rcpath - bac
TRANSCRIPT

Cytopathology Study Day
16 April 2017
Guy’s Hospital London
RCPath - BAC
Digital cytology: EUS FNA
pancreas and head and neck
R. Dina MD, FIAC, FRCPath
Consultant Cyto/Histopathologist
Hon Sen Lecturer
Hammersmith Hospital
Imperial College NHS Trust
Advantages of whole slide imaging in cytopathology practice. From :Patholog Res Int. 2011; 2011: 264683. Walid E. Khalbuss, 1, 2 * Liron Pantanowitz, 1, 2 and Anil V. Parwani 1
(1) Primary diagnosis (telecytology)
(2) Remote second opinion consultation
(3) Educational activity within the institution or remotely
(4) Archiving interesting and legal cases (digital cytology slides replication)
(5) Quality assurance
(6) Educational conferences such as tumor boards (locally or remotely)
(7) Online cytology proficiency testing
(8) Online board exam or certification
(9) Detailed image analysis and cytomorphometry
(10) Annotation of various entities on the slides for teaching purpose
(11) Easy acquisition of static images from whole-slide images
(12) Provide cytopathology services to remote hospitals
(13) Gains access to cytology subspecialty expertise
(14) Remote on-site evaluation and triage
(15) Synchronous consultation
Disadvantages of whole slide imaging in cytopathology practice
(1) Costly: an expensive initial setup and storages
(2) Limited focusing functions at present
(3) Scanning time
(4) Storage: large file size
(5) Training requirements
(6) Limited validation studies
(7) Lack of standardization: multiple vendors, software, and lack of interoperability
(8) Information technology infrastructure support (bandwidth limitation of networks)
(9) Professional reluctance to adopt
Patholog Res Int. 2011; 2011: 264683.
Walid E. Khalbuss, 1, 2 * Liron Pantanowitz, 1, 2 and Anil V. Parwani 1
1Division of Pathology Informatics, Department of Pathology, University of Pittsburgh Medical Center, Pittsburgh,
PA 15232, USA2Division of Cytology, UPMC Shadyside Hospital, 5150 Centre Avenue, POB2, Suite 201, Pittsburgh, PA 15232, USA

Use of Digital Imaging At Imperial College we have been using in the past fixed digital
images for
cytology tests during our MSc in Cytopathology
Cytology mock exams during our Advanced Courses which prepare for the MRCPath examination
WSI for research purposes and testing.
We currently informally review WSI of cases but we do not issue a formal report on them. This is because although technology on the different platforms available on the market has markedly improved we do not feel that there is an agreed standardised practice for it.

Conclusions WSI is here to stay and is fast improving and getting
cheaper
It is an important teaching and training tool
It is used for EQA schemes and Quality Assurance
It is used in MDT meetings (Tumour Boards)
It helps retaining a screening component to all
assessment tests
BUT…… it is one of the many tools!

Digital Histology vs digital
Cytology
Digital Histology and digital Cytology need a different
technical approach for many reasons

Digital Histology vs digital
Cytology Dimension:

Digital Histology vs digital
Cytology Dimension:

Digital Histology vs digital
Cytology The nature of the material is different:
Histology
Cytology

Digital Histology vs digital
Cytology The microscopy is different:
A histological slide requires minimal focus adjustment
Micro focusing is the “essence” of cytological screening

Digital Histology vs digital
Cytology The scanning technique is different:
If the scanner autofocus works well, a single layer virtual
slide allows a high quality screen of a histological
preparation.
A multi level scanning is compulsory to get an acceptable
cytological virtual slide.
Digital Histology vs digital
Cytology
Digital Histology vs digital
Cytology In essence:
Digital Histology is two dimensional
Digital Cytology is three-dimensional.
This entails at least four problems.
Digital Cytology: a 3D
problem The first:
How many levels are needed to define "acceptable" a
virtual slide?
An immediate and seemingly logical answer is:
The more the better

Digital Cytology: a 3D
problem The second problem:
Which is the optimal distance between each level?

