regulation of the university - janardan rai nagar ... sallybus.pdf · regulation of the university...
TRANSCRIPT

PAGE- 1
REGULATION OF THE UNIVERSITY In exercise of the powers conferred by the Board of Management, Janardan Rai Nagar Rajasthan Vidyapeeth (Deemed) University, Pratapnagar – Udaipur, hereby makes following Regulations & Syllabus for the Master of Physiotherapy Programme.
1. Short Title
These regulations shall be called “THE REGULAITONS FOR THE MASTER OF PHYSIOTHERAPY
(MPT) DEGREE COURSE OF JANARDAN RAI NAGAR RAJASTHAN VIDYAPEETH (DEEMED)
UNIVERISTY”
2. Commencement
They shall come into force from the Academic year of July 2007-08 onwards.
The regulations and the syllabus are subject to modification by the Standing Academic Council from time to time.
3. Title of the Course
It shall be called Master of Physiotherapy (MPT)
4. Goal of the Course
1. To prepare a postgraduate student towards professional autonomy with self regulation discipline
2. To form base of professional practice by referral as well as first contact mode using evidence based practices.
3. To impart research basis in order to validate techniques and technology in practice of physiotherapy.
4. To acuaint a student with concept of quality care at the institutional as well as at the community levels.
5. To inculcate appropriate professional relationships in multi-disciplinary set up , patient management and co-partnership basis.
6. To prepare students to address problems related to health education and community physiotherapy
7. To practice the concept to protection of rights of the community during referral as well as first contact practice.
8. To incorporate concept of management in physiotherapy.
9. To provide experience in clinical training & undergraduate teaching partly
10. To provide honest, competent and accountable physiotherapy services to the community.
PAGE- 2
5. Philosophy
The Physiotherapy faculty believes that this program prepare physiotherapist for leadership in physiotherapy and health fields who can function as specialists. Physiotherapy practitioner, consultants, educator, administrators and researchers in a wide Varity of professional settings in meeting the demands and changing needs of society.
6 Eligibility for Admissions
Candidates who have passed B. Sc. (PT) or BPT degree from this university or any other university in India or
abroad recognized as equivalent by Janardan Rai Nagar Rajasthan Vidyapeeth University with not less than 50%
of marks in aggregate are eligible.
7 Criteria for Selection
Students for MPT degree courses shall be admitted based on the following:
a) 50% marks from the performance at the Entrance Examinations held by this University. b) 25% marks from the percentage of UG marks. c) 25% marks from the Personal Interview.
8 Registration
A candidate admitted into MPT degree course in Physiotherapy in Janardan Rai Nagar Rajasthan Vidyapeeth
(Deemed) University shall register with the University by remitting the prescribed fee along with the application
form for registration duly filled in and forwarded to the Principal within the stipulated date.
9 Duration of the Course
The duration of the course shall be two academic years. All the candidates for the degree are required to pursue
the recommended course for two academic years as full time candidate. Each academic year shall consist of not
less than 200 working days. No exemption shall be given from this period of study and training for any other
experience gained prior to the admission of the course.
10 Medium of Instruction
English will be the medium of instruction for the subjects of study and for the examination of the MPT Course.
11 Course of Study The Course of study are shown in Table No 1 & 2
The detailed syllabus in respect of the course is appended to this regulation.
12 Specialties in the Course a MPT IN MUSCULO- SKELETAL DISORDERS b MPT IN NEUROLOGICAL & PSYCHOSOMATIC DISORDERS c MPT IN CARDIO- RESPIRATORY DISORDER & INTENSIVE CARE d MPT IN SPORTS PHYSIOTHERAPY e MPT IN PEDIATRICS
13 Subject of Study
PAGE- 3
The Courses of the study, subjects and teaching schedule for Ist & IInd year MPT Course is shown separately in Table 1 & 2
14 Method of Training
The training of Postgraduate for MPT degree shall be on a full time pattern with graded responsibilities in the management and treatment of patients entrusted to his/ her care. Training should include involvement in Laboratory, experimental work and research studies. The participation of students in all facets of educational process in essential. Every candidate should take part in Seminars, Group discussions, Clinical rounds, Case demonstrations, Clinics , Journal review meetings and other continuing education activities every candidate should be required to participate in the teaching and training programme of undergraduate students.
15 Monitoring progress of studies (Internal Monitoring)
It is essential to monitor the learning progress each candidate through continuous appraisal and regular assessment. it not only helps teachers to evaluate students , but also students to evaluate themselves. The monitoring be done by the staff of the department based on participation of students in various teaching / learning activities. it may be structed and assessment be done using checklists that assess various aspects. Model checklists are given in table No. 5 to 12.
a. Work Dairy: Every candidate shall maintain a work dairy and record his / her participation in the training programmers conducted by the department such as journal reviews , seminars etc.
Special mention may be made of the presentations by the candidate as well as details of clinical or laboratory procedures, if any conducted by the candidate. The work diary shall be scrutinized and certified by the head of the department and head of the institution and presented in the university examination.
b. Internal Examination : The college may conduct minimum two Exams one is Sessional Exam and the other one is Pre University Examination before the University Examination. The test may include written theory papers, practical, viva voce and clinical in the pattern of university examination, records and marks obtained in such tests will be maintained by the Head of the Department and sent to the Head of the Institution , when called for by the principal
16 Attendance
A candidate is required to attend a minimum of 75% of training and of the total classes conducted during each academic year of the MPT course. Provided further, leave of any kind shall not be counted as part of academic tern without prejudice to minimum 75% of training period every year and student who fails to complete the course in this manner shall not be permitted to appear for the University examination
17 Condonation of Lack of Attendance
There shall be no condonation of attendance in post- graduate degree courses.
18 Commencement of Examination
There will be two examinations in a year, one is Annual examination and the other one is Supplementary examination to be conducted as per notification issued by the University from time to time. First and Second year examination of MPT course shall be held at end of Ist year & IInd year respectively the examination for main subjects shall be conducted by the University and for subsidiary subjects by the respective college.
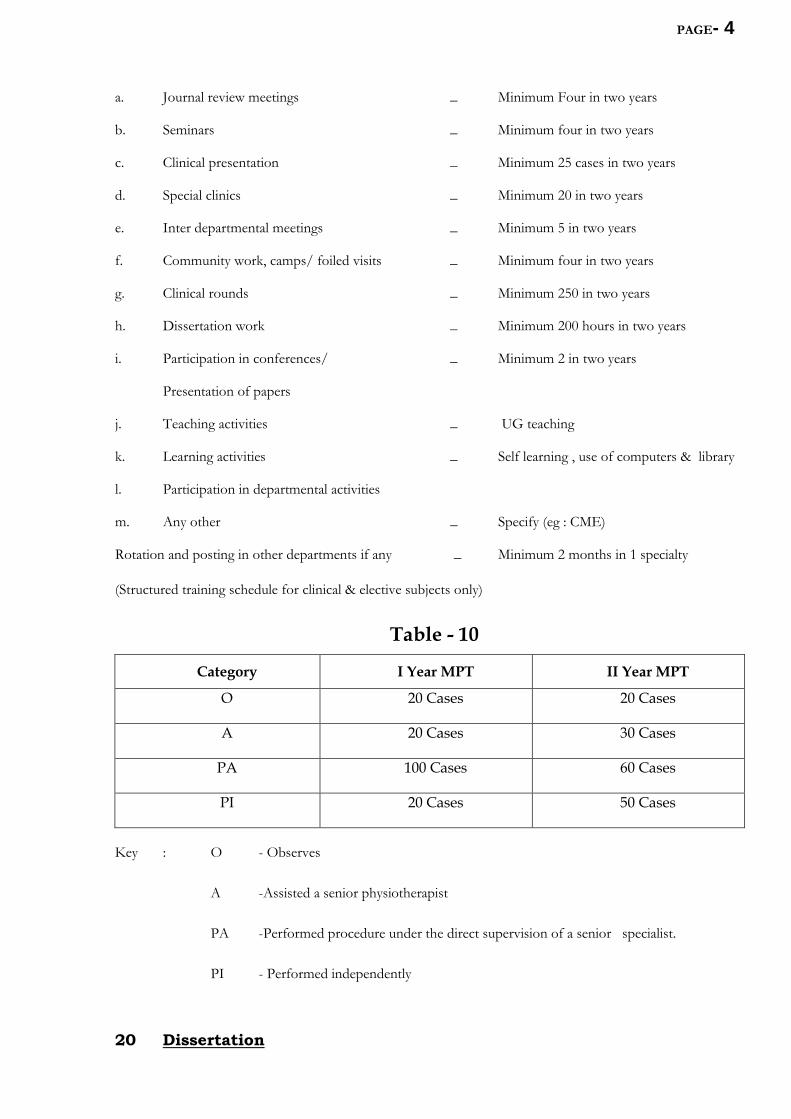
19 Teaching & Learning experience & Graded responsibility in care of patients and operative work.
PAGE- 4
a. Journal review meetings _ Minimum Four in two years
b. Seminars _ Minimum four in two years
c. Clinical presentation _ Minimum 25 cases in two years
d. Special clinics _ Minimum 20 in two years
e. Inter departmental meetings _ Minimum 5 in two years
f. Community work, camps/ foiled visits _ Minimum four in two years
g. Clinical rounds _ Minimum 250 in two years
h. Dissertation work _ Minimum 200 hours in two years
i. Participation in conferences/ _ Minimum 2 in two years
Presentation of papers
j. Teaching activities _ UG teaching
k. Learning activities _ Self learning , use of computers & library
l. Participation in departmental activities
m. Any other _ Specify (eg : CME)
Rotation and posting in other departments if any _ Minimum 2 months in 1 specialty
(Structured training schedule for clinical & elective subjects only)
Table - 10
Category I Year MPT II Year MPT
O 20 Cases 20 Cases
A 20 Cases 30 Cases
PA 100 Cases 60 Cases
PI 20 Cases 50 Cases
Key : O - Observes
A -Assisted a senior physiotherapist
PA -Performed procedure under the direct supervision of a senior specialist.
PI - Performed independently
20 Dissertation

PAGE- 5
Every candidate pursing MPT degree course is required to carry out work on a selected research project under
the guidance of a recognized postgraduate teacher. The results of such a work shall be submitted in the form of
dissertation.
The dissertation is aimed to train a graduate student in research methods and techniques. It includes
identification of a problem, formulation of a hypothesis, search and review of literature getting acquainted with
recent advances, designing of a research study, collection of data , critical analysis, comparison of results and
drawing conclusions .
Every candidate shall submit to the Principal of the Institute in the prescribed Performa, a synopsis containing
particular of proposed dissertation work within 6 months for the date of commencement of the course on or
before the dates notified by the university. The synopsis shall be sent through the proper channel to the
University.
Such synopsis will be reviewed and the university will register the dissertation topic. No Change in the
dissertation topic or guide shall be made without prior approval of the university.
21 Guide
The academic qualification ad teaching experience required for recognition by this university for a postgraduate teacher for guiding MPT candidates shall be.
1. M.Sc. (PT) / MPT with five years teaching experience working on a full time position at any esteemed institution.
2. The age of teacher / guide shall not exceed 65 years.
3. The guide student ratio shall be 1:3
4. Not with standing above, in view of acute shortage of teachers, the teachers having two years teaching experience after MPT and working on a full time basis be considered as P.G. teachers for a period of five year i.e. upto 2010
Co- guide : may be included provide the work requires substantial contribution from a sister department or
from another medical institution recognized for teaching / training by Janardan Rai Nagar Rajasthan Vidyapeeth
(Deemed) University , College of Physiotherapy . the co-guide shall be a recognized post graduate teacher of
College of Physiotherapy .
22 Change of Guide
In the event of a recognized guide leaving the college for any reason or in the event of death of guide , guide may be changed with prior permission from the university
23 Scheme of Examination
The examination for MPT Course shall be held at the end of each academic year). Particular of subjects,
section and distribution of marks is listed in Table No 3 & 4..
24 Examiners

PAGE- 6
MPT degree with minimum 2 years of teaching experience shall be appointed as examiners.
25 Paper Setters
MPT degree with minimum 2 years of teaching experience shall be appointed as paper setters.
26 Criteria for Declaring as Pass in University Examination.
A candidate shall be declared to have passed the examination if he/she secures 50% of the marks in the
university written examination , 50% of the marks in the University practical examination, and not less that
50% of marks in the aggregate. Failed candidate may appear in any subsequent examination upon payment of
fresh fee to the Institute.
27 Classification of Successful Candidates
The candidate who obtain
a) 75% in aggregate is considered to have passed in first class with distinction.
b) 60 % in aggregate is considered to have passed in first class.
c) 50 % is considered to have passed.
28 Type of questions in Examination
Theory Examination
1. Long Essay (5 questions) - 5x10=50 marks
Short Essay (10questions) - 10X5 = 50 marks
Practical Examination
Note: All cases for clinical examination should be on patients and not on models.
Ist Year : Day One – Practical Day Two - NIL IInd Year : Day One – Elective Practical Day Two – Dissertation
1- Elective Long case (1) - 1x40 = 40 marks
2- Short case (2) - 2x 20= 40 marks
29 Evaluation of dissertation
Approval of dissertation work is an essential precondition for a candidate to appear in the final university examination. The evaluation apart from the guide out of which either is external outside the university or other postgraduate college of this university shall value the dissertation.
30 Number of appearance (S)
a. A candidate registered for the MPT degree course must pass the I year and II year examinations within five years from the date of his / her admission . i.e. the candidate should pass the I year and II year examinations with in 9 attempts in the university examination.
31 Migration & transfer of candidates

PAGE- 7
Migration & Transfer of candidates from – one affiliated institution to another institution of this university or from another university will not be considered in any circumstances.
32. Award of medals and prizes
The best out going student award will be given to the candidate in each batch after the course completion
The criteria for selecting best out going students will be based on their aggregate marks (without any reappearance) attendance, discipline and extra curricular activities.
TABLE -1
First Year Master of Physiotherapy (First 12 Months)
Teaching Hours
S.No. Subjects TEACHING HOURS
Theory Practical / Clinical Total
1 Anatomy & Applied Anatomy 60 40 100
2 Physiology, Applied Physiology and exercise Physiology
60 40 100
3 Biostatistics & Research Methodology ,
PT Education & Ethics
70
30
- 100
4 Movement Sciences 50 50 100
5 Advanced PT Modalities and Diagnostic Techniques
50 50 100
6 Clinical Training - 600 600
7 Seminars , Journal Clubs, Case- Presentations, Teaching Skills , Field Works etc.
- 150 150
1250 Hrs.
TABLE -2

