resq trial refresher training: the resq trial in whatcom county prepared by janice lapsansky january...
TRANSCRIPT
Refresher Training:The ResQ TrialResQ Trial in Whatcom County
Prepared by
Janice LapsanskyJanuary 2008
Topics
Adult CPR1
2 ResQ Trial Refresher
Click on this icon to reveal the answers to test preview questions
Click on this icon to reveal the answers to test preview questions
Learning Objectives
This is an online EMS continuing education module for EMS providers in Whatcom County. After completing this course you will be able to:
1. Briefly describe the study objectives and your role in the ResQ Trial.
2. List the patient inclusion/exclusion criteria.3. State the purpose of the randomization calendar and the
method your agency uses to insure the calendar is followed correctly each week.
4. Describe the correct performance of standard CPR (with the modified hand position) and use of the AED according to current AHA guidelines.
5. Describe the correct use of the ResQ POD with standard chest compressions during CPR.
6. Describe the correct performance of active compression-decompression (ACD-CPR) with the ResQ Pump and ResQ POD.
Terms
ACD-CPR – active compression-decompression cardiopulmonary resuscitation
AED – automated external defibrillator
cardiac arrest – abnormal heart activity insufficient to produce a pulse
chest decompression – chest expansion as a result of natural recoil or ResQ Pump use
compression to ventilation ratio – alternating sets of 30 chest compressions and 2 ventilations during adult CPR with an unsecured airway (BVM ventilations)
DNR – do not resuscitate
ETCO2 – carbon dioxide content of air measured at the end of exhalation
impedence threshold device (ITD) – valve that prevents air from entering lungs during the decompression phase of CPR; aka ResQ POD
inclusion/exclusion criteria – decision list to determine whether a victim of cardiac arrest meets the qualifications to be enrolled in the ResQ Trial
secure airway – a cuffed airway, such as provided by an endotracheal (ET) tube or Combi-tube, and held in place by a tube holder
study randomization – pre-determined schedule of CPR method, strictly followed by controlling the availability of study devices on rescue vehicles

Adult CPR1
ABC’s
• Open the airway• Check for breathing
• Look, listen, and feel
• Check for circulation
Opening the Airway1
head-tilt / chin-lift
head-tilt / chin-lift
• For all victims unless cervical spine injury is suspected.
Opening the Airway1
• Without head extension where cervical spine injury is suspected.
head-tilt / chin-lift
head-tilt / chin-lift
jaw thrustjaw thrust
If the jaw thrust does not adequately open the airway use the head-tilt,
chin-lift, because airway takes priority.
If the jaw thrust does not adequately open the airway use the head-tilt,
chin-lift, because airway takes priority.
Quality CPR w/ BVM
• The compression to ventilation ratio is 30:2• The ventilation rate during CPR is 1 breath
every 6-8 seconds Is this faster or slower than
the rate of rescue breathing?
• Deliver each rescue breath quickly (1 sec) with visible chest rise
• Provide immediate chest compressions
1
AHA says:
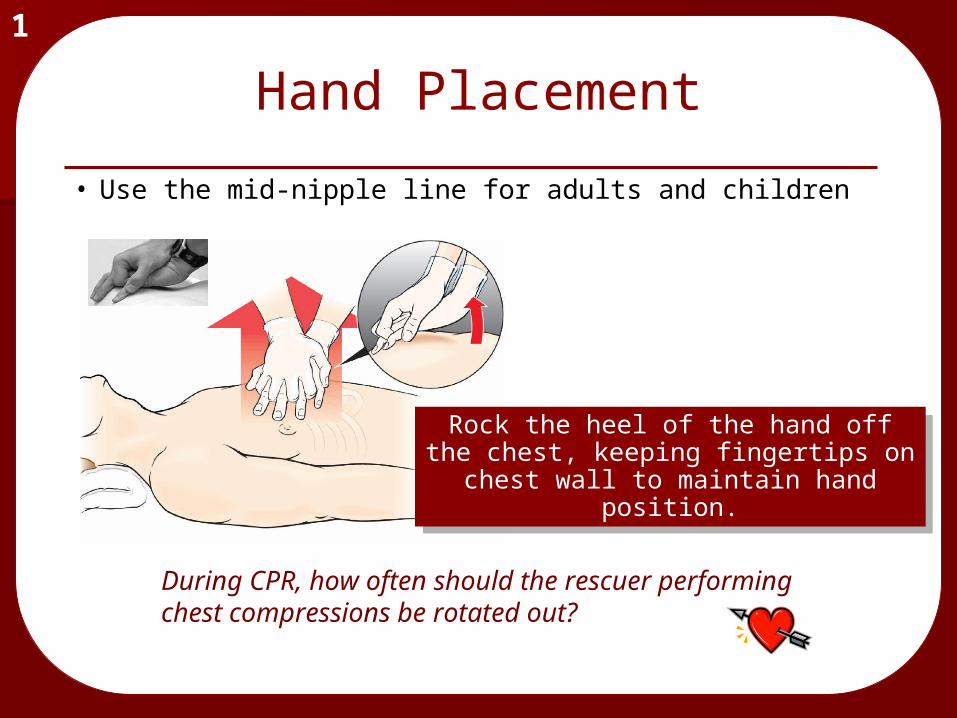
• Use the mid-nipple line for adults and children
1
Hand Placement
During CPR, how often should the rescuer performing chest compressions be rotated out?
Rock the heel of the hand off the chest, keeping fingertips on chest
wall to maintain hand position.
Rock the heel of the hand off the chest, keeping fingertips on chest
wall to maintain hand position.
AED & Defibrillation
Highlights of the 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Currents in Emergency Cardiovascular Care. Vol. 16 No. 4, Winter, 2005-2006
1
Cardiac arrest not witnessed by EMS:
• Perform 5 cycles or 2 minutes of CPR before analyzing rhythm
When should the defib pads be applied to the patient?
1
No stacked shocks
No pulse check after shock
Single shock will be followed immediately by 2 minutes of CPR, then pulse check, and re-analyze if necessary
Defibrillation
These measures limit the “no flow time”. Why is it important to reduce the amount of time when compressions are not performed?
Defibrillation
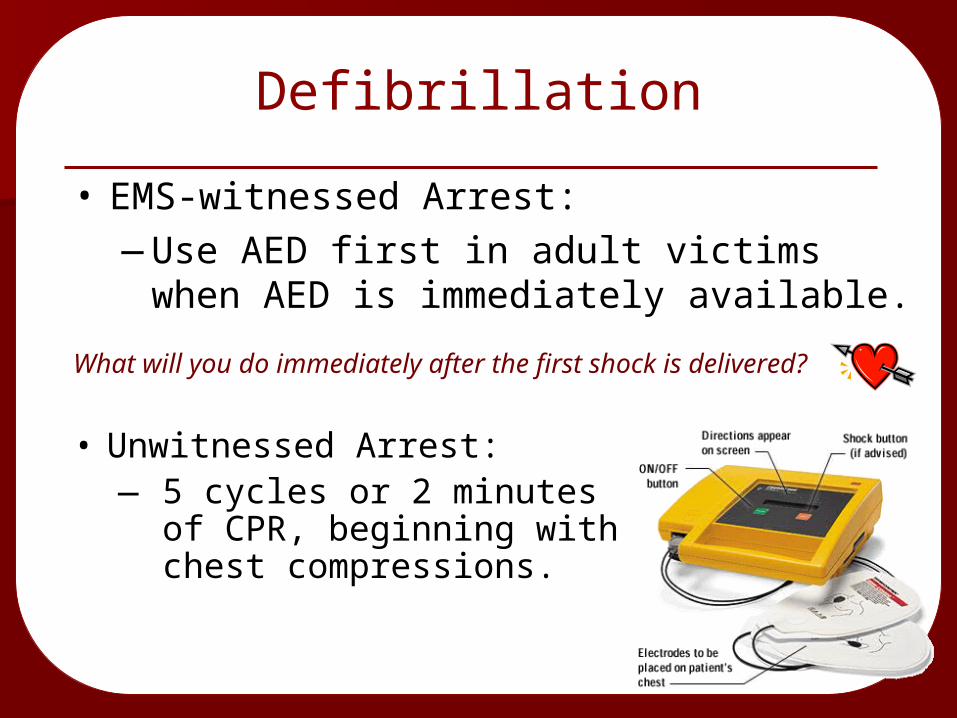
• EMS-witnessed Arrest: —Use AED first in adult victims when AED
is immediately available.
• Unwitnessed Arrest: — 5 cycles or 2 minutes of
CPR, beginning with chest compressions.
What will you do immediately after the first shock is delivered?
CPR and Rescue Breathing with a Bag-Valve Mask (BVM)
1
• 30:2 compression to ventilation ratio• Hold tight, two-handed face-to-mask
seal• Count compressions out loud
(“1 and 2 and 3 and…”)• Pause after 30 compressions for
delivery of 2 rescue breaths
Because each rescue breath is given more quickly, will you also give a larger volume of air with each breath?

