regulation of arterial pressure and cardiac output
DESCRIPTION
Good book for studying biology of circulatory systemTRANSCRIPT

REGULATION OF ARTERIAL PRESSURE REGULATION OF ARTERIAL PRESSURE AND CARDIAC OUTPUT
Dr. Adelina Vlad

By controlling the systemic mean arterial pressure, the circulatory system provides a great flexibility for distributingcirculatory system provides a great flexibility for distributing blood flow:
All organs receive approximately the same mean arterial pressurepressureEach organ controls local blood flow by adjusting local arteriolar resistanceAs long as the heart maintains the mean arterial pressure aAs long as the heart maintains the mean arterial pressure, a change in blood flow in one vascular bed does not affect blood flow in other beds
Arterial pressure is kept fairly constant over time, whereas cardiac output and peripheral resistance are quite variable
Regulation of Arterial PressureRegulation of Arterial PressureArterial pressure is regulated by
Sh t t h iShort-term mechanisms:seconds to minutesneural reflexes targets
o heart o vessels o adrenal meddula
Long-term mechanisms: hours dayshours, dayshumoral controltargets
o blood esselso blood vessels o kidneys in their control of extracellular fluid volume
Regulation of Cardiac OutputRegulation of Cardiac OutputCardiac output – influences to a large degree the arterial pressurepressureits regulation is important for maintaining arterial pressure within the normal range
Cardiac output is regulated by mechanisms intrinsic to the heart: preload, after-load, contractility etc.extrinsic to the heart: neural and hormonal pathways
The cardiac output is controlled mainly by the sum of all the local tissue flows (venous return)

Short-Term Regulation of Blood PressureMediated by neural reflexes that operate as negative feedback loopsEach loop is composed ofEach loop is composed of
Receptorsbaroreceptors (high-pressure receptors) - stretch receptors chemoreceptors sense changes in blood O2 CO2 and pHchemoreceptors – sense changes in blood O2, CO2 and pHlow-pressure receptors – stretch receptors (volume sensors)
Afferent neural pathwaysCNS center
processes the information and generates a responselocated in the medulla, hypothalamus, cerebral cortex
Efferent neural pathwaysEffectors
heart: pacemaker and muscle cellsheart: pacemaker and muscle cellsarteries and veins: VSCMsadrenal medulla

Baroreceptor Control of APBaroreceptor Control of APIncreased mean arterial pressure (AP) causes vasodilation and bradycardia; main mechanism for maintaining APbradycardia; main mechanism for maintaining AP

BaroreceptorsBaroreceptorsMechanoreceptorsL t d t t t i hi h it th tid i dLocated at strategic high-pressure sites: the carotid sinus and aortic archStimulus: distension of the vascular wall; baroreceptors are not
iti b t t t h itipressure sensitive, but stretch sensitiveEncode the mechanical response as a frequency-modulated signalThe overall baroreceptor response to a pressure increase includes
an increased firing raterecruitment of more units
Compared to the carotid sinus receptor, the aortic arch receptor have a higher threshold and a higher saturation levelhave a higher threshold and a higher saturation level
Response of Baroreceptors to Pressure
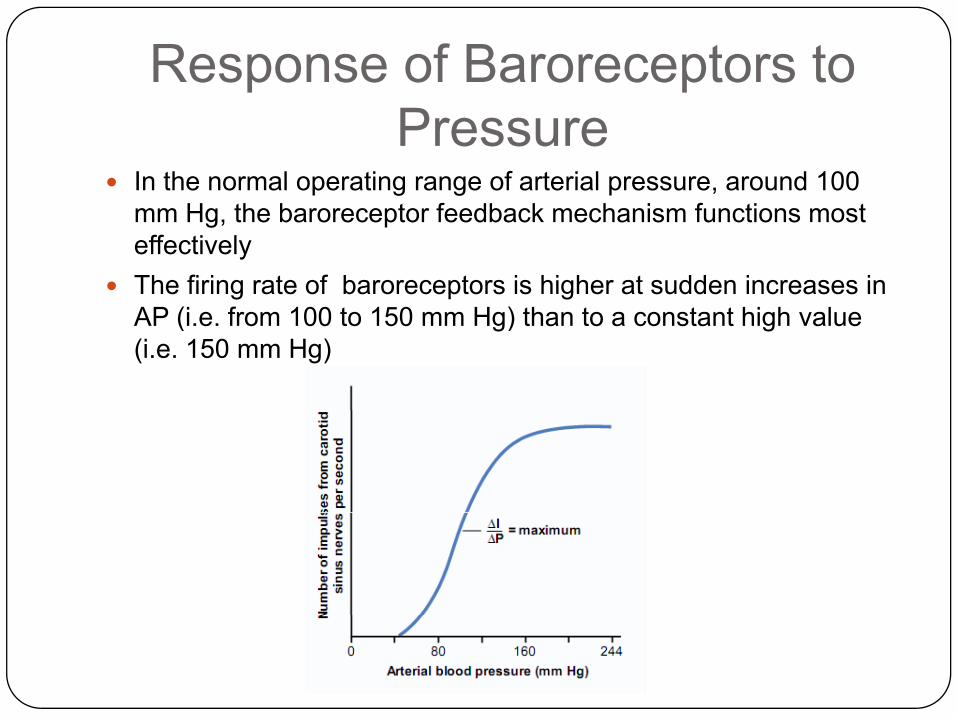
In the normal operating range of arterial pressure, around 100 H th b t f db k h i f ti tmm Hg, the baroreceptor feedback mechanism functions most
effectivelyThe firing rate of baroreceptors is higher at sudden increases in AP (i f 100 t 150 H ) th t t t hi h lAP (i.e. from 100 to 150 mm Hg) than to a constant high value (i.e. 150 mm Hg)