Digital Cytology: a 3D
problem
Strictly related to the first two
parameters comes the third problem:
the size of the file.
Digital Cytology: a 3D
problemThe relationship between file dimension and number of levels is linear.
Just for example:
In four years in the Ljnkoeping University Hospital Pathology department (Sweden) about 1 000 000 histological slides have been scanned . The space occupied is 400TB.
The same number of cytological cases scanned with just 5 levels would need
400 x 5 TB = 2000TB
Actually a huge amount of space!
Digital Cytology: a 3D
problemFinally the fourth problem: the time needed for a multi level
scanning.
A 20x20 mm wide area can be scanned in about 50
seconds.
The same area scanned with 5 z-stack levels takes more
than 4 minutes
Digital Cytology: a 3D
problemThis technique consists 3 steps:
1. dividing in small areas (tiles) the image resulting from the scanning of each level
1. taking the best-focused tile from each layer
1. building a new virtual slide where all the objects result in focus
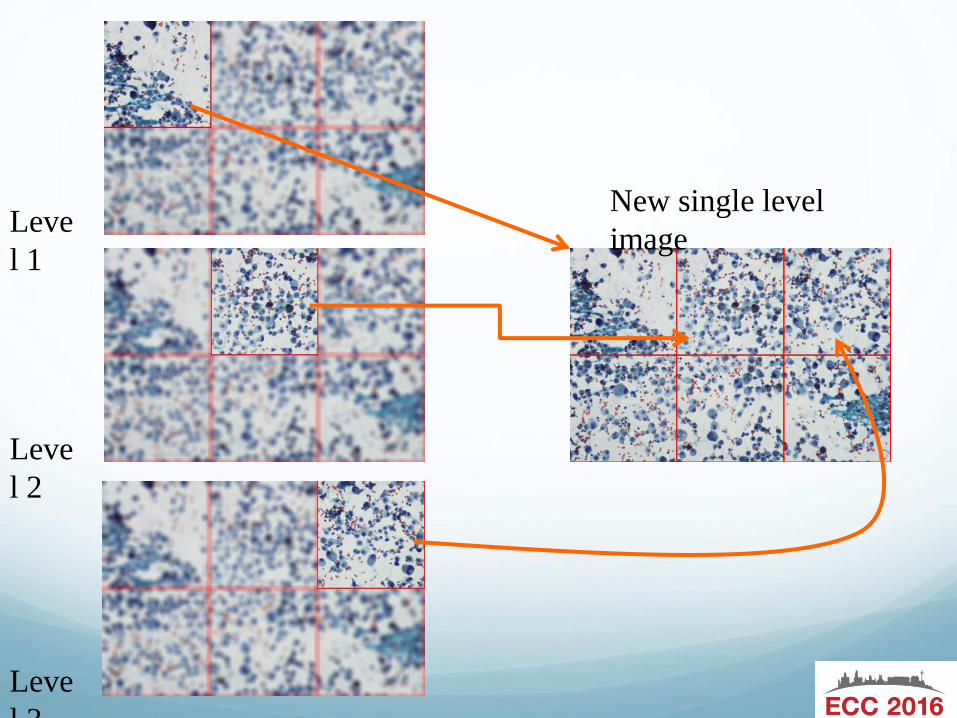
Leve
l 1
Leve
l 2
Leve
l 3
New single level
image
Digital Cytology: a 3D
problemThe final result is a single level virtual slides where all the
tiles are perfectly in focus.
Pros: - small dimension of the file
- good “visual” results
Cons: - long processing time
- a lot of unnecessary data generated

Digital Cytology: a 3D
problem
Digital Cytology: a 3D
problemA second interesting method is proposed in

Digital Cytology: a 3D
problem
A specific software generates during the scanning a three
dimensional focus map of the cells in the slide.
Following this map the scanner takes only the images of the cells
avoiding the generation of unnecessary and unwanted data.

1) The research has used the Google search engine:
www.google.com;
2) Searched nouns as keyword: nouns had to be the
most concise as possible. The used keywords are:
cytology web sites, cytology atlas, cytology and
cytopathology journal, and cytology societies;
How many web sites use
digital cytology?
1) Sponsor, scientific society, personal web page, academic institution or commercial site: whether a website is sponsored by a Society, a particular product or interest group, the owner of the web site. Personal web page web sites can list the author of the information and biographical information.
2) Society: the name of the involved Society.
3) Purpose: to provide educational information, professional advice, promoting the profession of cytologists, encouraging the science of cytology. Many web sites provide information on topics of interest to the owner, as well as tutorials or opinions.
4) Topic: FNA, gynaecologic or non-gynaecology cytology.
5) Target groups: whether the web site is recommended to cytologists, cytotechnologists, cytology trainees or students, laboratory personnel.
Criteria

6) Access: public, only registered members, any payment fees required.
7) Educational resources: each web site has been checked whether with or without educational purpose or to improve academic success.
8) Imaging: static or dynamic as virtual slides.
9) Passive or interactive: some web sites have just slides to look but no possibility to have an interactive approach. Other web sites allow the visitors to take quizzes or view solutions previously hidden, in order to test trainees or students.
Criteria

