renal update for internists: controversies and conundrums paul segal do assistant professor of...
TRANSCRIPT
Renal Update for Internists: Controversies
and ConundrumsPaul Segal DO
Assistant Professor of MedicineJohns Hopkins
ACP Meeting 2015
Objectives
• After viewing this presentation, the clinician will understand The staging system of Chronic Kidney Disease (CKD)
• The strengths and weaknesses of GFR equations• The clinical associations with various CKD stages• CKD progression• When to refer and when to dialyze
• The role of metabolic acidosis in CKD progression• The controversy surrounding sodium restriction• The Interaction of Physical Activity and CKD• Blood Pressure Targets in CKD
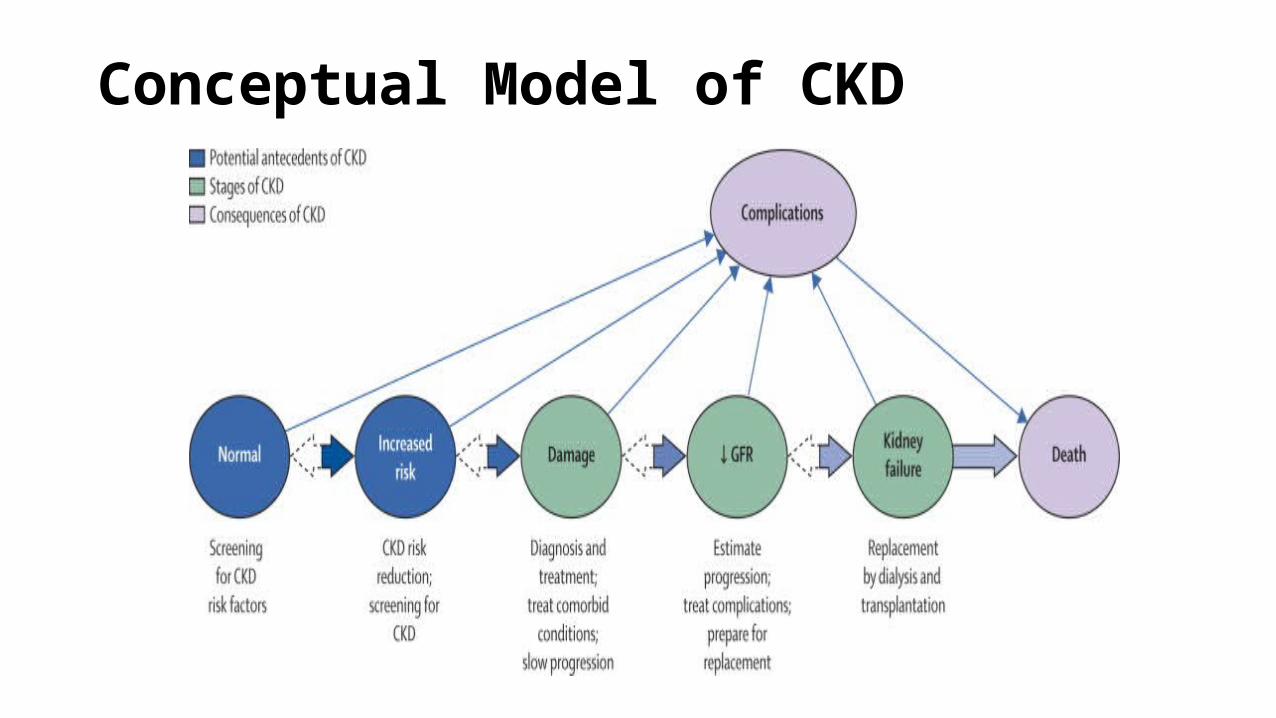
Conceptual Model of CKD
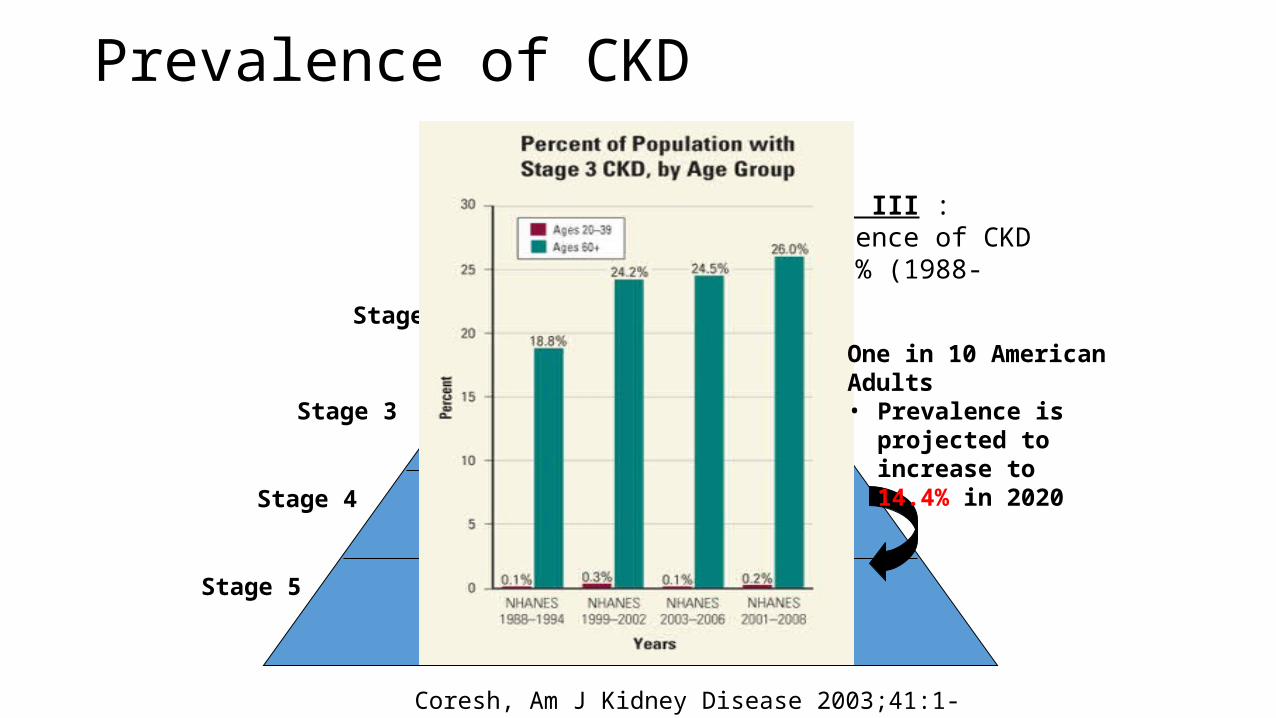
Prevalence of CKD
Stage 1
Stage 2
Stage 3
Stage 4
Stage 5
~ 7.6 million
~ 350- 400,000
~350, 000
NHANES III : prevalence of CKD ↑ 15.9% (1988-2004)
~ 5.3 million
~ 5.9 million
One in 10 American Adults• Prevalence is projected
to increase to 14.4% in 2020
Coresh, Am J Kidney Disease 2003;41:1-12.
