review article subsite-specific dietary risk factors for colorectal...
TRANSCRIPT

Hindawi Publishing CorporationJournal of OncologyVolume 2013, Article ID 703854, 14 pageshttp://dx.doi.org/10.1155/2013/703854
Review ArticleSubsite-Specific Dietary Risk Factors for Colorectal Cancer:A Review of Cohort Studies
Anette Hjartåker,1 Bjarte Aagnes,2 Trude Eid Robsahm,2 Hilde Langseth,2
Freddie Bray,3 and Inger Kristin Larsen4
1 Department of Nutrition, Institute of Basic Medical Sciences, University of Oslo, P.O. Box 1046 Blindern, 0317 Oslo, Norway2Department of Etiological Research, Cancer Registry of Norway, Institute of Population-Based Cancer Research, 0304 Oslo, Norway3 Section of Cancer Information, International Agency for Research on Cancer, 69372 Lyon, France4Department of Registration, Cancer Registry of Norway, Institute of Population-Based Cancer Research, 0304 Oslo, Norway
Correspondence should be addressed to Anette Hjartaker; [email protected]
Received 11 October 2012; Accepted 30 November 2012
Academic Editor: Anne-Kathrin Illner
Copyright © 2013 Anette Hjartaker et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Objective. A shift in the total incidence from left- to right-sided colon cancer has been reported and raises the question as to whetherlifestyle risk factors are responsible for the changing subsite distribution of colon cancer.The present study provides a review of thesubsite-specific risk estimates for the dietary components presently regarded as convincing or probable risk factors for colorectalcancer: red meat, processed meat, fiber, garlic, milk, calcium, and alcohol.Methods. Studies were identified by searching PubMedthrough October 8, 2012 and by reviewing reference lists. Thirty-two prospective cohort studies are included, and the estimates arecompared by sex for each risk factor. Results. For alcohol, there seems to be a stronger association with rectal cancer than with coloncancer, and formeat a somewhat stronger association with distal colon and rectal cancer, relative to proximal colon cancer. For fiber,milk, and calcium, there were only minor differences in relative risk across subsites. No statement could be given regarding garlic.Overall, many of the subsite-specific risk estimates were nonsignificant, irrespective of exposure. Conclusion. For some dietarycomponents the associations with risk of cancer of the rectum and distal colon appear stronger than for proximal colon, but notfor all.
1. Introduction
Global estimates for 2008 indicate that colorectal cancer isthe third most common cancer in the world [1]. Reports inseveral countries have described diverging incidence rates incolorectal cancer by subsite, including, in relative terms, anincreasing proportion of proximal tumors [2–15], and thusa shift in absolute incidence from left- to right-sided coloncancers.
The reasons for this trend are not well understood; thesubsites differ in physical function, artery supply, histology,and innervation, and they also derive fromdifferent segmentsin the primitive intestinal tract in the embryo [16]. Theproximal colon originates from themidgut, whereas the distalcolon and the rectum derivate originate from the hindgut.
Comparisons have also shown that proximal colon tumorstend to have different molecular characteristics, with a higherproportion of microsatellite instability, and are more likely tohave CpG islandmethylator phenotype and Ki-ras mutationsthan distal colon and rectal tumors [17].
It has been estimated that 45 percent of all colorectalcancer cases can be prevented in high-risk populationsthrough modifications of diet, physical activity habits, andweight control [18]. According to the recent report fromthe World Cancer Research Fund/American Institute forCancer Research (WCRF/AICR), there is convincing evi-dence that dietary fiber protects against colorectal cancerand that red and processed meat and alcohol (particularlyin men) increase the risk of the disease [19]. Further, itis stated that garlic, milk, and calcium probably protect

2 Journal of Oncology
Table 1: Search results as of October 8, 2012.
Queries Result1 Search colorectal neoplasms 1483742 Search risk factors 7459693 Search diet 3329114 Search nutrition 2597395 Search alcohol 7186226 Search cohort study 12532167 Search 3 OR 4 OR 5 12154928 Search 2 AND 7 813639 Search 1 AND 8 209910 Search 6 AND 9 62711 Search case control study 62238512 Search review 208203913 Search 10 NOT 11 NOT 12 35614 Search 13 Limits: Human, English 341
against colorectal cancer. No distinction is, however,made forthe different subsites of the colorectum [19]. Also, althoughmeta- [20–23] and pooled analyses [24–26] have providedquantitative synthesis for several of the dietary risk factors,little emphasis has been placed on subsite risks.
Based on the biological differences in the colorectalsegments and the reported differences in incidence, we maysuggest differences across the segments in their associationto lifestyle factors, such as diet. The aim of the present paperis to give an updated overview summarizing the etiologicaldifferences between the colorectal subsites with regard to thedietary factors considered to be convincing or probable riskfactors for colorectal cancer.
2. Material and Methods
The specific risk factors studied were red meat, processedmeat, fiber, garlic, milk, calcium, and alcohol, selected givenan a priori assessment of their importance in colorectalcancer etiology following the WCRF/AICR report in 2011[19], and for which their modification could lead to areduction in rates of colorectal cancer. The outcome was therisk of primary colorectal cancer according to subsite.
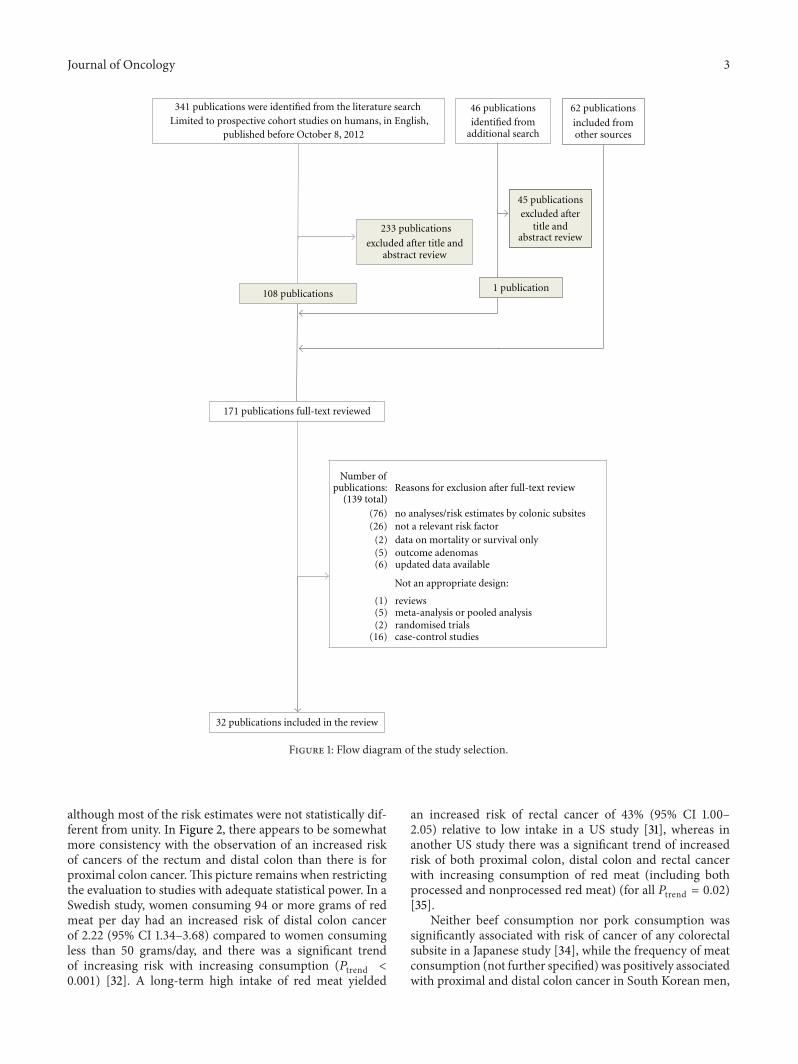
A search for cohort studies published as original arti-cles was conducted via a search of PubMed (http://www.ncbi.nlm.nih.gov/), using a search strategy that combinedthe term “colorectal neoplasms” with the terms “risk factors”and “cohort study” with either the term “diet,” “nutrition,”or “alcohol.” The search was restricted to studies publishedor available online as of October 8, 2012, in the Englishlanguage. A detailed description of the search strategy andthe resulting papers retrieved is given in Table 1, and theprocedure is described in Figure 1. A total of 341 articles wereidentified and reviewed according to title and abstract. Theinitial evaluation yielded 108 articles in the study databaseand underwent a second evaluation based on full-text review.A similar PubMed search for case-control studies nestedwithin a cohort identified 46 articles, of which one underwentfull-text review. In addition, further 62 articles were identified
by scanning the reference lists of retrieved articles, reviews,meta-, and pooled analyses and underwent full-text review(Figure 1).
Studies were included if they provided risk estimates (andcorresponding confidence intervals) for both proximal anddistal colon cancer. Proximal colon (right sided) includesceacum, ascending and transverse colon, while distal colon(left-sided) includes descending colon, sigmoid flexure, andsigmoideum. Some studies have not followed the above-mentioned classification [27–29], and this is specified inTable 2. Further, to be included, the cohorts had to beeither population based, registry based, or obtained fromcensuses. Studies on specific subpopulations (e.g., hospital-based cohorts) were not included nor were studies examiningsecond cancers, metastasis, survival, or mortality. Followingthe full-text evaluation, 139 articles were excluded for thereasons indicated in Figure 1, and 32 articles were includedin the review. Of these, seven gave data on (red) meat [30–36], five on processed meat [31–35], eight on fiber [37–44],one on garlic [37], three on milk [45–47], seven on calcium[28, 45, 47–51], and ten on alcohol [27, 29, 36, 52–58].
The number adds up to more than 32 as several papersgive data for more than one risk factor. If several papers onthe same risk factor were published for a given cohort, all datawas retrieved from the most recent paper. The relative risk(RR), hazard rate ratio (HRR), hazard ratio (HR), incidencerate ratio (IRR) or odds ratio (OR), and corresponding95% confidence intervals (95% CI) for each risk factor arepresented (as RR) in Figures 2–8, sorted in ascending orderof magnitude by sex. For one study the risk estimates weretabulated according to the lowest versus highest exposurecategory in the original paper [28] and are presented as theinverse of the value in the corresponding figure (Figure 7).
Meta-analyses were not performed as a consequence ofthe heterogeneity in factors such as exposure measurement,the categorization of risk factor levels, and the confoundersadjusted for in the studies [59].
3. Results
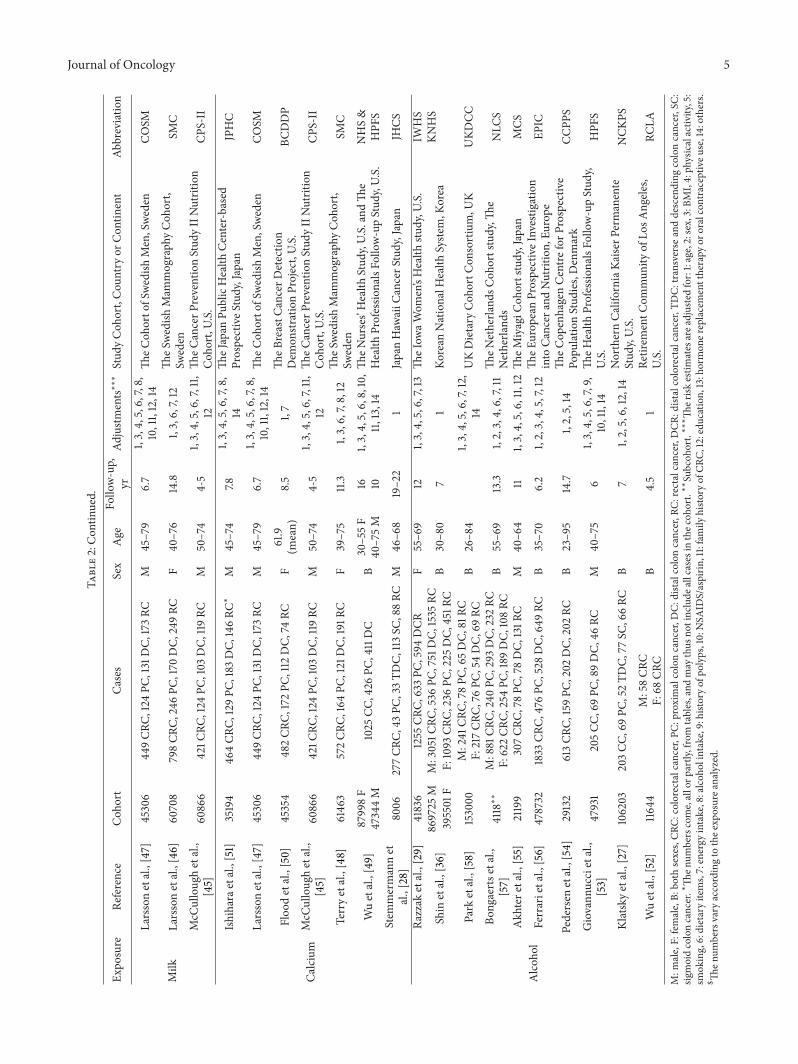
Overall, data from 21 cohorts with information on one ormore of the risk factors were included in this review. Table 2gives a detailed description of the studies, with informationon cohort size, number of cases, sex, age distribution, follow-up time, and factors adjusted for in the risk analyses. TheEuropean Prospective Investigation into Cancer and Nutri-tion (EPIC) study consists of subcohorts from 10 Europeancountries.The other cohorts were from the USA (10 cohorts),Sweden (2), Denmark (2), Japan (3), Korea (1), UK (1), andthe Netherlands (1). The subsite-specific results (Figures 2–8) are described according to the individual risk factors, aspresented in the following.