The number of web sites is about 671,000 results for
each keyword. Sites with only histopathology have
been excluded.
Based on the above mentioned criteria, the number of
web sites considered adequate is 31.
Results
There are numerous web sites available
Aims are different
Few are available in multiple languages
Cytology is notoriously more difficult to
comprehensively scan
Too few web sites are completely free to use
Few offer interactive e-training
However it is getting better all the time!
Conclusions
Incidence of Pancreatic Tumours Ductal adenocarcinoma - 80%
include all the variants, then 90%
Other tumours - 10%
MCN - 2%
PET - 2%
IPMN - 1%
Acinar carcinoma - 1%
Serous cystadenoma - 1%
SPPT - 1%
Pancreatoblastoma
Ductal Adenocarcinoma of the
Pancreas
85% of all pancreatic malignancies
Increasing incidence 4-5000pa in UK
M1.6:1F
55-75 years (average 60)
2% < 40 years

Incidence of Pancreatic Cancer

Ductal Adenocarcinoma of the
Pancreas- Investigations
CA19.9 >70IU/mL
Biopsy -
Core needle (histology)
FNA
Biliary brushings
Why cytology?
Resectable - just take it out?
Medical-legal issues related to a bad outcome with benign
disease
10% of jaundiced patients with an “obvious” malignant mass prove
to have a benign lesion
Potential for lymphoma diagnosis, a non-surgical disease
Cystic lesions
Patient compliance
Why cytology?
Unresectable, just leave it in?
Not all large masses that appear unresectable are ductal
adenocarcinoma
advances in surgical and anaesthetic practices have
improved surgical outcomes even in older, less fit patients
a positive tissue diagnosis is mandatory before
chemotherapy or radiation therapy can be instituted

Pancreatic Mass: Solid or
Cystic? Solid Pancreatic masses
- ductal adenocarcinoma
typical
variant
- chronic pancreatitis
- Acinar cell carcinoma
- pancreatic endocrine tumour
- pancreatoblastoma
Cystic pancreatic masses
- pseudocyst
- serous cystadenoma
- solid pseudopapillary tumour
- mucinous cyst
MCN
IPMN

EndosonographyHigh frequency miniature
ultrasound transducer is
incorporated into the tip of a
conventional endoscope
resulting in enhanced
resolution of the GI wall and
structures with close
proximity to the GI wall

USS advantages
High intrinsic spatial resolution
No ionizing radiation
Inexpensive and easily portable
USS Disadvantages
Gas and bone impede the passage of USS waves
As good as the operator
Types of Echoendoscopes
Radial
Linear
Miniprobes
Advantages of EUS and EUS
Guided FNAB Biopsy
Not percutaneous FNAB
no reported cases of needle tract seeding with EUS FNAB
Small trajectory to target compared to percutaneous method
More sensitive than CT for small masses (0.5 cm vs 2cm)
cost effective relative to CT biopsy
Staging/determining resectability
distant metastases or SMA invasion=unresectable
peripancreatic nodes and accessible liver lesions can be biopsied during the same procedure

Disadvantages to EUS and EUS
Guided FNAB
Expensive equipment
Technically difficult and requires significant
expertise
low tissue yield with inexperience
Currently no good core biopsy method
GI contamination of cytology specimens
particularly a problem with cystic lesions

