resuscitation science...medical services (ems) access, early cardiopulmonary resus-citation (cpr),...
TRANSCRIPT

1962
Out-of-hospital cardiac arrest (OHCA) leads to an esti-mated 330 000 deaths each year in the United States and
Canada.1 Although overall survival for treated OHCA is low, hospital discharge rates vary from 3.0% to 16.3%.1 This varia-tion in survival can be partly attributed to local differences in the 5 key links in the chain of survival: rapid emergency medical services (EMS) access, early cardiopulmonary resus-citation (CPR), early defibrillation, early advanced cardiac life
support, and effective postresuscitation care.2–6 Considerable efforts by communities and hospitals to strengthen these links have led to only modestly better survival rates in recent years.1
Clinical Perspective on p 1970
In recent years, those involved in cardiac resuscitation have recognized that the quality, quantity, and timeliness of CPR are key determinants for survival from cardiac arrest and that
Background—The 2010 American Heart Association guidelines suggested an increase in cardiopulmonary resuscitation compression depth with a target >50 mm and no upper limit. This target is based on limited evidence, and we sought to determine the optimal compression depth range.
Methods and Results—We studied emergency medical services–treated out-of-hospital cardiac arrest patients from the Resuscitation Outcomes Consortium Prehospital Resuscitation Impedance Valve and Early Versus Delayed Analysis clinical trial and the Epistry-Cardiac Arrest database. We calculated adjusted odds ratios for survival to hospital discharge, 1-day survival, and any return of circulation. We included 9136 adult patients from 9 US and Canadian cities with a mean age of 67.5 years, mean compression depth of 41.9 mm, and a return of circulation of 31.3%, 1-day survival of 22.8%, and survival to hospital discharge of 7.3%. For survival to discharge, the adjusted odds ratios were 1.04 (95% CI, 1.00–1.08) for each 5-mm increment in compression depth, 1.45 (95% CI, 1.20–1.76) for cases within 2005 depth range (>38 mm), and 1.05 (95% CI, 1.03–1.08) for percentage of minutes in depth range (10% change). Covariate-adjusted spline curves revealed that the maximum survival is at a depth of 45.6 mm (15-mm interval with highest survival between 40.3 and 55.3 mm) with no differences between men and women.
Conclusions—This large study of out-of-hospital cardiac arrest patients demonstrated that increased cardiopulmonary resuscitation compression depth is strongly associated with better survival. Our adjusted analyses, however, found that maximum survival was in the depth interval of 40.3 to 55.3 mm (peak, 45.6 mm), suggesting that the 2010 American Heart Association cardiopulmonary resuscitation guideline target may be too high.
Clinical Trial Registration—URL: http://www.clinicaltrials.gov. Unique identifier: NCT00394706. (Circulation. 2014;130:1962-1970.)
Key Words: cardiopulmonary resuscitation ◼ emergency medical services ◼ heart arrest
© 2014 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.114.008671
Received January 15, 2014; accepted September 11, 2014.From the Department of Emergency Medicine and Ottawa Hospital Research Institute, University of Ottawa, Ottawa, Ontario, Canada (I.G.S., C.V.);
Clinical Trials Center, Department of Biostatistics (S.P.B., G.N.) and Department of Medicine (G.N.), University of Washington, Seattle, WA; University of Washington-Harborview Center for Prehospital Emergency Care, Seattle, WA (G.N.); Division of Emergency Medicine, Department of Family and Community Medicine (S.C.), and Division of Emergency Medicine, Department of Medicine (L.J.M.), University of Toronto, Toronto, Ontario, Canada; Rescu, Li Ka Shing Knowledge Institute, St Michael’s Hospital, Toronto, Ontario, Canada (S.C., L.J.M.); Department of Emergency Medicine, University of Pittsburgh, Pittsburgh, PA (C.W.C., D.H.); Department of Emergency Medicine, University of British Columbia, Vancouver, British Columbia, Canada (J.C.); Department of Emergency Medicine, Medical College of Wisconsin, Milwaukee, WI (T.P.A.); Department of Emergency Medicine, University of California, San Diego, CA (D.P.D.); Camas Fire Department, Camas, WA (C.F.); Central Washington University, Ellensburg, WA (J.A.S.); Departments of Emergency Medicine and Internal Medicine, University of Texas Southwestern Medical Center, Dallas, TX (A.H.I.).
The online-only Data Supplement is available with this article at http://circ.ahajournals.org/lookup/suppl/doi:10.1161/CIRCULATIONAHA. 114.008671/-/DC1.
Correspondence to Ian G. Stiell, MD, Ottawa Hospital Research Institute, Clinical Epidemiology Unit, Office F657, The Ottawa Hospital, Civic Campus, 1053 Carling Ave, Ottawa, Ontario, K1Y 4E9, Canada. E-mail [email protected]
What Is the Optimal Chest Compression Depth During Out-of-Hospital Cardiac Arrest Resuscitation of Adult Patients?
Ian G. Stiell, MD; Siobhan P. Brown, PhD; Graham Nichol, MD; Sheldon Cheskes, MD; Christian Vaillancourt, MD; Clifton W. Callaway, MD; Laurie J. Morrison, MD;
James Christenson, MD; Tom P. Aufderheide, MD; Daniel P. Davis, MD; Cliff Free, EMT-P; Dave Hostler, PhD; John A. Stouffer, EMT-P; Ahamed H. Idris, MD;
and the Resuscitation Outcomes Consortium Investigators
Resuscitation Science
at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from

Stiell et al CPR Compression Depth 1963
delivery of chest compressions is often poor.7,8 Recent tech-nological advances now allow for the detailed measurement and review of key compression parameters.9–11 Using this technology, Christenson et al12 and Vaillancourt et al13 dem-onstrated an association between outcomes of OHCA patients and the proportion of each resuscitation minute during which compressions were delivered (chest compression fraction). Cheskes et al14 found that longer perishock and preshock pauses were independently associated with a decrease in sur-vival to hospital discharge in patients presenting in a shock-able rhythm. Idris et al15 described an association between chest compression rate and return of spontaneous circulation.
Chest compression depth is another aspect of CPR for which data are limited. Current CPR guidelines for compression rate and depth have been, for the most part, derived with relatively little robust human data to support them.3,16 The 2005 guide-lines recommended a depth range of 38 to 50 mm, whereas the new 2010 guidelines recommend a depth of ≥50 mm (2 in) with no upper limit specified. For compression depth, clini-cal studies to date have been small, with insufficient power to evaluate clinically important outcomes.7,17–22 Our group stud-ied 1029 OHCA cases and found lower-than-recommended compression depth in half of patients by 2005 guideline stan-dards and almost all by 2010 standards, as well as an inverse association between compression depth and rate.23 We found a strong association between survival outcomes and increased compression depth but no clear evidence to support or refute the 2010 recommendations of >50 mm. Our objective for the current study was to determine the optimal compression depth for adults in a large sample of OHCA patients.
MethodsDesign and SettingThe Resuscitation Outcomes Consortium (ROC) is composed of 10 US and Canadian universities and their regional EMS systems and has a mandate to conduct large controlled trials of prehospital interven-tions for cardiac arrest and trauma. This study represents an analysis of consecutive OHCA cases prospectively gathered in the recent ROC Prehospital Resuscitation Impedance Valve and Early Versus Delayed Analysis (PRIMED) trial or in the ROC Epistry-Cardiac Arrest.24 The ROC PRIMED trial used a partial factorial design, whereby most patients were randomly assigned to 2 concurrent protocols. The first protocol compared early rhythm analysis versus later rhythm analy-sis, and the second protocol compared use of an impedance threshold device versus use of a sham impedance threshold device. The ROC Epistry is a prospective multicenter observational registry of OHCA in EMS agencies and receiving institutions and includes patient out-comes and electronic data on the CPR process.25
The ROC EMS network consists of 36 000 EMS professionals within 260 EMS agencies; provides coverage to an estimated 24 million people from urban, suburban, and rural communities; and transports patients to 287 different hospitals.26 This analysis included OHCA patients treated by EMS and for whom electronic compres-sion depth data were available. Sites that did not have the techni-cal capacity to measure compression depth were not included, and, hence, this study included data from 95 participating EMS agencies affiliated with 9 US and Canadian ROC sites. At the time of data collection, OHCA patients were being treated according to the 2005 guideline standards for compression depth (38–50 mm).
PopulationWe included all individuals from the ROC PRIMED trial or the ROC Epistry, ≥18 years of age, who experienced nontraumatic
cardiopulmonary arrest outside of the hospital within the catch-ment area of a participating ROC EMS agency and were treated with defibrillation or delivery of chest compressions by EMS providers. We included patients with any initial cardiac rhythm. We excluded patients who did not have attempts at resuscitation by EMS, with an obvious cause of arrest, whose arrests were EMS witnessed, who received a shock from a bystander-applied automated external defi-brillator, and anyone who had >5 minutes of EMS CPR before the pads were applied. We also excluded patients for who ≥1 minute of electronic CPR compression depth data were not available. These data may have been unavailable because some EMS agencies do not use defibrillators with accelerometers capable of measuring compres-sion depth or because of inadvertent failure to capture and transmit the data.
The ROC PRIMED trial and the ROC Epistry were reviewed and approved by the appropriate local institutional review boards (United States) or research ethics boards (Canada) without the need for informed consent from subjects. Strict confidentiality was maintained at all times, and no personal identifiers were retained in the database.
Data CollectionThe characteristics of chest compressions were measured via an accelerometer interface between the rescuer and the patient’s chest using commercially available defibrillators. Tracings were acquired and downloaded from Phillips (N=1869; Andover, MA) and ZOLL (N=7246; Chelmsford, MA) defibrillators.10,27 CPR process mea-sures, including compression rate, chest compression fraction, and compression depth, were calculated by proprietary automated exter-nal defibrillator analytic software. Chest compression fraction was defined as the proportion of resuscitation time without spontaneous circulation during which chest compressions were administered. Compression depth was defined as the posterior depression of the anterior chest wall in millimeters. The mean compression values for all minute intervals were averaged for each patient using all available minutes in the first 10 minutes after pads were placed. For compres-sion depth, we defined depth within the recommended range as per the 2005 international guidelines, with an average depth of ≥38 mm. We described the case as being within the recommended depth if the mean depth was ≥38 mm for >60% of the minutes recorded.
Patient and clinical data were abstracted from EMS and hospital records using standardized definitions for patient characteristics, EMS process, and outcome at hospital discharge. Data were abstracted locally, coded without personal health information, and transmitted to the data coordinating center electronically. Site-specific quality assur-ance included initial EMS provider training in data collection and continuing education of EMS providers. The data coordinating center assured the quality of the data by a variety of techniques.1
Outcome MeasuresThe primary outcome was survival to hospital discharge, defined as discharged alive from hospital after the index OHCA. Patients who were transferred to another acute care facility (eg, to undergo implant-able cardioverter defibrillator placement) were considered to still be hospitalized. Patients were considered discharged if transferred to a nonacute ward or facility. The secondary outcomes were survival to the next calendar day and return of spontaneous circulation (ROSC). Survival for 1 day meant that the patient was still alive 1 day past the date of the event. ROSC refers to the presence of a palpable pulse for any duration of time before arrival at the hospital. Data were abstracted from collated EMS and hospital source documents.