Afferent PathwaysAfferent Pathways
Aff t th f thAfferent pathway for the aortic arch reflex:- depressor branch of the vagus nerve
Afferent pathway for the carotid sinus reflex:- sinus nerve
vagus nerve- superior laryngeal nerves- nodose ggl of the vagus
- glossopharyngeal trunk- petrosal ggl

Medullary Cardiovascular CenterMedullary Cardiovascular CenterIs the major coordinating center for cardiovascular homeostasisB d bdi i i b di ti i h d hBroad subdivisions can be distinguished, such as
a vasomotor area in the ventrolateral medulla, includesA1 and C1 areas in the rostral ventrolateral medullaInferior olivary complex and other nuclei
- C1 area produces a spontaneous tonic output that promotes vasoconstriction
a cardioinhibitory area includes nucleus ambiguus dorsal motor nucleus of the vagus – the cardiac componentdorsal motor nucleus of the vagus the cardiac component of the baroreceptor reflex (bradycardia)
a cardioacceleratory area in the dorsal medulla (increased heart rate and contractility)heart rate and contractility)

Baroreceptor Signals Coordinated by the Medulla
Impulses from baroreceptors project to the nucleus tractusImpulses from baroreceptors project to the nucleus tractus solitarius (NTS) in the brain stemFrom NTS project
Inhibitory interneurons onto the vasomotor area:Inhibitory interneurons onto the vasomotor area: increased mean arterial pressure baroreceptors NTS neurons inhibit C1 neurons vasodilationExcitatory interneurons onto the cardioinhibitory area:Excitatory interneurons onto the cardioinhibitory area:increased mean arterial pressure baroreceptors NTS neurons stimulate the cardioinhibitory area bradycardiaI hibit i t t th di l tInhibitory interneurons onto the cardioacceleratory area:increased mean arterial pressure baroreceptors NTS neurons inhibit the cardioacceleratory area decreased heart rate and contractility


Efferent PathwaysEfferent PathwaysSympathetic efferents
N f t i t C1 d di l tNeurons from vasoconstrictor C1 and cardioacceleratoryareas send axons down the spinal cord preganglionic sympathetic neurons located in the intermediolateral gray matter T1 – L3 postganglionic sympathetic neuronsmatter, T1 – L3 postganglionic sympathetic neurons located within ganglia of the paravertebral sympathetic chain
postganglionic fibers innervate arteries, arterioles and veins or, through the cardiac nerves, the heart; someveins or, through the cardiac nerves, the heart; some preganglionic fibers innervate the adrenal gland through the splanhnic nervesIncreased sympathetic activity produces vasoconstriction; the y p y p ;baroreceptor reflex produces vasodilation because it inhibits the output of C1 neurons