EUS-guided FNA for diagnosis
of solid pancreatic neoplasms
False –ve results up to 20-40 %
False positive very rare
Optimizing diagnostic yield from
EUS-FNA. Cytopathology June 2013
ROSE increases diagnostic sensitivity and accuracy of
FNA for solid pancreatic masses by up to 10-15 %
Meta-analysis of 34 studies with 3644 patients : ROSE :
p=0.001 for accuracy
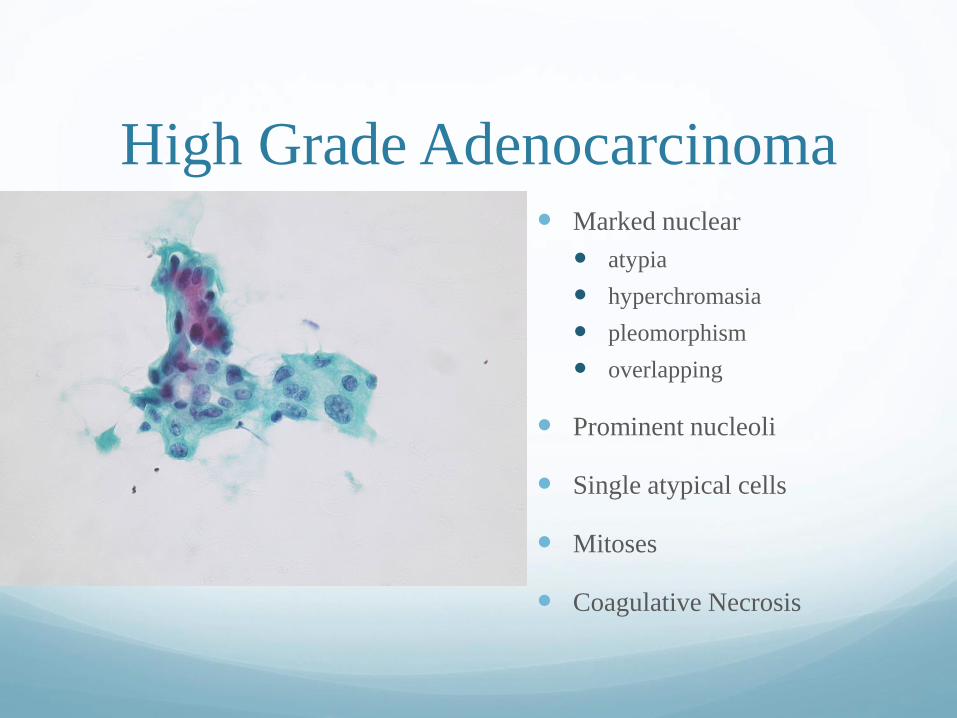
High Grade Adenocarcinoma Marked nuclear
atypia
hyperchromasia
pleomorphism
overlapping
Prominent nucleoli
Single atypical cells
Mitoses
Coagulative Necrosis
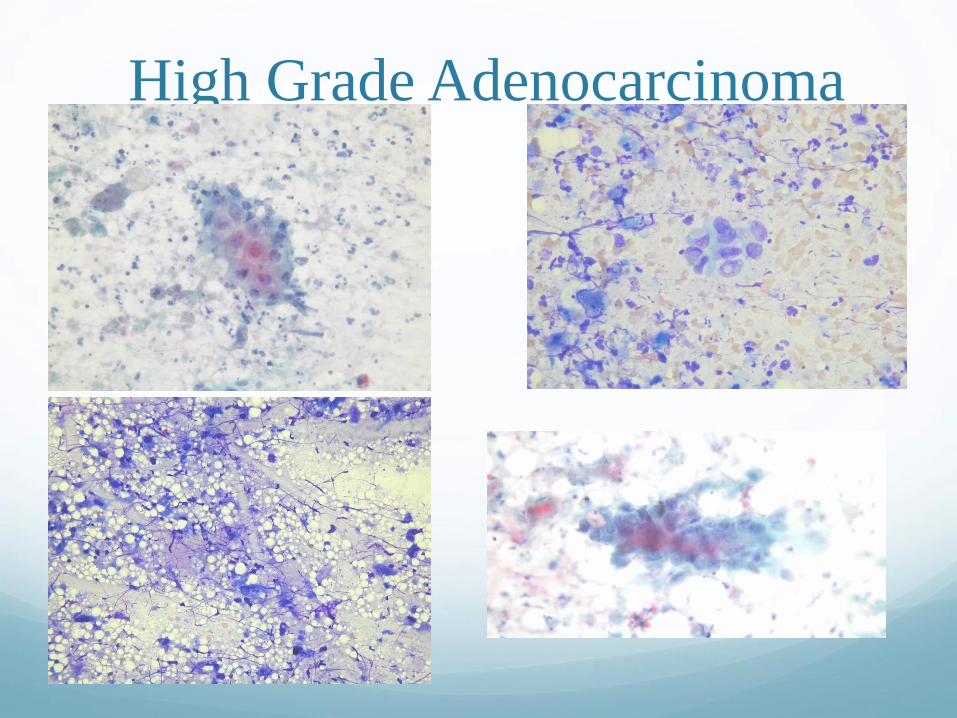
High Grade Adenocarcinoma
win.eurocytology.eu/virtualslides/git-eus/vs-064

Pitfalls
Liver cells
Intestinal cells
Mesothelial cells
Endothelial cells

Early stages of Chronic active
pancreatitis
Both ductal and acinar cells
Background inflammation
Granulation tissue
Fat necrosis