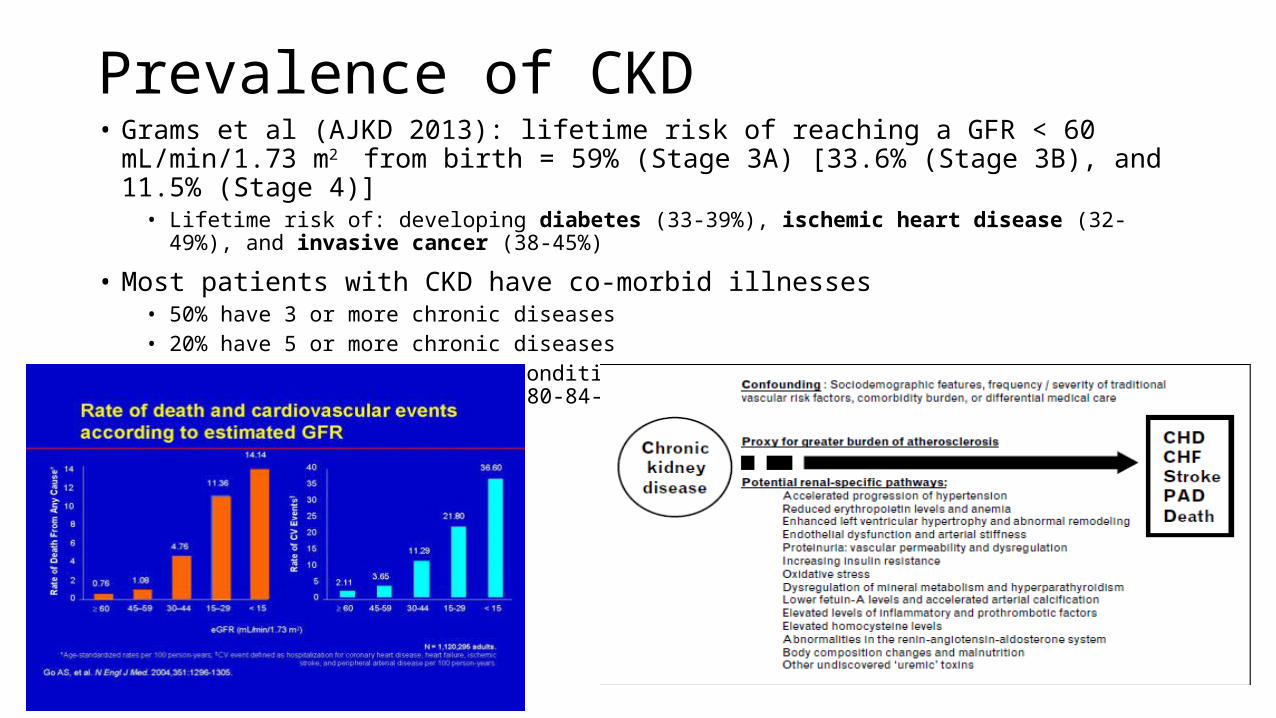
Prevalence of CKD• Grams et al (AJKD 2013): lifetime risk of reaching a GFR < 60 mL/min/1.73 m2 from birth = 59%
(Stage 3A) [33.6% (Stage 3B), and 11.5% (Stage 4)]• Lifetime risk of: developing diabetes (33-39%), ischemic heart disease (32-49%), and invasive cancer (38-45%)
• Most patients with CKD have co-morbid illnesses• 50% have 3 or more chronic diseases• 20% have 5 or more chronic diseases• The mean number of chronic conditions per individual increased from 1.88 (65-69-year age group) to 2.71 (80-84-
year age group)
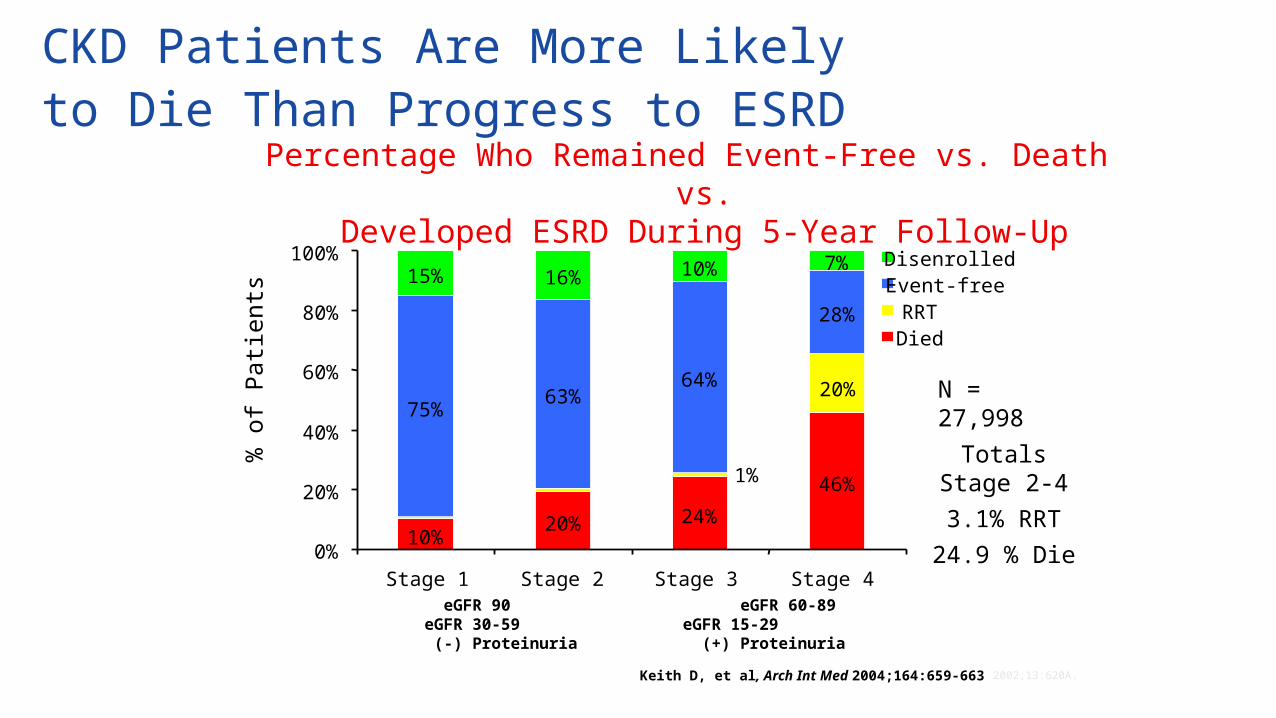
CKD Patients Are More Likely to Die Than Progress to ESRD
Percentage Who Remained Event-Free vs. Death vs.Developed ESRD During 5-Year Follow-Up
10%20% 24%
46%
75%63%
64%
28%
15% 16% 10% 7%
20%
1%
0%
20%
40%
60%
80%
100%
Stage 1 Stage 2 Stage 3 Stage 4
% o
f P
atie
nts
DisenrolledEvent-freeRRTDied
Totals Stage 2-43.1% RRT
24.9 % Die
Keith D, et al, Arch Int Med 2004;164:659-663 2002;13:620A.
N = 27,998
eGFR 90 eGFR 60-89 eGFR 30-59 eGFR 15-29 (-) Proteinuria (+) Proteinuria
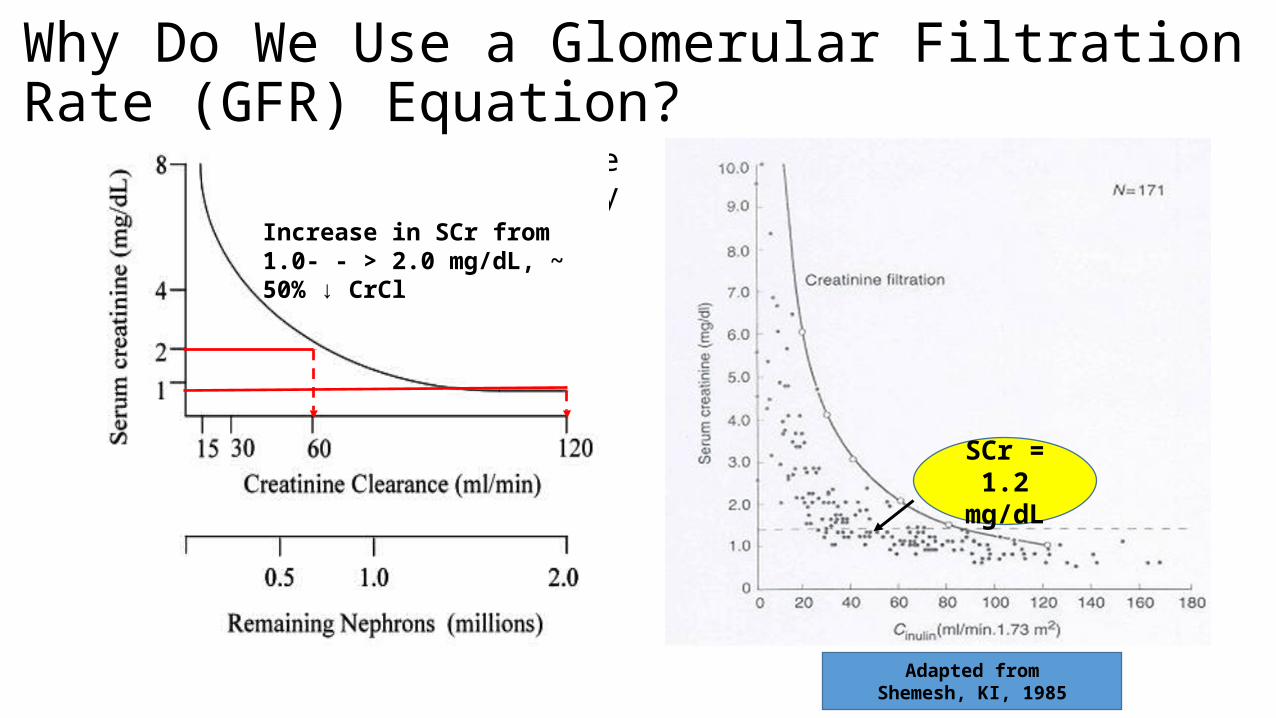
Why Do We Use a Glomerular Filtration Rate (GFR) Equation?
