rapidarc in bergen britt nygaard, harald valen and ellen wasbø haukeland university hospital,...
TRANSCRIPT
RapidArc in Bergen
Britt Nygaard, Harald Valen and Ellen Wasbø
Haukeland University Hospital, Bergen, Norway
2
• 2007: – Trilogy with RapidArc option
• 2008: – Scandidos Delta4 QA tool– Aria upgrade: RapidArc on the Trilogy and 23iX
• Autumn 2009: – Course in Bellinzona and Zug– Stay-and-learn in Copenhagen– Eclipse AAA configuration– Machine QA and patient QA procedures
• 2010:– Decisions, decisions.. Which category of patients?– Learning RapidArc doseplanning in Eclipse– 1st patient on 14th of June – 2nd on 22nd of November
3
Quality control
• Commisioning tests as suggested by Memorial Sloan-Kettering CC and Varian– A picket fence test during RapidArc– 7 adjacent fields with varying Dose rate & Gantry
speed– 4 adjacent fields with varying MLC speed & Gantry
speed
– Possible to study combined effect of • dose rate and gantry speed• dynamic MLC and variable dose rate
C. C. Ling et. al: Commissioning and Quality Assurance of RapidArc Delivery System. Radiotherapy, Int. J. Radiation Oncology Biol. Phys., Vol. 72, No. 2, pp. 575–581, 2008.
4
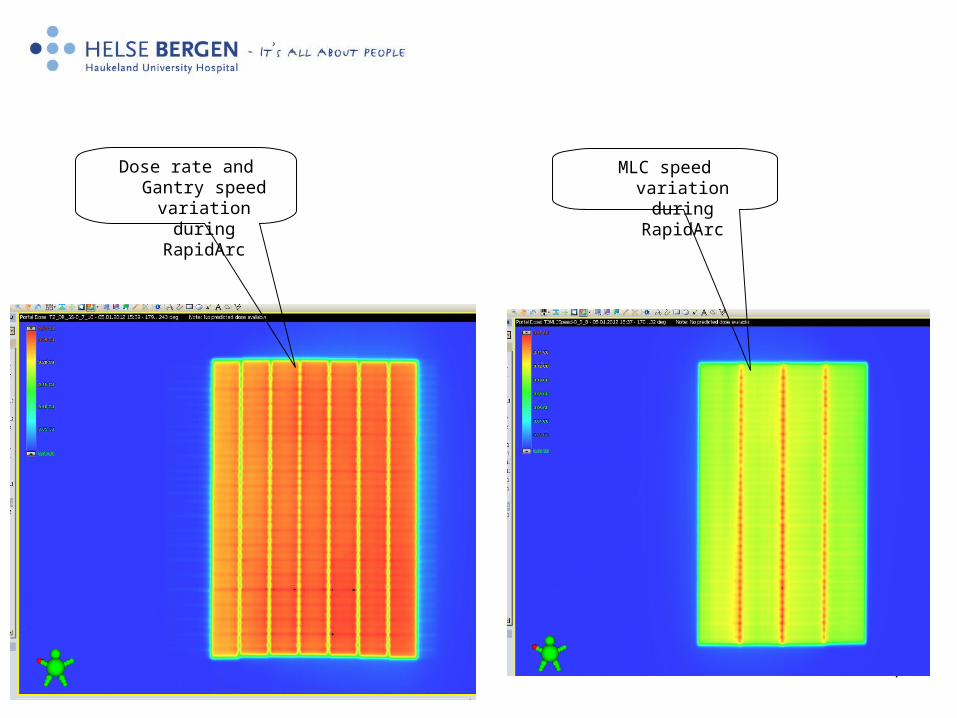
MLC speed variation during RapidArc
Dose rate and Gantry speed variation during RapidArc
5