Late Chronic Pancreatitis
• mostly ductal cells
• few to no acinar cells
• some islet cells
• monolayered sheets
• cohesive, few single cells
• maintained polarity
• minimal nuclear overlap
• mild anisonucleosis
• smooth nuclear membranes
• rare/normal mitoses
• no coagulative necrosis
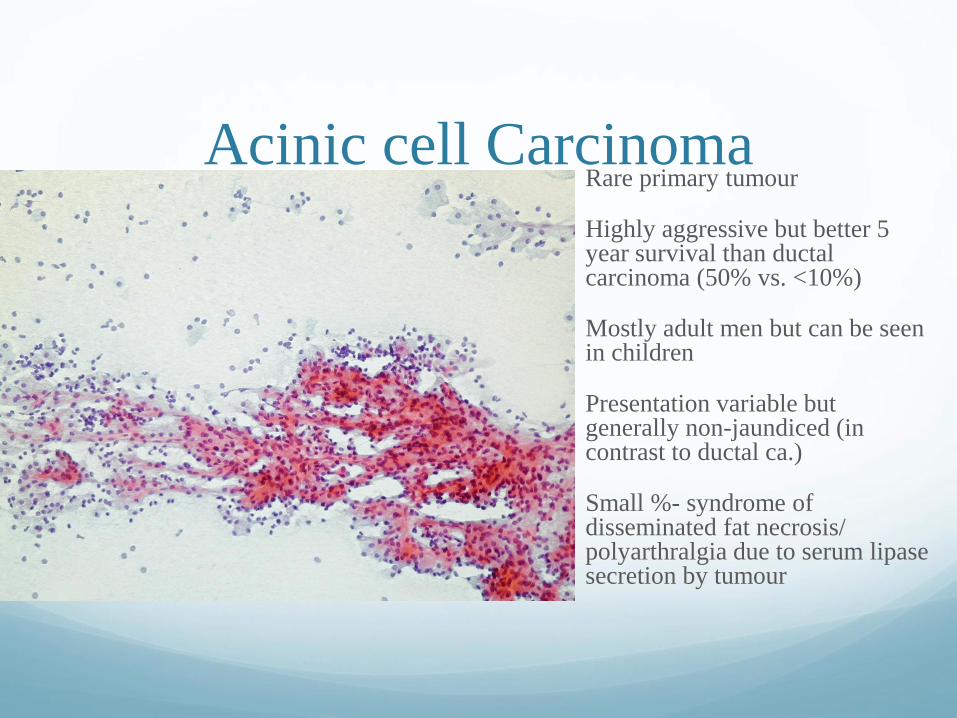
Acinic cell Carcinoma Rare primary tumour
Highly aggressive but better 5 year survival than ductal carcinoma (50% vs. <10%)
Mostly adult men but can be seen in children
Presentation variable but generally non-jaundiced (in contrast to ductal ca.)
Small %- syndrome of disseminated fat necrosis/ polyarthralgia due to serum lipase secretion by tumour


Acinic cell carcinoma
High cellularity
No ducts
No fatty stroma
Poorly formed acini
Variable cells
Atypia variable
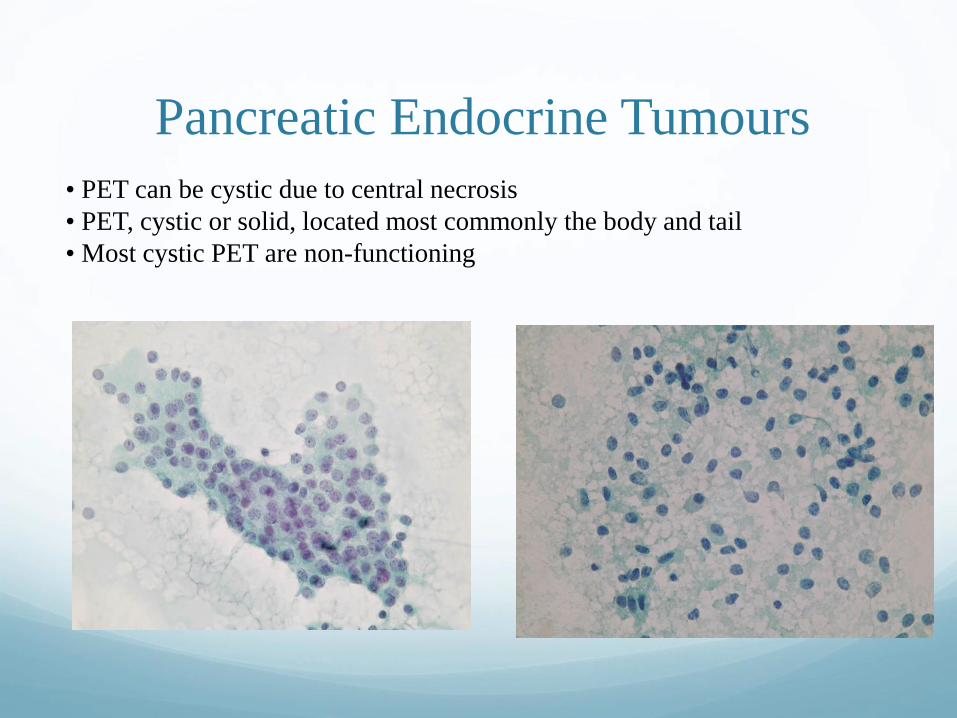
Pancreatic Endocrine Tumours
• PET can be cystic due to central necrosis
• PET, cystic or solid, located most commonly the body and tail
• Most cystic PET are non-functioning