PAGE- 8
Second Year Master of Physiotherapy (First 12 Months)
Teaching Hours
S.No. Subjects TEACHING HOURS
Theory Practical/ Clinical Total
1 Clinical Aspects and Recent advances in
speciality
60 40 100
2 Advanced Physical and Functional Diagnoses 50 50 100
3 Advanced PT Interventions in the speciality 50 50 100
4 Clinical Training - 600 600
5 Seminars , Journal Clubs, Case- Presentations,
Teaching Skills , Field Works etc.
- 150 150
6 Research Project Work 200 200
1250

PAGE- 9
MPT SYLLABUS I YEAR
1. ANATOMY
A. COURSE CONTENT 1) Anatomy of Musculoskeletal system, (Osteology. Myology , Arthrology)
2) Anatomy of Cardio pulmonary systems (Structure of Heart , Structure of Long Broncho Pulmonary
segments)
3) Anatomy of Nervous system (Dermatomes and myotomes, cerebrum and cerebral , hemispheres,
cerebral cortex, cerebellum and its connections, brain stem- mid brain , Pons, medulla)
4) Structure of Kidney.
5) Structure of Bladder.
B. REFERENCE
1) Grays anatomy
2) Derek : Anatomy , palpanon and surface marking
3) Sieg : IIIustrated essentials of musculoskeletal anatomy
4) Nigel : Anatomy and human movement
5) Chaitow : Palpation skills assessment & Diagnosis through touch
6) Moffat : Anatomy & Physiology for physiotherapists
7) Textbook of Anatomy by T.S. Ranganathan
8) Textbook of anatomy & Physiology, by Tora Tora
9) Text book of anatomy by B.D. Chaurasia
10) Williams Peter Late : Gray’s anatomy the anatomical basis of medicine and surgery, 38 Edi 1995 .
11) Lumely John S.P. Surface Anatomy . The anatomical basis of clinical examination 2nd Edi 1995.
12) Anatomy and Human Movement – Palastanga
2- PHYSIOLOGY AND EXERCISE PHYSIOLOGY
A . COURSE CONTENT
1) Physiology of Musculo – Skeletal system
2) Phsyioloy of Cardio _ Pulmonary system
3) Physiology of nervous system
4) Physiology of bladder and bowel
PAGE- 10
B. REFERENCE
1) Offat : Anatomy & physiology for Physiotherapists
2) Robert : Fundamentals of sensory physiology
3) Guyton : Textbook of Physiology
4) Textbook of anatomy & physiology by Tora Tora
5) Chatterjee : p[ Textbook of physiology
EXERCISE PHYSIOLOGY
A . COURSE CONTENT
1) Nutrition – The basis for human performance Carbohydrates Lipids & Proteins Vitamins minerals and water Optimal Nutrition for exercise
2) Energy for physical activity - Energy value of food introduction to energy transfer, energy, transfer in the body phosphate bond energy, energy released from food energy transfer n exercise measurement of human energy expenditure Human energy expenditure during rest and physical activity Energy expenditure during walking , jogging running and swimming individual differences and measurement of energy capacities.
3) System of energy delivery and utilization : the cardiovascular system cardiovascular regulation and integration functional capacity of cardiovascular system .
4) Dynamics of pulmonary ventilation : Regulation of pulmonary ventilation, pulmonary ventilation during exercise, acid – base regulation .
5) The endocrine system: Organization, acute, and chronic response to exercise.
6) Enhancement of energy capacity Training fro anaerobic and aerobic power muscular strength: Training muscles to become stronger strength measurements and resistance training, structural and functional adaptation to resistance training special aids to exercise training and performance.
7) Exercise performance and environmental stress Exercise at medium and high attitude exercise and thermal stress – Mechanism of thermo regulation . Thermoregulation and environmental stress during exercise Sport diving Micro gravity : the cost frontier.
8) Body composition assessment, physique. Performance, and physical activity over weight , obesity and weight control.
9) Body composition, energy balance and weight control
10) Exercise, successful, aging and disease prevention.
11) Physical Activity , health aging physical activity in the population aging and physiologic function physical activity, health and longevity Coronary heart disease.
12) Clinical Exercise physiology for cancer, cardiovascular and pulmonary Rehabilitation.
B. REFERENCE
1) Axen : Illustrated Principal of exercise physiology
2) Katch : Exercise physiology energy nutrition and human performance
3) Frank : Exercise Physiology for health care professionals
4) Kisner : Therapeutic exercise foundation and technique
5) Power : Exercise Physiology
PAGE- 11
6) Basmajian : Therapeutic exercises
7) Brunnstorn : Movement therapy
8) Lamb : Physiology of exercise .
3. BIOSTATISTICS , RESEARCH METHODOLOGY AND PT EDUCATION & ETHICS
A. COURSE CONTENT
1) Introduction t Statistics
2) Exploratory tools for unvaried date types of variables : quantitative and qualitative variables Simple plots for continuous variables – dot plots , stem and leaf plots, histograms, interpreting plots numerical summarizes fro continuous variables – Mean, mode and standard deviation, quartiles, percentiles Interquartiles range Frequency tables various types of graphs, obtaining graphs using statistical Software’s like Excel, Miritah. 5 Plus.\
3) Probabilities and Proportion - Introduction to probability and proportions.
4) Discrete random variables - Binomial distribution Expected value for the mean and standard deviation.
5) Continuous random variables - Normal distribution, 2 score Obtaining normal distribution probabilities from tabular and statistical software’s
6) Sampling distribution of estimates - parameters and extimates sampling distribution of sample proportions standard errors of differences students t-distribution
7) Confidence intervals - confidence intervals for mean Confidence internals for difference between mean confidence internals for difference between proportions obtaining Confidence intervals using statistical software like excel, menials, and 5 plus.
8) Significance testing - difference between tests and intervals Types of hypothesis – research hypothesis , Null hypothesis- T tests and P values distinction between statistical and clinical significance.
9) Tables of counts One dimensional tables – chi square test for goodness of fit tables for the Chi
square distribution Two way tables of counts – Chi square test of homogeneity Chi square test of
independence. 2x2 table. Validity of Chi – square test performing the Chi square test using
statistical software like excel, minitah and plus.
10) Data on a continuous variable One way analysis of variance and the f-rest The f-rest and analysis of variance table.
11) Relationship between quantities variables: regression and correlation- correlation versus regression
Relationship modeling: The straight line inference for the simple linear model – inference about
stop and intercept, regression model and prediction, model checking Correlation and association:
Two regression lines, correlation co-efficient.

PAGE- 12
B. REFERENCE
1) Carolin hicks’ research for physiotherapist
2) Mehtod’s in biostatics B.K. Mahaja.
3) John : Statistics a guide for therapists
4) Jan : basic statistics for health care research
5) Barbara : Statistical methods for healthcare research.
6) Barlene : documenting functional outcomes in physical therapy
RESEARCH METHODOLOGY
A. COURSE CONTENT
1) INTRODUCTION TO RESEARCH
a) The importance of research in physiotherapy. Physiotherapy Past. Present and Future. Paradigms. The positivist paradigm an the naturalistic paradigm.
b) Ethical Consideration in physiotherapy Research. Introduction the conceptual. Empirical and interpretive Quantitative and qualitative Research: phases of research.
2) CONCEPTUAL PHASE
a) Formulation of the problem: Basic terms relating to research problems - Development and refinement of research problems Communication the research problem , purpose and questions.
b) Concepts and variables: Phenomena, concepts and constructs Theory – Variables: Dependent variables and independent variables. Operational definition of variables.
c) Literature Review and theoretical basis - Purpose and use of Literature review . Locating relevant literature fro a review: use of electronic databases like Medicine. CLINAHL and ALT HEALTHWATHCH etc. Preparing written literature reviews Reading and using existing research reviews Reading and using existing research reviews Theories, models and frameworks.
d) Hypothesis: Function of hypothesis in quantitative research - Types of Hypothesis. Characteristics of testable hypothesis Wording of the Hypothesis. Brief introduction to Hypothesis testing.
3) EMPIRICAL/ CONDUTING PHASE
a) Research Design - Quantitative Research Designs : Experimental Research : Characteristics of experiments. Basic designs ,Factorial design. Repeated measures design. Advantages and disadvantages of experiments Quasi-Experimental Research Non – equivalent control group design. Time series design. Advantages and disadvantages of quasi experiments non experimental.
b) Research : Co relational Research. Advantages and disadvantages of non- experimental research - Research design and the time dimension Cross- sectional designs., longitudinal designs specific types of quantitative research surveys, Evaluations , and outcomes research Techniques of research control what is research control ? controlling extrinsic & intrinsic factors qualitative research design Distinction between quantitative & qualitative design qualitative research tradition :Brief overview of ethnography phenomenology & grounded theory Brief overview of qualitative & quantitative approaches.
PAGE- 13
c) population & sample - population target population accessible population sampling rationale Non- probability sampling convenience sampling quota sampling purposive sampling advantages and disadvantages of non- probability sampling Probability sampling simple random sampling , stratified random sampling cluster sampling , systematic sampling , advantages and disadvantages of probability sampling Sample size in quantitative studies sampling in qualitative research- logic types and size .
d) Collection of data - Data collection methods : Self Reports : Interviews , questionnaires, scales advantages and disadvantages of self reports methods, observational methods _ Structured and unstructured observational methods, advantages and disadvantages of observational methods Biophysiologic measures : In vivo measures in vitro measures , Advantages and disadvantages of Biophysiologic measures Measurement and assessment of quantitative data: Measurement : Errors of Measurement, Readability of measuring instruments : Content validity , criterion related validity, construct validity. Assessment of qualitative data , Credibility prolonged engagement and persistent observation triangulation . peer debriefing and member cheeks searching for disconfirming evidence Dependability Conformability Transferability
f) Research data and analysis - Analysis of quantitative data Descriptive statistics : Frequency distribution , central tendency variability , bi variant descriptive statistics _ contingency table and correlation Inferential statistic : Sampling distributions hypothesis testing type I and II errors level
of significance. Statistical significance. Parametric and nonparametric tests, a nova chi squared test correlation co-efficient, regression NCOV.
Note : In this par the course, the emphasis will be on application and interpretation of the tests rather than computation analysis of qualitative data : General Consideration is qualitative analysis. Qualitative data management and organization – categorization coding Overview of grounded theory analysis, phenomenological analysis .
4) INTERPRETIVE PHASE
a) Discussion and conclusions : interpreting quantitative results Interpreting hypothesized significant results , interoperating non – significant results interpreting UN hypothesized significant results interpreting mixed results;
b) Interpreting qualitative results
5) CRITIQUING PUBLISHED RESEARCH
a) Need for critiquing research
b) Guidelines for critiquing research
6) WRITING RESERCH FOR PUBLICATON
Guidelines fro writing research – Title, abstract introduction. Literature review. Methodology results, discussion referencing documenting and structuring papers in social science using the American psychological association (APA) style guide (can be downloaded from the website http//www.apastyleguide.org. plagiarism and copyright laws
B. REFERENCE 1) Introduction to Research in Health Sciences – Poddar S. Churchhill Livingstone, London 1988
2) Elements of Research in physical therapy – Currier D.P. Williams & Wilkins, Baltimore 1990 Ed. 3
3) Hand Book of Research Method – Sproull, Scarecrow Press, 1998
4) Physical Therapy Research – Domholdt , W.B. Saunders, Philadelphia. 1993

PAGE- 14
4. MOVEMENT SCIENCE (BIOMECHANICS AND KINESIOLOGY)
A) COURSE CONTENT
1) BASIC MOVEMENT TERMINOLOGY – Core areas of study – Anatomy functional Anatomy, Biomechanics, Kinesiology, Liner motion. Angular motion, kinematics, kinetics. Static and dynamic. Anatomical movement description – segmental names, anatomical terms. Movement descriptions – basics and specialized. Relative systems – relative – Absolute. Planes/axis. Characters of joint movement – single and multiple joint movements.
2) SKELETAL CONSIDERATION OF MOVEMENT – Functions of skeletal system. Types of bones. Biomechanical Characteristics of bones :- Bone tissue, architecture of bone, strength and stiffness of bone . Types of load. Bony articulations. Types of joints and its descriptions such as diarthrodial or synovial etc.
3) MUSCULAR CONSIDERATIOIN FOR MOVEMENT - Structure of muscle. Physical organization of muscle. Fiber organization, Fiber type. Muscle attachment. Functional characteristics of muscles, Muscle fiber potential. Functions of Muscles, Role of Muscle, Mechanical components in the muscle, Net muscle action . Factors influencing muscle force. Angle of attachment of muscle . length – tension relationship, force velocity relationship, stretch shortening cycle, one and two joint muscle. Extra and intra fusal muscle fibers, Action potential, evoke potential kinetic potential , Torque. Power strength & Endurance.
4) NEUROLOGICAL CONSIDERATIONS FOR MOVEMENT :- General Organization of nervous system. Motor neurons. Structure of the motor neuron. Motor unit. Functional characteristics of motor unit. measurement of motor unit activities. Sensory neurons. Functions of neural control. Reflex arc, myotonic, proprio spinal and supra spinal reflexes, sensory receptors – muscle spindle – nuclear bag, nuclear chain fibers. Gamma and fusimotor . innervations’ Golgi tendon organ (GTO) Joint receiptors.
5) FUNCTIONAL ANATOMY - Classifications of joints (Natural, Anatomical & Kinesiological) for Upper extremity. Lower extremity The trunk (spine)
6) PATHOMECHANICS & PATHOKINETCS OF PARALYTIC DISABILITIES - Joints of Upper extremity. Joints of Lower extremity. The trunk (Spine)
7) ERGONOMIC – Work capacity analysis roe of physiotherapy industrial setup. Job site disability. Pre – employment screening. Workers functional capacity assessment, work hardening Programme industrial therapy CCINC. Postural examination, Job task analysis, educational Programme. For prevention of injury, adult education, document .
Practical agronomy for different section in the society.
WORKING CLASS - Labour. Hard labour. Very hard labour
CHAIR CLASS. EXECUTIVE CLASS. BUREACRATICS CLASS ……. CLASS

