rehabilitation of patellofemoral joint disorders: a critical review
TRANSCRIPT

Rehabilitation of Patellofemoral Joint Disorders: A Critical Review Christopher M. Powers, A D , PT'
Christopher M. Powers
atellofemoral pain is the most prevalent disorder involving the knee ( 1 5, 46). Over a $year period, Devereaux and Lachmann
( 1 1') demonstrated that 25% of all knees evaluated in a sports injun clinic were diagnosed with patel- lofemoral pain, while McConnell (50) reports that patellofemoral pain affects one in four of the general population. In addition, a study of 100 painful knees conducted by Outerbridge and Dunlop (56) re- ported patellofemoral joint pathology in 40 of 50 women and in 15 of 50 men. While patellofemoral-related problems occur with an incidence of two to one in females w. males, men outnumber women when athletes are studied (41 ).
The symptoms of patellofemoral pain are multiple (16,41,68). Pain is generally characterized as being dif- fuse and arising from the anterior aspect of the knee (68). Pain along the medial aspect of the patella is the most common complaint; however, retropatellar pain and pain along the lateral border is often reported ( 1 7). Generally, onset is insidious and pro- gression is slow. Patellofemoral pain
Patellofemoral pain is one of the most common knee disorders seen in orthopaedic practice. Despite its high incidence, treatment of this disorder remains controversial. Traditionallv, nonoperative management of patellofemoral pain has focused on restoring normal patellar tracking by improving dynamic stability. Of particular interest to clinicians has been the vastus medialis oblique, which has been implicated as being the primary medial stabilizer of the patella. Although emphasis on the vastus medialis oblique continues to be the mainstay of conservative care of patellofemoral pain, there exists considerable disagreement between research outcomes and clinical practice. This article criticallv reviews the current literature concerning the treatment of patellofemoral pain with respect to the vastus medialis oblique, taping, and bracing, as well as various forms of therapeutic exercise, and relates these findings to the prevailing views regarding the management of this disorder.
Key Words: patellofemoral pain, rehabilitation, vastus medialis oblique ' Assistant Professor and Director, Musculoskeletal Biomechanics Research Laboratory, Department of Biokinesiology and Physical Therapv, University of Southern California, 1540 E. Alcazar St., CHP-155. Los Angeles, CA 90033
is typically activity-induced and aggra- vated with functions that increase patellofemoral compressive forces. such as ascending and descending stairs, inclined walking, squatting, and prolonged sitting (13,41). Ortho- paedic assessment is usually positive for a patellar grind test and discom- fort with palpation of the medial and lateral borders of the patella (41,58). Swelling, loss of motion, and a sensa- tion of giving way o r instability may also be present (6).
Despite the high incidence of patellofemoral pain in the general population, the pathophysiology of this disorder is not clearly under- stood. The most commonly accepted hypothesis is related to abnormal pa- tellar tracking which increases patel- lofemoral joint stress and subsequent articular cartilage wear (18,27,30,34, 53,55). Although articular cartilage is aneural and has been dismissed as a possible source of symptoms, it has been proposed that the subadjacent
endplate is exposed to pressure varia- tions that would normally be a b sorbed by healthy cartilage (22). This mechanical stress is believed to stimu- late pain receptors in the subchon- dral bone (22).
Historically, conservative treat- ment of patellofemoral pain has fo- cused on restoring normal patellar tracking by improving dynamic stabil- ity (29,40,49). Of particular interest to clinicians has been the vastus me- dialis oblique (VMO), which has been implicated as being the primary medial stabilizer of the patella (42). In their classic work, Lieb and Pen). (42) identified the distal fibers of the vastus medialis to be angled at a p proximately 55" from the longitudi- nal axis of the femur, making this portion of the muscle best suited to prevent lateral subluxation of the patella (Figure 1 ) . As a result of this mechanical advantage, it has been proposed that the VMO is capable of counterbalancing the lateral pull of
JOSPT Volume 28 Number 5 November 1 9 8
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
8, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
199
8 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

L I T E R A T U R E R E V I E W
FIGURE 1. F ik r orientation of the quadriceps muscu- lature in relation to the iemur (VL = Vastus lateralis, VI = Vastus intermedius, RF = Rectus [emoris, VML = Vastus medialis longus, VMO = Vastus medialis oblique).
the larger vastus lateralis to ensure patellar stability within the trochlear groove (42).
A lack of equilibrium between the VMO and vastus lateralis is widely accepted as contributing to lateral patellar subluxation (48,76,86). Most authors and clinical protocols at- tribute this dynamic imbalance to W O insuffkiency, which has been associated with atrophy, hypoplasia, inhibition, and impaired motor con- trol (2,15,49). k s a result of these assertions, there has been a strong clinical focus on selective rehabilita- tion of the VMO in the treatment of patellofemoral pain. The goal of such treatment is to restore dynamic bal- ance of the patella to correct patellar tracking (49,56,59,79). In addition, external suppor~5 such as taping and bracing are commonly used as adjuncts to supplement specific VMO strength- ening techniques (26,33,49,57).
Although emphasis on restoring patella stability continues to be the
mainstay of consewative care of patel- lofemoral pain, there exists consider- able controversy between research outcomes and clinical practice. For example, despite the commonly ac- cepted clinical practice of focusing on the VMO in the treatment of patellofemoral pain, recent studies in this area are not entirelv supportive (8,25,36,37,62). The apparent dis- crepancv between research findings and clinical practice may lie in the interpretation of the available re- search and its subsequent application clinically. Therefore, the purpose of this paper was to 1) compare and contrast the current literature relat- ing specifically to the treatment of patellofemoral pain and 2) relate these findings to the prevailing views regarding the clinical management of this disorder.
Does VMO Insufficiency Exist in the Patellofemoral Pain Population?
The apparent need to focus on the VMO in the treatment of patel- lofemoral pain is related to the belief that the W O is selectively atrophied or more readily inhibited by pain and/or effusion compared with the other vasti. The only support of this hypothesis, however, was presented by Gerber et al (1 9), who reported that in patients with anterior-cruciate- deficient knees, the vastus medialis was found to demonstrate greater atrophy than the rest of the quadri- ceps. Although this study did not look at the \'MO specificallv, the rela- tive difference was only 2.7%.
In contrast, the notion of selec- tive \'MO inhibition has been refuted by Spencer et al (77), who reported that through assessment of the H re- flex, joint effusion resulted in inhibi- tion of the quadriceps as a whole. Although it appeared that the vastus medialis was affected to a greater ex- tent (the VMO was not isolated), there was no statisticallv significant . .
difference to support this observa- tion. These authors concluded that
reflex inhibition of the quadriceps was not selective as to the various components it affects. This conclu- sion was recently supported by the work of Powers et al (62). who found that subjects with patellofemoral pain demonstrated reduced recruitment of the entire quadriceps muscle group during gait activities. These authors reported that this reduced recruit- ment was similar for all the vasti and that there were no differences that would suggest a preferential inhibi- tion of the VMO.
Since assessment of isolated VMO and vastus lateralis strength in v i m is not possible, electromvographv (EMG) has been used to compare the relative recruitment of these mus- cles with the rationale that decreased activity of the \'MO relative to the vastus lateralis is indicative of com- promised medial patellar stabilih. Although several investigators have studied the EMG activity of the dy- namic patellar stabilizers in subjects with patellofemoral pain, the results of these studies are equivocal. M'hile some authors have found significant differences in VMO and vastus latera- lis activity in patients with patel- lofemoral pain (48,76,86), others have not (6,45,52,85). Direct compar- isons of these studies are difficult be- cause of differences in experimental technique and methods of assessing EMG data.