• Creatinine is an imprecise value and affected by many influences:
• High protein meal• Medications:
• Cimetidine, trimethoprim, fibrates• Hemolysis• Hyperglycemia• Edematous states• Hydration• Age, race and gender
SCr = 1.2 mg/dL
Adapted fromShemesh, KI, 1985
Increase in SCr from 1.0- - > 2.0 mg/dL, ~ 50% ↓ CrCl
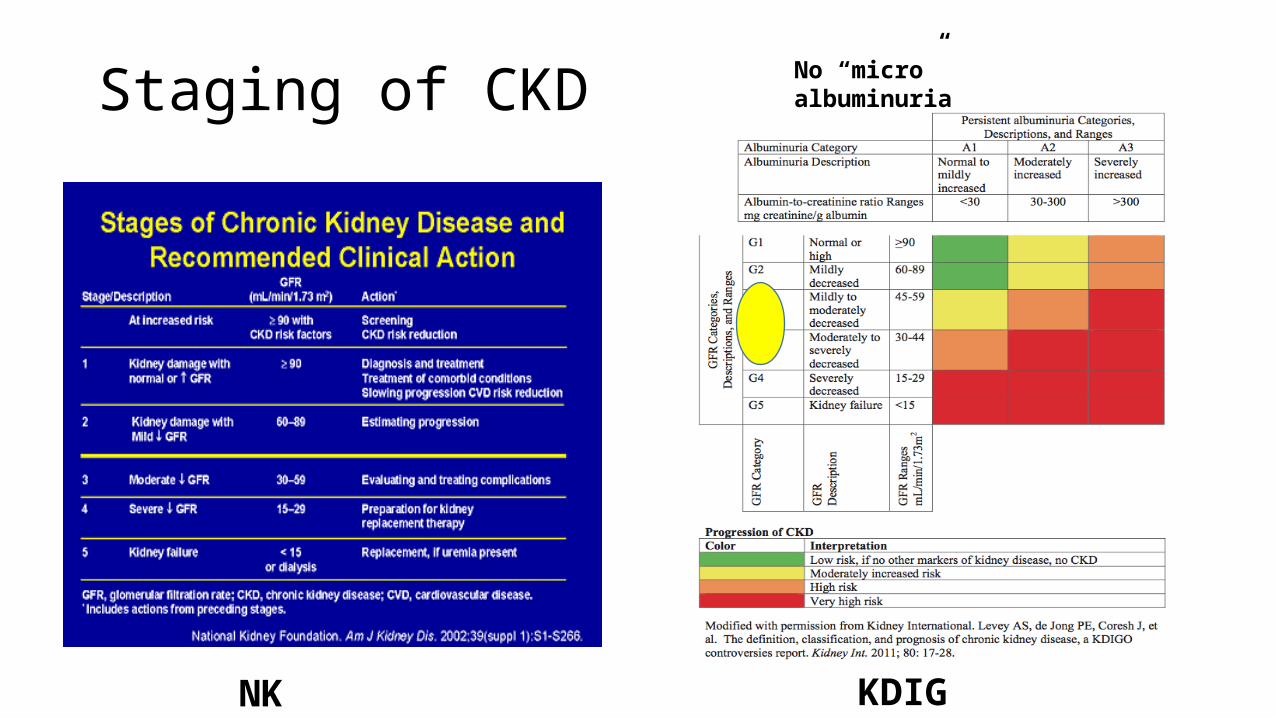
Staging of CKD No “micro” albuminuria
NKF KDIGO
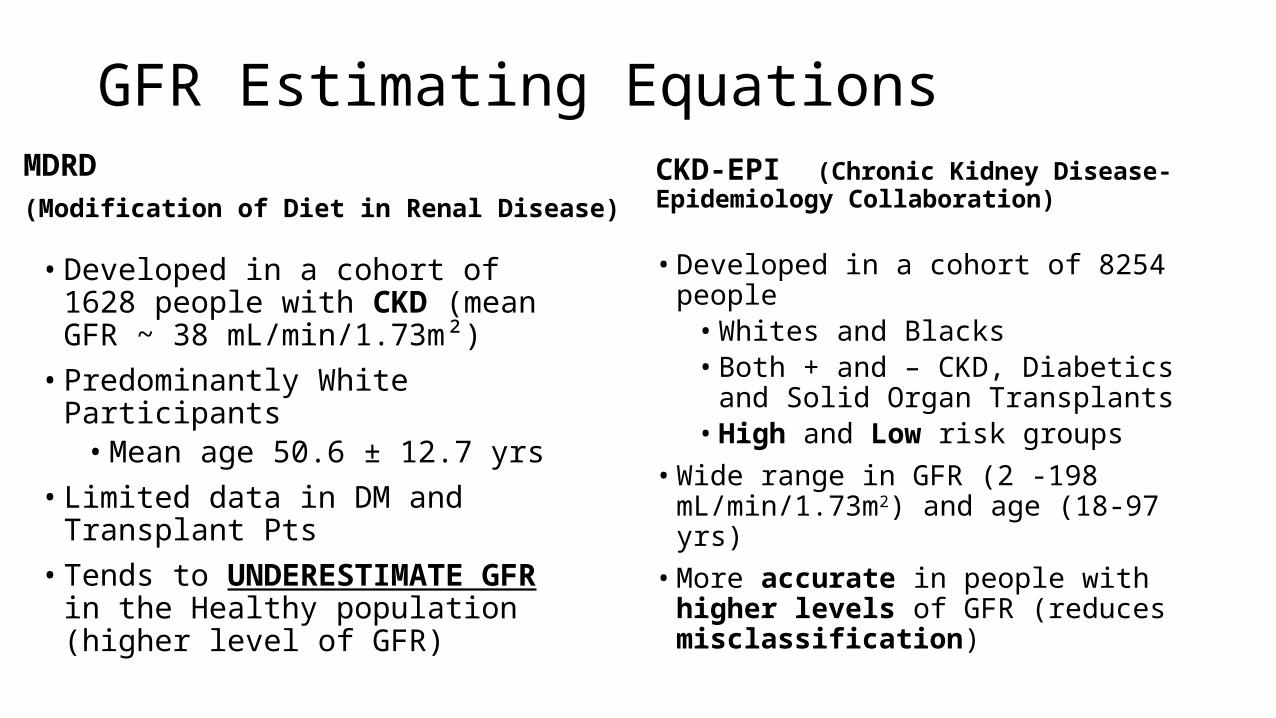
GFR Estimating EquationsMDRD (Modification of Diet in Renal Disease)
• Developed in a cohort of 1628 people with CKD (mean GFR ~ 38 mL/min/1.73m²)
• Predominantly White Participants• Mean age 50.6 ± 12.7 yrs
• Limited data in DM and Transplant Pts• Tends to UNDERESTIMATE GFR in the
Healthy population (higher level of GFR)
CKD-EPI (Chronic Kidney Disease- Epidemiology Collaboration)
• Developed in a cohort of 8254 people• Whites and Blacks• Both + and – CKD, Diabetics and
Solid Organ Transplants• High and Low risk groups
• Wide range in GFR (2 -198 mL/min/1.73m2) and age (18-97 yrs)
• More accurate in people with higher levels of GFR (reduces misclassification)
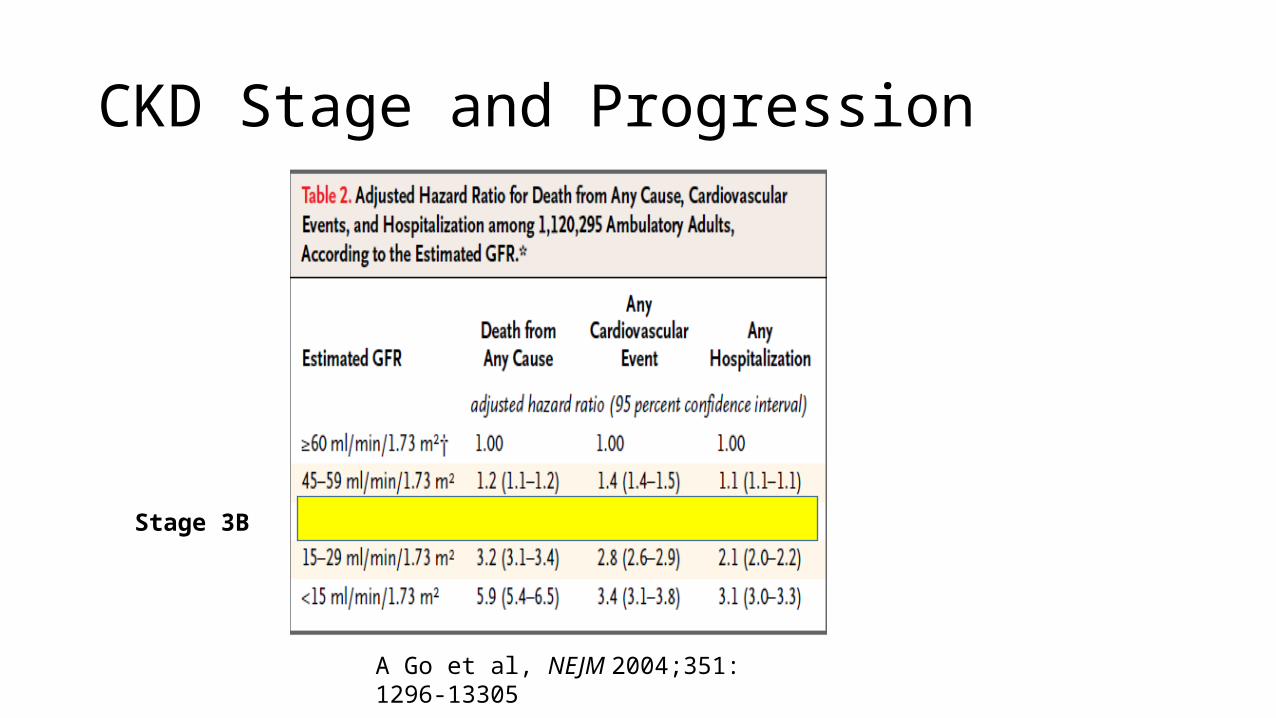
CKD Stage and Progression
A Go et al, NEJM 2004;351: 1296-13305
Stage 3B
What is a Disease?A pathological condition characterized by an identifiable group of signs or symptoms or
A condition that impairs normal functioning or
Illness or sickness often characterized by typical patient problems (symptoms) and physical findings (signs).
