radiological evaluation & classification in pelvic · pdf file„complex“ pelvic...
TRANSCRIPT
1/21/2013
1
Hakan Kınık M.D.
Professor of Orthopaedics & Traumatology
Ankara University Medical School, Turkey
RADIOLOGICAL EVALUATION &
CLASSIFICATION IN PELVIC
FRACTURES
Disclosures
No conflicts of interest
Pelvis is a ring: % 96.8 post lesion (Scheyerer MJ 2012)

1/21/2013
2
Pelvic Injuries
AP pelvic radiogram is diagnostic in 90% of patients
AP Pelvic Radiogram
• Anterior pelvic lesions
• Associated acetabular
fracture
• Posterior pelvic lesions
• Deformities
• rotational
• vertical
S2
Gap < 5 mm
2-4 mm

1/21/2013
3
• Promontorium should overlap ant border of S1
• Posterior displacement
• Rotational deformities
• Subtle SI joint injuries
• Sacral ala
Inlet View
Outlet View
• Upper border of pubic symphysis should be on the level of S2
body
• Vertical displacement
• Sacral foramens
• Flexion deformities
Outlet View

1/21/2013
4
Computerized Tomography
• More detailed information
from posterior lesions
• Sacral foramina
• Subtle sacral impactions
• Rotation of hemipelvis,
comminution
• Associated lesions
Computerized Tomography
Radiological Instability
Criteria

1/21/2013
5
Radiological Instability Criteria
• Posterior displacement > 5 mm
Radiological Instability Criteria
• Vertical displacement > 5 mm
• Displacement
instead of impaction
in posterior pelvis
Radiological
Instability
Criteria

1/21/2013
6
Radiological Instability Criteria
• Symphyseal diastasis > 2.5 cm
Radiological Instability Criteria
• Avulsion fxs:
• L5 transverse
process
• Ischiadic spine
• Lateral border of
sacrum
Attention !
• Stationary pelvic radiograms do not
always reflect true pathology
• All apparantly stable patients should
get EUA

1/21/2013
7
Floroscopic
Imaging
Classification

1/21/2013
8
Young & Burgess Classification
LATERAL COMPRESSION
ANTEROPOSTERIOR
COMPRESSION
VERTICAL SHEAR
COMBINED
MECHANISM
Young & Burgess Classification
• Mechanism of injury
• Severity of the injury
• Associated injuries
• Hemodynamic instability
• Mechanical instability
Lateral Compression Injury
• Internal rotation
• Anterior SI, SS & ST ligaments shorten, but not torn
• Posterior neurovascular injury seldom
• Pathognmonic: Transverse pubic rami fx (inlet)
• Fx:unilateral, contrlateral or bilateral
• If bilateral, one set of rami will always have a transverse fx pattern

1/21/2013
9
• Most common LC
type
• Transverse rami fxs +
sacral impaction
• Mostly mechanically
and hemodynamically
stable
Lateral Compression Type I Injury
Lateral Compression Type I Injury
Lateral Compression Type II Injury
• Posterior iliac wing fx
• Fx line may go into SI joint (crescent fx)
• Mechanically unstable
• Posttraumatic arthritis risk (crescent)
• Vascular injury 8%

1/21/2013
10
Lateral Compression Type II Injury
Lateral Compression Type II Injury
• Day Classification of
Crescent Fxs:
– Type I: Fx enters ant
1/3 of SI joint
– Type II: Fx enters
middle 1/3
– Type III:Fx enters post
1/3
Crescent fracture-dislocation of the sacroiliac joint: a functional classification.
Day AC, Kinmont C, Bircher MD, Kumar S. J Bone Joint Surg Br. 2007 May;89(5):651-8.
Lateral Compression Type III Injury
• Rolled – over pelvis
(wind swept)
• LC on trauma side APC on
the other side
• Neurovascular injury: 23%

1/21/2013
11
>2-4 mm
AP Compression Injury
• External rotation force
• Neurovascular structures stretched
• Symphyseal diastasis or vertical rami fx (inlet)
AP Compression Type I
• Symphyseal diastasis < 2 cm
• Min widening in ant SI joint
• Ligaments are stretched, but
not torn, no ER instability

