raised intracranial pressure
TRANSCRIPT

Raised Intracranial Pressure
Soumya Ranjan ParidaBasic B.Sc. Nursing 4th year
Sum Nursing College

Clinical History
9 yr Male
℅ 1) Fever : 5 days Mod grade continuous 2) Headache : 4 days 3) Irrelevant talking : 3 days 4) Altered consciousness : 2 days Past history : Not significant Family history : Not significant

Pt admitted in private hospital and treated with i.v. antibiotics & mannitol
LP Protein :156 Sugar : 107 Total cells: 6 (p:4, l:2)
No response to above management hence transferred to B.J.Wadia hospital for further management.

Examination On Admission
O/E Pt drowsy P : 60/min regular RR : 24/min BP : 120/70 mm of Hg GCS: 8/15 E4 : spontaneous M3 :Abn Flexion V1 :None
Pupils : B/L Equal, reacting to light Reflexes : ++ Plantar : ↑↑ No neck stiffness No sign of meningeal irritation

Initial Treatment
1) Head End Elevation 30˚
2) Head Straight in Midline
Started on
1) Acyclovir
2) Ceftriaxone
3) Manitol

DAY 1
BP maintaining at 130/70 mm of Hg HR : 84/min RR : 24/min GCS : 8/15
Pt was shifted for Neuroimaging (MRI) accompanied by resident

Further Course
BP : 160/110 mm of Hg HR : 80/min RR : 18/min
CNS : Pupil :Unequal, Right sided dilated, Sluggish reacting to light Reflexes +++ Plantars ↑↑
GCS: 3/15

MRI

MRI
Trans tentorial Herniation
Cerebral Edema Hyperintensities in
temporal and frontal lobe suggestive of VIRAL ENCEPHALITIS

Management Pt intubated and Hyperventilated
Injection Manitol i.v. bolus 3% NaCl over 30 min – shifted to OT
Sx : Right Craniectomy, dura split, scalp sutured back
Immediate post op
Pupils : b/l equal reacting to light BP : 110/70 mm of Hg HR : 90/ min
Pt electively ventilated for 36 hrs Mean BP maintained at 70 mm of Hg S.electrolytes and ABG kept WNL

Day 2 Extubated after 36 hrs Pupils : b/l equal reacting to light Moving all 4 limbs No cranial nerve , Focal Neurological Deficit
GCS :10/15 E3 : eye opening to verbal stimulus M5 : localises pain V2 : incoherent sounds

DAY 4
GCS : 13/15
E4 : spontaneous eye opening
M6 :obeys commands
V3 : inappropriate words

DAY 6
D6
Normal

On discharge :21 days post op

3 Months post op Cranioplasty done

Attends school

Thank you
BRAIN HERNIATIONS
Brain herniations represent shift of the normal brain through or across regions to another site due to mass effect.
These are generally complications of mass effect whether from tumor, trauma, or infection.
These include transtentorial, subfalcine, foramen magnum, and alar or sphenoid herniation.

Signs Where does displaced
brain go? Side to side:
subfalcine Side to bottom:
uncal (transtentorial)
Top to bottom: central tentorial
Bottom to top: “upward”
Bottom thru the “hole”: tonsillar
falx
tentoriumforamen magnum
SUBFALCINE HERNIATION Subfalcine herniations occur as the brain
extends under the falx in the supratentorial cerebrum.
Herniating tissue:Cingulate gyrus herniates under the anterior falxCompression:Anterior cerebral artery
Subfalcine herniations can present clinically as headache. Later on as the herniation progresses, contralateral leg weakness can occur.
Complications of subfalcine herniations include ipsilateral anterior cerebral infarction.

Figure 56.1. Herniation syndromes: (A) subfalcine and cingulate,
(B) uncal, (C) foramen magnum Subfalcine herniation occurs
when one cerebral hemisphere is displaced under the falx cerebri across the midline(A)
. Uncal herniation refers to displacement of supratentorial structures inferiorly under the tentorium cerebelli, causing distortion and compression of the blood supply to infratentorial structures(B)
Downward herniation of the cerebellum causes compression of the brainstem (C).