Analyse results
• MLC speed variation (”Test3”)
• Dose rate and Gantry speed variation (”Test2”)
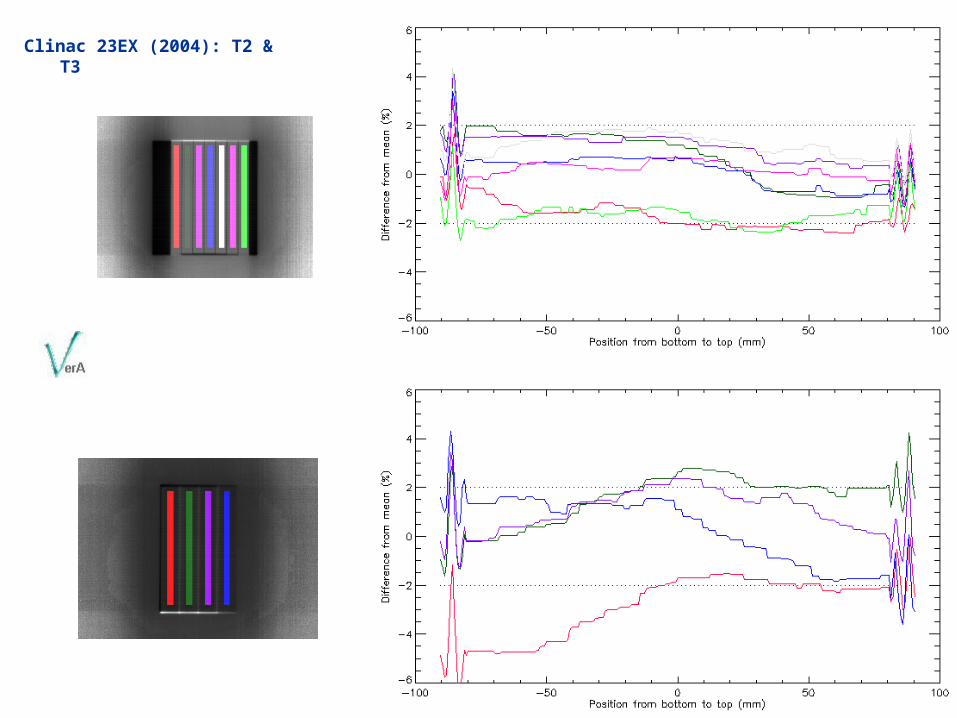
Clinac 23EX (2004): T2 & T3
7
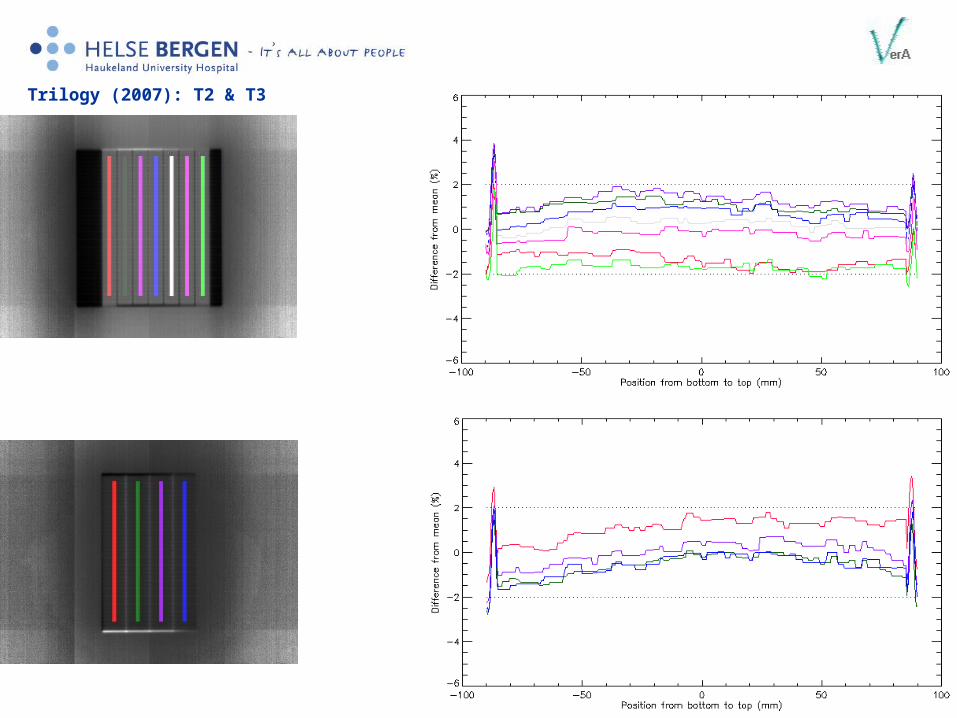
Trilogy (2007): T2 & T3

8
Clinac 23iX (2005): T2 & T3

9
TrueBeam (2011): T2 & T3
10
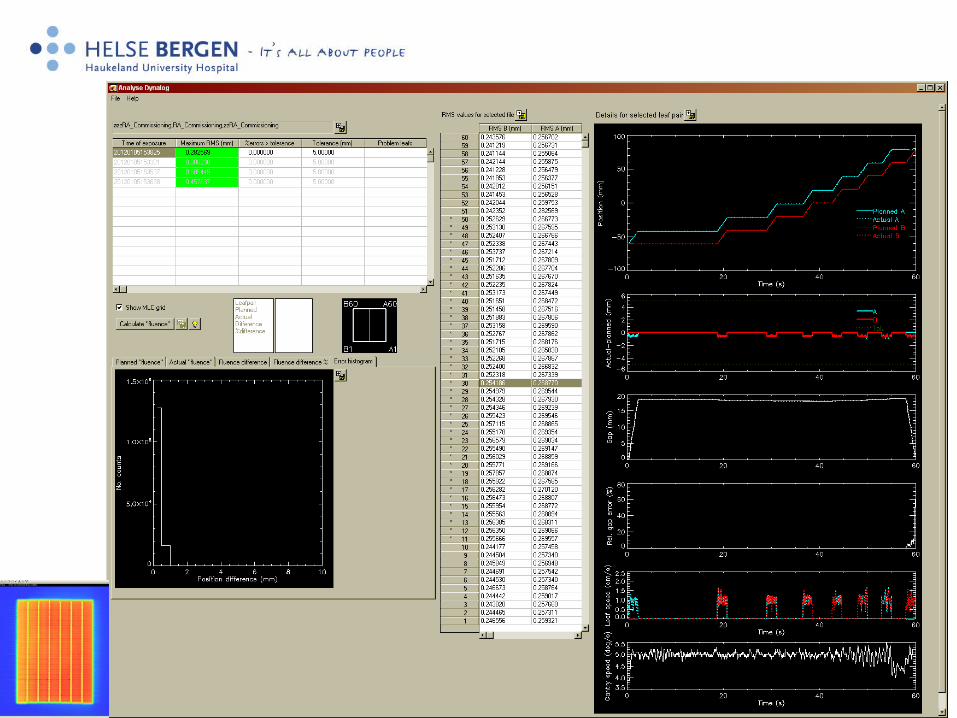
Analyse results• Dynalog files
– Log planned and actual leaf positions and leaf speed vs. time
– Log gantry speed vs. Time– How TrueBeam
• Tool: ”Analyse Dynalog”– In-house developed (EW)– Language: IDL
11
12
Patient QA
• Delta4– Daily dose correction– Run and measure Verification plan– Pass / Fail criteria
