reciprocal cooperation between peer supporters and
TRANSCRIPT
Reciprocal Cooperation between Peer Supporters and Community Health
Centers in China
Dr Zhong Xuefeng
Institute of Health Education, Anhui
CDC
Project Objectives
• To evaluate feasibility of peer support group approach for individuals with type 2 diabetes in community settings in Anhui province, China
• To evaluate effectiveness of peer support approach for individuals with type 2 diabetes self-management practices
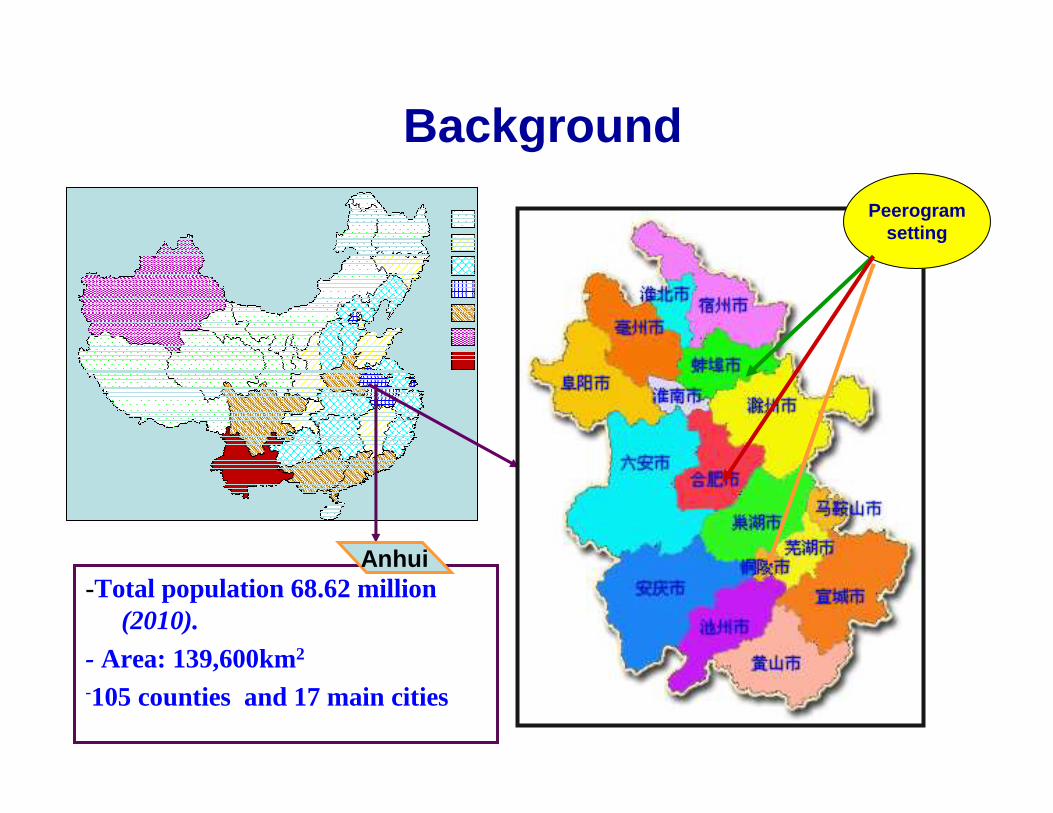
Background
-Total population 68.62 million (2010).
