radiotherapy for rectal cancer -...
TRANSCRIPT

Karin HaustermansDepartment of Radiation Oncology
Radiotherapy for rectal cancer
• RT with TME surgery?
• Neoadjuvant or adjuvant RT?
• 5 x 5 Gy or long-course CRT?
• RT with new drugs?
•Selection of patients?
OU T L I N E
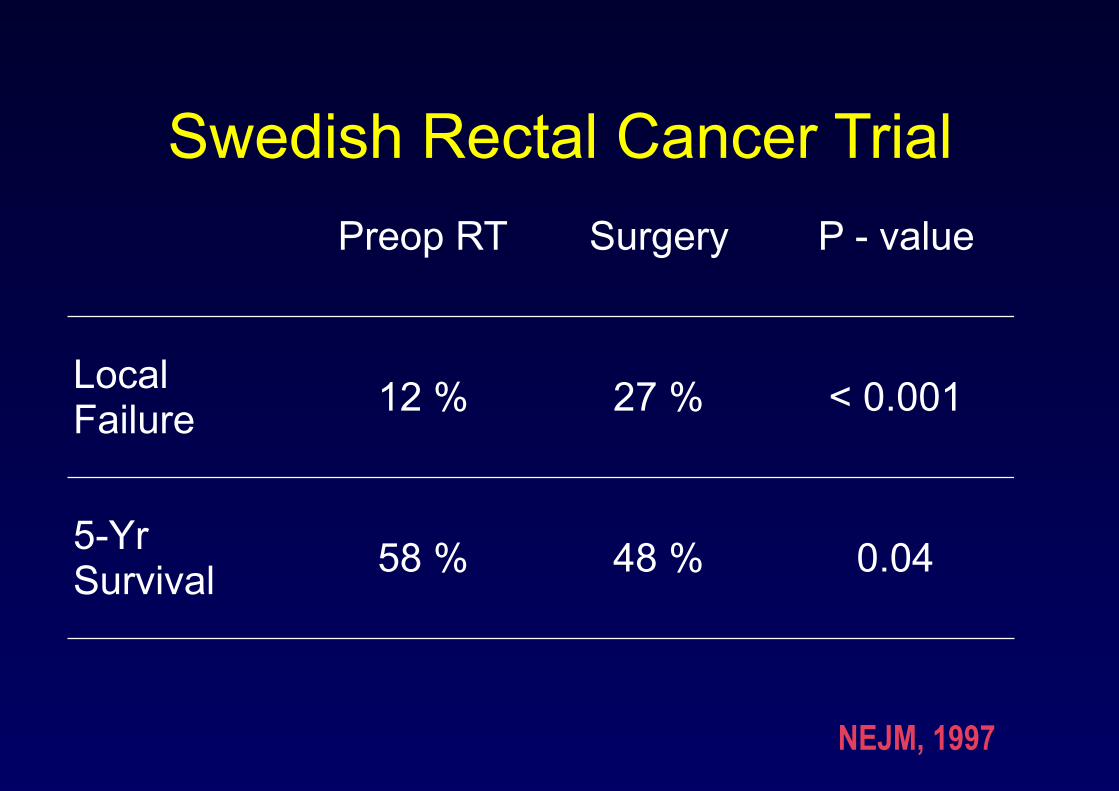
Swedish Rectal Cancer TrialPreop RT Surgery P - value
Local Failure 12 % 27 % < 0.001
5-Yr Survival 58 % 48 % 0.04
NEJM, 1997
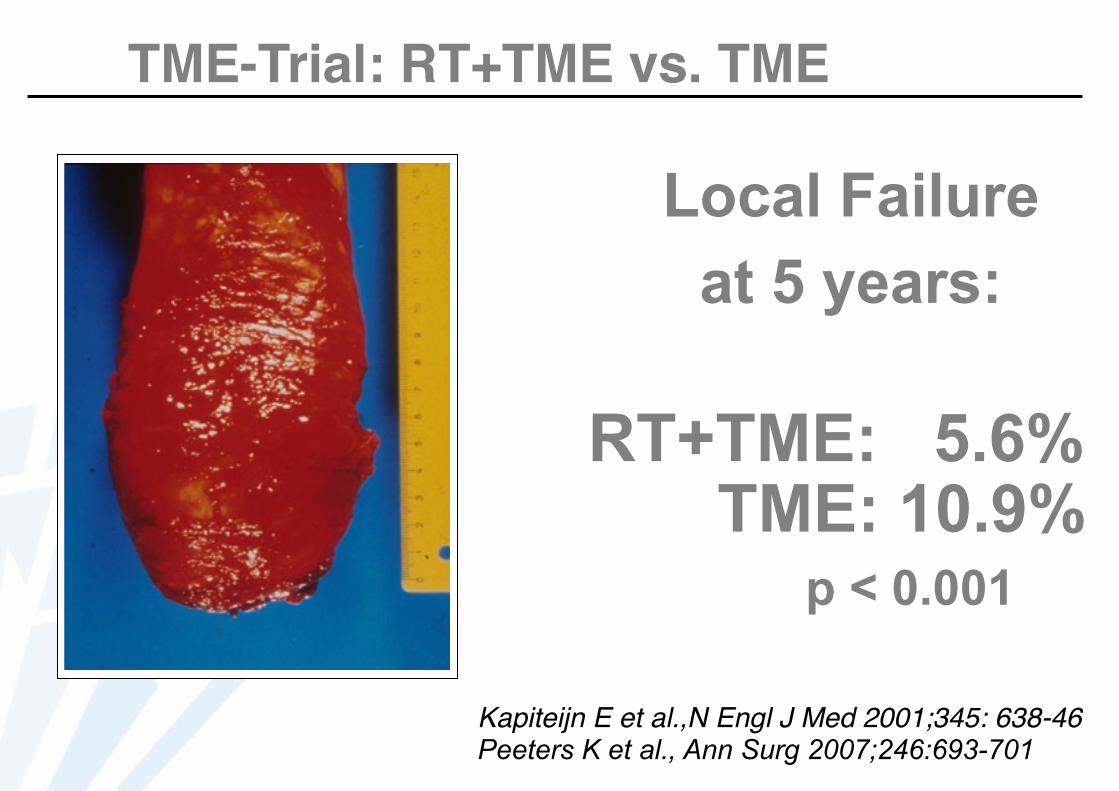
TME-Trial: RT+TME vs. TME
Local Failure at 5 years:
RT+TME: 5.6% TME: 10.9% p < 0.001
Kapiteijn E et al.,N Engl J Med 2001;345: 638-46 Peeters K et al., Ann Surg 2007;246:693-701

Influence of CRM on LR
Preop RT (%)
Surgery (%) P-value
CRM ≤ 2 mm 15.5 23.3 NS
CRM > 2 mm 3.6 8.5 <0.001
CRM > 10 mm 1.1 1.1 NS
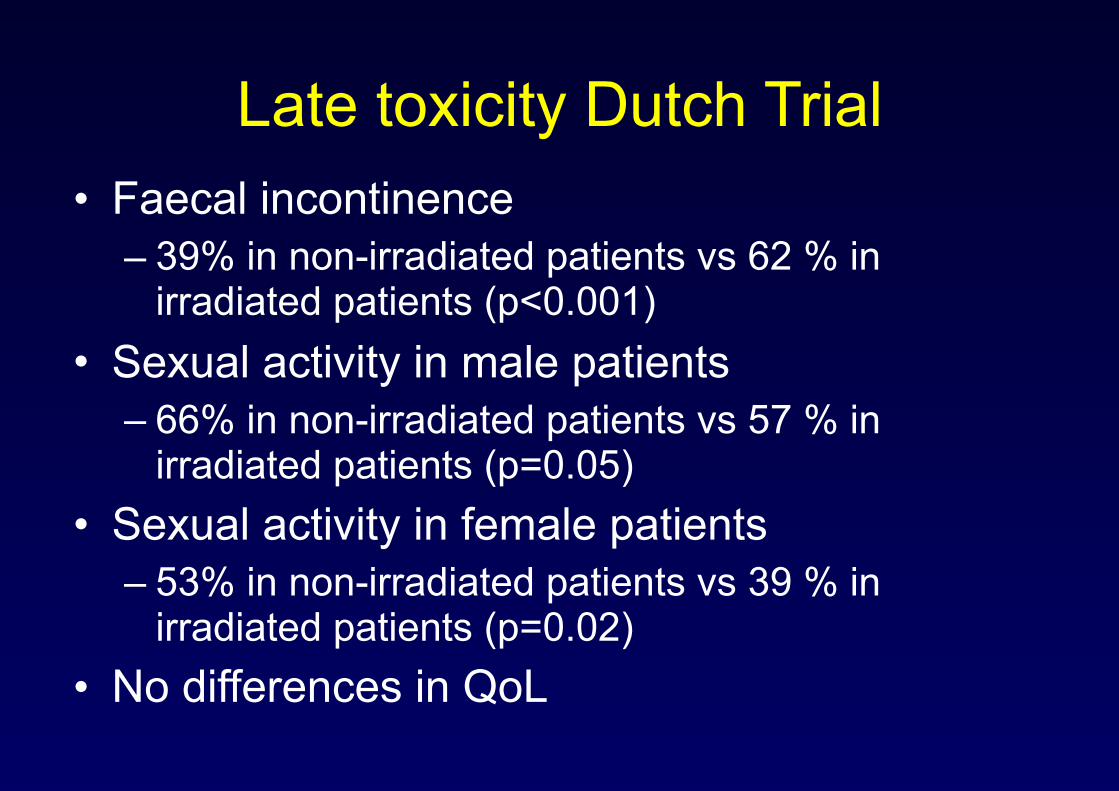
Late toxicity Dutch Trial• Faecal incontinence
– 39% in non-irradiated patients vs 62 % in irradiated patients (p<0.001)
• Sexual activity in male patients – 66% in non-irradiated patients vs 57 % in
irradiated patients (p=0.05) • Sexual activity in female patients
– 53% in non-irradiated patients vs 39 % in irradiated patients (p=0.02)
• No differences in QoL