Statistical AnalysisAll of the statistical analyses were performed with commercially available statistical packages (SAS version 9.1.3; SAS Institute, Cary, NC; R version 2.14.1; R Foundation for Statistical Computing, Vienna, Austria). Summary results are presented as mean (±SD) or median (interquartile range). To test differences in baseline charac-teristics between subjects who did and did not survive to discharge, likelihood ratio χ2 tests or t tests were used as appropriate. ANOVA
at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from
1964 Circulation November 25, 2014
was used to compare mean compression depths across study sites. The association between depth and rate categories was tested with a likelihood ratio χ2 test. The association between compression depth (evaluated separately with 4 approaches) and outcomes of interest was quantified using multivariate logistic regression with the Huber-White sandwich SE.28 The key covariates/potential confounders assessed were age, sex, public location, bystander witnessed arrest, bystander CPR, EMS response time, CPR fraction, compression rate, site, and device manufacturer. We did not include cardiac rhythm, because this is potentially a path variable. Smoothing splines were used to explore the relationship between average compression depth and outcome, with a goal of finding the optimal 15-mm interval for depth.29 Smoothing splines were creating by including the b-spline basis for a natural cubic spline of depth in a logistic regression model in place of the other depth measures. Four degrees of freedom were used in the unadjusted models and 5 in the adjusted.
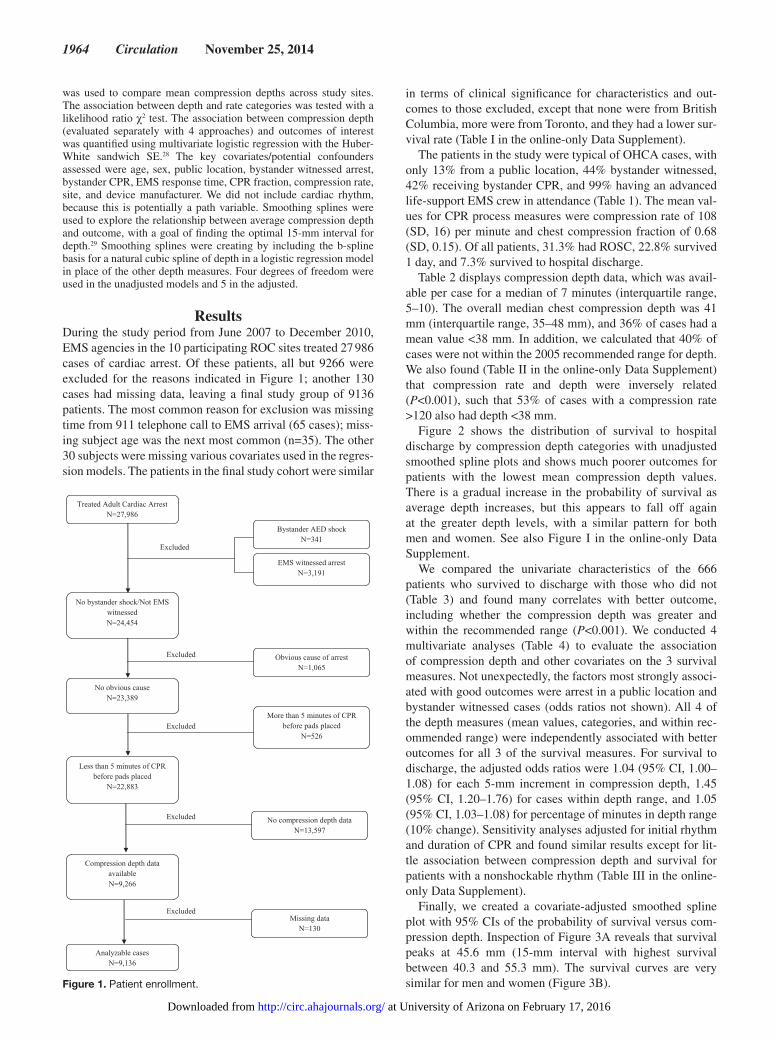
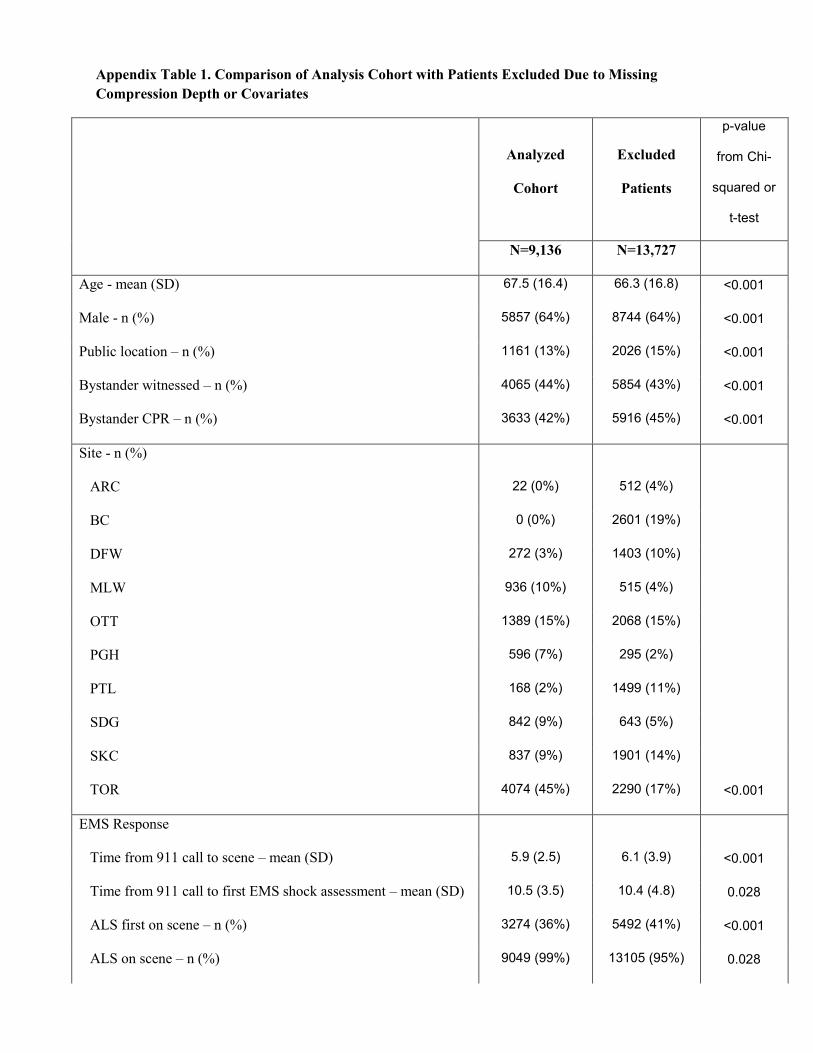
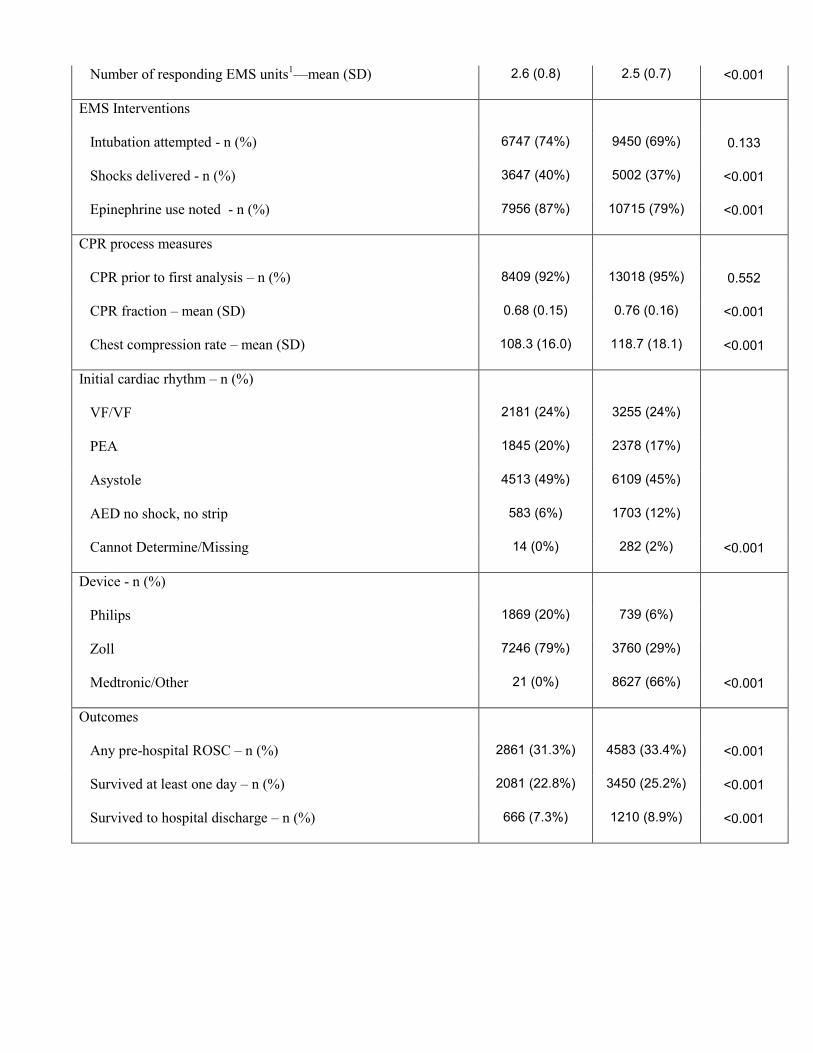
ResultsDuring the study period from June 2007 to December 2010, EMS agencies in the 10 participating ROC sites treated 27 986 cases of cardiac arrest. Of these patients, all but 9266 were excluded for the reasons indicated in Figure 1; another 130 cases had missing data, leaving a final study group of 9136 patients. The most common reason for exclusion was missing time from 911 telephone call to EMS arrival (65 cases); miss-ing subject age was the next most common (n=35). The other 30 subjects were missing various covariates used in the regres-sion models. The patients in the final study cohort were similar
in terms of clinical significance for characteristics and out-comes to those excluded, except that none were from British Columbia, more were from Toronto, and they had a lower sur-vival rate (Table I in the online-only Data Supplement).
The patients in the study were typical of OHCA cases, with only 13% from a public location, 44% bystander witnessed, 42% receiving bystander CPR, and 99% having an advanced life-support EMS crew in attendance (Table 1). The mean val-ues for CPR process measures were compression rate of 108 (SD, 16) per minute and chest compression fraction of 0.68 (SD, 0.15). Of all patients, 31.3% had ROSC, 22.8% survived 1 day, and 7.3% survived to hospital discharge.
Table 2 displays compression depth data, which was avail-able per case for a median of 7 minutes (interquartile range, 5–10). The overall median chest compression depth was 41 mm (interquartile range, 35–48 mm), and 36% of cases had a mean value <38 mm. In addition, we calculated that 40% of cases were not within the 2005 recommended range for depth. We also found (Table II in the online-only Data Supplement) that compression rate and depth were inversely related (P<0.001), such that 53% of cases with a compression rate >120 also had depth <38 mm.