- Area: 139,600km2
-105 counties and 17 main cities
Anhui
Peerogramsetting
Overview of Program & Evaluation
• a community randomized controlled trial study in three sub-community,three cities in Anhui Province, China
• 726 eligible participants with type II diabetes being recruited from CHC diabetes-managed records
• 365 intervention group, 351 comparison group • 19 peer group were organized and based on
neighbourhoods• 19 peer supporters were nominated/recruited
by CHC • groups consisted of 10 to 15 individuals
20年020年020年020年0
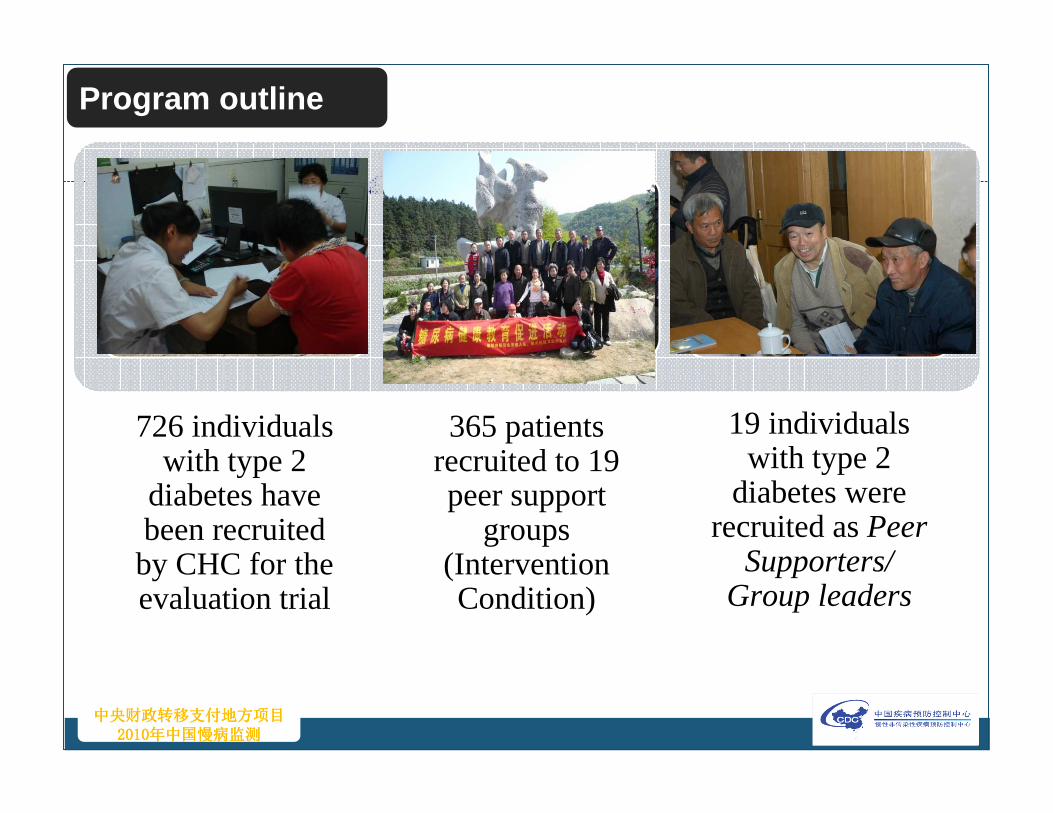
726 individuals with type 2
diabetes have been recruited by CHC for the evaluation trial
365 patients recruited to 19 peer support
groups (Intervention Condition)
19 individuals with type 2
diabetes were recruited as Peer
Supporters/ Group leaders
Program outline
Characteristics of peer supporters
• retired people (100%)• average age 64 years old• 84.2% them are males (16/19 )• 100%have middle or high educational level • suffering diabetes average age 9.3 years • good communication skills (1/3 of them used to be
teachers/administration staff/health worker/salesman )• compliance to community health professionals and workers• 36% of them used to be leader before retired)• have positive personality and be social • to be volunteer, no pay
Peer support intervention
• a community-and primary care-based model
• face to face meetings/ activities twice per month
• group meeting/activities co-led by CHC staff and PS (peer group leaders) monthly
• sub-group informal meeting/activity(Taji group央 Fishing央shopping央 jogging) led by peer group leaders at unschedued time (daily or weekly)