• Dose deviation– > 85% within ±3% deviation
• Distance to agreement– > 98% with DTA ≤ 3mm
• Gamma index 3%, 3mm– > 95% with index ≤ 1

13
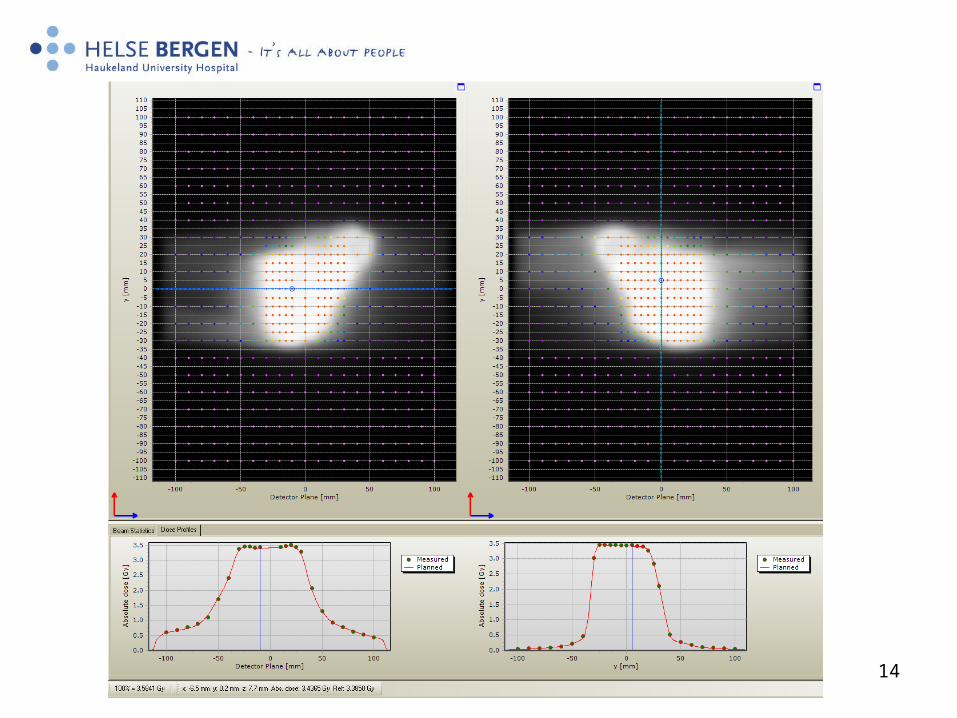
1 arc, 135° to 225°, TrueBeam 6MV photons
14
15
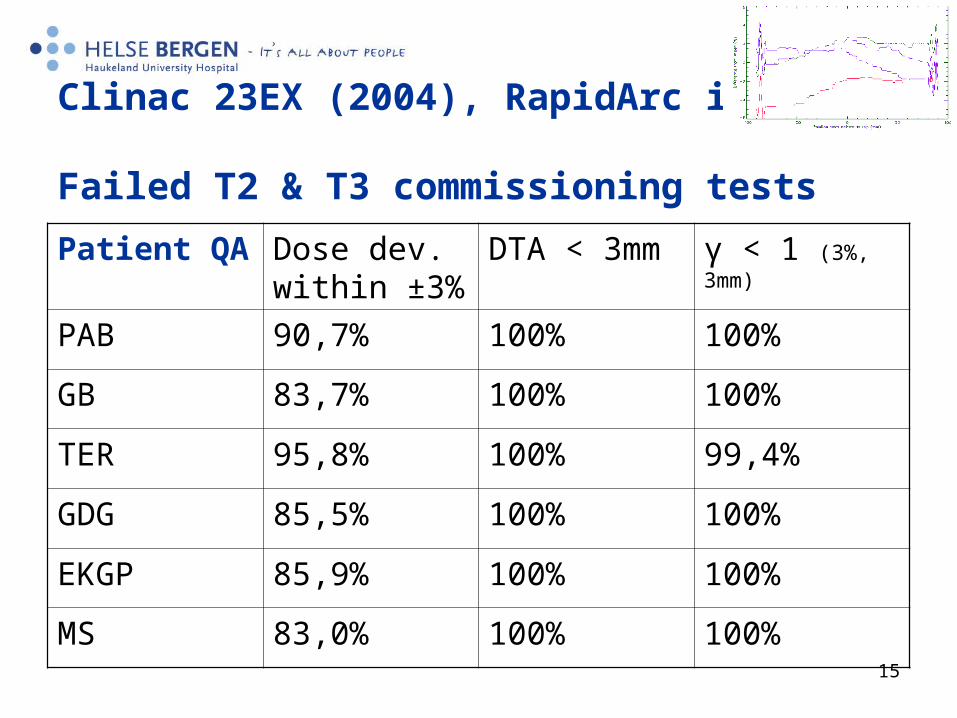
Clinac 23EX (2004), RapidArc in 2011: Failed T2 & T3 commissioning tests
Patient QA Dose dev. within ±3%
DTA < 3mm γ < 1 (3%, 3mm)
PAB 90,7% 100% 100%
GB 83,7% 100% 100%
TER 95,8% 100% 99,4%
GDG 85,5% 100% 100%
EKGP 85,9% 100% 100%
MS 83,0% 100% 100%
16
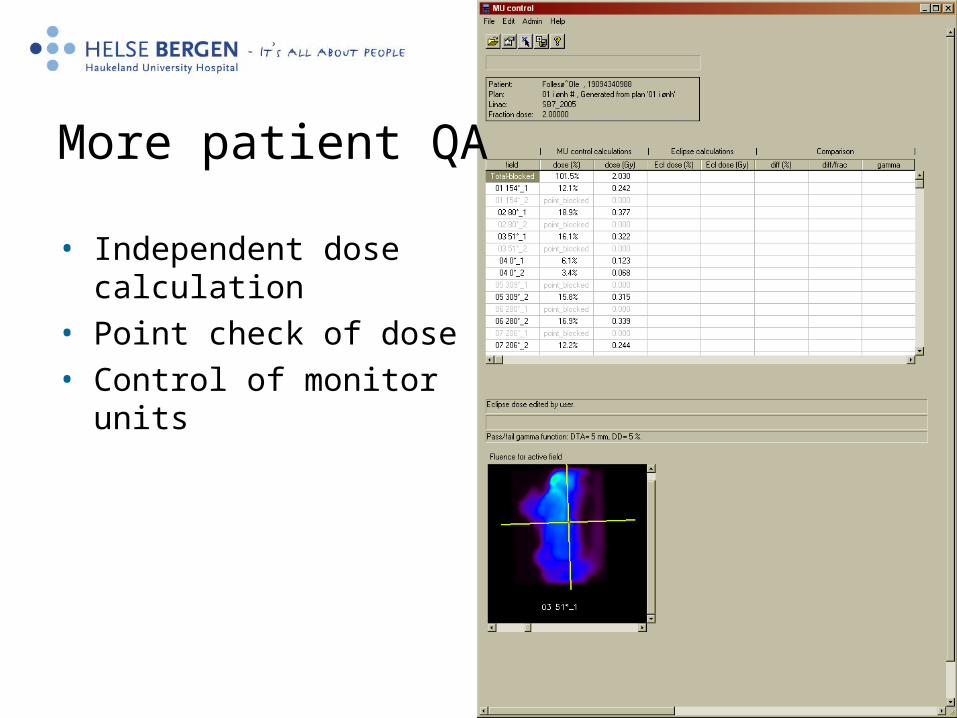
More patient QA
• Independent dose calculation
• Point check of dose• Control of monitor units