Trial Design
Randomise
Clinically operable adenocarcinoma of the rectum <15cm from anal verge; no metastases
Adjuvant chemotherapy given as per local policy
PRE POST
Pre-operative RT 25Gy / 5F
Surgery
Pathology
Surgery
Pathology
CRM-ve CRM+ve
Post-op CRT 45Gy / 25F
+ concurrent 5FU
No RT
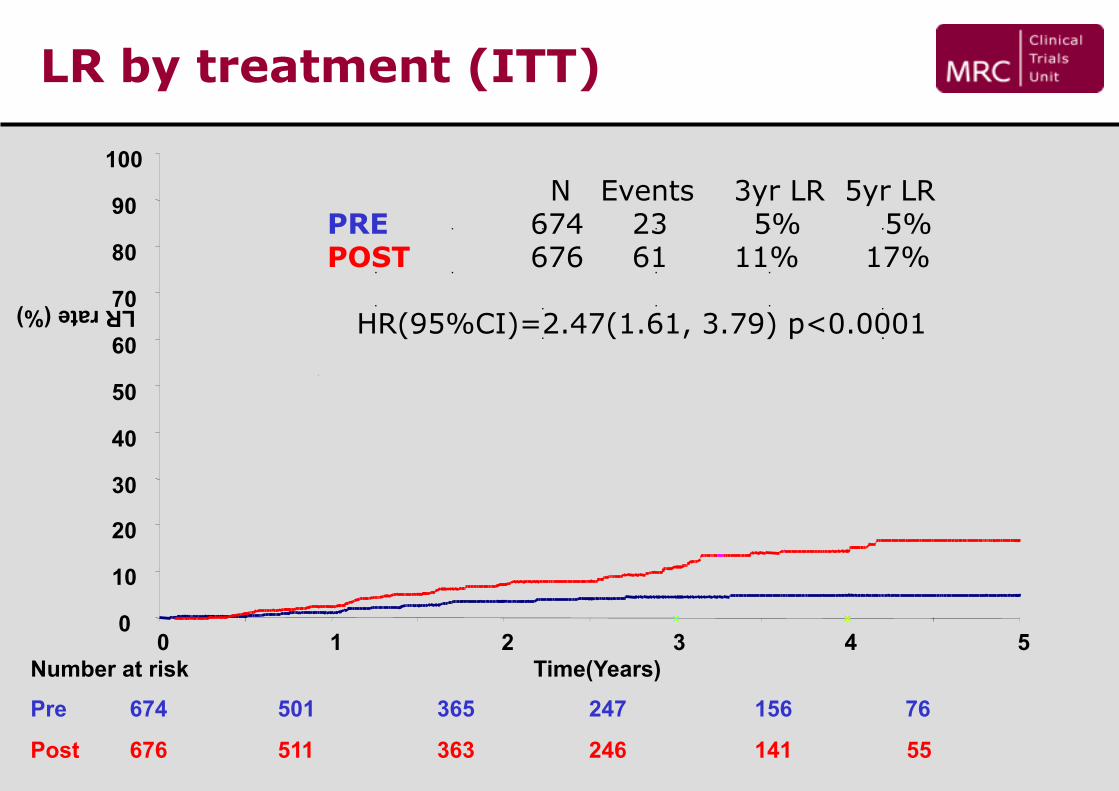
LR by treatment (ITT)
Number at risk
Pre 674 501 365 247 156 76
Post 676 511 363 246 141 55
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5Time(Years)
LR rate (%)
N Events 3yr LR 5yr LR PRE 674 23 5% 5% POST 676 61 11% 17%
HR(95%CI)=2.47(1.61, 3.79) p<0.0001
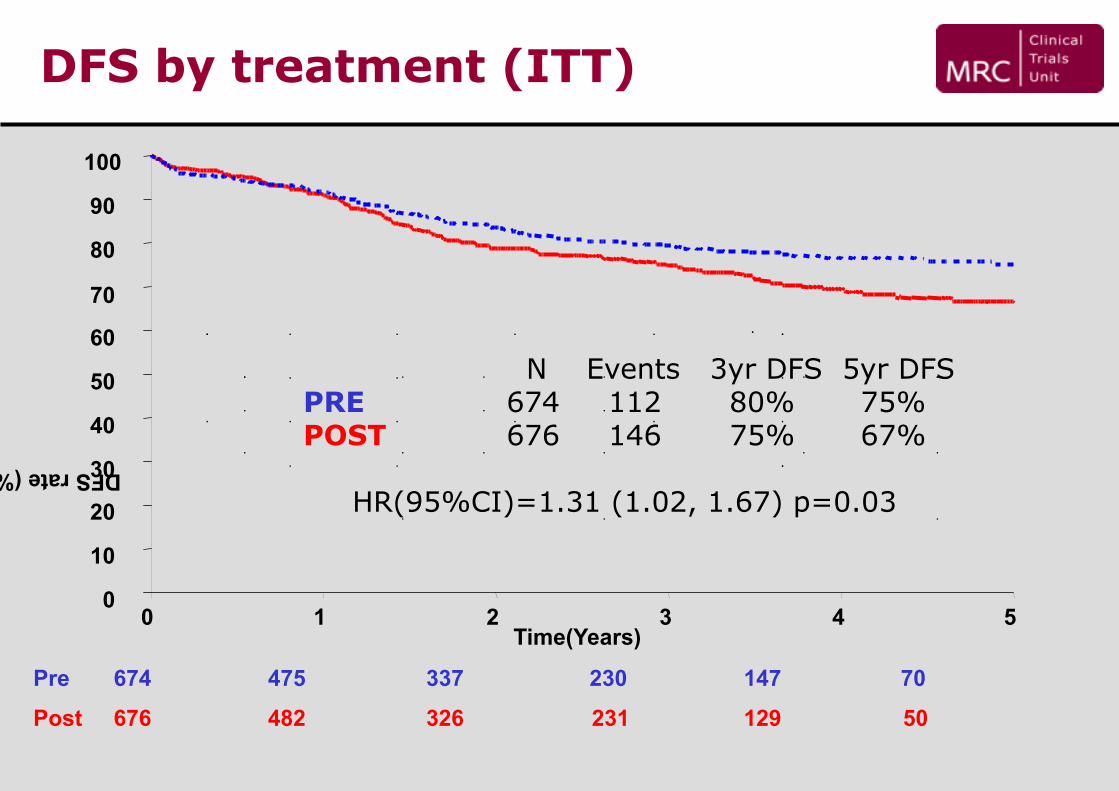
DFS by treatment (ITT)
Time(Years) 0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5
Pre 674 475 337 230 147 70
Post 676 482 326 231 129 50
DFS rate (%)
N Events 3yr DFS 5yr DFS PRE 674 112 80% 75% POST 676 146 75% 67%
HR(95%CI)=1.31 (1.02, 1.67) p=0.03

• RT with TME surgery? YES! But some subgroups may not benefit
• Neoadjuvant or adjuvant RT?
• 5 x 5 Gy or long-course CRT?
• RT with new drugs?
• Selection of patients?