PAGE- 15
B. REFERENCE
1) Biomechanics of Human Joints - Cynthia Norkin
2) Biomechanics of Human Joints - Kapand J.
3) Clinical Kinesiology – Brunstorms
4) Biomechanics of Joints – Frankel Nordin
5. ADVANCED P.T. MODALITIES AND
DIAGNOSTIC TECHNIQUE
A) OBJECTIVES
• The students should have in depth knowledge of the Electrotherapy modalities, their
configurations, instrumentation and the principles on which the machine works (Physics), the clinical
implications (selection of dosage, techniques. indications, contraindications, method of application,
precautions, advantages, dangers, therapeutic effects physiological effects, uses) and sound rationale
for selecting a particular modality in a specific condition, able to justify how the modality selected is
suitable for the particular condition.
• To trouble shoot a problem early, physiotherapist should know the circuit. various designs and
replacements of all the equipments, if he/she handles.
• The student should find should find solutions for recurrent problems/remedial measures.
• The students should also have a knowledge about varies investigative procedures and method of
reading the images and the results.
• Additionally, student should update with the latest development with regard to Electro modality by
critically reviewing the journal. (In practical and orals, a candidate will be asked questions with regard
to recent advances and evidence that he/she has reviewed the journals. In orals, examiner should
have discussions with regard to recent advances).
B) COURSE CONTENT
1) INTRODUCTION TO PHYSICAL AGENTS - • Definition, Categories, History of Physical Agents • History of physical agents in Medicine and Rehabilitation • Roll of physical agents in rehabilitations • Effects of physical agents.
Thermal Agents - • Cryotherapy, Moist heat therapy, Contrast bath, Hydro collateral Packs. Wax therapy.
Electromagnetic radiations - • Short wave diathermy – Pulsed and continuous, Micro Wave diathermy – Pulsed and continuous, ultra violet therapy, ultra sound, laser.
2) PRINCIPLES OF NEURO-MUSCULAR EXCITATION- • Interferential therapy (IFT). transcutaneuous electrical nerve stimulation ( TENS), Electrical Stimulation – Faradic, Galvanic, SD curve etc. lontophoreis. Russian Currents, dynamic currents • Mechanical modalities – Electronic traction Sustained traction – effects, Compression, Continuous passive motion to alleviate

PAGE- 16
impending Post Traumatic Stiffness (PTS) • Shock wave therapy- Used widely as a revolutionary measure for almost all reactive inflammatory conditions.
3) ELECTRO PHYSIOLOHGY & ELECTRO DIAGNOSTIC - • Excitable issue-Nerve Excitation and conduction • Measurement of electrical events, ionic basis of excitation and conduction • Physiologic basis of nerve conduction tests- their reliability & access.
Excitable Tissue Muscle- • Skeletal muscle, Electrical phenomena and ionic fluxes, contractile responses, Physiological basis of Electromyogram (EMG) • Cardiac Muscle: Electrical properties. Electro cardiogram (ECG). Physiological basis of ECG- Normal & Abnormal ECG • Smooth Muscle: Electrical properties • Electrical events at synapse, chemical transmission of synaptic activity • Electrical and ionic events in receptors • Electro Encephalogram (EEG) - Physiological basis • Echocardiogram & Doppler studies.
Physiology of Pain - • History of clinical neurophysiology • an introduction to electro diagnostic signals and their measurements • Nerve conduction study. Principles of nerve conduction, study, median nerve, Ulnar nerve, radial nerve, brachial plexus, cervical radiculopathy, lumber plexus and its terminal branches, lumbosacral radiculopathy, anomalous innervations of the extremities, nerve conduction of non limb nerves, late responses. Autonomic nervous system resting.
• Electromyography–Introduction to electromyography, technique of electromyography.
• Clinical application of electromyography and nerve conduction. Electromyography findings in neurological disorders, nerve conduction ND and EMG studies in Polyneuropathy.
• Repetitive nerve stimulation.
• Single fiber and macro electromyography.
• Visual evoked potential.
• Brainstem auditory evoked potential.
• Somatosensory evoked potentials.
• Motor evoked potential.
a. RADIOLOGY, RADIO DIAGNOSTICS & SONOGRAPHY- • Introduction to radiography, radio imaging and radio diagnostic • Dimension in radiography • Radio density • A roentgen rose • Analysis of image • Positioning, Viewing of radiograph, film markers • Image quality factors – Radiographic density, contrast, distortion, recorded results
Common Imaging Studies - • X-ray – spinal, skull and peripheral • conventional topography • Computed tomography (CT) • Contrast enhanced radiography • Radio Nuclide scan • Magnetic resonance imaging (MRI) with spectroscopy • Positron emission tomography (PET) • Myelography • Nuclear imaging • Pneumoencephalogram • Electro encephalography (EEG) • Ultra sonogram • Echocardiogram & Doppler studies • MUGA – Nuclear test.
B. REFERENCE
1) Low and Rced : Electrotherapy Explained
2) Nelson : Clinical Electrotherapy
3) Claytons : Electrotherapy
4) Kimura : Electro Diagnosis in disease of nerve and muscle
5) Joseph Khan : Electrotherapy Explained

PAGE- 17
6) Prentice : Therapeutic Modalities and Sports Medicine
7) Cameron : Physical agents in Rehabilitation
II YEAR
MPT ORTHOPEDICS
1. CLINICAL ASPECTS AND RECENT ADVANCES IN ORTHOPEDICS
A) COURSE CONTENT
1. Embryological development of musculoskeletal system.
2. Osteology: Structure of bone, ossification of bones, Skull bones, Facial bones, Bones of Upper Extremity, Pelvis, Vertebral Column, ribs.
3. Myology: Structure of muscle, Types of muscle, muscle fibers, Origin, insertion, action, Nerve supply of Muscles of Face, Upper Extremity, Lower Extremity, Trunk.
4. Arthrology: Structure of joint, types of joints, detailed structure and formation of all the joints, detailed structure and formation of all the joints, Neurobiology of joint.
5. Neurology: Peripheral Nerves; Peripheral Nerves; Dermatomes and myotomes, Physiology: joint physiology [Movements], muscle physiology. Patho mechanics of Fractures, deformed joints.
B) CLINICAL CONDITIONS
1) Definitions Causes, Clinical Features, Patho physiology, general investigation {blood test, serum, creatinine, etc.}, Medical and surgical management of the below mentioned conditions:
2) Fractures and dislocation- • Upper Limb: Fracture of clavicle, scapula, humerus, forearm bones, carpal bones, metacarpal bones, and phalanx. Shoulder dislocation, elbow dislocation, dislocation of radius, dislocation of radio-ulnar joint, dislocation of carpo metacarpal joint of thumb • Lower Limb: Fracture of Pelvis, femur, patella, tibia, fibula, tarsal bones, metatarsal, and phalanx. Dislocation of hip, patella, knee, ankle, sub-talar joint • spine: Fractures and dislocation sub- luxation of vertebra • skull Bones and Ribs. (With emphasis made to Post traumatic complications & preventive Measures). Amputation.
3) Sprains and Strains: Injuries of soft tissue of body.
4) Disease of joints: • Infective, Rheumatoid, Degenerative, Neuropathic. Metabolic, Arthritis in systemic disorders, Miscellaneous, Periarthritis, juvenile rheumatoid arthritis.
5) Deformities; of Upper limb, lower limb and spine.
6) Plexus and peripheral nerve injuries.
7) Arthropathies: • Spondylitis Spondyllolisthesis, spondylosis, Ankylosing •Spondylitis.
8) Metabolic diseases of bones: • Osteopenia, Rickets, Osteomalacia. Osteoporosis.
9) Tumors of bones and joints.
10) Infectious disorders of bones and joints.
PAGE- 18
11) Congenital disorders.
12) Developmental disorders bones.
13) Bony Abnormalities secondary to endocrine disorders.
14) A vascular necrosis of bone and epiphyseal osteochondritis.
15) Disorders of bone& joint secondary to neurological conditions like: • Cerebral palsy, anterior poliomyelitis, Leprosy, Spinal cord injuries,.
16) Disorders of bone & joint secondary to neurological conditions like • Cerebral palsy, anterior
poliomyelitis , Leprosy, spinal cored Injuries.
17) Disorders of bone & joint secondary to Muscular Dystrophies • Arthogryposis Multiplex congenital.
Fibro dysplasia progressiva.
18) Regional conditions of neck and upper limb: •Brachial neuralgia, cervical rib, Thoracic outlet syndrome Torticollis , Supraspinatus Syndromes, Rupture of rotator cuff, Deltoid fibrosis, Tennis Elbow, Ganglion, Dequearvain’s disease, Trigger finger, Trigger thumb, Carpal tunnel syndrome. Deputrens contracture.
19) Regional Conditions of Lower limb & Spine: • Backache, Lumbo sacral strain, Fibrositis Back, Sacralisation of 5th lumbar vertebra. IVAP. Lumbar canal stenosis, Epiphyseolysis. Idiopathic chondrolysis of hip. Quadriceps fibrosis, Bursitis around the knee, Loose bodies in the knee, Chondromalacia patella, planter facitis, Calcaneal spur, Osgood Schlatter disease, Tarsal tunnel syndrome.
20) Miscellaneous: • Perthes disease, Paget’s disease, Connective tissue disorders (SLE. Polymyositis, dermatomyositis, polyarteritis nodosa).
21) Bone, skin grafting/tendon transfer procedures: • The student should know the latest advances in orthopedic surgical procedures.
22) Sports injuries: • Classification of sports injuries, bio mechanics of common sports injuries, head injuries in sports, running injuries, swimming injuries, facial injuries, neck pain, shoulder pain, elbow pain, forearm pain, wrist pain and other regional condition that is related to sports and common sports related infections etc.
23) Geriatric condition: • Theories of aging, physiological changes of musculoskeletal changes in aging, aging of nervous system and other pathological manifestations of aging, etc.
24) Chronic pain: • Historical perspective, theories of pain, and classification of pain, clinical manifestations, etc.
25) Surgical procedure: • Describe the following surgical procedures: osteomotomy, arthodesis, arthoplasty, etc.
26) Hand injuries: • Flexor tendon injuries, extensor tendon injuries, nerve compression syndromes, nerve injuries, cumulative trauma, traumatic injuries to hand, reflex sympathetic dystrophy, rheumatoid hand, evolution of thumb, and other regional hand conditions etc.

PAGE- 19
27) Orthopaedics problem in paediatric patients: • clavicular fracture, humeral fracture, supracondlylar fracture, nursemaids elbow, Hip fracture, tibial fracture, ankle fracture, and other regional condition that is related to paediatric cases.
28) Miscellaneous condition: • Myofascial trigger point (definitions, types, pathophysiology, clinical features etc.)
2. ADVANCED PHYSICAL AND FUNCTIONAL DIAGNOSTS
A) COURSECONTENT
1) Principles and Concepts - • Patient history, Observation, Examination • Principles, Scanning examination, Examination of specific joints, Functional Assessment, Special Tests, Reflexes and Cutaneous • Distribution, joint play Movement, Palpation, Diagnostic Imaging.
2) Head and Face - • Patient History, Observation, Examination • Examination of the Head, Examination of the face, Examination of the Eye, Examination of the Nose, Examination of the Teeth, Examination of the Ear, Special, Tests, Reflexes and Cutaneous Distribution, Joint play Movements, Palpation, Diagnostic Imaging.
3) Cervical spine - • Patient History, Observation, Examination • Active movements, Passive movements, Resisted Isometric Movements, Functional Assessment, Special Tests Reflexes and Cutaneous Distribution, Joint play Movements, Palpation, and Diagnostic lmaging.
4) Tempero mandibular Joint - • patient History, Observation, Examination • Active movement, Passive movements, Resisted Isometric Movements, Functional Assessment, Special Test, Reflexes and Cutaneous Distribution, joint play Movements, Palpation and Diagnostic Imaging.
5) Shoulder - • Patient History, Observation, Examination • Active movements, Passive movements, Resisted Isometric Movements, Functional Assessment, Special Tests, Reflexes and Cutaneous Distribution, Joint play Movements, Palpation and Diagnostic Imaging.
6) Elbow - • Patient History Observation, Examination • Active movements, Passive movement, Resisted Isometric Movements, Functional Assessment, Special Tests, Reflexes and Cutaneous Distribution, Joint play Movements, Palpation, and Diagnostic Imaging.
7) Forearm. Wrist and Hand Finger Deformities, Other physical Finding, Examination • Active Movements, Passive movements, Resisted Isometric Movements, Functional Assessment, Special Tests, Reflexes and Cutaneous Distribution, Joint play Movements, Palpation, and Diagnostic Imaging.
8) Thoracic (Dorsal) - • Patient History, Observation, Examination • Kyphosis, Scoliosis, Breathing, Chest Deformities, Active Movements, Passive movements, Resisted Isometric Movements, Functional Assessment, Special Tests, Reflexes and Cutaneous Distribution, joint play Movements, Palpation, and Diagnostic Imaging.
9) Lumber Spine - • Patient History, Observation, Examination • Active movements, Passive movements, Resisted Isometric Movements, Functional Assessment, Special Tests, Reflexes and Cutaneous Distribution, Joint play Movements, Palpation, and Diagnostic Imaging.
10) Pelvis - • Patient History, Observation, Examination • Active movements, Passive movements, Resisted Isometric Movements, Functional Assessment, Special Tests, Reflexes and Cutaneous Distribution, Joint play Movements, Palpation, and Diagnostic Imaging.