3.1. Red Meat. Seven cohort studies were included in thereview, of which five reported on redmeat [30–33, 35], one onbeef and pork [34], and one on meat (not further specified)[36].Thefive studies on redmeat reported an increased risk ofcolorectal cancer with increasing intake [30–33, 35] (Table 2),
Journal of Oncology 3
341 publications were identified from the literature searchLimited to prospective cohort studies on humans, in English,
published before October 8, 2012
46 publicationsidentified from
additional search
62 publications
included fromother sources
233 publications
excluded after title andabstract review
45 publicationsexcluded after
title andabstract review
1 publication108 publications
171 publications full-text reviewed
32 publications included in the review
(76) no analyses/risk estimates by colonic subsites(26) not a relevant risk factor
(2) data on mortality or survival only(5) outcome adenomas(6) updated data available
Not an appropriate design:
(1) reviews(5) meta-analysis or pooled analysis(2) randomised trials
(16) case-control studies
Number ofpublications:
(139 total)Reasons for exclusion after full-text review
Figure 1: Flow diagram of the study selection.
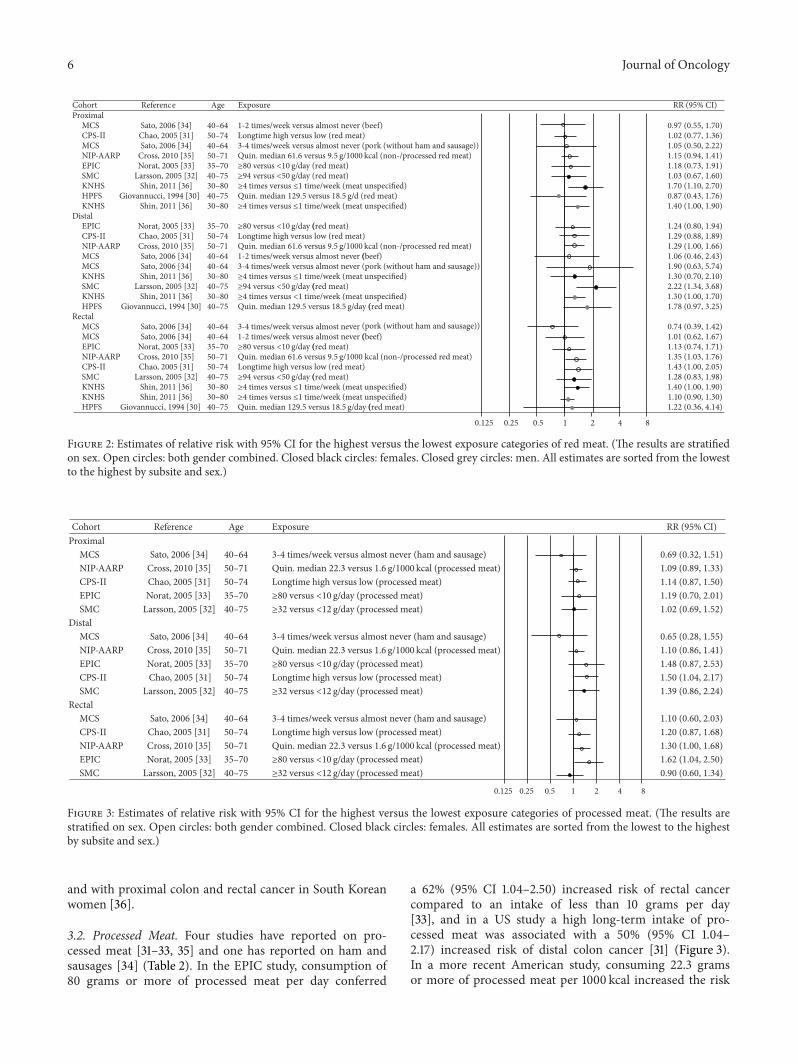
although most of the risk estimates were not statistically dif-ferent from unity. In Figure 2, there appears to be somewhatmore consistency with the observation of an increased riskof cancers of the rectum and distal colon than there is forproximal colon cancer.This picture remains when restrictingthe evaluation to studies with adequate statistical power. In aSwedish study, women consuming 94 or more grams of redmeat per day had an increased risk of distal colon cancerof 2.22 (95% CI 1.34–3.68) compared to women consumingless than 50 grams/day, and there was a significant trendof increasing risk with increasing consumption (𝑃trend <
0.001) [32]. A long-term high intake of red meat yielded
an increased risk of rectal cancer of 43% (95% CI 1.00–2.05) relative to low intake in a US study [31], whereas inanother US study there was a significant trend of increasedrisk of both proximal colon, distal colon and rectal cancerwith increasing consumption of red meat (including bothprocessed and nonprocessed red meat) (for all 𝑃trend = 0.02)[35].
Neither beef consumption nor pork consumption wassignificantly associated with risk of cancer of any colorectalsubsite in a Japanese study [34], while the frequency of meatconsumption (not further specified) was positively associatedwith proximal and distal colon cancer in South Korean men,

4 Journal of Oncology
Table2:Ch
aracteris
ticso
fcoh
ortstudies
inclu
dedin
ther
eviewon
subsite
specificd
ietary
riskfactorsfor
colorectalcancer.
Expo
sure
Reference
Coh
ort
Cases
Sex
Age
Follo
w-up,
yrAd
justm
ents∗∗∗
Stud
yCoh
ort,Cou
ntry
orCon
tinent
Abbreviatio
n
Red
meat
Shin
etal.,[36]
869725
MM:3051C
RC,536
PC,751
DC,
1535
RCB
30–8
07
1Ko
rean
NationalH
ealth
Syste
m,K
orea
KNHS
395501
FF:1093
CRC,
236PC
,225
DC,
451R
CCr
osse
tal.,[35]
300948
2719
CRC,
1150
PC,787
DC,
724RC
B50–71
7.22,3,5,6,7,12
NIH
-AARP
Dietand
Health
Stud
y,U.S.
NIH
-AARP
Sato
etal.,[34]
41835
396/368CR
C,123/115PC
,85/75
DC,
159/155RC∗$
B40
–64
111,2,3,4,5,6,7,
8,11,12
TheM
iyagiC
ohortStudy,Japan
MCS
Chao
etal.,[31]
148610
1667
CRC,
667PC
,408
DC,
470RC
B50–74
8-9
1,2,3,4,5,6,7,
8,10,12,13
TheC
ancerP
reventionStud
yIINutrition
Coh
ort,U.S.
CPS-II
Larssonetal.,[32]
61433
733CR
C,234PC
,155
DC,
230RC
F40
–75
13.9
1,3,6,7,8,12
TheS
wedish
Mam
mograph
yCoh
ort,
Sweden
SMC
Noratetal.,[33]
478040
1329
CRC,
351P
C,391D
C,474RC
B35–70
4.8
1,2,3,4,5,6,7,
8,14
TheE
urop
eanProspectiveInvestig
ation
into
Cancer
andNutrition,
Europe
EPIC
Giovann
uccietal.,
[30]
47949
251C
RC,69PC
,89DC,
46RC
M40
–75
61,3,4,5,8,9,10,
11,14
TheH
ealth
Professio
nalsFo
llow-upStud
y,U.S.
HPF
S
Processed
meat
Crosse
tal.,[35]
300948
2719
CRC,
1150
PC,787
DC,
724RC
B50–71
7.22,3,5,6,7,12
NIH
-AARP
Dietand
Health
Stud
y,U.S.
NIH
-AARP
Sato
etal.,[34]
41835
474CR
C,142PC
,100
DC,
198RC∗
B40
–64
111,2,3,4,5,6,7,
8,11,12
TheM
iyagiC
ohortStudy,Japan
MCS
Chao
etal.,[31]
148610
1667
CRC,
667PC
,408
DC,
470RC
B50–74
8-9
1,2,3,4,5,6,7,
8,10,12,13
TheC
ancerP
reventionStud
yIINutrition
Coh
ort,U.S.
CPS-II
Larssonetal.,[32]
61433
733CR
C,234PC
,155
DC,
230RC
F40
–75
13.9
1,3,6,7,8,12
TheS
wedish
Mam
mograph
yCoh
ort,
Sweden
SMC
Noratetal.,[33]
478040
1329
CRC,
351P
C,391D
C,474RC
B35–70
4.8
1,2,3,4,5,6,
7,8,14
TheE
urop
eanProspectiveInvestig
ation
into
Cancer
andNutrition,
Europe
EPIC
Fiber/
who
legrain
Murph
yetal.,[44]
142250
M335062
F4517
CRC,
1298
PC,1266DC,
1648
RCB
25–70
111,2,3,4,5,6,7,
8,12,13,14
TheE
urop
eanProspectiveInvestig
ation
into
Cancer
andNutrition,
Europe
EPIC
Egebergetal.,[43]
26630M
M:244
CC,89PC
,140
DC,
169RC
B50–6
410.6
1,3,4,6,8,12,13Th
eDanish
Diet,Cancera
ndHealth
ProspectiveC
ohortstudy,D
enmark
DDCH
PC29189F
F:217CC
,84PC
,118
DC,
114RC
Kabatetal.,[42]
158800
1476
CRC,
798PC
,351
DC,
303RC
F50–79
7.81,3,4,5,6,7,11,
12,13,14
TheW
omen’sHealth
Initiative,U.S.
WHI
Nom
urae
tal.,[40]
85903M
M:1138CR
C,382PC
,327
DC,
276RC
B45–75
7.31,3,4,5,6,8,9,
10,11,13,14
TheM
ultie
thnicC
ohortStudy,H
awaiiand
LosA
ngeles,U
.S.
MEC
105108
FF:972CR
C,356PC
,234
DC,
179RC
Schatzkinetal.,
[41]
489611
2974
CRC,
1139
PC,914
DC,
858RC∗
B50–71
52,3,4,5,6,7,8,
11,12,13,14
NIH
-AARP
Dietand
Health
Stud
y,U.S.
NIH
-AARP
Larssonetal.,[39]
61433
805CR
C,249PC
,170
DC,
252RC
F40
–76
14.8
1,3,6,7,12
TheS
wedish
Mam
mograph
yCoh
ort,
Sweden
SMC
Fuchse
tal.,[38]
88757
787CR
C,281P
C,255DC,
143RC∗
F34–59
161,3,4,5,6,7,
8,9,10,11
TheN
urses’Health
Stud
y,U.S.
NHS
Steinm
etze
tal.,
[37]
41837
212CC
,86PC
,120
DC∗
F55–6
95
1,7
TheIow
aWom
en’sHealth
Stud
y,U.S.