• RT with TME surgery? YES! But some subgroups may not benefit
• Neoadjuvant or adjuvant RT?
• 5 x 5 Gy or long-course CRT?
• RT with new drugs?
• Selection of patients?
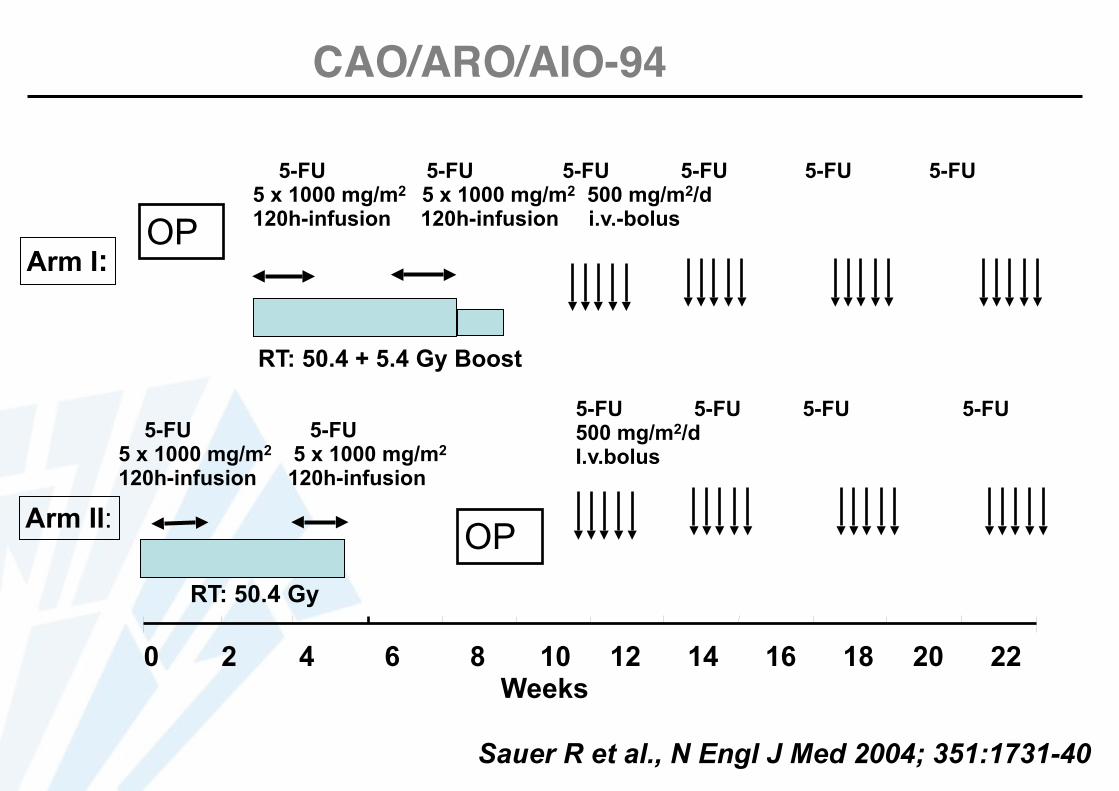
0 2 4 6 8 10 12 14 16 18 20 22 Weeks
OP
5-FU 5-FU 5 x 1000 mg/m2 5 x 1000 mg/m2 120h-infusion 120h-infusion
RT: 50.4 Gy
Arm II:
5-FU 5-FU 5-FU 5-FU 5-FU 5-FU 5 x 1000 mg/m2 5 x 1000 mg/m2 500 mg/m2/d 120h-infusion 120h-infusion i.v.-bolus
RT: 50.4 + 5.4 Gy Boost
Arm I:
5-FU 5-FU 5-FU 5-FU 500 mg/m2/d I.v.bolus
OP
Sauer R et al., N Engl J Med 2004; 351:1731-40
CAO/ARO/AIO-94

0.3
0.2
0.0
0.1
0 2412 4836 60
p = 0.006
6%
Months
Cum
ulat
ive
Inci
denc
e
Preop. RCT
Postop. CRT 13%
Local Relapse
Preop CRT: + • Downstaging • Compliance • Local control • Toxicity • Sphincter
Sauer R et al., N Engl J Med 2004; 351:1731-40
Pre vs. Postop. RCT: CAO/ARO/AIO-94

Postop. CRT CAO/ARO/AIO-94 UICC- I 18 %
UICC-II 29 %
UICC-III 40 %
UICC-IV 7 %
Missing 6 %
MSMMP
Risk of “Overtreatment”
Pathological Stage
Sauer R et al., N Engl J Med 2004; 351:1731-40
• RT with TME surgery? YES! But some subgroups may not benefit
• Neoadjuvant or adjuvant RT? Neoadjuvant! But need for improved staging (MRI)
• 5 x 5 Gy or long-course CRT?
• RT with new drugs?
• Selection of patients?

