restriction enzyme cytomegalovirus dna to
TRANSCRIPT

J Clin Pathol 1986;39:318-324
Restriction enzyme analysis of cytomegalovirus DNAto study transmission of infectionCATHERINE S PECKHAM,* AJ GARRETT,t KS CHIN,* PM PREECE,*D B NELSON,* DIANE E WARREN,t
From the *Departments ofCommunity Medicine and Paediatrics, Charing Cross and Westminster MedicalSchool, London, and tNational Institutefor Biological Standards and Control, London
SUMMARY Restriction enzyme analysis of cytomegalovirus deoxyribonucleic acid (DNA) has beenused to characterise virus isolates and has provided information on patterns of viral transmission.
It was shown that virus isolated from a congenitally infected infant was unlikely to have origi-nated from the 13 congenitally infected children with whom the mother, a nurse, had been incontact. Of nine mother and infant pairs, from whom cytomegalovirus was isolated, seven yieldedstrains that were indistinguishable for mother and child; one pair showed minor differences and onewas clearly distinguishable. Virus isolates from seven children attending a day nursery were typed,and only siblings were excreting similar strains of cytomegalovirus. Further examples of the appli-cation of this technique to studies of cytomegalovirus in a family environment are given.
It is concluded that characterisation of virus strains by restriction analysis ofDNA is a valuableepidemiological tool.
Cytomegalovirus infection during pregnancy and inthe immunosuppressed patient can have seriousconsequences.' 2 Considerable concern has beenexpressed that infection may spread to nursery schoolteachers, nurses, and medical personnel who may bein close contact with infected subjects.34 In the courseof our studies on the consequences of congenital cyto-megalovirus infection,5 and the prevalence ofacquired infection in infants as well as in childrenattending day nurseries, it became clear that there wasa need for a readily applicable technique for typingstrains of cytomegalovirus to identify patterns oftransmission of infection. The source of cytomegalo-virus infection cannot be determined unequivocallyby serology or by isolation of the virus from epi-demiologically related cases. Restriction enzymeanalysis of DNA for identifying different strains ofcytomegalovirus was first developed by Huang et al.6More recently, Garrett and Warren described amodification of this technique that is simpler andrequires smaller quantities of virus.7 The applicationof this modified method, which is applicable for rou-tine use in large epidemiological surveys, is shown inthis paper.Accepted for publication 14 November 1985
Subjects and methods
The subjects reported were derived from severaldifferent sources: a congenitally infected infant bornto a nurse who had been in contact with 13 childrenwith cytomegalovirus infection during her pregnancy;a family study; seven children excreting cyto-megalovirus in a day nursery; and nine mother andinfant pairs from whom the virus was isolated. Iso-lates of cytomegalovirus grown from throat swabs,urine, or breast milk were stored in liquid nitrogen.They were subsequently regrown in culture bottlescontaining 25 cm2 sheets of human embryo lungfibroblasts and incubated at 36-370C.The method for differentiation of cytomegalovirus