IWHS
Garlic
Steinm
etze
tal.,
[37]
41837
212CC
,86PC
,120
DC∗
F55–6
95
1,7
TheIow
aWom
en’sHealth
Stud
y,U.S.
IWHS
Journal of Oncology 5
Table2:Con
tinued.
Expo
sure
Reference
Coh
ort
Cases
Sex
Age
Follo
w-up,
yrAd
justm
ents∗∗∗
Stud
yCoh
ort,Cou
ntry
orCon
tinent
Abbreviatio
n
Milk
Larssonetal.,[47]
45306
449CR
C,124PC
,131
DC,
173RC
M45–79
6.7
1,3,4,5,6,7,8,
10,11,12,14
TheC
ohorto
fSwedish
Men,Sweden
COSM
Larssonetal.,[46]
60708
798CR
C,246PC
,170
DC,
249RC
F40
–76
14.8
1,3,6,7,12
TheS
wedish
Mam
mograph
yCoh
ort,
Sweden
SMC
McC
ulloug
hetal.,
[45]
60866
421C
RC,124
PC,103
DC,
119RC
M50–74
4-5
1,3,4,5,6,7,11,
12Th
eCancerP
reventionStud
yIINutrition
Coh
ort,U.S.
CPS-II
Calcium
Ishihara
etal.,[51]
35194
464CR
C,129PC
,183
DC,
146RC∗
M45–74
7.81,3,4,5,6,7,8,
14Th
eJapan
PublicHealth
Center-based
ProspectiveS
tudy,Japan
JPHC
Larssonetal.,[47]
45306
449CR
C,124PC
,131
DC,
173RC
M45–79
6.7
1,3,4,5,6,7,8,
10,11,12,14
TheC
ohorto
fSwedish
Men,Sweden
COSM
Floo
detal.,[50]
45354
482CR
C,172PC
,112
DC,
74RC
F61.9
(mean)
8.5
1,7
TheB
reastC
ancerD
etectio
nDem
onstr
ationProject,U.S.
BCDDP
McC
ulloug
hetal.,
[45]
60866
421C
RC,124
PC,103
DC,
119RC
M50–74
4-5
1,3,4,5,6,7,11,
12Th
eCancerP
reventionStud
yIINutrition
Coh
ort,U.S.
CPS-II
Terryetal.,[48]
61463
572CR
C,164PC
,121
DC,
191R
CF
39–75
11.3
1,3,6,7,8,12
TheS
wedish
Mam
mograph
yCoh
ort,
Sweden
SMC
Wuetal.,[49]
87998F
47344M
1025
CC,426
PC,411DC
B30–55F
40–75M
16 101,3,4,5,6,8,10,
11,13,14
TheN
urses’Health
Stud
y,U.S.andTh
eHealth
Professio
nalsFo
llow-upStud
y,U.S.
NHS&
HPF
SStem
mermannet
al.,[28]
8006
277CR
C,43
PC,33TD
C,113SC
,88RC
M46
–68
19–22
1JapanHaw
aiiC
ancerS
tudy,Japan
JHCS
Alcoh
ol
Razzak
etal.,[29]
41836
1255
CRC,
633PC
,594
DCR
F55–6
912
1,3,4,5,6,7,13
TheIow
aWom
en’sHealth
study,U
.S.
IWHS
Shin
etal.,[36]
869725
MM:3051C
RC,536
PC,751
DC,
1535
RCB
30–8
07
1Ko
rean
NationalH
ealth
Syste
m,K
orea
KNHS
395501
FF:1093
CRC,
236PC
,225
DC,
451R
C
Park
etal.,[58]
153000
M:241
CRC,
78PC
,65DC,
81RC
F:217CR
C,76
PC,54DC,
69RC
B26–8
41,3,4,5,6,7,12,
14UKDietary
Coh
ortC
onsortium,U
KUKD
CC
Bong
aertse
tal.,
[57]
4118∗∗
M:881
CRC,
240PC
,293
DC,
232RC
F:622CR
C,254PC
,189
DC,
108RC
B55–6
913.3
1,2,3,4,6,7,11
TheN
etherla
ndsC
ohortstudy,Th
eNetherla
nds
NLC
S
Akh
tere
tal.,[55]
21199
307CR
C,78
PC,78DC,
131R
CM
40–6
411
1,3,4,5,6,11,12Th
eMiyagiC
ohortstudy,Japan
MCS
Ferrarietal.,[56]
478732
1833
CRC,
476PC
,528
DC,
649RC
B35–70
6.2
1,2,3,4,5,7,12
TheE
urop
eanProspectiveInvestig
ation
into
Cancer
andNutrition,
Europe
EPIC
Pedersen
etal.,[
54]
29132
613CR
C,159PC
,202
DC,
202RC
B23–9
514.7
1,2,5,14
TheC
openhagenCentre
forP
rospectiv
ePo
pulationStud
ies,Denmark
CCPP
S
Giovann
uccietal.,
[53]
47931
205CC
,69PC
,89DC,
46RC
M40
–75
61,3,4,5,6,7,9,
10,11,14
TheH
ealth
Professio
nalsFo
llow-upStud
y,U.S.
HPF
S
Klatsk
yetal.,[27]
106203
203CC
,69PC
,52TD
C,77
SC,66RC
B7
1,2,5,6,12,14
NorthernCa
liforniaK
aiserP
ermanente
Stud
y,U.S.
NCK
PS
Wuetal.,[52]
11644
M:58CR
CF:68
CRC
B4.5
1Re
tirem
entC
ommun
ityof
LosA
ngeles,
U.S.
RCLA
M:m
ale,F:
female,B:
both
sexes,CR
C:colorectalcancer,P
C:proxim
alcoloncancer,D
C:distalcoloncancer,R
C:rectalcancer,D
CR:d
istalcolorectalcancer,T
DC:
transverse
anddescending
coloncancer,SC:
sigmoidcoloncancer.∗Th
enum
berscome,allorp
artly,from
tables,and
may
thus
notinclude
allcasesin
thec
ohort.∗∗
Subcoh
ort.∗∗∗
Ther
iskestim
atesarea
djustedfor:1:age,2:sex,3:BM
I,4:ph
ysicalactiv
ity,5:
smok
ing,6:dietaryitems,7:energy
intake,8:alcoh
olintake,9:historyo
fpolyps,10:N
SAID
S/aspirin
,11:family
histo
ryof
CRC,
12:edu
catio
n,13:hormon
ereplacementtherapy
ororalcontraceptiveu
se,14:others.
$ Then
umbersvary
accordingto
thee
xposurea
nalyzed.
6 Journal of Oncology
Cohort Referenc Age Exposure RR (95% CI)Proximal
MCS Sato, 2006 [34] 40–64 1-2 times/week versus almost never (beef) 0.97 (0.55, 1.70)CPS-II Chao, 2005 [31] 50–74 Longtime high versus low (red meat) 1.02 (0.77, 1.36)MCS Sato, 2006 [34] 40–64 3-4 times/week versus almost never (pork (without ham and sausage)) 1.05 (0.50, 2.22)NIP-AARP Cross, 2010 [35] 50–71 Quin. median 61.6 versus 9.5 g/1000 kcal (non-/processed red meat)
(non-/processed red meat)
1.15 (0.94, 1.41)EPIC Norat, 2005 [33] 35–70 ≥80 versus <10 g/day 1.18 (0.73, 1.91)SMC Larsson, 2005 [32] 40–75 ≥94 versus <50 g/day 1.03 (0.67, 1.60)KNHS Shin, 2011 [36] 30–80 ≥4 times versus ≤1 time/week 1.70 (1.10, 2.70)HPFS Giovannucci, 1994 [30] 40–75 Quin. median 129.5 versus 18.5 g/d 0.87 (0.43, 1.76)KNHS Shin, 2011 [36] 30–80 ≥4 times versus ≤1 time/week 1.40 (1.00, 1.90)
DistalEPIC Norat, 2005 [33] 35–70 ≥80 versus <10 g/day ( 1.24 (0.80, 1.94)CPS-II Chao, 2005 [31] 50–74 Longtime high versus low 1.29 (0.88, 1.89)NIP-AARP Cross, 2010 [35] 50–71 Quin. median 61.6 versus 9.5 g/1000 kcal 1.29 (1.00, 1.66)MCS Sato, 2006 [34] 40–64 1-2 times/week versus almost never ( 1.06 (0.46, 2.43)MCS Sato, 2006 [34] 40–64 3-4 times/week versus almost never 1.90 (0.63, 5.74)KNHS Shin, 2011 [36] 30–80 ≥4 times versus ≤1 time/week 1.30 (0.70, 2.10)SMC Larsson, 2005 [32] 40–75 ≥94 versus <50 g/day ( 2.22 (1.34, 3.68)KNHS Shin, 2011 [36] 30–80 ≥4 times versus <1 time/week 1.30 (1.00, 1.70)HPFS Giovannucci, 1994 [30] 40–75 Quin. median 129.5 versus 18.5 g/day ( 1.78 (0.97, 3.25)
RectalMCS Sato, 2006 [34] 40–64 3-4 times/week versus almost never 0.74 (0.39, 1.42)MCS Sato, 2006 [34] 40–64 1-2 times/week versus almost never ( 1.01 (0.62, 1.67)EPIC Norat, 2005 [33] 35–70 ≥80 versus <10 g/day ( 1.13 (0.74, 1.71)NIP-AARP Cross, 2010 [35] 50–71 Quin. median 61.6 versus 9.5 g/1000 kcal (non-/processed red meat) 1.35 (1.03, 1.76)CPS-II Chao, 2005 [31] 50–74 Longtime high versus low 1.43 (1.00, 2.05)SMC Larsson, 2005 [32] 40–75 ≥94 versus <50 g/day ( 1.28 (0.83, 1.98)KNHS Shin, 2011 [36] 30–80 ≥4 times versus ≤1 time/week 1.40 (1.00, 1.90)KNHS Shin, 2011 [36] 30–80 ≥4 times versus ≤1 time/week 1.10 (0.90, 1.30)HPFS Giovannucci, 1994 [30] 40–75 Quin. median 129.5 versus 18.5 g/day ( 1.22 (0.36, 4.14)
10.125 0.25 0.5 2 4 8
(red meat)
(red meat)
(red meat)
(red meat)(red meat)
(red meat)
(red meat)
(red meat)
(red meat)
(red meat)
(red meat)(meat unspecified)
(meat unspecified)
(meat unspecified)
(meat unspecified)(meat unspecified)
(meat unspecified)
(beef)
(beef)
(pork (without ham and sausage))
(pork (without ham and sausage))
e
Figure 2: Estimates of relative risk with 95% CI for the highest versus the lowest exposure categories of red meat. (The results are stratifiedon sex. Open circles: both gender combined. Closed black circles: females. Closed grey circles: men. All estimates are sorted from the lowestto the highest by subsite and sex.)