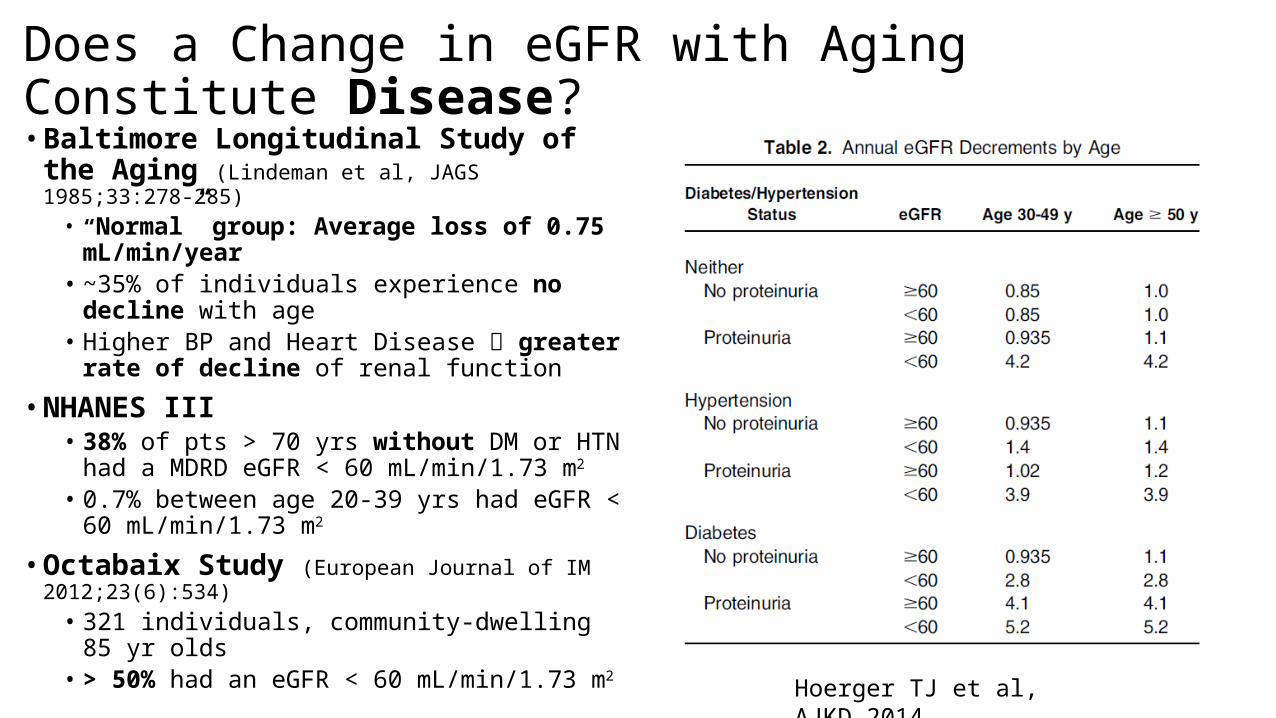
Does a Change in eGFR with Aging Constitute Disease?• Baltimore Longitudinal Study of the Aging
(Lindeman et al, JAGS 1985;33:278-285)• “Normal” group: Average loss of 0.75
mL/min/year• ~35% of individuals experience no decline
with age• Higher BP and Heart Disease greater rate of
decline of renal function
• NHANES III• 38% of pts > 70 yrs without DM or HTN had a
MDRD eGFR < 60 mL/min/1.73 m2
• 0.7% between age 20-39 yrs had eGFR < 60 mL/min/1.73 m2
• Octabaix Study (European Journal of IM 2012;23(6):534)
• 321 individuals, community-dwelling 85 yr olds
• > 50% had an eGFR < 60 mL/min/1.73 m2
Hoerger TJ et al, AJKD 2014.
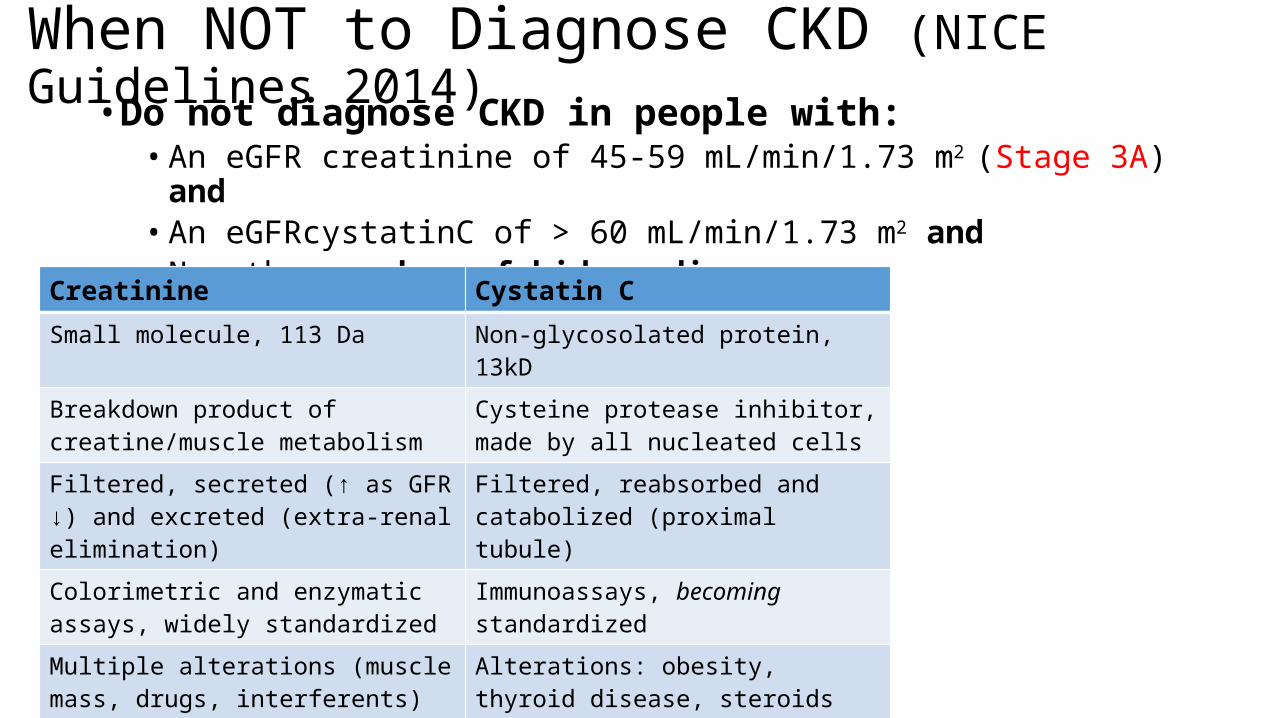
When NOT to Diagnose CKD (NICE Guidelines 2014)
• Do not diagnose CKD in people with:• An eGFR creatinine of 45-59 mL/min/1.73 m2 (Stage 3A) and• An eGFRcystatinC of > 60 mL/min/1.73 m2 and• No other marker of kidney disease
Creatinine Cystatin CSmall molecule, 113 Da Non-glycosolated protein, 13kD
Breakdown product of creatine/muscle metabolism
Cysteine protease inhibitor, made by all nucleated cells
Filtered, secreted (↑ as GFR ↓) and excreted (extra-renal elimination)
Filtered, reabsorbed and catabolized (proximal tubule)
Colorimetric and enzymatic assays, widely standardized
Immunoassays, becoming standardized
Multiple alterations (muscle mass, drugs, interferents)
Alterations: obesity, thyroid disease, steroids and HIV
“Tried and true”, GFR estimation “New kid”, GFR estimation and prognostic marker: CVD, all-cause mortality, DM, unsuccessful aging
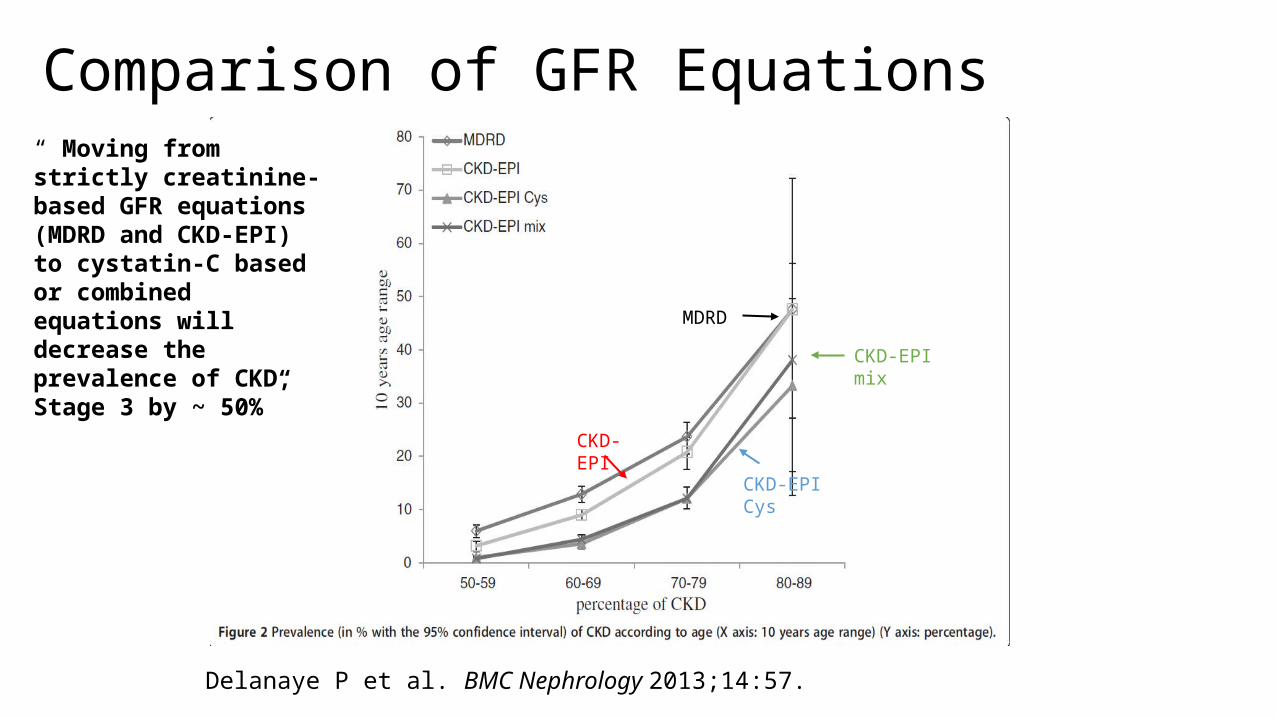
Comparison of GFR Equations
MDRD
CKD-EPI
CKD-EPI Cys
CKD-EPI mix
Delanaye P et al. BMC Nephrology 2013;14:57.