strains by restriction enzyme nuclease analysis ofvirus DNA has been described in detail by Garrettand Warren.7 In brief, cultures infected with cyto-megalovirus were labelled with 32P, and crude DNAwas extracted and digested with restriction endo-nuclease (EcoRI, Bam HI, Bgl II, or Hind III). Theresultant oligonucleotides were separated by electro-phoresis on agarose gels. As a reference for eachdigest and each electrophoretogram, the appropriateDNA digest from cytomegalovirus strain Ad 169 was
318
on April 1, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.3.318 on 1 March 1986. D
ownloaded from
Restriction enzyme analysis of cytomegalovirus DNA and transmission of infection
Cytomegalovirus serological state* IgMtIndex case
Father AA
Mother A A AP AP
_Virus isolation-**Index case 0*0 0 0 0
Father (30) 0 0
Mother (27) 0 0 0 o
Sibling 1 (7) 0 0 0
2(5) 0 0
3(3k) o
4(2) 0 *
transfusions 111111r Discharge of index case
-2 0 2 4 6 8 10 12 14
Months from birth of index case
I16 18 20
* CMV Complement fixation test <5A 20
t IgM A absent
P present
** Virus isolation o negative* positive
( ) Parental and sibling age in years
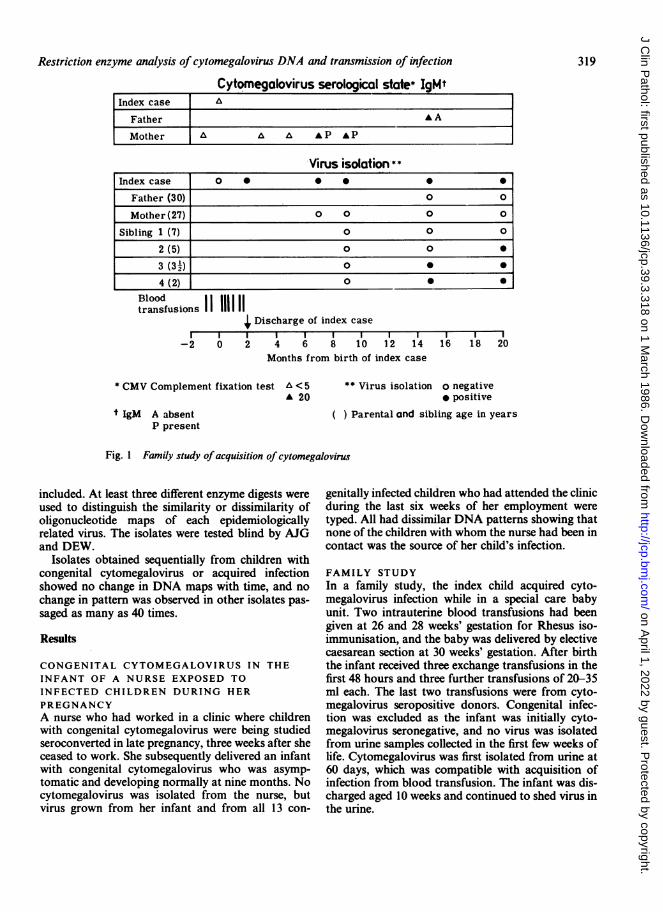
Fig. I Family study ofacquisition of cytomegalovirus
included. At least three different enzyme digests wereused to distinguish the similarity or dissimilarity ofoligonucleotide maps of each epidemiologicallyrelated virus. The isolates were tested blind by AJGand DEW.
Isolates obtained sequentially from children withcongenital cytomegalovirus or acquired infectionshowed no change in DNA maps with time, and nochange in pattern was observed in other isolates pas-saged as many as 40 times.
Results
CONGENITAL CYTOMEGALOVIRUS IN THE
INFANT OF A NURSE EXPOSED TOINFECTED CHILDREN DURING HER
PREGNANCYA nurse who had worked in a clinic where childrenwith congenital cytomegalovirus were being studiedseroconverted in late pregnancy, three weeks after sheceased to work. She subsequently delivered an infantwith congenital cytomegalovirus who was asymp-tomatic and developing normally at nine months. Nocytomegalovirus was isolated from the nurse, butvirus grown from her infant and from all 13 con-
genitally infected children who had attended the clinicduring the last six weeks of her employment weretyped. All had dissimilar DNA patterns showing thatnone of the children with whom the nurse had been incontact was the source of her child's infection.
FAMILY STUDYIn a family study, the index child acquired cyto-megalovirus infection while in a special care babyunit. Two intrauterine blood transfusions had beengiven at 26 and 28 weeks' gestation for Rhesus iso-immunisation, and the baby was delivered by electivecaesarean section at 30 weeks' gestation. After birththe infant received three exchange transfusions in thefirst 48 hours and three further transfusions of 20-35ml each. The last two transfusions were from cyto-megalovirus seropositive donors. Congenital infec-tion was excluded as the infant was initially cyto-megalovirus seronegative, and no virus was isolatedfrom urine samples collected in the first few weeks oflife. Cytomegalovirus was first isolated from urine at60 days, which was compatible with acquisition ofinfection from blood transfusion. The infant was dis-charged aged 10 weeks and continued to shed virus inthe urine.