Cohort Reference Age Exposure RR (95% CI)Proximal
MCS S ato, 2006 [34] 40–64 3-4 times/week versus almost never 0.69 (0.32, 1.51)NIP-AARP Cross, 2010 [35] 50–71 Quin. median 22.3 versus 1.6 g/1000 kcal 1.09 (0.89, 1.33)CPS-II Chao, 2005 [31] 50–74 Longtime high versus low 1.14 (0.87, 1.50)EPIC Norat, 2005 [33] 35–70 ≥80 versus <10 g/day 1.19 (0.70, 2.01)SMC Larsson, 2005 [32] 40–75 ≥32 versus <12 g/day 1.02 (0.69, 1.52)
DistalMCS Sato, 2006 [34] 40–64 3-4 times/week versus almost never 0.65 (0.28, 1.55)NIP-AARP Cross, 2010 [35] 50–71 Quin. median 22.3 versus 1.6 g/1000 kcal 1.10 (0.86, 1.41)EPIC Norat, 2005 [33] 35–70 ≥80 versus <10 g/day 1.48 (0.87, 2.53)CPS-II Chao, 2005 [31] 50–74 Longtime high versus low 1.50 (1.04, 2.17)SMC Larsson, 2005 [32] 40–75 ≥32 versus <12 g/day 1.39 (0.86, 2.24)
RectalMCS Sato, 2006 [34] 40–64 3-4 times/week versus almost never 1.10 (0.60, 2.03)CPS-II Chao, 2005 [31] 50–74 Longtime high versus low 1.20 (0.87, 1.68)NIP-AARP Cross, 2010 [35] 50–71 Quin. median 22.3 versus 1.6 g/1000 kcal 1.30 (1.00, 1.68)EPIC Norat, 2005 [33] 35–70 ≥80 versus <10 g/day 1.62 (1.04, 2.50)SMC Larsson, 2005 [32] 40–75 ≥32 versus <12 g/day 0.90 (0.60, 1.34)
10.125 0.25 0.5 2 4 8
(ham and sausage)
(ham and sausage)
(ham and sausage)
(processed meat)(processed meat)
(processed meat)(processed meat)
(processed meat)(processed meat)
(processed meat)(processed meat)
(processed meat)(processed meat)
(processed meat)(processed meat)
Figure 3: Estimates of relative risk with 95% CI for the highest versus the lowest exposure categories of processed meat. (The results arestratified on sex. Open circles: both gender combined. Closed black circles: females. All estimates are sorted from the lowest to the highestby subsite and sex.)
and with proximal colon and rectal cancer in South Koreanwomen [36].
3.2. Processed Meat. Four studies have reported on pro-cessed meat [31–33, 35] and one has reported on ham andsausages [34] (Table 2). In the EPIC study, consumption of80 grams or more of processed meat per day conferred
a 62% (95% CI 1.04–2.50) increased risk of rectal cancercompared to an intake of less than 10 grams per day[33], and in a US study a high long-term intake of pro-cessed meat was associated with a 50% (95% CI 1.04–2.17) increased risk of distal colon cancer [31] (Figure 3).In a more recent American study, consuming 22.3 gramsor more of processed meat per 1000 kcal increased the risk
Journal of Oncology 7
Cohort Reference Exposure RR (95% CI)Proximal
EPIC Murphy, 2012 [44] 25–70 Per 10 g/day increase 0.83 (0.75, 0.92)EPIC Murphy, 2012 [44] 25–70 ≥28.5 versus <16.4 g/day 0.92 (0.71, 1.20)NIH-AARP Schatzkin, 2007 [41] 50–71 Quin. median 15.9 versus 6.6 g/1000 kcal/day 0.93 (0.72, 1.18)SMC Larsson, 2005 [39] 40–76 ≥4.5 versus <1.5 serv/day 0.69 (0.40, 1.20)NHS Fuchs, 1999 [38] 34–59 Quin. median 24.9 versus 9.8 g/day 1.00 (0.61, 1.61)IWHS Steinmetz, 1994 [37] 55–69 ≥24.7 versus <14.5 g/day 1.03 (0.48, 2.22)WHI Kabat, 2008 [42] 50–79 Quin. 21.2 versus <9.9 g/day 1.20 (0.73, 1.95)MEC Nomura, 2007 [40] 45–75 Quin. median 18.6 versus 7.5 g/1000 kcal/day 1.31 (0.86, 1.97)DDCHPC Egeberg, 2010 [43] 50–64 Per every 50 g increment/day 0.78 (0.66, 0.92)MEC Nomura, 2007 [40] 45–75 Quin. median 16.5 versus 6.1 g/1000 kcal/day 0.81 (0.54, 1.23)
DistalEPIC Murphy, 2012 [44] 25–70 ≥28.5 versus <16.4 g/day 0.70 (0.53, 0.92)NIH-AARP Schatzkin, 2007 [41] 50–71 Quin. median 15.9 versus 6.6 g/1000 kcal/day 0.97 (0.73, 1.28)EPIC Murphy, 2012 [44] 25–70 Per 10 g/day increase 0.98 (0.88, 1.08)SMC Larsson, 2005 [39] 40–76 ≥4.5 versus <1.5 serv/day 0.54 (0.27, 1.08)IWHS Steinmetz, 1994 [37] 55–69 >24.7 versus <14.5 g/day (fiber) 0.66 (0.34, 1.29)MEC Nomura, 2007 [40] 45–75 Quin. median 18.6 versus 7.5 g/1000 kcal/day 0.69 (0.41, 1.17)WHI Kabat, 2008 [42] 50–79 Quin. 21.2 versus <9.9 g/day 0.97 (0.46, 2.05)NHS Fuchs, 1999 [38] 34–59 Quin. median 24.9 versus 9.8 g/day 1.08 (0.67, 1.72)MEC Nomura, 2007 [40] 45–75 Quin. median 16.5 versus 6.1 g/1000 kcal/day 0.56 (0.35, 0.90)DDCHPC Egeberg, 2010 [43] 50–64 Per every 50 g increment/day 0.90 (0.79, 1.02)
RectalEPIC Murphy, 2012 [44] 25–70 Per 10 g/day increase 0.87 (0.79, 0.96)EPIC Murphy, 2012 [44] 25–70 ≥28.5 versus <16.4 g/day 0.90 (0.72, 1.14)NIH-AARP Schatzkin, 2007 [41] 50–71 Quin. median 15.9 versus 6.6 g/1000 kcal/day 1.13 (0.84, 1.51)NHS Fuchs, 1999 [38] 34–59 Quin. median 24.9 versus 9.8 g/day (fiber) 0.63 (0.37, 1.08)MEC Nomura, 2007 [40] 45–75 Quin. median 18.6 versus 7.5 g/1000 kcal/day 0.82 (0.48, 1.43)WHI Kabat, 2008 [42] 50–79 Quin. 21.2 versus <9.9 g/day (fiber) 0.88 (0.39, 2.01)DDCHPC Egeberg, 2010 [43] 50–64 Per every 50 g increment/day 1.02 (0.88, 1.19)SMC Larsson, 2005 [39] 40–76 ≥4.5 versus <1.5 serv/day 1.11 (0.67, 1.83)MEC N omura, 2007 [40] 45–75 Quin. median 16.5 versus 6.1 g/1000 kcal/day 0.52 (0.32, 0.84)DDCHPC Egeberg, 2010 [43] 50–64 Per every 50 g increment/day 0.90 (0.80, 1.01)
10.125 0.25 0.5 2 4 8
(whole grain)
(whole grain)(whole grain)
(whole grain)
(whole grain)
(whole grain)
(whole grain)
(fiber)
(fiber)
(fiber)
(fiber)(fiber)
(fiber)(fiber)
(fiber)(fiber)
(fiber)
(fiber)(fiber)
(fiber)
(fiber)(fiber)
(fiber)(fiber)
(fiber)(fiber)
(fiber)
Age
Figure 4: Estimates of relative risk with 95% CI for the highest versus the lowest exposure categories of fiber and whole grain. (The results arestratified on sex. Open circles: both gender combined. Closed black circles: females. Closed grey circles: men. All estimates are sorted fromthe lowest to the highest by subsite and sex.)
Cohort Reference Age Exposure
Proximal
IWHS 55–69
55–69
Distal
RR (95% Cl)
1.00 (0.56, 1.79)
0.52 (0.30, 0.93)
Steinmetz, 1994 [37]
IWHS Steinmetz, 1994 [37]
10.125 0.25 0.5 2 4 8
≥1 versus 0serv/day
≥1 versus 0serv/day
Figure 5: Estimates of relative risk with 95% CI for the highest versus the lowest exposure categories of garlic. (Closed black circles: females.)
of rectal cancer with 30% (95% CI 1.00–1.68) compared toconsuming 1.6 gram or less per 1000 kcal [35]. No significantassociations were seen in Swedish [32] and Japanese studies[34].
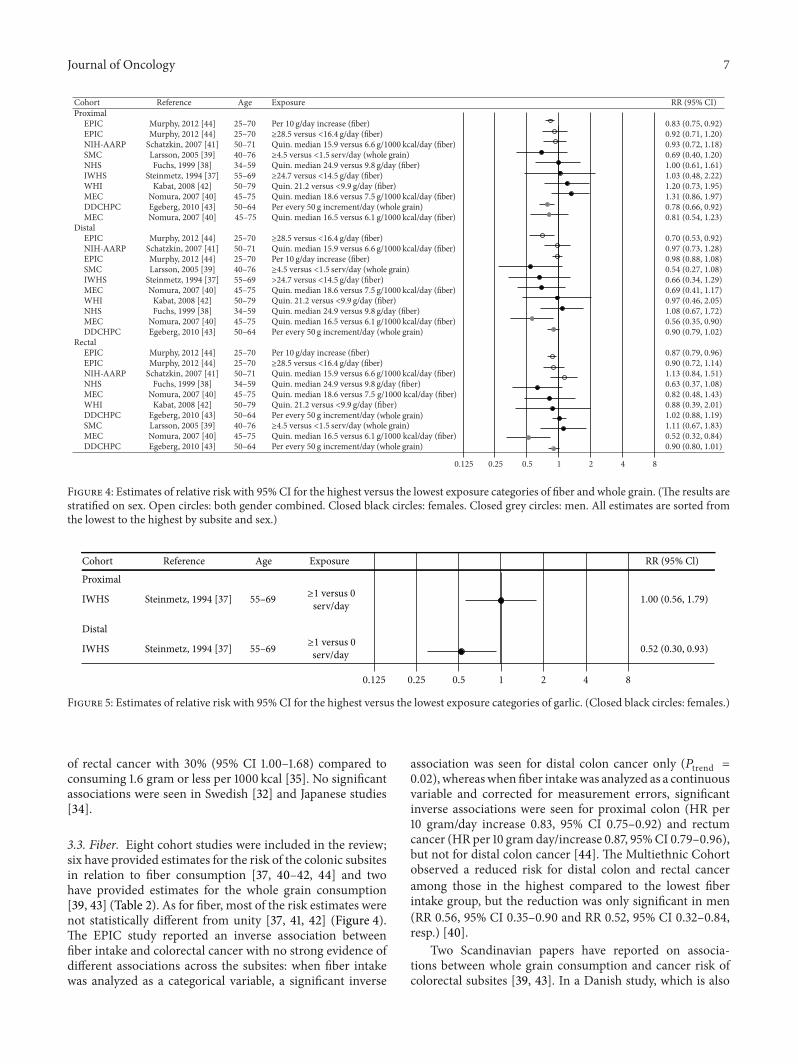
3.3. Fiber. Eight cohort studies were included in the review;six have provided estimates for the risk of the colonic subsitesin relation to fiber consumption [37, 40–42, 44] and twohave provided estimates for the whole grain consumption[39, 43] (Table 2). As for fiber, most of the risk estimates werenot statistically different from unity [37, 41, 42] (Figure 4).The EPIC study reported an inverse association betweenfiber intake and colorectal cancer with no strong evidence ofdifferent associations across the subsites: when fiber intakewas analyzed as a categorical variable, a significant inverse
association was seen for distal colon cancer only (𝑃trend =
0.02), whereaswhenfiber intakewas analyzed as a continuousvariable and corrected for measurement errors, significantinverse associations were seen for proximal colon (HR per10 gram/day increase 0.83, 95% CI 0.75–0.92) and rectumcancer (HR per 10 gramday/increase 0.87, 95%CI 0.79–0.96),but not for distal colon cancer [44]. The Multiethnic Cohortobserved a reduced risk for distal colon and rectal canceramong those in the highest compared to the lowest fiberintake group, but the reduction was only significant in men(RR 0.56, 95% CI 0.35–0.90 and RR 0.52, 95% CI 0.32–0.84,resp.) [40].