Rescue Breathing During CPRwith an Advanced Airway
1
• ET tube or Combi-tube• Ventilations at 8-10 times per minute,
or approximately every 6-8 seconds• For all victims in cardiac arrest
Should you pause chest compressions
to deliver breaths after tube placement?

Quality of Chest Compressions1
• Push hard, push fast• Adult compressions must
be 1 ½ - 2 inches deep• Standard rate is 100/min • Do not interrupt chest
compressions for longer than 10 seconds
How will you insure that the heart fills to the greatest extent possible between chest compressions?
CPR Success
• Provide effective chest compressions (and decompressions) with appropriate timing
• Limit no flow time (NFT) – i.e. limit pauses in chest compressions
• Manage the airway & apply ventilations correctly (DO NOT hyperventilate!)
• Use defibrillation appropriately
1
How often should rescuers practice their CPR skills?

ResQ Trial Overview2
ResQ Trial Research Question
Is it possible to provide more effective CPR with one or both of these tools?
2
ResQ Trial Research Question
Your participation in the trial will provide critical information about EMS-provided CPR for adult victims of cardiac arrest.
The ResQ Trial will analyze:• Return of pulse, for any duration• Patient survival to the emergency department• Patient survival to hospital discharge• Neurologic health (quality of life) after
discharge
2
What does AHA say is the most important factor in overall patient outcome following cardiac arrest?
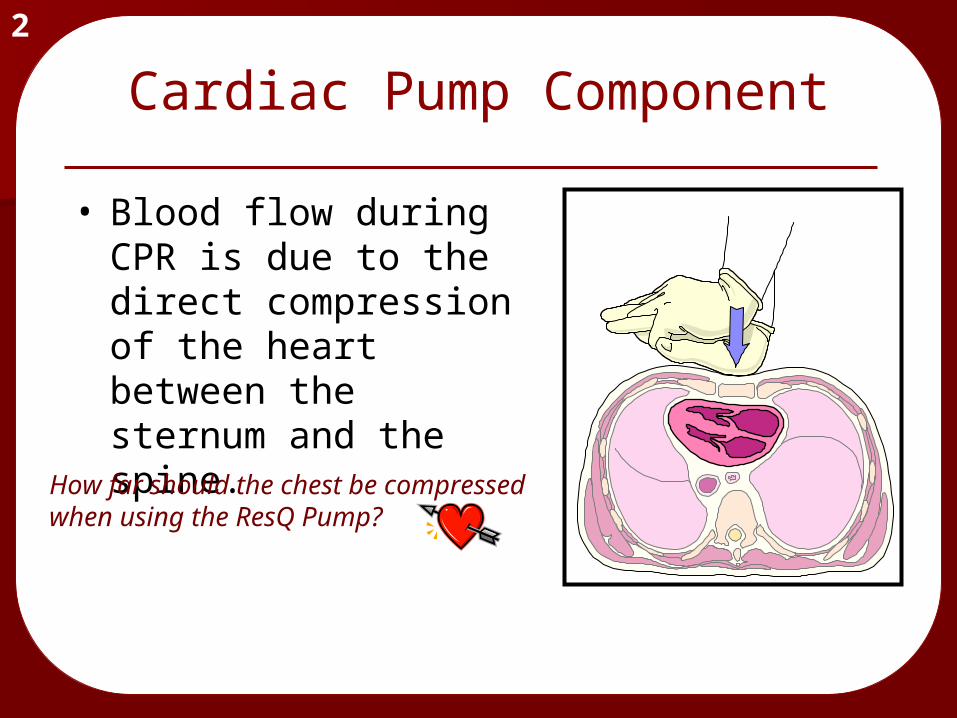
• Blood flow during CPR is due to the direct compression of the heart between the sternum and the spine.
2
Cardiac Pump Component
How far should the chest be compressed when using the ResQ Pump?
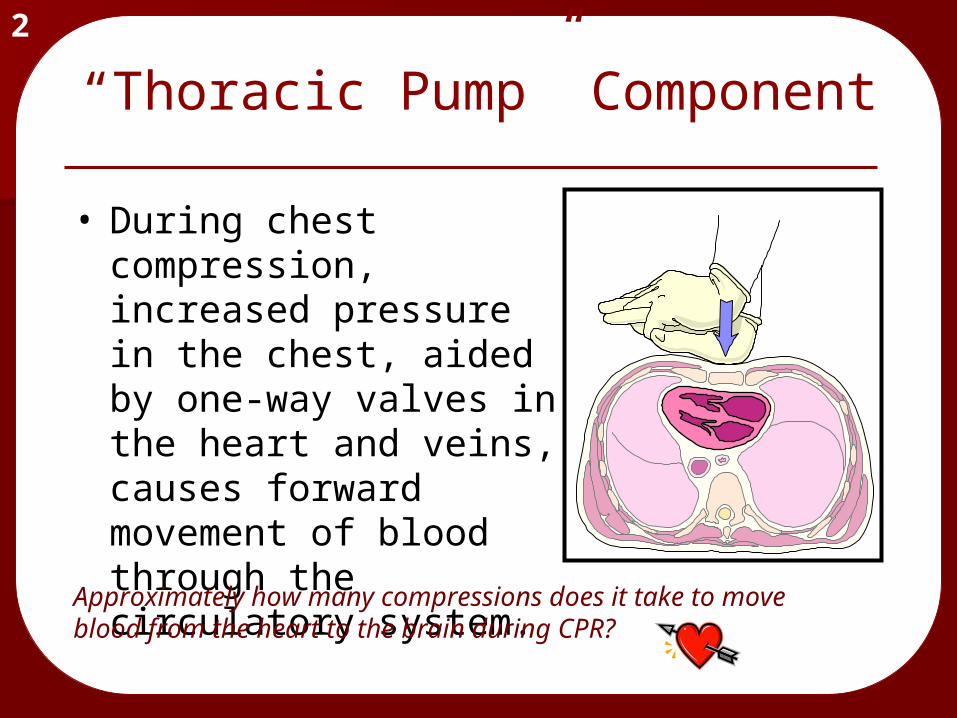
• During chest compression, increased pressure in the chest, aided by one-way valves in the heart and veins, causes forward movement of blood through the circulatory system.
2
“Thoracic Pump” Component
Approximately how many compressions does it take to move blood from the heart to the brain during CPR?
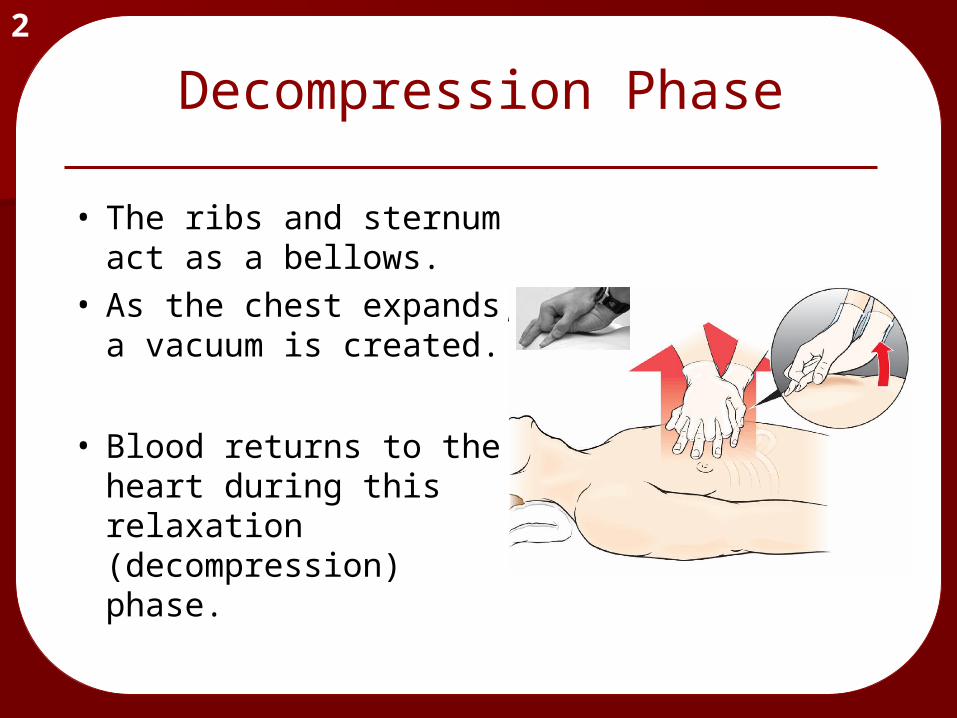
Decompression Phase2
• The ribs and sternum act as a bellows.
• As the chest expands, a vacuum is created.
• Blood returns to the heart during this relaxation (decompression) phase.