PAGE- 20
11) Hip- • Patient History, Observation, Examination • Active movements, Passive movements, Resisted Isometric Movements, Functional Assessment, Special Tests, Reflexes and Cutaneous Distribution, Joint play Movements, Palpation, and Diagnostic Imaging.
12) Knee - • Patient History, Observation, Examination • Active movements, Passive movements, Resisted Isometric Movements, Functional Assessment, Special Tests, Reflexes and Cutaneous Distribution, Joint play Movements, Palpation, and Diagnostic Imaging.
13) Lower leg, Ankle and Foot - • Patient History, Observation, Examination • Active movements, Passive movements, Resisted Isometric Movements, Functional Assessment, Special Tests, Reflexesand Cutaneous Distribution, Joint play Movements, Palpation, and Diagnostic Imaging.
14) Assessment of Gait - • Normal Patterns of Gait • Stance Phase, Swing Phase, Joint motion during normal gait • Normal Parameters of Gait • Base width, Step length, Stride length, lateral pelvic shift, Vertical pelvic shift, Pelvic rotation, Center of gravity, Normal cadence • Overview and patient story • Observation • Footwear • Examination •Locomotion score, Compensatory Mechanisms.
15) Abnormal Gait - • Antalgic (painful) Gait, Arthrogenic (stiff Hip or Knee) Gait, Ataxic Gait, Ataxic ait, Contracture Gaits, Equines Gait, Gluteus Maximus Gait, Gluteus Medius (Trendelenburg’s) Gait, Hemiplegic or Hemiparetic Gait, Parkinson’s Plantar flexor Gait, Psoriatic limp, Quadriceps Gait, Scissors Gait short Leg Gait, Steppage or Drop Foot Gait.
16) Assessment of Posture - • Postural development • Factors affecting posture, Causes of poor posture • Common spinal Deformities • Lordosis, Kyphosis Scoliosis • Patient History • Observation • Standing, Forward Flexion, Sitting, Supine Lying, Prone Lying • Examination.
17) Assessment of the Amputee - • Levels of amputation • Patient History, Observation, Examination • Measurements related to Amputation • Active movements, Passive, Movements, Resisted Isometric Movements, Functional Assessment, Sensation Testing, Psychological • Testing, Palpation, Diagnostic Imaging.
18) Assessment & evaluation of pain - • Apart from the above student is expected to learn assessment and evaluation in the following clinical conditions (preoperative & Post operative)
a) Fractures and dislocations: • Upper Limb: Fracture of clavicle, scapula, humerus, forearm bones, carpal bones, metacarpal bones, and phalanx Shoulder dislocation, elbow dislocation, dislocation of radius, dislocation of radio-ulnar joint, dislocation of carpo- metacarpal joint of thumb • Lower limb: Fracture of Pelvis, femur, patella, tibia, fibula, tarsal bones, metatarsal, and phalanx, Dislocation of hip, patella, knee, ankle, sub-talar joint • Spine: Fractures and dislocation subluxation of vertebrae • Skull Bones and Ribs. (With emphasis mad to Post traumatic complications & preventive & preventive Measures).
b) Amputation.
c) Sprains and Strains: Injuries of soft tissue of body.
d) Disease of joints; Infective, Rheumatoid, Degenerative, Neuropathic, Metabolic, Arthritis in systemic disorders, Miscellaneous, Peri- arthritis, juvenile rheumatoid arthritis.
e) Deformities: of Upper limb, lower limb and spine.
f) Plexus and peripheral nerve injuries.
g) Arthropathies: Spondylitis, Spondylolisthesis, spondylosis, Ankylosing spondylitis.
h) Metabolic diseases of bones, Osteopenia, Rickets, Osteomalacia, Osteoporosis.
i) Tumors of bones and joints.
j) Infectious disorders of bones and joints.

PAGE- 21
k) Congenital disorders.
l) Developmental disorders bones.
m) Bony Abnormalities secondary to endocrine disorders.
n) Avascular necrosis of bone and epiphyseal osteochondritis.
o) Disorders of bone & joint secondary to Muscular Dystrophies: Arthrogryposis Multiplex Congenita, Fibro dysplasia progressiva.
p) Disorders of bone & joint secondary to Muscular Dystrophies: Arthrogryposis Mulitplex Congenita, Fibro dysplasia progressiva.
q) Regional conditions of neck and upper limb: Brachial neuralgia, cervical rib, Thoracic, outlet syndrome Torticollis, Supraspinatus Syndromes, Rupture of rotator cuff, Deltoid, fibrosis, Tennis Elbow, Ganglion, Dequervain’s disease, Trigger finger, Trigger thumb, Carpal tunnel syndrome, Deputrens contracture.
r) Regional Conditions of Lower limb & Spine: Back ache, Lumbo sacral strain, Fibrositis back, Sacralisation of 5th lumbar vertebra, IVDP, Lumbar canal stenosis, Epiphyseolysis, Idiopathic chondrolysis of hip, Quadriceps fibrosis, Bursitis around the knee, Loose bodies in the knee, Chondromalacia patella, plantar fascitis, Calcaneal spur, Osgood Schlatter disease, Tarsal tunnel syndrome.
s) Miscellaneous: Perthes disease, Paget’s disease, Connective tissue disorders (SLE. Polymyositis, dermatomyositis, polyarteritis nodosa).
t) Bone, skin grafting/tendon transfer procedures.
19) Assessment of spots injuries - • Principles of diagnosis, preliminary health screening, and risk classification, assessing cardio respiratory fitness, assessing strength and muscle endurance, assessing cardio respiratory fitness, assessing strength and muscle endurance, assessing body composition, assessment of flexibility, stress assessment, assessment of other sports related regional condition etc.
20) Assessment of geriatric condition - • Assessment instruments-mental status assessment, functional assessment, modified physical therapy assessment (musculoskeletal, gait, cardio pulmonary assessment NCV. ethnicity assessment, patient evaluation and other geriatric related assessment etc.)
21) Chronic pain assessment- • Patient interview, body charts, and pathological assessment (SIP, MPI, MCGILL, PAIN questionnaire, vas, sel-90 and other methods of pain assessment).
22) Assessment of following surgical procedures – • Describe the following surgical procedures: osteomotomy, arthodesis, arthoplasty, etc.
23) Assessment of hand - • Clinical evaluation of hand, sensibility testing, functional evaluation, hand volume measurements of its m9otion for fingers and thumb, grip and pinch strength measurements, boyes classifications, assessment of rheumatoid hand and other methods of hand evaluation etc....
24) Assessment of orthopaedic problem in paediatric cases - • Clavicular fracture, humeral fracture, supracondlylar fracture, nursemaids elbow, Hip fracture, tibial fracture, ankle fracture, and other regional condition that is related to paediatric cases, etc.
25) Implications and management - • Total hip replacement • Total knee replacement •Arthroplasty • Arthroscopy • lllizaro ring fixation • External fixation.
26) Implications and management - • Disability evaluation • Assessment of urinary incontinence •Assessment of trunk muscles dysfunction • Evaluation of Swiss ball’ exercise prescription for orthopaedic problems •Clinical reasoning processes • Assessment of myofascial trigger point-diagnosis, pressure algometry etc, Student is expected to learn the latest developments in the assessment and evaluation protocols used in orthopedic physiotherapy.

PAGE- 22
3. ADVANCED PHYSIOTHERAPEUTIC INTERVENTIONS Student should learn the physiotherapy interventions and recent advance in the physiotherapy management of following conditions. (Preoperative’& Postoperative)
A) COURSE CONTENT
1) Fractures and dislocations - • Upper Limb: Fracture of clavicle, scapula, humerus, forearm bones, carpal bones, metacarpal bones, and phalanx. Shoulder dislocation, elbow dislocation, dislocation, dislocation of radius, dislocation of radio-ulnar joint, dislocation of carpo metacarpal joint of thumb • Lower Limb: Fracture of Pelvis, femur, patella, tibia, fibula, tarsal bones, metatarsal, and phalanx. Dislocation of hip, patella, knee, ankle, sub-talar joint • Spine: Fractures and dislocation subluxation of vertebrae • Skull Bones and Ribs (With emphasis made to Post traumatic complications & preventive Measures)
2) Amputation.
3) Sprains and Strains: Injuries of soft tissue of body.
4) Disease of joints- • Infective, Rheumatoid, Degenerative, Neuropathic, Metabolic, Arthritis in systemic disorders, Miscellaneous, Periarthritis, juvenile rheumatoid arthritis.
5) Deformities of Upper limb, lower limb and spine.
6) Plexus and peripheral nerve injuries.
7) Arthropathies: Spondylitis, Spondylolisthesis, spondylosis, Ankylosing Spondylitis.
8) Metabolic diseases of bones. • Osteopenia, Rickets, Osteomalacia, Osteoporosis.
9) Tumors of bones and joints.
10) Infectious disorders of bones and joints.
11) Congenital disorders.
12) Developmental disorders bones.
13) Bony Abnormalities secondary to endocrine disorders.
14) Avascular necrosis of bone and epiphyseal osteochondritis.
15) Disorders of bone & joint secondary to neurological conditions- like: Cerebral palsy, anterior poliomyelitis, and Leprosy Spinal cord injuries.
16) Disorders of bone & joint secondary to Muscular dystrophies: Arthrogryposis Mulitplex Congenita,Fibro dysplasia progressiva.
17) Regional conditions of neck and upper limb: Brachilal neuralgia, cervical rib, Thoracic outlet syndrome, Torticollis, Supraspinatus Syndromes, Rupture of rotator cuff, Deltoid fibrosis, Tennis Elbow, Ganglion, Dequervain;s disease, Trigger finger, Trigger thumb, Carpal tunnel syndrome, Deputrens contracture.
18) Regional Conditions of Lower limb & Spine: Back ache, Lumbo sacral strain, Fibrositis Back, Sacralisation of 5th lumbar vertebra, IVDP, Lumber canal stehosis, Epiphyseolysis, Idiopathic chondrolysis of hip, Quadriceps-fibrosis, Bursitis around the knee, Loose bodies in the knee, Chondromalacia patella, planter facitis, Calcaneal spur, Osgood Schlatter, disease, Tarasl tunnel syndrome.

PAGE- 23
19) Miscellancous: Perthes disease, Paget’s disease, Connective tissue disorders (SLE. Polymyositis, dermatomyositis, polyarteritis nodosa).
20) Bone, skin grafting/tendon transfer procedures.
21) Manual therapy intervention for orthopaedics problem: Maid land’s conepts. mulligan mobilization- concepts, principles, MWMS, SNAGS, osteopathic approaches, McKenzie approaches, and David buters’ nervous tissue mobilization etc.
22) Swiss ball management for orthopaedics problems: History of Swiss ball, point of observation, planning of exercises, evaluation, and treatment, exercises prescription and assistive devices etc.
23) Core stabilization exercises: Concepts, principles and applications etc.
24) Management of myofascial trigger point: Medical, physical therapy interventions and ergonomics management etc.
25) Management of incontinence (Conservative and other moderns; procedures)
26) KALTENBORN AND CYRIAX – (concepts, principles and techniques of applications)
27) Sports physical therapy: Principles of injury prevention, principles of treatment, principles of rehabilitation, taping procedures, bracing procedures, and other practical spots medicine etc.
28) Geriatric rehabilitation: Principles of and practice in geriatric rehabilitation and orthopaedic treatment consideration etc.
29) Chronic pain management: Medical, central pain management and other physical therapy interventions etc.
30) Physical therapy for following surgical procedures: Osteomotomy, arthodesis, arthoplasty, (pre operative and post operative Mangement) etc.
31) Hand rehabilitation: Concepts in clinical treatment, therapeutic exercises, physical agents and electrotherapy techniques inhand rehabilitation, and role of hand splint inrehabilitation etc.
32) Treatment for orthopaedic problems in paaeadiatric cases: Clavicular fracture, humeral fracture, supracondylar fracture, nursemaids elbow Hip fracture, tibial fracture, ankle fracture, and other regional condition that is related to paediatric cases, etc.
33) Miscellaneous: • Role of physical therapist in-DM and obesity, • Effects of acupuncture and yoga therapy in orthopaedic problems • Wheelchair prescription • Role of PNF in orthopaedic condition• Common methods of improving muscular strenght, flexibility and endurance • Burnscomplications and its physiotherapeutic interventions • Physiotherapeutic interventions for relief of pain. Apart from the above student should learn Basic concept of orthopedic manual therapy, orthotics & prostherics, spinal braces & corsets.
B. REFERENCE
1) Barbara : Muscles, Nerves and Movement kinesiology in daily living.
2) Loth : Orthopeacdics review for physical therapist
3) Brotzman ; Clinical orthopedic rehabilitation .