• RT with TME surgery? YES! But some subgroups may not benefit
• Neoadjuvant or adjuvant RT? Neoadjuvant! But need for improved staging (MRI)
• 5 x 5 Gy or long-course CRT?
• RT with new drugs?
• Selection of patients?
RT
RTCT
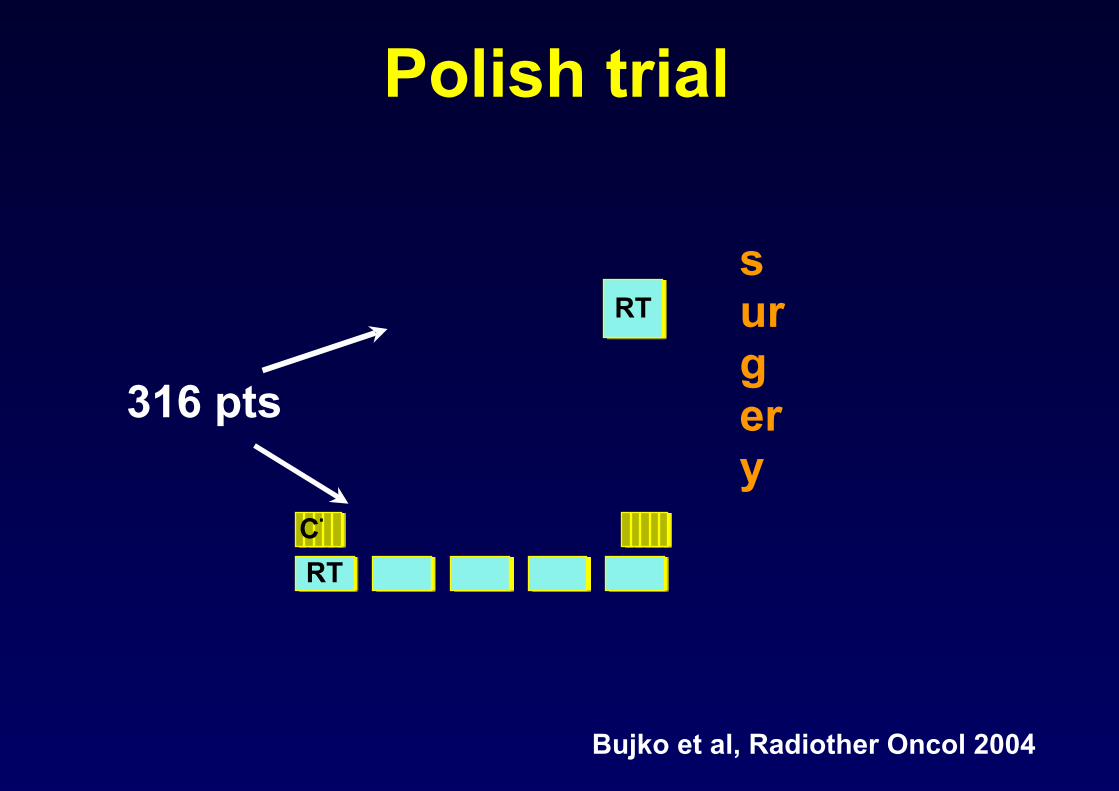
Polish trial
Bujko et al, Radiother Oncol 2004
316 pts
surgery
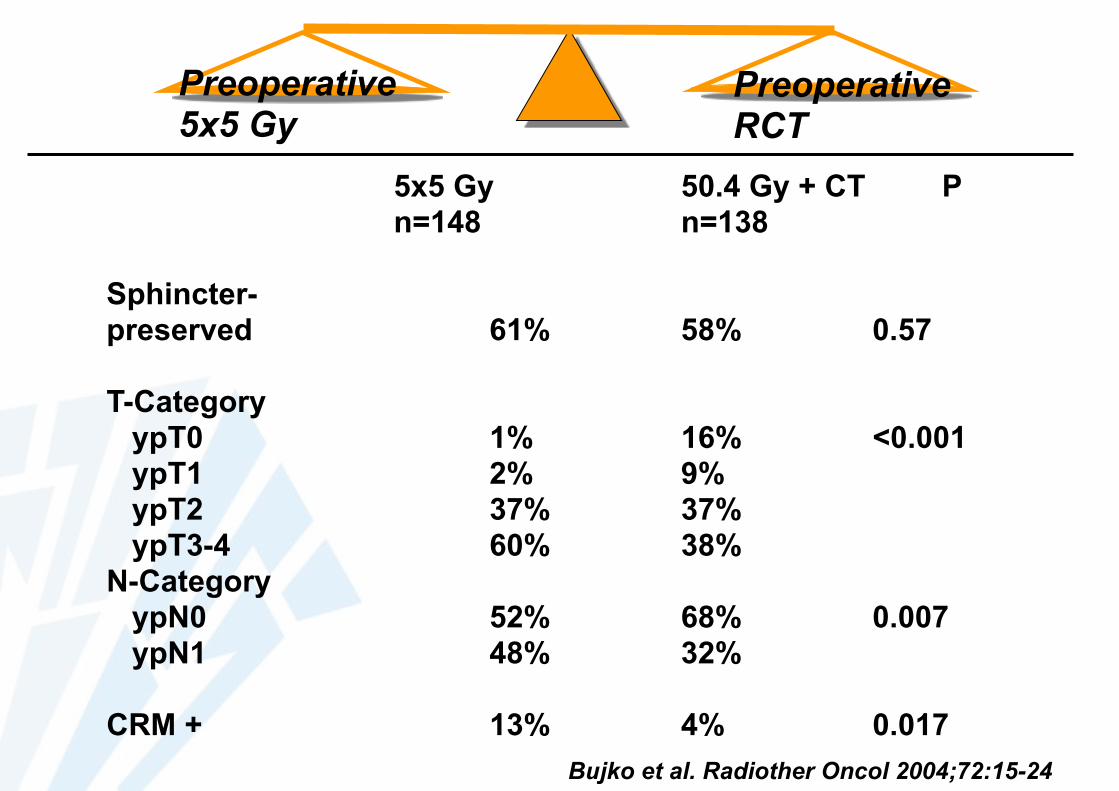
5x5 Gy 50.4 Gy + CT P n=148 n=138
Sphincter- preserved 61% 58% 0.57
T-Category ypT0 1% 16% <0.001 ypT1 2% 9% ypT2 37% 37% ypT3-4 60% 38% N-Category ypN0 52% 68% 0.007 ypN1 48% 32%
CRM + 13% 4% 0.017 Bujko et al. Radiother Oncol 2004;72:15-24
Preoperative 5x5 Gy
Preoperative RCT
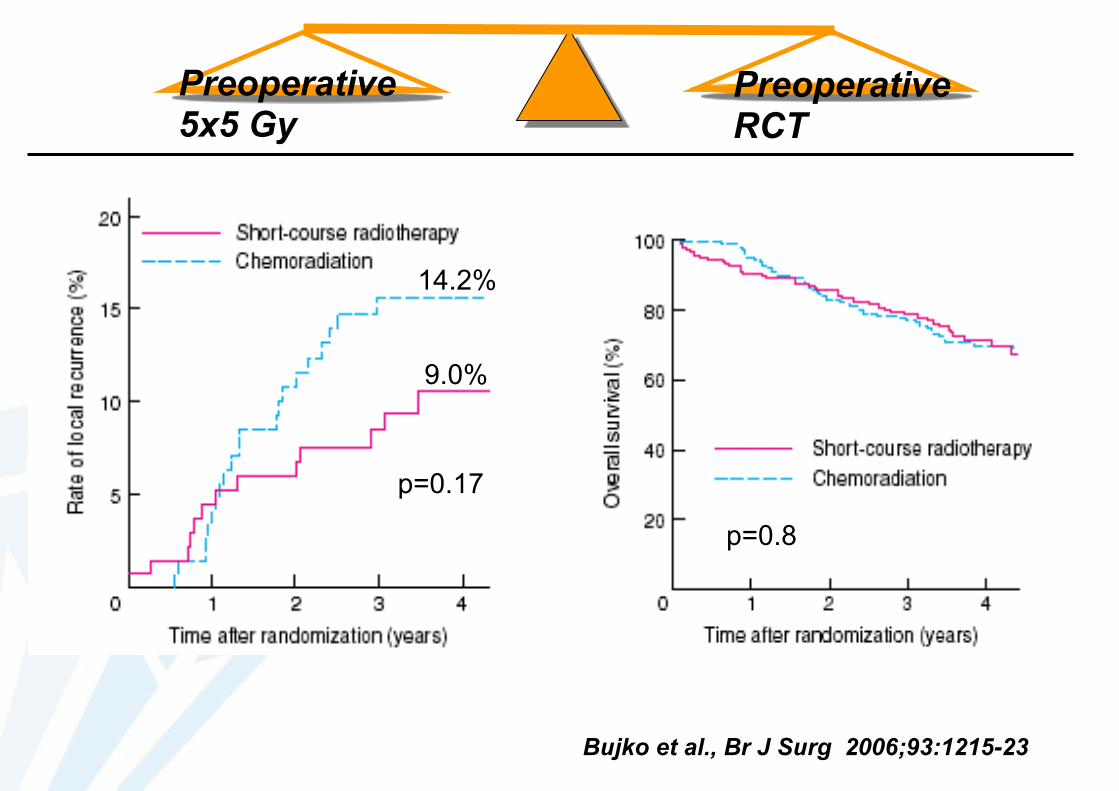
Bujko et al., Br J Surg 2006;93:1215-23
p=0.8
p=0.17
9.0%
14.2%
Preoperative 5x5 Gy
Preoperative RCT
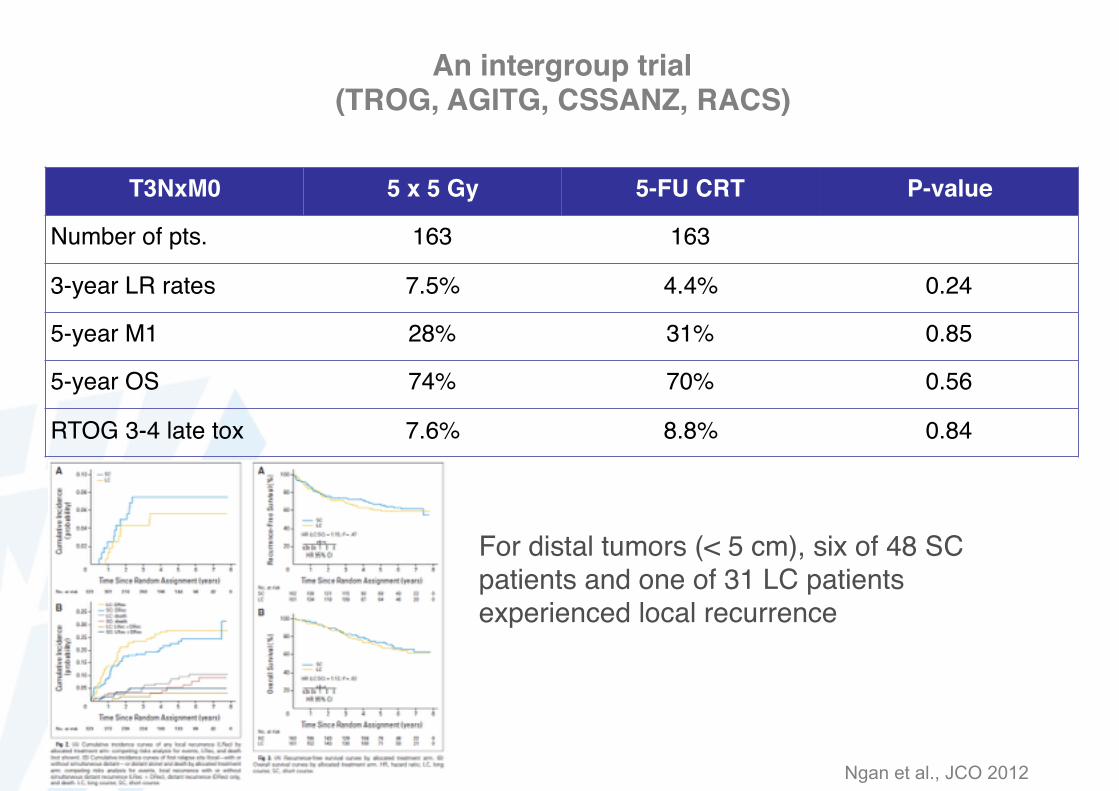