319
on April 1, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.3.318 on 1 March 1986. D
ownloaded from
Peckham, Garrett, Chin, Preece, Nelson, Warren
e.. U; _ BgI 11
3 4 Ad169 5. 6 8 3 4 Adl69 5 6 7 8" __a_ _ sE _ _
- i as-
i
a.V.?::"'w..-a
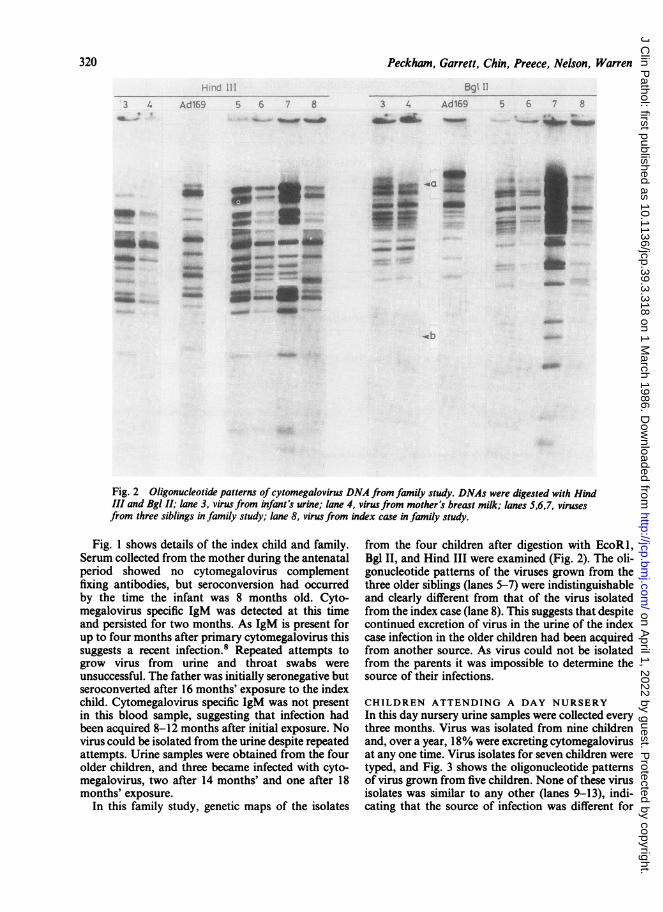
Fig. 2 Oligonucleotide patterns of cytomegalovirus DNA from family study. DNAs were digested with HindIII and Bgl II; lane 3, virus from infant's urine; lane 4, virusfrom mother's breast milk; lanes 5,6,7, virusesfrom three siblings in family study; lane 8, virusfrom index case in family study.
Fig. 1 shows details of the index child and family.Serum collected from the mother during the antenatalperiod showed no cytomegalovirus complementfixing antibodies, but seroconversion had occurredby the time the infant was 8 months old. Cyto-megalovirus specific IgM was detected at this timeand persisted for two months. As IgM is present forup to four months after primary cytomegalovirus thissuggests a recent infection.8 Repeated attempts togrow virus from urine and throat swabs wereunsuccessful. The father was initially seronegative butseroconverted after 16 months' exposure to the indexchild. Cytomegalovirus specific IgM was not presentin this blood sample, suggesting that infection hadbeen acquired 8-12 months after initial exposure. Novirus could be isolated from the urine despite repeatedattempts. Urine samples were obtained from the fourolder children, and three became infected with cyto-megalovirus, two after 14 months' and one after 18months' exposure.
In this family study, genetic maps of the isolates
from the four children after digestion with EcoRl,Bgl II, and Hind III were examined (Fig. 2). The oli-gonucleotide patterns of the viruses grown from thethree older siblings (lanes 5-7) were indistinguishableand clearly different from that of the virus isolatedfrom the index case (lane 8). This suggests that despitecontinued excretion of virus in the urine of the indexcase infection in the older children had been acquiredfrom another source. As virus could not be isolatedfrom the parents it was impossible to determine thesource of their infections.