“ Moving from strictly creatinine-based GFR equations (MDRD and CKD-EPI) to cystatin-C based or combined equations will decrease the prevalence of CKD, Stage 3 by ~ 50%”

What do we know about CKD Progression?• Stage 3B is more likely to progress to Stage 4 and 5 than Stage
3A• Predictors: degree of albuminuria microscopic hematuria Stage 3 subgroup
• ≤ 45 mL/min/1.73 m2 = clinically significant breakpoint• GFR trajectory may be an important predictor of progression
2 x ↑ risk for disease progression
> 3 mL/min/1.73 m2/year requires CLOSER follow-up and identification of potentially reversible factors
Ann O’Hare
When to Refer?• KDIGO 2012 Guidelines
• Abrupt or sustained fall in eGFR (↓ GFR of ≥ 25%, change in GFR category or sustained ↓ in GFR of ≥ 15 mL/min/1.73 m2 within 12 months)
• eGFR < 30 mL/min/1.73m2 ± Diabetes• Urinary RBC casts or RBC > 20/hpf (microscopic hematuria without an
anatomic cause)• Refractory HTN (≥ 3 drugs)• Significant albuminuria:
• ACR ≥ 300mg/gm or AER ≥ 300mg/24 hrs• PCR ≥ 500mg/gm or PER ≥ 500mg/24 hrs
• NICE 2014 Guidelines• Take into account the individual’s wishes and co-morbidities• Rare or genetic renal disease
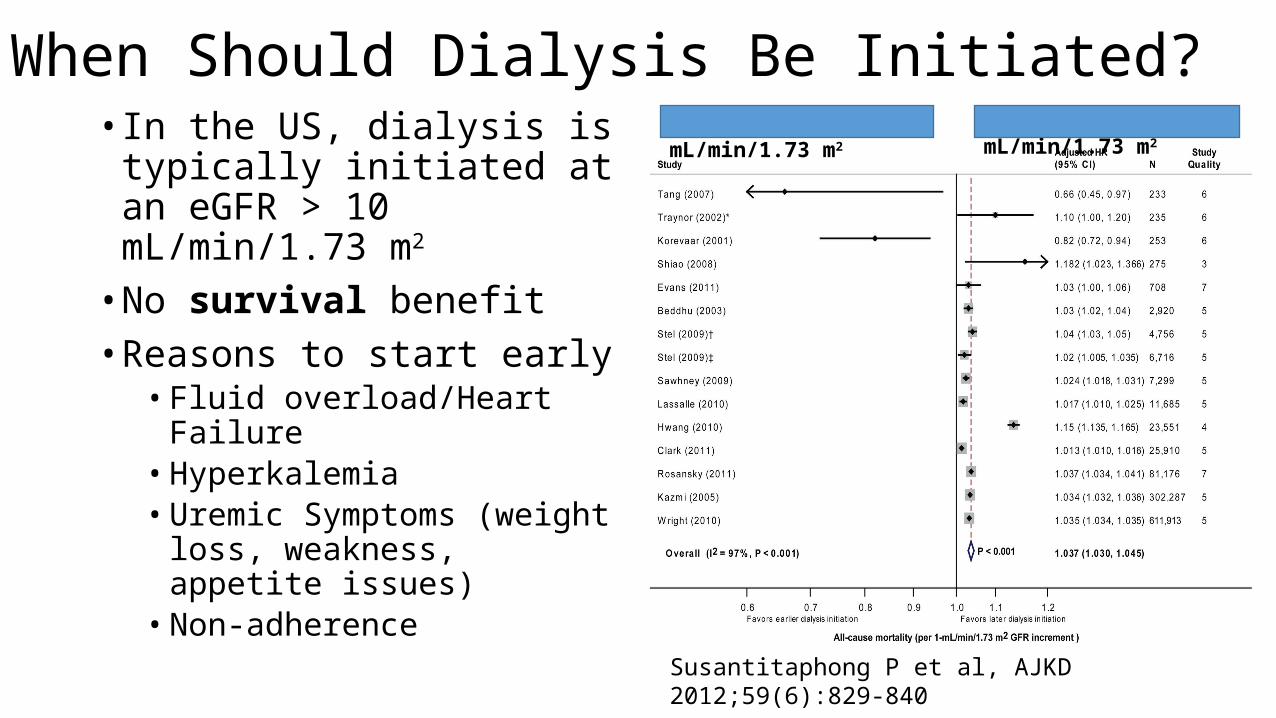
When Should Dialysis Be Initiated?• In the US, dialysis is typically
initiated at an eGFR > 10 mL/min/1.73 m2
• No survival benefit• Reasons to start early
• Fluid overload/Heart Failure• Hyperkalemia• Uremic Symptoms (weight loss,
weakness, appetite issues)• Non-adherence
eGFR 10-14 mL/min/1.73 m2 eGFR 5-7 mL/min/1.73 m2
Susantitaphong P et al, AJKD 2012;59(6):829-840
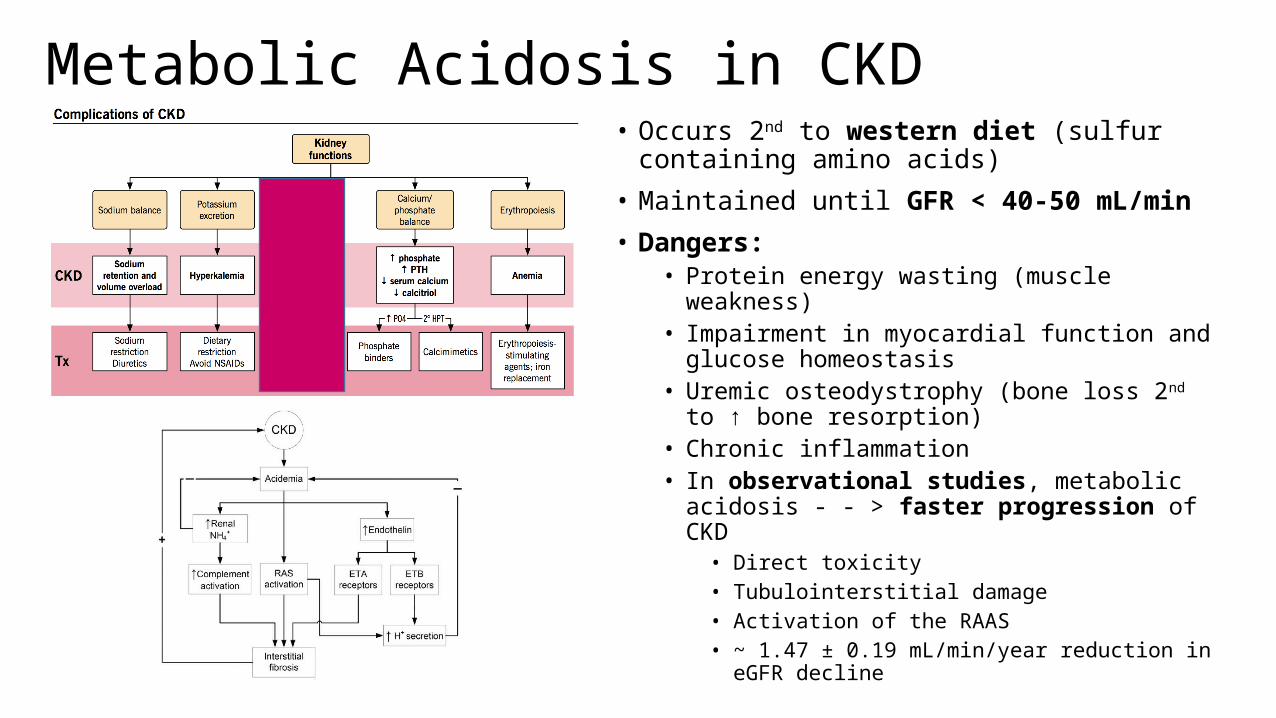
Metabolic Acidosis in CKD• Occurs 2nd to western diet (sulfur containing amino
acids)
• Maintained until GFR < 40-50 mL/min
• Dangers:• Protein energy wasting (muscle weakness)• Impairment in myocardial function and glucose