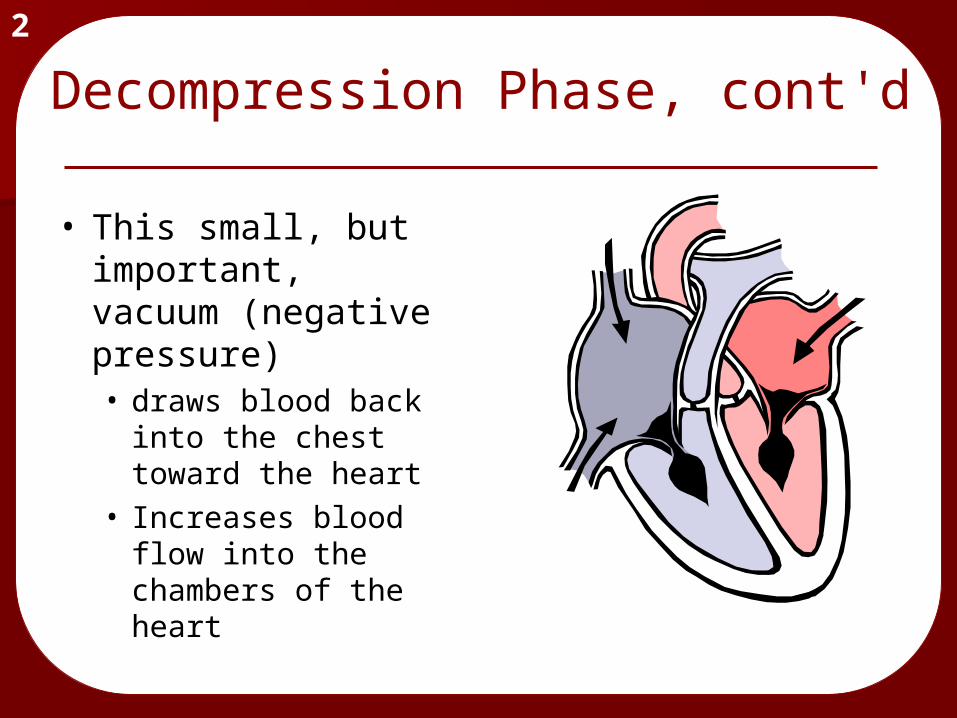
Decompression Phase, cont'd2
• This small, but important, vacuum (negative pressure) • draws blood back
into the chest toward the heart
• Increases blood flow into the chambers of the heart

Decompression Phase, cont'd2
• The more blood that returns to the heart (preload)…
…the more that is circulated forward (cardiac output) with the next chest compression.• increases blood flow to the
brain• increases blood flow through
the arteries of the heart

“Allowing complete chest recoil after each compression allows blood to return to the heart to refill the heart. If the chest is not allowed to
recoil/re-expand, there will be less venous return
to the heart, and filling of the heart is reduced. As a result, cardiac output produced by subsequent chest compressions will be
reduced.”Highlights of the 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.Currents in Emergency Cardiovascular Care. Vol. 16 No. 4, Winter, 2005-2006
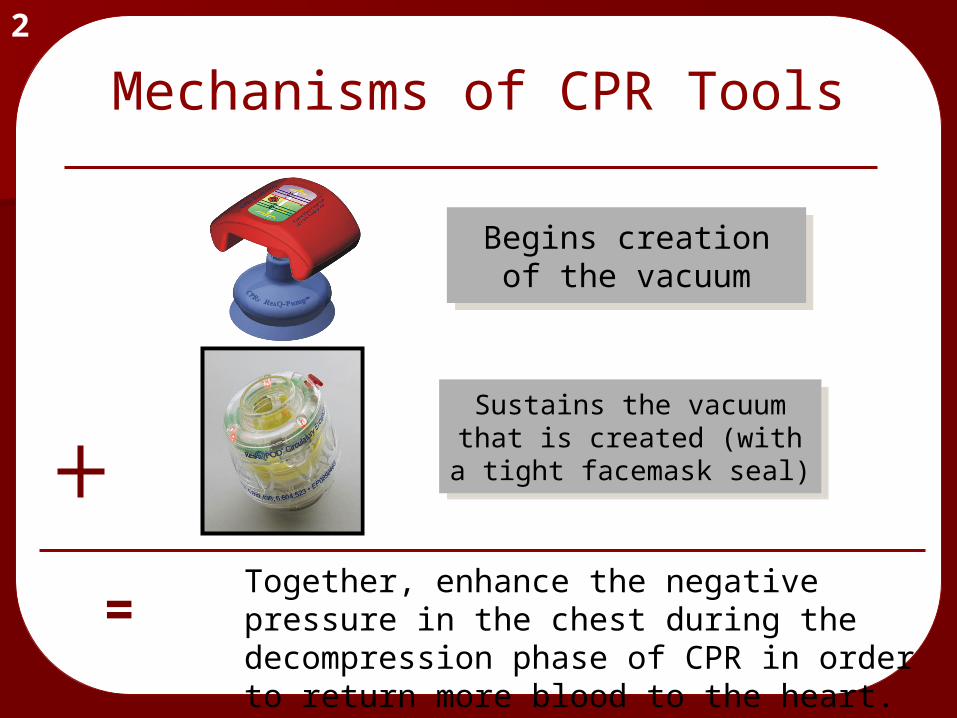
Mechanisms of CPR Tools2
Begins creation of the vacuum
Begins creation of the vacuum
Sustains the vacuum that is created (with a tight facemask seal)
Sustains the vacuum that is created (with a tight facemask seal)
=Together, enhance the negative pressure in the chest during the decompression phase of CPR in order to return more blood to the heart.
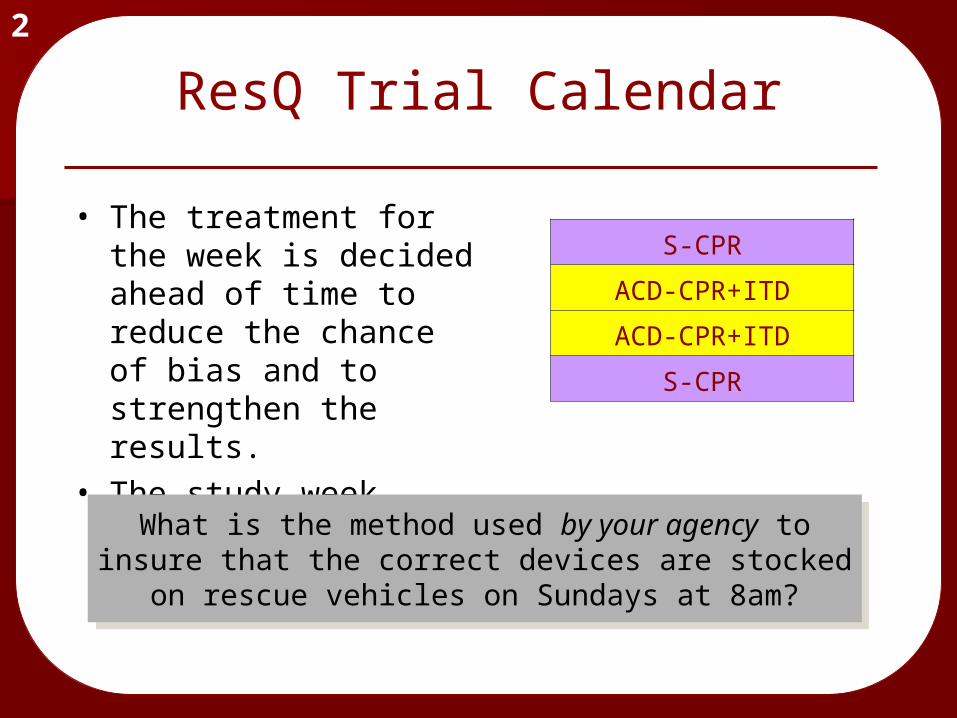
ResQ Trial Calendar
• The treatment for the week is decided ahead of time to reduce the chance of bias and to strengthen the results.
• The study week begins on Sunday at 8am.
2
What is the method used by your agency to insure that the correct devices are stocked on
rescue vehicles on Sundays at 8am?
What is the method used by your agency to insure that the correct devices are stocked on
rescue vehicles on Sundays at 8am?
S-CPR
ACD-CPR+ITD
ACD-CPR+ITD
S-CPR
ResQ Trial Calendar
• Patients will be analyzed according to the treatment that they should have received, not what they actually got.— Follow the schedule exactly— If a “yellow” week, use the ResQ POD pre-loaded
on the facemask & ResQ Pump immediately, or within the first 2 minutes of CPR— Do not delay for intubation or other procedures
— Report any problems during the hotline call
2
Where can you find the phone number for the ResQ Trial hotline?