Neuroendocrine Cytology
win.eurocytology.eu/virtualslides/git-eus/vs-052
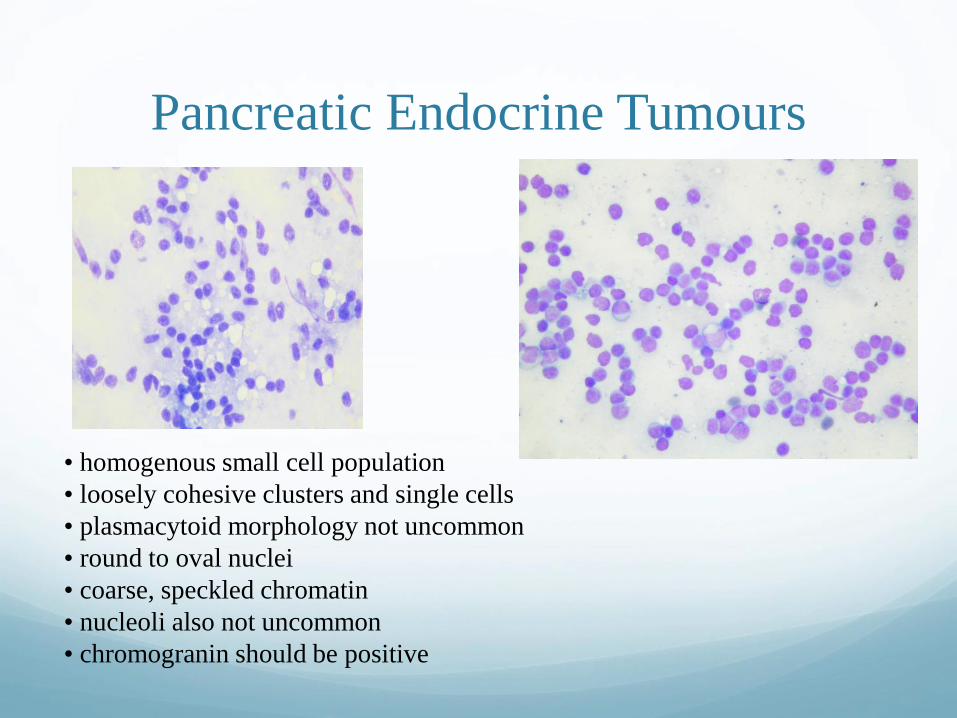
Pancreatic Endocrine Tumours
• homogenous small cell population
• loosely cohesive clusters and single cells
• plasmacytoid morphology not uncommon
• round to oval nuclei
• coarse, speckled chromatin
• nucleoli also not uncommon
• chromogranin should be positive
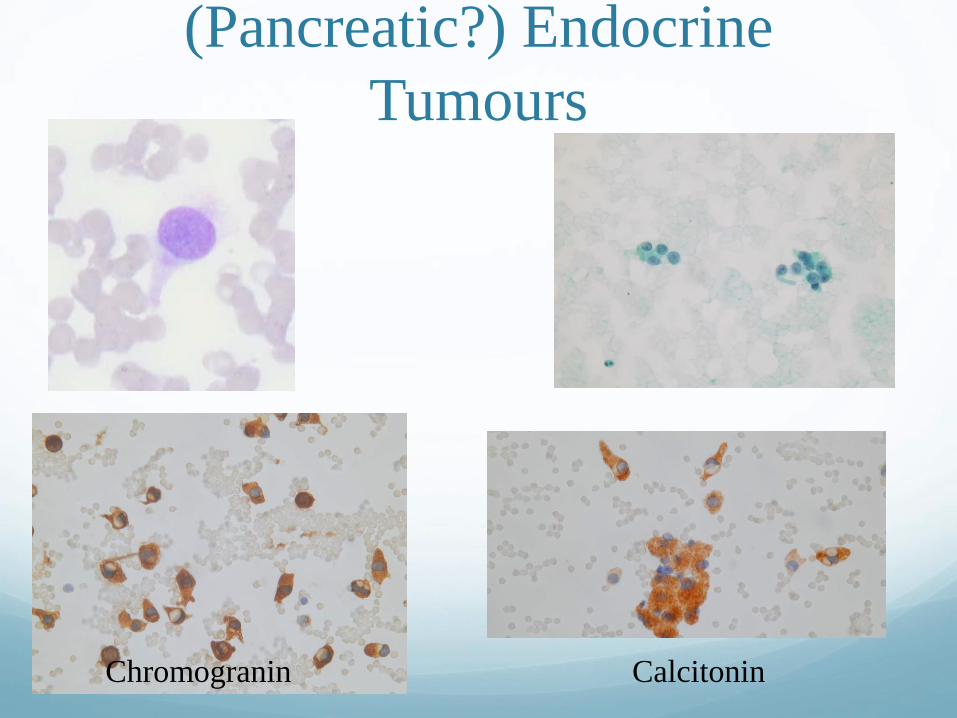
(Pancreatic?) Endocrine
Tumours
Chromogranin Calcitonin
Pancreatic cysts(most common and clinically relevant)
Pseudocyst
Serous cystadenoma
Solid pseudopapillary tumour
Mucinous cysts
mucinous cystic neoplasm
intraductal papillary mucinous neoplasm