One likelv reason for the incon- sistent results in these investigations may be related to the inherent vari- ability within the patellofemoral pain population. Since etiology of patel- lofemoral pain has been considered a dynamic entity, it is logical that a de- ficiency of the medial stabilizers should result in lateral displacement of the patella. It has been docu- mented through radiological exami- nation, however, that less than 50% of patients with patellofemoral pain demonstrate isolated lateral subluxa- tion (70.71 ). This would suggest that lateral patellar tracking is not a uni- versal finding in this disorder and,
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
8, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
199
8 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.
L I T E R A T U R E R E V I E W
therefore, such an inference cannot be generalized to all patients.
If medial quadriceps deficiency is responsible for patellar malalign- ment, then it stands to reason that subjects with documented lateral s u h luxation may exhibit imbalances be- tween the dynamic patellar stabiliz- ers, while patients that demonstrate relatively normal alignment may not. To date, only two studies have at- tempted to control for this potential variation within the patellofemoral pain population. Moller et al (52) classified patients into two categories: those with a histoy and clinical find- ings of patellar instability and those without evidence of patellar instabil- ip. Results showed no differences in VMO and vastus lateralis EMG activity within groups or between groups. indicating that EMG could not be used to identifi subjects with patellar subluxation. This finding is somewhat understandable, considering EMG is not an indicator of muscular strength and, therefore, may not be an appro- priate measure to estimate the dy- namic forces acting on the patella.
In contrast, Powers et al (65) have provided evidence suggesting that individuals with greater amounts of lateral subluxation demonstrate increased recniitment of the vastus medialis. Using kinematic magnetic resonance imaging techniques and dynamic EMG, these authors found an inverse relationship between lat- eral subluxation and vastus medialis activity, suggesting that increased re- cruitment of the vastus medialis rela- tive to the vastiis lateralis is in re- sponse to abnormal patellar alignment, and that diminished vas- tus medialis activity is not necessarily a cause of abnormal patellar tracking.
Although it is not clear from a research standpoint whether VMO insufficiency exists in the patel- lofemoral pain population (as as- sessed through EMG) , decreased VMO activity relative to the \astiis lateralis is commonlv reported clini- cally with the use of EMG biofeed- back units. Rased on information o b
RAW EMG (knee extension)
VMO
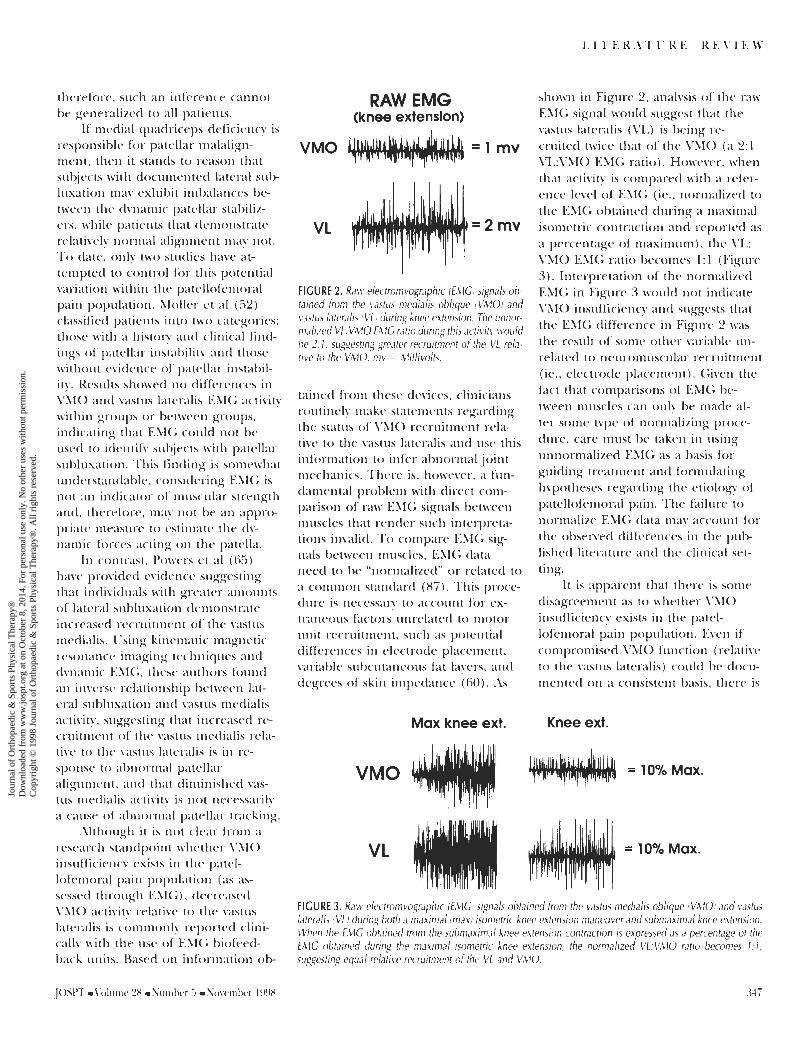
FIGURE 2. Raw electromvographic (EMGJ signals ob- tained irom the vastus medialis oblique (VMOI and vastus lateralis (VL) during knee extension. The unnor- malized VL:VMO EMG ratio during this activity would be 2: I , suggesting greater recruitment of the VL rela- tive to the VMO. mv = Millivolts.
tained from these devices, clinicians routinely make statements regarding the status of W O recruitment rela- tive to the vastus lateralis and use this information to infer abnormal joint mechanics. There is, however, a fun- damental problem with direct com- parison of raw EMG signals between muscles that render such interpreta- tions invalid. To compare EMG sig- nals between muscles, EMG data need to be "normalized" or related to a common standard (87). This proce- dure is necessay to account for ex- traneous factors unrelated to motor unit recruitment, such as potential differences in electrode placement, variable subcutaneous fat layers, and degrees of skin impedance (60). As
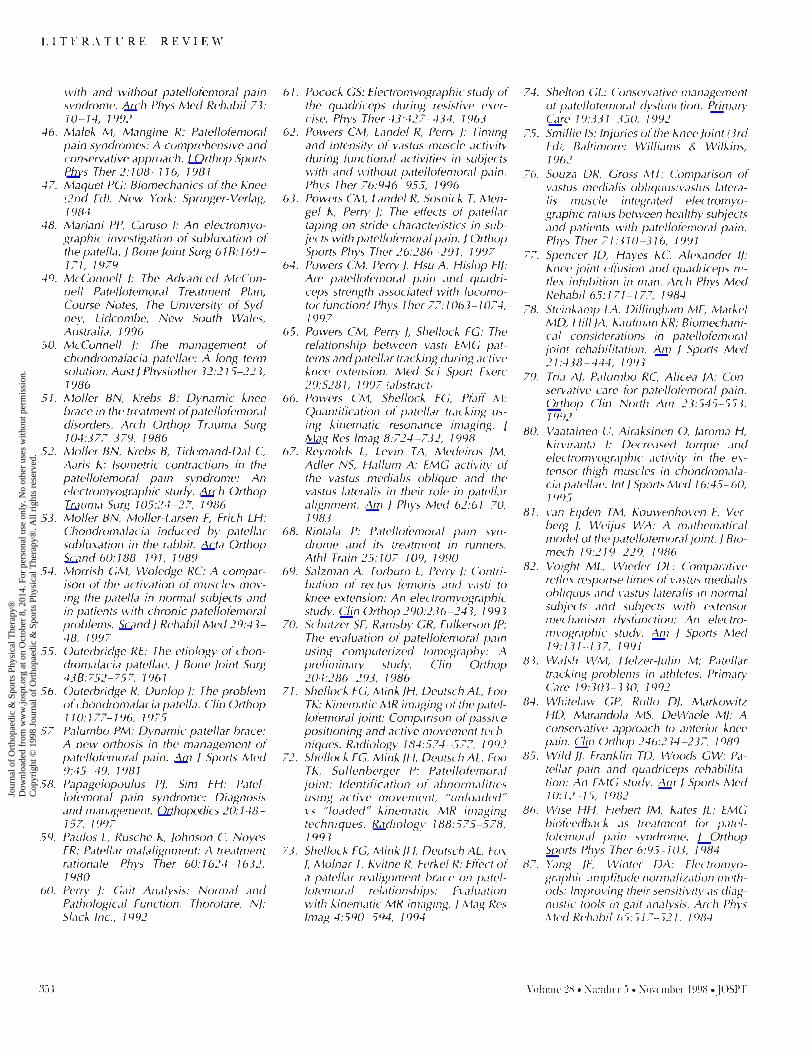
Max knee ext.