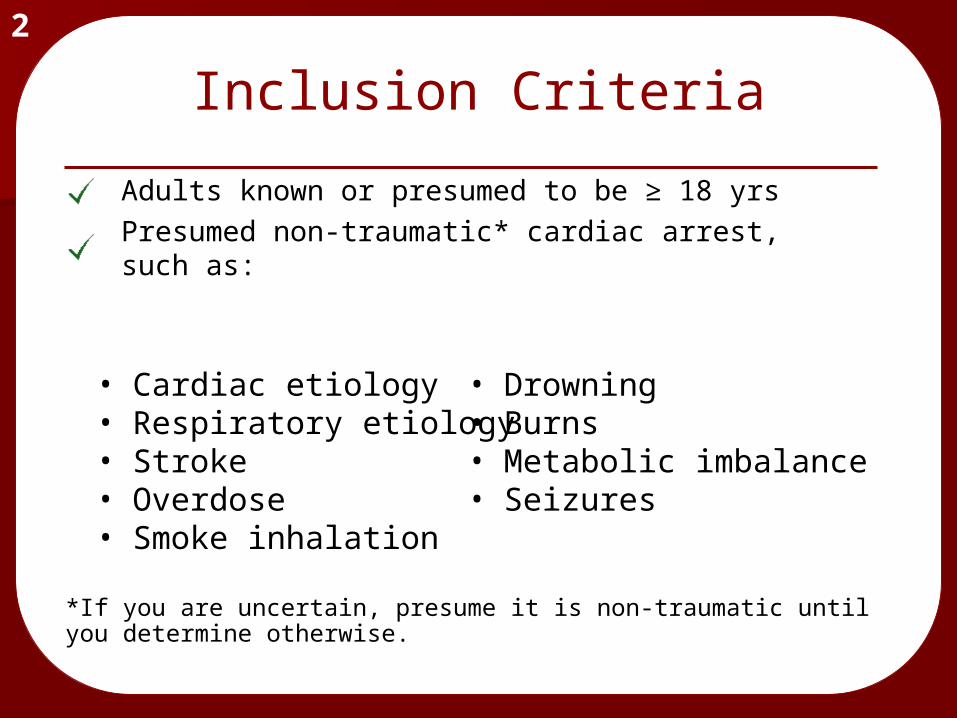
Inclusion Criteria
*If you are uncertain, presume it is non-traumatic until you determine otherwise.
2
• Cardiac etiology• Respiratory etiology• Stroke• Overdose• Smoke inhalation
Adults known or presumed to be ≥ 18 yrsPresumed non-traumatic* cardiac arrest, such as:
• Drowning• Burns• Metabolic imbalance• Seizures
Exclusion Criteria
If the patient meets ANY of the exclusion criteria, perform Standard CPR.
2
Known or presumed < 18 yearsObvious or likely traumatic etiology
Penetrating or blunt trauma
Pre-existing DNR ordersObvious signs of clinical death (DOA)Family members who request exclusionFor ACD-CPR+ITD arm: recent sternotomy (wound not appearing completely healed or, if known, < 6 months)
Study Protocol—3100 patients
Cardiac arrest
Cardiac arrest
outcome
2
Study Protocol—3100 patients
Cardiac arrest
Cardiac arrest
S-CPRACD-CPR + ITD
S-CPRACD-CPR + ITD
outcome
• Randomized by week
2

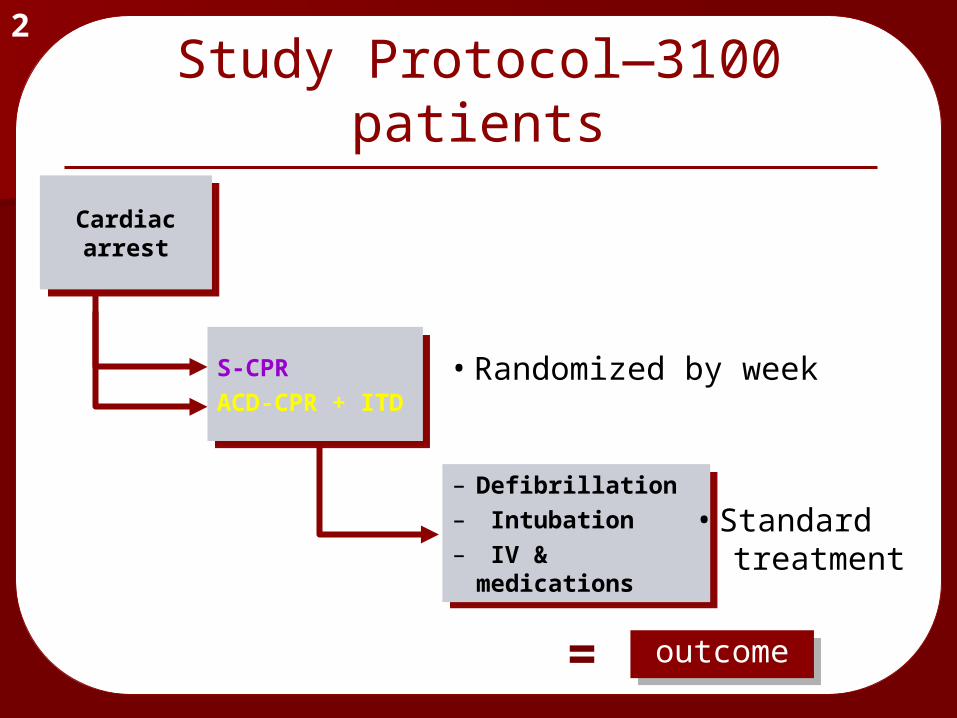
Study Protocol—3100 patients
Cardiac arrest
Cardiac arrest
S-CPRACD-CPR + ITD
S-CPRACD-CPR + ITD
– Defibrillation– Intubation– IV &
medications
– Defibrillation– Intubation– IV &
medications
outcome
• Standard treatment
2
• Randomized by week
Study Protocol—3100 patients
Cardiac arrest
Cardiac arrest
S-CPRACD-CPR + ITD
S-CPRACD-CPR + ITD
– Defibrillation– Intubation– IV &
medications
– Defibrillation– Intubation– IV &
medications
=
outcome
outcomeoutcome
2
• Standard treatment
• Randomized by week
• Follow the correct compression rates:— S-CPR: 100/min— ResQPump: 80/min
• Allow chest to completely recoil• Do not hyperventilate!• Facemask: 30:2 compressions to
vents• Advanced airway: 8-10/min
2
CPR Success
If a pulse cannot be restored, how long should resuscitative efforts last at the scene?

Run Follow-up
• Complete patient care record accurately:— Attempt to record times (scribe sheet available)
—CPR starts/stops—time of Pump and POD use—time of intubation, etc.
• Call the research hotline 24/7— 1-866-640-2832— for ALL ARRESTS; regardless of whether the
patient was entered into the study and regardless of whether resuscitation was attempted (DOAs).
2
Run Follow-up, continued
• ResQPOD: place sticker on run report— Discard used ResQPOD, unless there
were problems— Re-stock with a new ResQPOD from
your agency’s supply.(do not restock from the medic rig)
• ResQPump: record number on run report— clean ResQPump and return to service.
2
Standard CPR—Facemask Only2
• Airway not secured (facemask)— Compress @ 100/min — Pause for breaths — Compression to ventilation ratio 30:2
Is this the correct compression rate?
Standard CPR—Advanced Airway
2
• Airway secured (ET or Combi-tube)— Continuous compressions @ 100/min— Do not pause for breaths— Ventilate at 10/min (once every 10
compressions)
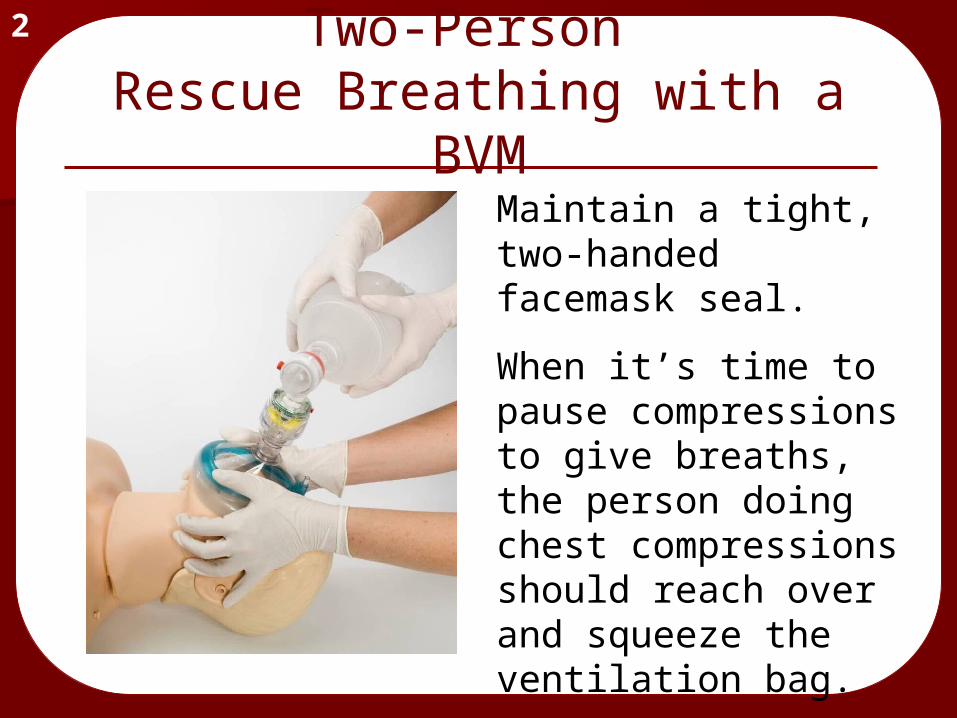
2Two-Person
Rescue Breathing with a BVM
Maintain a tight, two-handed facemask seal.
