role of ureteroscopic biopsy in the management of upper urinary tract malignancy
TRANSCRIPT

International Journal of Urology
(2003)
10,
627–630
Blackwell Science, LtdOxford, UKIJUInternational Journal of Urology1442-20422003 Blackwell Publishing Asia Pty LtdDecember 20031012627630Original Article
Ureteroscopic biopsy for upper urinary tract TCCK Shiraishi
et al.
Correspondence: Koji Shiraishi
MD
,
P
h
D
, Department ofUrology, Saiseikai Shimonoseki General Hospital, 3-4-1Kifune-cho, Shimonoseki, Yamaguchi 751-8502, Japan.Email: [email protected]
Received 22 January 2003; accepted 16 June 2003.
Original Article
Role of ureteroscopic biopsy in the management ofupper urinary tract malignancy
KOJI SHIRAISHI, SATOSHI EGUCHI, JUN MOHRI AND YORIAKI KAMIRYO
Department of Urology, Saiseikai Shimonoseki General Hospital, Yamaguchi, Japan
Abstract
Background
: The aim of the study presented here was to examine the accuracy of ureteroscopicbiopsy in the diagnosis of upper urinary tract transitional cell carcinoma (TCC) and whethernephron-sparing management (holmium YAG laser, transurethral resection or partial ureterectomy)is possible or not based on pathological diagnosis.
Methods
: Forty consecutive patients underwent ureteroscopic biopsy with the use of 3-Fr cold cupforceps. Pathological diagnosis of the biopsy sample and grade or stage of surgically resected tumorswere compared. In patients with grade 1 or 2 TCC diagnosed by ureteroscopic biopsy, the disease-free and survival rates determined whether nephron-sparing management was performed or not.
Results
: There were no major complications associated with ureteroscopic biopsy. The pathologicalgrading of the biopsy specimen was almost the same as that of the surgically resected specimen.Eighty five percent of grade 2 or 3 TCC showed muscle invasive disease. There were no significantdifferences in the disease-free and survival rates between the nephroureterectomy and the nephron-sparing management groups, except for grade 3 or pT3 tumors.
Conclusion
: Ureteroscopic biopsy is safe and accurate if sufficient tissue sample is obtained.Ureteroscopic biopsy should be performed in patients who require nephron-sparing management.Nephroureterectomy can be avoided if the tumor is confirmed as low-grade.
Key words
biopsy, transitional cell carcinoma, upper urinary tract.
Introduction
Recent advances in ureteroscopy are changing the diag-nostic and treatment processes of upper urinary tractdiseases. Rigid or flexible small diameter ureteroscopyhas permitted direct examination and sampling of radio-logical abnormalities in the upper urinary tract. Neph-roureterectomy with excision of bladder cuff has beenthe treatment of choice for upper urinary tract transi-tional cell carcinoma (TCC).
1
Nephron-sparing manage-ment of upper urinary tract lesions has become anaccepted treatment option for patients with bilateral dis-ease, impaired renal function, or a solitary kidney.
2
Aswell as partial ureterectomy, endoscopic management ofupper urinary tract TCC, which includes endoscopicresection, holmium (Ho): or neodymium (Nd): yttrium-
aluminum-garnet (YAG) laser, has been widely prac-ticed.
3
In terms of stratifying patients and selecting thebest treatment according to prognosis, the use of uret-eroscopic biopsy in the diagnosis of upper tract TCCprovides accurate grading and staging information.
The accuracy and importance of ureteroscopic biopsyin the diagnosis of upper urinary tract tumors has alreadybeen reported.
2,4–6
However, ureteroscopic biopsy shouldbe performed less invasively because some complica-tions can arise, such as perforation, spillage of tumorcells and ureteral strictures.
3
To minimize the risk of thesecomplications, our method is to obtain biopsy specimensfrom the surface of the suspected lesion using 3-Fr coldcup forceps. We present here a series of patients whounderwent ureteroscopic biopsy in whom we comparedthe pathological grade obtained from ureteroscopicbiopsy to that of the surgically resected specimen. Addi-tionally, based on the histopathological findings obtainedfrom ureteroscopic biopsy, we examined the prognosis ofpatients who underwent nephron-sparing managementafter ureteroscopic biopsy.