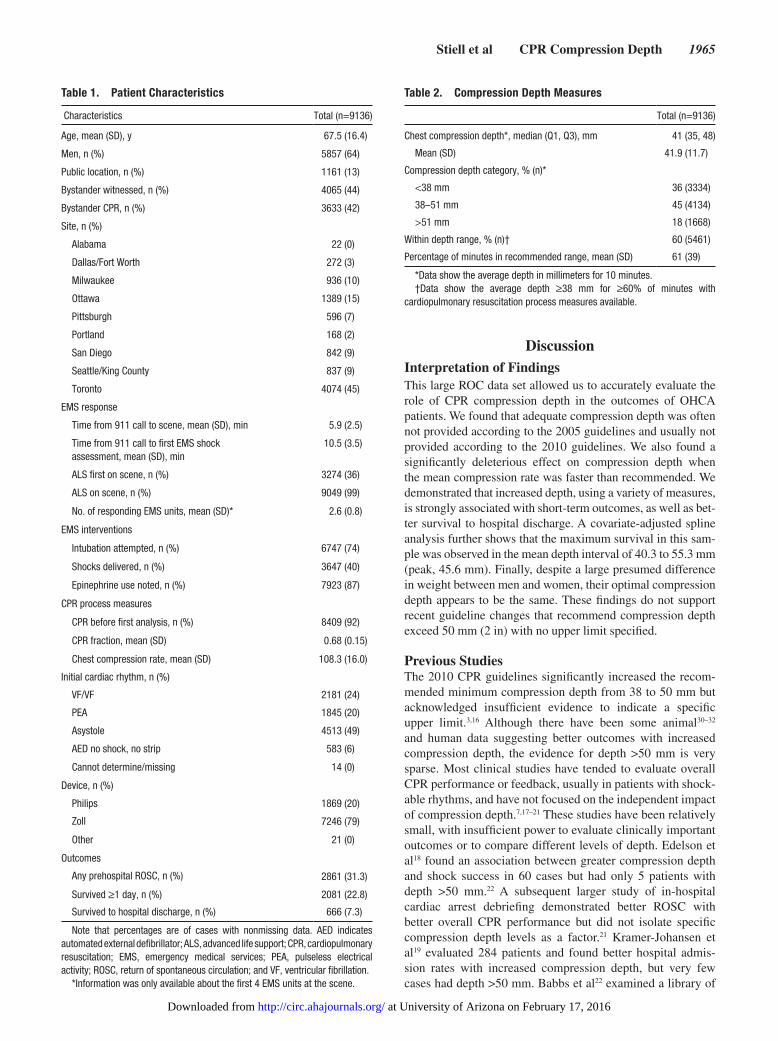
Figure 2 shows the distribution of survival to hospital discharge by compression depth categories with unadjusted smoothed spline plots and shows much poorer outcomes for patients with the lowest mean compression depth values. There is a gradual increase in the probability of survival as average depth increases, but this appears to fall off again at the greater depth levels, with a similar pattern for both men and women. See also Figure I in the online-only Data Supplement.
We compared the univariate characteristics of the 666 patients who survived to discharge with those who did not (Table 3) and found many correlates with better outcome, including whether the compression depth was greater and within the recommended range (P<0.001). We conducted 4 multivariate analyses (Table 4) to evaluate the association of compression depth and other covariates on the 3 survival measures. Not unexpectedly, the factors most strongly associ-ated with good outcomes were arrest in a public location and bystander witnessed cases (odds ratios not shown). All 4 of the depth measures (mean values, categories, and within rec-ommended range) were independently associated with better outcomes for all 3 of the survival measures. For survival to discharge, the adjusted odds ratios were 1.04 (95% CI, 1.00–1.08) for each 5-mm increment in compression depth, 1.45 (95% CI, 1.20–1.76) for cases within depth range, and 1.05 (95% CI, 1.03–1.08) for percentage of minutes in depth range (10% change). Sensitivity analyses adjusted for initial rhythm and duration of CPR and found similar results except for lit-tle association between compression depth and survival for patients with a nonshockable rhythm (Table III in the online-only Data Supplement).
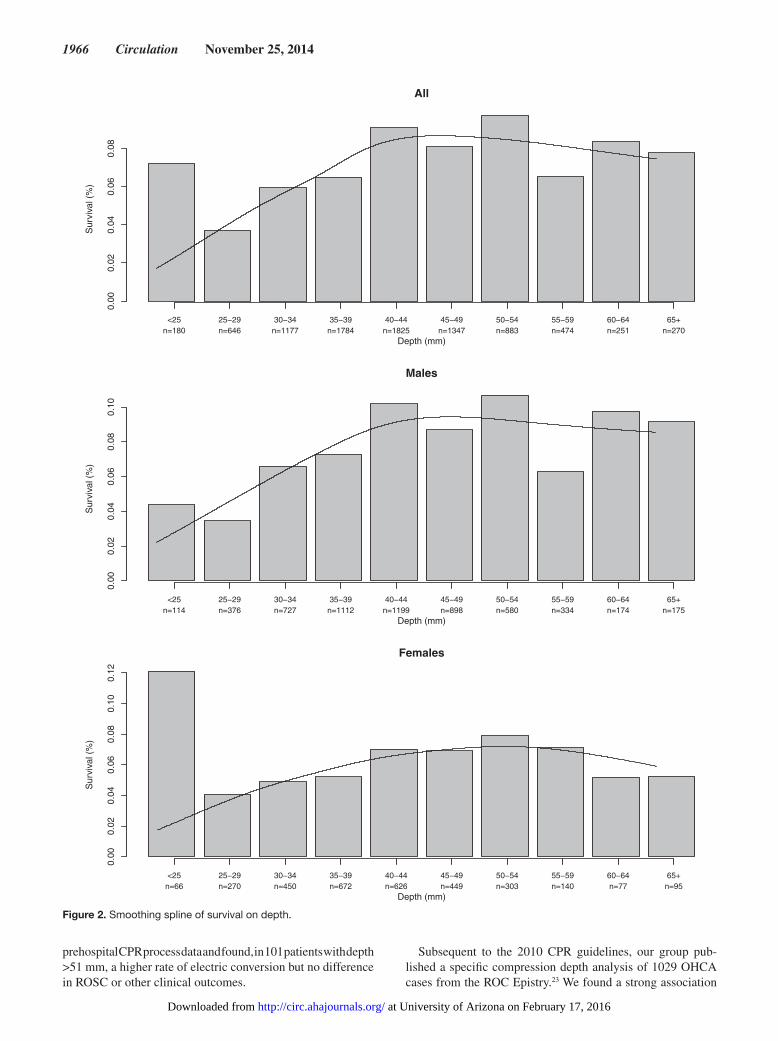
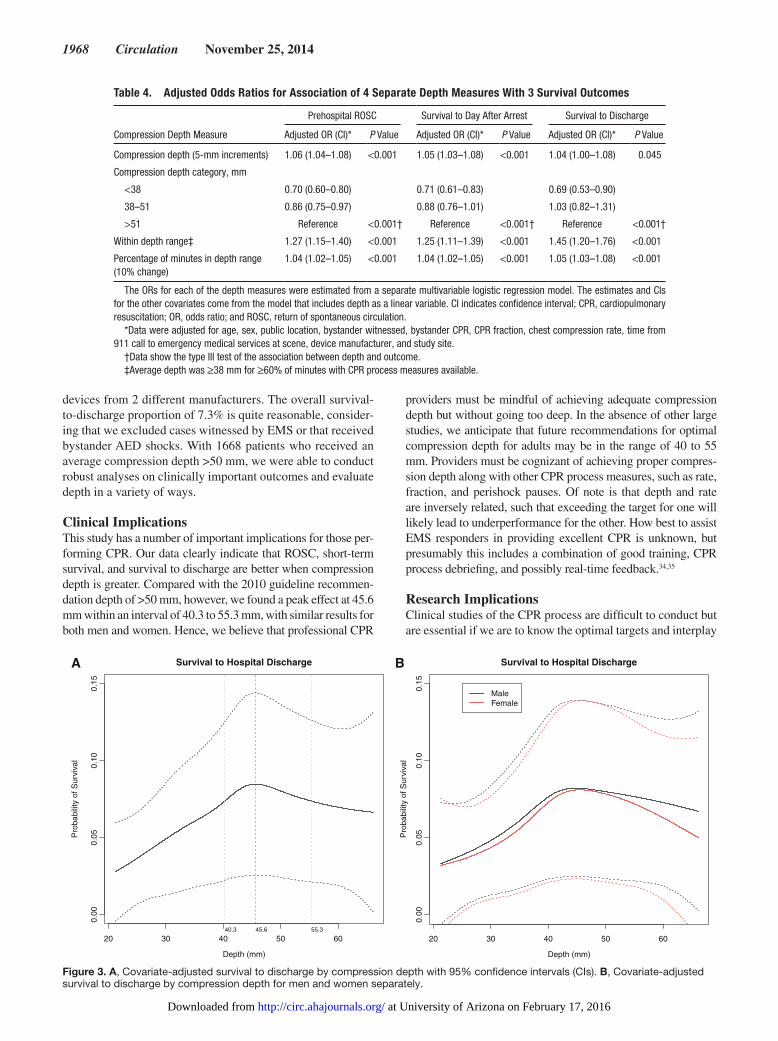
Finally, we created a covariate-adjusted smoothed spline plot with 95% CIs of the probability of survival versus com-pression depth. Inspection of Figure 3A reveals that survival peaks at 45.6 mm (15-mm interval with highest survival between 40.3 and 55.3 mm). The survival curves are very similar for men and women (Figure 3B).Figure 1. Patient enrollment.
at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from
Stiell et al CPR Compression Depth 1965
DiscussionInterpretation of FindingsThis large ROC data set allowed us to accurately evaluate the role of CPR compression depth in the outcomes of OHCA patients. We found that adequate compression depth was often not provided according to the 2005 guidelines and usually not provided according to the 2010 guidelines. We also found a significantly deleterious effect on compression depth when the mean compression rate was faster than recommended. We demonstrated that increased depth, using a variety of measures, is strongly associated with short-term outcomes, as well as bet-ter survival to hospital discharge. A covariate-adjusted spline analysis further shows that the maximum survival in this sam-ple was observed in the mean depth interval of 40.3 to 55.3 mm (peak, 45.6 mm). Finally, despite a large presumed difference in weight between men and women, their optimal compression depth appears to be the same. These findings do not support recent guideline changes that recommend compression depth exceed 50 mm (2 in) with no upper limit specified.
Previous StudiesThe 2010 CPR guidelines significantly increased the recom-mended minimum compression depth from 38 to 50 mm but acknowledged insufficient evidence to indicate a specific upper limit.3,16 Although there have been some animal30–32 and human data suggesting better outcomes with increased compression depth, the evidence for depth >50 mm is very sparse. Most clinical studies have tended to evaluate overall CPR performance or feedback, usually in patients with shock-able rhythms, and have not focused on the independent impact of compression depth.7,17–21 These studies have been relatively small, with insufficient power to evaluate clinically important outcomes or to compare different levels of depth. Edelson et al18 found an association between greater compression depth and shock success in 60 cases but had only 5 patients with depth >50 mm.22 A subsequent larger study of in-hospital cardiac arrest debriefing demonstrated better ROSC with better overall CPR performance but did not isolate specific compression depth levels as a factor.21 Kramer-Johansen et al19 evaluated 284 patients and found better hospital admis-sion rates with increased compression depth, but very few cases had depth >50 mm. Babbs et al22 examined a library of
Table 2. Compression Depth Measures
Total (n=9136)
Chest compression depth*, median (Q1, Q3), mm 41 (35, 48)
Mean (SD) 41.9 (11.7)
Compression depth category, % (n)*
<38 mm 36 (3334)
38–51 mm 45 (4134)
>51 mm 18 (1668)
Within depth range, % (n)† 60 (5461)
Percentage of minutes in recommended range, mean (SD) 61 (39)
*Data show the average depth in millimeters for 10 minutes.†Data show the average depth ≥38 mm for ≥60% of minutes with
cardiopulmonary resuscitation process measures available.