Parasympathetic efferents:th di i hibitthe cardioinhibitory area (nucleus ambiguus, dorsal motor nucleus of the vagus) activated by baroreceptoractivated by baroreceptor impulses stimulates preganglionic parasympathetic fibers of theparasympathetic fibers of the vagus nerve postganglionic neurons in the walls of the atria and the vessels short postganglionic fibers to the SAN, the atria, the ventricles,
f S Cor the vicinity of VSMCs

Cardiac Sympathetic and P i th ti NParasimpathetic Nerves

Effectors in the Neural Control of APEffectors in the Neural Control of APHEART
S th ti i t ( di )Sympathetic input (cardiac nerves) – norepinephrine, to SA, atria, ventricles increased heart rate and contractility;
t t th i fi i t i l th th t f th- at rest their firing rate is lower than that of the vagus nerve low tonic cardioacceleratory effect on the heart
Parasympathetic input (vagus nerve) – acetylcholine, to SA node (right branch), AV node (left branch), atria; - exerts an intense tonic activity: decreases heart rate, conduction through AV node and to a lesser extent, contractility

BLOOD VESSELSBLOOD VESSELSSympathetic input – vasoconstrictor response (norepinephrine); postganglionic fibers are most abundant in the skin and the kidney sparse infibers are most abundant in the skin and the kidney, sparse in the coronary and the cerebral vessels, absent in the placenta; - vasodilator response in the skeletal muscle (acetylcholine); sympathetic vasodilator fibers receive impulse from cerebralsympathetic vasodilator fibers receive impulse from cerebral cortex – hypothalamus – spinal cord – preganglionic sympathetic neurons – sympathetic ganglia – postganglionic fibers – VSMCs of the blood vessels of the skeletal musclefibers VSMCs of the blood vessels of the skeletal muscle vasodilation in “fight or flight” response
Parasympathetic inputParasympathetic input- vasodilator response (acetylcholine – indirectly, NO); the fibers are far less compared to the sympathetic ones; they supply the salivary and some gastrointestinal glands; they aresupply the salivary and some gastrointestinal glands; they are crucial for vasodilating erectile tissue in the external genitalia

V t i t TVasoconstrictor Tone The continual firing of the C1 area is called sympathetic vasoconstrictor tone and maintains a partial state ofvasoconstrictor tone and maintains a partial state of contraction in the blood vessels, called vasomotor tone; a total spinal anesthesia induces a fall in AP from 100 mm Hg to 50 mm Hg, proving the importance of the vasomotor tone in keeping APHg, proving the importance of the vasomotor tone in keeping AP at normal levels

Sympathetic Effects on Vascular Tone


ADRENAL MEDULLAP li i th ti fib l A h ffiPreganglionic sympathetic fibers release Ach on cromaffin cells of the adrenal medulla (= modified postganglionic neurons) release into the blood epinephrine and some norepinephrine generalized effects on the circulation (heartnorepinephrine generalized effects on the circulation (heart and blood vessels); epinephrine binds mostly on vascular β2
receptors (skeletal muscle, coronary vessels), inducing vasodilation, and on cardiac β1 receptors, increasing thevasodilation, and on cardiac β1 receptors, increasing the cardiac output

EFFECTOR RESPONSE ANATOMIC NEUROTRANS RECEPTOR
EFFECTS OF SYMPATHETIC AND PARASYMPATHETIC PATHWAYS ON THE CARDIOVASCULAR SYSTEMEFFECTOR RESPONSE ANATOMIC
PATHWAYNEUROTRANSMITTER
RECEPTOR
Tachycardia Sympathetic Norepinephrine β1 on cardiac pacemakerp
Bradycardia Parasympathetic Acetylcholine M2 on cardiac pacemaker
Increase cardiac contractility Sympathetic Norepinephrine β1 on cardiacc ease ca d ac co t act ty Sy pat et c o ep ep e β1 on cardiac myocyte
Decrease cardiac contractility Parasympathetic Acetylcholine M2 on cardiac myocyte
Vasoconstriction in most blood vessels (skin, kidney)
Sympathetic Norepinephrine α1 on VSMCs
Vasodilation in most blood Adrenal medulla Epinephrine β2 on VSMCsvessels (muscle, myocardium)
Vasodilation in “fight or flight” response
Sympathetic Acetylcholine M2 receptor
Vasodilation in blood vessels of salivary gland and erectile blood vessels
Parasympathetic Acetylcholine M2 and M3 receptor