1/21/2013
12
• Symphyseal diastasis >2.5 cm,
also posterior diastasis
• Ant SI, ST & SS ligaments are
torn, post SI lig intact
• SS or lateral sacral border
avulsion in inlet view
• Neurovascular stretch
• Vascular injury 10 %
AP Compression Type II
AP Compression Type III
• All ligaments are torn
• No superior displacement in initial film
• Severe blood loss
• Pelvic vascular injury 22%
• Visceral injury common
• Laparatomy: 20%
• Mortality: 20%
• All ligaments are torn with
vertical load (internal
hemipelvectomy)
• Superior displacement
(outlet view) & posterior
displacement (inlet view)
• Associated injuries common
• Pelvic vascular injury 10%
Vertical Shear Injury

1/21/2013
13
• Different plane forces
• LC + VS most common
Combined Injury
Thank You
Das Saarland
www.unfallchirurgie-homburg.de
T. Pohlemann
Klinik für Unfall-, Hand und Wiederherstellungschirurgie
Universitätskliniken des Saarlandes,
Homburg/Saar
SICOT presents Pelvic Fractures
Damage Control after
Pelvic Fractures in
Polytrauma
Das Saarland
www.unfallchirurgie-homburg.de
„Polytrauma Management“?
Primary Emergency Room
treatment is only one,
but essential part of a
„chain of resucitation,
treatment and
rehabilitation“! Mutschler et al. 2002, Radiologe 42: 506-514
Das Saarland
www.unfallchirurgie-homburg.de
Surgical strategy?
Patient stable:
Early Total Care
Damage Control Surgery
Patient unstable:

Das Saarland
www.unfallchirurgie-homburg.de
What is special in polytrauma patients with
severe, concomitant pelvic injuries?
•Letality up to 70%!
•No surgical control of
•retroperitoneal haematomas!
•Patients in extremis!
Das Saarland
www.unfallchirurgie-homburg.de
Pelvic Classification:
AO/OTA 1996: Combination MECHANISMUS &RESID. STAB
A B C
50-70% 15-30% 10-20%
AG Becken I (n= 1722) & AG Becken Ii (n= 2550)& AG Becken III (n=1990) &
MHH-Unfallchirurgie 1972-1999 (n=2576)
Incidence:
appr.8900 patients!
Das Saarland
www.unfallchirurgie-homburg.de
=
≠
Typ C Typ C
The Need For Clear Definitions!
Pelvic Classification:

Das Saarland
www.unfallchirurgie-homburg.de
„plain“ oder „uncomplicated“ pelvic injury
peripelvic soft tissue injury neclectable
Goal: Osteoligamentous Reconstruction
Present Definitions:
Das Saarland
www.unfallchirurgie-homburg.de
„Complex“ Pelvic Injury
Significant peripelvic soft tissue injury
(urogenital, holovisceral, muscle, nervs/vessels)
Exsanguination, Shock
peripelvic
soft tissues
unstable circulation (blood loss > 2000 ml)
hemipelvectomy
(neurovasc. dissoziation)
Present Definitions:
Das Saarland
www.unfallchirurgie-homburg.de
AG Becken I DGU & AO (1991-1993, 10 Zentren, n =1722 )
Complex trauma
„all“
No
Complex trauma 0 10 20 30 40 50 60 70 80 90 100
Hemipelvektomy
Complex trauma
„unstable““
Frequency
Letality
Pelvic injuries: frequency vs. lethality
20 40 60 80 100%

Das Saarland
www.unfallchirurgie-homburg.de
Treatment options: literature
„self tamponade“ effective
MAST effective, compl.
pelvic girdle, binders positiv
ligature Aa. iliacae effective
pass. aortal occlusion short term effect
angiography effective
mech. stab. + tamponade effective
definitive ORIF effective
Das Saarland
www.unfallchirurgie-homburg.de
Interpretation of literature: clear definitions missing!
methods? management?
2000ml?
150 ml/min?
Blood subst.
Lab-tests?
Autotamponade?
MAST
Stabilization?
Embolization?
Tamponade?
Ligature?
Severety of heamorrh.?
Timing?
„Protocol“?
clear criteria for inclusion
simple decisions
reproducable, universal treatment
Das Saarland
www.unfallchirurgie-homburg.de
Inclusion criteria:
„Life threatening pelvic injury
present/non exclusable “
MHH Unfallchirurgie 1972-95 n=2002 cases
Beckengruppe DGU/AO I 91-93 n=1722 cases
Beckengruppe DGU/AO II n=2500 cases
Frequency ?
ca.2%
Pelvic fractures in Germany : ca. 20.000 p.a ca.400 p.a
clinically unstable pelvis
primary Hb below 8 g/%