Two Scandinavian papers have reported on associa-tions between whole grain consumption and cancer risk ofcolorectal subsites [39, 43]. In a Danish study, which is also
8 Journal of Oncology
Cohort Reference Exposure RR (95% CI)Proximal
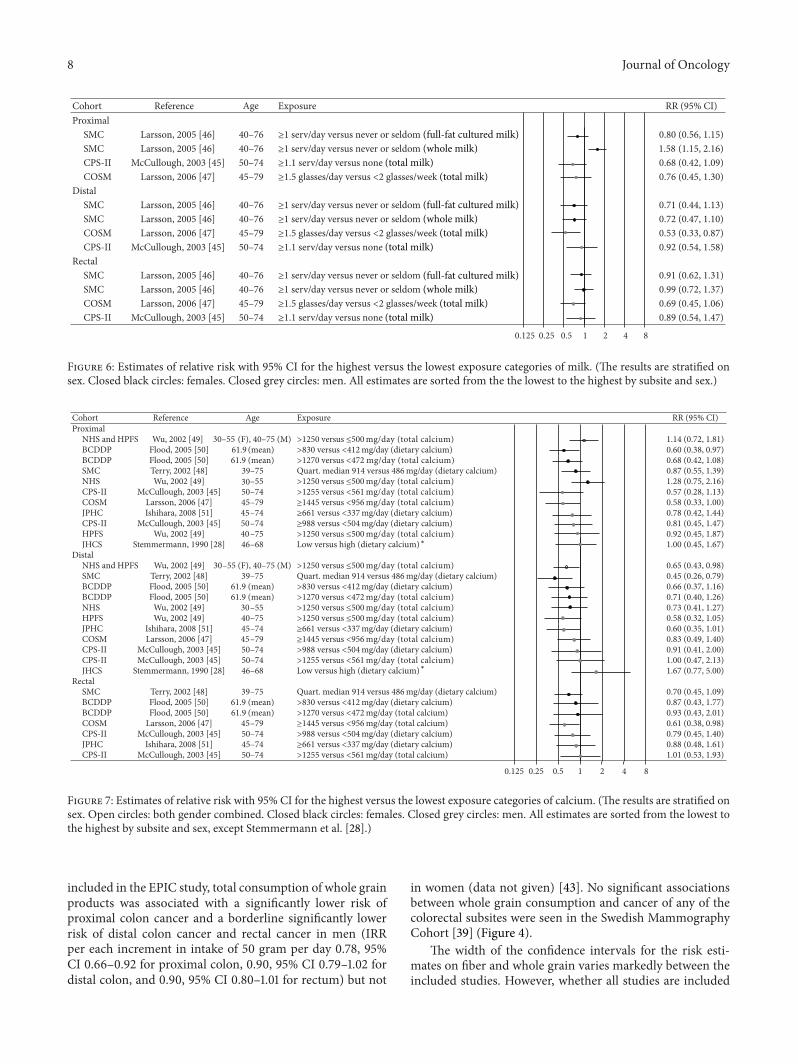
SMC Larsson, 2005 [46] 40–76 ≥1 serv/day versus never or seldom 0.80 (0.56, 1.15)SMC Larsson, 2005 [46] 40–76 ≥1 serv/day versus never or seldom 1.58 (1.15, 2.16)CPS-II McCullough, 2003 [45] 50–74 ≥1.1 serv/day versus none 0.68 (0.42, 1.09)COSM Larsson, 2006 [47] 45–79 ≥1.5 glasses/day versus <2 glasses/week 0.76 (0.45, 1.30)
DistalSMC Larsson, 2005 [46] 40–76 ≥1 serv/day versus never or seldom 0.71 (0.44, 1.13)SMC Larsson, 2005 [46] 40–76 ≥1 serv/day versus never or seldom 0.72 (0.47, 1.10)COSM Larsson, 2006 [47] 45–79 ≥1.5 glasses/day versus <2 glasses/week 0.53 (0.33, 0.87)CPS-II McCullough, 2003 [45] 50–74 ≥1.1 serv/day versus none 0.92 (0.54, 1.58)
RectalSMC Larsson, 2005 [46] 40–76 ≥1 serv/day versus never or seldom 0.91 (0.62, 1.31)SMC Larsson, 2005 [46] 40–76 ≥1 serv/day versus never or seldom 0.99 (0.72, 1.37)COSM Larsson, 2006 [47] 45–79 ≥1.5 glasses/day versus <2 glasses/week 0.69 (0.45, 1.06)CPS-II McCullough, 2003 [45] 50–74 ≥1.1 serv/day versus none 0.89 (0.54, 1.47)
10.125 0.25 0.5 2 4 8
(full-fat cultured milk)
(full-fat cultured milk)
(full-fat cultured milk)
(whole milk)
(whole milk)
(whole milk)
(total milk)(total milk)
(total milk)(total milk)
(total milk)(total milk)
Age
Figure 6: Estimates of relative risk with 95% CI for the highest versus the lowest exposure categories of milk. (The results are stratified onsex. Closed black circles: females. Closed grey circles: men. All estimates are sorted from the the lowest to the highest by subsite and sex.)
(RRerusopxEegAecnerefeRtrohoC 95% CI)Proximal
NHS and HPFS
NHS and HPFS
30–55 (F), 40–75 (M) >1250 versus ≤500 mg/day (total calcium) 1.14 (0.72, 1.81)BCDDP Flood, 2005 [50]
2005 [50]
2005 [50]2005 [50]2006 [47]
2003 [45]
2003 [45]2008 [51]
(mean) >830 versus <412 mg/day (dietary calcium)
mg/day (dietary calcium)mg/day (dietary calcium)
0.60 (0.38, 0.97)BCDDP Flood, (mean)
30504545504046
>1270 versus <472 mg/day (total calcium) 0.68 (0.42, 1.08)SMC Terry, 2002 [48]
2002 [49]
39–75 Quart. median 914 versus 486 mg/day (dietary calcium) 0.87 (0.55, 1.39)NHS Wu, –55 >1250 versus ≤500 mg/day (total calcium) 1.28 (0.75, 2.16)CPS-II McCullough, 2003 [45] –74 >1255 versus <561 mg/day (total calcium) 0.57 (0.28, 1.13)COSM Larsson, 2006 [47] –79 ≥1445 versus <956 mg/day (total calcium)
mg/day (total calcium)
mg/day (total calcium)
0.58 (0.33, 1.00)JPHC Ishihara, 2008 [51] –74 ≥661 versus <337 0.78 (0.42, 1.44)CPS-II McCullough, 2003 [45] –74 ≥988 versus <504 0.81 (0.45, 1.47)HPFS Wu, 2002 [49] –75 >1250 versus ≤500 0.92 (0.45, 1.87)JHCS Stemmermann, 1990 [28] –68 Low versus high (dietary calcium) 1.00 (0.45, 1.67)
Distal–5530
39
30
40
45
45
50
50
46
39
45
50
50
45
61.9
61.9
(F), 40–75 (M) >1250 versus ≤500 0.65 (0.43, 0.98)SMC Terry, 2002 [48] –75 Quart. median 914 versus 486 mg/day (dietary calcium) 0.45 (0.26, 0.79)BCDDP Flood, 2005 [50] (mean) >830 versus <412 mg/day (dietary calcium) 0.66 (0.37, 1.16)BCDDP Flood, (mean) >1270 versus <472 mg/day (total calcium) 0.71 (0.40, 1.26)NHS Wu, 2002 [49] –55 >1250 versus ≤500 mg/day (total calcium) 0.73 (0.41, 1.27)HPFS Wu, –75 >1250 versus ≤500 mg/day (total calcium) 0.58 (0.32, 1.05)JPHC Ishihara, –74 ≥661 versus <337 mg/day (dietary calcium) 0.60 (0.35, 1.01)COSM Larsson, –79 ≥1445 versus <956 mg/day (total calcium) 0.83 (0.49, 1.40)CPS-II McCullough, 2003 [45] –74 >988 versus <504 mg/day (dietary calcium) 0.91 (0.41, 2.00)CPS-II McCullough, 2003 [45] –74 >1255 versus <561 mg/day (total calcium) 1.00 (0.47, 2.13)JHCS Stemmermann, 1990 [28] –68 Low versus high (dietary calcium) 1.67 (0.77, 5.00)
RectalSMC Terry, 2002 [48] –75 Quart. median 914 versus 486 mg/day (dietary calcium) 0.70 (0.45, 1.09)BCDDP Flood, (mean) >830 versus <412 mg/day (dietary calcium) 0.87 (0.43, 1.77)BCDDP Flood, (mean) >1270 versus <472 mg/day (total calcium) 0.93 (0.43, 2.01)COSM Larsson, –79 ≥1445 versus <956 mg/day (total calcium) 0.61 (0.38, 0.98)CPS-II McCullough, –74 >988 versus <504 mg/day (dietary calcium) 0.79 (0.45, 1.40)JPHC Ishihara, –74 ≥661 versus <337 mg/day (dietary calcium) 0.88 (0.48, 1.61)CPS-II McCullough, –74 >1255 versus <561 mg/day (total calcium) 1.01 (0.53, 1.93)
10.125 0.25 0.5 2 4 8
∗
∗
Wu, 2002 [49]
Wu, 2002 [49]
61.9
61.9
61.9
61.9
2005 [50]
2002 [49]2008 [51]2006 [47]
Figure 7: Estimates of relative risk with 95% CI for the highest versus the lowest exposure categories of calcium. (The results are stratified onsex. Open circles: both gender combined. Closed black circles: females. Closed grey circles: men. All estimates are sorted from the lowest tothe highest by subsite and sex, except Stemmermann et al. [28].)
included in the EPIC study, total consumption of whole grainproducts was associated with a significantly lower risk ofproximal colon cancer and a borderline significantly lowerrisk of distal colon cancer and rectal cancer in men (IRRper each increment in intake of 50 gram per day 0.78, 95%CI 0.66–0.92 for proximal colon, 0.90, 95% CI 0.79–1.02 fordistal colon, and 0.90, 95% CI 0.80–1.01 for rectum) but not
in women (data not given) [43]. No significant associationsbetween whole grain consumption and cancer of any of thecolorectal subsites were seen in the Swedish MammographyCohort [39] (Figure 4).