PAGE- 24
4) Magee : Orthopedic physical assessment
5) Reider : the orthopeadic assessment guide
6) Frederic : Reheumatoid arthritis .
7) Todd : Knee IIramnet rehabilitation
8) Text book of orthopedics by – Dr. Natharajan
9) Jayanth Joshi – Text book of orthopaedic for physiotherapist
10) Cash Textbook of orthopedics
11) Textbook of orthopedics – Ebnezar
12) Orthopaedic physical examination- Robert Donatelle
II YEAR MPT IN NEUROLOGY
1. CLINICAL ASPECTS AND RECENT ADVANCES IN NEUROLOGY
A) COURSE CONTENT
1) NEURO ANATOMY - • Basic units of nervous system • Central nervous system covering of CNS. Cerebral Hemisphere, Cerebral Cortex, Cerebellum, Thalamus, Basal ganglia, Hypothalamus, Limbic system, Ventricular system, CSF, Blood Brain Barrier, Blood Supply and Venous drainage of CNS. Brain Stem and Spinal Cord • Peripheral Nervous System-Spinal Nerves Cranial Nuclei and Cranial Nerves, Blood Supply, Plexus, Individual Nerves – Dermatomes, Myotomes and Sclerotomes and & NMJ • Autonomic Nerves system • Tracts: Pyramidal, Extra Pyramidal and Ascending Tracts • Development of Nervous system.It is mandatory to see and comprehend the dissected parts of the nervous system.
2) NEURO PHYSIOLOGY – Functions of all the organs mentioned below • Cerebral hemisphere, Cerebral cortex, Cerebellum, Thalamus, Basal ganglia, Hypothalamus, Limbic system, Brain stem and spinal cord, PNS & ANS •Membrane Potential Action potential, Neuro Muscular Transmission, Physiology of Hyper Sensitivity, Receptors and Effectors, Neural Circuits. Somato Sensory System, Micturition Reflex, Bowel Activity, Neurogenic shock, Nervous Regulation of Circulation, Perception, Pain Physiology of Pain, Articular Neurology, Neural Development-degeneration and regeneration, Myelination, Nerve Immunology and Aging of Nervous System.
3) NEUROSCIENCE- • Nature of movement, Motor control, Theories of Motor Control, Postural Control, Development of Postural Control, Development of Locomotion, Neural Control of Human Locomotion, Theories of Neural Control of Reach and Grasp and Plasticity.
4) PATHOMECHANICS - • The student should get well acquainted with the Pathomechanics of individual joints, gait and posture related to neurological diseases.
5) CLINICAL CONDITIONS - • Definitions, Causes, Clinical Features, pathophysiology, general investigation, Medical and surgical management of the the below mentioned conditions: Pyogenic infections of CNS • Viral Infections of CNS • Polyneuropathy • Disorders of Spinal Cord • Peripheral Nerve and plexus lesions • Cerebellar lesions • Myopathies • Cerebro-Vascular Diseases •Degenerative diseases of the nervous system • UMN syndrome •Motor neuron diseases •Congenital Myopathies •Coma • Dementia • Extra pyramidal syndrome • Encephalitis •

PAGE- 25
Autonomic disorder •Movement disorders •Peripheral nerve lesions, Paediatric neurology – CP, spinal bifida • Craniovertebral junction anomalies – Hydrocephalus • Toxic Nerve disorders – Alcohol, drug abuse, asphyxia, Cancer chemotherapy, oral contraceptive and epidural & spinal anesthesia.
2. ADVANCED PHYSICAL AND FUNCTIONAL DIAGNOSIS
COURSE CONTENT
Principle of Assessment - • Assessment of motor system • Assessment of sensory system • Assessment of Perception • Assessment of Posture • Assessment of Balance •Assessment of Pain •Assessment of Incoordination •Assessment of Higher centre •Assessment of Voluntary control • Gait analysis • Writing SOAP notes •Analysis of Functional Mobility • Assessment procedures in children & elderly • Environinental Analysis •Use of investigation measures in assessment (CT. MRI. PET etc) • Types of Impairment • Conceptual Models of Disability • Self-assessment & Self efficacy scale • Tools used in Neuro assessment (scales, grades etc) • NCV & EMG • Disability Evaluation.
Measures of cognitive impairment and disability - • Glasgow coma scale, & Children’s coma scale.
Measures of motor impairment - • Motor club assessment, River mead motor assessment, Motricity index, Trunk control test, Motor assessment scale, Modified Ashworth scale for spasticity, isomeric muscle strength & Dynamometry.
Measures of focal disability - • Standing balance, Functional ambulation categories, timed walking test, River mead mobility index, nine hole peg test, Action research arm test.
Activities of daily living and extended ADL test- •Barthel ADL index, Katz ADL index, River mead ADL scale, Kenny self Care evaluation, Nottingham extended ADL index & Global Measures of disability, Functional independence measure, PULSES profile, Measures of Handicap and quality of life, WHO handicap scale, Glasgow outcome scale, Quality of life – a measure, Environmental assessment–non-standard.
Multiple Sclerosis - • Kurtzke Multiple sclerosis rating scale, an illness severity scores for multiple sclerosis.
Stroke scales- • National institute of health stroke scale, hemispheric stroke scale, Clinical classification of stroke [Branford] & Allen score for prognosis of stroke.
Spinal cord injury- • Frankel’s scale, Motor index and sensory indices & American spinal cord in injury association assessment chart.
Pain assessment and evaluation.
Assessment of Posture, gait, co-ordination & Voluntary control.
Investigation Techniques - • CT scans, MRI, X-Ray, Nuclear imaging, EEG, NCV, EMG: Evoked potentials, Basic procedure, principles and interpretation of results and neurological conditions.
3. ADVANCED PHYSIOTHERAPEUTIC INTERVENTIONS
COURSE CONTENT
1) General Principles of Treatment.
2) Theoretical basis of treatment concepts.
3) Different types of Approaches in Neuro rehabilitation.

PAGE- 26
4) Latest advancement in Therapeutic approaches.
5) Techniques to optimize and Restoration of Functional Performance.
6) Musculoskeletal Treatment concepts applied to Neurology.
7) Hypothesis Oriented Clinical Practice.
8) Evidence based Neurological Physiotherapy.
9) Strategies to improve Motor control.
10) Physiotherapeutic intervention for patients with – Perceptual dysfunction, Balance dysfunction, mobility controls disorders, postural control disorders & Incoordination problems.
11) Role of sensory system in performance with sensory reeducation & desensitizing techniques.
12) Abnormal gait & Gait training.
13) Pain Relieving Measures.
14) Motor Learning – Theories & Stages of learning skills, Motor relearning programme.
15) Feed Back, Models of Practice & Biofeed back in clinics.
16) Plasticity.
17) Adjuncts used in Neuro rehabilitation (Swiss ball, mat etc.)
18) Splinting & Orthotic appliances in Neurological disorders.
19) Environmental Modifications& Ergonomics.
20) Clinical Psychology in Neurological rehabilitation.
21) Multi-disciplinary Team (MDT) in Neuro Rehabilitation.
22) Sensory biofeedback.
Describe problem list, assessment & physiotherapeutic treatment for following conditions.
1) UMN Syndrome.
2) Polyneuropathy.
3) Peripheral Neuropathy.
4) Motor neuron disease.
5) Myopathies.
6) Disorders of Spinal cord.
7) Cerebellar Ataxia.
8) Extra pyramidal Syndrome.
9) Movement Disorders.
10) Cerebral Palsy & Spina bifida.

PAGE- 27
11) Cerebro- Vascular Diseases.
12) Peripheral Nerve and plexus lesions.
13) Traumatic Brain injury.
14) Poliomyelitis.
15) Irreversible neurological damage beyond relearning.
B. REFERENCE
1) Barbara : Muscles , nerves and movement kinesiology in daily living.
2) Barbra : Disease of the nervous system.
3) Richard : Neurological rehabilitation.
4) Susan , neurological physiotherapy
5) Omer : management of peripheral nerve problems.
6) Darcy : Neurological rehabilitation.
7) Charles : the Neuroscience of human movement
8) Janet : a motor relearning programme for stroke .
9) Snell Richards clinical Neuro Anatomy for medical students .
10) Pediatric physical therapy- Shepard
11) John pattern : neurological differential diagnosis
12) Fredericks : Pathophysiology of motor system .
II YEAR MPT IN CARDIO- RESPIRATORY DISORDER & INTENSIVE
CARE
1. CLINICAL, ASPECTS AND RECENT ADVANCES IN CARDIO
RESPIRATORY CONDITIONS
A) COURSE CONTENT
1) ANATOMY/PHYSIOLOGY AND APPLIED ASPECTS – • Development of cardio pulmonary system • Anatomy & Physiology of cardio pulmonary system • Biomechanics of Respiration • Mechanics of breathing – work of breathing, airway resistance, lung compliance •Control of respiration •Respiratory muscle – efficiency, endurance, training, fatigue, weakness •

PAGE- 28
Normal and abnormal patterns of breathing •Cough reflex •Regulation of blood pressure • Autonomic nervous system – cardio pulmonary system •Vital signs.
2) CLINICAL CONDITIONS - • Definitions, Causes, Clinical Features: pathophysiology, general investigation, Medical and surgical management of the below mentioned conditions • Pulmonary diseases in premature babies, neonatal distress, birth asphyxia, COPD, Asthma, cystic fibrosis, lmmunological deficits, bronchiectasis, lung abscess, pneumonia, interstitial lung diseases, lung cancer, pulmonary tuberculosis, Occupational lung disorders, fracture ribs, pnemothorax, haemothorax, empyema •Congenital heart diseases – persistant ductus arteriosus, co-arctation of aorta, atrial septal defect, ventricular septal defect, transposition of great vessels, tetralogy of fallot • Coronary artery diseases and its manifestation • Valvular diseases disease • Burns, cardiopulmonary complications in burns • Indications and Various types abdominal surgeries.
2. ADVANCED PHYSICAL AND FUNCTIONAL DIAGNOSIS
A) COURSE CONTENT
1) MEASUREMENTS & DOCUMENTATION- • Measurements- Types of measurement, Selecting, measurements, performing measurements, Interpreting measurements •Documentation Purpose of documentation, Types of documentation, General guidelines for content and organization: i) Subjective information, ii) Objective information, iii) Assessment, iv) plan, v) Summary.
2) HISTORY- •History of illness, past medical history, Present medical history, occupational history, Social history, history of personal habits (smoking), Family history, previous treatment history.
3) GENERAL RESPIRATORY EVALUATION - • History, chest examination.
4) COMPONENTS OF CHEST EXAMINATION - • Inspection – a. Evaluation of general appearance, topographical anatomic land marks, b. Specific evaluation of head and neck, c. Chest wall configuration, Chest wall deformities, d. Evaluation of cough, and sputum, Anemia, Cyanosis, Clubbing, Respiratory Pattern •Auscultation – a. The stethoscope, b. Nomenclature & interpretations of breath and heart sounds. c. The examination technique, d. Interpretation of examination • Palpation – a. Evaluation of mediastinum and tracheal deviation, b. Evaluation of chest wall expansion. c. Evaluation of fremitus, d. Evaluation of accessory respiratory muscles. e. Evaluation of chest pain, f. Evaluation of diaphragmatic movement, g. Evaluation of edema • Mediate Percussion- resonance and diaphragmatic excursion.
5) LABORATORY EVALUATION- •Principles, analysis and Guideline for interpretation of ABG, PFT, treadmill text, exercise tolerance test. ECG, ECHO, angiography, Doppler study chest radiography, bacteriological- and cytological tests, MUGA test. •Evaluation of a Patient with Coronary Artery Disease – 1. Review of medical records and extraction of pertinent data, 2. Interview and examination of patient, 3. Preliminary assessment of clinical status, 4. Determination of candidacy for further evaluation, 5.Evaluation of functional activities, 6. Evaluation of activities of daily living, 7. Monitored ambulation. 8. Low level exercise test, 9. Definitive assessment regarding candidacy for exercise therapy, 10. Individually monitored aerobic exercise and strengthening program, 11 Maximal exercise test, 12. Additional invasive and noninvasive testing, 13. Serum lipid profile, 14. Evaluation of monitored job simulation, 15. Cardiac enzymes Low Level Exercise Testing- • Purpose, Contra- indications, Termination points.
6) CARDIOPULMONARY EVALUATION IN INTENSIVE CARE UNIT.
7) CARDIOPULMONARY EVALUATION OF VENTILATORY DEPENDENT PATIENT - Assessment of ventilators, Respiratory rate, Respiratory pattern, Pulse rate, Temperature, Blood
PAGE- 29
Pressure, Fluid and electrolyte balance; Chest tube drainage and fluid collection system. Arterial blood gas analysis. ECG monitoring, Intra-arterial lines, Pulmonary artery balloon flotation catheter, Intravenous lines, Central venous pressure, Electroencephalogram.
Physiotherapy Evaluation of Cardiac conditions- •Pre Operative evaluation of Cardiac Surgeries •Post Operative evaluation of Cardiac Surgeries.
Apart from the above, the student is expected to know the latest developments in physiotherapy evaluation of cardio respiratory conditions.
Role of Physiotherapist in Interventional cardiology.
Palliative cardiology-• Primary •Secondary
3. ADVANCED PHYSIOTHERAPEUTIC INTERVENTIONS
A) COURSE CONTENT
1) Definitions, Causes, Clinical Features; path physiology, general investigation. Medical Medical and surgical management of the below mentioned conditions.
2) Pulmonary diseases in premature babies, neonatal distress, birth asphyxia. bronchopulmonary dysphasia, Nickity Wilson syndrome, Me conium aspiration.
3) COPD, Asthma, cystic fibrosis, Immunological deficits, bronchiectasis, lung abscess, pneumonia, interstitial lung disease, lung cancer, pulmonary tuberculosis, and Occupational lung disorders, fracture ribs, pnemothorax. haemothorax, emphysema.
4) Congenital heart diseases- patent ductus arteriosus, co-arctation of aorta, atrial septal Defect, ventricular septal defect, transposition of great vessels, tetra logy of fallot.
5) Coronary artery diseases and its manifestations.
6) Valvular diseases.
7) Rheumatic heart disease.
8) Diseases of myocardium.
9) Peripheral vascular disease.
10) Burns, cardiopulmonary complications in burns.
11) Indications and various types abdominal surgeries.
B. REFERENCE
1) Goodman : Pathology implication for the physical therapist .
2) Mandy : cardiovascular respiratory physiotherapy
4) Jennifer : physiotherapy for respiratory and cardiac problems , adult and pediatrics
5) Mathews : cardiopulmonary anatomy and physiology .
6) John : pulmonary rehab. The obstructive and paralytic condition
7) Jennifer & Barbara : Physiotherapy for respiratory and cardiac problems
8) Donna: Cardiopulmonary physical therapy
PAGE- 30
II YEAR MPT IN PAEDIATRICS
1. CLINICAL ASPECTS AND RECENT ADVANCES
A) COURSE CONTENT
1) INTRODUCTION- • Genetics and genetic counseling • General & systemic embryology • Ossification of bones • Motor Development •Language Development • Gait development and analysis •Immunization schedule.
2) ANATOMY & PHYSIOLOGY- Anatomy of brain and Spinal cord, including Blood supply or brain and Spinal Cord: • Cranial nerve - courses and connections • Cerebellum connections &
functions • Spinal nerves & spinal cord • Pyramidal & Extra pyramidal systems, Myelination of pyramidal tract • Neuro physiological basis of tone, posture, Movement, Co-ordinations, balance & its abnormal Neuro mechanics • Primitive, brasinstem, cortical reflexes • Anatomy & physiology of
cardio vascular system.
3) PATHO MECHANICS - • Pathomechanics of common deformities in Neurological and musculo skeletal disorders • Pathomechanics of gait deviations.
4) PAEDIATRIC NUTRITION -• Elements of nutrition, Daily allowances / requirement of nutrients • Common Nutritional disorders and their relevance to physiotherapy.
5) CLINICAL CONDITIONS
6) DEVELOPMENTAL DISORDERS - • Factors related to developmental disorders, Early/late detection of disorders. Various disorders related to development. Heredity and genetic disorders.
7) HIGH RISK INFANTS – Asphyxia, respiratory distress syndrome, Broncho pulmonary dysplasia Meconium aspiration, intraventricular hemorrhage. hyperbilirubinemia, hypoxic ischemic encephalopathy, SGA infants, premature infants.
8) NEONATAL CARE- Handling, positioning, feeding, parent education.
9) NEUROLOGICAL CONDITIONS WITH EMPHASIS ON:- • Spina bifida •Cerebral palsy • Poliomyelitis • Encephalitis and Meningitis • Traumatic Brain injury & sequelae • Brain tumors •Movement Disorders •Neuro muscular disorders • Hydrocephalus •Peripheral Neuro muscular disorders • Brachial palsies •Spinal cord injuries.
10) MUSCULO SKELETAL IMPAIRMENT WITH EMPHASIS ON: - • Juvenile rheumatoid arthritis • Congenital dislocation of hip (CDH) • CTEV • Perthes disease • Blount’s disease •Rickets • Osteomalacia • Haemophilic • Developmental muscular Torticollis • Spinal Conditions