shown in Figure 2, analysis of the raw EMG signal would suggest that the vastus lateralis (VL) is being re- cruited twice that of the VMO (a 2:l VL:VMO EMG ratio). However, when that activity is compared with a refer- ence level of EMG (ie., normalized to the EMG obtained diiring a maximal isometric contraction and reported as a percentage of maximum), the VL: VMO EMG ratio becomes 1 :1 (Figure 3). Interpretation of the normalized EMG in Figure 3 would not indicate VMO insufficiency and suggests that the EMG difference in Figure 2 was the result of some other variable un- related to neuromuscular recniitment (ie., electrode placement). Given the fact that comparisons of EMG be- tween muscles can only be made af- ter some type of normalizing proce- dure, care must be taken in using unnormalized EMG as a basis for guiding treatment and formulating hypotheses regarding the etiology of patellofemoral pain. The failure to normalize EMG data may account for the observed differences in the p ~ i h lished literature and the clinical set- ting.
It is apparent that there is some disagreement as to whether VMO insufficiency exists in the patel- lofemoral pain population. Even if compromised VMO function (relative to the vastus lateralis) could be docu- mented on a consistent basis, there is
Knee ext.
VMO = 10Yo Max.
VL = 10% Max.
FIGURE 3. Raw electromvographic fEMGJ signals obtained from the vastus medialis oblique (VMOI and vastus laterah (VL) during both a maximal (max) isometric knee extension maneuver and submaximal knee extension. When the EMG obtained from the submaximal knee extension contraction is expressed as a percentage of the EMG obtained during the maximal isometric knee extension, the normalized VL:VMO ratio becomes l : l , suggesting qua1 relative recruitment of the VL and VMO.
JOSPT \'olrmc ?8 Numhrr .', Sovemlxr 1998
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
8, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
199
8 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

L I T E R A T U R E R E V I E W
evidence suggesting that decreased VMO recruitment may not translate to patellar instability and altered patellofemoral joint function. Further research is necessary to correlate EMG patterns with patellar tracking to clearly define the role of the vasti in contributing to patellar kinemat- ics. Until this evidence is available, however, the role of the VMO in con- tributing to patellar malalignment will remain somewhat speculative.
Neuromuscular Timing of VMO Relative to the Other Vasti
In addition to the magnitude of motor unit activity, asynchronous tim- ing of vasti muscle contraction also has been implicated as contributing to patellar instability. In this model, it is hypothesized that the vastus latera- lis contracts earlier than the VMO, therefore, contributing to a laterally directed force on the patella (82). Evidence in support of a timing dif- ference with respect to the onset of VMO activity relative to the vastus lateralis was first presented by Voight and Wieder (82) who reported that activation of the VMO was delayed compared to the vastus lateralis in patients with patellofemoral pain dur- ing a monosynaptic reflex (patellar tendon tap), and that this trend was reversed in control subjects. Despite statistical significance, the magnitude of these differences was not reported. and, therefore, the clinical rele\ance of the results could not be assessed.
Voight and Wieder (82) also pos- tulated that a feedforward mecha- nism may exist, in which the VMO normally contracts prior to the vastus lateralis. Such a temporal advantage would theoretically facilitate the abil- ity of the VMO to maintain patellar stability against the laterally directed forces of the much larger vastus late- ralis. The concept of a feedforward mechanism is supported by the find- ings of Grabiner et al (24) who also reported that activity of the VMO preceded that of the vastus lateralis
in normal subjects. The magnitude of this timing difference, however, was only 5.6 milliseconds, thus, casting doubt as to the clinical significance of this finding.
In contrast, recent investigations have failed to find significant timing differences between the different vasti in subjects with patellofemoral pain (21,37,54,62). These studies var- ied from those of Voight and Wieder (82) and Grabiner et al (24). in that timing was assessed during tasks that typically reproduce patellofemoral pain. In addition, neither of the lat- ter studies reported any evidence of a possible feedforward mechanism with respect to the onset of vasti activity. However, the study by Gilleard et al (21) found that when the patel- lofemoral joint was taped the VMO was recnlited earlier than the vastus lateralis during both stepup and stepdown tasks.
Based on the results of the above studies, it would appear that the ar- gument for a neuromuscular timing is somewhat tenuous. Vasti timing differences that have been identified in the patellofemoral pain population are of the magnitude of a couple of milliseconds, well below the temporal resolution of most EMG biofeedback units. Although there remains a strong clinical focus on altering the timing of the VMO relative to the vastus lateralis through the use of muscle reeducation techniques (49), further research is necessary to vali- date these treatment approaches.
Can the VMO Be Selectively Recruited or Strengthened?
As mentioned previously, the treatment of patellofemoral pain has focused on restoring dynamic patella stability through strengthening of the VMO. Such clinical practice is based on the assumption that the VMO is disproportionately weak relative to the vastus lateralis, despite the fact that assessment of VMO strength in vivo cannot be quantified. Although
isolated strengthening of the VMO would appear to be desirable from a biomechanical standpoint, there is little evidence suggesting that this is possible. The concept of VMO strengthening is prefaced on the be- lief that the VMO can be selectively recruited independently of the vastus lateralis through various exercises (29,31,50). The most common activi- ties which have been postulated to facilitate VMO strengthening include various quadriceps exercises (ie., straight leg raises, isometric quadri- ceps sets, terminal knee extension), hip adduction, and internal tibia1 rotation.
Quadric+ ~xmri.ws For many years, short arc knee extension exer- cises were thought to selectively strengthen the VMO, as this portion of the vastus medialis was implicated as being responsible for terminal knee extension (1 1,75). A mechani- cal study by Lieb and Perry (42) demonstrated, however, that the VMO was not capable of indepen- dent terminal knee extension and that this range of motion was the re- sult of all vasti working in concert to achieve knee extension. Subsequent to this investigation, there have been many studies supporting the concept that there is no selective function attributable to the VMO with respect to knee extension (1,28,35,43,61,67, 69).
Recent investigations have evalu- ated whether the VMO can be prefer- entially recruited with various types of activities in both normal and patel- lofemoral pain subjects. Cerny (8) examined 22 variations of quadriceps exercises (ie., quadriceps sets, isomet- ric holds with knee flexion, knee ex- tension, wall slides, etc.) and found that neither resulted in greater VMO activity relative to the vastus lateralis. Likewise, studies by Laprade et al (39) and Vaatainen et al (80) found no differences in VMO and vastus lateralis activity during isometric knee extension in both patellofemoral pain and control subjects.
\'nlume 28 Number 3 November 1998 JOSPT
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
8, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
199
8 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

L I T E R A T U R E R E V I E W
Hip n0hrt ion Various types of hip adduction exercises (either inde- pendently or in conjunction with knee extension) have been advocated as means by which the VMO can be preferentially recruited (29.31 ). The foundation for this hypothesis is based on the anatomical work of Bose et al (5), who observed that the VMO originates from the adductor magnus tendon and, to a lesser ex- tent, from the adductor longus ten- don. From a clinical standpoint, i t is thought that contraction of the hip adductors may transfer a physiologi- cal stretch to VMO, which could pos- sibly alter the length-tension proper- ties of these fibers, thus, promoting enhanced force of contraction (31 ). Additionally, it has been proposed that contraction of the hip adductors may provide a more stable proximal attachment and, therefore, facilitate preferential activation of the VMO (36,5O).