Das Saarland
www.unfallchirurgie-homburg.de
Anatomical basis: sources of bleeding
10-20% arterial (Arteries of the true pelvis)
80-90% venous praesacral vein plexus
perivesical vein plexus
fracture surfaces
Das Saarland
www.unfallchirurgie-homburg.de
Angiography:
retroperitoneum closed
no surgical intervention
success rate 40-80%?
Pro´s: Con`s:
only art. heamorhage
accessable (10-20%)
qualified specialist requir.
time issue?
high lethality reported
Das Saarland
www.unfallchirurgie-homburg.de
Our treatment algorithm pelvis:
1. decision (0-5 min)
Mass bleeding ?
Overroll trauma
OR, surg. heamostasis
extended shock
therapy
radiographs
chest, pelvis
sonography
abdomen
Polytrauma
Algorithm no

Das Saarland
www.unfallchirurgie-homburg.de
circulation &
pelvic ring-unstable
emergency stabilization pelvis,
mass -transfusion
extended
diagnostics
Polytrauma
Algorithm
2. decision (10-15 min)
no
Das Saarland
www.unfallchirurgie-homburg.de
Mechanical stabilization of the pelvic ring?
C-clamp
External fix.
Pelvic girdle
Sling
Das Saarland
www.unfallchirurgie-homburg.de
Indication:
C-type injury (Sacrum fracture, SI-dislocations)
beware: overcompression sacrum
beware: transiliacale fx-dislocation, ilium fracture)
Pelvis is the most possible source of haemorrhage!
Pelvic clamps

Das Saarland
www.unfallchirurgie-homburg.de
Pohlemann et al. JOT 2005
Das Saarland
www.unfallchirurgie-homburg.de
Das Saarland
www.unfallchirurgie-homburg.de

Das Saarland
www.unfallchirurgie-homburg.de
Contin. haem. instab
surgical haeostasis
pelvine tamponade
erweiterte
Diagnostik
3. decision (20-35 min)
no
extended
diagnostics
Polytrauma
algorithm
Das Saarland
www.unfallchirurgie-homburg.de
Technique of pelvic tamponade:
The source of hemorrhage is within
the true pelvis and can therefore be
accessed without laparotomy!
Das Saarland
www.unfallchirurgie-homburg.de
Technique of pelvic tamponade:
infraumbilical medial incision
underneath fascia no further dissection neccessary!

Das Saarland
www.unfallchirurgie-homburg.de
Surgical technique pelvic tamponade:
Das Saarland
www.unfallchirurgie-homburg.de
Surgical technique pelvic tamponade:
Das Saarland
www.unfallchirurgie-homburg.de
Surgical technique pelvic tamponade:

Das Saarland
www.unfallchirurgie-homburg.de
1985-92
n=84 MHH: 1972-84
n=108
AG Beck. II 98/99
n=180
0
30
60
46%
25% 21%
PTS 31
PTS 35
HFS: 9,1
PTS 34
HFS: 8,6
Results of treatment
2004/5
20%
Das Saarland
www.unfallchirurgie-homburg.de
Summary:
Successfull polytrauma management is based on
standardized, rapid evaluation and treatment
Apply relyable protocols (e.g. ATLS™)!
Sequence of interventions?
stable conditions „Early total care“
unstable conditons „Damage control“
Module for pelvic fractures?
Mechanical pelvis stabilization &
Surgical haemostases (tamponade)
Das Saarland
www.unfallchirurgie-homburg.de

1/22/2013
1
VuMedi Iliosacral
ML Chip Routt Jr MD
Iliosacral Function
• Stability
• Ilium to Sacrum
• Reduction
• Percutaneous
• A&P
• SI-Sacral-Combo
The Posterior Pelvis – Door Hinges
• Pelvic Ring Injury
• Broken Door(s)

1/22/2013
2
Iliosacral
• Injury
Lock the Door
Fix the Hinge
Why Do We Need It?
• Closed
• Casting
• Traction
• Neglect
• Others
2009
Why Do We Need It?
• Operative Tx
• Bleeding
• Exposures
• Wounds
• Complications

1/22/2013
3
Why Do We Need It?
• Operative Tx
• Newer Gear
• Techniques
• O(R)IF
• Experience
• Education
• Confused
Osseus Fixation Pathways (OFP)
Osseus Fixation Pathways (OFP)

1/22/2013
4
Accurate Reduction
• Improves Stability
• Unloads Implants
• Optimal Space
• Safer Implants
• More Implants
• Improves Union
• Avoids Deformity
Reductions
• Open
• Traction
• Frames
• CPAS
• Anterior ORIF
• Others – Simple/Smart
Reduction - Skeletal Traction
• Distal Femoral
• 10-15#
• Simple