When it’s time to pause compressions to give breaths, the person doing chest compressions should reach over and squeeze the ventilation bag.
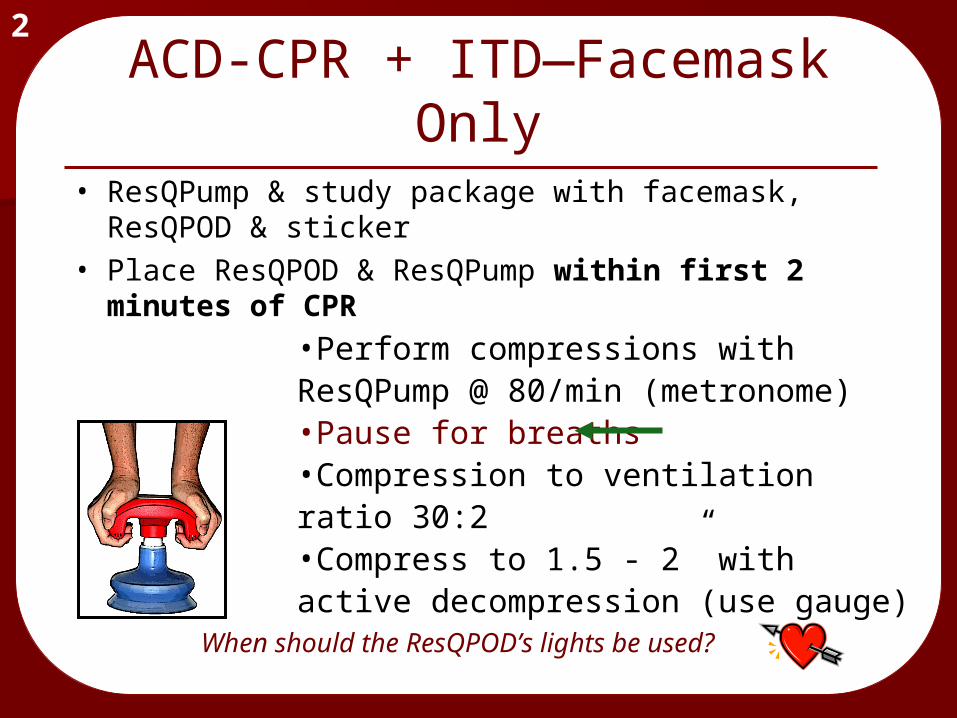
•Perform compressions with ResQPump @ 80/min (metronome) •Pause for breaths•Compression to ventilation ratio 30:2•Compress to 1.5 - 2” with active decompression (use gauge)
2ACD-CPR + ITD—Facemask
Only• ResQPump & study package with facemask,
ResQPOD & sticker• Place ResQPOD & ResQPump within first 2
minutes of CPR
When should the ResQPOD’s lights be used?
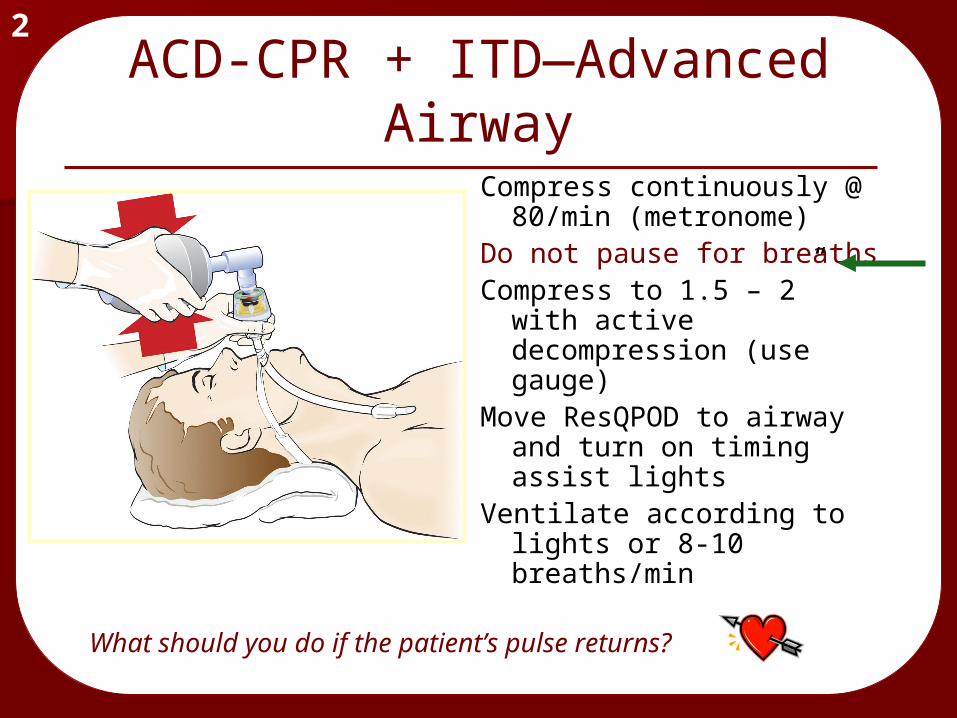
2ACD-CPR + ITD—Advanced
AirwayCompress continuously @
80/min (metronome)Do not pause for breathsCompress to 1.5 – 2” with
active decompression (use gauge)
Move ResQPOD to airway and turn on timing assist lights
Ventilate according to lights or 8-10 breaths/min
What should you do if the patient’s pulse returns?
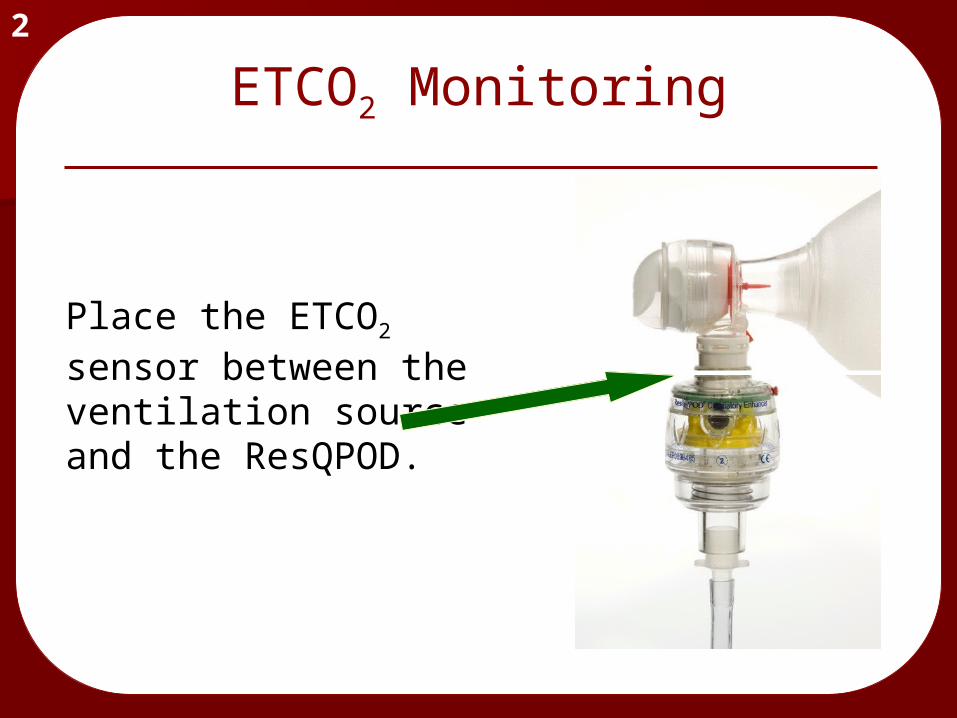
ETCO2 Monitoring
Place the ETCO2 sensor between the ventilation source and the ResQPOD.
2
Troubleshooting2
• Timing assist light function is independent of inspiratory impedance valve feature.
• If timing assist lights fail to operate or appear to blink at a rate different than 8-10/minute, disregard the lights, continue using the ResQPOD, and ventilate the patient at 10 breaths/minute.