628 K Shiraishi
et al.
Methods
From 1995 to 2001, 40 consecutive (24 men, 16 women)patients with a mean age of 69.7 years diagnosed byradiological and cytological examinations, were foundto have upper urinary tract tumors and underwent ure-teroscopic biopsy. Urine cytologies were obtained atleast once prior to ureteroscopic biopsy being per-formed. Under spinal anesthesia, the upper urinary tractwas examined using a combination of rigid and flexibleureteroscopes (external diameter, 8.5-Fr; tip, 7.0-Fr).Thirteen (33%) of the 40 lesions were located in therenal pelvis, and two (5%) in the upper, nine (23%) inthe middle and 16 (40%) in the lower ureter. Patientswith multiple tumors suspected by radiological findingsand/or ureteroscopic inspection were excluded from thestudy. After a lesion was found, the 3-Fr cold cup for-ceps were introduced through the ureteroscope, the sur-face of the lesion was grasped using the forceps and thetissue was pulled out along with the scope. The resultsof the ureteroscopic biopsy were compared with thepathological diagnosis of surgical specimens. As one ofnephron-sparing management options, we used Ho:YAG laser (Coherent Medical Systems, Palo Alto, CA,USA) with a frequency of 10 Hz. We began treatmentat the lowest available energy setting of 0.5 J and grad-ually increased the energy to 1.0 J as necessary untilfragmentation or vaporization was achieved.
Using the Kaplan–Meier method, we compared thedisease-free and cause-specific survival curves from theresults of ureteroscopic biopsy and surgical specimens.In addition, patients who underwent nephroureterec-tomy and those who underwent nephron-sparing man-agement were compared using the log–rank test.
Results
None of the patients had any major perioperative compli-cations. Transient gross hematuria, which was controlledby intravenous hemostatics, was observed in one patient.
Of the 40 patients, pathological diagnoses were con-ducted for 35 (88%). Another five patients could not be
diagnosed because the biopsy samples were not largeenough. Pathological diagnosis was grade 1 in four,grade 2 in 18, grade 3 in five patients, and no malig-nancy in eight (Table 1). We performed the operation inpatients who were positive for urine cytology or hadabnormal findings (papillary change, eruption or cysticchange) on ureteroscopic inspection, even if their uret-eroscopic biopsy results were insufficient or had nomalignancy. A total of 23 patients subsequently under-went nephroureterectomy. Nephron-sparing