rupture tendo achillis
TRANSCRIPT

Achilles Tendon Rupture
BY:
AHMED NABEEL EMARA
• often misdiagnosed as an ankle sprain
• may be missed in up to 25%
• Epidemiology
incidence
18:100,000 per year
demographics
more common in men
most common in ages 30-40

Risk factors
episodic athletes, "weekend warrior"
flouroquinolone antibiotics
steroid injections
Mechanism
usually traumatic injury during a sporting event
may occur with
sudden forced plantar flexion
violent dorsiflexion in a plantar flexed foot
Pathoanatomy
rupture usually occurs 4-6 cm above the calcaneal insertion in hypovascular
region
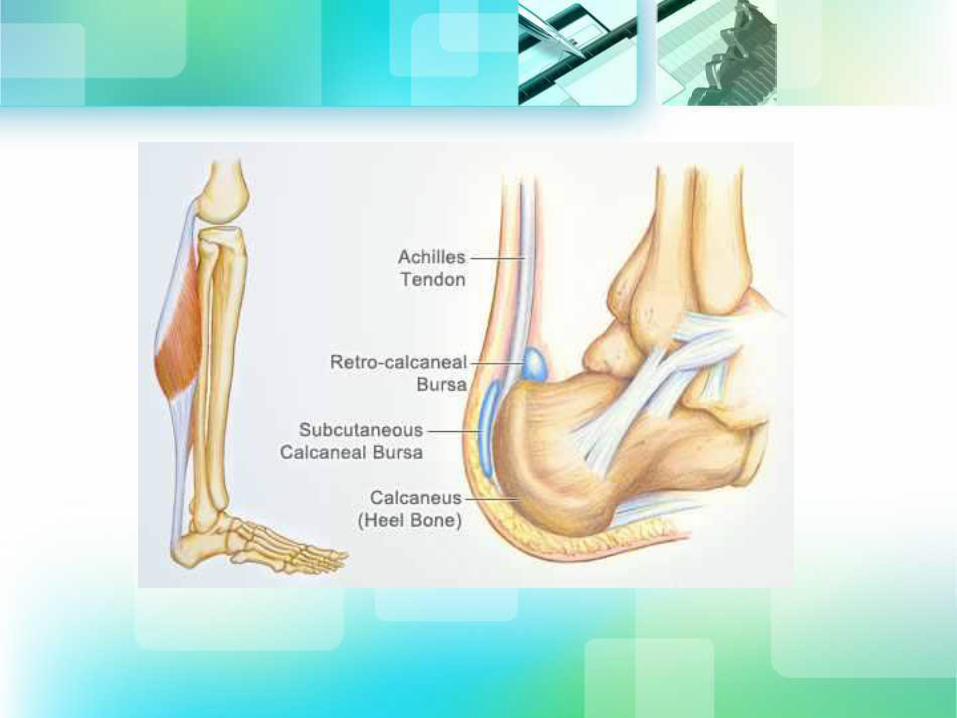
• Anatomy
largest tendon in body
formed by the confluence of
soleus muscle tendon
medial and lateral gastrocnemius
tendons
• blood supply from posterior tibial artery
Presentation
• History
patients usually reports a "pop"
• Symptoms