An intergroup trial (TROG, AGITG, CSSANZ, RACS)
T3NxM0 5 x 5 Gy 5-FU CRT P-value
Number of pts. 163 163
3-year LR rates 7.5% 4.4% 0.24
5-year M1 28% 31% 0.85
5-year OS 74% 70% 0.56
RTOG 3-4 late tox 7.6% 8.8% 0.84
Ngan et al., JCO 2012
For distal tumors (< 5 cm), six of 48 SC patients and one of 31 LC patients experienced local recurrence
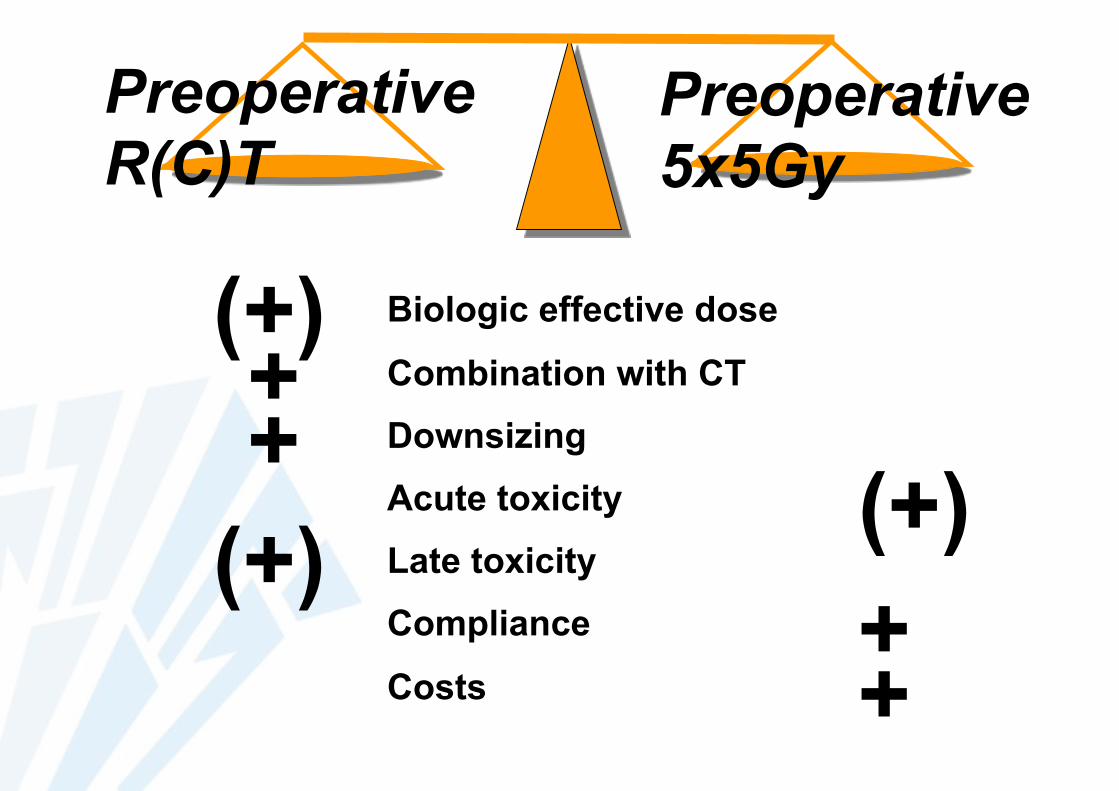
Preoperative R(C)T
Preoperative 5x5Gy
(+) Biologic effective dose
Combination with CT
Downsizing
Acute toxicity
Late toxicity
Compliance
Costs
++
(+)(+)++
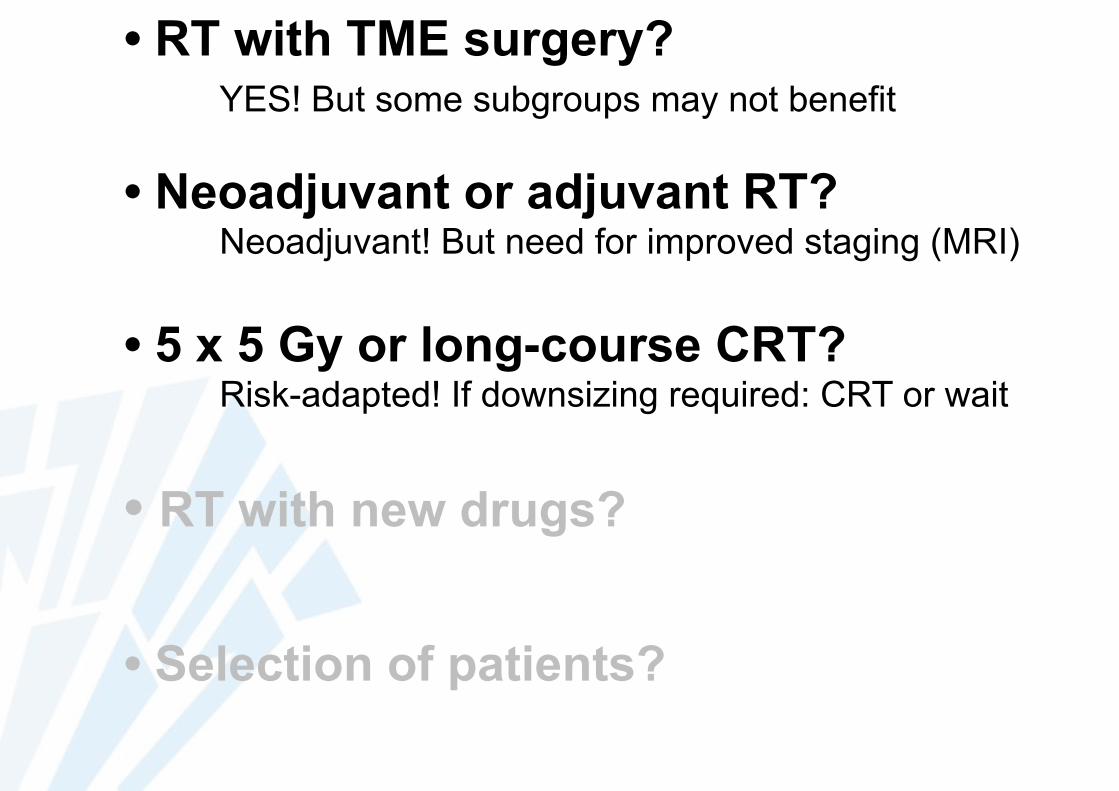
• RT with TME surgery? YES! But some subgroups may not benefit
• Neoadjuvant or adjuvant RT? Neoadjuvant! But need for improved staging (MRI)
• 5 x 5 Gy or long-course CRT? Risk-adapted! If downsizing required: CRT or wait
• RT with new drugs?
• Selection of patients?