The width of the confidence intervals for the risk esti-mates on fiber and whole grain varies markedly between theincluded studies. However, whether all studies are included
Journal of Oncology 9
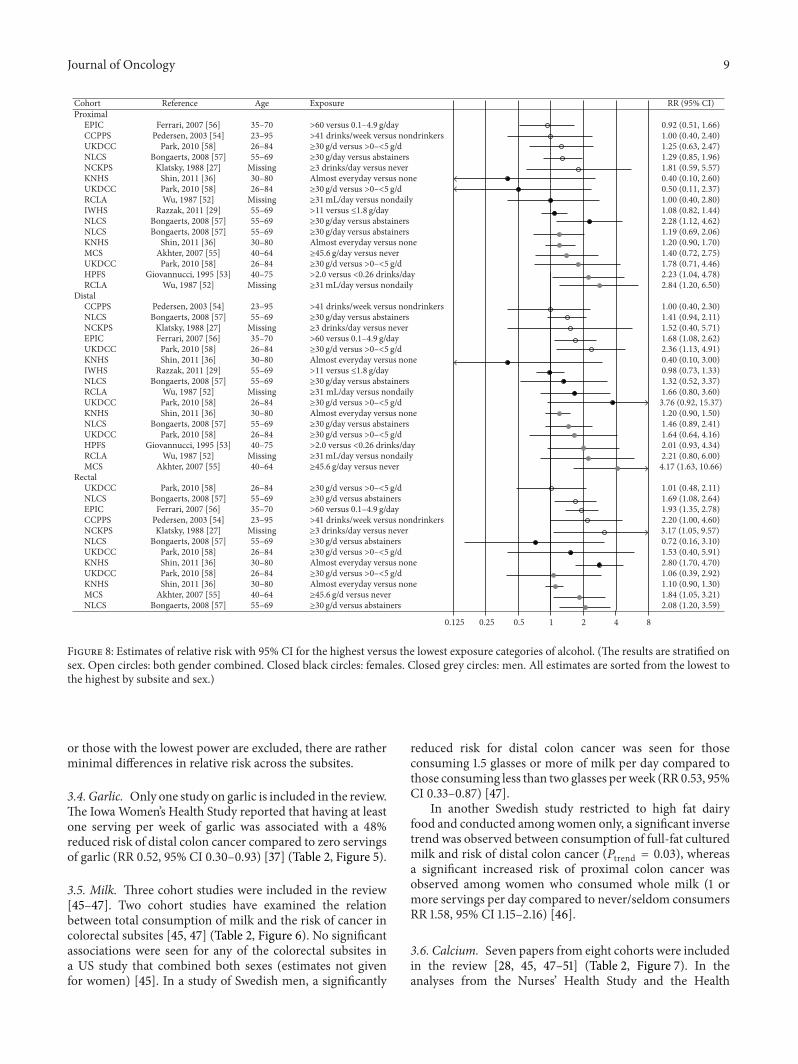
Cohort Reference Age Exposure RR (95% CI)Proximal
EPIC Ferrari, 2007 [56] 35–70 >60 versus 0.1–4.9 g/day 0.92 (0.51, 1.66)CCPPS Pedersen, 2003 [54] 23–95 >41 drinks/week versus nondrinkers 1.00 (0.40, 2.40)UKDCC Park, 2010 [58] 26–84 ≥30 g/d versus >0–<5 g/d 1.25 (0.63, 2.47)NLCS Bongaerts, 2008 [57] 55–69 ≥30 g/day versus abstainers 1.29 (0.85, 1.96)NCKPS Klatsky, 1988 [27] Missing ≥3 drinks/day versus never 1.81 (0.59, 5.57)KNHS Shin, 2011 [36] 30–80 Almost everyday versus none 0.40 (0.10, 2.60)UKDCC Park, 2010 [58] 26–84 ≥30 g/d versus >0–<5 g/d 0.50 (0.11, 2.37)RCLA Wu, 1987 [52] Missing ≥31 mL/day versus nondaily 1.00 (0.40, 2.80)IWHS Razzak, 2011 [29] 55–69 >11 versus ≤1.8 g/day 1.08 (0.82, 1.44)NLCS Bongaerts, 2008 [57] 55–69 ≥30 g/day versus abstainers 2.28 (1.12, 4.62)NLCS Bongaerts, 2008 [57] 55–69 ≥30 g/day versus abstainers 1.19 (0.69, 2.06)KNHS Shin, 2011 [36] 30–80 Almost everyday versus none 1.20 (0.90, 1.70)MCS Akhter, 2007 [55] 40–64 ≥45.6 g/day versus never 1.40 (0.72, 2.75)UKDCC Park, 2010 [58] 26–84 ≥30 g/d versus >0–<5 g/d 1.78 (0.71, 4.46)HPFS Giovannucci, 1995 [53] 40–75 >2.0 versus <0.26 drinks/day 2.23 (1.04, 4.78)RCLA Wu, 1987 [52] Missing ≥31 mL/day versus nondaily 2.84 (1.20, 6.50)
DistalCCPPS Pedersen, 2003 [54] 23–95 >41 drinks/week versus nondrinkers 1.00 (0.40, 2.30)NLCS Bongaerts, 2008 [57] 55–69 ≥30 g/day versus abstainers 1.41 (0.94, 2.11)NCKPS Klatsky, 1988 [27] Missing ≥3 drinks/day versus never 1.52 (0.40, 5.71)EPIC Ferrari, 2007 [56] 35–70 >60 versus 0.1–4.9 g/day 1.68 (1.08, 2.62)UKDCC Park, 2010 [58] 26–84 ≥30 g/d versus >0–<5 g/d 2.36 (1.13, 4.91)KNHS Shin, 2011 [36] 30–80 Almost everyday versus none 0.40 (0.10, 3.00)IWHS Razzak, 2011 [29] 55–69 >11 versus ≤1.8 g/day 0.98 (0.73, 1.33)NLCS Bongaerts, 2008 [57] 55–69 ≥30 g/day versus abstainers 1.32 (0.52, 3.37)RCLA Wu, 1987 [52] Missing ≥31 mL/day versus nondaily 1.66 (0.80, 3.60)UKDCC Park, 2010 [58] 26–84 ≥30 g/d versus >0–<5 g/d 3.76 (0.92, 15.37)KNHS Shin, 2011 [36] 30–80 Almost everyday versus none 1.20 (0.90, 1.50)NLCS Bongaerts, 2008 [57] 55–69 ≥30 g/day versus abstainers 1.46 (0.89, 2.41)UKDCC Park, 2010 [58] 26–84 ≥30 g/d versus >0–<5 g/d 1.64 (0.64, 4.16)HPFS Giovannucci, 1995 [53] 40–75 >2.0 versus <0.26 drinks/day 2.01 (0.93, 4.34)RCLA Wu, 1987 [52] Missing ≥31 mL/day versus nondaily 2.21 (0.80, 6.00)MCS Akhter, 2007 [55] 40–64 ≥45.6 g/day versus never 4.17 (1.63, 10.66)
RectalUKDCC Park, 2010 [58] 26–84 ≥30 g/d versus >0–<5 g/d 1.01 (0.48, 2.11)NLCS Bongaerts, 2008 [57] 55–69 ≥30 g/d versus abstainers 1.69 (1.08, 2.64)EPIC Ferrari, 2007 [56] 35–70 >60 versus 0.1–4.9 g/day 1.93 (1.35, 2.78)CCPPS Pedersen, 2003 [54] 23–95 >41 drinks/week versus nondrinkers 2.20 (1.00, 4.60)NCKPS Klatsky, 1988 [27] Missing ≥3 drinks/day versus never 3.17 (1.05, 9.57)
NLCS Bongaerts, 2008 [57] 55–69 ≥30 g/d versus abstainers 0.72 (0.16, 3.10)UKDCC Park, 2010 [58] 26–84 ≥30 g/d versus >0–<5 g/d 1.53 (0.40, 5.91)KNHS Shin, 2011 [36] 30–80 Almost everyday versus none 2.80 (1.70, 4.70)UKDCC Park, 2010 [58] 26–84 ≥30 g/d versus >0–<5 g/d 1.06 (0.39, 2.92)KNHS Shin, 2011 [36] 30–80 Almost everyday versus none 1.10 (0.90, 1.30)MCS Akhter, 2007 [55] 40–64 ≥45.6 g/d versus never 1.84 (1.05, 3.21)NLCS Bongaerts, 2008 [57] 55–69 ≥30 g/d versus abstainers 2.08 (1.20, 3.59)
10.125 0.25 0.5 2 4 8
Figure 8: Estimates of relative risk with 95% CI for the highest versus the lowest exposure categories of alcohol. (The results are stratified onsex. Open circles: both gender combined. Closed black circles: females. Closed grey circles: men. All estimates are sorted from the lowest tothe highest by subsite and sex.)
or those with the lowest power are excluded, there are ratherminimal differences in relative risk across the subsites.
3.4. Garlic. Only one study on garlic is included in the review.The IowaWomen’s Health Study reported that having at leastone serving per week of garlic was associated with a 48%reduced risk of distal colon cancer compared to zero servingsof garlic (RR 0.52, 95% CI 0.30–0.93) [37] (Table 2, Figure 5).
3.5. Milk. Three cohort studies were included in the review[45–47]. Two cohort studies have examined the relationbetween total consumption of milk and the risk of cancer incolorectal subsites [45, 47] (Table 2, Figure 6). No significantassociations were seen for any of the colorectal subsites ina US study that combined both sexes (estimates not givenfor women) [45]. In a study of Swedish men, a significantly
reduced risk for distal colon cancer was seen for thoseconsuming 1.5 glasses or more of milk per day compared tothose consuming less than two glasses perweek (RR 0.53, 95%CI 0.33–0.87) [47].
In another Swedish study restricted to high fat dairyfood and conducted among women only, a significant inversetrend was observed between consumption of full-fat culturedmilk and risk of distal colon cancer (𝑃trend = 0.03), whereasa significant increased risk of proximal colon cancer wasobserved among women who consumed whole milk (1 ormore servings per day compared to never/seldom consumersRR 1.58, 95% CI 1.15–2.16) [46].
3.6. Calcium. Seven papers from eight cohorts were includedin the review [28, 45, 47–51] (Table 2, Figure 7). In theanalyses from the Nurses’ Health Study and the Health

10 Journal of Oncology
Professionals Follow-Up Study that studied colon canceronly, non-significant inverse associations were seen betweentotal calcium and distal colon cancer for both men andwomen, and a pooled analysis of the two cohorts gave asignificant inverse trend for distal colon cancer (𝑃trend =
0.01) [49]. Likewise, a significant inverse trend was reportedbetween total calcium and distal colon cancer in the SwedishMammography Cohort (𝑃trend = 0.02) [48], while ina US female cohort, a significant inverse trend was seenbetween dietary calcium intake and proximal colon cancer(𝑃trend = 0.01) [50]. No association was seen for totalcalcium. In a US study examining both sexes, total calciumintake was significantly inversely associated with proximalcolon cancer among men (𝑃trend = 0.04), but not dietarycalcium, and there were no significant associations seen forwomen (estimates not given) [45]. In a study of Swedishmen,a significant inverse relation was found between total calciumand rectal cancer (𝑃trend = 0.02), whereas nonsignificantinverse associationswere seen for cancer of the colon [47]. Nosignificant associations between dietary calcium and cancerof any colorectal subsite were reported in a Japanese studyeither formen or for women (estimates not given for women)[51]. An earlier study of Hawaiian-Japanese men reported asignificant inverse association between dietary calcium andsigmoid colon cancer (𝑃trend = 0.02) [28]. In addition tothe eight cohorts included in this paper, an additional cohortstudy amongAmericanwomen states that their data providedlittle support for a protective effect of total calcium at eithertumor subsite, but does not present risk estimates [60].
3.7. Alcohol. Ten articles [27, 29, 36, 52–58] were includedin the review (Table 2). Three analyses for both sexes com-bined consistently showed a higher risk of rectal cancerwith increasing alcohol consumption and no significantassociations for any of the colon subsites [27, 54, 57]. Inthe EPIC study [56] an increased risk was reported both forrectal and distal colon cancer, whereas in the UK dietarycohort consortium (part of which is included in the EPICstudy) [58] a significantly increased risk was found for distalcolon cancer only (Figure 8). Several sex-specific analyseshave been done. Among men, two older studies with limitedstatistical power reported that alcohol consumption waspositively related to proximal colon cancer only [52, 53],whereas four more recent studies reported non-significantassociations with proximal colon cancer [36, 55, 57, 58]. Astudy among Japanese men reported increased risk for distalcolon cancer, but the confidence interval for the risk estimatewas very wide (consumption of 45.6 grams alcohol or moreper day compared to never drinkers HR 4.17, 95% CI 1.63–10.66) [55]. In terms of consumption of alcohol and rectumcancer among men, two of four studies have reported apositive association [55, 57].
For women, fewer significant associations have beenreported. In the Iowa Women’s Health Study, alcohol wasnot significantly associated with either proximal colon ordistal colorectal cancer, nor did further separation intodistal colon and rectal cancer reveal any significant associ-ations (estimates not given) [29]. Furthermore, no significantassociationswere seen in an earlier study ofAmericanwomen
[52] or in the UK dietary cohort consortium [58]. In TheNetherlands Cohort Study, however, women consuming 30grams or more of alcohol per day had HRR of proximal coloncancer of 2.28 (95% CI 1.12–4.62) compared to abstainers,whereas analyses for the other subsites were not sufficientlyrobust to draw any conclusions [57]. In a Korean study,women who frequently consumed alcohol or who consumedgreater amounts of alcohol had a higher risk of rectal cancer[36].
4. Discussion
This review provides an overall and updated synthesis ofthe results from cohort studies examining the associationbetween dietary factors that are convincingly or probablyrelated to the risk of colorectal cancer and subsite-specificcolorectal cancer. Our study indicates that consumption ofalcohol is more strongly related to the risk of rectal cancerthan to colon cancer, also that meat consumption tends tobe somewhat more strongly related to the risk of distal coloncancer and rectal cancer than proximal colon cancer, thatthere are only minor differences in relative risk for colorectalcancer across the major subsites for fiber, milk, and calcium,and that no statement can be given for garlic due to limiteddata. It should be noted that for all exposures the majority ofthe analyses showed nonsignificant associations with cancerrisk, the exception being the positive association betweenalcohol consumption and rectal cancer.