weakness and difficulty walking
pain in heel
• Physical exam
• inspection
increased resting ankle dorsiflexion in
prone position with knees bent
calf atrophy may be apparent in chronic
cases
• palpation
palpable gap
• motion
weakness to ankle plantar flexion
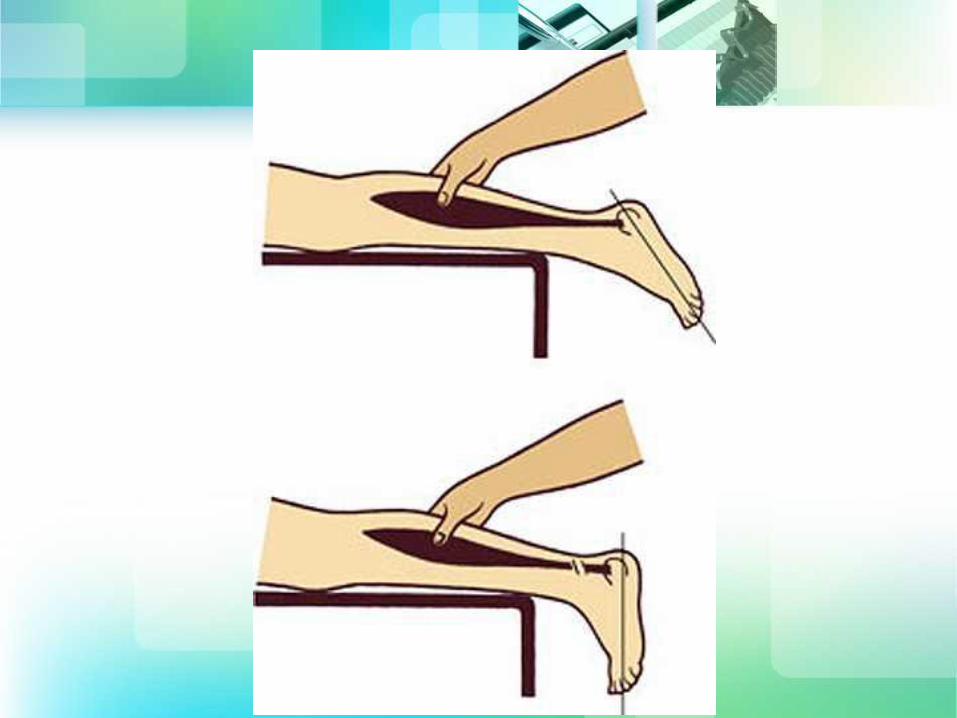
• provocative test
Thompson test
lack of plantar flexion when calf is
squeezed

Imaging
• Radiographs
used to rule-out other
pathology

• Ultrasound
may be useful to determine complete vs.
partial ruptures
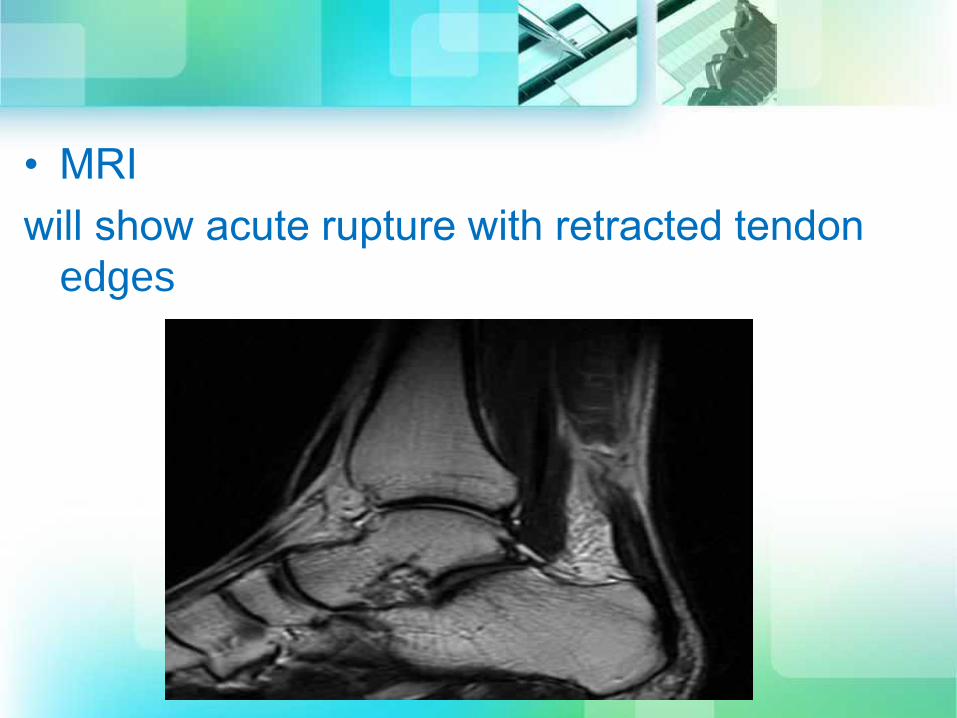
• MRI
will show acute rupture with retracted tendon
edges
Treatment
• Nonoperative
functional bracing/casting in resting equinus
sedentary patient
elderly patients
medically frail patients
technique
cast/brace in 20 degrees of plantar flexion
early functional rehab for those treated
without a cast

• Operative
• end-to-end achilles tendon repair