homeostasis• Uremic osteodystrophy (bone loss 2nd to ↑ bone
resorption)• Chronic inflammation• In observational studies, metabolic acidosis - - > faster
progression of CKD• Direct toxicity• Tubulointerstitial damage• Activation of the RAAS• ~ 1.47 ± 0.19 mL/min/year reduction in eGFR decline
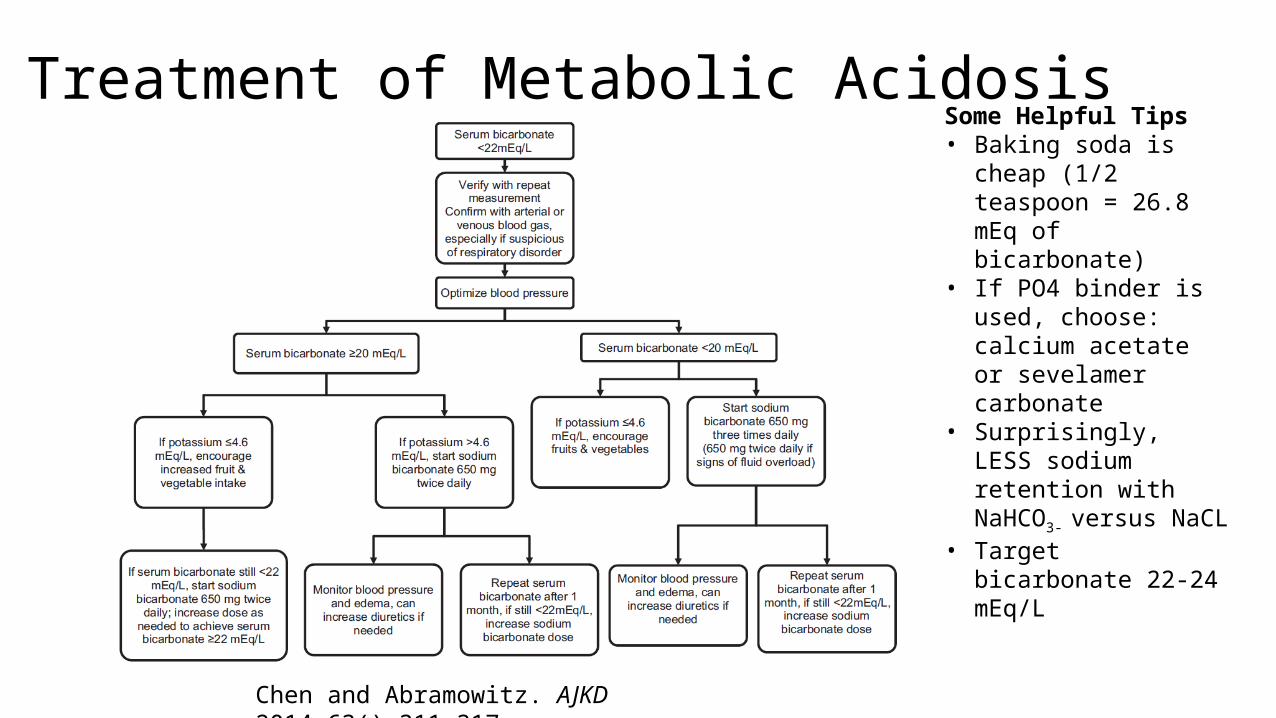
Treatment of Metabolic AcidosisSome Helpful Tips• Baking soda is cheap (1/2
teaspoon = 26.8 mEq of bicarbonate)
• If PO4 binder is used, choose: calcium acetate or sevelamer carbonate
• Surprisingly, LESS sodium retention with NaHCO3-
versus NaCL• Target bicarbonate 22-24
mEq/L
Chen and Abramowitz. AJKD 2014;63():311-317
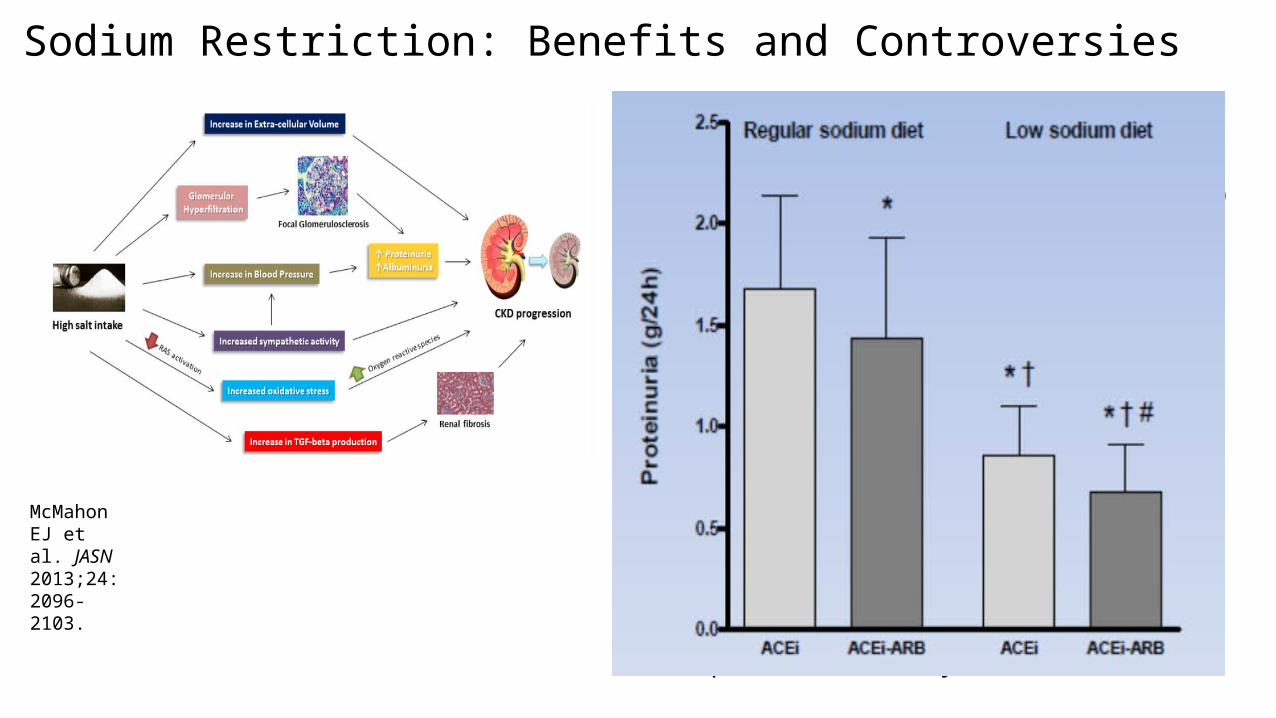
Sodium Restriction: Benefits and Controversies• Benefits
• Reduction in SBP (~ 10 mmHg)• Helpful in resistant HTN
• Reduction in proteinuria (≥ 300 mg/day)• Especially if > 1 gram/day• Control of sodium excess improves the response to
RAAS blockade in CKD -- > ↓ proteinuria• Reduction in progression of CKD• Decrease in mortality (all-cause, ~ 28%)
• Risks• ↑ in plasma renin, aldosterone, adrenaline and
cholesterol• ↑ risk of progression to ESRD• ↑ NT-proBNP• May be augmented by very low sodium diets (< 1.5
grams/day)
• Safe suggestion: 2300 mg/day ≈ 1 teaspoonful salt/day
McMahon EJ et al. JASN 2013;24:2096-2103.
Crash Test Dummies Gain Weight to Save Lives!
Minimum Amount of PA for Reduced Mortality and Extended Life Expectancy
Largest health gains occur within the 1st 15-29 min/day in inactive people
Minimum Amount of PA and Benefits• 15 minutes/day or 90 minutes/week (6
days/week) of moderate-intensity exercise)
• Reduction in all-cause mortality by 14%
• Reduction in cancer mortality by 10%• Reduction in mortality from CVD by
20%• 3 year longer life expectancy
Wen CP et al. Lancet 2011;378:1244-1253.