1/22/2013
5
Treatment?
• ORIF Symphysis Pubis
• Supine
• I&D/ORIF Posterior Pelvis
• Prone
Construct
• Symphysis Plate
• Iliosacral

1/22/2013
6
Reduction – Clinical Decision
• Angiography
• Embolization
Clinical Course
• S

1/22/2013
7
Reduction - Stability
• Plain Films
• CT
• Closed
• Open
• Screw
Iliosacral Details
• Dependant
• SI – Sacral -Others
• Start Point
• Aim
• Length
• Level S1/S2

1/22/2013
8
Supine > Prone
• Airway
• Face
• Access
• Anterior Ring
• Abdomen
• GU
• Vascular
• Chest
• Extremities
10#
Prone • Direct
• Open
• “Manipulators”
• Outrigger Frames
• No Anterior Ring
• Gravity Deformation
• Screw-in-situ
Sacral “Style”
• Sacral - Others
• Start Point
• Aim
• Length
• Balance
• Level S1/S2
Sacral SI

1/22/2013
9
SI “Style”
• SI – Others
• Start Point
• Aim
• Length
• Balance
• Level S1/S2
Sacral SI
Is It “Normal” or “Dysmorphic”?
• Segmentation-Upper-Narrowed Alar-Oblique
AP Inlet Outlet
Normal - Dysmorphic
• Outlet
• Features

1/22/2013
10
“Normal”
• Axial CT
• Options
• Oblique
• Linear
Upper
SI
Sacral
Sacral
Second
“Dysmorphic”
• Axial CT
• Upper
• Second
• OFPs
SI
Upper Second SI
Sacral
Levels
• S1
• S2
Lock the Door
Fix the Hinge

1/22/2013
11
Osseus Fixation Pathways
• Edges
• Shapes
• Areas
• OFPs
Imaging
• Preop
• Planning
• Sagittal
• Mid
• NonO
Table - Supine
Outlet
Inlet
Anterior Posterior Cranial
Caudal
Imaging
• Variety
• Adjusted
• Tilt
Outlet Inlet
Table - Supine
Anterior
Posterior
Cranial
Caudal

1/22/2013
12
Iliosacral Summary
• Early
• Small Wounds
• Blood Loss
• Reduction
• Osteology-OFPs
• Stability
• Variety Options

1/21/2013
1
Anterior and posterior pelvic plate fixation
Indications
Decisions
MARTIN BIRCHER ST.GEORGE’S HOSPITAL LONDON
General principles
You cannot consider the anterior and posterior injury in isolation
Beware the pelvic binder
The soft tissues may govern the management
The time since injury - open or closed techniques
Your system and experience
Anterior plate fixation of the pelvis

1/21/2013
2
Anterior injuries
Symphysis disruption – options
Plate or external fixation
Rami fractures – options
Plate, screw or external fixation
Combination injuries – tilts
Plates only
Symphysis pubis separation The plate rules !
Decisions
The soft tissues?
Bladder or urethral injury?
Urgency of the situation?
1 or 2 plates ?
4 hole or 6 hole?
3.5,4.5 recon, Matta or DCP?
Symphysis pubis separation The plate rules !
The soft tissues?
Bladder or urethra
urethra

1/21/2013
3
Symphysis pubis separation The plate rules !
Decisions
1 or 2 plates ?
4 hole or 6 hole?
3.5,4.5 recon, Matta or DCP?
THE POSTERIOR INJURY
THE SIZE OF THE PATIENT
BEWARE THE APC 2 INJURY
Pubic rami fractures
Most fractures do not need reduction or fixation
Is the periosteal sleeve violated ?
18 year old 100 mph motorcycle accident Binder
Soft tissue injury posterior laterally SIJ open a little

1/21/2013
4
The tilt fracture Uni-lateral(LC) or bilateral(APC)
The tilt fracture Bilateral(APC)

1/21/2013
5
Posterior plating of the pelvis
Posterior injuries
Sacroiliac dislocation – SI screws or plates
Crescent and iliac fractures – usually plates
Sacral fractures – screws or plates
U and H fractures – usually plates
Combinations

1/21/2013
6
Double plating of the S.I.Joint
Key points –Relaxation of psoas, lumbosacral nerve, screw direction and length
18 year old multiple injuries
Right posterior degloving
Iliac blade fractures