Lateral Transtentorial (uncal) herniation
A descending transtentorial herniation occurs when the supratentorial brain herniates downward through the incisura.
C/F 1) Ipsilateral dilatation of the pupil and abnormal
extraocular movements.2) Contralateral hemiparesis 3) Ipsilateral hemiparesis also can occur (Kernohan
notch) 4) The thalamic area herniates down over the tentorial
notch. This can lead to decorticate posturing during which the individual's body is in an extended position but the arms and wrists flew in response to pain.

Complications • Unilateral or bilateral occipital lobe infarction
-compression of the posterior cerebral artery.
• Brainstem hemorrhage(durette hemorrhage) -compression or kinking of pontine perforating vessels.
• Compression on the midbrain (compression of aqueduct or perimesencephalic cistern)may cause hydrocephalus.

Central Transtentorial herniation
Herniating tissue:Downward displacement of one or both cerebral hemispheres
Compression:Diencephalon and midbrain through tentorial notch
ICP is usually raised
Bilateral decorticate or decerebrate posturing

Ascending Transtentorial Conversely, an ascending transtentorial
herniation occurs when the infratentorial brain herniates upward through the incisura.
Ascending transtentorial herniation causing brainstem compression can cause nausea and vomiting, which may progress rapidly to coma if rapid changes occur in the intracranial anatomy.

Foramen magnum
Increased pressure in the posterior fossa leads to brainstem compression
Herniating tissue:Downward mesial displacement of cerebellar hemispheres
Compression:Unilateral or bilateral medulla by ventral parafollicular or tonsillae through foramen magnum
. Loss of consciousness from compression of reticular activating
system Episodic tonic extension with opisthotonic posturing, leading to
quadriparesis. Focal lower cranial nerve dysfunction.
Respiratory and cardiovascular function can be significantly affected early.
Changes in blood pressure, heart rate, and arrhythmias Ataxic breathing Small pupils and disturbance of conjugate gaze
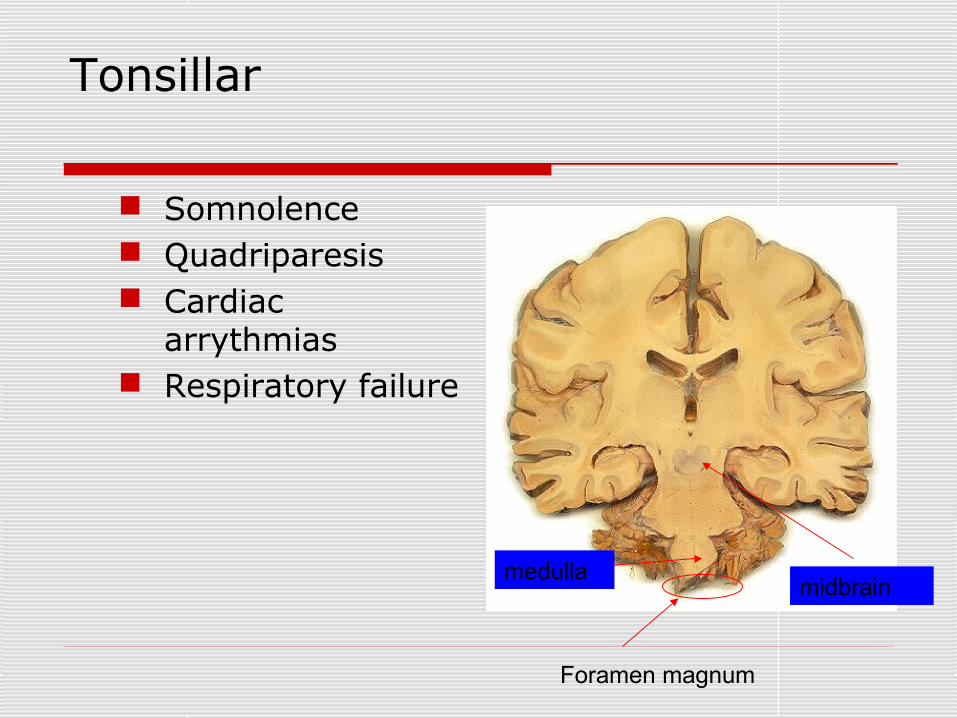
Tonsillar
Somnolence Quadriparesis Cardiac
arrythmias Respiratory failure
midbrainmedulla
Foramen magnum