There have been many investiga- tions looking at whether the VMO can be preferentially recruited with various hip adduction exercises. Hanten and Schulthies (29) reported greater VMO activity compared with the vastus lateralis during hip adduc- tion, while Hodges and Richardson (31) found that simultaneous hip adduction and knee extension during weight bearing increased VMO EMG activity relative to the vastus lateralis. The latter study did not use normal- ized EMG, however, and, therefore, the validity of the results must be questioned.
In contrast to the findings of the above studies, other authors have re- ported no differences in relative re- cruitment of the VMO compared with the vastus lateralis during vari- ous exercises incorporating hip ad- duction. Kxst and Jewett (36) found that the concurrent use of the hip adductors during knee extension did not increase VMO activitv. Subsequent studies by Grabiner et al (25). Cernv (8). and Laprade et al (39) have also reported that hip adduction has no effect on W O recruitment.
As mentioned previously, differ- ences in experimental technique (ie., surface vs. fine wire electrodes), methods of quantif\ing EMG (nor- malized vs. nonnormalized) data, and the inherent variability of EMG mea- surements may partially explain these conflicting findings. Additional stnd- ies utilizing larger sample sizes and appropriate experimental techniques are necessan to further explore whether or not hip adduction influ- ences \&I0 activation.
J n t m n l tihinl rotntion As a result of the fascia1 attachment of the VMO to the anteromedial aspect of the tihia through the medial extensor aponeurosis, it has been proposed that the VMO can resist tibial exter- nal rotation and be preferentially ac- tivated through internal rotation of the tihia (29.39). Although the VMO would appear to have a role in limit- ing tibial rotation, Hanten and Schul- thies (29) found no etidence of pref- erential activation of the VMO with resisted internal tihial rotation in normal subjects. This finding is s u p ported by recent work of Cernv (8). who reported no selective recruit- ment of the W O when subjects per- formed an isometric quadriceps con- traction with the tibia held in internal rotation. In contrast, La- prade et al (39) found that the WO:VL EMG ratio was significantly greater when the motion of internal tibial rotation was resisted simulta- neously with knee extension when compared with isolated internal tihial rotation and hip adduction exercises. It should be noted, however, that the \%IO:C'L EMG ratio during the com- bined internal tibial rotation and knee extension exercise was no dif- fcrent from the EMG ratio obtained during knee extension alone.
S u m m t r ~ Although there is con- siderable controversy as to whether the \WO can be preferentially re- cruited relative to the vastus lateralis, one fact remains consistent: the VMO was never functioning independent of the vastus lateralis in any of the
studies cited. This indicates that iso- lated recruitment of the VMO does not occur with exercises that are commonly prescribed for the treat- ment of patellofemoral pain, and that selective strengthening is un- likely. Even if greater VMO EMG ac- tivity could be elicited relative to the vastus lateralis, the magnitude of VMO contraction would have to be at least 60% of maximum to stimulate hypertrophy (24,44). Given as such, it would appear that isolated recruit- ment or strengthening of the VMO through selected exercises may not be a realistic goal, and any emphasis on selective strengthening of the VMO would most likely translate into a general quadriceps strengthening effect.
Strengthening of the Extensor Mechanism and Its Role in the Treatment of Patellofemoral Pain
Physical therapy treatment of patellofemoral pain typically includes one or more of the following: lower e x t r e m i ~ strengthening (especially the quadriceps), stretching of tight musculature and the patellar retinac- ulum, anti-inflammatory agents (ie., ice), the use of patellofemoral brac- ing or taping, foot orthotics, and re- striction of aggravating activities (41, 50,57-59,74,79,85,84). Treatment approaches for patellofemoral pain v a n however, one component that is regularly recommended and com- monly incorporated into most pro- grams is strengthening of the exten- sor mechanism with emphasis on the vastus medialis or the VMO.
Although it can be debated whether exercises used to isolate the VMO actually increase VMO strength or pro\ide a generalized quadriceps strengthening effect, it is apparent from the literature that this form of treatment has produced successful clinical results (10,50,84). A recent study by Powers et al (64) has sug- gested that locomotor function in persons with patellofemoral pain is
JOSPT Yolume 28 Number 5 Novcmber 1998 349
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
8, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
199
8 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

;~ssociated with incrc;~sed qriadriceps femoris ~nuscle torque, thus. lending slipport to the concept of strengthen- ing ;IS a usrfd treatment option. De- spite thcsc findings, however, the mcch;~nism by which strcngthcning improves patellofi~~~ol-al pain symp toms and functional ability has not heen established.
As mentioned ahovc, the fact that only 50% of patients with patel- lofemoral pain demonstrate tracking ;thnormalitics, but still appear to re- spond f;~vol-;~bly to qriadriceps strengthening, suggests that this form of treatment may have a more subtle efkct on the patellofemol-al joint. For example, i t is possible that gross quadriceps strengthening may alter the contact location and pressure distribution, possibly relieving ;I sensi- tive area. Further resc;\rch in this arca is needed to identify this niccha- nisrn.
\\'hatcver the means by which qu;~driccps strengthening improves patcllokrnoraI p i n symptoms, such a program should he b;~scd on sound biomech;mic;d foundations and sensi- ble cxercisc pl-ogrcssion. Two com- ~nonly employed mcthods for strengthening the extensor mecha- nism, open ; ~ n d closed chain excr- cises, will now be discussed fi-om a biomcch;~nic;~l standpoint, with impli- cation for their use in the trcatrnent of patclIofemol-;d pain.
Patellofemoral Joint Biomechanics During Open and Closed Chain Exercises
Sincc p;ttcllofc.niol-;~l pain is ?pi- c;~lly I-rproduccd with acti\ities th;~t are associated with high patcllokmtr ral joint I-eaction forces (ie., stair climbing and sqi~atting) (13.41 ), it would appear that an exercise prw gram shotild be designed to enhance qt~;~driceps strengtlicning while k e e p ing.joint stress to a minimum. This is p;wticularly important during the i~cutc phase of p;~tellofemoral pain when symptoms can hc reatlil!. exac-
FIGURE 4. Compressive iorces on the patelloiemoral joint are determined hv the resultant o i M , (quadriceps tendon iorce vector) and M, patellar ligament iorce vector). from Fulkerson jP, Hungehrd DS: Disorders o i the Patelloiemoral joint (2nd €dl, Baltimore: MM- liams & Mlilkins, 1990, 0 john P. Fulkerson, MD, reprinted with perminionJ.
e r k ~ t e d . To ;~ccomplish this task, klio\vlcdge of the biomcchanics of the patcllofelnoral joint is ncccssal?.
The patellofhol-;~I joint reaction fi~rce is the n1c;lsrircrncnt of compres- sion of the patella against the femur and is dependent upon the angle of knec flexion as well as muscle ten- sion (3,47,81). Thc rcsi~ltant of the qmdriccps forcc vector and patellar tendon fiwce vector is cqrial mid o p posite to the patellofemor;d joint re- action force (7 , which evokes com- pressivc stresses on the patello- fi.niol-;d articular c;~rtilage (Figure 4). Another important \;~ri;~hle to con- sider regarding the biomechanics of the patellofernoral joint is the arca of contact bc twcn the patella and fc- mur. As repor-tcd h!. Good fellow ct ;11 (23), the patellofcmol-;d contact area increases with kncc flexion, with the total areit ;it 90" being ;~ppro>ti~nately twice that at 30' (Figure .5). i2'hen considering the forccs tl-ansmittcd
FIGURE 5. Contact areas on the patella as a iunction oiknee ilevion at 20, 45, 90, and 135: ((A-B = Path of medial margin o i contact zone, I = Inierior, S = Superior, 1 = Lateral, M = Medial). f r o m Goodiellow 1, Hungerford DS, Zindel M: Patelloiemoral joint me- chanics and patholqqv. / Bone joint Surg 58B13):287- 290. 1976, reprinted with permission/.
through the patellofemoral joint, an assumption is made that the joint reaction force is equally distributed across the entire contact area. The fact that the q~~adr iceps forcc and the contact area changes with vaying knee flexion angles has significant implications for prescribing different hpes of theraprutic exercise.