Increased Decreased
Arterial
pressure pressure
Arterial pressure
Action potentials (AP)
Action potentials(APs) (AP)
Baroreceptor membrane
(APs)
potential (mV)
Basal frequency Increased frequency of APs
Decreased frequency of APs


Pressure “Buffer” Function of the Baroreceptor Control SystemBaroreceptor Control System
buffering Because the baroreceptor system ith iopposes either increases or
decreases in arterial pressure, it is called a pressure buffer systemA d t d d tA denervated dog presents an extreme variability of pressure caused by simple events of the day, such as lying down standingsuch as lying down, standing, excitement, eating, defecation, and noises
a primary purpose of the arteriala primary purpose of the arterial baroreceptor system is to reduce the minute by minute variation in arterial pressurearterial pressure

Resetting of BarorecetporsResetting of BarorecetporsBaroreceptors tend to reset in 1 to 2 days to the pressure level to which they are exposedwhich they are exposedThis “resetting” of the baroreceptors may attenuate their potency as a control system for correcting AP for longer than a few days at a timeat a time
However, baroreceptors have a role in long-term regulation of AP: during prolonged increases in AP, the baroreceptor reflexes mediate decreases in renal sympathetic nerve activity increased excretion of sodium and water by the kidneys gradual decrease in extracellular fluid volume and eventually ingradual decrease in extracellular fluid volume and eventually in blood volume, which helps to restore arterial pressure toward normal

Higher Brain CentersNeurons located throughout the reticular substance of the pons mesencephalon
Higher Brain Centerssubstance of the pons, mesencephalon, and diencephalon can either excite or inhibit the vasomotor center: lateral and superiorportions of the reticular substance causeportions of the reticular substance cause excitation, whereas the more medial and inferior portions cause inhibitionHypothalamus – exerts powerful excitatoryHypothalamus exerts powerful excitatory (posterolateral areas) or inhibitory (anterior nuclei) cardiovascular effects; integrates many cardiovascular responses (e.g. during exercise)p ( g g )Forebrain areas – influence the hypothalamic integration areas along inhibitory and excitatory pathways (e.g. emotions fainting); p y ( g g);conditioned reflexes cardiovascular responses such as change heart rate

Response to ExerciseExerciseHypothalamus, under the general control of the cerebral cortex, coordinate the earlyof the cerebral cortex, coordinate the early response to exercise = an increased alertness that anticipates exercise by producing:- Increased cardiac output- Vasoconstriction in inactive muscle
regions and renalregions, and renal, splanchnic and
cutaneouscirculations- Early vasodilation in active musclein active muscle