• percutaneous achilles tendon repair
• reconstruction with VY advancement
• flexor hallucis longus transfer +/- VY
advancement of gastrocnemius
• End-to-end achilles tendon repair
approach
make incision just medial to achilles
tendon to avoid sural nerve
technique
incise paratenon
expose tendon edges
repair with heavy non-absorbable
suture
postoperative care
immobilize in 20° of plantar flexion to
decrease tension on skin and protect
tendon repair for 4-6 weeks

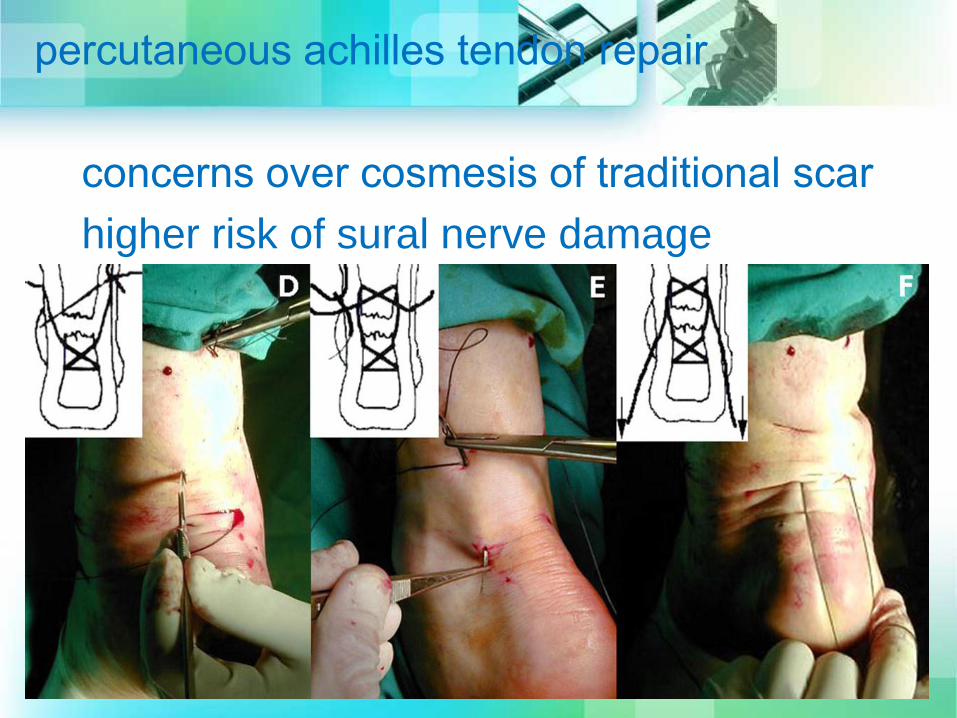
percutaneous achilles tendon repair
concerns over cosmesis of traditional scar
higher risk of sural nerve damage
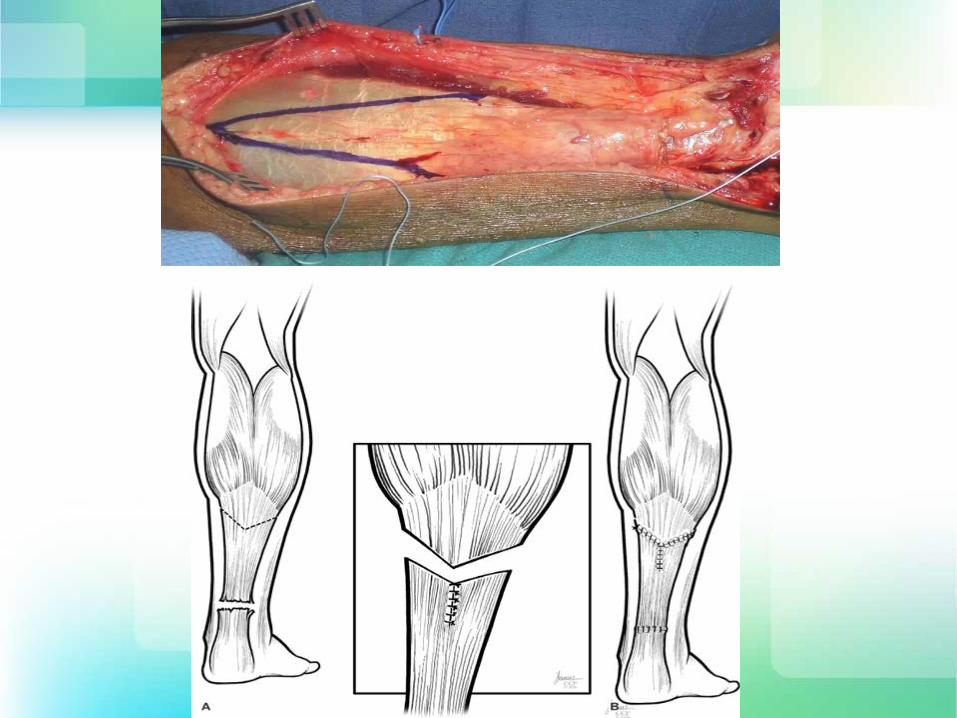
• reconstruction with VY advancement
chronic ruptures with defect < 4cm
– technique
make V cut with apex at
musculotendinous junction with limbs
divergent to exit the tendon undefined