During an open chain exercise (ic., knec extension with resistance applied at the ankle), the amount of quadriceps force required to extend thc knee steadil! increases as the knce movcs from 90" to frill knee cxtcnsion. r l study performed by Lieb and Per17 (42) demonstrated that ;I
60% increase in quadriceps forcc was necessary to complete the last 1.5" of
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
8, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
199
8 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

L I T E R A T U R E R E V I E W
knee extension. This increase in force was attributed to a decrease in mechanical advantage of the extensor mechanism. In addition to the in- crease in quadriceps force as the knee extends, the patellofemoral con- tact area steadily decreases. This com- bination of increased quadriceps force and decreased contact area dur- ing terminal knee extension results in greater patellofemoral joint con- tact stress/pressure compared with greater knee flexion angles where the quadriceps force is not as great and the contact area is larger (32).
Conversely, during closed chain exercise (ie., squatting), the quadri- ceps force is relatively minimal as the knee is extended and steadily in- creases as the knee flexes (32). This increase in force is distributed over a greater surface area as the contact area also is increasing as the knee flexes. The greater contact area pre- vents excessive patellofemoral joint pressure during flexed knee activities (32).
An analysis of patellofemoral joint stress during open and closed chain exercises was undertaken by Steinkamp et al (78). The results of this studv found that compared with knee extension against resistance, the patellofemoral joint stress while per- forming a leg press maneuver was less at knee flexion angles from 0 to 48". Revond 48" of knee flexion, how- ever, the patellofemoral joint stress for the closed chain exercise was greater than the open chain exercise (Figure 6) . The results of Steinkamp et al (78) are similar to that reported by Hungerford and Bar? (32). who also estimated patellofemoral contact stress during both open and closed chain exercise. These studies suggest that quadriceps strengthening can be safely performed throughout the 0-90" knee flexion range by varying the mode of exercise. Since both forms of exercise can be used to pro- mote qi~adriceps hypertrophy, it a p pears that a comprehensive strength- ening program woiild incorporate both open and closed chain exercise
so that strengthening can be per- formed throughout a large arc of motion.
The Role of Taping and Bracing in the Treatment of Patellofemoral Pain
External patellar supports are commonly employed in the manage- ment of patellofemoral pain and are typically used as an adjunct to other treatment methods (ie., strengthen- ing) (50,5i,i4,79,83). The primary goal of patellofemoral joint bracing is to centralize the patella within the trochlear groove, thus improving pa- tellar tracking (33,57). The patellar taping technique as described by Mc- Connell (49) has gained widespread clinical acceptance as an effective treatment option. In this protocol, rigid strapping tape is applied to the patella to correct malalignment (as determined by clinical evaluation) and is followed bv functional strengthening of the quadriceps. Likewise, the various patellofemoral braces on the market have employed a number of methods to improve pa- tellar tracking, including the use of patellar cut-outs, lateral buttresses, air bladders, and various VelcrodU and Neoprene straps.
The therapeutic success associ- ated with use of external patellar s u p ports in conjunction with other treat- ment methods is supported by various clinical trials. Utilizing patel- lar taping, McConnell (50) reported that 92% of patients were pain free after eight treatment sessions, which was comparable with the 96% success rate reported by Gerrard (20) after only five treatments involving taping. Similar success rates have been re- ported for various patellofemoral braces ( 1 4 5 1.57).
The fact that the various forms of external patellar supports have been shown to be effective in reducing svmptoms immediately after applica- tion (4.26.63) indicates that such or- thoses have a mechanical effect on the patellofemoral joint. For exam-
0 30 48.4 60 90
Knee flexion (Degrees)
FIGURE 6. Comparison of patellofemoral joint stress in millipascals (MPa/ during open and closed chain exercise at four knee flexion angles. Error bars repre- sent one standard deviation. f r om Steinkamp LA, Dillingham MF, Markel MD, Hill )A, Kauiman KR: Biomechanical considerations in patellofemoral joint rehabilitation. Am) Sports Med2 1(3):438-444, 1993, reprinted with permission).
ple, Powers et al (63) reported that patellar taping resulted in small but significant increases in loading re- sponse knee flexion, which suggested more willingness by patellofemoral pain subjects to load the knee joint during gait. The mechanism by which taping or bracing affects the patellofemoral joint, however, is not entirely clear.
Although i t is assumed that brac- ing and taping improve patellar tracking, various radiological studies have reported mixed results. Rockrath et al (4) reported that de- spite a significant reduction in pain patellar taping was not effective in changing patella position. Larsen et al (38) found that patellar taping was effective in moving the patella medi- ally; however, this change was not maintained after exercise. In con- trast, Shellock et al (73) reported that 76% of patients demonstrated a qualitative correction in patellar sub- luxation while wearing the Rauer- feind Genutrdn P3 brace. The study by Shellock et al (73) differed from those described above in that patellar
JOSPT \'olrme 28 Number .3 Nownher 19!)8 35 1
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
8, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
199
8 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

L I T E R A T U R E R E V I E W
tracking was assessed dynamically against resistance using kinematic magnetic resonance imaging instead of through passive positioning tech- niques. The advantage of the kine- matic magnetic resonance imaging approach is that the contribution of the quadriceps to patellar tracking can be assessed (66,71,72). Al- though the results of Shellock et a1 (73) appear promising, care must be taken in interpreting these find- ings as no objective measures were taken.
Whether or not external patellar supports can change patellar tracking patterns can be debated at this point. It is possible, however, that the use of external supports may cause a change in the contact area between the pa- tella and the trochlea. For example, an elastic sleeve brace can induce
I t is apparent from the literature that external patellar supports can
offer pain relief.
patellofemoral joint compression which could increase patellofemoral joint contact area by seating the pa- tella deeper within the trochlear groove. This could potentially reduce contact stress as the joint reaction force would be distributed over a greater surface area. As shown in Fig- ure 7, the silicon inserts which are designed to center the patella within the trochlear groove are positioned anteriorly to the patella, therebv gen- erating joint compression.
Another proposed mechanism by which taping or bracing influences the patellofemoral joint is that such external supports may change the recruitment patterns of the vasti. As mentioned above, Gilleard et al (21) reported earlier activation of the W O following taping during both step-up and step-down tasks. On the
FIGURE 7. Avial v~ew oi the p~ te l l o f~ rno r~ l joint ioh- tained at 18' o i knee ilexionr usin,? kinematic mg- netic resonance imaging techniques irom a patient wearing the Bauedeind Genutrain P3 elastic sleeve brace. The silicon inserts which are designed to center the patella within the trochlear groove can be visual- ized anterior to the patella, therebv potentiallv inducing patellofemoral joint compression.
other hand, Cernv (8) found that taping had no effect on the VM0:VL EMG ratio. Further research is needed to document the effect of patellar taping and bracing on patel- lofemoral joint biomechanics and neuromuscular recruitment.
It is apparent from the literature that external patellar supports can offer pain relief. This is significant from a clinical standpoint, as pain may have an influence on quadriceps inhibition (9). If the goal of conser- vative treatment of patellofemoral pain is strengthening of the extensor mechanism, then it would appear that pain reduction would facilitate recruitment of the quadriceps. Such a decrease in pain would allow for adequate exercise progression and subsequent muscle hypertrophy.