Pathophysiology
The MONRO-KELLY doctrine: volume of intracranial vault is constant.
Fixed volume : Brain (80%),CSF (10%),Blood(10%)
CPP = MAP – ICP

Pathophysiology of increased ICP
Increased brain volume: vasogenic edema cytotoxic edema interstitial edema

Regulation of cerebral blood flow
Cerebral oxygen delivery = CBF x CaO2
Determinants of CBF1) CPP2) CMRO2
3) PaCO2
4) PaO2

Management of Increased Intracranial Pressure
Airway Management GCS < 8 require intubation to protect
airway
Hemodynamically stable : Thiopental and Propofol
Hemodynamically unstable : Etomidate

Head Positioning
Elevate head of bed to 15 to 30%
Head should be kept in midline

Temperature Control
1) Temperature can be lowered with Acetaminophen and cooling blankets
2) Shivering prevented by Neuromuscular blocked

Hemodynamic Management
1) Infants upto 1 year : CPP > 50 mm Hg
2) 1 to 10 years : CPP > 60 mm Hg3) Older than 10 years : CPP > 70 MM
Hg Initial fluid of choice is 0.9% NaCl Serum Sodium maintained between
140 to 150

Seizure Management
1) Lorazepam 0.1 mg/kg every 10 min2) Loading dose of phenytoin 20mg/kg

Analgesia, Sedation & NM blockade Analgesia : Opoid like Fentanyl and Morphine Sedation : Benzodiazepines like Lorazepam and Midazolam
Both classes cause HYPOTENSION
NM block : Pancuronium and vecuronium

Ventilator management
Normoxia ( PaO2 of 80 – 120 mmHg)
Normocapnia (PaCO2 of 35 – 40 mmHg)

Specific Therapies
Manitol Osmotic diuretic Mechanism1) Rheologic2) Osmotic
Adverse affect 1) Intravascular volume deplecent2) ARF

Glycerol Glycerol acts in a similar fashion but is used less often.
Glycerol has the advantage of being a physiologic agent with caloric value, which is beneficial for nutritional support.
Because glycerol has less diuretic effect and is not dependent solely on renal function, it can be given to patients with renal insufficiency.
The main side effect is intravascular hemolysis, which can be prevented by giving a low concentration (< 20%) at a slow infusion rate (>1 hour).
Glycerol is most effective via enteroduodenal administration.
Direct oral intake or gastric tube administration is less effective.
Glycerol is usually given as a continuous drip.

Hypertonic saline A more recent treatment for increased ICP is IV administration of 3–
23.4% hypertonic saline. IV boluses can reduce ICP and augment CPP for several hours.
Creates an osmotic gradient and draws water from the intracellular and extracellular spaces into the intravascular compartment
No immediate concern exists for volume depletion, as can occur with mannitol.
Potential side effects Hyperosmolar central pontine myelosis Congestive heart failure Subdural hematomas Coagulopathy (rarely)
The trauma guidelines recommend: Continuous infusion of 3% saline between 0.1 and 1.0 mL/kg/hour Administration on a sliding scale, with the minimal dose needed to
maintain ICP under 20 mm Hg Serum osmolarity should be maintained below 360 mOsm/L when
using hypertonic saline as the only hyperosmolar therapy, to control brain edema
Barbiturate Therapy
Pentobarbital 5 mg/kg
Burst suppression correlates with maximal metabolic suppression

Hyperventilation
1) Lowers ICP by causing cerebral vasoconstriction, which decreases CBV
2) Moderate hyperventilation, achieving carbon dioxide tensions between 25 and 35 prevents excessive CBF
Surgical Decompression
Lowers ICP by increasing intracranial volume

Future trends
In the future, cerebral protectants may be part of the cocktail in the initial emergent management of acutely increased ICP. Free radical scavengers Excitotoxic amino acid antagonists Lazeroids N-methyl-D-aspartate-receptor
antagonists