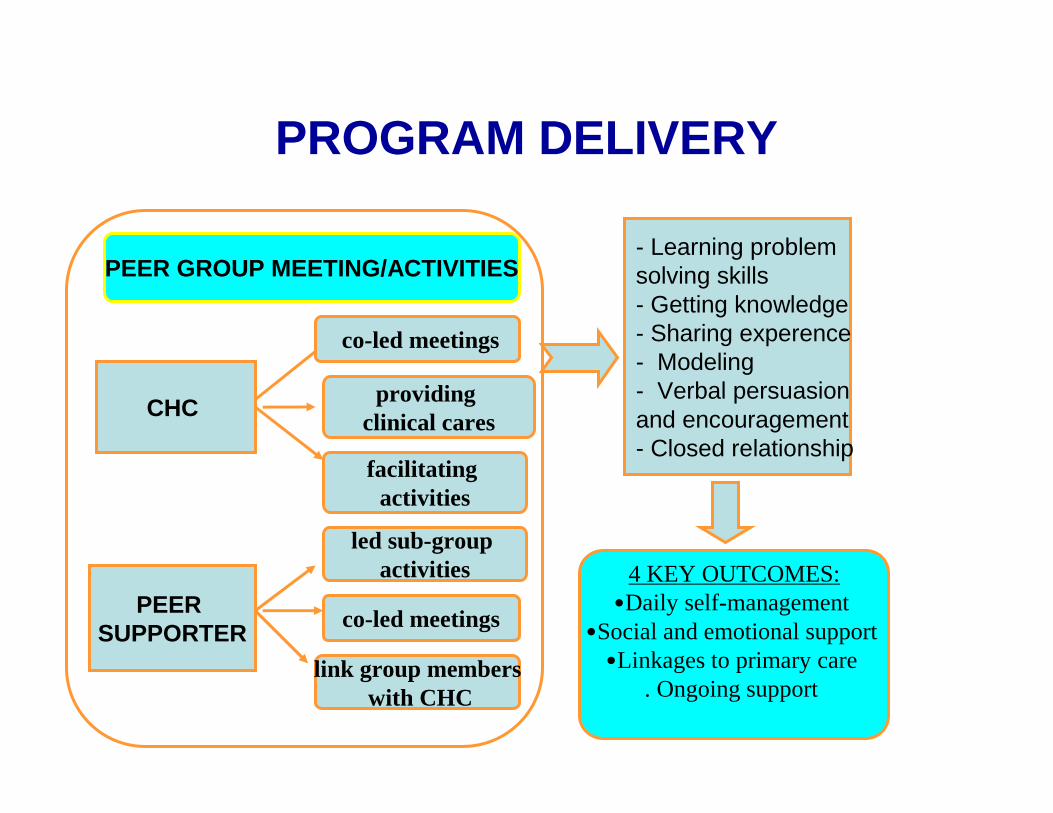
PROGRAM DELIVERY
PEER GROUP MEETING/ACTIVITIES
CHC
PEER SUPPORTER
co-led meetings
providing clinical cares
facilitating activities
led sub-group activities
co-led meetings
link group memberswith CHC
- Learning problem solving skills- Getting knowledge- Sharing experence- Modeling- Verbal persuasion and encouragement- Closed relationship
4 KEY OUTCOMES:•Daily self-management
•Social and emotional support •Linkages to primary care
. Ongoing support
How the 4 key functions of peer support were delivered?
1. Assist with daily self-management• get information and leaning new skills about self-management
• learn good modeling from group members
• sharing experience of daily self-management
• sub-group activities (exercises and shopping food)
2. Provide social & emotional support• “second-home”/“common language”and could talk about their
feelings and concerns
• "group belongs''/"social belongs", feel helped and supported each other
• "encouraged by peer supporters and group members when felt depression and stress"
–
3.Link to clinical care• peer supporters become bridge of CHC and
diabetes patients in the community
• CHC providing clinical services based on peer group member needs (discussion in group meeting)
4. Ongoing support (after 6 months)–sub -peer group keep activities
–PS keep closed relationship with CHC staffs
–CHC continue to provide clinical services to patientsbased on their needs proposed through PS
Results
1. Self-management Diabetes self-management practices1. Healthy diet•The mean score increased 0.44 and -0.53, sig. (P<0.01)