Table 1. Patient Characteristics
Characteristics Total (n=9136)
Age, mean (SD), y 67.5 (16.4)
Men, n (%) 5857 (64)
Public location, n (%) 1161 (13)
Bystander witnessed, n (%) 4065 (44)
Bystander CPR, n (%) 3633 (42)
Site, n (%)
Alabama 22 (0)
Dallas/Fort Worth 272 (3)
Milwaukee 936 (10)
Ottawa 1389 (15)
Pittsburgh 596 (7)
Portland 168 (2)
San Diego 842 (9)
Seattle/King County 837 (9)
Toronto 4074 (45)
EMS response
Time from 911 call to scene, mean (SD), min 5.9 (2.5)
Time from 911 call to first EMS shock assessment, mean (SD), min
10.5 (3.5)
ALS first on scene, n (%) 3274 (36)
ALS on scene, n (%) 9049 (99)
No. of responding EMS units, mean (SD)* 2.6 (0.8)
EMS interventions
Intubation attempted, n (%) 6747 (74)
Shocks delivered, n (%) 3647 (40)
Epinephrine use noted, n (%) 7923 (87)
CPR process measures
CPR before first analysis, n (%) 8409 (92)
CPR fraction, mean (SD) 0.68 (0.15)
Chest compression rate, mean (SD) 108.3 (16.0)
Initial cardiac rhythm, n (%)
VF/VF 2181 (24)
PEA 1845 (20)
Asystole 4513 (49)
AED no shock, no strip 583 (6)
Cannot determine/missing 14 (0)
Device, n (%)
Philips 1869 (20)
Zoll 7246 (79)
Other 21 (0)
Outcomes
Any prehospital ROSC, n (%) 2861 (31.3)
Survived ≥1 day, n (%) 2081 (22.8)
Survived to hospital discharge, n (%) 666 (7.3)
Note that percentages are of cases with nonmissing data. AED indicates automated external defibrillator; ALS, advanced life support; CPR, cardiopulmonary resuscitation; EMS, emergency medical services; PEA, pulseless electrical activity; ROSC, return of spontaneous circulation; and VF, ventricular fibrillation.
*Information was only available about the first 4 EMS units at the scene.
at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from
1966 Circulation November 25, 2014
prehospital CPR process data and found, in 101 patients with depth >51 mm, a higher rate of electric conversion but no difference in ROSC or other clinical outcomes.
Subsequent to the 2010 CPR guidelines, our group pub-lished a specific compression depth analysis of 1029 OHCA cases from the ROC Epistry.23 We found a strong association
All
Depth (mm)
Sur
viva
l (%
)
0.00
0.02
0.04
0.06
0.08
<25 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 65+n=180 n=646 n=1177 n=1784 n=1825 n=1347 n=883 n=474 n=251 n=270
Males
Depth (mm)
Sur
viva
l (%
)
0.00
0.02
0.04
0.06
0.08
0.10
<25 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 65+n=114 n=376 n=727 n=1112 n=1199 n=898 n=580 n=334 n=174 n=175
Females
Depth (mm)
Sur
viva
l (%
)
0.00
0.02
0.04
0.06
0.08
0.10
0.12
<25 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 65+n=66 n=270 n=450 n=672 n=626 n=449 n=303 n=140 n=77 n=95
Figure 2. Smoothing spline of survival on depth.
at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from
Stiell et al CPR Compression Depth 1967
between survival outcomes and increased compression depth but had insufficient power to identify the optimal compression depth for adult men or women.
Limitations and StrengthsThe study population represents a consecutive sample of cases from sites where compression depth could be measured and during a period when the 2005 guideline standards were in use. Regardless, we could detect no selection bias in our cases compared with those not included. Our records could not cap-ture CPR data before the placement of accelerometer pads, a time period estimated to be <30 seconds (median, 16 seconds;
mean, 29 seconds), and we did not examine data beyond 10 minutes of CPR. We did not have data for body size, firm-ness of the surface under the patient, leaning, or duty cycle, all possible confounders to the interpretation of compression depth data.33 We did, however, adjust for sex, which may be considered a crude proxy for weight, and found no difference between men and women. We had no measurements for chil-dren under age 18 years. We did not reliably capture data on whether device feedback was provided to providers.
The major strengths of the study include a large sample of patients with all initial rhythms, from 9 geographically dis-parate locations in the US and Canada, and receiving use of
Table 3. Univariate Comparison of Clinical Characteristics of Patients Who Did and Did Not Survive to Hospital Discharge
Outcome
Deaths (n=8470) Survivors (n=666) P Value From χ2 or t Test
Age, mean (SD), y 68.2 (16.3) 58.8 (15.3) <0.001
Men, n (%) 5387 (63.6) 470 (70.6) <0.001
Public location, n (%) 932 (11.0) 229 (34.4) <0.001
Bystander witnessed, n (%) 3546 (41.9) 519 (77.9) <0.001
Bystander CPR, n (%) 3269 (40.9) 364 (56.9) <0.001
EMS response
Time from 911 call to scene, mean (SD) 5.9 (2.5) 5.2 (2.0) <0.001
Time from 911 call to first EMS shock assessment, mean (SD) 10.6 (3.5) 9.2 (2.9) <0.001
ALS first on scene, n (%) 3017 (35.8) 257 (38.9) 0.258
ALS on scene, n (%) 8385 (99.0) 664 (99.7) 0.037
Number of responding EMS units, mean (SD)* 2.6 (0.8) 2.7 (0.8) <0.001
EMS interventions
Intubation attempted, n (%) 6274 (74.1) 473 (71.0) 0.088
Shocks delivered, n (%) 3099 (36.6) 548 (82.3) <0.001
Epinephrine use noted, n (%) 7547 (89.2) 376 (56.5) <0.001
CPR process measures
CPR before first analysis, n (%) 7796 (92.0) 613 (92.0) 1.000
CPR fraction, mean (SD) 0.69 (0.14) 0.64 (0.17) <0.001
Chest compression rate, mean (SD) 108.4 (16.0) 107.1 (16.1) 0.038
Chest compression depth, mean (SD), mm 41.8 (11.8) 43.5 (10.7) <0.001
Compression depth category, % (n)
<38 mm 3150 (37.2) 184 (27.6)
38–51 mm 3790 (44.7) 344 (51.7)
>51 mm 1530 (18.1) 138 (20.7) <0.001
Within recommended depth range, % (n)† 5006 (59.1) 455 (68.3) <0.001
Percentage of minutes in depth range, mean (SD) 61% (39) 69% (37) <0.001
Initial cardiac rhythm, n (%)
VF/VF 1670 (19.7) 511 (76.7)
PEA 1754 (20.7) 91 (13.7)
Asystole 4462 (52.7) 51 (7.7)
AED no shock, no strip 571 (6.7) 12 (1.8)
Cannot determine/missing 13 (0.2) 1 (0.2) <0.001
Note that percentages are of cases with nonmissing data. AED indicates automated external defibrillator; ALS, advanced life support; CPR, cardiopulmonary resuscitation; EMS, emergency medical services; PEA, pulseless electrical activity; ROSC, return of spontaneous circulation; and VF, ventricular fibrillation.
*Information was only available for the first 4 EMS units at the scene.†Average depth was ≥38 mm for ≥60% of minutes with CPR process measures available.
at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from
1968 Circulation November 25, 2014
devices from 2 different manufacturers. The overall survival-to-discharge proportion of 7.3% is quite reasonable, consider-ing that we excluded cases witnessed by EMS or that received bystander AED shocks. With 1668 patients who received an average compression depth >50 mm, we were able to conduct robust analyses on clinically important outcomes and evaluate depth in a variety of ways.
Clinical ImplicationsThis study has a number of important implications for those per-forming CPR. Our data clearly indicate that ROSC, short-term survival, and survival to discharge are better when compression depth is greater. Compared with the 2010 guideline recommen-dation depth of >50 mm, however, we found a peak effect at 45.6 mm within an interval of 40.3 to 55.3 mm, with similar results for both men and women. Hence, we believe that professional CPR
providers must be mindful of achieving adequate compression depth but without going too deep. In the absence of other large studies, we anticipate that future recommendations for optimal compression depth for adults may be in the range of 40 to 55 mm. Providers must be cognizant of achieving proper compres-sion depth along with other CPR process measures, such as rate, fraction, and perishock pauses. Of note is that depth and rate are inversely related, such that exceeding the target for one will likely lead to underperformance for the other. How best to assist EMS responders in providing excellent CPR is unknown, but presumably this includes a combination of good training, CPR process debriefing, and possibly real-time feedback.34,35
Research ImplicationsClinical studies of the CPR process are difficult to conduct but are essential if we are to know the optimal targets and interplay
Table 4. Adjusted Odds Ratios for Association of 4 Separate Depth Measures With 3 Survival Outcomes
Compression Depth Measure
Prehospital ROSC Survival to Day After Arrest Survival to Discharge
Adjusted OR (CI)* P Value Adjusted OR (CI)* P Value Adjusted OR (CI)* P Value
Compression depth (5-mm increments) 1.06 (1.04–1.08) <0.001 1.05 (1.03–1.08) <0.001 1.04 (1.00–1.08) 0.045
Compression depth category, mm
<38 0.70 (0.60–0.80) 0.71 (0.61–0.83) 0.69 (0.53–0.90)
38–51 0.86 (0.75–0.97) 0.88 (0.76–1.01) 1.03 (0.82–1.31)
>51 Reference <0.001† Reference <0.001† Reference <0.001†
Within depth range‡ 1.27 (1.15–1.40) <0.001 1.25 (1.11–1.39) <0.001 1.45 (1.20–1.76) <0.001
Percentage of minutes in depth range (10% change)
1.04 (1.02–1.05) <0.001 1.04 (1.02–1.05) <0.001 1.05 (1.03–1.08) <0.001
The ORs for each of the depth measures were estimated from a separate multivariable logistic regression model. The estimates and CIs for the other covariates come from the model that includes depth as a linear variable. CI indicates confidence interval; CPR, cardiopulmonary resuscitation; OR, odds ratio; and ROSC, return of spontaneous circulation.
*Data were adjusted for age, sex, public location, bystander witnessed, bystander CPR, CPR fraction, chest compression rate, time from 911 call to emergency medical services at scene, device manufacturer, and study site.
†Data show the type III test of the association between depth and outcome.‡Average depth was ≥38 mm for ≥60% of minutes with CPR process measures available.
20 30 40 50 60
0.00
0.05
0.10
0.15
SurvivA Bal to Hospital Discharge
Depth (mm)
Pro
babi
lity
of S
urvi
val
40.3 45.6 55.3
20 30 40 50 60
0.00
0.05
0.10
0.15
Survival to Hospital Discharge
Depth (mm)
Pro
babi
lity
of S
urvi
val
MaleFemale
Figure 3. A, Covariate-adjusted survival to discharge by compression depth with 95% confidence intervals (CIs). B, Covariate-adjusted survival to discharge by compression depth for men and women separately.
at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from

Stiell et al CPR Compression Depth 1969
among compression depth, compression rate, ventilations, compression fraction, duty cycle, and recoil. In addition, more data for children are required to understand the best CPR pro-cess parameters to optimize survival. Ultimately we need ran-domized intervention trials that evaluate the impact of different combinations of CPR process targets on patient survival.