Troubleshooting, cont'd2
Discontinue ResQPOD if:• Chest does not rise
with ventilation• Device appears to
malfunction in any way
• The POD fills with fluid twice (the airway may be suctioned as needed)
• Clear fluids or secretions from the ResQPOD by removing it from the airway adjunct and blowing out debris using the ventilation source.
• Discontinue use if the device cannot be cleared.
• Discontinue use if the ResQPOD fills with fluid more than once.
2
ResQPOD Fills With Fluid
• You may replace POD with new one (preferred), or discontinue completely.
• Suctioning of the airway (w/o fluid in POD) does not require that the POD be discontinued
• If you have any problems with the ResQPOD, save in a red bag and return to researcher coordinator.
2ResQPOD Fills With Fluid,
cont'd

ACD-CPR Compression
• Same objective as in standard CPR
• 1 ½ - 2” in depth (65 - 90 lbs)
• 80 compressions/minute
• Body position is critical to avoid fatigue
• Do not straddle patient• Rotate compressor
role every 2 minutes.
2
How long should CPR be performed on a patient with an unwitnessed cardiac arrest before analyzing with the AED?
2
• Suction problems in 10-15% of patients— Reposition, shave, or dry off chest— Continue use, unless distracting
• May interfere with AP patch placement— Move patches
• Requires 25% more rescuer energy— Rotate every 2 minutes
Troubleshooting ACD-CPR
When using the ResQPump, how hard should a
rescuer pull up (decompress the chest)?
2
• Rib fractures— Check placement and continue
• Hickey or bruising to chest— Continue
• Discontinue use if device appears to malfunction.
Troubleshooting ACD-CPR, cont'd
Cleaning/Reuse
• Clean cup with soap and water.
• May be cleaned with bleach solution or other disinfectant.
• Check gauge for proper calibration.
2
Untrained Healthcare Providers
2
Do not leave the ResQPOD or ResQPump in the hands of
healthcare providers who have not been trained in their use.
Do not leave the ResQPOD or ResQPump in the hands of
healthcare providers who have not been trained in their use.
Finally…
Give both CPR methods the greatest opportunity to work…
Do the best CPR possible!
Written Test2
Click here to return to the start of thispresentation…or Close this window and click the ResQ Trial exam link on the main course page.
Ventilation During CPR
• The ventilation rate during CPR is 1 breath every 6-8 seconds
This is slower than for rescue breathing alone.
• Rescue breathing (without CPR) is 12 times per minute (every 5 seconds)
back
AHA says…
“Push hard and push fast”• A faster compression rate (that allows
full chest recoil) produces the blood pressure required to send blood to the brain and heart muscle.
• Adequate compression depth before each shock directly affects shock success – deeper compressions lead to more successful shocks
• Resuscitation. 2006; epub, September 16
back
Fatigue Factor
• Change roles every 2 minutes (5 cycles)• Regardless of whether you feel tired!• Switch quickly to avoid interruptions in
CPR
1
back
Apply the AED
• Apply the AED pads as soon as the patient is determined to be without pulse or respirations.
• If the cardiac arrest was not witnessed by EMS (or the downtime is known to be greater than 4 minutes) perform 2 minutes or 5 cycles of CPR before analyzing for a shockable rhythm
back
1
No stacked shocks
No pulse check after shockDo not interrupt CPR for rhythm analysis or defibrillation for long periods of time. During these “no flow times” the brain and heart are not receiving oxygen in the blood. Prolonged no flow times decrease the chance that defib will work!
Appropriate Defibrillation
back
Following each shock
Immediate chest compressions of good quality will supply blood to the heart muscle that will help it
respond better to medications and AED shocks
Immediate chest compressions of good quality will supply blood to the heart muscle that will help it
respond better to medications and AED shocks
back
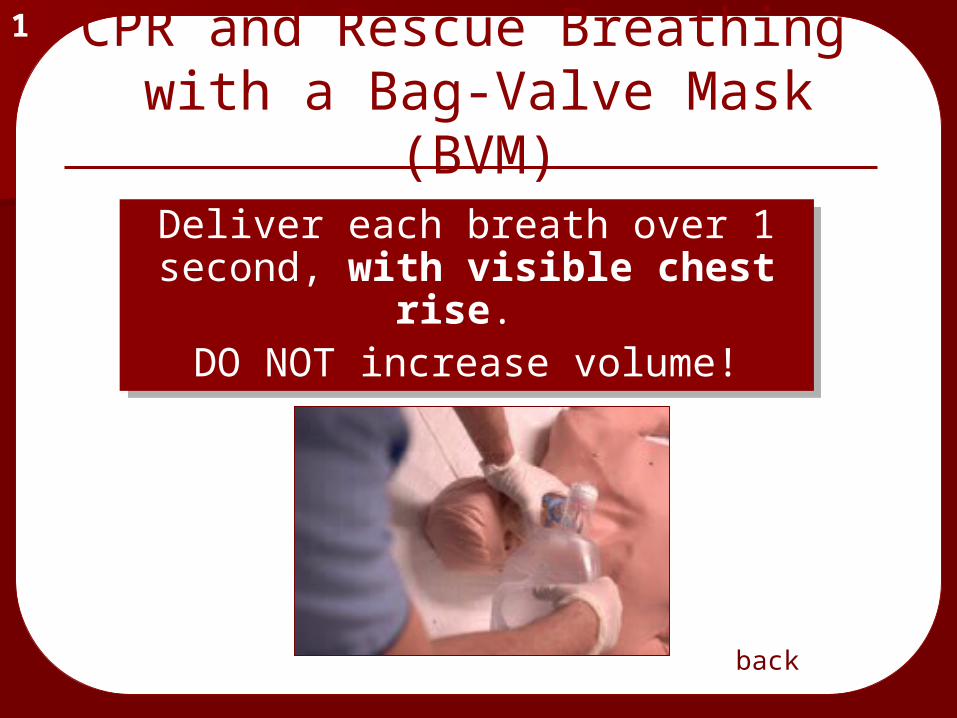
CPR and Rescue Breathing with a Bag-Valve Mask (BVM)
1
Deliver each breath over 1 second, with visible chest
rise. DO NOT increase volume!
Deliver each breath over 1 second, with visible chest
rise. DO NOT increase volume!
back
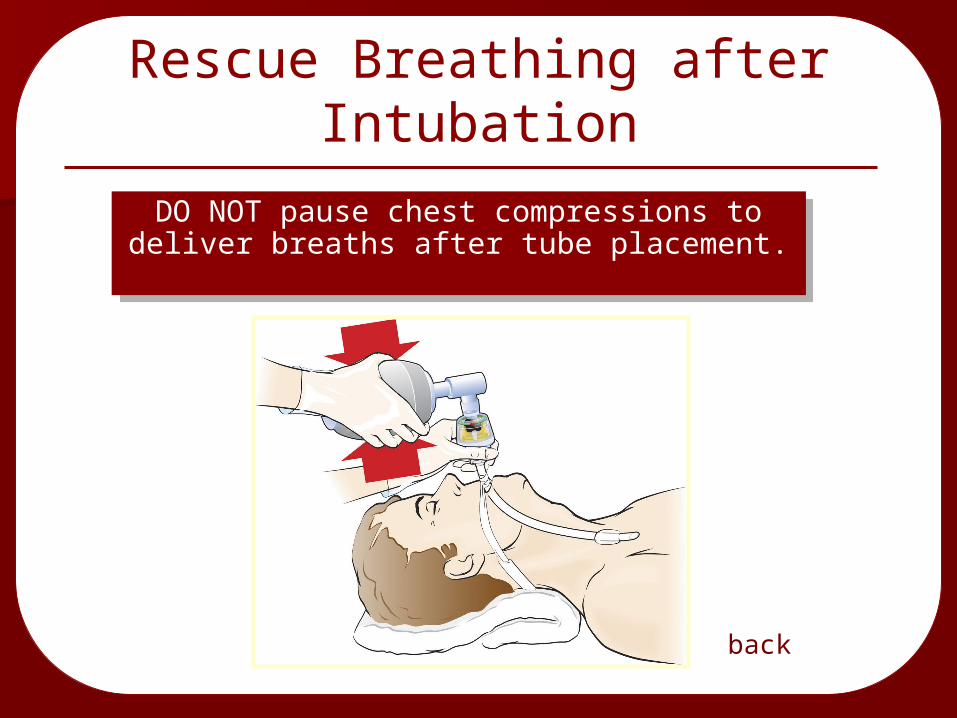
Rescue Breathing after Intubation
DO NOT pause chest compressions to deliver breaths after tube placement.DO NOT pause chest compressions to deliver breaths after tube placement.