Delayed cardiovascular response to exerciseresponse to exercise
Response to Acute Emotional Stress
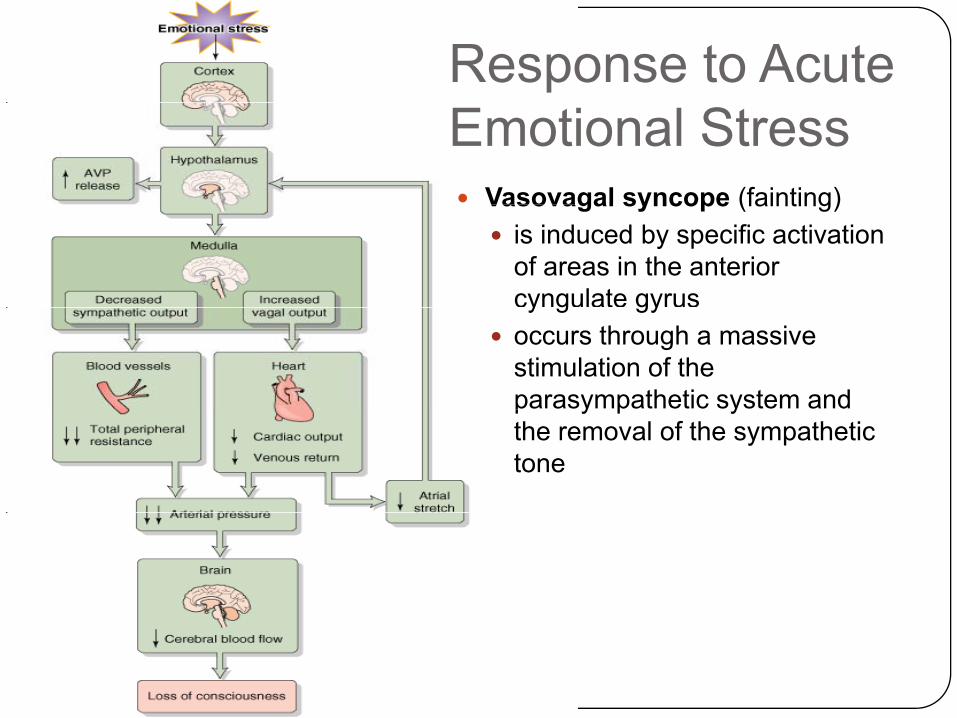
Vasovagal syncope (fainting)Vasovagal syncope (fainting)is induced by specific activation of areas in the anterior cyngulate gyrusy g gyoccurs through a massive stimulation of the parasympathetic system and p y p ythe removal of the sympathetic tone
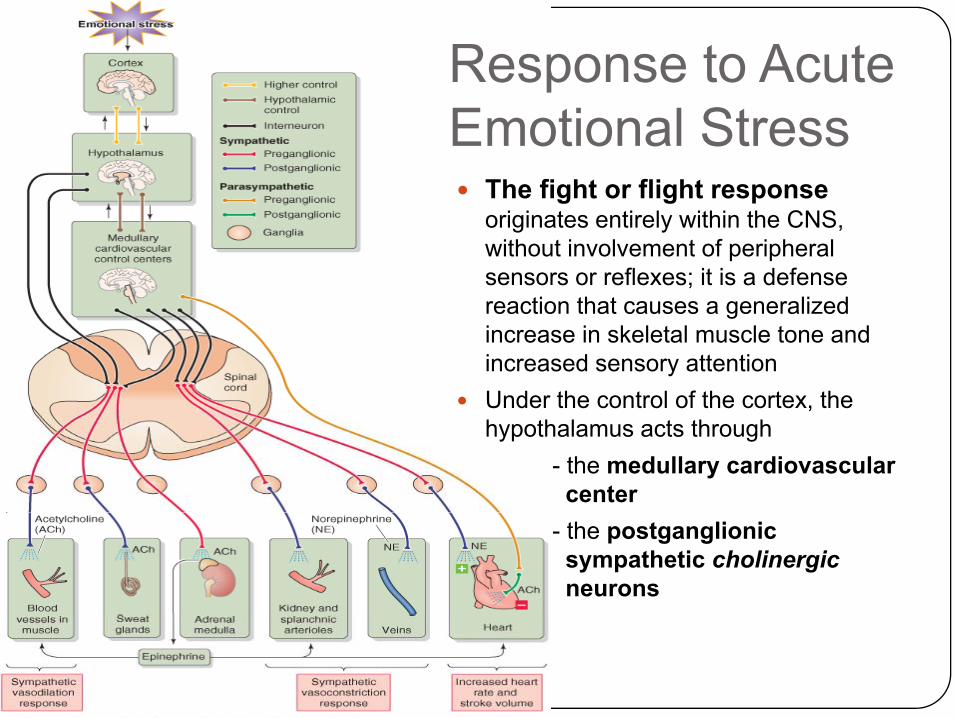
Response to Acute
The fight or flight response
Emotional Stressoriginates entirely within the CNS, without involvement of peripheral sensors or reflexes; it is a defense reaction that causes a generalizedreaction that causes a generalized increase in skeletal muscle tone and increased sensory attentionUnder the control of the cortex, the ,hypothalamus acts through
- the medullary cardiovascular center
- the postganglionic sympathetic cholinergicneurons

Chemoreceptor Control of BPChemoreceptor Control of BPA secondary neural regulation of arterial blood pressure that operates like the baroreceptor reflex except it is initiated byoperates like the baroreceptor reflex except it is initiated by chemoreceptorsChemoreceptors
Are cells sensitive to oxygen lack (low PO2) carbon dioxideAre cells sensitive to oxygen lack (low PO2), carbon dioxide excess (high PcO2), and hydrogen ion excess (low pH)Their primary role is to regulate ventilationPeripheral chemoreceptors primarily sense a low PO andPeripheral chemoreceptors primarily sense a low PO2 and are located in several small chemoreceptor organs:
two carotid bodies (glomus caroticum) in the bifurcation of common carotid arteries; glomus cells synapses with fiberscommon carotid arteries; glomus cells synapses with fibers of the glossopharyngeal nerveone to three aortic bodies adjacent to the aorta, that synapse with fibers of the vagus nervesynapse with fibers of the vagus nerve