The pathway of colorectal cancer is complex. The subsiteetiology is rather poorly understood, and the mechanism forthe various dietary factors is likely to differ. Even for red andprocessed meat, both established risk factors for colorectalcancer, the underlying mechanisms are not well defined. Onesuggested mechanism for the somewhat stronger associationfor rectum and distal colon relative to proximal colon cancerrelates to the enhanced endogenous formation of carcino-genic N-nitroso compounds with a high intake of meat [61].The level of markers of N-nitroso compounds appears to behigher in tissue from distal colon and rectum than in thatof the proximal colon [62]. This finding is in keeping witha previously meta-analyses which implicated processed meatconsumption as a stronger risk factor for cancer occurrenceat the distal colon relative to the proximal colon [22].
A suggested mechanism by which dietary fiber maydecrease the risk of colorectal cancer is linked to the fer-mentation of fiber. The fermentation produces short-chainfatty acids and, in particular, acetic, propionic, and butyricacids. Butyrate is particularly of interest, as it has beenshown to induce apoptosis and to be cytotoxic to bothcolorectal adenoma and carcinoma cells [63]. Studies onmicehave shown that the concentration of butyrate is highestin the distal colon [64]. In humans, fiber is fermented inthe proximal colon, and the total amount of short-chainfatty acids has been estimated to be considerably higher inthe proximal site compared to the distal [65]. One studyon proximal and distal colonocytes indicates, however, thatbutyrate is a more important source of energy for the distal,than for the proximal, colonic mucosa [66]. If so, this

Journal of Oncology 11
could be a relevant biological mechanism explaining anydifferences in risk between the sites. In addition, fiber maydilute the concentration of carcinogenic substances in thedistal colon. Despite these findings, a pooled analysis on fiberreported no convincing differences in colorectal risk for thevarious anatomical subsites [25], in line with our own resultspublished here.
The reduced risk of colorectal cancer with increasingconsumption of milk is likely to be at least partly mediated bycalcium, which is thought to have a protective effect throughits ability to bind bile acids, and its growth-restraining anddifferentiation- and apoptosis-inducing effect on colorectalcells [67]. No convincing site-specific associations regardingmilk and calcium were seen in our review. A former pooledanalysis reported an inverse association for milk limited tocancer of the distal colon and rectum [24], while the resultsfrom two meta-analysis on site-specific impact of calciumhave been conflicting [20, 21].
The consumption of alcohol is associated with increas-ing risk of cancer in several organs in the digestive tract,including the colorectum [18]. Alcohol is not a carcinogenitself, but acts as a tumor promoter and possibly as a co-carcinogen. Alcohol also acts as a solvent and thus mightincrease the exposure to other carcinogens by enhancing thepenetration of carcinogens into the cell [18]. Acetaldehydeis a metabolite of alcohol and may be the most importantagent responsible for the carcinogenic effect as it is highlytoxic, mutagenic, and carcinogenic [68]. A pooled analyseson alcohol reported similar risk across all areas of the largebowel [26]. However, a stronger association with alcoholfor rectal cancer compared with colon cancer as seen inour paper could possibly be related to a higher degree ofepithelial hyperregeneration in rectum [69]. The numberof sex-specific analysis is presently too low to suggest anysignificant interaction by sex at the subsite level.
There are somemethodological issues in this study whichmay have impacted on the findings. There is considerablevariability in several key characteristics of the assembledcohort studies: the follow-up time across studies includedin this paper varied from 4 to 22 years, while the totalnumber of colorectal cancer cases analyzed ranged from126 to 2974. Short-term follow-up studies tend to accrue alower number of cases, and the resulting estimates are subjectto greater uncertainty. The substratification of cases by sex,tumor location, and exposure categories, as presented here,inevitably leads to smaller numbers and a greater degreeof imprecision in the estimates, even for relatively largestudies. Statistically significant associationsmay thus bemorespurious at the subsite-specific level. However, restrictingthe evaluation to studies with adequate statistical power didnot change the overall picture. Long-term follow-up studieswill commonly accrue a greater number of cases, but aremore prone to measurement error given that an increasingfollow-up time raises the possibility that exposure status ofthe participants will change, leading to misclassification ofexposure and under- or overestimation of the risk estimates.However, the natural history of colorectal cancer is on averageof long duration, and exposure in the more distant past maybe the most relevant when estimating subsequent risk.
Another issue is the difference in risk factor dosagesbetween studies and that the categories compared sometimesvary considerably between studies. For instance, for calcium,in the Swedish study by Larsson et al. [47] daily intakeof 1445mg or more is compared to an intake of less than956mg/day, whereas in the Japanese study by Ishihara et al.[51] daily intake of 661mg ormore is comparedwith an intakeof less than 337mg/day. Careful reading of the exposurecategories (given in the figures) is therefore necessary whenevaluating the findings. In addition, the specific confoundingfactors adjusted for at the analysis stage differ betweenstudies.
Of the studies that were full-text reviewed, 76 wereexcluded as they did not reveal information at the level ofsubsite location. Given the high proportion of cohort studiesfailing to report subsite-specific estimates, the potentialpublication bias prohibited a formal meta-analysis [59]. Afurther rationale for this decision is the lack of uniformity inexposure categories within each risk factor.
In summary, the strength of the association betweendietary components and cancer of the large bowel maypartially depend on the anatomic location within the colorec-tum. The most consistent finding is the stronger associationbetween alcohol and rectal cancer, compared with alcoholand proximal and distal colon cancer. Meat (red and pro-cessed) is possibly more strongly associated with risk of distalcolon cancer and rectal cancer than the risk of proximal coloncancer. For fiber, milk, and calcium there seem to be onlyminor differences in relative risk across the subsites.However,caution is required as the number of papers presenting riskestimates by colorectal subsite is limited, particularly formilkand garlic. Also, most of the subsite-specific analyses reportnon-significant findings.
Conflict of Interests
The authors declare that they have no conflict of interests.
Acknowledgment
Theauthors thank Lena Leder for her contribution to the dataextraction and paper preparation.
References
[1] J. Ferlay, H. R. Shin, F. Bray, D. Forman, C. Mathers, and D.M. Parkin, GLOBOCAN 2008: Cancer Incidence and MortalityWorldwide, IARC Cancer Base, no. 10, International Agency forResearch on Cancer, Lyon, France, 2012.
[2] F. Kee, R. H. Wilson, R. Gilliland, J. M. Sloan, B. J. Rowlands,and R. J. Moorehead, “Changing site distribution of colorectalcancer,” British Medical Journal, vol. 305, no. 6846, p. 158, 1992.
[3] G. I. Slater, R. H. Haber, and A. H. Aufses Jr., “Changingdistribution of carcinoma of the colon and rectum,” Surgery,Gynecology & Obstetrics, vol. 158, pp. 216–218, 1984.
[4] Y. Toyoda, T. Nakayama, Y. Ito, A. Ioka, and H. Tsukuma,“Trends in colorectal cancer incidence by subsite in Osaka,Japan,” Japanese Journal of Clinical Oncology, vol. 39, no. 3, pp.189–191, 2009.

12 Journal of Oncology
[5] C. Cucino, A. M. Buchner, and A. Sonnenberg, “Continuedrightward shift of colorectal cancer,” Diseases of the Colon andRectum, vol. 45, no. 8, pp. 1035–1040, 2002.
[6] S. L. Saltzstein and C. A. Behling, “Age and time as factors in theleft-to-right shift of the subsite of colorectal adenocarcinoma:a study of 213,383 cases from the California Cancer Registry,”Journal of Clinical Gastroenterology, vol. 41, no. 2, pp. 173–177,2007.
[7] R. W. Beart, L. J. Melton, M. Maruta, M. B. Dockerty, H. B.Frydenberg, andW.M.O’Fallon, “Trends in right and left-sidedcolon cancer,” Diseases of the Colon & Rectum, vol. 26, pp. 393–398, 1983.
[8] F. Levi, L. Randimbison, and C. La Vecchia, “Trends in subsitedistribution of colorectal cancers and polyps from the VaudCancer Registry,” Cancer, vol. 72, no. 1, pp. 46–50, 1993.
[9] E. Mitry, A. M. Benhamiche, C. Couillault et al., “Effect of age,period of diagnosis and birth cohort on large bowel cancerincidence in a well-defined French population, 1976–1995,”European Journal of Cancer Prevention, vol. 11, no. 6, pp. 529–534, 2002.
[10] H. Singh, A. A. Demers, L. Xue, D. Turner, and C. N. Bern-stein, “Time trends in colon cancer incidence and distributionand lower gastrointestinal endoscopy utilization in Manitoba,”American Journal of Gastroenterology, vol. 103, no. 5, pp. 1249–1256, 2008.
[11] H. Takada, T. Ohsawa, S. Iwamoto et al., “Changing sitedistribution of colorectal cancer in Japan,”Diseases of the Colon& Rectum, vol. 45, pp. 1249–1254, 2002.
[12] M. Thorn, R. Bergstrom, U. Kressner, P. Sparen, M. Zack, andA. Ekbom, “Trends in colorectal cancer incidence in Sweden1959–93 by gender, localization, time period, and birth cohort,”Cancer Causes and Control, vol. 9, no. 2, pp. 145–152, 1998.
[13] J. R. Jass, “Subsite distribution and incidence of colorectalcancer in New Zealand, 1974–1983,” Diseases of the Colon &Rectum, vol. 34, pp. 56–59, 1991.
[14] R. Scheiden, P. Pescatore, Y. Wagener, N. Kieffer, and C.Capesius, “Colon cancer in Luxembourg: a national population-based data report, 1988–1998,” BMC Cancer, vol. 5, article 52,2005.
[15] I. K. Larsen and F. Bray, “Trends in colorectal cancer incidencein Norway 1962–2006: an interpretation of the temporal pat-terns by anatomic subsite,” International Journal of Cancer, vol.126, no. 3, pp. 721–732, 2010.
[16] F. Y. Li and M. D. Lai, “Colorectal cancer, one entity or three,”Journals of Zhejiang University-Science B, vol. 10, pp. 219–229,2009.
[17] M. L. Slattery, K. Curtin, R. K. Wolff et al., “A comparison ofcolon and rectal somatic DNA alterations,”Diseases of the Colon& Rectum, vol. 52, no. 7, pp. 1304–1311, 2009.
[18] World Cancer Research Found and American Institute forCancer Research, Food, Nutrition, Physical Activity, and thePrevention of Cancer: A Global Perspective, Washington, DC,USA, 2007.
[19] World Cancer Research Found and American Institute forCancer Research, Food, Nutrition, Physical Activity, and thePrevention of Colorectal Cancer. Continuous Update Project,Colorectal Cancer Report 2010, Summary, Washington, DC,USA, 2011.
[20] M. Huncharek, J. Muscat, and B. Kupelnick, “Colorectal cancerrisk and dietary intake of calcium, vitamin D, and dairy
products: a meta-analysis of 26,335 cases from 60 observationalstudies,” Nutrition and Cancer, vol. 61, no. 1, pp. 47–69, 2009.
[21] J. A. Bergsma-Kadijk, P. van’t Veer, E. Kampman, and J. Burema,“Calcium does not protect against colorectal neoplasia,” Epi-demiology, vol. 7, no. 6, pp. 590–597, 1996.
[22] S. C. Larsson and A. Wolk, “Meat consumption and riskof colorectal cancer: a meta-analysis of prospective studies,”International Journal of Cancer, vol. 119, no. 11, pp. 2657–2664,2006.
[23] D. S. Chan, R. Lau, D. Aune et al., “Red and processed meatand colorectal cancer incidence: meta-analysis of prospectivestudies,” PLoS ONE, vol. 6, no. 6, article e20456, 2011.
[24] E. Cho, S. A. Smith-Warner, D. Spiegelman et al., “Dairy foods,calcium, and colorectal cancer: a pooled analysis of 10 cohortstudies,” Journal of the National Cancer Institute, vol. 96, pp.1015–1022, 2004.
[25] Y. Park, D. J. Hunter, D. Spiegelman et al., “Dietary fiberintake and risk of colorectal cancer: a pooled analysis ofprospective cohort studies,”The Journal of the AmericanMedicalAssociation, vol. 294, pp. 2849–2857, 2005.