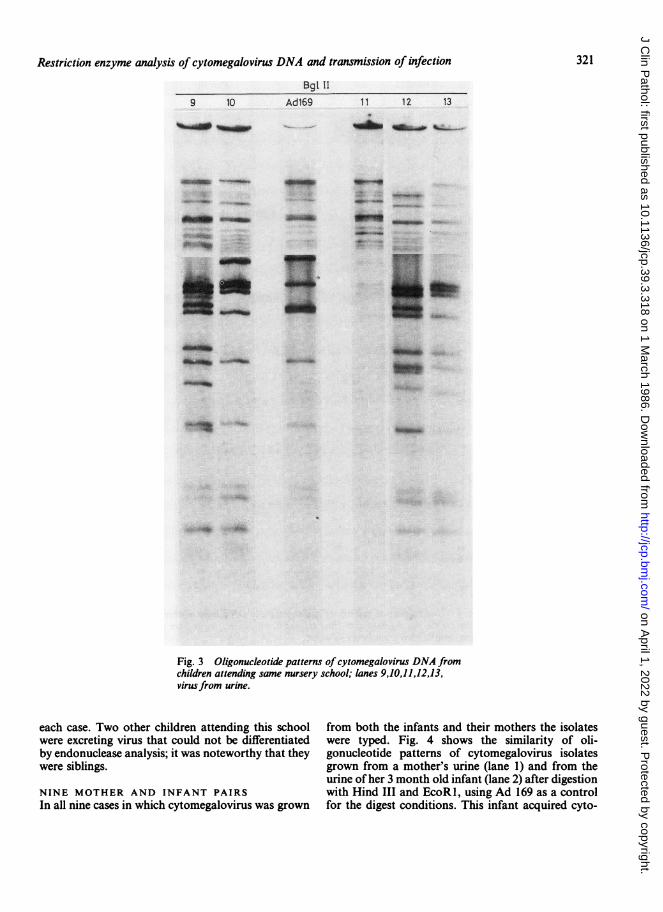
CHILDREN ATTENDING A DAY NURSERYIn this day nursery urine samples were collected everythree months. Virus was isolated from nine childrenand, over a year, 18% were excreting cytomegalovirusat any one time. Virus isolates for seven children weretyped, and Fig. 3 shows the oligonucleotide patternsof virus grown from five children. None of these virusisolates was similar to any other (lanes 9-13), indi-cating that the source of infection was different for
do-
USe,...'
320
on April 1, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.3.318 on 1 March 1986. D
ownloaded from
Restriction enzyme analysis of cytomegalovirus DNA and transmission of infection
Bgt 119 10 Ad169
..:. m. ....._:,." W
W.."f
uis_wut
11 12 13
_gib -
4_ _
__- __~I......W
'ASMOM,~~~~.so"..
--p .ir
:i;..:,...:..
-F
Fig. 3 Oligonucleotide patterns of cytomegalovirus DNA fromchildren attending same nursery school; lanes 9,10,11,12,13,virusfrom urine.
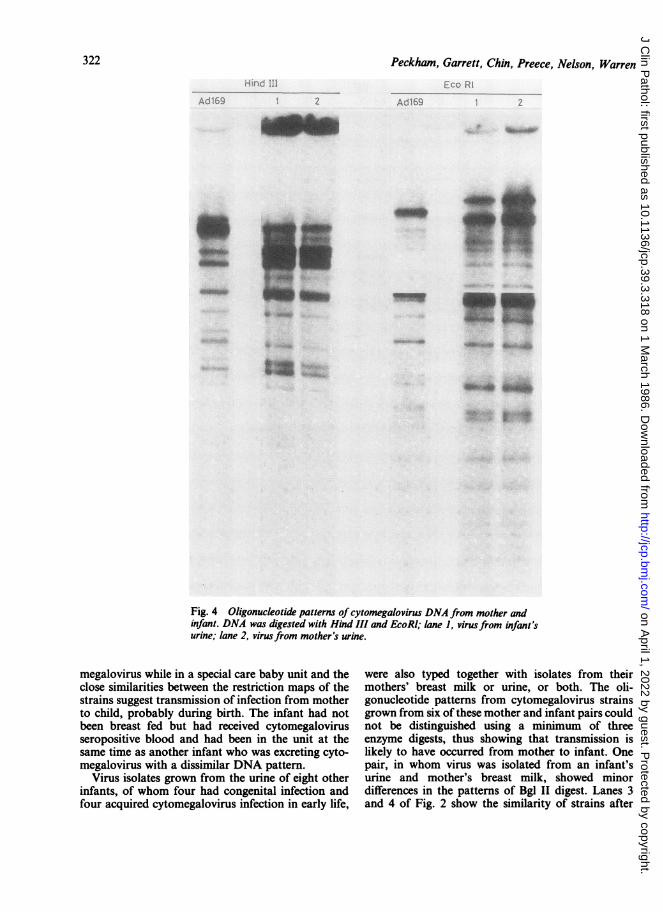
each case. Two other children attending this school from both the infants and their mothers the isolateswere excreting virus that could not be differentiated were typed. Fig. 4 shows the similarity of oli-by endonuclease analysis; it was noteworthy that they gonucleotide patterns of cytomegalovirus isolateswere siblings. grown from a mother's urine (lane 1) and from the
urine of her 3 month old infant (lane 2) after digestionNINE MOTHER AND INFANT PAIRS with Hind III and EcoRl, using Ad 169 as a controlIn all nine cases in which cytomegalovirus was grown for the digest conditions. This infant acquired cyto-
321
AUOMakwaft _:-.*#*m
-W-"Ib
on April 1, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.3.318 on 1 March 1986. D
ownloaded from
322
a .-1 :...