back
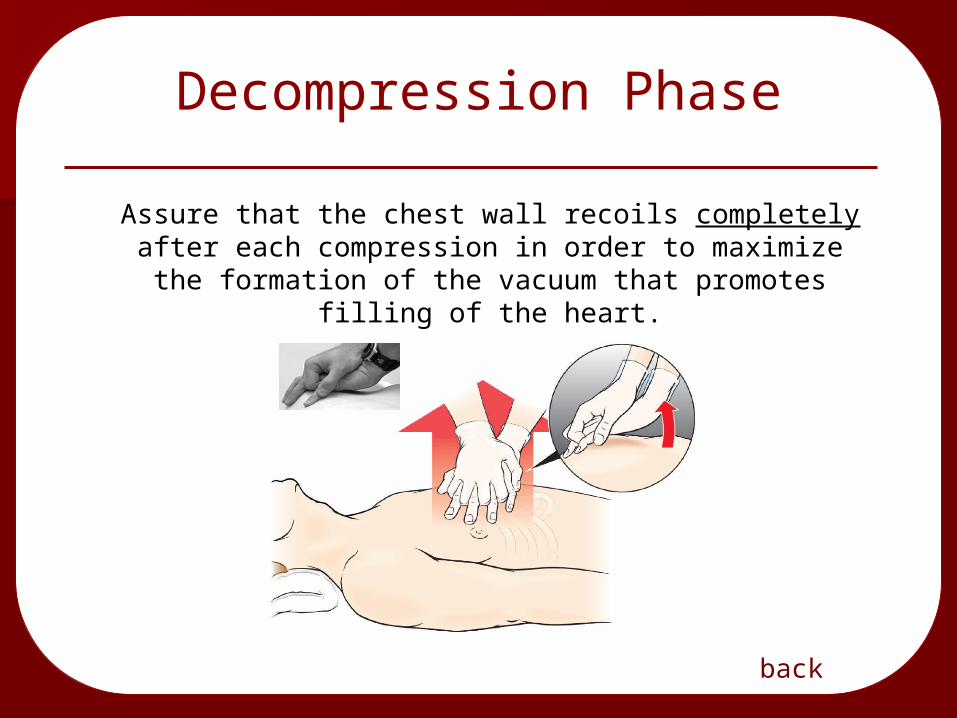
Decompression Phase
back
Assure that the chest wall recoils completely after each compression in order to maximize the
formation of the vacuum that promotes filling of the heart.
Practice your CPR skills frequently
Good CPR takes training Good CPR takes training ANDAND practicepractice
Research shows that students continue to Research shows that students continue to show improvement in both knowledge and show improvement in both knowledge and skills after skills after 44 training sessions training sessions
Understanding and skills begin to weaken Understanding and skills begin to weaken after only 10 weeks following trainingafter only 10 weeks following training
Rescuers should practice their skills Rescuers should practice their skills 3-43-4 times times per yearper year
Plan to practice with the manikin and other Plan to practice with the manikin and other training materials on your own or with a training materials on your own or with a partner for ~10 minutes each monthpartner for ~10 minutes each month
Good CPR takes training Good CPR takes training ANDAND practicepractice
Research shows that students continue to Research shows that students continue to show improvement in both knowledge and show improvement in both knowledge and skills after skills after 44 training sessions training sessions
Understanding and skills begin to weaken Understanding and skills begin to weaken after only 10 weeks following trainingafter only 10 weeks following training
Rescuers should practice their skills Rescuers should practice their skills 3-43-4 times times per yearper year
Plan to practice with the manikin and other Plan to practice with the manikin and other training materials on your own or with a training materials on your own or with a partner for ~10 minutes each monthpartner for ~10 minutes each month
back
BLS & ALS work together to save lives!
One of the most important factors in overall patient outcome is the quality of CPR. The AHA recently revised their ACLS course, stating that
“high-quality CPR is more effective than any ACLS drug. The science tells us that our focus should be on BLS skills to maintain perfusion.”
Currents in Emergency Cardiovascular Care. Vol. 17 No. 4, Winter, 2006-2007
One of the most important factors in overall patient outcome is the quality of CPR. The AHA recently revised their ACLS course, stating that
“high-quality CPR is more effective than any ACLS drug. The science tells us that our focus should be on BLS skills to maintain perfusion.”
Currents in Emergency Cardiovascular Care. Vol. 17 No. 4, Winter, 2006-2007
back
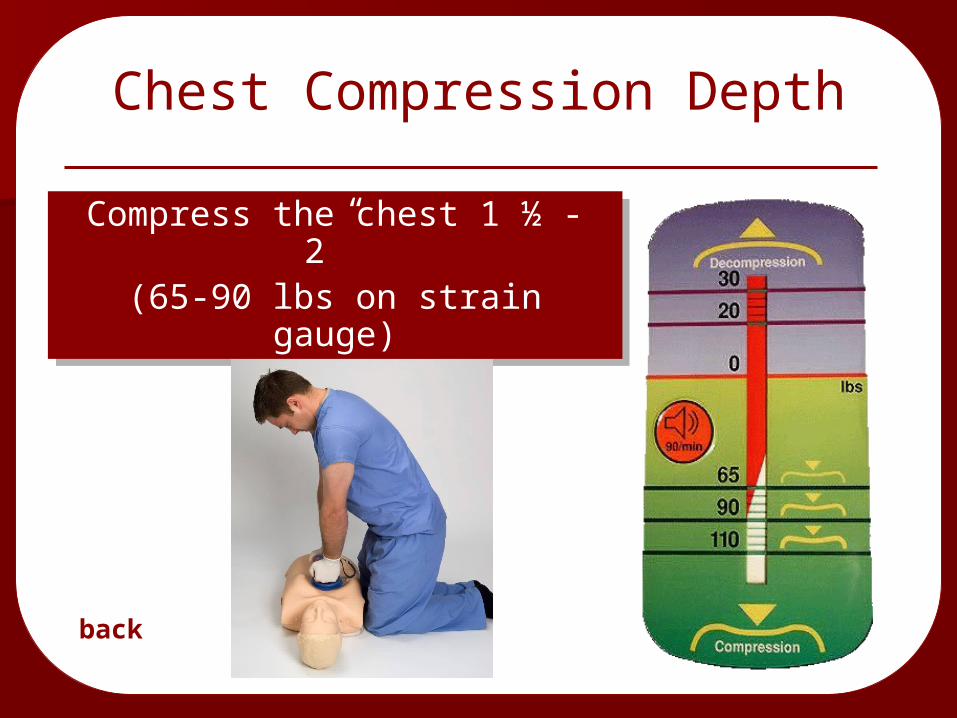
Chest Compression Depth
Compress the chest 1 ½ - 2” (65-90 lbs on strain gauge)
Compress the chest 1 ½ - 2” (65-90 lbs on strain gauge)
back
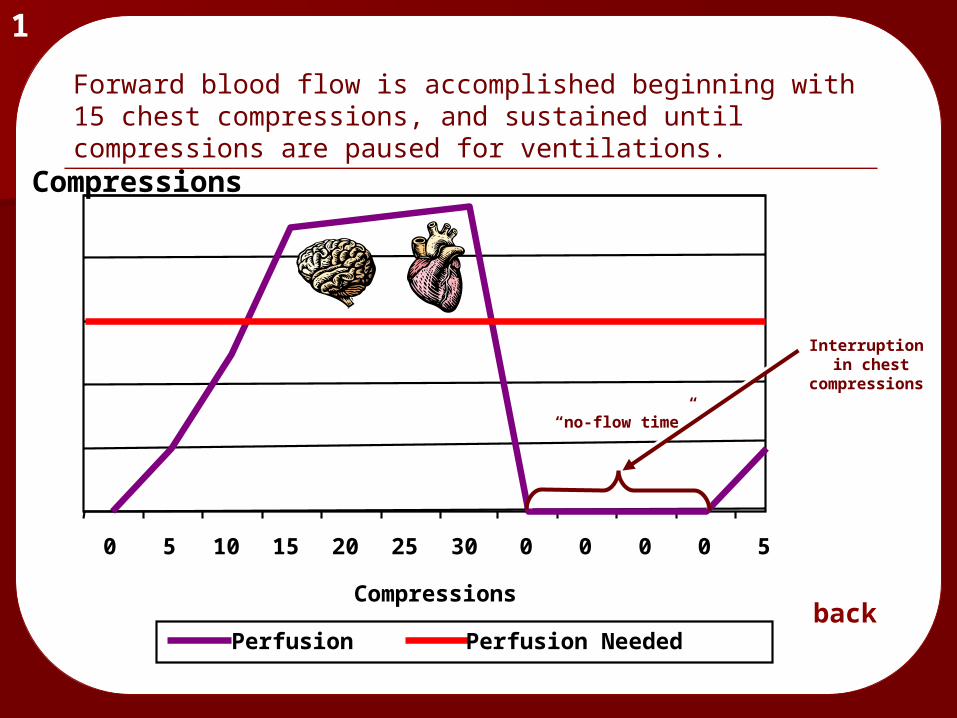
Blood Flow to Vital Organs During Chest Compressions
Compressions
Perfusion Perfusion Needed
0 5 10 15 20 25 30 0 0 0 0 5
Interruption in chest
compressions
1
Forward blood flow is accomplished beginning with 15 chest compressions, and sustained until compressions are paused for ventilations.
back
“no-flow time”
ResQ Trial Hotline
You can find the hotline phone number in:• Resource Guide (yellow folder)• Easy-to-Read ResQ Trial Calendar
Call the hotline after every cardiac arrest (including peds, trauma victims, & DOAs).