manage-ment included partial ureterectomy in six, openlaparotomy in two, and Ho: YAG laser in seven patients.Seven patients underwent imperative nephron-sparingmanagement because of impaired renal function or asolitary kidney. Another seven patients underwent elec-tive nephron-sparing management. These treatmentswere performed within 2 months after ureteroscopicbiopsy. Three patients were followed-up without anytreatment (Table 1). For 29 patients, pathological diag-nosis was available from both ureteroscopic and opensurgical specimens (Table 2). None of the 17 patientswith grade 1 or 2 ureteroscopic specimens had highgrade TCC on examination of the open surgical speci-men. Comparison of the ureteroscopic biopsy grade tothe tumor grade of the surgical specimen revealed anassociation between the ureteroscopic biopsy and surgi-cal pathological grade. Five of nine patients (56%) diag-nosed with no malignancy or insufficient sampleshowed grade 2 or 3 TCC. The pathological diagnosisfor no malignancy includes inflammatory polyp andothers include metastatic or invasive gastric cancer.Table 3 shows data regarding ureteroscopic biopsy andcorresponding surgical pathological stage for 27patients. As demonstrated, there is no correlationbetween ureteroscopic biopsy grade and subsequent sur-gical pathological stage. Seventeen of 20 (85%) of grade2 or 3 tumors showed muscle invasive disease. Voidedurine cytology was positive (class IV or V) for 0/2 (0%)in grade 1, 8/15 (53%) in grade 2, 4/5 (80%) in grade3, 3/6 (50%) in no malignancy, 2/3 (67%) in insufficientsamples according to the results of ureteroscopic biopsy.Figures show the disease-free and survival curves ofgrade 1 or 2 TCC after treatment, except for pT3
Table 1
Management of upper urinary tract transitional cell carcinoma after ureteroscopic biopsy
Management afterureteroscopic biopsy
No. ureteroscopic biopsy resultsG1
(
n
= 4)G2
(
n
= 18) G3
(
n
= 5)No malignancy
(
n
= 8)Insufficient sample
(
n
= 5)
Nephroureterectomy 1 11 5 4 2Nephron-sparing treatment 3 7 0 3 1Follow-up 0 0 0 1 2
Ureteroscopic biopsy for upper urinary tract TCC 629
disease. There was no significant difference in thedisease-free and survival rates between the nephrou-reterectomy group (
n
= 10) and the nephron-sparingsurgery group (
n
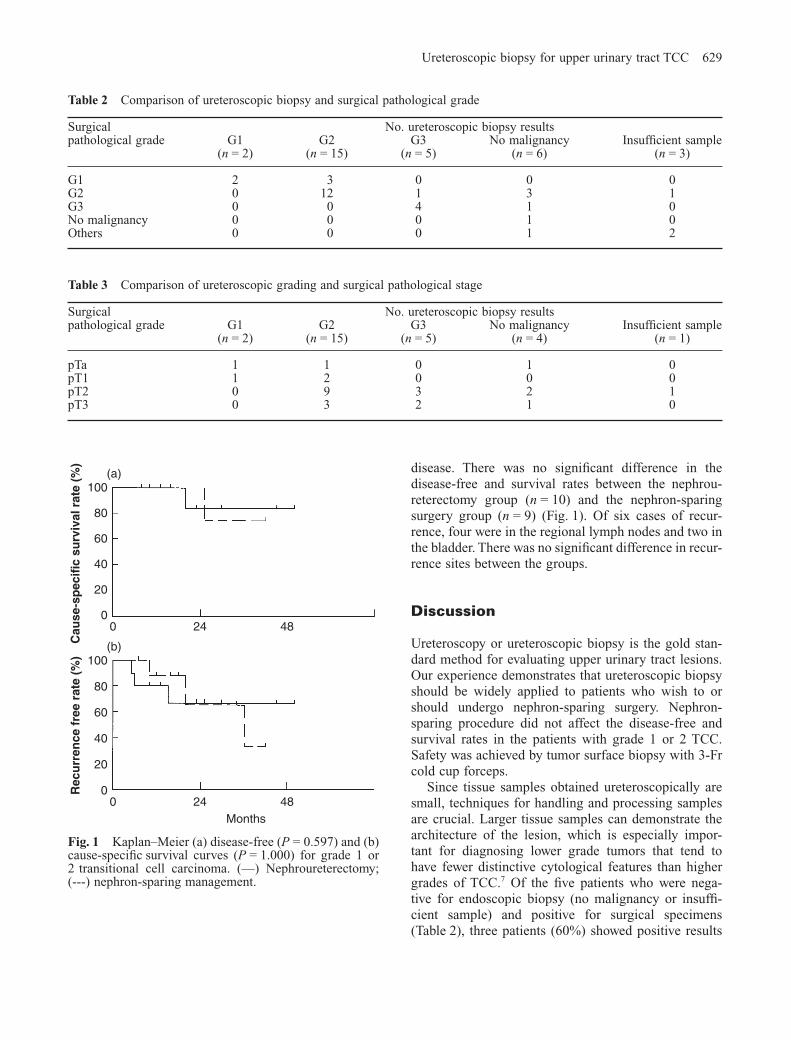
= 9) (Fig. 1). Of six cases of recur-rence, four were in the regional lymph nodes and two inthe bladder. There was no significant difference in recur-rence sites between the groups.