1/21/2013
7
Posterior plates
Decisions
As for anterior plating…….and
Is there evidence of nerve compression?
Front or back first ?
One or two positions?
Posterior plating
The state of the skin
Open SIJ and posterior surgery

1/21/2013
8
Open SIJ and posterior surgery
14 year old 12 foot fall from tree

1/21/2013
9
Summary Anterior and posterior pelvic plating
Strong biomechanical fixation solutions
Soft tissues must be quiet
Must consider both the front and the back lesion
Surgery as soon as possible
Watch the binder
Beware of the APC 2’s
THANK YOU

1/21/2013
1
Amir Matityahu, MD Director of Pelvic and Acetabular Trauma and Reconstruction
UCSF Department of Orthopaedic Surgery
Orthopaedic Trauma Institute
San Francisco General Hospital
Geriatric Pelvis Fracture care
Outline
Epidemiology
Pelvis Fractures – Misconceptions
– Morbidity and mortality
– Fracture repair options
– Outcomes from fracture repair
Anticipated Growth in the US Elderly Population >65 yrs
Year No.
2001 28 million
2020 52 million
2040 68 million JH Lonner et al CORR, 318:136; 1995

1/21/2013
2
Elderly population growing in size
MVA survival greater Elderly are surviving with more complex chronic illnesses Elderly more active
Epidemiology
In 2005, osteoporosis-related fractures = $19 billion in costs.
By 2025, costs = $25.3 billion.
osteoporosis was responsible for more than 2 million fractures in 2005, including:
135,000 pelvic fractures
297,000 hip fractures
547,000 vertebral fractures
397,000 wrist fractures
675,000 fractures at other sites

1/21/2013
3
Epidemiology of Pelvis Fractures
5% of all fractures in Octogenarians
But, 23% of admissions to level I trauma centers
T. A. Dechert, T. M. Duane, B. P. Frykberg, M. B. Aboutanos, A. K. Malhotra, and R. R. Ivatury, “Elderly patients with
pelvic fracture: interventions and outcomes,” American Surgeon, vol. 75, no. 4, pp. 291–295, 2009.
The severity may be frequently missed Retrospective study, N – 37, age 85 All had anterior ring fractures 60% had posterior ring fractures – 24% had LC-2 fractures with iliac wing component
81% were treated conservatively Still need the x-ray and CT scan to help in diagnosis
J Orthop Surg (Hong Kong). 2010 Aug;18(2):153-7. Occult posterior pelvic ring fractures in elderly patients with osteoporotic pubic
rami fractures. Lau, TW, Leung F. ,Department of Orthopaedics and Traumatology, Queen Mary Hospital, Hong Kong
Study to evaluate elderly patients with pelvis fractures
National Trauma Databank – 2002-2006
900 Trauma Centers in the USA
2.7 million patients total
45,000 had pelvis fractures included in the study
Amir Matityahu, Joshua Elson, Saam Morshed, and Meir Marmor
Survivorship and Severe Complications Are Worse for Octogenarians and Elderly Patients with Pelvis Fractures as
Compared to Adults: Data from the National Trauma Data Bank, Journal of Osteoporosis Volume 2012
1/21/2013
4
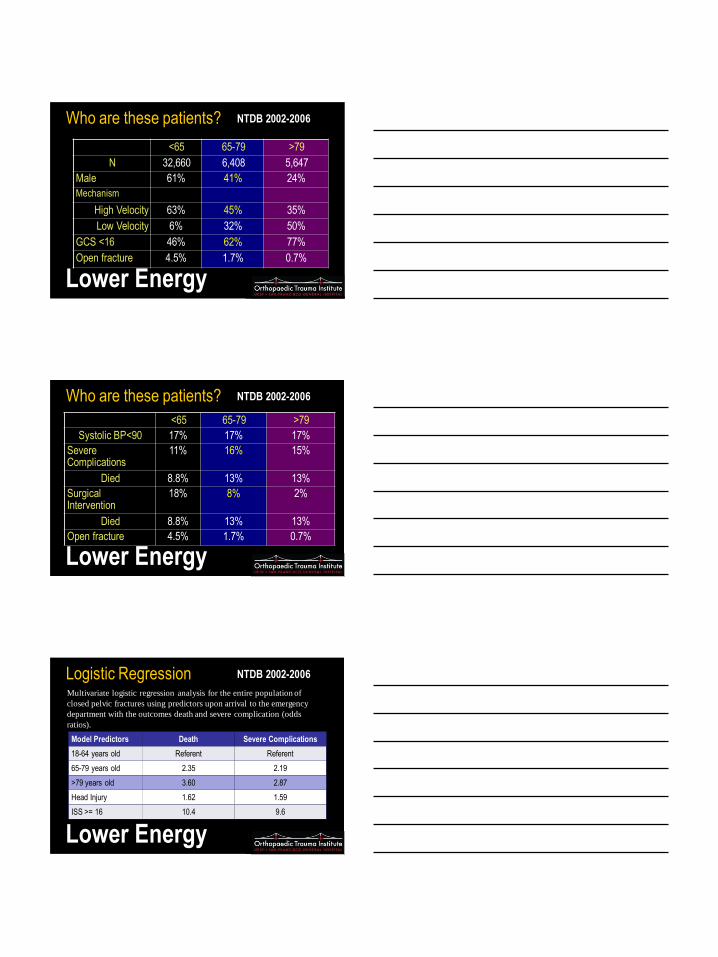
Who are these patients?
<65 65-79 >79
N 32,660 6,408 5,647
Male 61% 41% 24%
Mechanism
High Velocity 63% 45% 35%
Low Velocity 6% 32% 50%
GCS <16 46% 62% 77%
Open fracture 4.5% 1.7% 0.7%
NTDB 2002-2006
Lower Energy
Who are these patients?
<65 65-79 >79
Systolic BP<90 17% 17% 17%
Severe Complications
11% 16% 15%
Died 8.8% 13% 13%
Surgical Intervention
18% 8% 2%
Died 8.8% 13% 13%
Open fracture 4.5% 1.7% 0.7%
NTDB 2002-2006
Lower Energy
Logistic Regression NTDB 2002-2006
Lower Energy
Model Predictors Death Severe Complications
18-64 years old Referent Referent
65-79 years old 2.35 2.19
>79 years old 3.60 2.87
Head Injury 1.62 1.59
ISS >= 16 10.4 9.6
Multivariate logistic regression analysis for the entire population of
closed pelvic fractures using predictors upon arrival to the emergency
department with the outcomes death and severe complication (odds
ratios).