Peripheral chemoreceptors Afferent fibers from glomus caroticus and aortic bodies project to the NTS in theaortic bodies project to the NTS in the medulla dis-inhibition of vasomotor center from NTS influences vasoconstriction; the final effect on the heartvasoconstriction; the final effect on the heart is tachycardia (primary - bradicardia)The fluctuation in PO2 that normally occur in humans cannot induce changes in arterial gpressure of heart rate peripheral chemoreceptor play a role only during severe hypoxia (hemorrhagic hypotension)
Central chemoreceptors
Central chemoreceptors, present in the ventrolateral medulla, sense mainly a lowventrolateral medulla, sense mainly a low brain PCO2 and pH
Once stimulated, these areas dis-inhibit the vasomotor area from NTS influencesthe vasomotor area from NTS influencesinduced by baroreceptor signals (if the case) vasoconstriction

Chemoreceptor Control of theChemoreceptor Control of the Cardiovascular System

Low Pressure BaroreceptorsLow-Pressure BaroreceptorsStretch receptors located at low-pressure sites: pulmonary artery, the junction of the atria with their veins, the atria themselves, the
t i lventriclesTheir distension depends on the venous return to the heart detect fullness of the circulation (volume sensors) Help regulating CO and effective circulating volume indirectly regulate AP

Regulation of Cardiac OutputRegulation of Cardiac OutputHeart is an important effector organ in the feedback loops that regulate APregulate APCO = SV x HRBoth SV and HR are under the control of regulatory mechanisms i t i i d t i i t th h tintrinsic and extrinsic to the heart

Intrinsic Control of Heart RateIntrinsic Control of Heart RateThe firing rate of SA node depends on the maximumdepends on the maximum diastolic potential, the slope of the diastolic depolarization (phase 4), and the threshold(phase 4), and the threshold potential
[K+] and [Ca++] influence the[K+]o and [Ca++]o influence the SA node activity without being part of a cardiovascular feedback loopfeedback loop

Intrinsic Control of Stroke VolumeIntrinsic Control of Stroke VolumeSV = EDV – ESVEDV d dEDV depends on
Filling pressure – increased venous return increases atrial filling pressure EDV risesFilling time – increased HR may decrease EDVVentricular compliance – high compliance for a given filling pressure, produces an increase in ventricular volume rising EDV
ESV depends onPre-load – Starling principle: a high pre-load increases SVAfter-load – increased after-load increases ESVHR – increased HR increases contractility, may reduce ESVContractility – positive inotropic agents enhance the force ofContractility positive inotropic agents enhance the force of contraction and decrease ESV

Extrinsic Control of HR and SVExtrinsic Control of HR and SVBaroreceptor reflex – adjusts CO only as a response to an alteration of AP:alteration of AP: baroreceptors do not respond to an increase in CO that matches a decrease in peripheral resistance, leaving AP unchangedif i h l i t lt AP th b t fl dj tif peripheral resistance alters AP, the baroreceptor reflex adjustes CO and arterial tonus in order to maintain AP at a proper level
Chemoreceptor reflex – adjusts CO only when this affects pH, PO2, PCO2 : low CO low AP decreased perfusion low PO2, high pH, p , g p ,PCO2 peripheral and central chemoreceptor are stimulated tachycardia Tachycardia induced by increased PCO2 also compensates the y y pnegative inotropic effect of low pH (acidosis decreases calcium sensitivity of myofilaments, decreasing contractility)

Low Pressure BaroreceptorsLow-Pressure BaroreceptorsAtrial receptors – A or B fibers that join the vagus nerve
A fib fi i h ith t i l t l it HRA fibers – fire in synchrony with atrial systole monitor HRB fibers – increase their firing as the atria fill monitor the atrial volume and the central venous pressure (CVP)Aff t ff t th d th ff t i il t thAfferent, efferent pathways and the effectors are similar to the baroreceptor reflex
B-fibers stimulation- raises the heart rate ( increases CO in response to an increased venous return) = Bainbridge reflex- decreases vasoconstrictor output only to the kidney increased renal blood flow increased urinary output low-pressure receptors attempt to eliminate fluid