PAGE- 31
with emphasis on scoliosis • Osteogenesis imperfecta •Arthrogryphosis Multiplex congenital • Fractures in childhood • Infective arthritis • Pyogenic arthritis.
11) CARDIOPULIMONARY CONDITIONS- •Growth & Development of lungs • Paediatric asthma, bronchitis, atelectasis • Respiratory muscle weakness •Cystic fibrosis •Congenital heart diseases – cyanotic and acynotic, Acynotic – ASD, VSD, PDA, Coarctation of aorta, pulmonary stenosis, Aortic stenosis • Cyanotic – Tetralogy of fallot, transposition of great arteries, tricuspid • Artesia, pulmonary Artesia, truncus arteriosus • Thoracic surgeries • Deformities of chest wall • Pulmonary tuberculosis, Pneumonia.
12) PAEDIATRIC ONCOLOGY
13) PAEDIATRIC BUFNS AND MANAGEMENT- • Classification and pathophysiology • Burn unit and team approach • Musculo skeletal problems.
14) MENTAL RETARDATION
15) CHILD WITH SPECIAL NEEDS - • Mongolism, down syndromes’, Seizures, Attention Disorders, HIV
16) RECENT ADVANCES - • NEONATAL INTENSIVE CARE • Premature nursery • Early intervention • Special schooling • Assistive technology.
2. ADVANCED PHYSICAL AND FUNCTIONAL DIAGNOSIS
A) COURSE CONTENT
1) ASSESSEMT & EVALUATION - • Assessment of premature infants • Evaluation of neonatal infants • Sharing information from parents/care giver • Securing cooperation • Special communication skills • Assessment of various neurological conditions in premature and full term
babies • Assessment of various musculo skeletal disorders • Assessment of cardio respiratory diseases • pre operative and post operative assessment in surgical conditions.
2) VARIOUS FUNCTIONAL SCALES USED FOR PAEDIATRIC ASSESSMENT IN VARIOUS NEURO MUSCULAR DISORDERS.
3) DISABILITY EVALUATION- •Apsgar score • Pediatric evaluation of disability inventory, (PEDI) • Morgan neonatal neuro behavioral evaluation • Neonatal behavioral assessment scale • Bruninks – Oseretsky test of motor proficiency (BOT).
3. ADVANCED PHYSOTHERAPEUTIC INTERVENTION
A) COURSE CONTENT
1) PRINCIPLES OF PAEDIATRIC PHYSIOTHERAPY : - • Specific goals of paediatric physiotherapy • Managing high risk & premature infant • SGA Infants • Correct use of various

PAGE- 32
adaptive aids • Communication skills • Family centered intervention • Setting of special care nurseries/ educational environment • Management of associated problems like visual, hearing,
speech impairment • Knowledge about motor control in general • knowledge of moter development in general • Disability Evaluation In Neonates And Infants • Physiotherapeutic Management in Neurological conditions including its surgical mangement • Physiotherapeutic
Management in musculo skeletal disorders including its surgical management • Physiotherapeutic mamagement in cardio pulmonary diseases including its surgical management • Physiotherapy
managemnt ofor paediatric burns and mental retardation.
2) ADAPTIVE DEVICES - • Mobility aids • Orthotics/prosthesis • Various splints used in
Paediatric • Advanced mobility equipments •Various positional devices • Electronic Aids to daily living.
3) MODALITIES AND TECHNIQUES- • Evaluation of child and choosing the modality •
Awareness of various equipment in the paediatric setting • Various approaches with emphasis on roods, Bobath, motor relearining, PNF, Vojta and Neuro Developmental Therapy (NDT)
4) DEVELOPMENTAL INTERVENTIONS- • Positioning • Sensory motor stimulation • Oral motor therapy
5) Physiotherapeutic interventions in Neonatal intensive care unit (NICU) • Techniques – postural drainage, percussion, vibration
6) PLAY THERAPY - • Need for recreation in educational environment • Importance of play
therapy.
7) CBR IN PAEDIATRICS - • Importance of community rehabilitation in paediatircs Awareness of
society about impairment and disability Monitoring and evaluation of disability • Monitoring and evaluation of disability • Counseling
8) EMPHASIS ON BIOFEEDBACK
9) SETTING OF PAEDIATRIC HOME
10) Importance of Occupational Therapy in Pediatric Rehabilitation
B. REFERENCE
1) Barbara : Muscles , nerves and movement kinesiology in daily living.
2) Barbara : Disease of the nervous system.
3) Richard : Neurological rehabilitation.
4) Susan , neurological physiotherapy
5) Omer : management of peripheral nerve problems.
6) Darcy : Neurological rehabilitation.

PAGE- 33
7) Charles : the Neuroscience of human movement
8) Janet : a motor relearning programme for stroke .
9) Snell Richards clinical Neuro Anatomy for medical students .
10) Pediatric physical therapy- Shepard
11) John pattern : neurological differential diagnosis
12) Fredericks : Pathophysiology of motor system .
II YEAR MPT IN SPORTS
1. CLINICAL ASPECTS AND RECENT ADVANCES IN
SPORTS MEDICINE
A) COURSE CONTENT
1) ANATOMY, PHYSIOLOGY & PATHOMECHANICS- • Psychological f actors of sports injuries • Physiological factors of sports injuries – Type of injuries, Reaction to injury, Response of joint structures to injury, Effect of immobilization, effects of remobilization, Inflammatory and healing process, micro trauma, stress reactions • Rules ®ulations of sports, sport specific injuries • Patho mechanics of sport injuries • Physical demand in different sports • Flexibility exercises.
2) NEUROPHYSIOLOGY - • Physiological effects of stretching & mobilizations prior to the participation in sports • Types of exercises and their physiological effects related to sports. Biomechanics of sports and its relationship to joint injuries • Uses & application of biomechanics different sport events (like throwing mechanics, running mechanics, swimming mechanics) • Aquatic: Physical properties of water, Physiologic effects of water immersion and its therapeutic value • Embryological development of musculoskeletal system • Osteology: Structure of bone, ossification of bones, Skull bones, Facial bones, Bones of Upper Extremity, Lower Extremity, Pelvis, Vertebral column, ribs • Myology: Structure- of muscle, Types of muscle, muscle fibers, Origin, insertion, action, nerve supply of Muscles of Face, Upper Extremity, Lower Extremity, and Trunk • Arthrology: Structure of joint, types of joints, detailed structure and Formation of all the joints. Neurobiology of joint • Neurology: Peripheral Nerves: Dermatomes and myotomes • Physiology: Joint Physiology [Movements]. Muscle physiology. Patho mechanics of Fractures, deformed joints.
B) CLINICAL CONDITIONS
Student is expected to learn common causes, mechanism, pathophysiology, signs, symptoms, medical and surgical treatments of following sports related injuries and also should know the recent advances in the surgical, medical management of sports related injuries.
PAGE- 34
1) Epiphyseal injuries- Classification, complications and prognosis of epiphyseal injuries, Osgood Schlatter disease, traction epiphysitis, tendinitis at the insertion of patellar tendon, complete avulsion of the epiphysis of the tibial tubercle, shoulder, Contributing risk factors- intrinsic factors, and extrinsic factors.
2) Shoulder Girdle injuries – Injuries to the sternoelavicular joint – sprains, dislocations, Scapulothoracic joint lesions, acromioclavicular joint sprains, anterior dislocation of glenohumeral joint, recurrent anterior dislocation of the shoulder, posterior dislocation of shoulder, thoracic outlet syndrome. Painful are, Rotator cuff injuries, Impingement syndromes, Glenoid Labrum lesions.
3) Elbow joint Injuries- Olecranon bursitis, Vagues extension overload, elbow, Ulnar nerve lesions, Ulnar & Radial collateral ligament sprains, Contusions and strains, Dislocations, Osteochondritis dissicans, Little Leaguers elbow, problems resulting from throwing –medial lesions, lateral lesions posterior lesions.
4) Elbow injuries from Tennis- Epicondylitis- Incidence, pathology, and mechanism of injury.
5) Wrist and hand Injuries- Colle’s fracture, scaphoid fracture, Gamekeeper’s Thumb, DIP joint fracture & dislocation, Jersey finger, Boutonniere deformity, pseudo boutonniere deformity, fractures of the metacarpales, Bennett’s fracture, mallet finger, Dequervain’s tenosynovitis of the thumb, Bowler’s, thumb, handler palsy, Hamate fracture, Ganglion cysts, Trigger finger: Carpal tunnel syndrome.
6) Thigh Injuries- Contusion to the quadriceps, strain of the quadriceps musculature, acute strain of the hamstring group, complete rupture of the patellar tendon.
7) Knee Injuries- Knee ligament injuries first- degree sprain, second-degree sprain, Third degree sprain, Anterior and posterior cruclate tears, anteriolateral instability meniscal-lesion, Articular cartilage lesions, Patello femoral dysfunction.
8) Injuries of the patella – Patella fracture- acute-dislocation, recurrent disloc3tion, subluxation and spontaneous reduction of a dislocated patella, Osteochondritis dissicans, Jumper’s knee.
9) Injuries to lower leg, ankle and foot- Tibiofibular synostosis, Rupture of the gastrocnemius, tennis leg, total rupture of the Achilles tendon, partial rupture of the Achilles tendon, Tendinopathies-Achilles tendonitis, Anterior tibialis tendonitis, Peroneal tendinitis. Poster tibialis tendonitis, Flexor hallucis longus tendinits, Flexor digitorum longus tendinitis. Compartmental compression syndromes, Heel bruiese, Os trigonum injury, Calcaneal apophysitis, Tarsometatarsal injuries. Tarsal tunnel syndrome, Cuboids syndrome, Metatarsal stress fracture, Interdigital neuroma, Stair Climbers transient parasthesia, Turf toe, sesmoitidis.
10) Injuries to the Ankle- Syndesmotic ankle sprain, Inversion sprains. eversion sprains, dorsiflexion sprains, tarsal tunnel syndrome, stress fracture of the metatarsal, vorton’s neuromas, corns and calluses, blisters, ingrown toenails, peroneal tendon subluxation.

