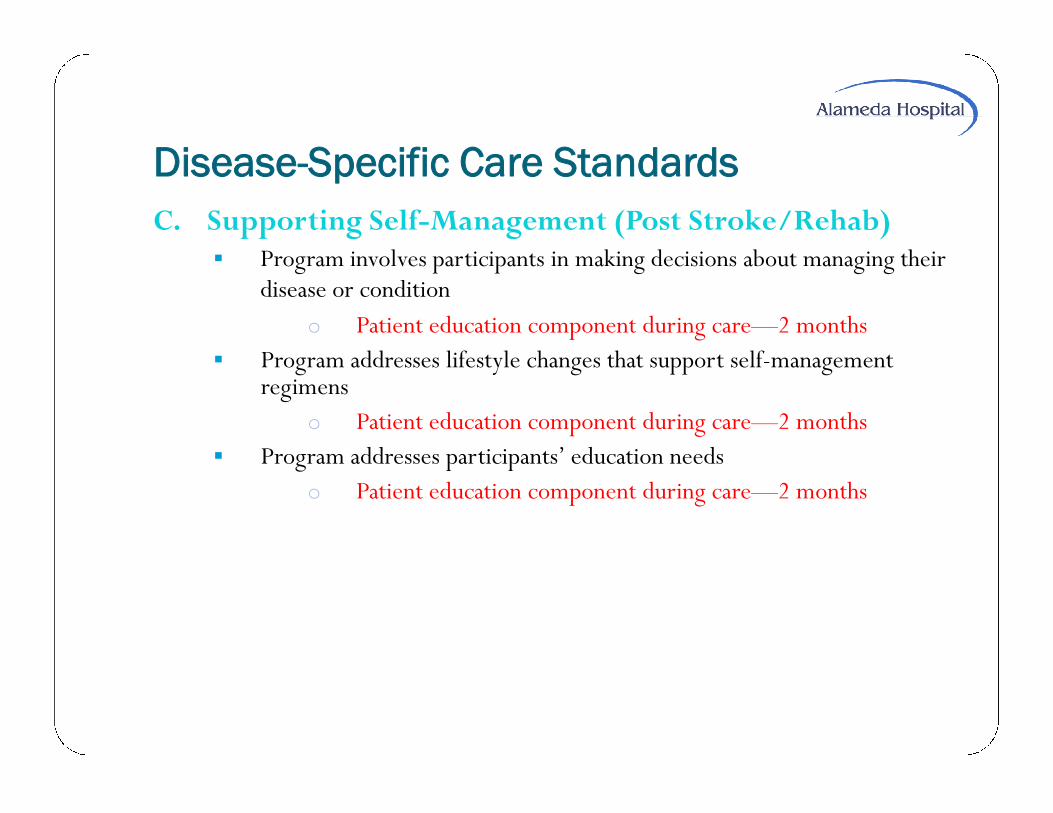
Disease-Specific Care Standards
C. Supporting Self-Management (Post Stroke/Rehab) Program involves participants in making decisions about managing their
disease or condition
o Patient education component during care—2 months
Program addresses lifestyle changes that support self-managementregimens
o Patient education component during care—2 months
Program addresses participants’ education needs
o Patient education component during care—2 months

Disease-Specific Care StandardsD. Clinical Information Management
Participant information is confidential and secure
o Patient records per Alameda Hospital protocol exist
o Data collection & use explained to participant, a double-check onexisting protocol required, 1-2 wks
o All other requirements per AH existing protocols
Information Management Processes meet the programs internal & externalinformation needs
o Record retention & retrieval per AH current protocol
o Use of aggregate data to support decisions, operations, PI, andparticipant care—get with the guidelines participation—4 months ofdata required—evaluation to occur on 1-18-2011
Participant information is gathered from a variety of sources
o Per existing AH policies for charting
Program shares information with relevant practitioner across the continuum of care
o Per existing AH policies for HIM
Program initiates, maintains, and makes accessible a health or medical record forevery participant
o Record contents and requirements are per AH existing protocol

Disease-Specific Care Standards
E. Performance Measurement Program has an Organized, Comprehensive Approach to Performance
Improvemento Per Existing AH Policies for PIo Performance Improvement Plan Approval—2-4 wks
Program Uses Measurement Data to Evaluate Process and Outcomeso Participation with GetWith The Guidelines-Existso Data Collection Ongoingo Measurement and Analysis Education-1/18/2011o Use of Data to Improve Processes-Begins 1/18/2011
Program Maintains Data Quality & Integrityo Per Existing AH Performance Improvement Requirements
and GetWithThe Guidelines Protocols and Practices for DataCollection

Disease-Specific Care StandardsPerformance Measurement (cont)
Process for identifying, reporting, managing, and tracking sentinelevents is defined and implemented
o Per existing AH Sentinel Event Reporting Policy
Variance from the Clinical Practice Guidelines is collected and analyzedto improve care
o Pending education on use of data collected in the GWTGProgram—1/18/2011
Program evaluates participant perception of the quality of care
o To be developed by StrokeTeam—February 2011