ConclusionsThis large study of OHCA patients from a variety of set-tings demonstrated that increased CPR compression depth is strongly associated with better survival to hospital discharge. An adjusted analysis, however, found that maximum survival was in the mean depth interval of 40.3 to 55.3 mm (peak, 45.6 mm), suggesting that the 2010 American Heart Association CPR guideline target may be too high. We encourage the use of all validated strategies for prehospital and in-hospital car-diac arrest resuscitations to assist rescuers to stay within range for key CPR parameters.
AcknowledgmentsWe gratefully acknowledge the tremendous effort and contribu-tion of thousands of EMS providers and first responders who made this logistically challenging trial possible. We also thank Catherine Clement and Angela Marcantonio for their assistance with the article, as well as Tom Rea for insightful comments.
Sources of Funding The ROC is supported by a series of cooperative agreements to 10 regional clinical centers and 1 data coordinating center (5U01 HL077863, HL077881, HL077871 HL077872, HL077866, HL077908, HL077867, HL077885, HL077887, HL077873, and HL077865) from the National Heart, Lung, and Blood Institute in partnership with the National Institute of Neurological Disorders and Stroke, US Army Medical Research and Materiel Command, the Canadian Institutes of Health Research–Institute of Circulatory and Respiratory Health, Defense Research and Development Canada, the Heart and Stroke Foundation of Canada, and the American Heart Association.
DisclosuresNone.
References 1. Nichol G, Thomas E, Callaway CW, Hedges J, Powell JL, Aufderheide TP,
Rea T, Lowe R, Brown T, Dreyer J, Davis D, Idris A, Stiell I; Resuscitation Outcomes Consortium Investigators. Regional variation in out-of-hospital cardiac arrest incidence and outcome. JAMA. 2008;300:1423–1431.
2. Cummins RO, Ornato JP, Thies WH, Pepe PE. Improving survival from sudden cardiac arrest: the “chain of survival” concept. Circulation. 1991;83:1832–1847.
3. 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2005;112:IV1–203.
4. Stiell IG, Wells GA, Field B, Spaite DW, Nesbitt LP, De Maio VJ, Nichol G, Cousineau D, Blackburn J, Munkley D, Luinstra-Toohey L, Campeau T, Dagnone E, Lyver M; Ontario Prehospital Advanced Life Support Study Group. Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004;351:647–656.
5. Rea TD, Cook AJ, Stiell IG, Powell J, Bigham B, Callaway CW, Chugh S, Aufderheide TP, Morrison L, Terndrup TE, Beaudoin T, Wittwer L, Davis D, Idris A, Nichol G; Resuscitation Outcomes Consortium Investigators. Predicting survival after out-of-hospital cardiac arrest: role of the Utstein data elements. Ann Emerg Med. 2010;55:249–257.
6. Peberdy MA, Ornato JP. Post-resuscitation care: is it the missing link in the Chain of Survival? Resuscitation. 2005;64:135–137.
7. Wik L, Kramer-Johansen J, Myklebust H, Sørebø H, Svensson L, Fellows B, Steen PA. Quality of cardiopulmonary resuscitation during out-of- hospital cardiac arrest. JAMA. 2005;293:299–304.
8. Abella BS, Sandbo N, Vassilatos P, Alvarado JP, O’Hearn N, Wigder HN, Hoffman P, Tynus K, Vanden Hoek TL, Becker LB. Chest compression rates during cardiopulmonary resuscitation are suboptimal: a prospective study during in-hospital cardiac arrest. Circulation. 2005;111:428–434.
9. Kramer-Johansen J, Edelson DP, Losert H, Köhler K, Abella BS. Uniform reporting of measured quality of cardiopulmonary resuscitation (CPR). Resuscitation. 2007;74:406–417.
10. Aase SO, Myklebust H. Compression depth estimation for CPR quality assessment using DSP on accelerometer signals. IEEE Trans Biomed Eng. 2002;49:263–268.
11. Ornato JP, Peberdy MA. Measuring progress in resuscitation: it’s time for a better tool. Circulation. 2006;114:2754–2756.
12. Christenson J, Andrusiek D, Everson-Stewart S, Kudenchuk P, Hostler D, Powell J, Callaway CW, Bishop D, Vaillancourt C, Davis D, Aufderheide TP, Idris A, Stouffer JA, Stiell I, Berg R; Resuscitation Outcomes Consortium Investigators. Chest compression fraction determines sur-vival in patients with out-of-hospital ventricular fibrillation. Circulation. 2009;120:1241–1247.
13. Vaillancourt C, Everson-Stewart S, Christenson J, Andrusiek D, Powell J, Nichol G, Cheskes S, Aufderheide TP, Berg R, Stiell IG. The impact of increased chest compression fraction on return of spontaneous circulation for out-of-hospital cardiac arrest patients not in ventricular fibrillation. Resuscitation. 2011;82:1501–1507.
14. Cheskes S, Schmicker RH, Christenson J, Salcido DD, Rea T, Powell J, Edelson DP, Sell R, May S, Menegazzi JJ, Van Ottingham L, Olsufka M, Pennington S, Simonini J, Berg RA, Stiell I, Idris A, Bigham B, Morrison L; Resuscitation Outcomes Consortium (ROC) Investigators. Perishock pause: an independent predictor of survival from out-of-hospital shock-able cardiac arrest. Circulation. 2011;124:58–66.
15. Idris AH, Guffey D, Aufderheide TP, Brown S, Morrison LJ, Nichols P, Powell J, Daya M, Bigham BL, Atkins DL, Berg R, Davis D, Stiell I, Sopko G, Nichol G; Resuscitation Outcomes Consortium (ROC) Investigators. Relationship between chest compression rates and outcomes from cardiac arrest. Circulation. 2012;125:3004–3012.
16. Sayre MR, Koster RW, Botha M, Cave DM, Cudnik MT, Handley AJ, Hatanaka T, Hazinski MF, Jacobs I, Monsieurs K, Morley PT, Nolan JP, Travers AH; Adult Basic Life Support Chapter Collaborators. Part 5: adult basic life support–2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2010;122(16 suppl 2):S298–S324.
17. Abella BS, Alvarado JP, Myklebust H, Edelson DP, Barry A, O’Hearn N, Vanden Hoek TL, Becker LB. Quality of cardiopulmonary resuscitation during in-hospital cardiac arrest. JAMA. 2005;293:305–310.
18. Edelson DP, Abella BS, Kramer-Johansen J, Wik L, Myklebust H, Barry AM, Merchant RM, Hoek TL, Steen PA, Becker LB. Effects of compres-sion depth and pre-shock pauses predict defibrillation failure during car-diac arrest. Resuscitation. 2006;71:137–145.
19. Kramer-Johansen J, Myklebust H, Wik L, Fellows B, Svensson L, Sørebø H, Steen PA. Quality of out-of-hospital cardiopulmonary resuscitation with real time automated feedback: a prospective interventional study. Resuscitation. 2006;71:283–292.
20. Olasveengen TM, Tomlinson AE, Wik L, Sunde K, Steen PA, Myklebust H, Kramer-Johansen J. A failed attempt to improve quality of out-of-hospital CPR through performance evaluation. Prehosp Emerg Care. 2007;11:427–433.
21. Edelson DP, Litzinger B, Arora V, Walsh D, Kim S, Lauderdale DS, Vanden Hoek TL, Becker LB, Abella BS. Improving in-hospital cardiac arrest process and outcomes with performance debriefing. Arch Intern Med. 2008;168:1063–1069.
22. Babbs CF, Kemeny AE, Quan W, Freeman G. A new paradigm for human resuscitation research using intelligent devices. Resuscitation. 2008;77:306–315.
23. Stiell IG, Brown SP, Christenson J, Cheskes S, Nichol G, Powell J, Bigham B, Morrison LJ, Larsen J, Hess E, Vaillancourt C, Davis DP, Callaway CW; Resuscitation Outcomes Consortium (ROC) Investigators. What is the role of chest compression depth during out-of-hospital cardiac arrest resuscitation? Crit Care Med. 2012;40:1192–1198.
24. Stiell IG, Nichol G, Leroux BG, Rea TD, Ornato JP, Powell J, Christenson J, Callaway CW, Kudenchuk PJ, Aufderheide TP, Idris AH, Daya MR, Wang HE, Morrison LJ, Davis D, Andrusiek D, Stephens S, Cheskes S, Schmicker RH, Fowler R, Vaillancourt C, Hostler D, Zive D, Pirrallo RG, Vilke GM, Sopko G, Weisfeldt M; ROC Investigators. Early versus later
at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from

1970 Circulation November 25, 2014
rhythm analysis in patients with out-of-hospital cardiac arrest. N Engl J Med. 2011;365:787–797.
25. Morrison LJ, Nichol G, Rea TD, Christenson J, Callaway CW, Stephens S, Pirrallo RG, Atkins DL, Davis DP, Idris AH, Newgard C; ROC Investigators. Rationale, development and implementation of the Resuscitation Outcomes Consortium Epistry-Cardiac Arrest. Resuscitation. 2008;78:161–169.
26. Davis DP, Garberson LA, Andrusiek DL, Hostler D, Daya M, Pirrallo R, Craig A, Stephens S, Larsen J, Drum AF, Fowler R. A descriptive analysis of Emergency Medical Service Systems participating in the Resuscitation Outcomes Consortium (ROC) network. Prehosp Emerg Care. 2007;11:369–382.
27. ZOLL Medical Corporation. E Series Operators Guide. Chelmsford, MA: ZOLL Medical Corporation; 2010.
28. Huber P. Robust Statistics. New York, NY: Wiley; 1981. 29. Hastie TJ. Generalized additive models. In: S. Chambers JM, Hastie TJ, eds.
Statistical Models. Pacific Grove, CA: Wadsworth & Brooks/Cole. 1992. 30. Li Y, Ristagno G, Bisera J, Tang W, Deng Q, Weil MH. Electrocardiogram
waveforms for monitoring effectiveness of chest compression during car-diopulmonary resuscitation. Crit Care Med. 2008;36:211–215.
31. Ristagno G, Tang W, Chang YT, Jorgenson DB, Russell JK, Huang L, Wang T, Sun S, Weil MH. The quality of chest compressions during car-diopulmonary resuscitation overrides importance of timing of defibrilla-tion. Chest. 2007;132:70–75.
32. Wu JY, Li CS, Liu ZX, Wu CJ, Zhang GC. A comparison of 2 types of chest compressions in a porcine model of cardiac arrest. Am J Emerg Med. 2009;27:823–829.
33. Perkins G, Kocierz L, Smith S, McCulloch R, Davies R. Compression feedback devices over estimate chest compression depth when performed on a bed. Resuscitation. 2009;80:79–82.
34. Hostler D, Everson-Stewart S, Rea TD, Stiell IG, Callaway CW, Kudenchuk PJ, Sears GK, Emerson SS, Nichol G; Resuscitation Outcomes Consortium Investigators. Effect of real-time feedback during cardiopul-monary resuscitation outside hospital: prospective, cluster-randomised trial. BMJ. 2011;342:d512.
35. Bobrow BJ, Vadeboncoeur TF, Stolz U, Silver AE, Tobin JM, Crawford SA, Mason TK, Schirmer J, Smith GA, Spaite DW. The influence of sce-nario-based training and real-time audiovisual feedback on out-of-hospital cardiopulmonary resuscitation quality and survival from out-of-hospital cardiac arrest. Ann Emerg Med. 2013;62:47–56.e1.