Afferent fibers of the atrial receptors project also on the hypothalamus inhibits arginine vasopressin release AVP (orhypothalamus inhibits arginine vasopressin release, AVP (or antidiuretic hormone, ADH) increased diuresis in response to increased venous returnAtrial stretch release of atrial natriuretic peptide (ANP)Atrial stretch release of atrial natriuretic peptide (ANP) followed by increased diuresis
In summary: Increased atrial filling stretch of atria mechanoreceptors stimulated diuresis (decrease of extracellular fluid) by three efferent mechanisms:
- 2 neurally mediated: tachycardia combined with renal vasodialtion, and inhibition of ADH release
- 1 non-neural: ANP release

CO is Proportional to Venous ReturnpHeart rate and venous return
Decreasing the effective circulating volume (= depletion or decreased venous return) increases heart rate due to decreased firing of high-venous return) increases heart rate due to decreased firing of high-pressure baroreceptorsIncreasing the effective circulating volume (= loading or increased venous return) increases heart rate through low-pressure baroreceptorvenous return) increases heart rate through low pressure baroreceptor reflex (Bainbridge reflex)Heart rate is at its minimum when effective circulating volume is normalnormal
Stroke volume and venous returnSV increases gradually with venous return during volume depletion (because of Starling’s law effect and sympathetic stimulation following(because of Starling s law effect and sympathetic stimulation following decreased firing from high-pressure baroreceptors)SV stays constant during volume overload (because Starling’s law effect is less steep and the baroreceptor reflex is reducing contractility)effect is less steep and the baroreceptor reflex is reducing contractility)
Therefore, the cardiac output (CO = HR x SV) rises monotonically with the effective circulating volume

CO dependence on venous return is the result of the interplay among:
1. Bainbridge reflex 2. baroreceptor reflex 3 Starling’s law3. Starling s law


Intermediate and Long-Term Control of the CirculationControl of the Circulation
Humoral controls operating within hours or days contribute to circulatory homeostasis:circulatory homeostasis:
1) Vasoactive substances released in the blood or in the i it f VSMC d l t th l t ff tproximity of VSMCs – modulate the vascular tone affect
blood pressure and the distribution of blood flow
2) Nonvasoactive substances – act on targets other than the cardiovascular system (kidneys) and modulate extracellular fluid volume control the effective circulating volume modulate the arterial pressure and cardiac output by determining the filling of the blood vessels

1 Vasoactive Compounds1. Vasoactive CompoundsBiogenic amines
1 Epinephrine produced by the adrenal medulla1. Epinephrine – produced by the adrenal medulla - binds to β2 receptors of VSMCs (skeletal muscle, heart, liver,
adrenal medulla itself) causing vasodilationbinds to receptors of VSMCs causing vasoconstriction- binds to α1 receptors of VSMCs causing vasoconstriction
- binds to β1 receptors in the heart increasing heart rate and contractility
Th ff t f i h i i d ith th fThe effects of epinephrine are minor compared with those of norepinephrine released by the sympathetic nerves
2. Serotonin - present in nerve terminals, platelets, mast cells- local vasoconstrictor; important with vessel damage
3. Histamine – present in nerve terminals, mast cells- local vasodilator, released in response to tissue injury andlocal vasodilator, released in response to tissue injury and
inflammation; increases capillary permeability edema (allergic reactions)

Peptides1. Angiotensin II (ANG II)
– genesis: angiotensinogen (liver) cleaved to angiotensin I by renin (kidney) cleaved to ANG II by angiotensin-converting enzyme (ACE, released by the endothelial cells, particularly those of the lung) cleaved by aminopeptidasesto angiotensin III, less vasoactive than ANG II- important during blood loss, exercise and other circumstances that reduce renal blood flow ( renin) - powerful vasoconstrictor in the renal and splanchnicterritories; keeps the glomerular filtration rate at functional levels during falls of renal artery blood pressure- increases cardiac contractility- reduces renal plasma flow, increases renal Na+ absorption- ANG II and ANG III stimulate the release of aldosterone- in CNS stimulates thirst and release of arginine vasopressing p- facilitates the release of norepinephrine- acts as a cardiac growth-factor (cardiac hypertrophy)