• Physical Activity Guidelines for Americans• 150 minutes/ week or more of moderate-
intensity aerobic PA or 75 minutes/ week of vigorous-intensity aerobic PA or a combination of moderate- and vigorous-intensity aerobic activity
• Episodes of at least 10 minutes, spread throughout the week
• For additional and more extensive health benefits, adults should increase their aerobic activity to 300 minutes/week of moderate-intensity or 150 minutes/ week of vigorous-intensity activity
• Adults should do muscle-strengthening activities at moderate or high intensity involving ALL muscle groups on 2 or more days a week
• Excess sitting harms lean and obese alike
CDC Guidelines December 2011
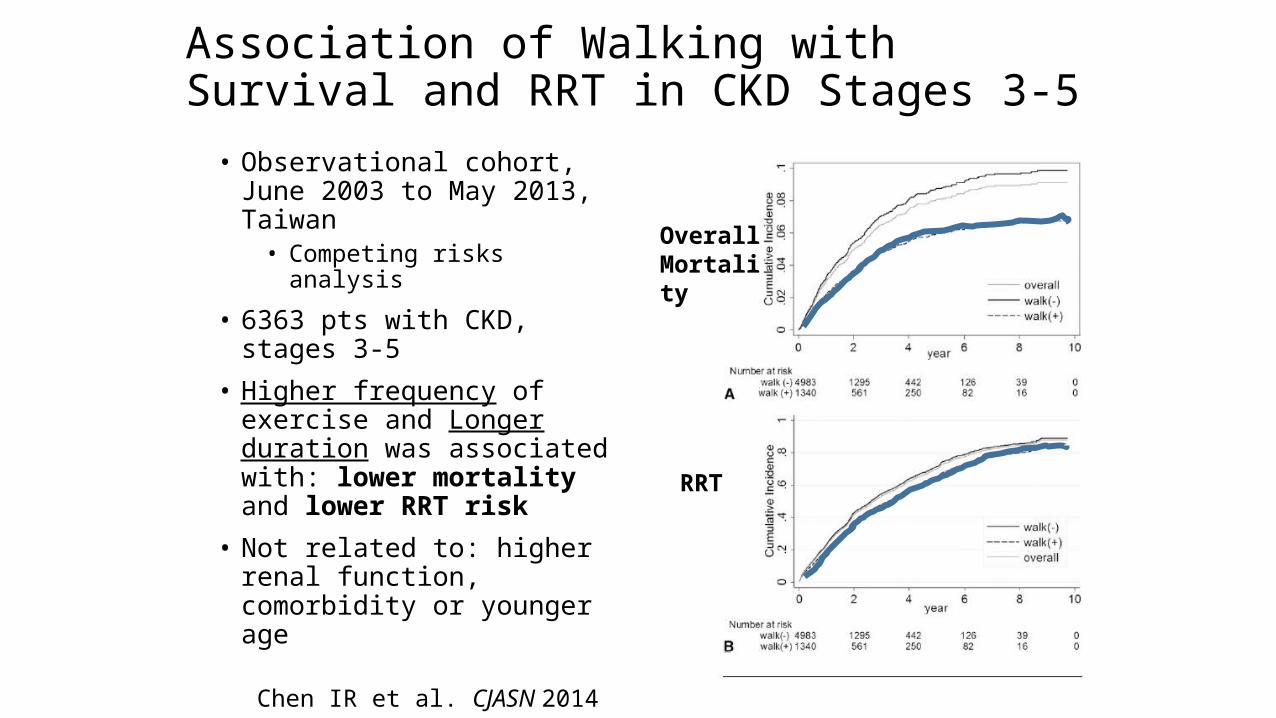
Association of Walking with Survival and RRT in CKD Stages 3-5
• Observational cohort, June 2003 to May 2013, Taiwan
• Competing risks analysis
• 6363 pts with CKD, stages 3-5
• Higher frequency of exercise and Longer duration was associated with: lower mortality and lower RRT risk
• Not related to: higher renal function, comorbidity or younger age
Chen IR et al. CJASN 2014
Overall Mortality
RRT
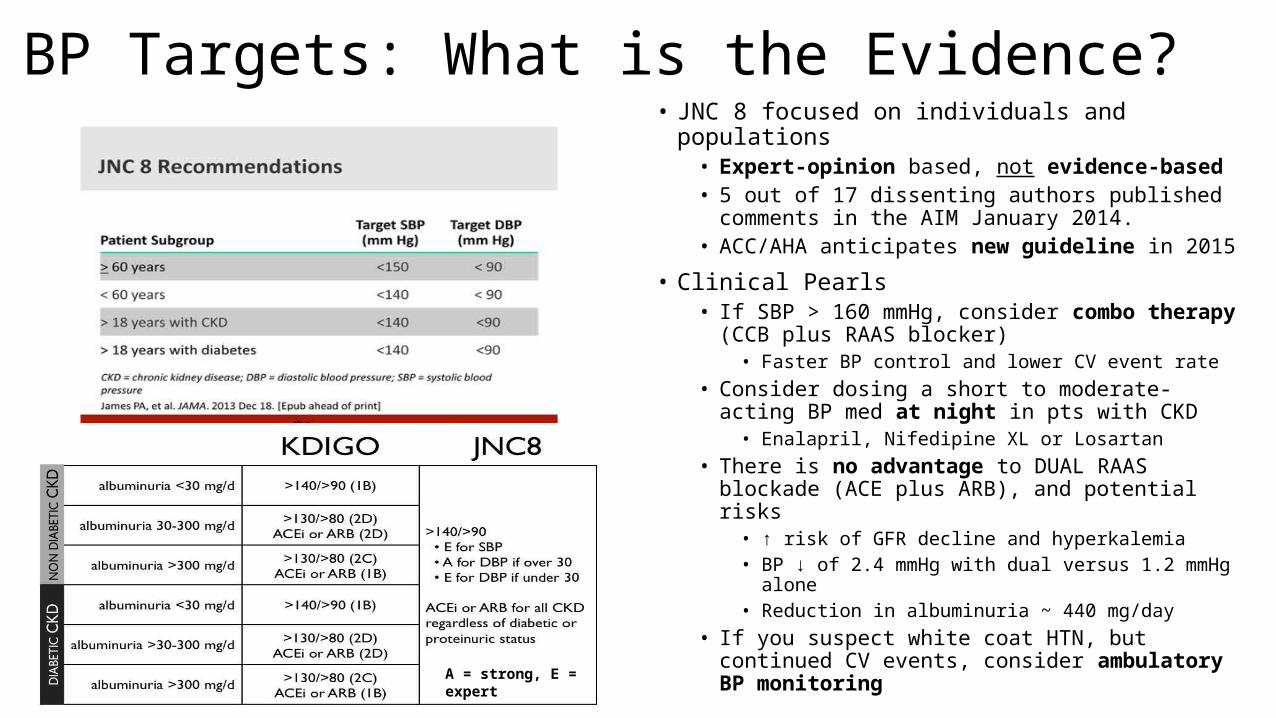
BP Targets: What is the Evidence?• JNC 8 focused on individuals and populations
• Expert-opinion based, not evidence-based• 5 out of 17 dissenting authors published comments
in the AIM January 2014.• ACC/AHA anticipates new guideline in 2015
• Clinical Pearls• If SBP > 160 mmHg, consider combo therapy (CCB
plus RAAS blocker)• Faster BP control and lower CV event rate
• Consider dosing a short to moderate-acting BP med at night in pts with CKD
• Enalapril, Nifedipine XL or Losartan• There is no advantage to DUAL RAAS blockade (ACE
plus ARB), and potential risks• ↑ risk of GFR decline and hyperkalemia• BP ↓ of 2.4 mmHg with dual versus 1.2 mmHg alone• Reduction in albuminuria ~ 440 mg/day
• If you suspect white coat HTN, but continued CV events, consider ambulatory BP monitoring
A = strong, E = expert
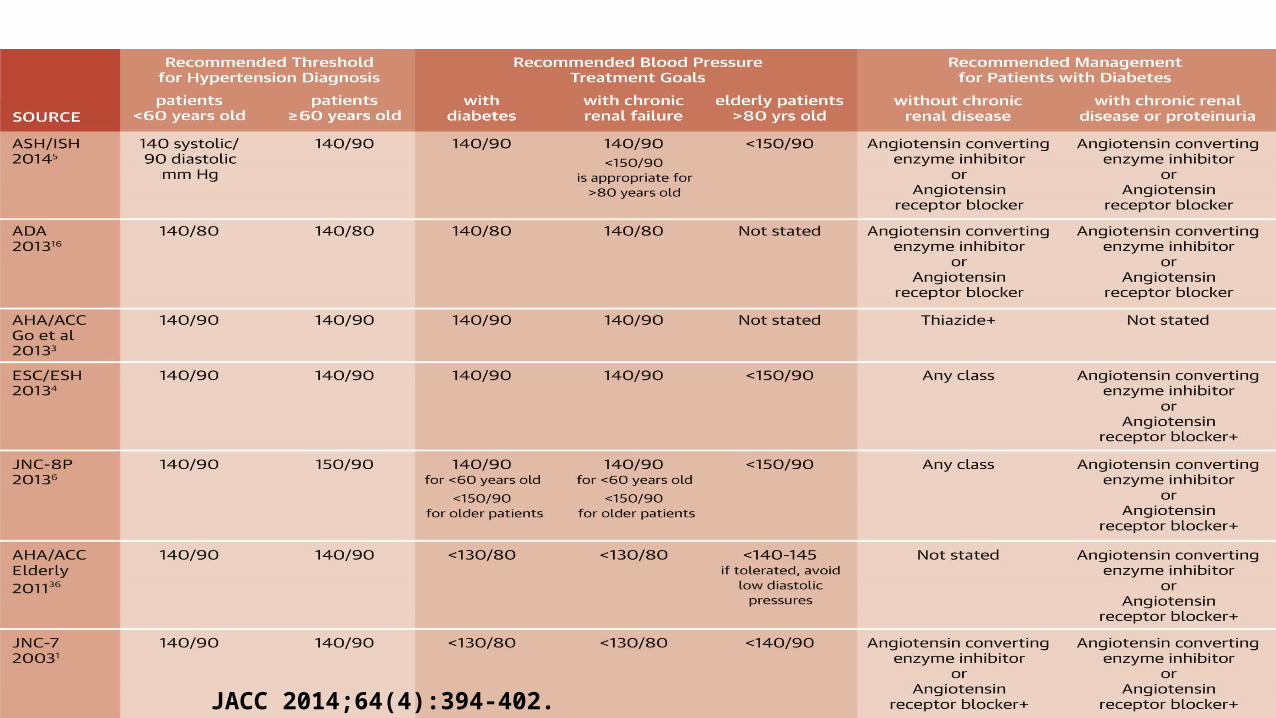
JACC 2014;64(4):394-402.