CLINICAL PeRSPeCTIveThe 2010 American Heart Association cardiopulmonary resuscitation (CPR) guidelines recommended a CPR compres-sion depth for adults of ≥50 mm (2 in), with no upper limit specified, although this was based on limited human data. This study of 9136 adult out-of-hospital cardiac arrest patients from 9 US and Canadian cities in the Resuscitation Outcomes Consortium found that adequate compression was often not provided, particularly when the compression rate was faster than recommended. The study clearly demonstrated that increased CPR compression depth is strongly associated with better survival to hospital discharge. In addition, however, analyses showed that the maximum survival was observed in the mean depth interval of 40.3 to 55.3 mm (peak, 45.6 mm). Finally, despite a large presumed difference in weight between men and women, their optimal compression depth appeared to be the same. The authors conclude that the 2010 American Heart Association CPR guideline target for compression depth may be too high. They encourage the use of all validated strategies for prehospital and in-hospital cardiac arrest resuscitations to assist rescuers to stay within range for key CPR parameters, including compression depth and rate.
at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from

and the Resuscitation Outcomes Consortium InvestigatorsDavis, Cliff Free, Dave Hostler, John A. Stouffer and Ahamed H. Idris
Clifton W. Callaway, Laurie J. Morrison, James Christenson, Tom P. Aufderheide, Daniel P. Ian G. Stiell, Siobhan P. Brown, Graham Nichol, Sheldon Cheskes, Christian Vaillancourt,
Resuscitation of Adult Patients?What Is the Optimal Chest Compression Depth During Out-of-Hospital Cardiac Arrest
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2014 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.114.008671
2014;130:1962-1970; originally published online September 24, 2014;Circulation.
http://circ.ahajournals.org/content/130/22/1962World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2014/09/24/CIRCULATIONAHA.114.008671.DC1.htmlData Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
at University of Arizona on February 17, 2016http://circ.ahajournals.org/Downloaded from
SUPPLEMENTAL MATERIAL

APPENDICES
Supplemental Methods
Summary results are presented as mean (±SD) or median (IQR). To test differences in
baseline characteristics between subjects who were included in the analysis and those excluded
due to missing data, likelihood ratio chi-squared tests or t-tests were used as appropriate. The
association between compression depth (evaluated separately with four approaches) and
outcomes of interest was quantified using multivariate logistic regression with the Huber-White
sandwich standard error.1 The key covariates/potential confounders assessed were age, sex,
public location, bystander witnessed arrest, bystander CPR, EMS response time, CPR fraction,
compression rate, site, and device manufacturer. Additional sensitivity analyses adjusted for
initial cardiac rhythm and duration of CPR. Smoothing splines were used to explore the
relationship between average compression depth and outcome.2 Unadjusted smoothing splines
were creating by including the b-spline basis with four degrees of freedom for a natural cubic
spline of depth in a logistic regression model in place of the other depth measures.
Supplemental References
1. Huber P. Robust Statistics. 1981. Wiley, New York.
2. Hastie TJ. Generalized additive models. In: Statistical Models in S. Chambers JM, Hastie TJ, eds.
1992. Wadsworth & Brooks/Cole, Pacific Grove, California.
Appendix Table 1. Comparison of Analysis Cohort with Patients Excluded Due to Missing
Compression Depth or Covariates
Analyzed
Cohort
Excluded
Patients
p-value
from Chi-
squared or
t-test
N=9,136 N=13,727
Age - mean (SD) 67.5 (16.4) 66.3 (16.8) <0.001
Male - n (%) 5857 (64%) 8744 (64%) <0.001
Public location – n (%) 1161 (13%) 2026 (15%) <0.001
Bystander witnessed – n (%) 4065 (44%) 5854 (43%) <0.001
Bystander CPR – n (%) 3633 (42%) 5916 (45%) <0.001
Site - n (%)
ARC 22 (0%) 512 (4%)
BC 0 (0%) 2601 (19%)
DFW 272 (3%) 1403 (10%)
MLW 936 (10%) 515 (4%)
OTT 1389 (15%) 2068 (15%)
PGH 596 (7%) 295 (2%)
PTL 168 (2%) 1499 (11%)
SDG 842 (9%) 643 (5%)
SKC 837 (9%) 1901 (14%)
TOR 4074 (45%) 2290 (17%) <0.001
EMS Response
Time from 911 call to scene – mean (SD) 5.9 (2.5) 6.1 (3.9) <0.001
Time from 911 call to first EMS shock assessment – mean (SD) 10.5 (3.5) 10.4 (4.8) 0.028
ALS first on scene – n (%) 3274 (36%) 5492 (41%) <0.001
ALS on scene – n (%) 9049 (99%) 13105 (95%) 0.028
Number of responding EMS units1—mean (SD) 2.6 (0.8) 2.5 (0.7) <0.001
EMS Interventions
Intubation attempted - n (%) 6747 (74%) 9450 (69%) 0.133
Shocks delivered - n (%) 3647 (40%) 5002 (37%) <0.001
Epinephrine use noted - n (%) 7956 (87%) 10715 (79%) <0.001
CPR process measures
CPR prior to first analysis – n (%) 8409 (92%) 13018 (95%) 0.552
CPR fraction – mean (SD) 0.68 (0.15) 0.76 (0.16) <0.001
Chest compression rate – mean (SD) 108.3 (16.0) 118.7 (18.1) <0.001
Initial cardiac rhythm – n (%)
VF/VF 2181 (24%) 3255 (24%)
PEA 1845 (20%) 2378 (17%)
Asystole 4513 (49%) 6109 (45%)
AED no shock, no strip 583 (6%) 1703 (12%)
Cannot Determine/Missing 14 (0%) 282 (2%) <0.001
Device - n (%)
Philips 1869 (20%) 739 (6%)
Zoll 7246 (79%) 3760 (29%)
Medtronic/Other 21 (0%) 8627 (66%) <0.001
Outcomes
Any pre-hospital ROSC – n (%) 2861 (31.3%) 4583 (33.4%) <0.001
Survived at least one day – n (%) 2081 (22.8%) 3450 (25.2%) <0.001
Survived to hospital discharge – n (%) 666 (7.3%) 1210 (8.9%) <0.001

Appendix Table 2. Compression Rate versus Compression Depth
Average Compression Rate / Minute
0 to 80 81 to 120 121+ Total
Average
Compression
Depth
<38 mm 45% (109) 32% (2256) 53% (969) 36% (3334)
38-51
mm
30% (73) 48% (3405) 36% (656) 45% (4134)
>51 mm 24% (58) 20% (1418) 11% (192) 18% (1668)
Total 100%
(240)
100%
(7079)
100%
(1817)
100%
(9136)
Chi-square test for association: p < 0.001
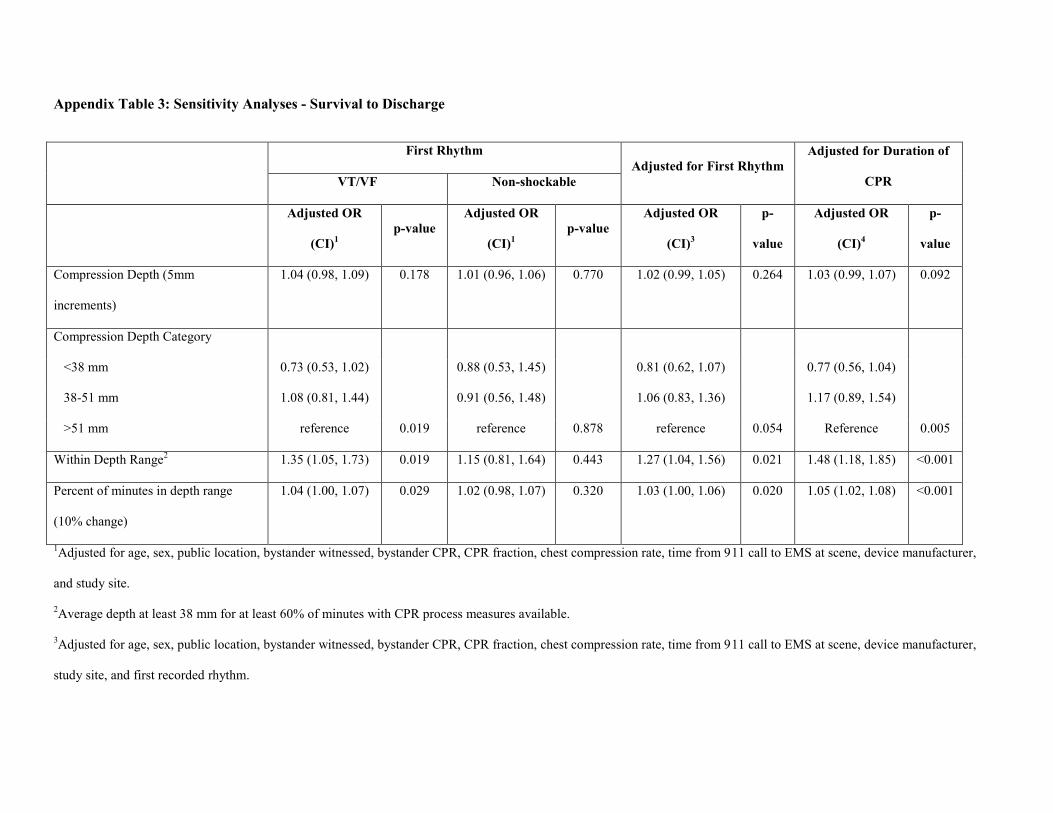
Appendix Table 3: Sensitivity Analyses - Survival to Discharge
First Rhythm
Adjusted for First Rhythm
Adjusted for Duration of
CPR VT/VF Non-shockable
Adjusted OR
(CI)1
p-value
Adjusted OR
(CI)1
p-value
Adjusted OR
(CI)3
p-
value
Adjusted OR
(CI)4
p-
value
Compression Depth (5mm
increments)
1.04 (0.98, 1.09) 0.178 1.01 (0.96, 1.06) 0.770 1.02 (0.99, 1.05) 0.264 1.03 (0.99, 1.07) 0.092
Compression Depth Category
<38 mm 0.73 (0.53, 1.02) 0.88 (0.53, 1.45) 0.81 (0.62, 1.07) 0.77 (0.56, 1.04)
38-51 mm 1.08 (0.81, 1.44) 0.91 (0.56, 1.48) 1.06 (0.83, 1.36) 1.17 (0.89, 1.54)
>51 mm reference 0.019 reference 0.878 reference 0.054 Reference 0.005
Within Depth Range2 1.35 (1.05, 1.73) 0.019 1.15 (0.81, 1.64) 0.443 1.27 (1.04, 1.56) 0.021 1.48 (1.18, 1.85) <0.001
Percent of minutes in depth range
(10% change)
1.04 (1.00, 1.07) 0.029 1.02 (0.98, 1.07) 0.320 1.03 (1.00, 1.06) 0.020 1.05 (1.02, 1.08) <0.001
1Adjusted for age, sex, public location, bystander witnessed, bystander CPR, CPR fraction, chest compression rate, time from 911 call to EMS at scene, device manufacturer,
and study site.
2Average depth at least 38 mm for at least 60% of minutes with CPR process measures available.
3Adjusted for age, sex, public location, bystander witnessed, bystander CPR, CPR fraction, chest compression rate, time from 911 call to EMS at scene, device manufacturer,
study site, and first recorded rhythm.