2. Arginine vasopressin (AVP) or antidiuretic hormone (ADH) l d b th t i it it– released by the posterior pituitary
- vasoconstrictor at high concentration (hemorrhagic shock)3. Endothelins (ETs) – produced by endothelial cells
- local vasoconstrictors, the most powerful4. Atrial natriuretic peptide (ANP) – released from atrial
myocytes in response to stretchmyocytes in response to stretch- potent vasodilator- powerful diuretic and natriuretic lowers plasma volume and
the arterial pressurethe arterial pressure5. Kinins (bradikinin) – breakdown products of kininogens,
catalised by kallikreins (enzymes present in plasma, digestive glands and kidney); produced during inflammation and otherglands and kidney); produced during inflammation and other tissue reactions; inactivated after only few minutes from their formation by kininases (kininase II is ACE that generates ANG II)
vasodilators- vasodilators- like histamine, increase capillary permeability edema (allergic reactions)

Prostaglandins – derivatives of arachidonic acid synthesized by many tissuesmany tissues- PGI2 and PGE2 are strong local vasodilatorsNitric oxide (NO) – produced from arginine in endothelial cells b it i d th (NOS)by nitric oxyde synthase (NOS)- strong local vasodilatorCarbon dioxide causes- moderate vasodilation in most tissues- marked vasodilation in the brain
acting on the brain vasomotor center has an extremely- acting on the brain vasomotor center, has an extremely powerful indirect effect, transmitted through the sympathetic nervous vasoconstrictor system, to cause widespread vasoconstriction throughout the bodyvasoconstriction throughout the body

IonsCalcium vasoconstriction by stimulating VSMCs contrationCalcium – vasoconstriction, by stimulating VSMCs contrationMagnesium – vasodilation, inhibits VSMCs contraction Potassium – vasodilation, inhibits VSMCs contractionHidrogen ions acidosis causes dilation of the arterioles whereas aHidrogen ions – acidosis causes dilation of the arterioles, whereas a discrete alkalosis produces arteriolar constriction
2 Renal Control of ECF2. Renal Control of ECFPlasma volume, and therefore blood pressure, is determined by extracellular fluid (ECF = plasma plus the interstitial fluid) and theextracellular fluid (ECF = plasma plus the interstitial fluid) and the Starling forces across the capillary wallThe effective circulating volume (functional blood volume as sensed by the fullness or pressure in the vessels) is defendedsensed by the fullness or pressure in the vessels) is defended by:- high-pressure receptors (in the short term they regulate blood pressure via direct cardiovascular effects and in the longer termpressure via direct cardiovascular effects, and in the longer term they regulate effective circulating volume)- low-pressure receptors, regulate effective circulating volume- other sensors: baroreceptors in the renal artery, stretch receptors in the liver, the atrial myocytes, osmoreceptors in the CNSThese sensors send signals to the dominant effector organ: the kidney

The signals to the kidney follow four efferent pathways:Th i ANG II ld t i1. The renin - ANG II - aldosterone axis
2. The autonomic nervous system3. The posterior pituitary that release AVP4. Atrial myocytes that release ANP
The kidney determines ECF volume by regulating total bodyThe kidney determines ECF volume by regulating total-body Na+ content ultimately governs the blood volume the kidney is the principal agent in the long-term control of mean arterial pressuremean arterial pressure
(The long-term renal regulation of blood pressure is going to be e plained in detail at the end of the lect res abo t renalexplained in detail at the end of the lectures about renal physiology)


Basic Principles Governing theBasic Principles Governing the Circulation of Blood
Th t f bl d fl t h ti f th b d iThe rate of blood flow to each tissue of the body is controlled in relation to the tissue need
The cardiac output is controlled mainly by the sum of all the local tissue flows
In general the arterial pressure is controlled independently of either local blood flow control or cardiac output control (nervous- and kidney-regulated mechanisms)
Arterial pressure is kept fairly constant over time whereasArterial pressure is kept fairly constant over time, whereas blood flow (cardiac output) and peripheral resistance are quite variable

Cardiovascular Control SystemsCardiovascular Control Systems
Filling AfterFilling time
Ventricular compliance
Contrac tility
After-load