• RT with TME surgery? YES! But some subgroups may not benefit
• Neoadjuvant or adjuvant RT? Neoadjuvant! But need for improved staging (MRI)
• 5 x 5 Gy or long-course CRT? Risk-adapted! If downsizing required: CRT or wait
• RT with new drugs?
• Selection of patients?

RANDOMIZE
Pre-op RT Pre-op RT + 5FU/LV x2
Pre-op RT Pre-op RT + 5FU/LV x2
Surgery Surgery Surgery Surgery
Post-op 5FU/LV x4
Post-op 5FU/LV x4
Rectal cancer T3/T4 NX M0 (UICC 1987) by DRE or EUSConsidered resectable, WHO PS 0-1, Age ≤ 80 y
Accrual : 1011 patients April 1993 - April 2003

Bosset et al, Lancet Oncology 2014
DFS
OS

Oxaliplatin
STAR-01 ACCORD 12 CAO/ARO/AIO-04
NSABP-R-04 PETACC-6
year of randomisation
11/2003-08/2008
11/2005-7/2008
7/2006-2/2010
7/2004-8/2010
11/2008-09/2011
number of patients
747 598 1265 1608 1094
preoperative regimen
50,4 Gy + fluorouracil
225mg/m² (CI)vs.
50,4 Gy + fluorouracil
225mg/m² (CI) + OX 60mg/m²
weekly
45 Gy + CAPb.i.d. 800mg/m²
vs.50 Gy + CAP
b.i.d. 800mg/m²+ OX 50mg/m²
weekly
50,4 Gy + fluorouracil
1000mg/m² d1-d5, d29-d33
vs.50,4 Gy +
fluorouracil 250mg/m² d1-d14, d22-d35 + OX 50mg/m² d1,8,22,29
45 Gy + 5,4-10,8Gy + fluorouracil
225mg/m² (CI) or CAP 825mg/m²
b.i.d.vs.
45 Gy + 5,4-10,8Gy + fluorouracil
225mg/m² (CI) or CAP 825mg/m²
b.i.d. + OX 50mg/m² weekly
45 Gy + optional boost 5,4 Gy +
CAP b.i.d. 825mg/m²
vs.45 Gy + optional boost 5,4 Gy +
CAP b.i.d. 825mg/m²
+ OX 50mg/m² d1,8,15,22,29
cumulative dose OX preop
360 mg/m² 250mg/m² 200mg/m² 250mg/m² 250mg/m²
primary endpoint OS pCR DFS pCR, sphincter saving surgery,
downstaging
DFS

STAR-01 ACCORD 12 CAO/ARO/AIO-04
NSABP-R-04 PETACC-6
G3-4 preop toxicity
8% vs. 24% (p<0,001)
10.9% vs. 25.4% (p<0,001)
20% vs. 23%
6,6% vs. 15,4% (p<0,0001)
15,1% vs. 36,7%
surgical toxicities
80% vs. 83% 20.9% vs. 18.1% 44% vs. 47%
NA 38% vs. 41%
full dose RT 92% vs. 84% 100% vs. 87% 96% vs. 94%
NA 97% vs. 94%
Dose modification CT
90% vs. 80% received ≥ 80% of fluorouracil and 66% received all OX cycles
50% vs. 59%
21% vs. 15%
From 84% to 97% of pts received >80% of the ideal CT dose
91% vs. 63% received <90%
Toxicity data of randomized trials with oxaliplatin

Gerard et al, JCO 2012
ACCORD 12
(years)
0 1 2 3 4 5 6
0
10
20
30
40
50
60
70
80
90
100
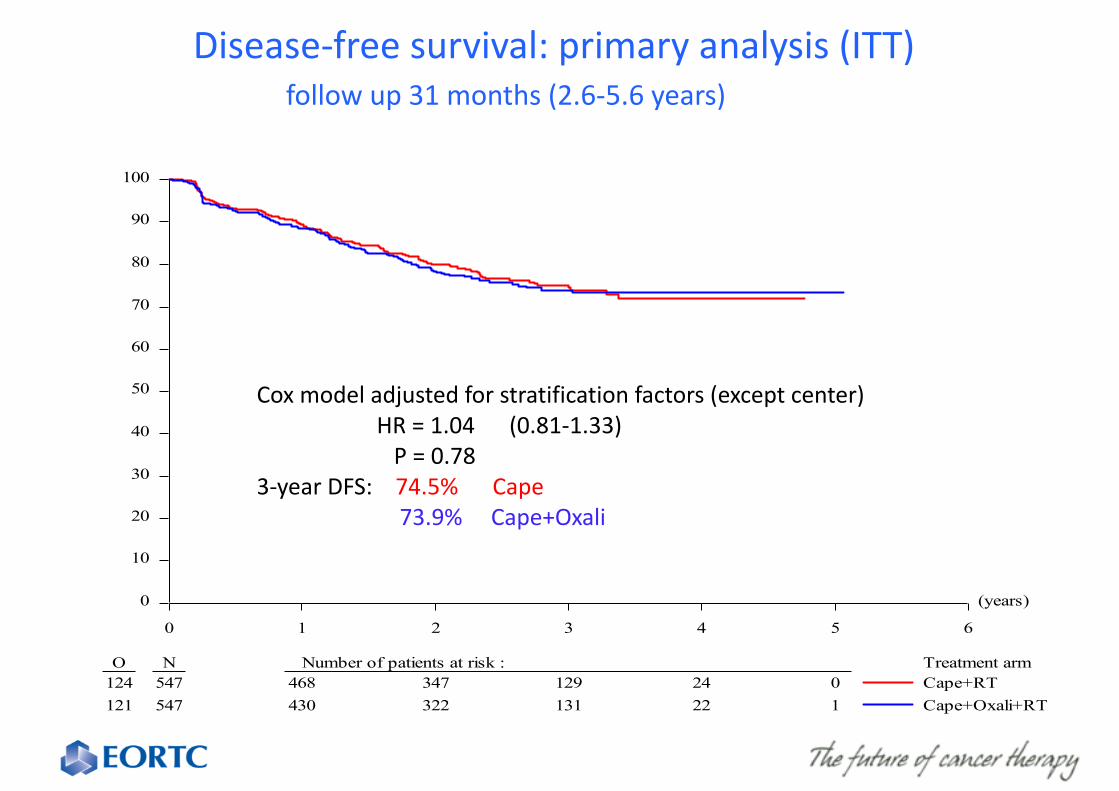
O N Number of patients at risk : Treatment arm124 547 468 347 129 24 0121 547 430 322 131 22 1
Cape+RTCape+Oxali+RT
Disease-‐free survival: primary analysis (ITT) follow up 31 months (2.6-‐5.6 years)
Cox model adjusted for stratification factors (except center) HR = 1.04 (0.81-‐1.33) P = 0.78 3-‐year DFS: 74.5% Cape 73.9% Cape+Oxali

Giralt J. et al., Radiother Oncol 2005;74:101-8
Rectal Cancer: Rationale to combine CRT with EGFR-Inhibition:
EGFR - EGFR +
pCR: 8/35 pCR: 2/52 29% 4% p=0.006
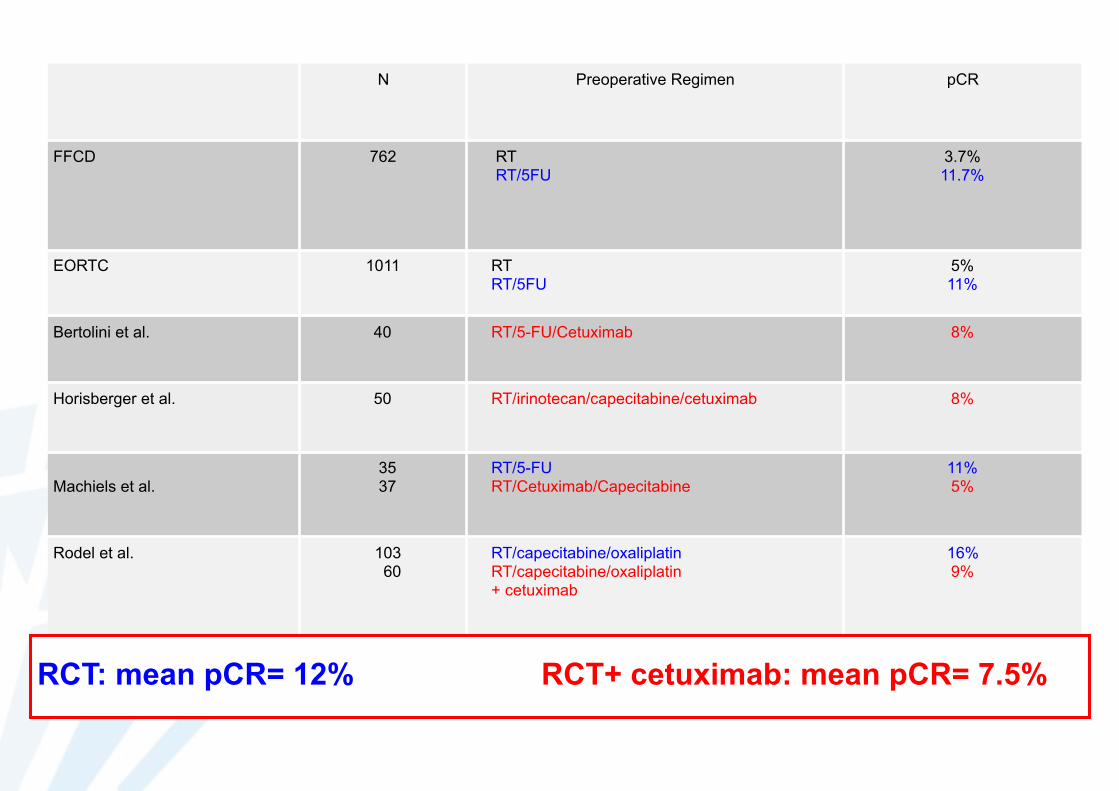
N Preoperative Regimen pCR
FFCD 762 RT RT/5FU
3.7% 11.7%
EORTC 1011 RT RT/5FU
5% 11%
Bertolini et al. 40 RT/5-FU/Cetuximab 8%
Horisberger et al. 50 RT/irinotecan/capecitabine/cetuximab 8%
Machiels et al. 35 37
RT/5-FU RT/Cetuximab/Capecitabine
11% 5%
Rodel et al. 103 60
RT/capecitabine/oxaliplatin RT/capecitabine/oxaliplatin + cetuximab
16% 9%
RCT: mean pCR= 12% RCT+ cetuximab: mean pCR= 7.5%