SUMMARY
Rased on the review of the cur- rent literature, emphasis on the VMO in the rehabilitation of individuals
with patellofemoral pain mav not be indicated. This premise is supported by the fact that VMO insufficiency has not been consistently docu- mented in this population, and that there is no evidence suggesting that the VMO can be recruited or selec- tively strengthened independent of the other vasti. Exercises attempting to isolate the VMO most likely result in a general quadriceps strengthen- ing effect; however, the mechanism by which quadriceps strengthening reduces symptoms is not known. Therefore, exercises utilized for the treatment of patellofemoral pain should be aimed at an overall quadri- ceps strengthening effect, keeping in mind the biomechanics of the patel- lofemoral joint and the type of exer- cise prescribed. The use of external patellar supports (ie., taping and bracing) appears to be beneficial in reducing symptoms and may be a useful acljunct to a therapeutic exer- cise program.
FUTURE RESEARCH
It is evident from this review that continued research is necessary to flirther our knowledge of patel- lofemoral joint mechanics and how this disorder may be treated most effectively. Of utmost importance are the following: 1) to clearly establish the role of the VMO in contributing to patellar kinematics and patel- lofemoral pain, 2) to identify the mechanisms by which treatment proce- dures, such as taping and quadriceps strengthening, influence patellofemcl ral joint biomechanics, and 3) clinical trials aimed at determining which treat- ment procedures are most effective in reducing the symptoms asociated with patellofemoral pain. 1 0 ~ 1 ~
ACKNOWLEDGMENTS
The author would like to ac- knowledge Jacklyn Heino, MS, PT; H. James Phillips, MS, PT, OCS; and Jaquelin Perry, MD, for their critical reviews of this manuscript.
\'olrlme ?8 Number .i Nowmher 1998 -1OSPT
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
8, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
199
8 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

L I T E R A T U R E R E V I E W
REFERENCES
7 . Basmajian /V, Harden TP, Regenos EM: Integrated actions of the four heads of quadriceps femoris: An electromyo- graphic study. Anat Rec 7 72: 75-20, 7977
2. Bennett JG, Stauber WT: Evaluation and treatrnent of anterior knee pain us- ing eccentric exercise. Med Sci Sports Exerc 7 8.526 -530, 7 986
3. Bentley G, Dowd G: Current concepts of etiology and treatment of chondro- malacia patellae. Clin Orthop 7 89:209-228, 7 984
4. Bockrath K, Wooden C, Worrell T, In- gersoll CD, Farr /: Effects of patella tap- ing on patella position and perceived pain. Med Sci Sports Exerc 25:989- 992, 7993
5. Bose K, Kanagasuntheram R, Osman MBH: Vastus rnedialis oblique: An an- atomic and physiologic study. Ortho- pedics 3:88O- 883, 7 980
6. BoucherlP, King MA, Lefebvre R, Pepin A: Quadriceps femoris muscle activity in patellofemoral pain syndrome. Am J Sports Med 20527-532, 7 992
7. Buff HU, )ones LC, Hungerford DS: Ex- perimental determination of forces transmitted through the patellofemoral joint. / Biomech 2 7: 7 7-23, 7 988
8. Cerny K: Vastus medialis oblique/vas- tus lateralis muscle activity ratios for selected exercises in persons with and without patellofemoral pain syndrome. Phys Ther 75:672-683, 1995
9. deAndrade /R, Grant C, Dixon A: Joint distension and reflex muscle inhibition in the knee. / Bone loint Surg 47A:3 73- 322, 7965
70. DeHaven KE, Dolan WA, Mayer PI: Chondromalacia patellae in athletes: Clinical presentation and conservative management. Am J Sports Med 7:s- 7 7 , 7 979
7 7 . DePalma AF: Diseases of the Knee, Philadelphia: 1. B. L ippincott Company, 7 954
12. Devereaux M, Lachmann S: Patel- lo femoral arthralgia in athletes attend- ing a sports injury clinic. Br / Sports Med 78:78-27, 7984
73. Douchette SA, Goble EM: The effects of exercise on patellar tracking in lateral patellar compression syndrome. Am J Sports Med 20:434 -440, 7 992
74. Finestone A, Radin EL, Lev B, Shlamko- vitch N, Wiener M, Milgrom C: Treat- ment of overuse patellofemoral pain: Prospective randomized controlled clinical trial in a military setting. Clin Orthop 293:208-2 7 0, 7 993
75. Fox TA: Dysplasia of the quadriceps mechanism: Hypoplasia of the vastus
medialis muscle as related to the hyper- mobile patella syndrome. Surg Clin North Am 55: 7 99-226, 7 975
76. Fulkerson JP: The etiology of patel- lofemoral pain in young, active pa- tients: A prospective study. Clin Orthop 779:729-733, 7983
7 7. Fulkerson JP, Hungerford DS: Disorders of the Patellofemoral Joint (2nd Ed), Baltimore: Williams R. Wilkins, 7 990
78. Fulkerson JP, Shea KP: Mechanical ba- sis for patellofemoral pain and cartilage breakdown. In: Ewing 1 W led), Articu- lar Cartilage and Knee Joint Function: Basic Science and Arthroscopy, pp 93- 707. New York: Raven Press, 7 990
7 9. Gerber C, Hoppeler H, Claassen H, Ro- botti G, Zehnder R, jakob RP: The low- er-extremity musculature in chronic symptomatic instability of the anterior cruciate ligament. / Bone Joint Surg 67A: 7 034 - 7 043, 7 985
20. Gerrard B: The patellofemoral pain syndrome in young, active patients: A prospective studv. Clin Orthop 779:729-733, 7989
27. Gilleard W, McConnell /, Parsons D: The effect of patellar taping on the on- set of vastus medialis obliquus and vas- tus lateralis muscle activity in persons with patellofemoral pain. Phys Ther 78: 25-3 7 , 7998
22. Goodfellow J, Hungerford DS, Woods C: Patello-femoral joint mechanics and pathology: Chondromalacia patellae. J Bone Joint Surg 58B:297-299, 7 976
23. Goodfellow /, Hungerford DS, Zindel M: Patello-femoral joint mechanics and pathology: Functional anatomy of the patello-femoral joint. / Bone loint Surg 58B:287-290, 7 976
24. Grabiner MD, Koh TI, Draganich LF: Neuromechanics of the patellofemoral joint. Med Sci Sports Exerc 26: 7 0-2 7 , 7 994
25. Grabiner MD, Koh TI, von Haefen 1: Effect of concomitant hip joint adduc- tion and knee extension forces on quadriceps activation. Eur / Exp Mus- culoskel Res 7: 72 7-724, 7 993
26. Grace K: New treatrnent method for patellofemoral pain and clinical impli- cations. J Orthop Sports Phys Ther 25: 86, 7 997 (abstract)
27. Grana W, Kriegshauser L: Scientific ba- sis of extensor mechanism disorders. Clin Sports Med 4:247-257, 7 985
28. Hallen LG, Lindahl 0 : Muscle function in knee extension. Acta Orthop Scand 38:434-444, 7 967
29. Hanten WP, Schulthies SS: Exercise ef- fect on electromyographic activity of the vastus medialis oblique and the vastus lateralis muscles. Phys Ther 70: 56 7-565, 7 990
30. Heywood WB: Recurrent dislocation of the patella. / Bone joint Surg 43B:508- 577, 7967
3 7 . Hodges PW, Richardson CA: The influ- ence of isometric hip adduction on quadriceps femoris activity. Scandl Re- habil Med 2557-62, 7 993
32. Hungerford DS, Barry M: Biomechan- ics of the patellofemoral joint. Clin Or- thop 744:9-75, 1979
33. Hunter LY: Braces and taping. Clin Sports Med 4:439-454, 7 985
34. lnsall 1, Falvo KA, Wise D W: Chondro- malacia patellae: A prospective study. / Bone Joint Surg 58A: 7-8, 7 976
35. Jackson RT, Merrifield HH: Electro- myographic assessment of quadriceps muscle group during knee extension with weighted boot. Med Sci Sports Ex- erc 4:776-779, 7972
36. Karst GM, Jewett PD: Electromyo- graphic analysis of exercises proposed ior differential activation of rnedial and lateral quadriceps femoris muscle com- ponents. Phys Ther 73:286-295, 7 993
37. Karst GM, Willett GM: Onset timing of electromyographic activity in the vas- tus medialis oblique and vastus lateralis muscles in subjects with and without patellofemoral pain. Phys Ther 75:8 73- 823, 1995
38. Larsen B, Andreasen E, Urfer A, Mick- elson MR, Newhouse KE: Patellar tap- ing: A radiographic examination of the rnedial glide technique. Am / Sports Med 23:465-477, 7 995
39. Laprade J, Culham E, Brouwer B: Com- parison of five isometric exercises in the recruitment of the vastus rnedialis oblique in persons with and without patellofemoral pain. J Orthop Sports Phys Ther 27: 7 97-204, 7 998
40. LeVeau BF, Rogers C: Selective training of the vastus medialis muscle using EMG biofeedback. Phys Ther 60: 74 70- 7 4 7 5, 7 980
4 1. Levine J: Chondromalacia patellae. Physician Sportsmed 7:4 1-49, 1979
42. Lieb FJ, Perry J: Quadriceps function: An anatomical and mechanical study using amputated limbs. / Bone Joint Surg 50A: 7535- 7548, 7 968
43. Lieh FJ, Perry /: Quadriceps function: An electromyographic study under iso- metric conditions. / Bone Joint Surg 53A:749-758, 7977
44. MacDougall ID: Morphological changes in human skeletal muscle following strength training and immobilization. In: Jones NL, McCartney N, McComas A/ (eds), Human Muscle Power, pp 269- 288. Champaign, 11: Human Kinetics Publishers, 1986
45. Maclntyre DL, Robertson GE: Quadri- ceps muscle activity in women runners
JOSPT Volume 28 Number 3 November 1998 3.53
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
8, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
199
8 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.