PAGE- 35
11) Injuries to the low back – Postural syndrome, Dysfunction syndrome, Derangement syndrome, spondylolisthesis.
12) Injuries to the Running Athlete- Causes of overuse injuries- Common running induced injuries to the lower back- common running induced injuries to the hip-lliotibial tract pain. Trochanteric bursitis, stress fracture of femoral neck. Slipped capital femoral epiphysis, vague hip pain.
13) Common Running related injuries to the knee – Medial patellar pains. pes anserine bursitis, patellar tendonitis, retro patellar pain, lateral patellar pain, lateral knee pain, biceps femoral tendinitis.
14) Common running related injuries to the lower leg- Tibial stress relation, stress fracture, medial tibial stress syndrome, compartment syndrome,- Anterior posterior lateral, fibular stress reaction and stress fracture, retrocalcaneal bursitis medial arch pain, plantar fascitis.
15) Swimming Injuries- “Swimmers Shoulder” anterior subluxation of the Glenohumeral Joint, breast stroke’s injury.
2. ADVANCED PHYSICAL AND FUNCTIONAL DIAGNOSIS
A) COURSE CONTENT
1) Emergency Sports Assessment Pre-event Preparation
2) Primary Assessment- Level of Consciousness, Establishing the airway, Assessment for Bleeding, Fluid loss and Shock, Pupil Check, Assessment for spinal cord injury, Assessment for Head Injury, Assessment for Movement, Positioning the patient, Injury severity.
3) Secondary Assessment- pre participation Evaluation, Objectives of the Evaluation, Setting up the Examination.
4) Pre participation History Examination- Eye examination, Musculoskeletal Examination and Convulsive Disorders, Pulmonary Examination, urogenital Examination, Gastrointestinal. Dermatological Examination, Examination for Heat Disorders, General Medical Problems; Dental Examination, Neurological examination Cardiovascular Examination, Application of isokinetics in testing.
Student should be able to use & understand result of electro diagnostic tools & being techniques used in the sport evaluation.
3. ADVANCED PHYSIOTHERAPEUTIC INTERVENTIONS
A) COURSE CONTENT
PAGE- 36
Student should be able to plan appropriate treatment regime based on the knowledge of various subjects learned during the two year Programme for the below mentioned condition, Additionally emphasis should be on special techniques.
1) Prevention of Athletic injuries- Athletic coordinating program-skeletal muscle-Type 1 and Type 2 fibers, General conditioning principle-strength, power, muscular endurance, flexibility, anaerobic metabolism.
2) Warm-up period- Warm-up schedule, stretching partner stretching partner stretching using the proprioceptive neuromuscular facilitation technique.
3) Protective and supportive equipment- Protective equipments: Supportive devices, motion limiting devices.
4) Treatment of athletic injuries.
5) Taping and wrapping techniques.
6) Emergency care and Athletic first aid- cardiopulmonary emergencies, ABC of resuscitation, Haimlick maneuver Shock Injurie: - internal injuries, Head and neck injuries, fractures, dislocations.
7) Injury first Aid- ICE or cold application, compression, elevation, gait instruction, stretcher and wheelchair uses.
8) Physiotherapeutic interventions for relief of pain- Therapeutic modalities and procedures- General principles of therapeutic modalities Hydrotherapy, short wave diathermy, Microwave diathermy, Ultrasound. lontophoresis, Phonophoresis, TENS, Cryotherapy, cold spray, contrast bath, paraffin wax bath, ultraviolet, massage Indications, contraindications, therapeutic and physiologic effects, treatment techniques.
9) Fitness training related to specific sports- Manipulative Therapy- Principles, concept, indications, and contraindications, Applications.
10) Injuries Rehabilitation- Goals of rehabilitation, types of exercises-isometric exercise, isotonic exercise, special forms of exercise-manual resistance. proprioceptive neuromuscular facilitation, surgical tubing, circuit training, sport-specific skills.
11) Application of isokinetics in athletic rehabihtation.
12) Nutrition and Athlete- Well balanced diet, pre event nutrition, increasing weight, decreasing weigh in wrestlers, carbohydrate loading diet, sugar before and after competition.
13) Prevention and physiotherapy treatment of following:
a) Epiphyseal injuries, Osgood Schlatter disease, traction epiphysitis, tendinitis at the insertion of patellar tendon, complete avulsion of the epiphysis of the tibial tubercle shoulder, contributing risk factors- intrinsic factors, extrinsic factors.
b) Shoulder Girdle Injuries: Injuries to the sternoclavicular joint- sprains, dislocations, Scapulothoracic joint lesions, acromioclavicular joint sprains, anterior dislocation of glenohumeral joint, recurrent anterior dislocation of the shoulder, posterior dislocation of shoulder, thoracic outlet syndrome. Painful are, Rotator cuff injuries, Impingement syndromes, Glenoid Labrum lesions.
c) Elbow joint Injuries: Olecranon bursitis, Valgus extension overload, elbow, Ulnar nerve lesions, Ulnar & Radial collateral ligament sprians contusions and strains, Dislocations, Osteochondritis dissicans, Little Leaguers elbow: problems resulting from throwing- medial lesions. lateral lesions posterior lesions.
PAGE- 37
d) Elbow injuries form Tennis: Epicondylitis- Incidence, pathology, mechanism of injury.
e) Wrist and hand Injuries: Colle’s fracture, scaphoid fracture, Gamekeeper’s Thumb, DIP joint fracture & dislocation, Jersey finger, Boutonniere deformity, pseudo boutonniere deformity, fractures of the thumb, Bowler’s, thumb, handler palsy, Hamate fracture, Ganglion cysts. Trigger finger: carpal tunnel syndrome.
f) Thigh Injuries Contusion to the quadriceps, strain of the quadriceps musculature, acute strain of the hamstring group, complete rupture of the patellar tendon.
g) Knee Injuries, Knee ligament injuries first- degree sprain, second-degree sprain, Third degree sprain, Anterior and posterior cruciate tears, anteriolateral instability meniscal lesion, Articular cartilage lesions. Patello femoral dysfunction.
h) Injuries of the patella: Patella fracture- acute dislocation, recurrent dislocation, subluxation and spontaneous reduction of a dislocated patella, Osteochondritis dissicans, and jumper’s knee.
i) Injuries to the lower leg, ankle and foot: Tibiofibular synostosis, Rupture of the gastrocnemius, tennis leg, total rupture of the Achilles tendon, partial rupture of the Achilles tendon, Tendinopathies-Achilles tendonitis, Anterior tibialis tendinitis, Peroneal tendinitis, Poster tibialis tendonitis, Flexor hallucis longus tendinitis, Flexor digitorum longus tendinitis. Compartmental compression syndromes, Heel bruises, Os trigonum injury, Calcaneal apophysitis, Tarsometatarsal injuries, Tarsal tunnel syndrome, Cuboids syndrome, Metatarsal stress fracture, Interdigital neuroma, Stair climbers transient parasthesia, Turf toe, sesmoitidis.
j) Injuries to the Ankle: Syndesmotic ankle sprain Inversion sprains, eversion sprains, dorsiflexion sprains, tarsal tunnel syndrome, stress fracture of the metatarsal, morton’s neuromas, corns and calluses, blisters, ingrown toenails, peroneal subluxation.
k) Injuries to the low back: Postural syndrome, Dysfunction syndrome. Derangement syndrome, Spondylolisthesis.
l) Injuries to the Running Athlete: Causes of overuse injuries – Common running induced injuries to the lower back- common running induced injuries to the hip- Hiotibial tract pain. Trochanteric bursitis, stress fracture of femoral neck, slipped capital femoral epiphysis, vague hip pain.
m) Common Running related injuries to the knee: Medial patellar pains, pesanserine bursitis, patellar tendonitis, retro patellar pain, lateral patellar pain lateral knee pain, biceps femoral tendinitis.
n) Common running related injuries to the lower leg: Tibial stress relation. Stress fracture, medial tibial stress syndrome, compartment syndrome. anterior posterior lateral, fibular stress reaction and stress fracture, retrocalcaneal bursitis medial arch pain, plantar fascitis.
o) Swimming Injuries: “Swimmers Shoulder” anterior subluxation of the Glenohumeral Joint, breastsrocker’s injury.
p) Sports for youth with disabilities: Role of physiotherapist in preparing the impaired for sport events (like Para Olympics).

PAGE- 38
Apart from the above student should know the pre & postoperative rehabilitation protocols used in sports physiotherapy.
B. REFERENCE
1) Thomas : Imaging of sports injuries.
2) Sandra : Assessment – athletic injuries
3) David : Sports injury assessment & rehabilitation
4) Christopher : Sports injuries diagnosis & management
5) Katch : Exercise physiology energy nutrition and human performance.
6) Frank : Exercise physiology for health care professionals
7) James : the biomechanics of sports techniques .
8) Sprots injuries – Christopher .
9) Oxford text book of sports physiotherapy
c. REFERENCE (Journals )
1) American physical therapy association
2) Archive of physical medicine and rehabilitation
3) Australin journal of physiotherapy
4) Canadian journal of physiotherapy
5) Physiotherapy U.K.
6) Journal of orthopedics and sports physiotherapy
7) Journal of manual and manipulative therapy
8) Janet : a motor relearning programme for stroke .
9) Snell Richards clinical Neuro anatomy for medical students .
10) Pediatric physical therapy- Shepard
11) John pattern : neurological differential diagnosis
12) Fredericks : Pathophysiology of motor system .