Molecular mechanisms?
Biomarkers?
Pooled pCR = 22%
SELECTION!
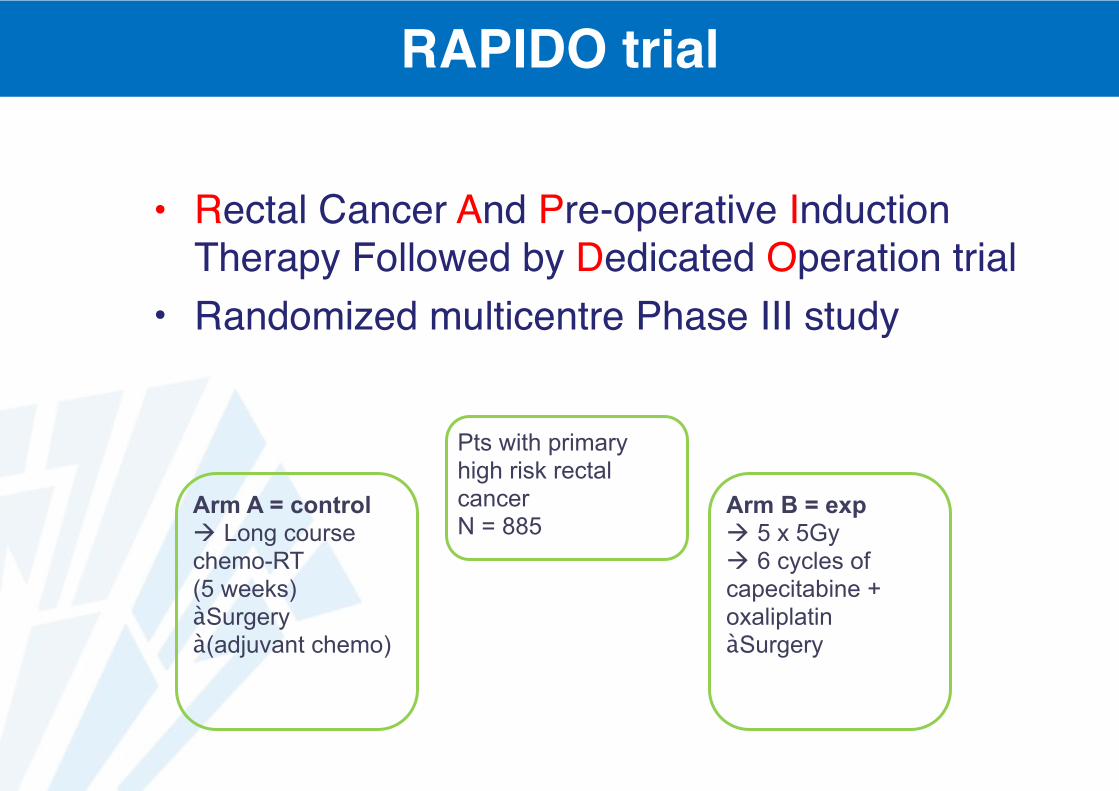
RAPIDO trial
• Rectal Cancer And Pre-operative Induction Therapy Followed by Dedicated Operation trial
• Randomized multicentre Phase III study
Pts with primary high risk rectal cancer N = 885
Arm A = control ! Long course chemo-RT (5 weeks) àSurgery à(adjuvant chemo)
Arm B = exp ! 5 x 5Gy ! 6 cycles of capecitabine + oxaliplatin àSurgery

Brachytherapy
• Danish Colorectal Cancer Group• Dose-escalation randomized phase III trial
Jakobsen et al. IJROBP 2012
Pts with resectable T3 and T4 tumours; CRM ≤ 5mm on MRI
Standard CRT (50,4 Gy in 28 fx) N = 123 (T3: 102; T4: 21)
Standard CRT + HDR brachy boost (10 Gy in 2 fx) N = 120 (T3: 102; T4: 18)
Endorectal BT as boost

Brachytherapy
Jakobsen et al. IJROBP 2012
TRG 1 and 2
Post-op complications
Grade 3 toxicity
T3 tumours
• Higher radiation dose increases the rate of major response (TRG1-2) by 50% in T3 tumours
• Endorectal boost is feasible, with no significant increase in toxicity or surgical complications
• RT with TME surgery? YES! But some subgroups may not benefit
• Neoadjuvant or adjuvant RT? Neoadjuvant! But need for improved staging (MRI)
• 5 x 5 Gy or long-course CRT? Risk-adapted! If downsizing required: CRT or wait
• RT with new drugs? Scheduling and intensification requires further study
• Selection of patients?
• RT with TME surgery? YES! But some subgroups may not benefit
• Neoadjuvant or adjuvant RT? Neoadjuvant! But need for improved staging (MRI)
• 5 x 5 Gy or long-course CRT? Risk-adapted! If downsizing required: CRT or wait
• RT with new drugs? Scheduling and intensification requires further study
• Selection of patients?
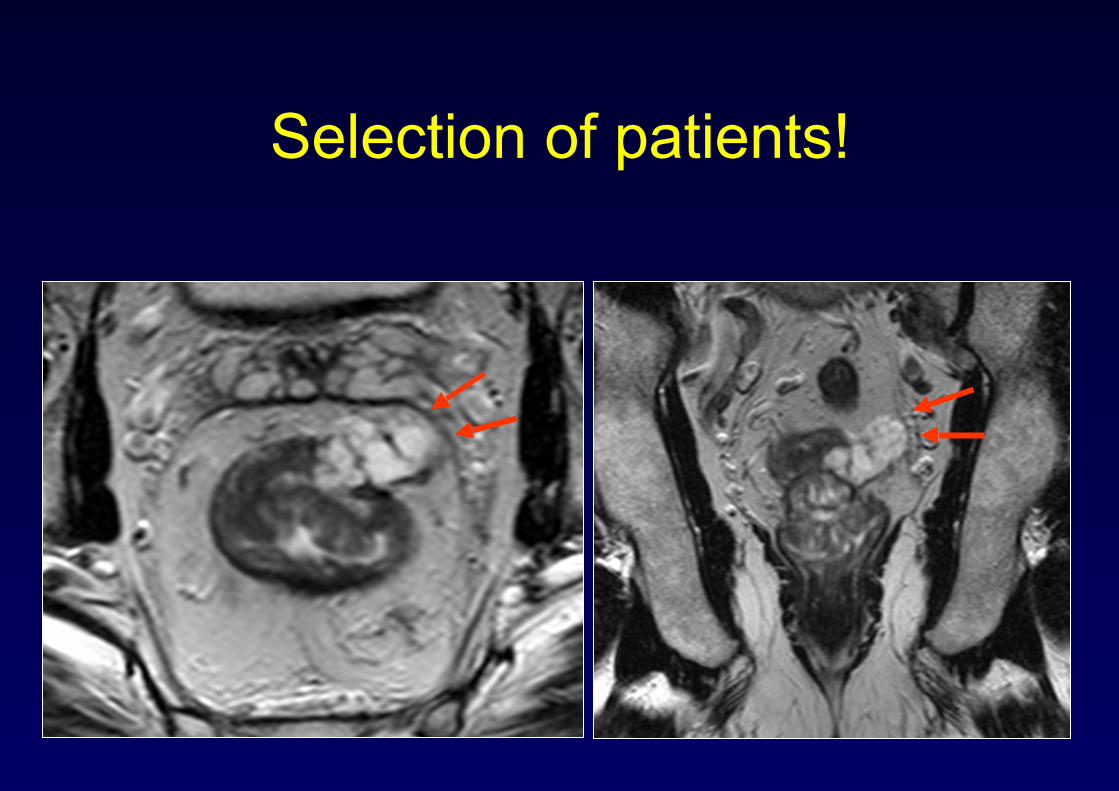
Selection of patients!