Discussion
Ureteroscopy or ureteroscopic biopsy is the gold stan-dard method for evaluating upper urinary tract lesions.Our experience demonstrates that ureteroscopic biopsyshould be widely applied to patients who wish to orshould undergo nephron-sparing surgery. Nephron-sparing procedure did not affect the disease-free andsurvival rates in the patients with grade 1 or 2 TCC.Safety was achieved by tumor surface biopsy with 3-Frcold cup forceps.
Since tissue samples obtained ureteroscopically aresmall, techniques for handling and processing samplesare crucial. Larger tissue samples can demonstrate thearchitecture of the lesion, which is especially impor-tant for diagnosing lower grade tumors that tend tohave fewer distinctive cytological features than highergrades of TCC.
7
Of the five patients who were nega-tive for endoscopic biopsy (no malignancy or insuffi-cient sample) and positive for surgical specimens(Table 2), three patients (60%) showed positive results
Fig. 1
Kaplan–Meier (a) disease-free (
P
= 0.597) and (b)cause-specific survival curves (
P
= 1.000) for grade 1 or2 transitional cell carcinoma. (––) Nephroureterectomy;(---) nephron-sparing management.
(a)
(b)
0 24 480
20
40
60
80
100
0 24 480
20
40
60
80
100
Cau
se-s
pec
ific
su
rviv
al r
ate
(%)
Rec
urr
ence
fre
e ra
te (
%)
Months
Table 3
Comparison of ureteroscopic grading and surgical pathological stage
Surgical pathological grade
No. ureteroscopic biopsy results G1
(
n
= 2)G2
(
n
= 15)G3
(
n
= 5)No malignancy
(
n
= 4)Insufficient sample
(
n
= 1)
pTa 1 1 0 1 0pT1 1 2 0 0 0pT2 0 9 3 2 1pT3 0 3 2 1 0
Table 2
Comparison of ureteroscopic biopsy and surgical pathological grade
Surgical pathological grade
No. ureteroscopic biopsy results G1
(
n
= 2)G2
(
n
= 15)G3
(
n
= 5)No malignancy
(
n
= 6)Insufficient sample
(
n
= 3)
G1 2 3 0 0 0G2 0 12 1 3 1G3 0 0 4 1 0No malignancy 0 0 0 1 0Others 0 0 0 1 2

630 K Shiraishi
et al.
for voided urine cytology. All patients with grade 3TCC from a surgical specimen (Table 2) showed posi-tive results for voided urine cytology (100%). To avoidtaking an insufficient sample size, operators mustobtain multiple or deeper samples according to uret-eroscopic inspection. Complications associated withureteroscopy have decreased with improved instru-ments and refined technique.
8
Together with urinecytology and ureteroscopic inspection, we recommendnephron-sparing management for patients with false-negative results.
Tumor stage appears to be the most importantprognostic factor. Several reports have stated thatincreased pathological grade is associated withincreased tumor stage and multifocality.
9–11
Keeley
et al
. observed an association between ureteroscopicbiopsy grade and surgical pathological stage, espe-cially in low-grade tumors.
5
Our results provide nodirect information regarding stage (Table 3). A 29–81% recurrence rate was noted after conservativeendourological management against low-grade upperurinary tract TCC.
5,12
In support of these data, 85%of grade 2 or 3 tumor revealed muscle invasive fromopen surgical specimens (Table 3). When nephron-sparing management is contemplated, the risk ofunderestimating the stage and grade of the tumormust be considered.
13,14
Appropriate adjuvant chemo-therapy can be conducted from the results of surgicalpathological stage by partial ureterectomy or trans-ureteral resection.
One of the major issues in the application of uret-eroscopic biopsy is the potential risk of tumor celldissemination outside the urinary tract.
15,16
However,there is a discrepant report regarding this issue.
17
Although, the present study provides no direct evi-dence regarding this issue, there was no apparent dis-ease progression in any of the patients afterureteroscopic biopsy.
Over the last few decades, evidence has arisenthat in some patients similar results can beachieved with nephron-sparing management and thatnephroureterectomy may be excessive. Heney
et al
.advocated that nephroureterectomy for low-gradeupper urinary tract tumors is unnecessary.