L I T E R A T U R E R E V I E W
with and without patellofemoral pain syndrome. Arch Phys Med Rehabil73: 10-14, 1992 Malek M, Mangine R: Patellofemoral pain syndromes: A comprehensive and conservative approach. / Orthop Sports Phys Ther2:108-116, 1981 Maquet PG: Biomechanics of the Knee (2nd Ed), New York: Springer-Verlag, 1 984 Mariani PP, Caruso I: An electromyo- graphic investigation of subluxation of the patella. / Bone Joint Surg 6 16: 169- 171, 1979 McConnell 1: The Advanced McCon- nell Patellofemoral Treatment Plan, Course Notes, The University of Syd- ney, Lidcornbe, New South Wales, Australia, 1996 McConnell 1: The management of chondromalacia patellae: A long term solution. Aust / Physiother 32:2 15-223, 7 986 Moller BN, Krebs B: Dynamic knee brace in the treatment ofpatellofemoral disorders. Arch Orthop Trauma Surg 1 O4:377-379, 1986 Moller BN, Krebs B, Tidemand-Dal C, Aaris K: Isometric contractions in the patellofemoral pain syndrome: An electromyographic study. Arch Orthop Trauma Surg 7 05:24 -27, 1 986 Moller BN, Moller-Larsen F, Frich LH: Chondromalacia induced by patellar subluxation in the rabbit. Acta Orthop Scand 60:188-191, 1989 Morrish GM, Woledge RC: A compar- ison of the activation of muscles mov- ing the patella in normal subjects and in patients with chronic patellofemoral problems. Scandl Rehabil Med 29:43- 48, 1997 Outerbridge RE: The etiology of chon- dromalacia patellae. / Bone Joint Surg 43 B:752-757, 7 96 1 Outerbridge R, Dunlop /: The problem of chondromalacia patella. Clin Orthop 1 10: 177- 1 96, 1 975 Palumbo PM: Dynamic patellar brace: A new orthosis in the management of patellofemoral pain. Am / Sports Med 9:45-49, 1981 Papagelopoulus PI, Sim FH: Patel- lofemoral pain syndrome: Diagnosis and management. Orthopedics 20: 148- 157, 1997 Paulos L, Rusche K, Johnson C, Noyes FR: Patellar malalignment: A treatment rationale. Ph ys Ther 60: 1624 - 1632, 7 980 Perry 1: Gait Analysis: Normal and Pathological Function, Thoro fare, N/: Slack Inc., 1992
6 1. Pocock GS: Electromyographic study of the quadriceps during resistive exer- cise. Phys Ther 43:427-434, 1 963
62. Powers CM, Landel R, Perry 1: Timing and intensity of vastus muscle activity during functional activities in subjects with and without patellofemoral pain. Phys Ther 76:946 -955, 1 996
63. Powers CM, Landel R, Sosnick T, Men- gel K, Perry /: The effects of patellar taping on stride characteristics in sub- jects with patellofemoral pain. / Orthop Sports Phys Ther 26:286 -29 1, 1997
64. Powers CM, Perry 1, Hsu A, Hislop HI: Are patellofemoral pain and quadri- ceps strength associated with locomo- tor function? Phys Ther 77: 1063- 1074, 1997
65. Powers CM, Perry 1, Shellock FG: The relationship between vasti EMG pat- terns and patellar tracking during active knee extension. Med Sci Sport Exerc 29:S28 1, 1997 (abstract)
66. Powers CM, Shellock FG, Pfaff M: Quantification of patellar tracking us- ing kinematic resonance imaging. / Mag Res lmag 8:724-732, 1998
67. Reynolds L, Levin TA, Medeiros lM, Adler NS, Hallum A: EMG activity of the vastus medialis oblique and the vastus lateralis in their role in patellar alignment. Am / Phys Med 62:61-70, 1983
68. Rintala P: Patellofemoral pain syn- drome and its treatment in runners. Athl Train 25: 107- 109, 1990
69. Salzman A, Torburn L, Perry /: Contri- bution of rectus femoris and vasti to knee extension: An electromyographic study. Clin Orthop 290:236-243, 1993
70. Schutzer SF, Ramsby GR, Fulkerson /P: The evaluation of patellofemoral pain using computerized tomography: A preliminary study. Clin Orthop 204~286-293, 1986
71. Shellock FG, MinklH, Deutsch AL, Foo TK: Kinematic MR irnaging of the patel- lofemoral joint: Comparison of passive positioning and active movement tech- niques. Radiology l84:574 -577, 1992
72. Shellock FG, MinklH, Deutsch AL, Foo TK, Sullenberger P: Patellofemoral joint: Identification of abnormalities using active movement, "unloaded" vs "loaded" kinematic MR imaging techniques. Radiology 188:575-578, 1993
73. Shellock FG, MinkJH, Deutsch AL, Fox 1, Molnar T, Kvitne R, Ferkel R: Effect of a patellar realignment brace on patel- lofemoral relationships: Evaluation with kinematic MR irnaging. / Mag Res Imag 4590-594, 1994
74. Shelton GL: Conservative management of patellofemoral dysfunction. Primary Care 19:33 1-350, 1992
75. Smillie IS: Injuries of the Knee Joint (3rd Ed), Baltimore: Williams & Wilkins, 1962
76. Souza DR, Gross MT: Comparison of vastus medialis ob1iquus:vastus latera- lis muscle integrated electromyo- graphic ratios between healthy subjects and patients with patellofemoral pain. Phys Ther 7 l :3 10-3 16, 1991
77. Spencer ID, Hayes KC, Alexander 11: Knee joint effusion and quadriceps re- flex inhibition in man. Arch Phys Med Rehabil65:171-177, 1984
78. Steinkamp LA, Dillingham MF, Markel MD, HiIIIA, Kaufman KR: Biomechani- cal considerations in patellofemoral joint rehabilitation. Am / Sports Med 2 1 :438-444, 1993
79. Tria Al, Palumbo RC, Alicea /A: Con- servative care for patellofemoral pain. Orthop Clin North Am 23:545-553, 1992
80. Vaatainen U, Airaksinen 0 , /aroma H, Kirviranta I: Decreased torque and electromyographic activity in the ex- tensor thigh muscles in chondromala- cia patellae. Int] Sports Med 16:45-60, 1995
81. van Eijden TM, Kouwenhoven E, Ver- berg 1, Weijus WA: A mathematical model of the patellofemoral joint. / Bio- mech 19:2 19-229, 1986
82. Voight ML, Wieder DL: Comparative reflex response times of vastus medialis obliquus and vastus lateralis in normal subjects and subjects with extensor mechanism dysfunction: An electro- myographic study. Am / Sports Med 19:131-137, 1991
83. Walsh WM, Helzer-lulin M: Patellar tracking problems in athletes. Primary Care 79303-330, 1992
84. Whitelaw GP, Rullo Dl, Markowitz HD, Marandola MS, DeWaele MI: A conservative approach to anterior knee pain. Clin Orthop 246:234-237, 1989