17
Treatment planning, Autumn 2010:
• 5 years experience with IMRT– head and neck– prostate with and without lymph nodes (LN)– ani (and gyn) with LN – Sarcoma, lymphoma and other
• RA configuration and acceptance tests OK • RA installed on 2 Clinacs • Patient start up
18
Which patient groups?
• Increased efficiency for the department – Prostate with LN, 7 splitted fields
• Patients unable to keep the supine position for 10-15 min– Head and neck
• Less MU and less risk for secondary cancer• A category that is easy to create acceptable and
standardized plans for– Prostate intermediate risk

19
Which patient groups?
• Increased efficiency for the department – Prostate with LN, 7 splitted fields
• Patients unable to keep the supine position for 10-15 min– Head and neck
• Less MU and less risk for secondary cancer• A category that is easy to create acceptable and
standardized plans for– Prostate intermediate risk

20
Prostate intermediate risk, criteria:• Treatment of prostate and seminal vesicles
• Equal plan or better than IMRT (PTV and rectum)
• We made two plans, one IMRT (backup) and one RA, 1 arc 135-225° (avoid couch slides) for the 10 first patients
• PTV 95%-107%, median 100%,
• Rectum: max 10ml >60 Gy and less than 50 Gy to half the circumference
• Delta4 measurements OK; • Gamma index 3%, 3mm