1/21/2013
5
Severe Pelvis Injury NTDB 2002-2006
Lower Energy
Model Predictors Death Severe Complications
18-64 years old Referent Referent
65-79 years old 2 2
>79 years old 5 5
Head Injury 3 3
ISS >= 16 15 18
Multivariate logistic regression analysis for the entire population of
closed pelvic fractures using predictors upon arrival to the emergency
department with the outcomes death and severe complication (odds
ratios).
Death increases 1% per 10 years 18 years old – 7.5%
88 years old – 14.5 %
Treatment of insufficiency fractures
Traditional – Analgesics
– Early Ambulation
• Complications with bed rest
– Pneumonia and PE
Proposed Surgical Treatments – Early fixation of the sacrum and/or rami
– Sacroplasty

1/21/2013
6
Mechanical testing
Biomechanical Comparison of Three Methods of Sacral Fracture Fixation in Osteoporotic Bone. Mears, Simon; MD, PhD; Sutter, Edward; Wall, Simon; Rose, David; Belkoff, Stephen
Spine. 35(10):E392-E395, May 1, 2010. DOI: 10.1097/BRS.0b013e3181cb4fcd
Sacroplasty
Screw into S1
Trans-sacral
Screw
What about fixation of unstable fractures? Elderly Pelvic Fx
Biomechanical Comparison of Three Methods of Sacral Fracture Fixation in Osteoporotic Bone. Mears, Simon; MD, PhD; Sutter, Edward; Wall, Simon; Rose, David; Belkoff, Stephen
Spine. 35(10):E392-E395, May 1, 2010. DOI: 10.1097/BRS.0b013e3181cb4fcd
(1) significant increase in average motion after fracture creation, (2) significant
reduction in average motion after fixation, and (3) nonsignificant increase in
average motion across the SI joint relative to intact SI motion. There were no
significant differences among treatments.
Pelvis fracture suspected on clinical exam or pubic rami fractures seen on x-ray
Perform CT Scan
Iliac wing or Sacral Fracture
Stable
Conservative management
Analgesics and Early Mobilization
Unstable
Surgical Stabilization
Trans-sacral screws, Rami screws, and plates
Not Sure
Exam Under Anesthesia
No Posterior ring fracture
Early Mobilization and Analgesics

1/21/2013
7
Summary
Less Energy
Higher mortality rate
Higher Complications
Early Mobilization
Or Early fixation then mobilization