[26] E. Cho, S. A. Smith-Warner, J. Ritz et al., “Alcohol intake andcolorectal cancer: a pooled analysis of 8 cohort studies,” Annalsof Internal Medicine, vol. 140, pp. 603–613, 2004.
[27] A. L. Klatsky,M.A.Armstrong,G.D. Friedman, andR.A.Hiatt,“The relations of alcoholic beverage use to colon and rectalcancer,” American Journal of Epidemiology, vol. 128, no. 5, pp.1007–1015, 1988.
[28] G. N. Stemmermann, A. Nomura, and P. H. Chyou, “Theinfluence of dairy and nondairy calcium on subsite large-bowelcancer risk,”Diseases of the Colon and Rectum, vol. 33, no. 3, pp.190–194, 1990.
[29] A. A. Razzak, A. S. Oxentenko, R. A. Vierkant et al., “Alcoholintake and colorectal cancer risk by molecularly defined sub-types in a prospective study of older women,”Cancer PreventionResearch, vol. 4, pp. 2035–2043, 2011.
[30] E. Giovannucci, E. B. Rimm, M. J. Stampfer, G. A. Colditz, A.Ascherio, and W. C. Willett, “Intake of fat, meat, and fiber inrelation to risk of colon cancer in men,” Cancer Research, vol.54, no. 9, pp. 2390–2397, 1994.
[31] A. Chao,M. J.Thun, C. J. Connell et al., “Meat consumption andrisk of colorectal cancer,” The Journal of the American MedicalAssociation, vol. 293, pp. 172–182, 2005.
[32] S. C. Larsson, J. Rafter, L. Holmberg, L. Bergkvist, and A. Wolk,“Red meat consumption and risk of cancers of the proximalcolon, distal colon and rectum: the Swedish MammographyCohort,” International Journal of Cancer, vol. 113, no. 5, pp. 829–834, 2005.
[33] T. Norat, S. Bingham, P. Ferrari et al., “Meat, fish, and colorectalcancer risk: the European Prospective Investigation into cancerand nutrition,” Journal of the National Cancer Institute, vol. 97,no. 12, pp. 906–916, 2005.
[34] Y. Sato, N. Nakaya, S. Kuriyama, Y. Nishino, Y. Tsubono, andI. Tsuji, “Meat consumption and risk of colorectal cancer inJapan: the Miyagi cohort study,” European Journal of CancerPrevention, vol. 15, no. 3, pp. 211–218, 2006.
[35] A. J. Cross, L. M. Ferrucci, A. Risch et al., “A large prospectivestudy of meat consumption and colorectal cancer risk: an inves-tigation of potential mechanisms underlying this association,”Cancer Research, vol. 70, no. 6, pp. 2406–2414, 2010.
Journal of Oncology 13
[36] A. Shin, J. Joo, J. Bak et al., “Site-specific risk factors forcolorectal cancer in a Korean population,” PLoS One, vol. 6,article e23196, 2011.
[37] K. A. Steinmetz, L. H. Kushi, R. M. Bostick, A. R. Folsom, andJ. D. Potter, “Vegetables, fruit, and colon cancer in the Iowawomen’s health study,” American Journal of Epidemiology, vol.139, no. 1, pp. 1–15, 1994.
[38] C. S. Fuchs, E. L. Giovannucci, G. A. Colditz et al., “Dietary fiberand the risk of colorectal cancer and adenoma in women,” NewEngland Journal of Medicine, vol. 340, no. 3, pp. 169–176, 1999.
[39] S. C. Larsson, E. Giovannucci, L. Bergkvist, and A. Wolk,“Whole grain consumption and risk of colorectal cancer: apopulation-based cohort of 60 000 women,” British Journal ofCancer, vol. 92, no. 9, pp. 1803–1807, 2005.
[40] A. M. Nomura, J. H. Hankin, B. E. Henderson et al., “Dietaryfiber and colorectal cancer risk: the multiethnic cohort study,”Cancer Causes and Control, vol. 18, no. 7, pp. 753–764, 2007.
[41] A. Schatzkin, T. Mouw, Y. Park et al., “Dietary fiber and whole-grain consumption in relation to colorectal cancer in the NIH-AARP Diet and Health Study,” American Journal of ClinicalNutrition, vol. 85, no. 5, pp. 1353–1360, 2007.
[42] G. C. Kabat, J. M. Shikany, S. A. Beresford et al., “Dietarycarbohydrate, glycemic index, and glycemic load in relation tocolorectal cancer risk in the Women’s Health Initiative,” CancerCauses and Control, vol. 19, no. 10, pp. 1291–1298, 2008.
[43] R. Egeberg, A. Olsen, S. Loft et al., “Intake of wholegrainproducts and risk of colorectal cancers in the Diet, Cancer andHealth cohort study,” British Journal of Cancer, vol. 103, no. 5,pp. 730–734, 2010.
[44] N. Murphy, T. Norat, P. Ferrari et al., “Dietary fibre intakeand risks of cancers of the colon and rectum in the EuropeanProspective Investigation into Cancer and Nutrition (EPIC),”PLoS One, vol. 7, article e39361, 2012.
[45] M. L. McCullough, A. S. Robertson, C. Rodriguez et al.,“Calcium, vitamin D, dairy products, and risk of colorectalcancer in the Cancer Prevention Study II Nutrition Cohort(United States),” Cancer Causes and Control, vol. 14, no. 1, pp.1–12, 2003.
[46] S. C. Larsson, L. Bergkvist, and A. Wolk, “High-fat dairy foodand conjugated linoleic acid intakes in relation to colorectalcancer incidence in the SwedishMammographyCohort,”Amer-ican Journal of Clinical Nutrition, vol. 82, no. 4, pp. 894–900,2005.
[47] S. C. Larsson, L. Bergkvist, J. Rutegard, E. Giovannucci, and A.Wolk, “Calcium and dairy food intakes are inversely associatedwith colorectal cancer risk in the Cohort of Swedish Men,”American Journal of Clinical Nutrition, vol. 83, no. 3, pp. 667–673, 2006.
[48] P. Terry, J. A. Baron, L. Bergkvist, L. Holmberg, and A. Wolk,“Dietary calcium and vitamin D intake and risk of colorectalcancer: a prospective cohort study in women,” Nutrition andCancer, vol. 43, no. 1, pp. 39–46, 2002.
[49] K. Wu, W. C. Willett, C. S. Fuchs, G. A. Colditz, and E.L. Giovannucci, “Calcium intake and risk of colon cancer inwomen and men,” Journal of the National Cancer Institute, vol.94, no. 6, pp. 437–446, 2002.
[50] A. Flood, U. Peters, N. Chatterjee, J. V. Lacey Jr., C. Schairer, andA. Schatzkin, “Calcium from diet and supplements is associatedwith reduced risk of colorectal cancer in a prospective cohort ofwomen,” Cancer Epidemiology Biomarkers and Prevention, vol.14, no. 1, pp. 126–132, 2005.
[51] J. Ishihara, M. Inoue, M. Iwasaki, S. Sasazuki, and S. Tsugane,“Dietary calcium, vitamin D, and the risk of colorectal cancer,”American Journal of Clinical Nutrition, vol. 88, no. 6, pp. 1576–1583, 2008.
[52] A. H. Wu, A. Paganini-Hill, R. K. Ross, and B. E. Henderson,“Alcohol, physical activity and other risk factors for colorectalcancer: a prospective study,” British Journal of Cancer, vol. 55,no. 6, pp. 687–694, 1987.
[53] E. Giovannucci, E. B. Rimm, A. Ascherio, M. J. Stampfer, G.A. Colditz, and W. C. Willett, “Alcohol, low-methionine—low-folate diets, and risk of colon cancer in men,” Journal of theNational Cancer Institute, vol. 87, no. 4, pp. 265–273, 1995.
[54] A. Pedersen, C. Johansen, andM.Grønbæk, “Relations betweenamount and type of alcohol and colon and rectal cancer in aDanish population based cohort study,” Gut, vol. 52, no. 6, pp.861–867, 2003.
[55] M. Akhter, S. Kuriyama, N.Nakaya et al., “Alcohol consumptionis associated with an increased risk of distal colon and rectalcancer in Japanese men: the Miyagi Cohort Study,” EuropeanJournal of Cancer, vol. 43, no. 2, pp. 383–390, 2007.
[56] P. Ferrari, M. Jenab, T. Norat et al., “Lifetime and baselinealcohol intake and risk of colon and rectal cancers in theEuropean prospective investigation into cancer and nutrition(EPIC),” International Journal of Cancer, vol. 121, no. 9, pp.2065–2072, 2007.
[57] B.W. C. Bongaerts, P. A. van den Brandt, R. A. Goldbohm, A. F.P. M. de Goeij, and M. P. Weijenberg, “Alcohol consumption,type of alcoholic beverage and risk of colorectal cancer atspecific subsites,” International Journal of Cancer, vol. 123, no.10, pp. 2411–2417, 2008.
[58] J. Y. Park, C. C. Dahm, R. H. Keogh et al., “Alcohol intake andrisk of colorectal cancer: results from the UK Dietary CohortConsortium,” British Journal of Cancer, vol. 103, no. 5, pp. 747–756, 2010.
[59] M. Egger, G. D. Smith, and J. A. Sterne, “Uses and abuses ofmeta-analysis,” Clinical Medicine, vol. 1, pp. 478–484, 2001.
[60] J. Lin, S. M. Zhang, N. R. Cook, J. E. Manson, I. M. Lee, and J. E.Buring, “Intakes of calcium and vitaminD and risk of colorectalcancer in women,” American Journal of Epidemiology, vol. 161,no. 8, pp. 755–764, 2005.
[61] S. A. Bingham, R. Hughes, and A. J. Cross, “Effect of whiteversus red meat on endogenous N-nitrosation in the humancolon and further evidence of a dose response,” Journal ofNutrition, vol. 132, no. 11, pp. 3522S–3525S, 2002.
[62] A. C. Povey, C. N. Hall, A. F. Badawi, D. P. Cooper, and P.J. O’Connor, “Elevated levels of the pro-carcinogenic adduct,O(6)-methylguanine, in normal DNA from the cancer proneregions of the large bowel,”Gut, vol. 47, no. 3, pp. 362–365, 2000.
[63] A. Hague, A. M. Manning, K. A. Hanlon, L. I. Huschtscha, D.Hart, and C. Paraskeva, “Sodium butyrate induces apoptosisin human colonic tumour cell lines in a p53-independentpathway: implications for the possible role of dietary fibre inthe prevention of large-bowel cancer,” International Journal ofCancer, vol. 55, no. 3, pp. 498–505, 1993.
[64] W. Scheppach and F. Weiler, “The butyrate story: old winein new bottles?” Current Opinion in Clinical Nutrition andMetabolic Care, vol. 7, no. 5, pp. 563–567, 2004.
[65] J. M. Wong, R. de Souza, C. W. C. Kendall, A. Emam, and D.J. Jenkins, “Colonic health: fermentation and short chain fattyacids,” Journal of Clinical Gastroenterology, vol. 40, no. 3, pp.235–243, 2006.

14 Journal of Oncology
[66] W. E. Roediger, “Role of anaerobic bacteria in the metabolicwelfare of the colonic mucosa in man,” Gut, vol. 21, no. 9, pp.793–798, 1980.
[67] S. A. Lamprecht and M. Lipkin, “Chemoprevention of coloncancer by calcium, vitamin D and folate: molecular mecha-nisms,” Nature Reviews Cancer, vol. 3, no. 8, pp. 601–614, 2003.
[68] G. Poschl and H. K. Seitz, “Alcohol and cancer,” Alcohol andAlcoholism, vol. 39, no. 3, pp. 155–165, 2004.
[69] U. A. Simanowski, F. Stickel, H. Maier, U. Gartner, and H. K.Seitz, “Effect of alcohol on gastrointestinal cell regenerationas a possible mechanism in alcohol-associated carcinogenesis,”Alcohol, vol. 12, no. 2, pp. 111–115, 1995.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com