18
Becauseof the possible involvement of invasive disease(Table 3), residual cancer cells must be consideredand patients should be monitored closely afternephron-sparing management. Based on the resultsof our study, we recommend ureteroscopic biopsyto patients who wish to or should undergo nephron-sparing management. Patients with low-grade TCCcan be offered the option of nephron-sparingmanagement.
References
1 Blute M, Segura J, Patterson D, Benson RC, Zincke H.Impact of endourology on diagnosis and management ofupper urinary tract urothelial cancer.
J. Urol.
1989;
141
:1298–301.
2 Elliott DS, Segura JW, Lightner D, Patterson D, BluteML. Is nephroureterectomy necessary in all cases ofupper tract transitional cell carcinoma? Long-termresults of conservative endourologic management ofupper tract transitional cell carcinoma in individuals witha normal contralateral kidney.
Urology
2001;
58
: 174–8.3 Borkowski A, Malouf D. The endourological manage-
ment of upper urinary tract tumors.
BJU Int.
1999;
83
:369–77.
4 Bagley DH, Rivas D. Upper urinary tract filling defects:flexible ureteroscopic diagnosis.
J. Urol.
1990;
143
:1196–2000.
5 Keeley FX, Kulp DA, Bibbo M, McCue PA, Bagley DH.Diagnostic accuracy of ureteroscopic biopsy in uppertract transitional cell carcinoma.
J. Urol.
1997;
157
: 33–7.6 Hara I, Hara S, Miyake H
et al.
Usefulness of uretero-pyeloscopy for diagnosis of upper urinary tract tumors.
J. Endourol.
2001;
15
: 601–5.7 Kannan V. Papillary transitional-cell carcinoma of the
upper urinary tract: a cytologic review.
Diagn. Cytopath.
1990;
6
: 204–9.8 Harmon WJ, Serson PD, Blute ML, Patterson DE, Seg-
ura JW. Ureteroscopy: current practice and long-termcomplications.
J. Urol.
1997;
157
: 28–32.9 Charbit L, Gendreau MC, Mee S, Cukier J. Tumors of
the upper urinary tract: 10 years of experience.
J. Urol.
1991;
146
: 1243–6.10 Murphy DM, Zincke H, Furlow WL. Primary grade 1
transitional cell carcinoma of the renal pelvis and ureter.
J. Urol.
1980;
123
: 629–31.11 Murphy DM, Zincke H, Furlow WL. Management of
high grade transitional cell carcinoma of the upper uri-nary tract.
J. Urol.
1981;
125
: 25–9.12 Chen G, Bagley D. Ureteroscopic management of upper
urinary tract transitional cell carcinoma in patients withnormal contralateral kidney.
J. Urol.
1999;
161
(Suppl.4): 76.
13 Kaufman RP, Carson CC. 3D ureteroscopic manage-ment of transitional cell carcinoma of the ureter usingthe neodymium: YAG laser.
Lasers Surg. Med.
1993;
13
:625–8.
14 Andersen JR, Kristensen JK. Ureteroscopic manage-ment of transitional cell tumors.
Scand. J. Urol. Neph-rol.
1994;
28
: 153–7.15 Lim DJ, Shattuck MC, Cook WA. Pyelovenous lym-
phatic migration of transitional cell carcinoma followingflexible ureterorenoscope.
J. Urol.
1993;
149
: 109–11.16 Kulp DA, Bagley DH. Does flexible ureteropyeloscopy
promote local recurrence of transitional cell carcinoma?
J. Endourol.
1994;
8
: 111–5.17 Hendin BN, Streem SB, Levine HS, Klein EV, Novick
AC. Impact of diagnostic ureteroscopy on long-termsurvival in patients with upper tract transitional cell car-cinoma.
J. Urol.
1999;
161
: 783–5.18 Heney NM, Nocks BN, Daly JJ, Blitzer PH, Parkhurst
EC. Prognostic factors in carcinoma of the ureter.
J.Urol.
1981;
125
: 632–6.