– > 95% with index ≤ 1
• Dose deviation– > 85% within ±3% deviation
21
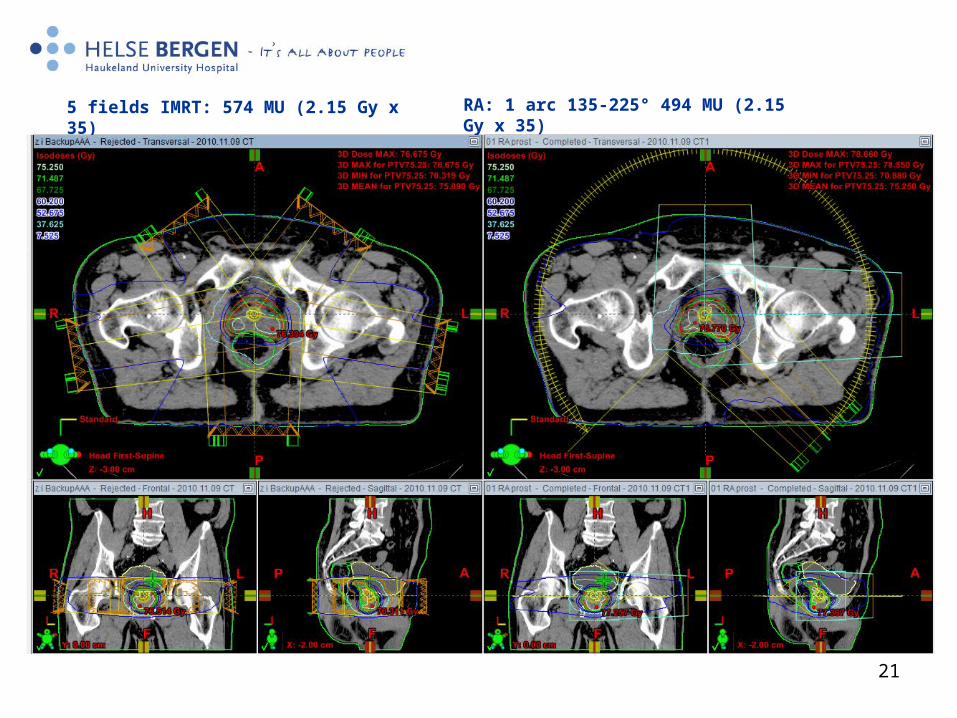
5 fields IMRT: 574 MU (2.15 Gy x 35) RA: 1 arc 135-225° 494 MU (2.15 Gy x 35)
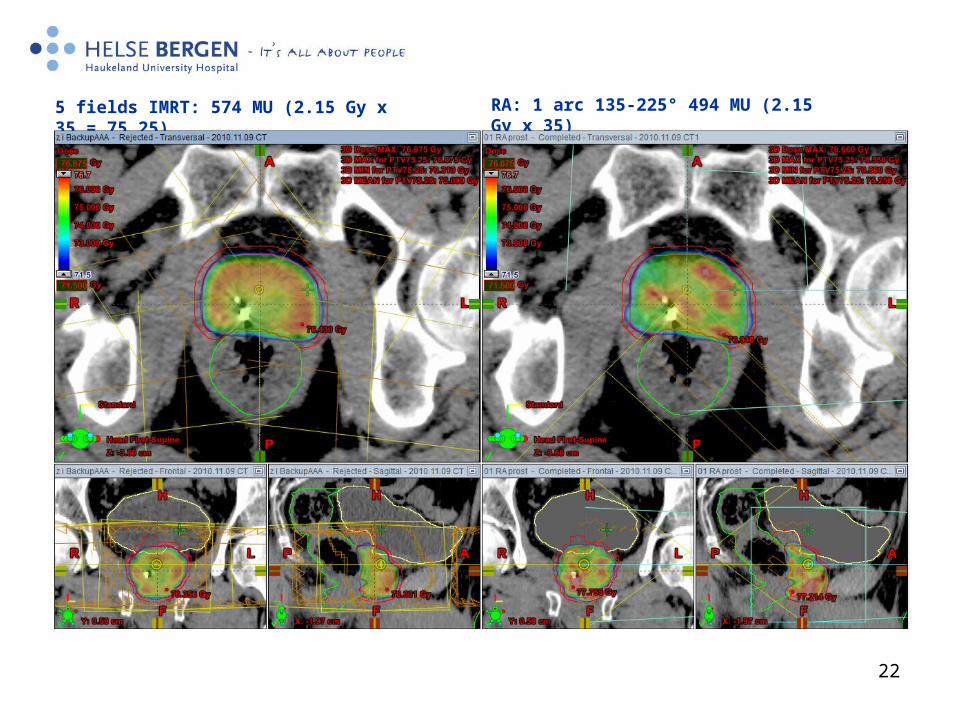
22
5 fields IMRT: 574 MU (2.15 Gy x 35 = 75.25) RA: 1 arc 135-225° 494 MU (2.15 Gy x 35)
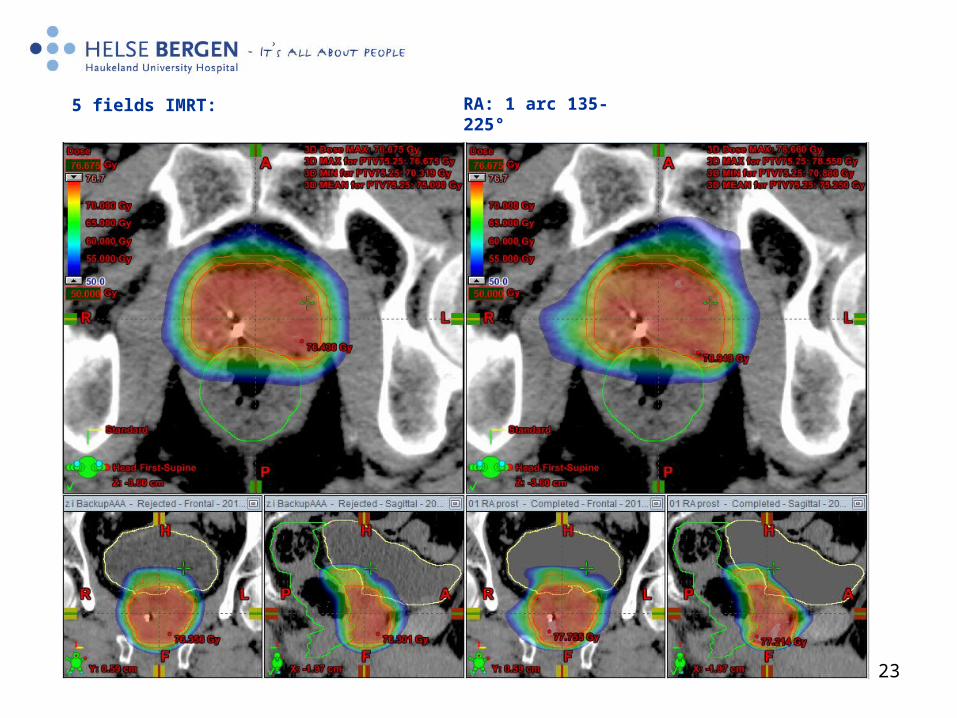
23
5 fields IMRT: RA: 1 arc 135-225°

24
IMRT
RA

25
RA today: (2.4 Gy sem.ves. and integrated boost 2.7 Gy prostate) x 25 = 67.5 Gy (EQD2= 81 Gy if α/β=1.5)

26
27
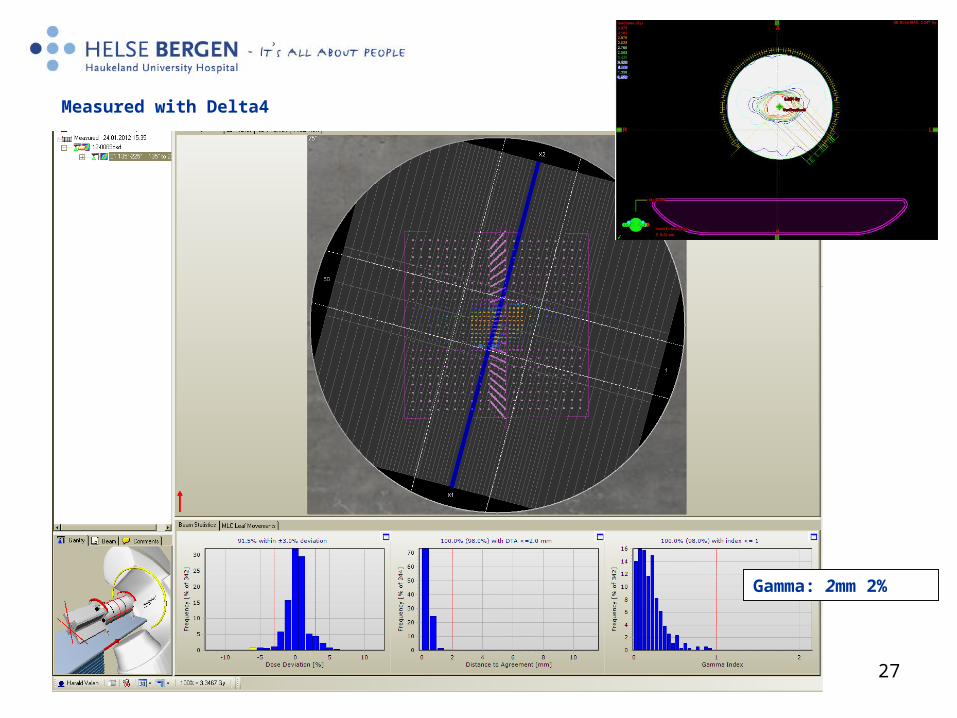
Gamma: 2mm 2%
Measured with Delta4
28
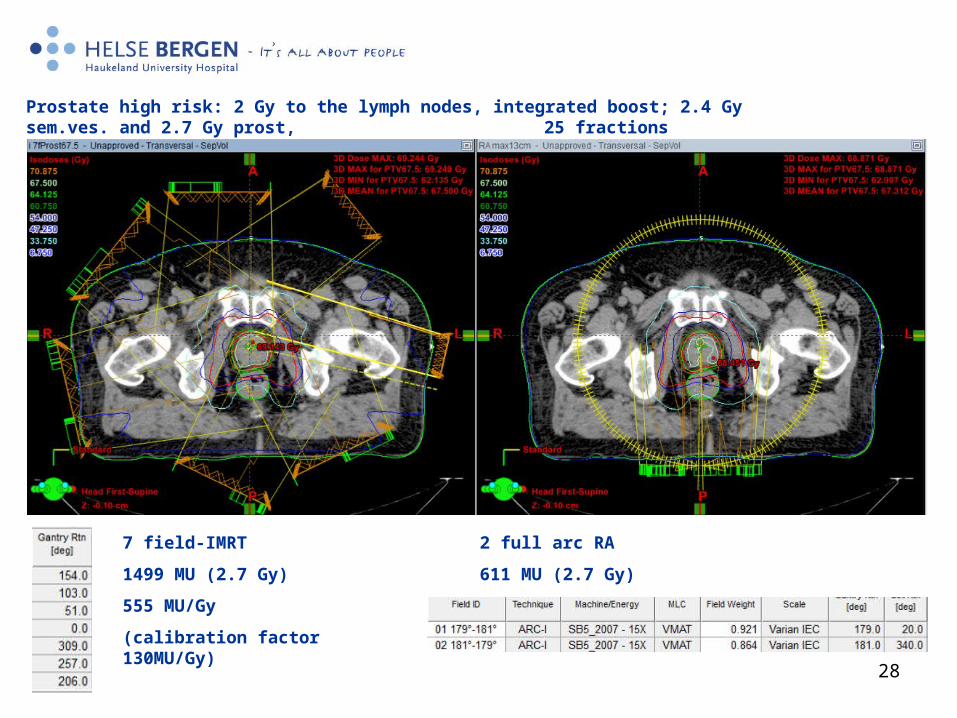