2. Physical activities•The mean score increased 2.22 and 1.03, sig. (P<0.01)
3. Monitoring glucose•The mean score changed 0.27and -0.79, sig. (P<0.001)
4. Medication adherence•The mean score changed 1.11 and 0.37, no sig. (P>0.05)
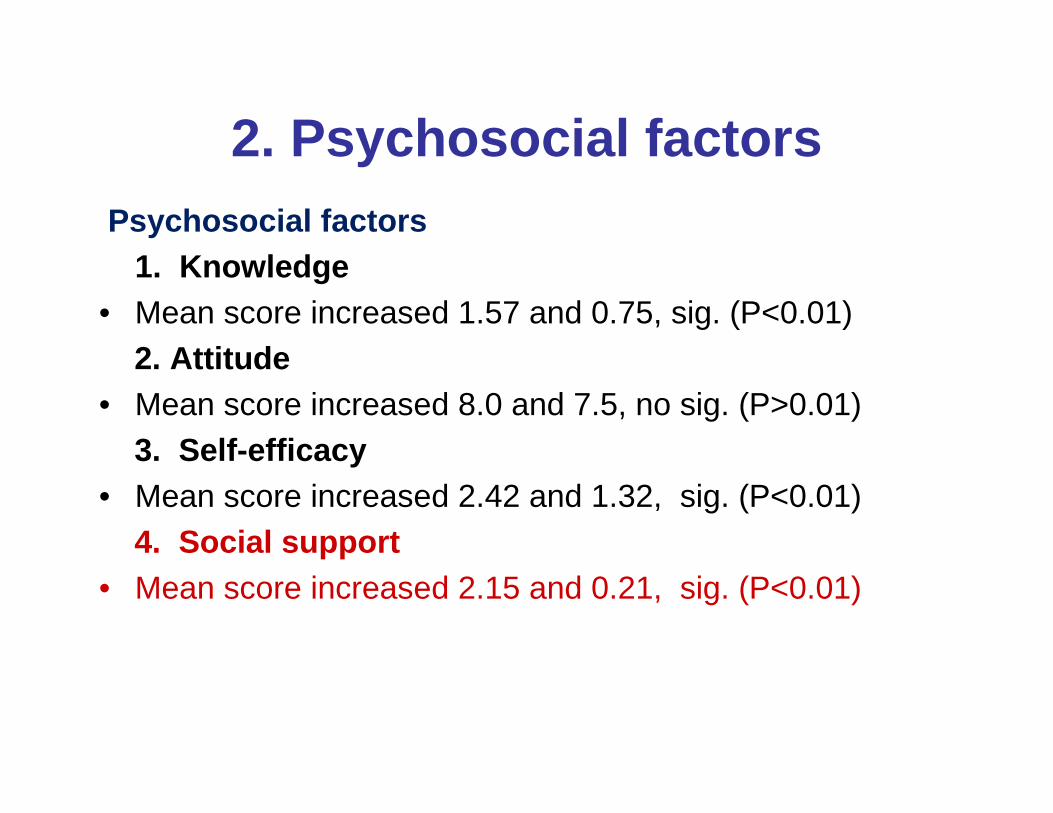
2. Psychosocial factorsPsychosocial factors
1. Knowledge • Mean score increased 1.57 and 0.75, sig. (P<0.01)
2. Attitude• Mean score increased 8.0 and 7.5, no sig. (P>0.01)
3. Self-efficacy• Mean score increased 2.42 and 1.32, sig. (P<0.01)
4. Social support• Mean score increased 2.15 and 0.21, sig. (P<0.01)
3. Emotional support
Qualitative evaluation outcome:A 61 year old woman commented,
“…I became sick two years ago, and when I found out I had diabetes, I felt upset, and thought that my life was meaningless. When I joined the peer support group, I discovered that many people had the same illness as me, and some people in our group had been living with diabetes for more than 20 years. They lived very well, and now they are more than 80 years old, so it encouraged me to believe that I too can live a long and healthy life if I can control my blood sugar and manage my life suitably.” ( female, housewife, 61years old, Da Qing community)
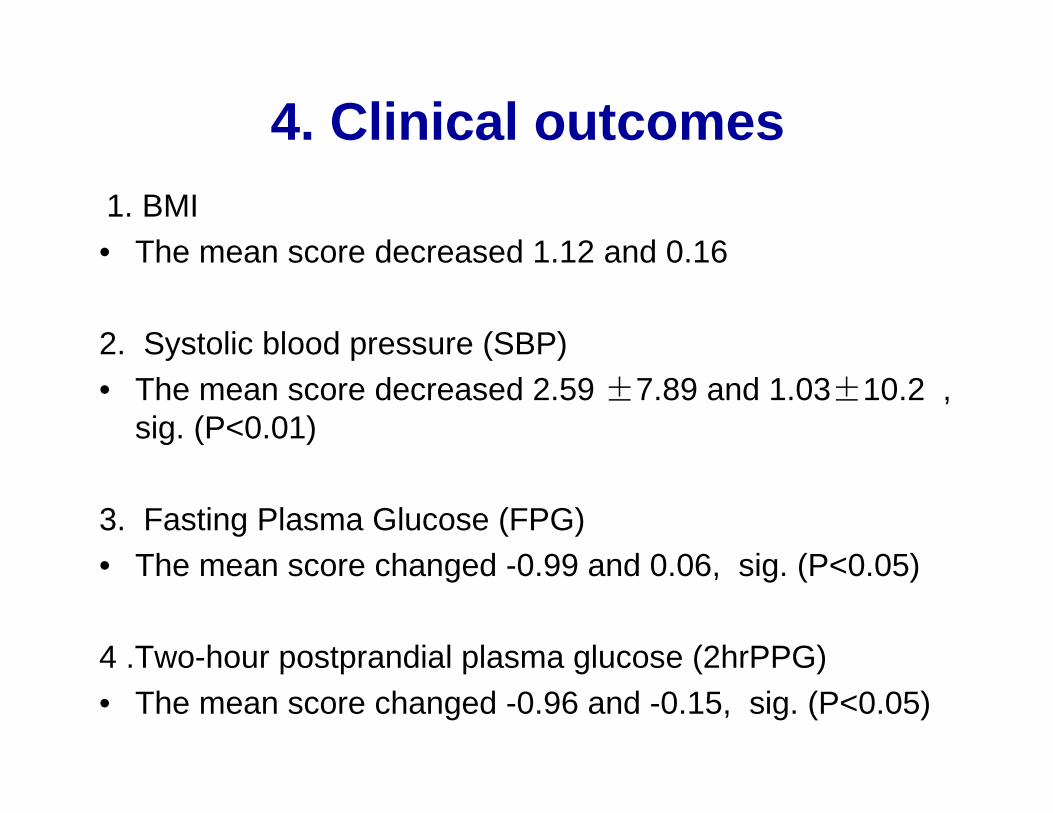
4. Clinical outcomes1. BMI• The mean score decreased 1.12 and 0.16
2. Systolic blood pressure (SBP) • The mean score decreased 2.59 ±7.89 and 1.03±10.2 ,
sig. (P<0.01)
3. Fasting Plasma Glucose (FPG)• The mean score changed -0.99 and 0.06, sig. (P<0.05)
4 .Two-hour postprandial plasma glucose (2hrPPG)• The mean score changed -0.96 and -0.15, sig. (P<0.05)