4Adjusted for age, sex, public location, bystander witnessed, bystander CPR, CPR fraction, chest compression rate, time from 911 call to EMS at scene, device manufacturer,
study site, and duration of CPR. Excludes 97 subjects who are missing duration of CPR.
The odds ratios for each of the depth measures was estimated from a separate multivariable logistic regression model.
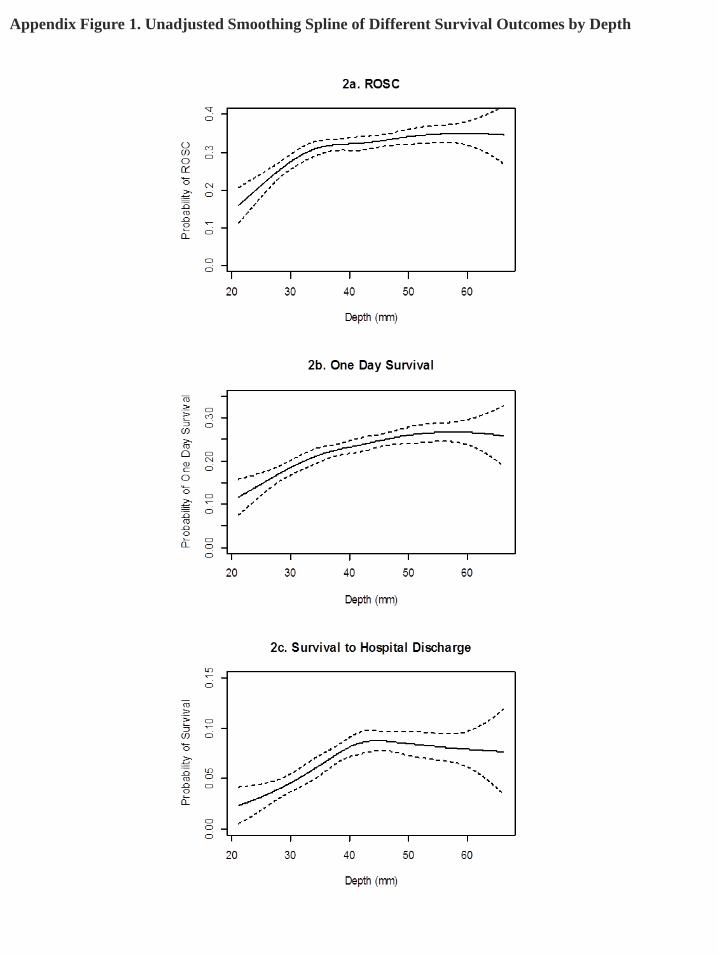
Appendix Figure 1. Unadjusted Smoothing Spline of Different Survival Outcomes by Depth
ROC PRIMED-ITD-ALvAE Appendix – 8/10/2010
ROC PRIMED-Appendix—12/22/2011 (for more information please go to the ROC website at www.uwctc.org and click on ROC) Alabama Resuscitation Center, University of Alabama at Birmingham, Birmingham, AL: Jeffrey D. Kerby, MD, PhD, Principal Investigator
Core Investigators: Henry E. Wang, MD, Todd B. Brown, MD, MSPH
Coordinators: Shannon W. Stephens, EMT-P, Carolyn R. Williams, BSN, BSME, Sandra Caldwell, MA, Katherine R. Lai, BS, Randal Gray, NREMT-P, MA Ed EMS Investigators/Collaborators: Joe E. Acker, EMT-P, MPH, Michael L. Minor, EMT-P, John Reed, BSN, EMT-P
Hospital Investigators/Collaborators: Jason Begue, MD, Willie Gilford, MD Participating EMS Agencies: Bessemer Fire Dept, Birmingham Fire and Rescue, Center Point Fire District, Pelham Fire Dept, Regional Paramedical Services, Rocky Ridge Fire District, Vestavia Hills Fire Dept, Hoover Fire Dept Dallas Center for Resuscitation Research, University of Texas Southwestern Medical Center, Dallas, TX: Ahamed H. Idris, MD, Principal Investigator
Core Investigators: Raymond Fowler, MD, Ronna Miller, MD, Joseph Minei, MD, Paul Pepe, MD, Michael Ramsay, MD, Robert Simonson, MD, Jane Wigginton, MD
Coordinators: Sarah Beadle, MD, Dixie Climer, RN, Melinda Moffat, RN, Pamela Owens, David Gallegos, Sandra O’Neill, MS, MA, LP, Ron Smith, MBA
EMS Investigators/Collaborators: Fernando Benitez, MD, Billy Craft, EMTP, Lucy Detamble, RN, Steven Deutsch, EMT-P, Tod Gillam, EMT-P Tony Harvey, EMTP, Suzanne Hewitt, RN, Marshal Isaacs, MD, Tami Kayea, EMTP, Richard LaChance, EMTP, Thomas Lehman, Dorothy Lemecha, MD, Chris Malvik, EMT-P, Paul Mayer, MD, Jeffrey Metzger, MD, Danny Miller, EMTP, Bobby Muse, EMT-P, Karen Pickard, RN, Bobby Ross, EMT-P, Chris Vinson, EMTP Hospital Investigators/Collaborators: Steven Arze, MD, Sean Black, MD, Matthew Bush, MD, Ralph Kelly, DO, Edward Thornton, MD, William Elder. MD, John Marcucci, MD, Lawrence Hum, MD, Mark Gamber, MD Participating EMS Agencies: Carrollton Fire Dept, Dallas Fire Rescue, Irving Fire Dept, Mesquite Fire Dept Milwaukee Resuscitation Research Center, Medical College of Wisconsin, Milwaukee, WI: Tom P. Aufderheide, MD, Principal Investigator
ROC PRIMED-ITD-ALvAE Appendix – 8/10/2010 Page 2 of 6
Core Investigators: Ronald G. Pirrallo, MD, MHSA, Karen J. Brasel, MD, MPH, Andrea L. Winthrop, MD, John P. Klein, PhD Coordinators: Joseph Brandt, BS, NREMT-P, Walter Bialkowski, MS, Jennifer Noldin, BS, Christopher Sandoval, BS, Kevin Morrow, MFA, David J. Kitscha, BS, MS, Barbara J. Burja, BA, EMT, Chris von Briesen, BA, CCRC, Christopher W. Sparks, Pamela Walsh, EMT EMS Investigators/Collaborators: John Chianelli, MS, Rosemarie Forster, MSOLQ, RHIA, EMT-P, Michael Milbrath, EMT-P, Lauryl Pukansky, BS, RHIA, Kenneth Sternig, MS-EHS, BSN, EMT-P, Eugene Chin, RN, EMT-P, Nancy Frieberg, RN, EMT-P, Kim Krueger, RN, EMT-P, Del Szewczuga, RN, EMT-P, Thomas Duerr, Rebecca Funk, BS, RHIA, EMT-B, Gail Jacobsen, BS, Janis Spitzer, Richard Demien, James Martins, John Cohn, Russell R. Spahn, M.A., EMT-P, Mike Jankowski, B.A., EMT-P, Timothy James, William E. Wentlandt Jr., MBA, EFO, David Berousek, Brian M. Satula, B.A., NREMT, Jay B. Behling, B.S., EMT-B, Dean K. Redman, B.A., EFO, Steven Hook, BS, CFOD, Andrew Neargarder, Jim Singer, RN Hospital Investigators/Collaborators: Thomas Reminga, MD, Dennis Shepherd, MD, Peter Holzhauer, MD, Jonathan Rubin, MD, Craig Skold, MD, Orlando Alvarez, MD, Heidi Harkins, MD, Edward Barthell, MD, William Haselow, MD, Albert Yee, MD, John Whitcomb, MD, Eduardo E. Castro, MD, Steven Motarjeme, MD, Paul Coogan, MD, Keith Rader, MD, Jeff Glaspy, MD, Gary Gerschke, MD, Howie Croft, MD, Mike Brin, MD, Cory Wilson, MD, Anne Johnson, MD, William Kumprey, MD Participating EMS Agencies: Cudahy Fire Dept, Franklin Fire Dept, Greendale Fire Dept, Greenfield Fire Dept, Hales Corners Fire Dept, Milwaukee County Airport Fire Dept, Milwaukee Fire Dept, North Shore Fire Dept, Oak Creek Fire Dept, South Milwaukee Fire Dept, Wauwatosa Fire Dept, West Allis Fire Dept Ottawa/OPALS/British Columbia RCC, Ottawa Health Research Institute, University of Ottawa, Ottawa, Ontario and St. Paul’s Hospital, University of British Columbia, British Columbia, Canada: Ian Stiell, MD, Principal Investigator Core Investigators: Jim Christenson, MD, Christian Vaillancourt, MD Coordinators: Cathy Clement, RN, Tammy Beaudoin, CCHRA, Marc-Andre Da Ponti, A-EMCA, ACP, Julie Cummins, A-EMCA, RN, MSc, Sarah Pennington, RN, Helen Connolly, RN, Stanley Morrow, A-EMCA, ACP, Christine Tym, CHIM, Ghislaine Lepage, CHIM, Jane Banek, CHIM EMS Investigators/Collaborators: Jonathan Dreyer, MD, Douglas Munkley, MD, Jason Prpic, MD, Justin Maloney, MD, Paul Colella, MD, Andrew Affleck, MD, David Waldbillig, MD, Paul Bradford, MD, Kenneth Boyle, EMCA, RRT, CMA, Lorie Luinstra-Toohey, BScN, MHA, John Trickett, BScN, Nicole Sykes, BScN, RN, Elaine Graham, ACP, Kieran Ballah, EMCA, Cathie Hedges, A-EMCA, ACP, Renee MacPhee, PhD, Bob DeRaad, RN, Dug Andrusiek, PCP, Dan Bishop, ACP, Ron Straight, ACP, Brian Twaites, ACP, Stuart Donn, PhD, Laura McCleary, ACP Participating EMS Agencies: Ottawa-OPALS-London Fire Dept, Ottawa Fire Rescue, Windsor Fire Rescue, Cambridge Fire Dept, Niagara Falls Fire Rescue, St Catharine's Fire Rescue,
ROC PRIMED-ITD-ALvAE Appendix – 8/10/2010 Page 3 of 6
Sudbury Fire Rescue, Thorold Fire Dept, Thunder Bay Fire Rescue, Waterloo Fire Rescue, Welland Fire Rescue, Niagara EMS, Prescott-Russell EMS, Sudbury EMS, Superior North EMS, Waterloo Regional EMS, AA and M Volunteer Ambulance, Essex-Windsor EMS, Harrow Ambulance Service, Ottawa Paramedic Service, Sun Parlour EMS, Thames EMS, Port Colborne Fire Vancouver BC-Abbotsford Fire Dept, Aggassiz Valley Fire Dept, Burnaby Fire Dept, City of North Vancouver Fire Dept, BC Ambulance, Coquitlam Fire Dept, Delta Fire Dept, Langley City Fire Dept, Langley Township Fire Dept, Maple Ridge Fire Dept, Mission Fire Dept, New Westminster Fire Dept, North Vancouver District Fire Dept, Pitt Meadows Fire Dept, Port Coquitlam Fire Rescue, Port Moody Fire Dept, Richmond Fire Dept, Squamish Fire Dept, Surrey Fire Dept, Vancouver Fire Dept, West Vancouver Fire Dept, Whistler Fire Dept, White Rock Fire Dept, Central Saanich Fire Dept, Esquimalt Fire Dept, Langford Fire Dept, Oak Bay Fire Dept, Qualicum Beach Fire Dept, Sooke V Fire Dept, Victoria Fire Dept BC Heath Authorities: Fraser Health Authority, Vancouver Island Health Authority, Vancouver Coastal Health Authority and Providence Health Care
Pittsburgh Resuscitation Network, the University of Pittsburgh, Pittsburgh, PA: Clifton Callaway, MD, PhD, Principal Investigator Core Investigators: Samuel Tisherman, MD, Jon Rittenberger, MD, David Hostler,PhD Coordinators: Joseph Condle, Mitch Kampmeyer, Timothy Markham, Maureen Morgan EMS Investigators/Collaborators: Paul Sabol, Gina Sicchitano, Anthony Shrader, Greg Stull, William Groft, Robert McCaughan, Rodney Rohrer, David Fuchs, MD, Francis Guyette, MD, MS, William Jenkins, MD, Ronald Roth, MD, Heather Walker, MD Hospital Investigators: Thomas Campbell, MD, Ankur Doshi, MD, Bruce MacLeod, MD Participating EMS Agencies: Ambulance and Chair, City of Pittsburgh EMS, City of Pittsburgh Fire, Mutual Aid Ambulance Portland Resuscitation Outcomes Consortium, Oregon Health and Science University, Portland, OR: Mohamud R. Daya MD, MS, Principal Investigator Core Investigators: Terri A. Schmidt MD, MS, Craig D. Newgard, MD, MPH, Jerris R. Hedges, MD, MS Coordinators: Denise E. Griffiths, BS, CCRP, Dana M. Zive, MPH, Aaron W. Monnig, EMT-P, Abdolaziz Yekrang, MPA, MA, Brett Tomlin, BS, Michael Kampp, BS, Jenny Cook, BS, Joan Burns, RN, Maria Nelson, MD, Yoko Nakamura, MD