Peckham, Garrett, Chin, Preece, Nelson, Warren
.1.6.......9z ~ ~~~~~ ~Adl1 ;
Ii" ,.
_ _~~
Fig. 4 Oligonucleotide patterns of cytomegalovirus DNA from mother andinfant. DNA was digested with Hind III and EcoRl; lane 1, virusfrom infant'surine; lane 2, virusfrom mother's urine.
megalovirus while in a special care baby unit and theclose similarities between the restriction maps of thestrains suggest transmission of infection from motherto child, probably during birth. The infant had notbeen breast fed but had received cytomegalovirusseropositive blood and had been in the unit at thesame time as another infant who was excreting cyto-megalovirus with a dissimilar DNA pattern.
Virus isolates grown from the urine of eight otherinfants, of whom four had congenital infection andfour acquired cytomegalovirus infection in early life,
were also typed together with isolates from theirmothers' breast milk or urine, or both. The oli-gonucleotide patterns from cytomegalovirus strainsgrown from six of these mother and infant pairs couldnot be distinguished using a minimum of threeenzyme digests, thus showing that transmission islikely to have occurred from mother to infant. Onepair, in whom virus was isolated from an infant'surine and mother's breast milk, showed minordifferences in the patterns of Bgl II digest. Lanes 3and 4 of Fig. 2 show the similarity of strains after
qqpw
4we
olqmw
46. '. A..,6
tg:4;.:
on April 1, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.3.318 on 1 March 1986. D
ownloaded from
Restriction enzyme analysis of cytomegalovirus DNA and transmission of infectiondigestion with Hind III and the differences thatemerged after digestion with Bgl II. The presence ofthe two additional bands in the high molecular weightregion (a) and concomitant deletion of a fragment ofabout 2 5 x 106 molecular weight (b) was shown inthree separate digestions of strains 3 and 4. Dissimi-larity of the virus strains was seen for only one motherand infant pair; virus was first isolated from the infantat 8 months and from the mother's milk for the firsttime at 18 months, suggesting an alternative source ofinfection.
Discussion
Cytomegalovirus infection is usually an asymp-tomatic or mild infection but it can result in seriousconsequences when acquired by immunosuppressedpatients or pregnant women.' 2 As infants with bothacquired and congenital infection continue to shedvirus in their urine for many years, concern has beenexpressed about the risk of young female staff acquir-ing the infection from children they care for, particu-larly from children with congenital cytomegaloviruswho are known excretors.34 Similarly, when a sero-negative infant is infected with cytomegalovirus afterblood transfusion the mother is thought to be at riskof acquiring cytomegalovirus from the child at thetime of her next pregnancy.9 Information on themode of transmission of cytomegalovirus is largelyanecdotal or based on circumstantial evidence includ-ing the age of acquisition of cytomegalovirus anti-bodies, the prevalence of cytomegalovirus antibodiesin a population, and the knowledge that virus can beisolated from the nasopharynx, genital tract, andsemen.