Conclusions
• The results demonstrate that, when adapted, PLSP is culturally acceptable and feasible in China when delivered according to a community-and primary care based model and integrated into the routine of community government organizations and community health services.
Future Challenges
• How to deliver this model to China rural areas?
• How to use group peer support for young individuals with diabetes?
• CHC capacity building
• How to integrate into the routine of health organizations(such as CDC) and community primary health services?
Acknowledgements
� This project was conducted in partial fulfillment of the requirements for the doctoral degree in health education and behavior science at Mahidol University in Bangkok. Dissertation chairs were: Profs. Chanuantong Tanasugarn and E. Fisher
�
Administration organization ( funder) : Anhui Provincial Bureau of Health
� Executive organization: Health Education Institute of Anhui Provincial Center for Disease Prevention and Control
� Partner organizations: Hefei Municipal Bureau of Health � Hefei City's Center for Disease Prevention and Control � Heyidi Community Health Service Center � District Bureau of Health, District CDC
� Tongling Municipal Bureau of Health� Tongling City's Center for Disease Prevention and Control� Yangguan Community and Rendong Community Health Service Station� District Bureau of Health, District CDC
� Bangbu Municipal Bureau of Health� Bangbu Center for Disease Prevention and Control� Daqing Community Health Service Center� District Bureau of Health, District CDC