ROC PRIMED-ITD-ALvAE Appendix – 8/10/2010 Page 4 of 6
EMS Investigators/Collaborators: Jonathan Jui, MD, MPH, Ritu Sahni, MD, MPH, Craig R. Warden, MD, MPH, Skip Freedman, MD, Mike Shertz, MD, Marc D. Muhr, EMT-P2, John A. Stouffer, EMT-P, Jay Cross, EMT-P, Joe Costigan, EMT-P, Kyle Gorman, MBA, EMT-P, Pontine Rosteck, EMT-P, Mike Verkest, EMT-P, Cyndi Newton, EMT-P, Tina Beeler, EMT-P, Karl Koenig, EMT-P, Jan Lee, EMT-P, Roxy Barnes, BSN, Doug Boyce, EMT-P, Brad Allen, EMT-P, TJ Bishop, EMT-P, Mike Hollingsworth, EMT-P, Eric Schult EMT-P, Scott Sullivan, EMT-P, Rick Williams, EMT-P, Steve Dehart, EMT-P, Mark Stevens, EMT-P, Rene Pizzo, EMT-P, Rob Hawks, EMT-P, Adam Glaser, EMT-P, Jonathan Chin, MS, EMT-P, Jason Blount, EMT-P, Gert Zoutendijk, Chris Koppenhafer, Corie Depuy, Kristen Hinds, Trish Noble Hospital Investigators/Coordinators: Lynn Wittwer, MD, Michael Albrich, MD, Tony Carnevale MD, Piroska Schlesinger, BS, Kristen Schmiedeskamp, BS, Amy Reiter, RN, Kathy Arnold, RN, Phyllis Ramey, RN, Roger McDonald, RN, Helen Walsh, RN Participating EMS Agencies: American Medical Response - Clackamas, Clark, and Multnomah Counties, Camas Fire Department, Clackamas County Fire District #1, Clark County Fire District #6, Gresham Fire and Emergency Services, Hillsboro Fire Department, Lake Oswego Fire Department, Metro West Ambulance, North Country Ambulance, Portland Fire and Rescue, Portland International Airport Fire Department, Tualatin Valley Fire and Rescue, Vancouver Fire Department UCSD-San Diego Resuscitation Research Center, University of California at San Diego, San Diego, CA: Daniel Davis, MD, Principal Investigator Core Investigators: Gary Vilke, MD, James Dunford, MD Coordinators: Donna Kelly Aker, RN, Thea Barsalou, RN EMS Investigators/Collaborators: Bruce Haynes, MD, Brad Schwartz, MD Hospital Investigators: Don Mebust MD, Robert Bei MD, Graydon Skeoch MD, Michele Grad MD, Ian Grover MD, Jerrold Glassman MD, Steven R. Andree MD, Lisa Morikado MD, Mark Kramer MD, Thomas Calkins MD, Mark Tamsen MD, William Linnik MD, Judd Glasser MD Participating EMS Agencies: El Cajon Fire Dept ALS, Julian-Cuyamaca Fire Dept ALS, North County Fire Dept ALS, Poway Fire Dept ALS, San Marcos Fire Dept ALS, Santee Fire Dept ALS, Viejas Fire Dept, City of San Diego Fire Rescue Department, Vista Fire Dept ALS Seattle-King County Center for Resuscitation Research at the University of Washington, University of Washington, Seattle, WA: Peter J. Kudenchuk, MD, Principal Investigator Core Investigators: Tom D. Rea, MD; Michael Copass, MD; Mickey S. Eisenberg, MD Coordinator: Michele Olsufka, RN; Debi Solberg, RN, MN; Sally Ragsdale, ARNP EMS Investigators/Collaborators: Jonathan Larsen, Mike Helbock
ROC PRIMED-ITD-ALvAE Appendix – 8/10/2010 Page 5 of 6
Participating EMS Agencies: Bellevue Fire Dept, Bothell Fire Dept, Burien Fire KCFD 2, Kirkland Fire KCFD 41, Renton Fire and Emergency Services, Snoqualmie Fire, Duvall Fire KCFPD 45, Eastside Fire & Rescue, Enumclaw Fire KCFPD 28, Fall City Fire KCFPD 27, Kent Fire Dept, Maple Valley Fire and Life Safety KCFPD #43, Mercer Island Fire Dept, KCFD #44 Mountainview, North Highline Fire KCFD 11, Northshore/ Kenmore Fire KCFD 16, Port of Seattle Fire Dept, KCFPD #47 Ravensdale/Palmer, Redmond Fire Dept, SeaTac Fire Dept, Seattle Fire Dept, Shoreline Fire KCFD 4, Skykomish Fire KCFD 50, KCFD #20 Skyway, Snoqualmie Pass Fire 51, South King County Medic 1, South King Fire & Rescue, Tukwila Fire Dept, Valley Regional Fire Authority, Vashon Island Fire KCFD 13, Woodinville Fire KCFD 36 Toronto Regional Resuscitation Research Out of Hospital Network (Toronto Regional RescuNET), University of Toronto, Toronto, Ontario, Canada: Arthur Slutsky, MD, MASc, Principal Investigator Core Investigators: Laurie J Morrison, MD, MSc, FRCPC; Paul Dorian, MD, MSc; Alan Craig, MScPl; Andrew Baker MD, FRCPC; , Jamie Hutchison, MD, FRCPC; Ori Rotstein, MD, MSc; P. Richard Verbeek, MD, FRCPC; Russell MacDonald, MD, MPH, FCFP, FRCPC; Sandra Black, MD, FRCP(C); Sandro Rizoli, MD, PhD, FRCSC, FACS; Sheldon Cheskes, MD, CCFP (EM), FCFP; Steven Brooks, MD, MHSc Coordinators: Adam Byers, Ahmed Taher, Anuar Turgulov, Blair Bigham, Bruce Cameron, Caitlin Wenkstern, Cathy Zhan, Christopher Foerster, Craig Beers, Jaime Beecroft, Jamie Frank, Malcolm Mercer, Markus Kernen, Michael Grife, Mohammad Qovaizi, Patrick Van Rooyen, Peter DeMaio, Rishab Chadha, Suzanne Chung, Tyrone Perreira, Welson Ryan EMS Investigators/Collaborators: Andy Benson, Dana Bradshaw, Dave Mokedanz, Doug Silver, Greg Sage, Jacob Stevens, Jason Whiteley, Jennifer Shield, John Locke, Judy Moore, Kenneth Webb, Kevin King, Marty Epp, Michael Feldman, Michael Nemeth, Philip Moran, Richard Renaud, Rob Burgess, Roy Suthons, Russ Olynyk, Steve McNenly, Steve Tyukodi, Terri Burton, Tim Waite, Verena Jones, Warren Beckett Hospital Investigators/Coordinators: Amy Back, Carolyn Vardy, Dina Braga, Don Redelmeier, Donna Chen, Evelina Kadic, Grace Burgess, Hannelore Mueller, Jacob Simonini, Jennifer Walker, Jessica Tyrwhitt, Judith Renton, Julie Spence, Katherine Allan, Kerri Bath, Laura Steeves, Lauren Lewarne, Lesley Ann Molyneaux, Margaret McGrath-Chong, Mariecar Pagulayan, Mark McLennan, Mediha Kadic, Melanie Piette, Nida Shahid, Raj Gobin, Roman Nowickyj, Selamawit Tessema, Shawn Hogan, Steve Driscoll Participating EMS Agencies: Ajax Fire and Emergency Services, Brampton Fire and Emergency Services, Clarington Fire Services, Central East Prehospital Care Program, District of Muskoka, Durham Region Emergency Medical Services, Halton Region Emergency Medical Services, Medavie Emergency Medical Services, Mississauga Fire and Emergency Services, Muskoka Ambulance Communication Center, Muskoka Ambulance Service, Muskoka Emergency Medical Services, Peel Regional Paramedic Services, Pickering Fire Services, Sunnybrook Osler Centre for Prehospital Care, Toronto Emergency Medical Services, Toronto Fire Services, Uxbridge Fire Services, Whitby Fire and Emergency Services
ROC PRIMED-ITD-ALvAE Appendix – 8/10/2010 Page 6 of 6
Steering Committee: Chair: Myron Weisfeldt, MD, Johns Hopkins University School of Medicine, Baltimore, MD Co-Chair–Cardiac: Joseph P. Ornato, MD, Virginia Commonwealth University Health System, Richmond, VA National Heart, Lung, and Blood Institute, Bethesda, MD: George Sopko, MD, MPH, Debra Egan, MPH, David Lathrop, PhD, Alice Mascette, MD, Patrice Desvigne Nickens, MD, Colin Wu, PhD, Phyllis Mitchell, PhD, Tracey Hoke, MD Clinical Trial Center, University of Washington, Department of Biostatistics, Seattle, WA: Gerald van Belle, PhD, Scott Emerson, MD, PhD, Graham Nichol, MD, MPH, Brian Leroux, PhD, Judy Powell, BSN, Lois Van Ottingham, BSN, Gena Sears, BSN, Siobhan Everson-Stewart, PhD, Robert Schmicker, MS, Andrea Cook, PhD, Kyle Rudser, PhD, Robert B. Ledingham, MS, Ben Bergsten-Buret, Richard Moore, BS, Amy Gest, MPA, Colleen Sitlani, MS, Kent Koprowicz, MS, Liz Thomas, MS, Erin Gabriel, MS, Ken Wu, MS, Danielle Schroeder, BS, Chi Shen, MS, Winnie Kirdpoo, BS, Jackie Berhorst, Anna Leonen, MS, Yang Wang, PhD, Al Hallstrom, PhD