win.eurocytology.eu/virtualslides/git-eus/vs-097

Pancreatic Pseudocyst
Most common cystic lesion in the pancreas (75-90%)
Associated with pancreatitis, trauma, surgery
Thick walled, unilocular, +/- communication with duct
Fluid aspirated is often dark and not viscous
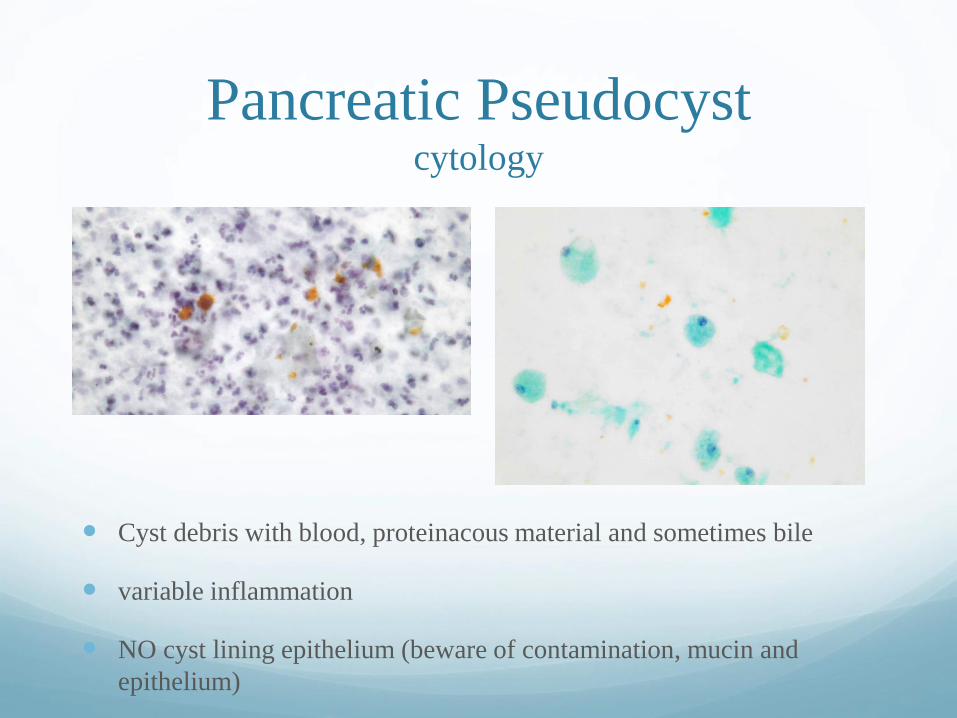
Pancreatic Pseudocystcytology
Cyst debris with blood, proteinacous material and sometimes bile
variable inflammation
NO cyst lining epithelium (beware of contamination, mucin and
epithelium)

Serous Cystadenoma
• benign neoplasm in the head and tail of elderly
men and women
• star-burst calcifications within a central scar
diagnostic on imaging when present, but this is
rarely present
• most tumours are “microcystic” with multiple,
<2cm cysts, but can be unilocular due to specific
variant or due to haemorrhagic degeneration,
causing problems with imaging diagnosis
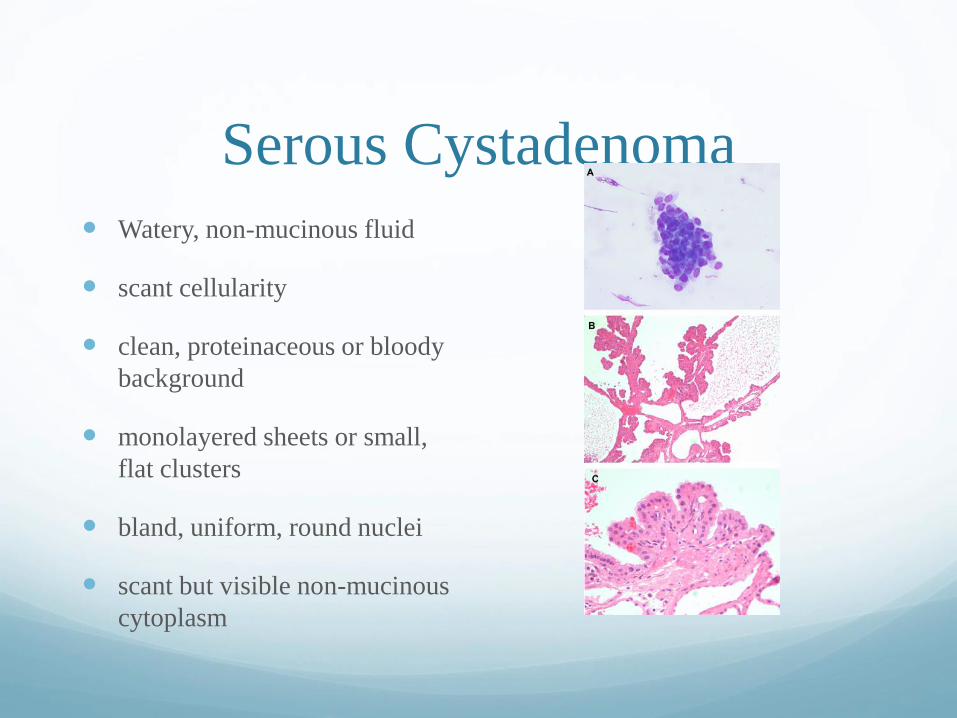
Serous Cystadenoma
Watery, non-mucinous fluid
scant cellularity
clean, proteinaceous or bloody
background
monolayered sheets or small,
flat clusters
bland, uniform, round nuclei
scant but visible non-mucinous
cytoplasm