Important Dates to Certification January 10th – Meeting w/Eden Hospital Stroke Staff to review status
January 18th – Stroke team meeting w/GWTG representative to reviewcertification, plan a mock survey, and learn how to use data entered intothe program
Week of January 17th – Bi-weekly meetings of Stroke Team untilcertification received
January 18th – Data collection completed
February 2011– Staff education in ECC both live & online self-study
February 2011–Physician education in ECC both live & online self-study
February 1st – Formal application filed withThe Joint Commission

Important Dates – Community Education January 4 – “Be Stroke Smart”Web page posted on the Alameda Hospital site.
Information about signs and symptoms, risk factors, upcoming comingcommunity events is provided.
January 21– Monthly Community Blood Pressure Screening will continue thisyear. This is offered the third Friday of every month from 10 a.m. – 12 noon.
January 28 – Free Community Stroke Risk Screenings. Appointmentsrequired. Basic screening will include: BP, body mass index, blood glucose,total cholesterol, quick look EKG for arrhythmias, personal health educationabout risk factors and signs and symptoms of stroke. High risk individuals:vascular (carotid ultrasound) studies
January 28, 1 – 4 p.m.
February 24, 8:30 – 11:30 a.m.
March 25, 1 – 4 p.m.
April 28, 8:30 am. – 11:30 a.m.
May 20, 2 – 5 p.m.
June 30, 8:30 a.m. – 11:30 a.m.

Important Dates – Community Education
Community Presentations on Stroke presented by Irene Pakel,RN, Clinical Educator:
Mastick Senior Center – February 7 and 28.
Will schedule similar presentations with Cardinal Point,Waters Edge, and other community groups.
Ongoing education for visitors and families of patients aboutrecognizing signs and symptoms of stroke.
City of Alameda Health Care District
Presented ByKerry J. Easthope, Associate Administrator

Legislation that requires California hospitalsto retrofit their facilities to make them safe inthe event of a major earthquake (7.0 orgreater).
Two Categories: Structural PerformanceCategory (SPC) and Non-StructuralPerformance Category (NPC).

Sep
tem
ber1
994
Janu
ary
2001
Janu
ary
2002
Janu
ary
2008
Janu
ary
2013
Janu
ary
2030
Sen
ate
Bill
(SB
)195
3si
gned
into
law
Hos
pita
lSei
smic
Eva
luat
ions
due
toO
SH
PD
NP
C–
2or
grea
terr
equi
red
SP
C–
2/N
PC
–3
orgr
eate
rreq
uire
d(u
nles
sex
tens
ion
gran
ted)
SP
C–
2/N
PC
–3
orgr
eate
rreq
uire
d(a
ssum
ing
exte
nsio
ngr
ante
d)
SP
C–
3/N
PC
–4
orgr
eate
rreq
uire
d
HA
ZUS
:All
SP
C–
2B
uild
ings
toS
PC
–5
/NP
C-5
SB
1661
,SB
499:
SP
C–
2/N
PC
–3
orgr
eate
rR
equi
red
(ass
umin
gex
tens
ion
gran
ted)
Janu
ary
2015
Janu
ary
2020
SB
306:
SP
C–
1B
uild
ings
are
delic
ense
d.N
ewB
uild
ings
SP
C–
5/N
PC
–4
(NP
C–
5by
2030
)
SB
499
&S
B16
61:A
llS
PC
–2
Bui
ldin
gsre
paire
d,de
mol
ishe
dor
retro
fitto
SP
C–
5/N
PC
–5.
SB 1953 Timeline

Building 01, Original Hospital: SPC 1
Building 02, Stephens Wing: SPC 1
Building 03, West Wing: SPC 1 (Liquefaction)
Building 04, South Wing: SPC 3*
Building 05, Radiology: SPC 5*
Building 06, Medical Gas Storage: SPC 3*
Building 07, Emergency Room: SPC 3*
Building 08, Compactor Shed: SPC 4
* = Additional joint testing required & verification of reported rating by theOffice of Statewide Healthcare Planning & Development (OSHPD).

The hospital is currently NPC-1 Alameda requested, as part of its 1/2008 to 1/2013 extension
application that NPC upgrades (NPC-1 to NPC-3), would occurby 2013. This was submitted (6/2004) and approved (11/2004)
The 1925 building will may need to be decommissionedcomplete NPC-2 anchorage requirements.
Provide documented evidence of compliance to OSHPD thatother NPC-2 issues have been addressed or complete work asrequired.
Key elements for NPC-2 include: bracing & anchoring of: bulkmedical gas, communication systems, emergency powersupply, fire alarms, emergency lights and signs in the means ofegress.