7 field-IMRT
1499 MU (2.7 Gy)
555 MU/Gy
(calibration factor 130MU/Gy)
2 full arc RA
611 MU (2.7 Gy)
Prostate high risk: 2 Gy to the lymph nodes, integrated boost; 2.4 Gy sem.ves. and 2.7 Gy prost, 25 fractions
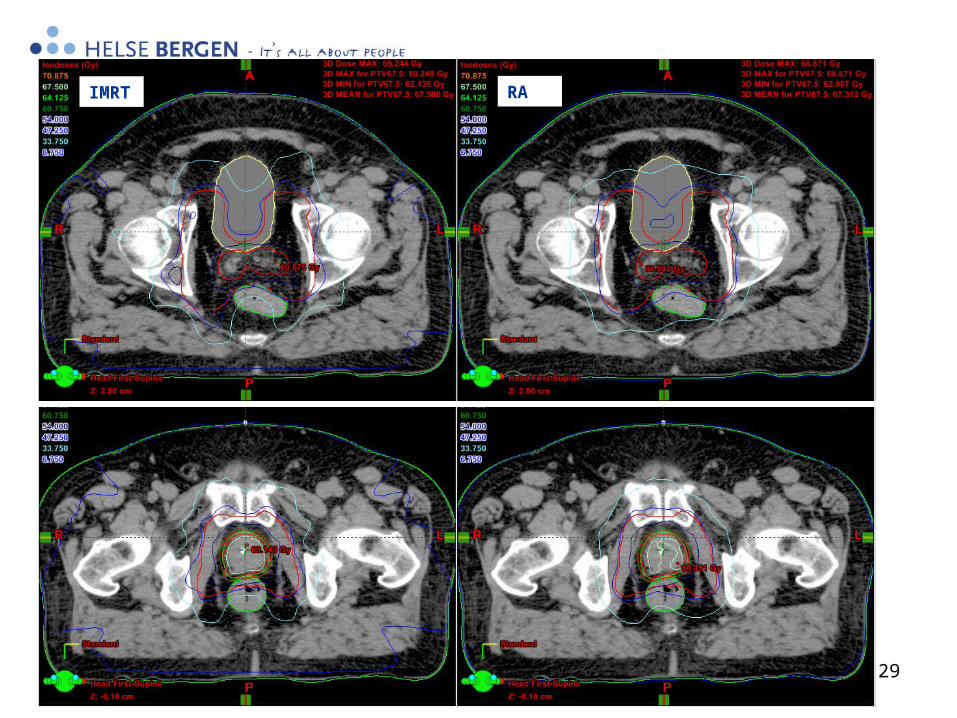
29
IMRT RA
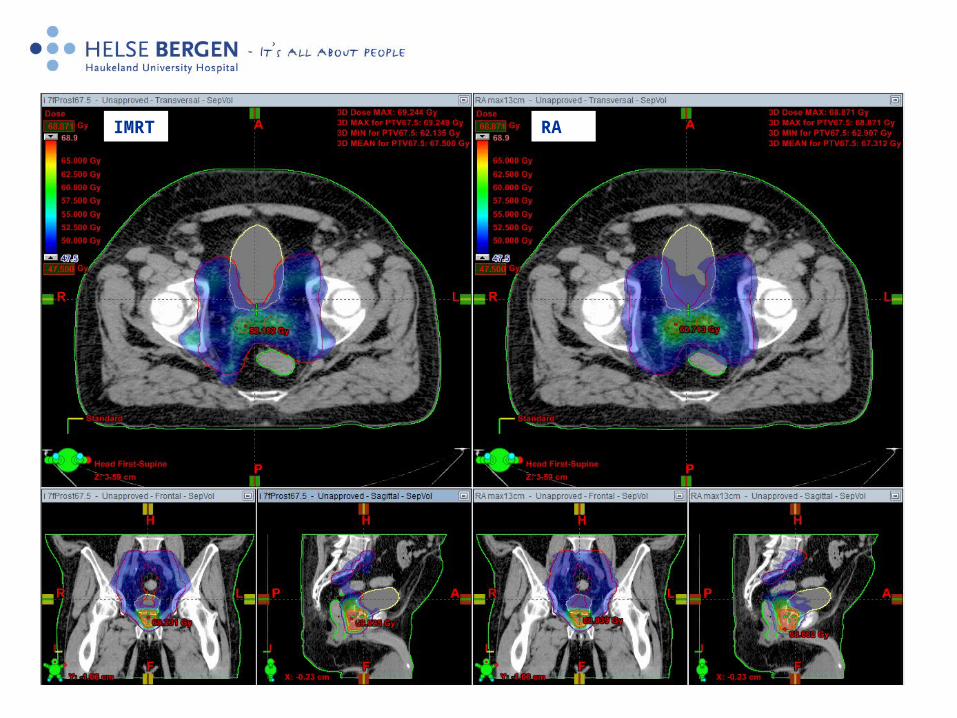
30
IMRT RA
31
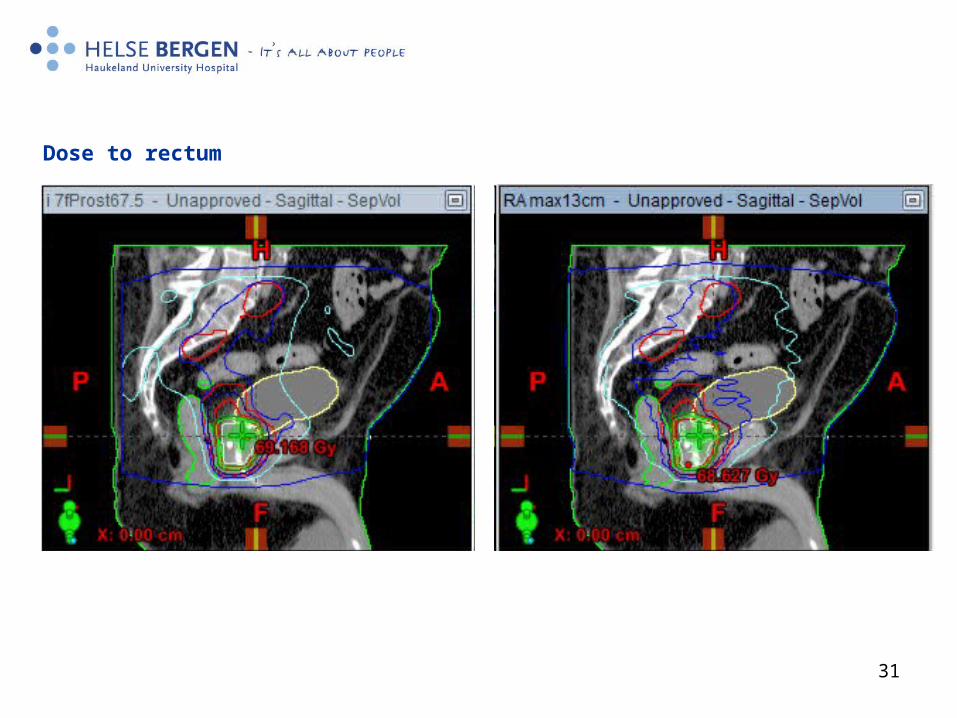
Dose to rectum
32
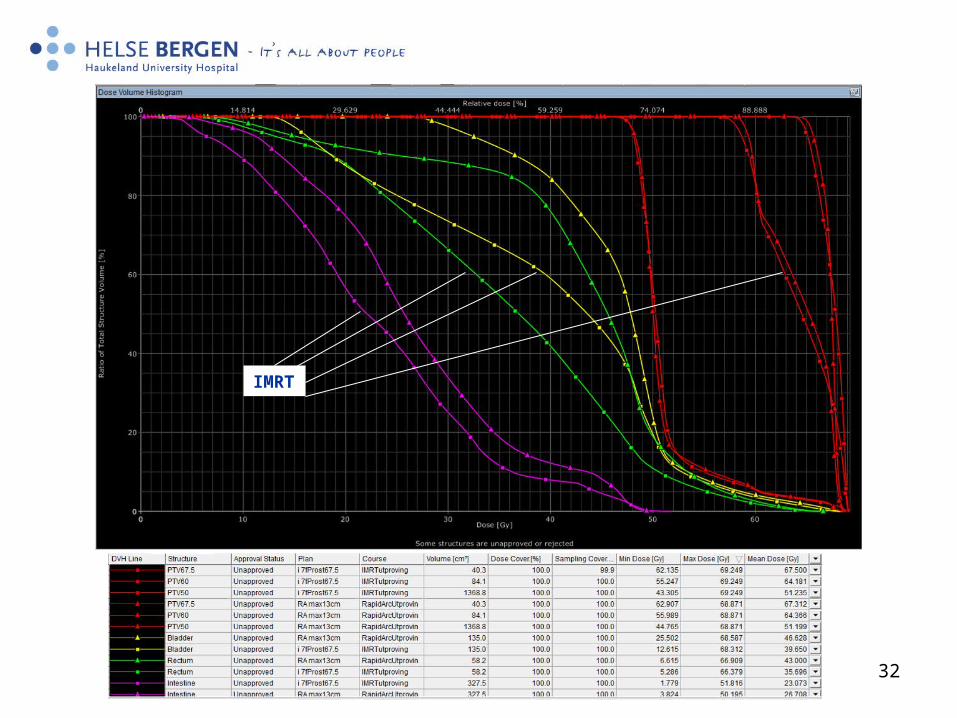
IMRT
33
Future:
• We would like to treat our high risk protate with LN with two arcs– Prerequisite: RA plan equal or better than IMRT (PTV and
rectum)
• This autumn we have been focusing on commissioning TrueBeam..