Research Hotline: 1-866-640-2832 back
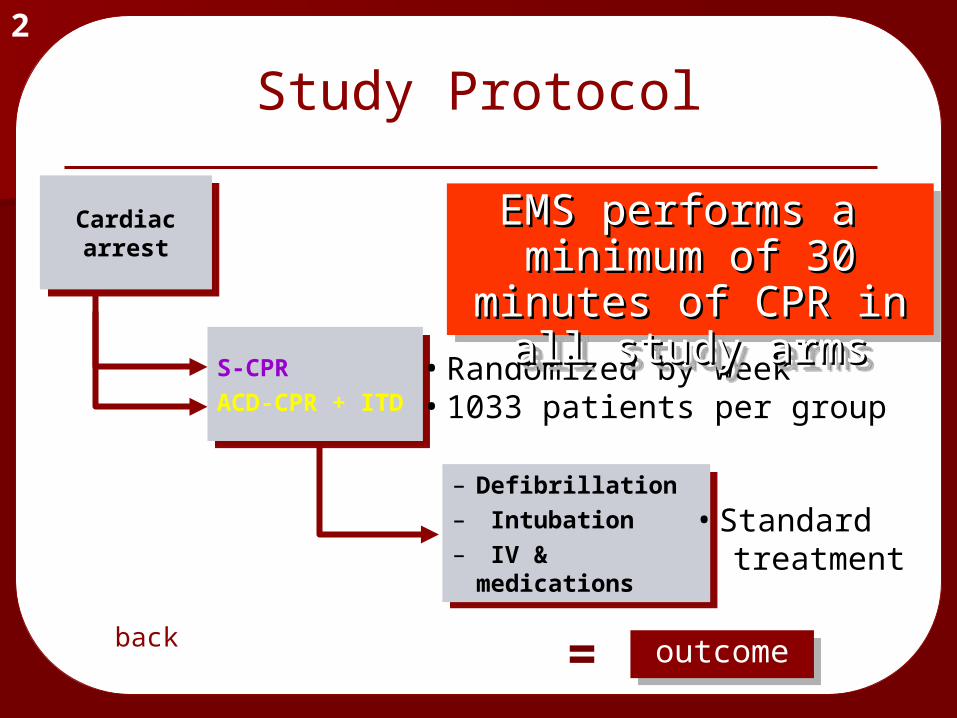
Study Protocol
Cardiac arrest
Cardiac arrest
S-CPRACD-CPR + ITD
S-CPRACD-CPR + ITD
– Defibrillation– Intubation– IV &
medications
– Defibrillation– Intubation– IV &
medications
=
outcome
outcomeoutcome
2
• Standard treatment
• Randomized by week• 1033 patients per group
EMS performs a EMS performs a minimum of 30 minimum of 30
minutes of CPR in all minutes of CPR in all study armsstudy arms
EMS performs a EMS performs a minimum of 30 minimum of 30
minutes of CPR in all minutes of CPR in all study armsstudy arms
back
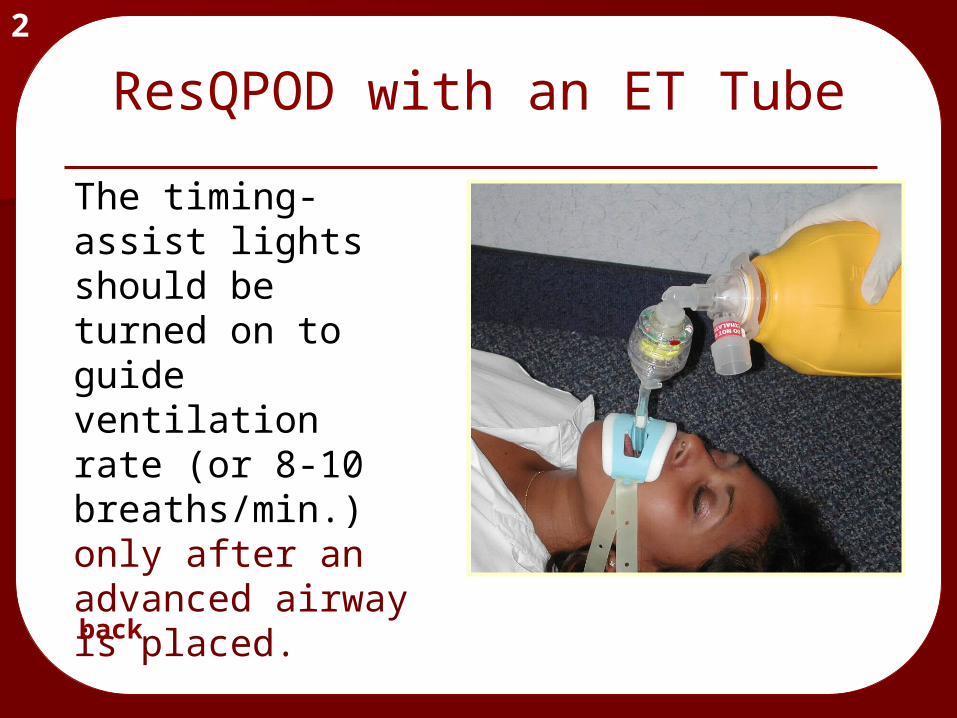
The timing-assist lights should be turned on to guide ventilation rate (or 8-10 breaths/min.) only after an advanced airway is placed.
2
ResQPOD with an ET Tube
back
2
The ResQPOD enhances circulation.
When pulse returns…
The ResQPOD is a CPR tool
Keep the ResQ POD nearby in case the patient re-arrests.back
AED
• Apply the AED pads as soon as the patient is determined to be without pulse or respirations.
• If the cardiac arrest was not witnessed by EMS (or the downtime is known to be greater than 4 minutes) perform 2 minutes or 5 cycles of CPR before analyzing for a shockable rhythm
back
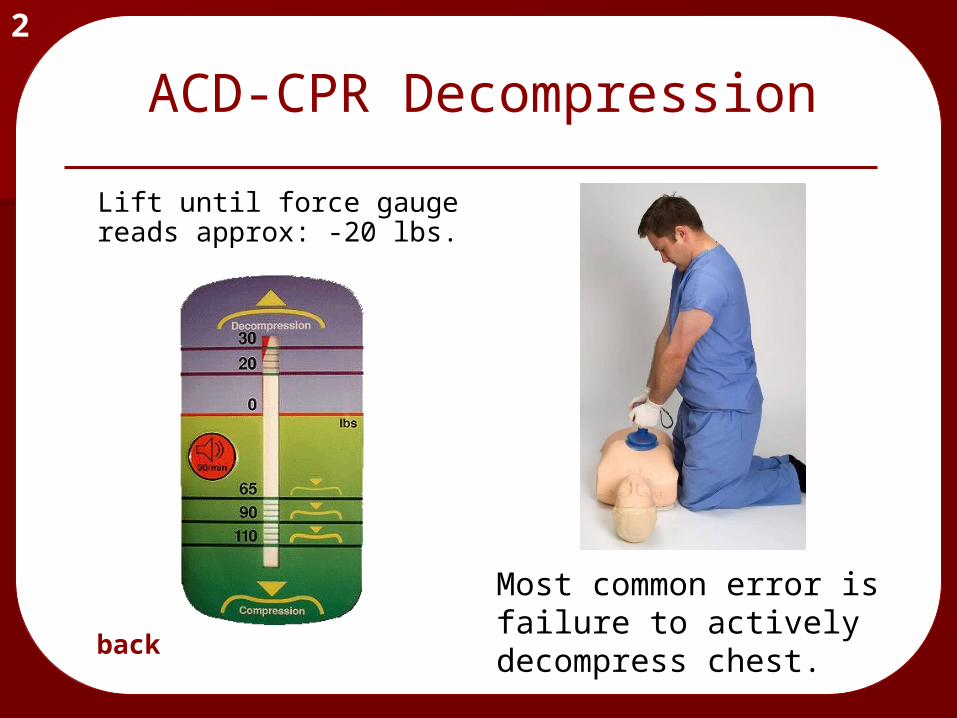
ACD-CPR Decompression
Lift until force gauge reads approx: -20 lbs.
2
back
Most common error is failure to actively decompress chest.
Compressions at a rate of 100/min.
YES! This is approximately 100 compressions per minute.
OR…you can hum the “Staying Alive” song
back