The hospital has submitted plans and received apermit for NPC-3 work in April 2010.
▪ One year to commence work or permit must be renewed.
▪ Key Elements on NPC – 3: bracing & anchoring of:laboratory equipment, pharmacy & central / sterile supply,ceilings, pipes & ductwork and bracing of walls throughoutsurgery area. Anchoring mechanical equipment on roof &mechanical rooms. Elevators.
Status of Alameda HospitalNPC (Non-structural Performance Categories)

Decommission 1925 building and remove all “required” services (SPC – 1). Administration Dietary Medical Records (HIM) Morgue
1925 building then falls under city building jurisdiction (not OSHPD) and wouldrequire some upgrades based upon any change of use. Met with Alameda city building department, to discuss plans
Complete OSHPD verification for SPC 3 – 5 buildings. Stephens & West Wings (SPC – 1)
Liquefaction (footings and slab on grade) Exterior wall structure Building composition Age of buildings Bridge removal
All of the hospital’s buildings will require NPC work (bracing and anchorage asdiscussed) Mechanical, surgery walls, equipment, piping, bulk oxygen, etc.
Stephens and West Wings will NOT meet 2030 standards
SPC-2 work: $9.4 million (October 2010)
NPC-3 work: $.5 million (estimate 2010)
NPC-2 work: Will need a cost estimate once extent of compliance and remaining work isdetermined.
Decommission 1925 Building: $.4 million (citybuilding jurisdiction)
This work would allow the Stephens and West Wingsto operate until 2030, at which point they wouldneed to be replaced as part of a larger buildingMaster Plan

HAZUS SB 1661 SB 306 SB 499

Focus of this extension option Facilities of fairly good construction and composition that are on solid soil and
not in proximity to a major fault line. Key Factors: Proximity to major fault line Age of buildings Number of floors Ground composition (for us liquefaction concern) Building composition & construction type Need to deal with relocation of key services in 1925 building.
Alameda: The hospital has applied for HAZUS 10. Additionaldocumentation and calculations may be required from engineers. OSHPD has verbally indicated that our ability to qualify for reassessment is
unlikely and that some of the work provided for in our current structural planswould improve our likelihood a successful reassessment.
List of facilities requesting HAZUS 10 re-assessment in board packet.

Focus of this Extension Option: To provide an additional two years for hospitals that are
making serious progress towards 2013 compliance butneed more time.
1/1/2009: the hospital must submit design plans deemedready by OSHPD for review.
There are progressive status reporting requirements thatmust be met in order to maintain compliant with thisextension. (6/2009, 6/2011)
Alameda began active planning for seismic in 2008,but was not in a position to meet this deadline.

Focus of this extension option:
City and County owned hospitals Safety net hospitals Hospitals that serve high numbers of Medi-Cal and uninsured. Hospitals that meet strict financial hardship criteria Hospitals that if not in operation, would significantly diminish the availability
or accessibility of health care services to an underserved community.
1/1/2009: Required financial information to be submitted to OSHPDalong with declaration that SB 306 conditions are met.
1/1/2010: Required facility master plan submitted to OSHPD.
2030 seismic standards to be met by 2020
Alameda applied for this extension and was denied (letter & relatedmaterial included in board packet).

New Legislation (February 2010)
Revised HAZUS reassessment option. NPC-3 extension option. Alameda applied,
but will not be reviewed/approved, until allbuildings are verified NPC-2.
Provides for two year extension options forSPC work, given benchmarks are achieved(similar to SB 1661).

SPC-2 plans to be submitted to OSHPD by 6/30/10(Alameda has complied with this).
▪ Must obtain building permit by 1/1/2012
▪ Be making steady progress towards completion.
Annual seismic compliance status report updatesfiled to OSHPD, beginning 11/1/2010
Alameda has submitted its report, indicating acompliance date of 1/1/2016.

We applied for SB 306 and were denied.
Submitted compliance status reports as required under SB 1661 andSB 499. (SB 499 indicated a delayed compliance date of 1/1/2016).
Have approved NPC-3 plans, expire April 2011.
Have submitted structural plans for Stephens and West Wing,including relocation of Kitchen – in the review process with OSHPD
Have performed additional soil testing as required. Pendingapproved plans for additional materials testing.
HAZUS 10 reassessment applied for and in process.
Taken steps to obtain capital financing through Cal-Mortgage.

Complete review to ascertain remaining NPC-2 work & compliance.
Meet with OSHPD to determine what is necessary to completeverification of SPC-3 – SPC 5 buildings.
Complete plan review process for structural and kitchen relocationprojects currently under review with OSHPD.
Continue to pursue new revenue opportunities and/or partnerships tofacilitate our ability to secure the necessary capital financing for theseprojects.
Understand the state of “California seismic compliance” followingsummary of SB 499 report to the state legislature.
Continue dialogue with local state legislatures do discuss our situationand possible Alameda Hospital specific extension legislation.