85. Wild /I, Franklin TD, Woods GW: Pa- tellar pain and quadriceps rehabilita- tion: An EMG study. Am / Sports Med 10:12-15, 1982
86. Wise HH, Fiebert IM, Kates /L: EMG biofeedback as treatment for patel- lofemoral pain syndrome. / Orthop Sports Phys Ther 6:95- 1 03, 1984
87. Yang IF, Winter DA: Electromyo- graphic amplitude normalization meth- ods: Improving their sensitivity as diag- nostic tools in gait analysis. Arch Phys Med Rehahi1655 17-52 1, 1984
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
8, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
199
8 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

This article has been cited by:
1. Mei-Hwa Jan, Da-Hon Lin, Chien-Ho Janice Lin, Yeong-Fwu Lin, Cheng-Kung Cheng. 2009. The Effects of QuadricepsContraction on Different Patellofemoral Alignment Subtypes: An Axial Computed Tomography Study. Journal of Orthopaedic& Sports Physical Therapy 39:4, 264-269. [Abstract] [PDF] [PDF Plus]
2. Tracy A. Dierks, Kurt T. Manal, Joseph Hamill, Irene S. Davis. 2008. Proximal and Distal Influences on Hip and Knee Kinematicsin Runners With Patellofemoral Pain During a Prolonged Run. Journal of Orthopaedic & Sports Physical Therapy 38:8, 448-456.[Abstract] [PDF] [PDF Plus]
3. Christine A. Iverson, Thomas G. Sutlive, Michael S. Crowell, Rebecca L. Morrell, Matthew W. Perkins, Matthew B. Garber,Josef H. Moore, Robert S. Wainner. 2008. Lumbopelvic Manipulation for the Treatment of Patients With Patellofemoral PainSyndrome: Development of a Clinical Prediction Rule. Journal of Orthopaedic & Sports Physical Therapy 38:6, 297-312. [Abstract][PDF] [PDF Plus]
4. Yeong-Fwu Lin, Jiu-Jenq Lin, Cheng-Kung Cheng, Da-Hon Lin, Mei-Hwa Jan. 2008. Association Between SonographicMorphology of Vastus Medialis Obliquus and Patellar Alignment in Patients With Patellofemoral Pain Syndrome. Journal ofOrthopaedic & Sports Physical Therapy 38:4, 196-202. [Abstract] [PDF] [PDF Plus]
5. Tony Wilson. 2007. The Measurement of Patellar Alignment in Patellofemoral Pain Syndrome: Are We Confusing AssumptionsWith Evidence?. Journal of Orthopaedic & Sports Physical Therapy 37:6, 330-341. [Abstract] [PDF] [PDF Plus]
6. Jonathan D. Lesher, Thomas G. Sutlive, Giselle A. Miller, Nicole J. Chine, Matthew B. Garber, Robert S. Wainner. 2006.Development of a Clinical Prediction Rule for Classifying Patients With Patellofemoral Pain Syndrome Who Respond to PatellarTaping. Journal of Orthopaedic & Sports Physical Therapy 36:11, 854-866. [Abstract] [PDF] [PDF Plus]
7. Cynthia J. Watson, Micah Propps, Jennifer Ratner, David L. Zeigler, Patricia Horton, Susan S. Smith. 2005. Reliability andResponsiveness of the Lower Extremity Functional Scale and the Anterior Knee Pain Scale in Patients With Anterior Knee Pain.Journal of Orthopaedic & Sports Physical Therapy 35:3, 136-146. [Abstract] [PDF] [PDF Plus]
8. Martin Whittingham, Shea Palmer, Fiona Macmillan. 2004. Effects of Taping on Pain and Function in Patellofemoral PainSyndrome: A Randomized Controlled Trial. Journal of Orthopaedic & Sports Physical Therapy 34:9, 504-510. [Abstract] [PDF][PDF Plus]
9. Christopher M. Powers. 2003. The Influence of Altered Lower-Extremity Kinematics on Patellofemoral Joint Dysfunction: ATheoretical Perspective. Journal of Orthopaedic & Sports Physical Therapy 33:11, 639-646. [Abstract] [PDF] [PDF Plus]
10. Catherine L. Mascal, Robert Landel, Christopher Powers. 2003. Management of Patellofemoral Pain Targeting Hip, Pelvis, andTrunk Muscle Function: 2 Case Reports. Journal of Orthopaedic & Sports Physical Therapy 33:11, 647-660. [Abstract] [PDF][PDF Plus]
11. Tony Wilson, Nicholas Carter, Gareth Thomas. 2003. A Multicenter, Single-Masked Study of Medial, Neutral, and LateralPatellar Taping in Individuals With Patellofemoral Pain Syndrome. Journal of Orthopaedic & Sports Physical Therapy 33:8, 437-448.[Abstract] [PDF] [PDF Plus]
12. Mario Bizzini, Capt. John D. Childs, Sara R. Piva, Anthony Delitto. 2003. Systematic Review of the Quality of RandomizedControlled Trials for Patellofemoral Pain Syndrome. Journal of Orthopaedic & Sports Physical Therapy 33:1, 4-20. [Abstract][PDF] [PDF Plus]
13. David A. Wallace, George J. Salem, Ruben Salinas, Christopher M. Powers. 2002. Patellofemoral Joint Kinetics While Squattingwith and without an External Load. Journal of Orthopaedic & Sports Physical Therapy 32:4, 141-148. [Abstract] [PDF] [PDF Plus]
14. Cynthia J. Watson, Hollis M. Leddy, Tine D. Dynjan, Jennifer L. Parham. 2001. Reliability of the Lateral Pull Test and TiltTest to Assess Patellar Alignment in Subjects With Symptomatic Knees: Student Raters. Journal of Orthopaedic & Sports PhysicalTherapy 31:7, 368-374. [Abstract] [PDF] [PDF Plus]
15. Laura H. Lathinghouse, Mark H. Trimble. 2000. Effects of Isometric Quadriceps Activation on the Q-angle in Women Beforeand After Quadriceps Exercise. Journal of Orthopaedic & Sports Physical Therapy 30:4, 211-216. [Abstract] [PDF] [PDF Plus]
16. Cynthia J. Watson, Micah Propps, Wendy Galt, Amy Redding, Debra Dobbs, Scott F. Dye, Jenny McConnell, Christopher M.Powers, Cynthia J. Watson, Micah Propps, Wendy Galt. 1999. Reliability of McConnell's Classification of Patellar Orientationin Symptomatic and Asymptomatic Subjects. Journal of Orthopaedic & Sports Physical Therapy 29:7, 378-393. [Abstract] [PDF][PDF Plus]
17. Christopher M. Powers, Susie Mortenson, Dawn Nishimoto, Debra Simon. 1999. Criterion-Related Validity of a ClinicalMeasurement To Determine the Medial/Lateral Component of Patellar Orientation. Journal of Orthopaedic & Sports PhysicalTherapy 29:7, 372-377. [Abstract] [PDF] [PDF Plus]
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t on
Oct
ober
8, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
199
8 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.