PAGE- 39
TABLE – I
MODEL CHECK LIST FOR EVALUATION OF JOURANAL REVIEW PRESENTATIONS
Name of Student : ………………………………
S.No. Items for observing during presentation * Grade
1 Article chosen was
2 Extent of understanding of scope & objectives of the paper by the candidate
3 Whether cross references have been consulted
4 Whether other relevant publications consulted
5 Ability to respond to questions on the paper / subject
6 Audio – visual aids used
7 Ability to defend to paper
8 Clarity of presentation
9 Any other observation
Total score/ overall grade
* Corollary for grade
0 _ Poor
1 _ Below average
2 _ Average
3 _ Good
4 _ Very Good
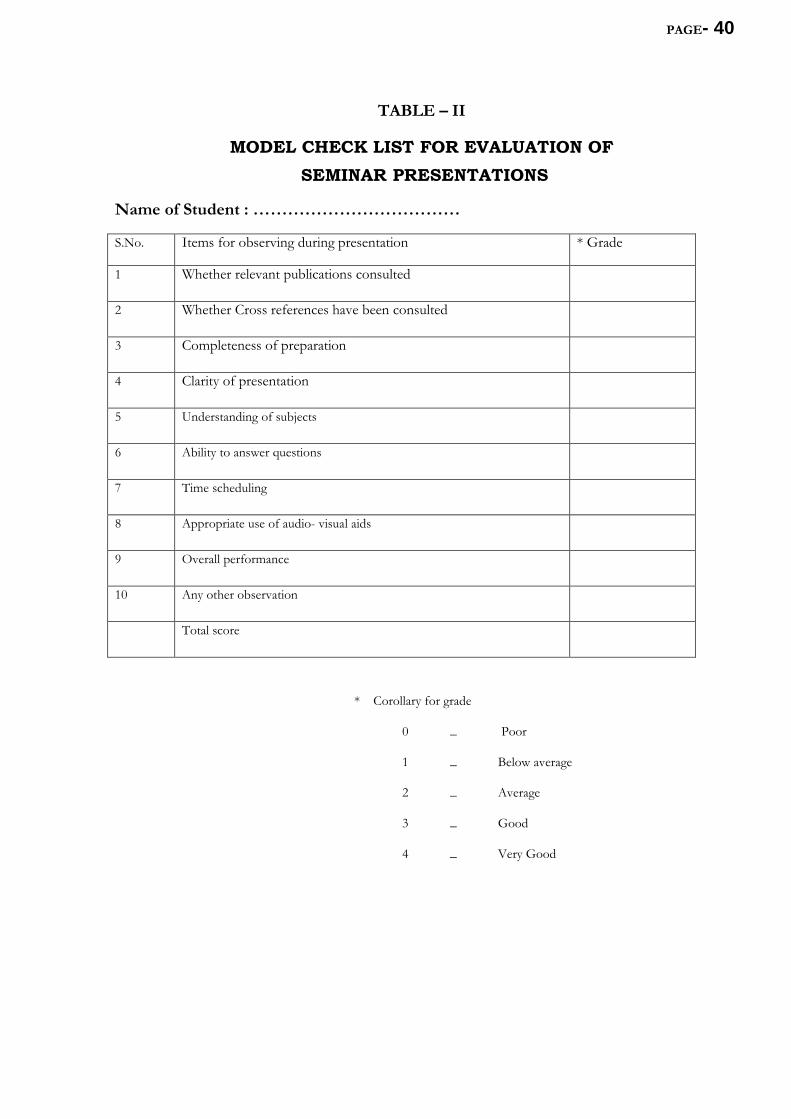
PAGE- 40
TABLE – II
MODEL CHECK LIST FOR EVALUATION OF SEMINAR PRESENTATIONS
Name of Student : ………………………………
S.No. Items for observing during presentation * Grade
1 Whether relevant publications consulted
2 Whether Cross references have been consulted
3 Completeness of preparation
4 Clarity of presentation
5 Understanding of subjects
6 Ability to answer questions
7 Time scheduling
8 Appropriate use of audio- visual aids
9 Overall performance
10 Any other observation
Total score
* Corollary for grade
0 _ Poor
1 _ Below average
2 _ Average
3 _ Good
4 _ Very Good
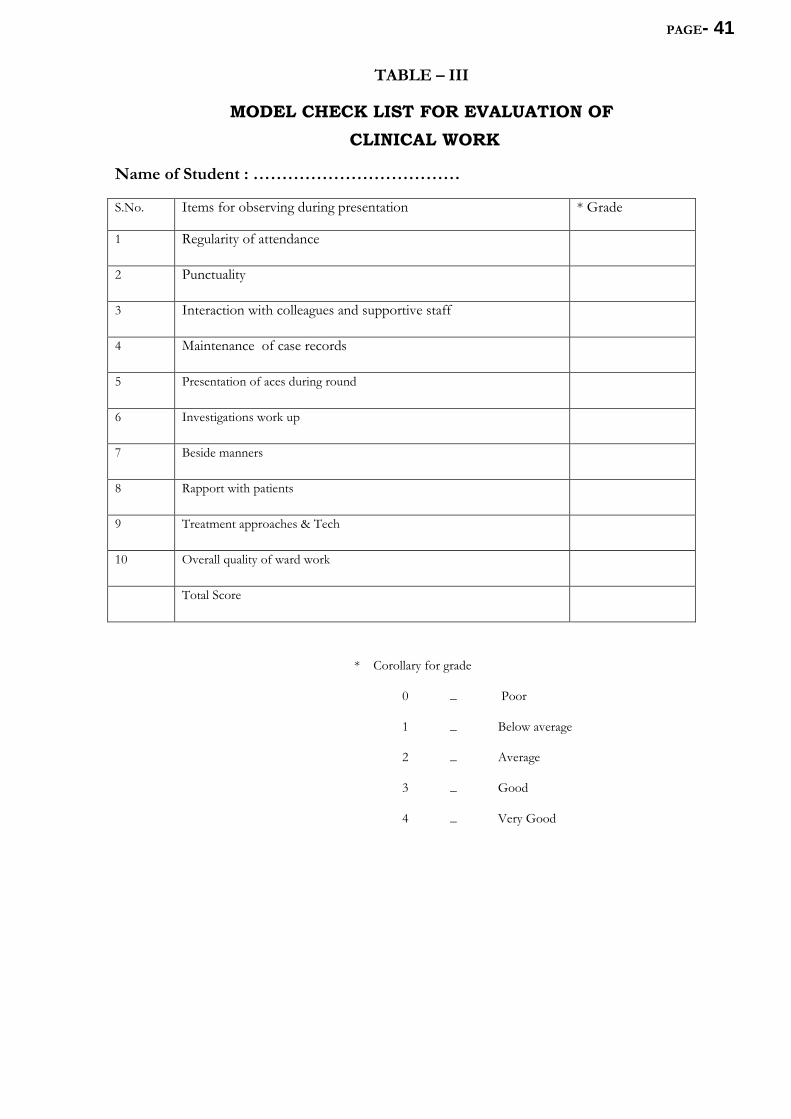
PAGE- 41
TABLE – III
MODEL CHECK LIST FOR EVALUATION OF CLINICAL WORK
Name of Student : ………………………………
S.No. Items for observing during presentation * Grade
1 Regularity of attendance
2 Punctuality
3 Interaction with colleagues and supportive staff
4 Maintenance of case records
5 Presentation of aces during round
6 Investigations work up
7 Beside manners
8 Rapport with patients
9 Treatment approaches & Tech
10 Overall quality of ward work
Total Score
* Corollary for grade
0 _ Poor
1 _ Below average
2 _ Average
3 _ Good
4 _ Very Good
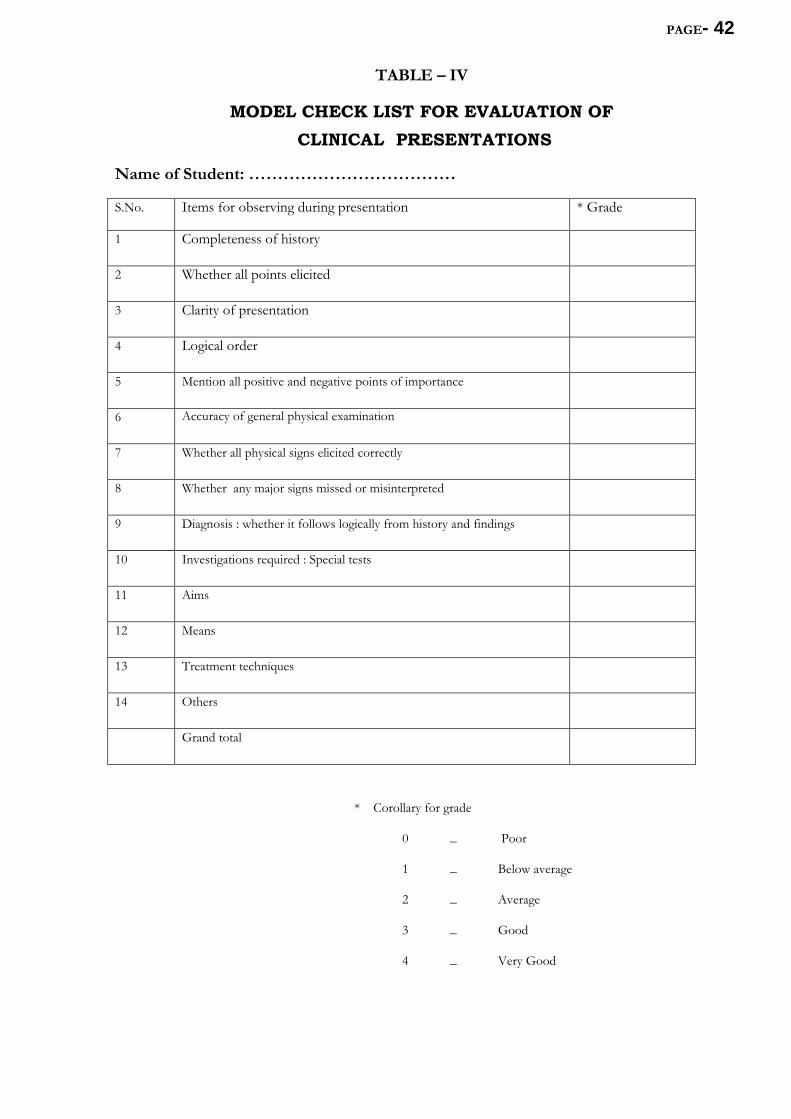
PAGE- 42
TABLE – IV
MODEL CHECK LIST FOR EVALUATION OF CLINICAL PRESENTATIONS
Name of Student: ………………………………
S.No. Items for observing during presentation * Grade
1 Completeness of history
2 Whether all points elicited
3 Clarity of presentation
4 Logical order
5 Mention all positive and negative points of importance
6 Accuracy of general physical examination
7 Whether all physical signs elicited correctly
8 Whether any major signs missed or misinterpreted
9 Diagnosis : whether it follows logically from history and findings
10 Investigations required : Special tests
11 Aims
12 Means
13 Treatment techniques
14 Others
Grand total
* Corollary for grade
0 _ Poor
1 _ Below average
2 _ Average
3 _ Good
4 _ Very Good
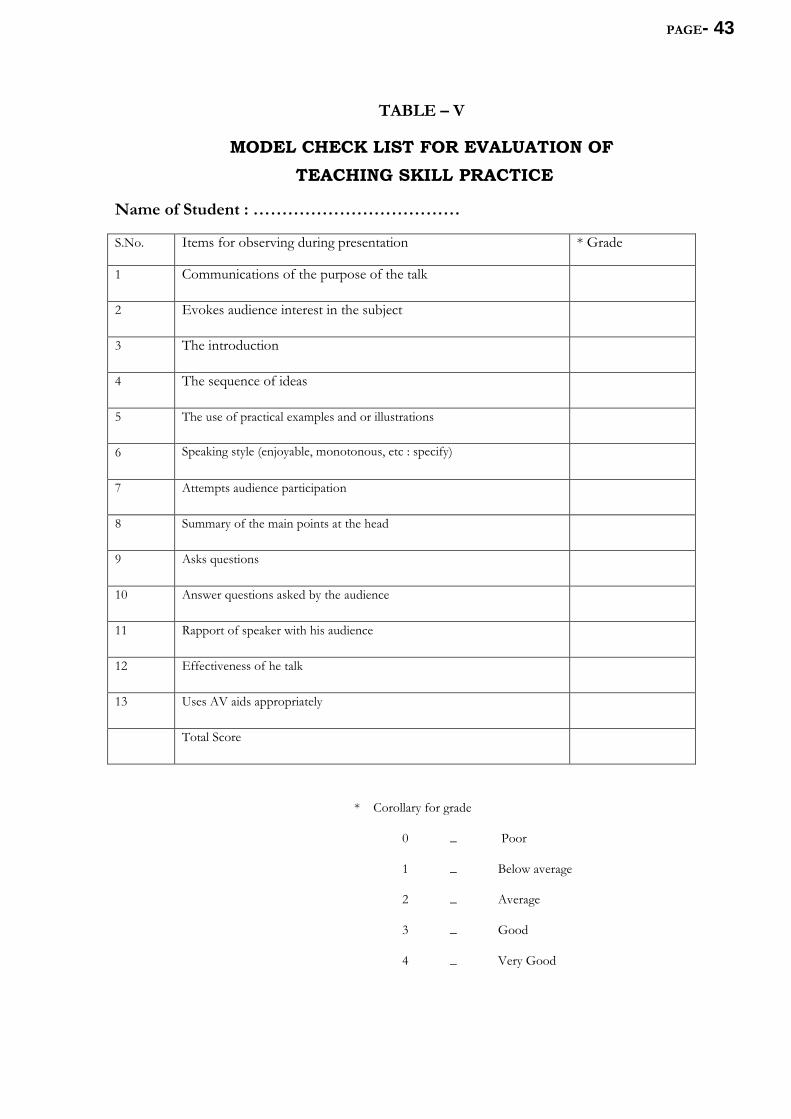
PAGE- 43
TABLE – V
MODEL CHECK LIST FOR EVALUATION OF TEACHING SKILL PRACTICE
Name of Student : ………………………………
S.No. Items for observing during presentation * Grade
1 Communications of the purpose of the talk
2 Evokes audience interest in the subject
3 The introduction
4 The sequence of ideas
5 The use of practical examples and or illustrations
6 Speaking style (enjoyable, monotonous, etc : specify)
7 Attempts audience participation
8 Summary of the main points at the head
9 Asks questions
10 Answer questions asked by the audience
11 Rapport of speaker with his audience
12 Effectiveness of he talk
13 Uses AV aids appropriately
Total Score
* Corollary for grade
0 _ Poor
1 _ Below average
2 _ Average
3 _ Good
4 _ Very Good
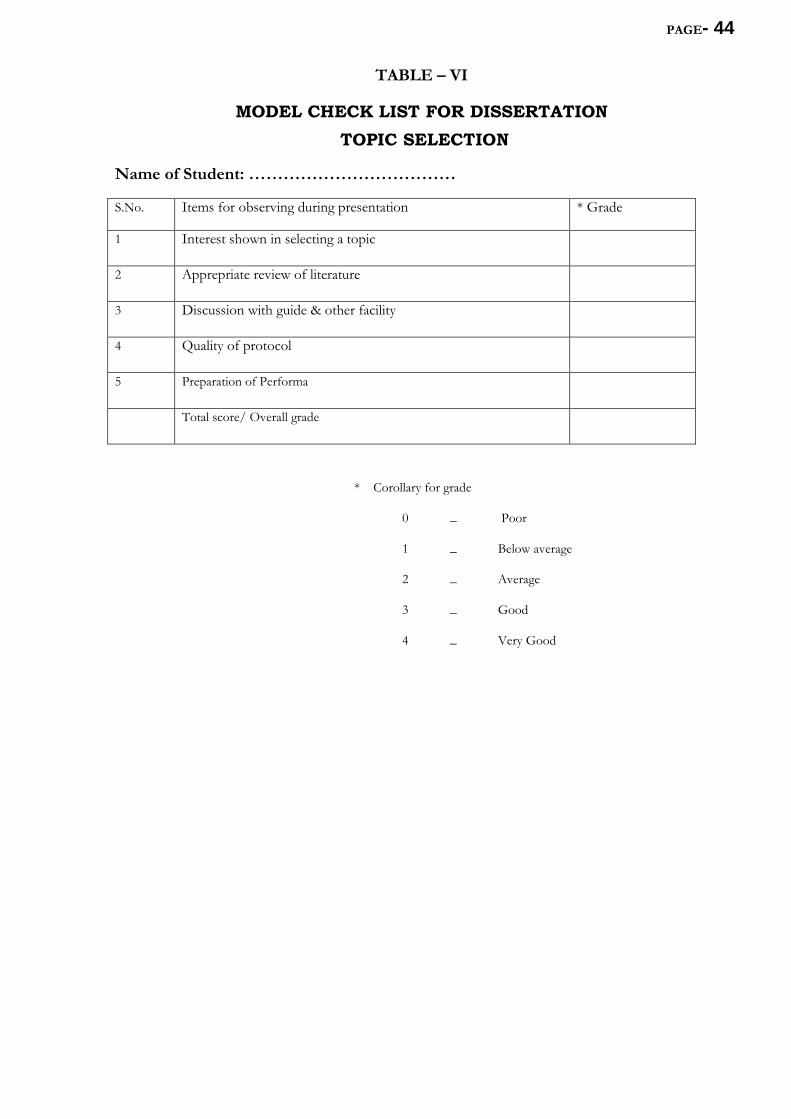
PAGE- 44
TABLE – VI
MODEL CHECK LIST FOR DISSERTATION TOPIC SELECTION
Name of Student: ………………………………
S.No. Items for observing during presentation * Grade
1 Interest shown in selecting a topic
2 Apprepriate review of literature
3 Discussion with guide & other facility
4 Quality of protocol
5 Preparation of Performa
Total score/ Overall grade
* Corollary for grade
0 _ Poor
1 _ Below average
2 _ Average
3 _ Good
4 _ Very Good
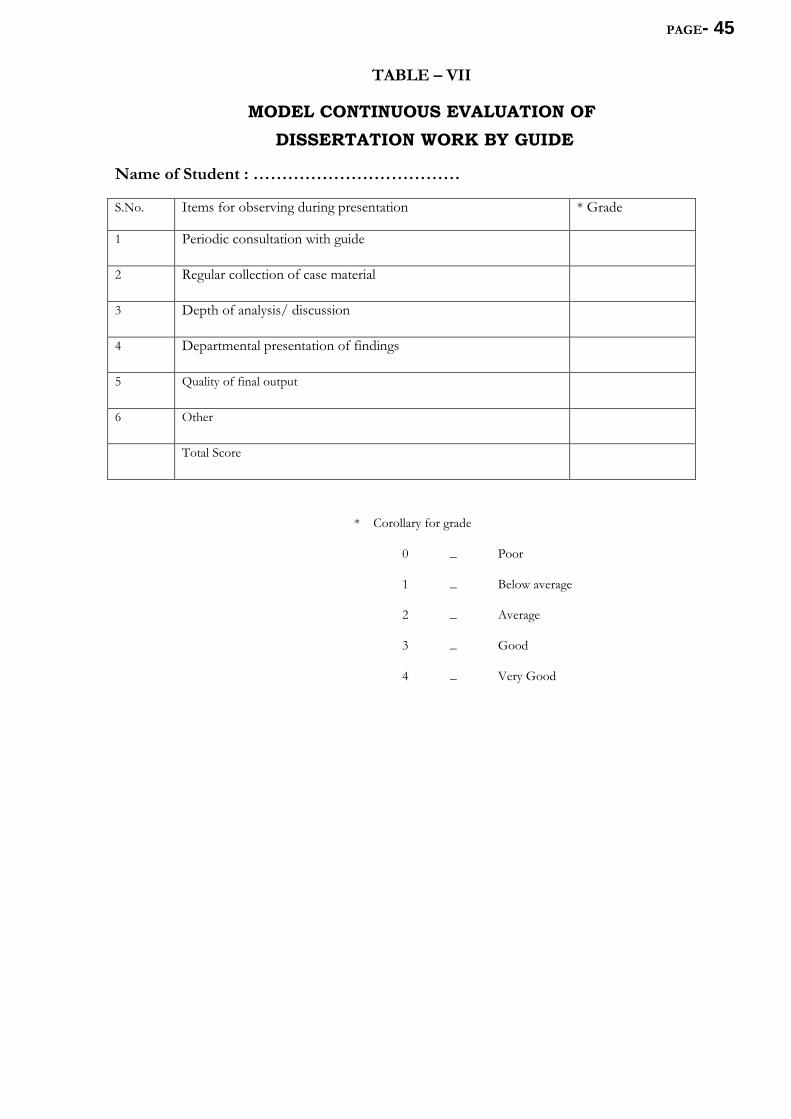
PAGE- 45
TABLE – VII
MODEL CONTINUOUS EVALUATION OF DISSERTATION WORK BY GUIDE
Name of Student : ………………………………
S.No. Items for observing during presentation * Grade
1 Periodic consultation with guide
2 Regular collection of case material
3 Depth of analysis/ discussion
4 Departmental presentation of findings
5 Quality of final output
6 Other
Total Score
* Corollary for grade
0 _ Poor
1 _ Below average
2 _ Average
3 _ Good
4 _ Very Good