Recent HTN Trials
Bakris GL. Lancet 2010;375:1173-1181
11,056 pts, randomized + double blindedSecondary Endpt:-Progression of CKD, doubling SCr , need for RRT or ESRD
Obesity Paradox
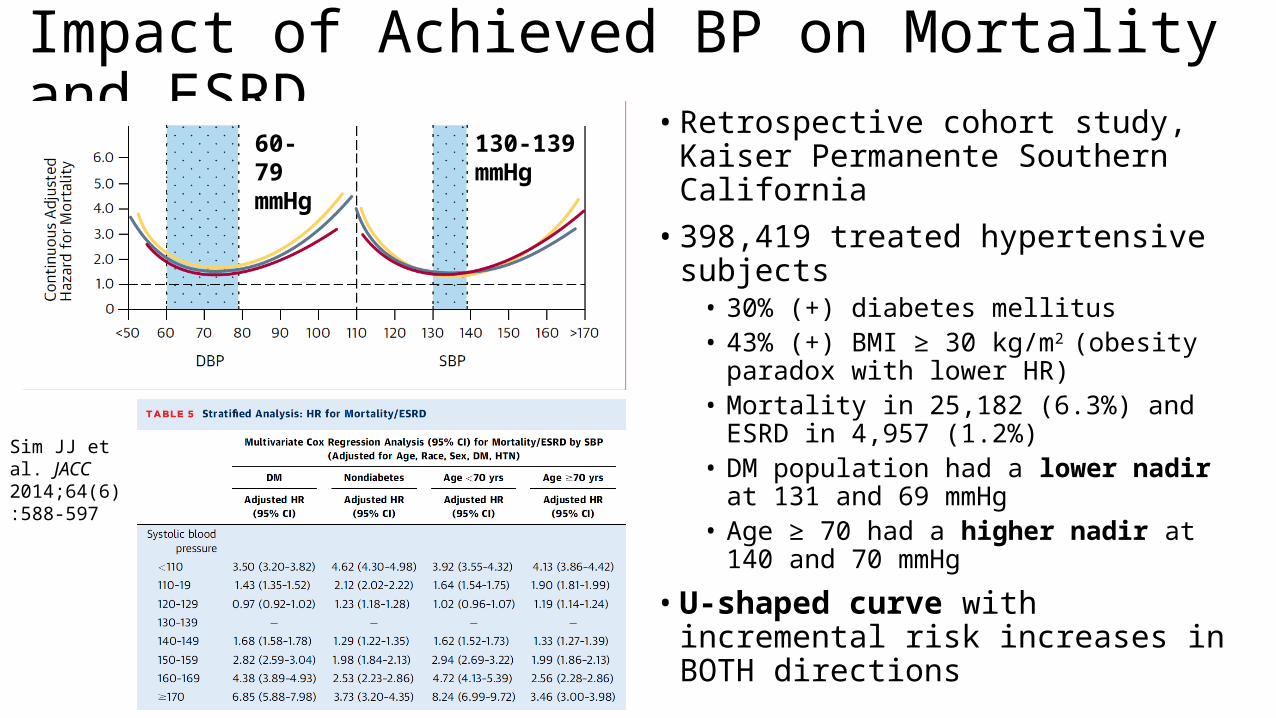
Impact of Achieved BP on Mortality and ESRD • Retrospective cohort study, Kaiser
Permanente Southern California• 398,419 treated hypertensive subjects
• 30% (+) diabetes mellitus• 43% (+) BMI ≥ 30 kg/m2 (obesity paradox with
lower HR)• Mortality in 25,182 (6.3%) and ESRD in 4,957
(1.2%)• DM population had a lower nadir at 131 and 69
mmHg• Age ≥ 70 had a higher nadir at 140 and 70
mmHg
• U-shaped curve with incremental risk increases in BOTH directions
60-79 mmHg
130-139 mmHg
Sim JJ et al. JACC 2014;64(6):588-597

What Medications to Use?
ASH Guidelines December 2013
Obesity Paradox
Chlorthalidone or Indapamide
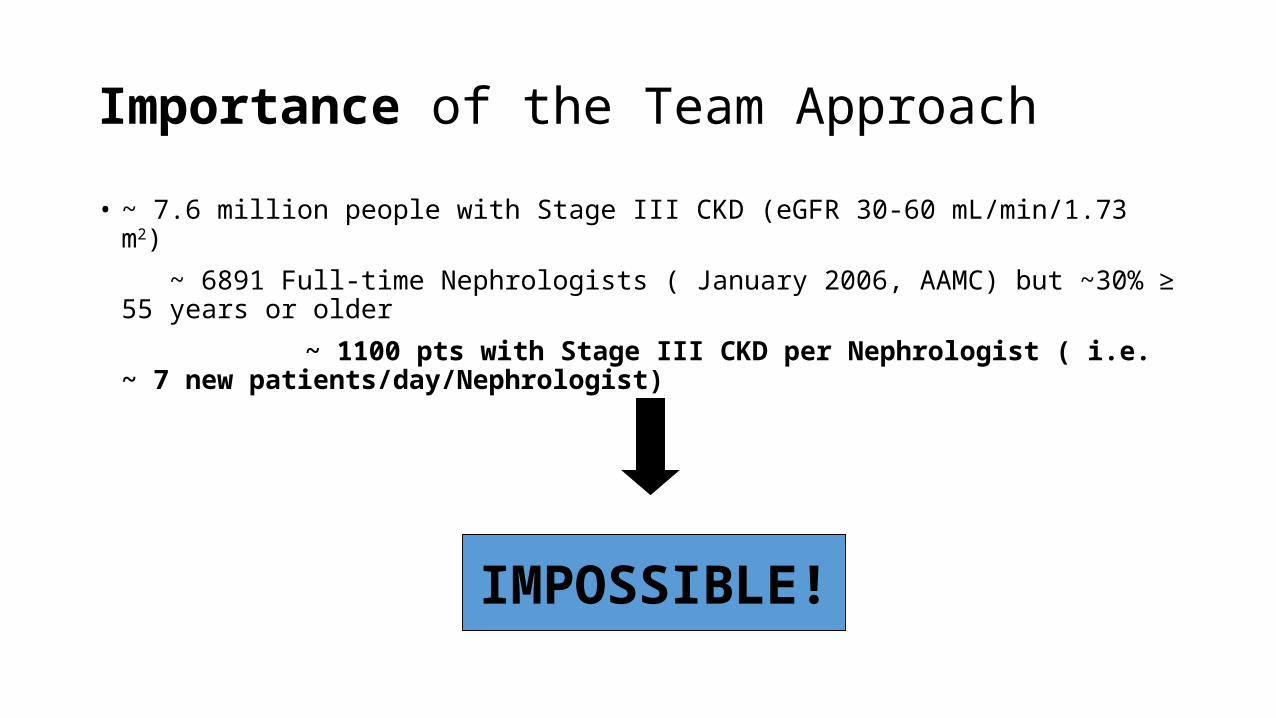
Importance of the Team Approach
• ~ 7.6 million people with Stage III CKD (eGFR 30-60 mL/min/1.73 m2)
~ 6891 Full-time Nephrologists ( January 2006, AAMC) but ~30% ≥ 55 years or older
~ 1100 pts with Stage III CKD per Nephrologist ( i.e. ~ 7 new patients/day/Nephrologist)
IMPOSSIBLE!
Take Home Points• Though GFR equations continue to evolve, they are helpful in predicting CKD complications and
provide prognostication.• CKD-EPI is the preferred equation due to less bias.• Newer markers such as cystatin C may provide advantages over creatinine-based assays.
• eGFR ≤ 45 mL/min/1.73 m2 is an important decision point.• Every individual likely has a unique GFR trajectory.• The addition of proteinuria (≥ 1 gram/day) or albuminuria (≥ 300 mg/gm creatinine) worsens every stage
of GFR.
• Metabolic acidosis (serum bicarbonate < 22 mEq/L) should be treated and may slow progression in CKD.
• The degree of salt restriction remains controversial, though moderate restriction (~ 2300 mg/day) may assist with proteinuria reduction and augment RAAS blockade.
• Inactivity has important associations (↑ CV morbidity/mortality, ↑ risk of malignancy as well as increases the risk of progression to RRT and death). Inactivity is more deadly than obesity.
• BP goals continue to be moving targets and hopefully further studies will elucidate the optimal values.