Mucinous Cysts of the PancreasWHO Classification
Mucinous cystic neoplasm
Mucinous cystadenoma
Borderline mucinous cystic neoplasm
Mucinous cystadenocarcinoma
Intraductal papillary mucinous neoplasm
Intraductal papillary mucinous adenoma
Intraductal papillary mucinous neoplasm of borderline malignancy
Intraductal papillary mucinous carcinoma
Intraductal papillary mucinous neoplasm with invasive carcinoma: tubular type or colloid carcinoma
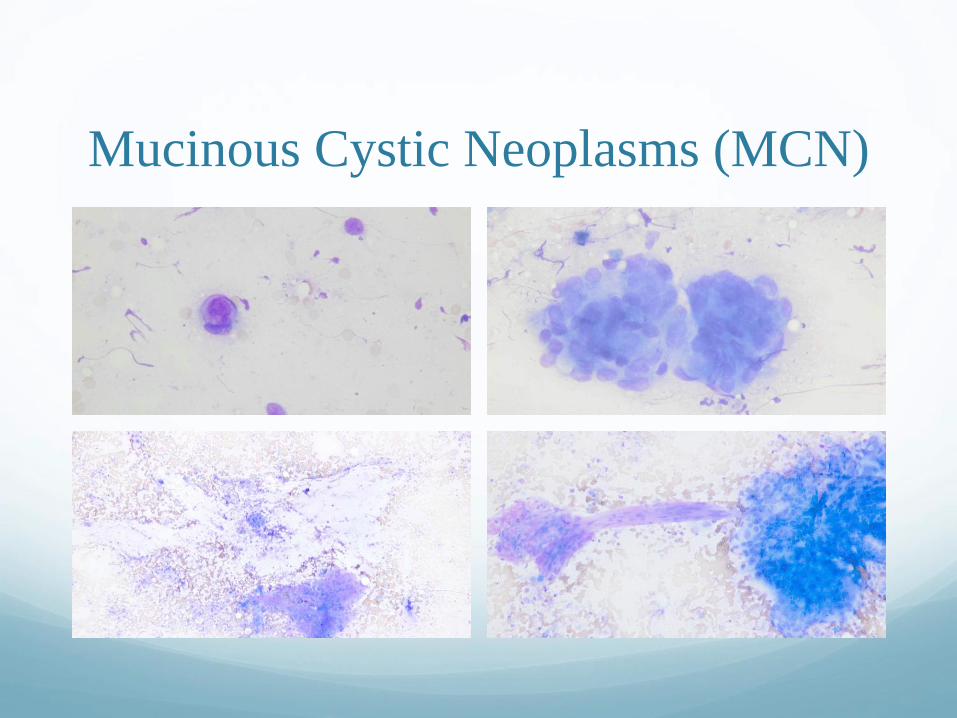
Mucinous Cystic Neoplasms (MCN)
Lined by mucinous,
generally non-papillary
epithelium, but can be
focally papillary
Associated with a
subepithelial “ovarian-like
stroma” (females)
Predominantly in middle
aged females
Mostly in the pancreatic
tail
Cysts do not
communicate with the
pancreatic ductal system
Thin septae
Mucinous Cystic Neoplasms (MCN)

Intraductal papillary mucinous
tumour (IPMT)
Main duct or branch duct types
Macroscopic papillae or mucin
Focal or diffuse > 1cm
PanIN < 5mm
M>F (Main Duct Equal)
60 years average

Thank you!