Quality of surgery: definitions
Complete mesorectum:
No defect deeper than 5 mm Smooth circumferential margin

Quality of surgery: definitions
Incomplete mesorectum:
Defects down onto muscularis Irregular circumferential margin
0
10
20
30
40
50
60
70
80
90
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5Time (years)
LR r
ate
(%
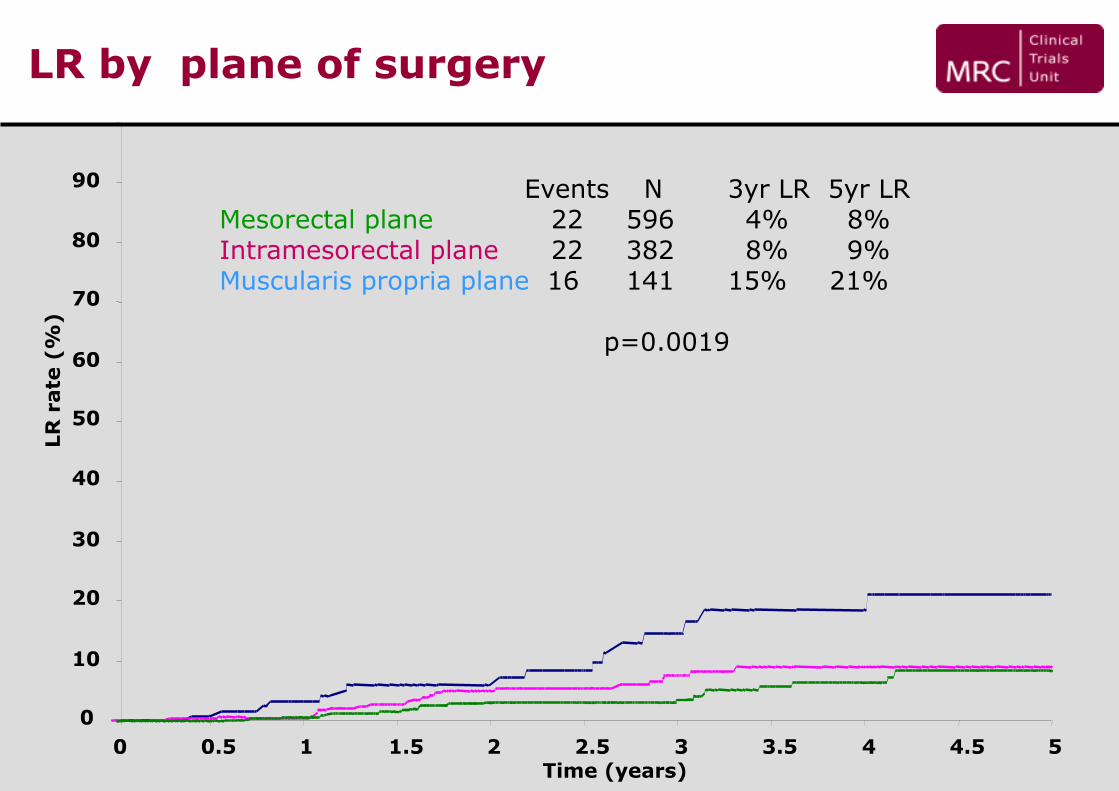
)LR by plane of surgery
Events N 3yr LR 5yr LR Mesorectal plane 22 596 4% 8% Intramesorectal plane 22 382 8% 9% Muscularis propria plane 16 141 15% 21%
p=0.0019

Fokas et al, JCO 2014
Organ preservation
Organ preservation is appealing…
• Avoidance of • significant postoperative mortality and morbidity• long-term urinary, sexual, and fecal dysfunction• temporary or definitive stoma
• Increasing quality of life
… and oncological outcome seems good…
Maas et al, JCO 2011
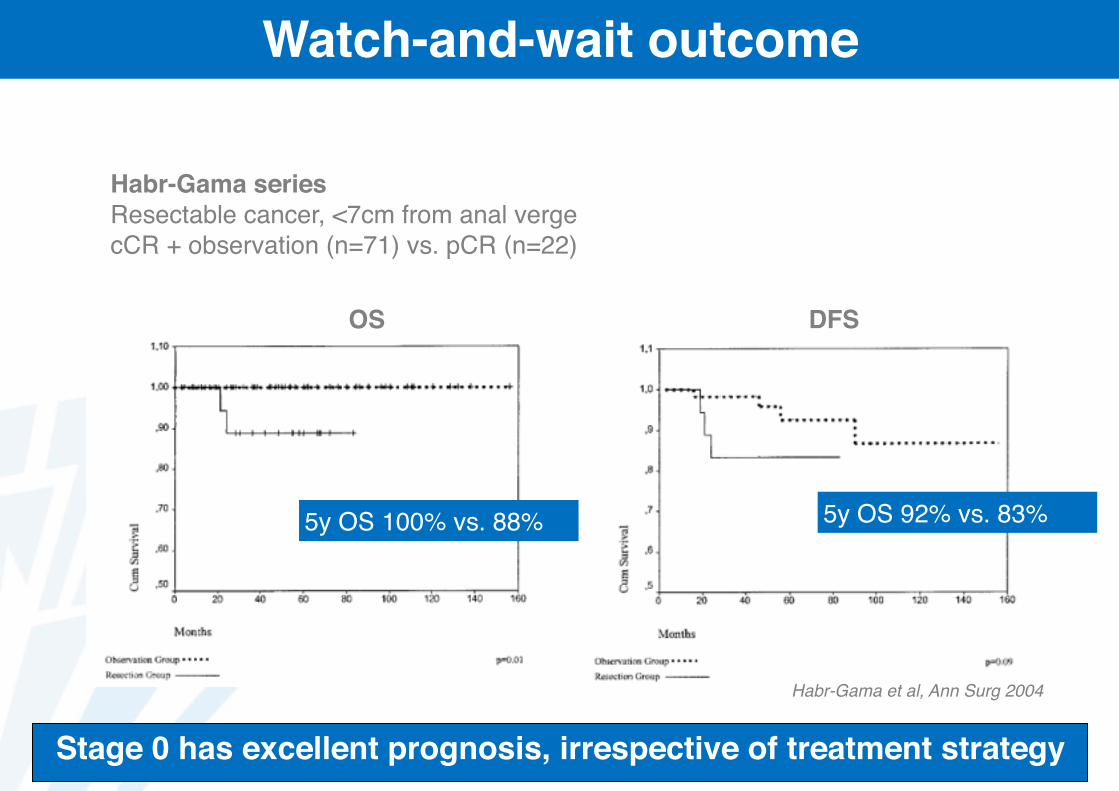
Watch-and-wait outcome
Habr-Gama et al, Ann Surg 2004
DFSOS
Habr-Gama series Resectable cancer, <7cm from anal vergecCR + observation (n=71) vs. pCR (n=22)
5y OS 100% vs. 88% 5y OS 92% vs. 83%
Stage 0 has excellent prognosis, irrespective of treatment strategy
• RT with TME surgery? YES! But some subgroups may not benefit
• Neoadjuvant or adjuvant RT? Neoadjuvant! But need for improved staging (MRI)
• 5 x 5 Gy or long-course CRT? Risk-adapted! If downsizing required: CRT or wait
• RT with new drugs? Scheduling and intensification requires further study
• Selection of patients? YES! Before and during …
SU M M A R Y

Thank you!