Several workers have shown the value of restrictionendonuclease analysis of cytomegalovirus DNA fordetermining likely transmission of infection.'01'There are innumerable genetic variants of cyto-megalovirus and restriction enzyme cleavage of cyto-megalovirus DNA obtained from random clinicalisolates indicates that no two viruses give identicalDNA fragments when multiple digests are com-pared.'° In contrast, epidemiologically related cyto-megalovirus strains such as those from mother andinfant pairs have identical restriction mapping pat-terns. Our results confirm the high degree of geneticvariability among cytomegalovirus strains. Although,routinely, three or four enzymes are used to charac-terise each isolate, isolates from epidemiologicallyunrelated cases usually differ sufficiently for differen-tiation to be established by examination of thedigestion products of one endonuclease. Given thelarge size of the genome, identity of DNA structuresis more difficult to establish unequivocally as only
about 0 I1% of the viral genome is specifically selectedby each endonuclease.More information is required about the effects of
transmission of cytomegalovirus to a new host and ofperiods of latency and reactivation on the stability ofviral DNA. The finding that DNA restriction enzymetyping of cytomegalovirus isolates from sex partnersshowed common strains suggests that the genomedoes not undergo major mutation after transmissionto a new host,'2 but this needs further study as minordifferences have been observed in mother and infantpairs. Mutation, selection of variants, or recombina-tion with reactivated virus could theoretically occur,but this was not shown to be the case when mixedinfections were studied in vitro (Garrett AJ, WarrenDE, unpublished observations, 1984). Under the con-ditions described in this paper no genetic variantswere detected after clinical isolates were passaged upto 40 times and Ad 169 passaged 100 times in vitro.Huang et al cloned and subcultivated strains Ad 169and Towne for over 100 passages and discovered onlyminor modifications in restriction enzyme sites andoverall homology with the parental virus retained.'3
In this study cytomegalovirus isolates recoveredfrom seven of nine mother and infant pairs were iden-tical. In one pair minor differences similar to thosereported by Huang were observed. These differenceswere quite distinct from the major differences seenbetween epidemiologically unrelated strains of cyto-megalovirus. Although repeat digests were per-formed, the possibility of incomplete digestion couldnot be excluded. Major differences in DNA patternswere found in only one mother and infant pair, but inthis case virus was first isolated from breast milk 10months after the infant had become infected. It isknown that different strains of herpes simplex viruscan be shed simultaneously from different sites of thesame host,'4 but there is, as yet, little evidence to sug-gest that this occurs with cytomegalovirus. Differentstrains of cytomegalovirus isolated from differentsites at the same time were, however, reported in twopatients with the acquired immune deficiency syn-drome.'5
Endonuclease analysis of cytomegalovirus isolatesfrom unrelated children attending a day nurseryshowed no genetic identities, thus showing a lack ofhorizontal transmission of infection among thesechildren. There was, however, genetic identity ofcytomegalovirus from each of two sibling pairs withinthe same nursery compatible with infection originat-ing in the home. A detailed prospective epi-demiological study of cytomegalovirus transmissionwithin a day nursery examining virus isolates fromchildren and staff is in progress to elucidate furtherthe mode of virus transmission and establish whetherthis poses an important occupational risk.
323
on April 1, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.3.318 on 1 March 1986. D
ownloaded from

324From examination of virus DNA of cyto-
megalovirus isolates from the mother and her infantin special care nosocomial transmission of infectionwas excluded. Had this not been done the source ofinfection may have been incorrectly ascribed to con-tact within the special care unit, and such a conclu-sion would have had major implications for manage-ment and infection control. In the past nosocomialtransmission has often been assumed on the basis ofcircumstantial evidence. For example, Gurevich andCunha concluded that cytomegalovirus was trans-mitted in a neonatal intensive care unit from an infantwith congenital cytomegalovirus who had lived onlyeight hours.'6 Such a conclusion is unwarranted as
analysis of viral DNA was not carried out. Spector,however, analysed cytomegalovirus isolates fromseven infants in an intensive care unit and found thatthe DNA patterns were similar in three.'7 This is theonly published evidence of cytomegalovirus trans-mission among infected babies.As in other studies in which restriction enzyme
analysis was possible, temporal associations of cyto-megalovirus infection in adults caring for infectedinfants failed to show a causal link,'8 21 suggestingthat infection had been acquired outside the hospital.As yet there have been no reports of the acquisition ofcytomegalovirus by staff from known excretors intheir care.
We thank all the doctors, nurses, and nursery schoolstaff who made this study possible, Dr K Pearl andMiss C Johnson for their help, Mrs EG Hogben forpreparing the manuscript, and Dr G Schild for hisuseful comments. The work was supported by grantsfrom The National Fund for Research into CripplingDiseases, the Medical Research Council and theHarrison Trust.
References
Preece PM, Pearl KN, Peckham CS. Congenital cytomegalovirusinfection. Arch Dis Child 1984;59:1 120-6.
2 Ho M. Virus infection after transplantation in man: brief review.Arch Virol 1977;55:1-24.
3Yeager AS. Longitudinal serological study of cytomegalovirusinfections in nurses and in personnel without patient contact.J Clin Microbiol 1975;2:448-52.
'Friedman HM, Lewis MR, Nemerofsky M, Plotkin SA. Acquisi-
Peckham, Garrett, Chin, Preece, Nelson, Warrention of cytomegalovirus infection among female employees of apediatric hospital. J Pediatr Infect Dis 1985;3:233-5.
'Peckham CS, Chin KS, Coleman JC, et al. Cytomegalovirus infec-tion in pregnancy: preliminary findings from a prospectivestudy. Lancet 1983;i:1352-5.
6Huang ES, Kilpatrick BA, Huang YT, et al. Detection of humancytomegalovirus and analysis of strain variation. Yale J BiolMed 1976;49:29-43.
'Garrett AJ, Warren DE. A simple technique for endonuclease map-ping of cytomegaloviruses. J Virol Methods 1985;10: 187-94.
8Griffiths PD. The presumptive diagnosis of primary cyto-megalovirus infection in early pregnancy by means of a radio-immunoassay for specific-IgM antibodies. Br J Obstet Gynaecol1981;88:582-7.
9 Yeager AS. Transmission of cytomegalovirus to mothers by infec-ted infants: another reason to prevent transfusion-acquiredinfections. Pediatr Infect Dis 1983;2:295-7.
0Huang ES, Alford CA, Reynolds DW, et al. Molecular epi-demiology of cytomegalovirus infections in women and theirinfants. N Engl J Med 1980;303:958-62.
l Spector SA, Spector D. Molecular epidemiology of cyto-megalovirus infections in premature twin infants and theirmother. Pediatr Infect Dis 1982;1:405-9.
1 Handsfield HH, Chandler SM, Caine VA, et al. Cytomegalovirusinfection in sex partners: evidence for sexual transmission.J Infect Dis 1985;151:344-8.
13Huang ES, Hung SM, Tegtmeier GE, Alford CA. Cyto-megalovirus: genetic variation of viral genome. Ann NY AcadSci 1980;354:332-46.
"Buchman TG, Roizman B, Nahmias AJ. Demonstration ofexogenous genital re-infection with herpes simplex virus type 2by restriction endonuclease fingerprinting by viral DNA.J Infect Dis 1979;140:295-304.
"Spector SA, Hirata KK, Neuman TR. Identification of multiplecytomegalovirus strains in homosexual men with acquiredimmunodeficiency syndrome. J Infect Dis 1984;150:953-6.
iGurevich I, Cunha BA. Non-parental transmission of cyto-megalovirus in a neonatal intensive care unit. Lancet 1981;ii:222-4.
Spector SA. Transmission of cytomegalovirus among infantsin hospital documented by restriction-endonuclease-digestionanalyses. Lancet 1983;i:378-81.
"Grillner L, Blomberg I. Restriction enzyme analysis of humancytomegalovirus using DNA extracted from infected cells.J Med Virol 1984;14:313-22.
9Yow MD, Lakeman AD, Stagno S, et al. Use of restrictionenzymes to investigate the source of a primary cytomegalovirusinfection. Pediatrics 1982;70:713-6.
20Wilfert CM, Huang ES, Stagno S. Restriction endonucleaseanalysis of cytomegalovirus deoxyribonucleic acid as anepidemiological tool. Pediatrics 1982;70:717-24.
21 Dworsky M, Lakeman A, Stagno S. Cytomegalovirus trans-mission within a family. Pediatr Infect Dis 1984;3:236-8.
Requests for reprints to: Professor CS Peckham, Institute ofChild Health, 30 Guilford Street, London WCIN IEH,England.
on April 1, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.3.318 on 1 March 1986. D
ownloaded from