V is incised through only the superficial
tendinous portion leaving the muscle fibers
intact
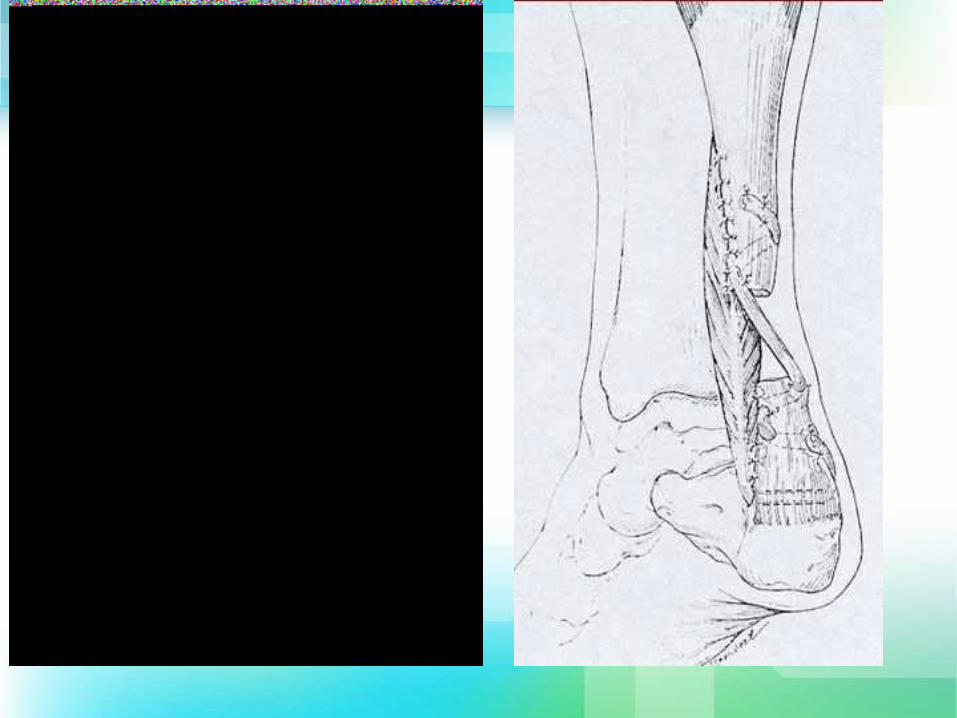
• flexor hallucis longus transfer +/- VY
advancement of gastrocnemius
chronic ruptures with defect > 4cm
technique
excise degenerative tendon edges
release FHL tendon at the Knot of
Henry and transfer through the calcaneus
Complications
• Re-ruptur
generally considered to be higher with
non-operative management (~10-40%
vs 2%
Wound healing complications 5-10%
• Sural nerve injury
higher incidence when percutaneous
approach is used
postoperative care
• Traditionally, postoperative rehabilitation
involved wearing a splint with the ankle in
equinus during the immediate
postoperative period. A cast is then placed
within a few days and continued for 6
weeks. The patient is seen in the clinic at
2-week intervals during which the cast is
changed and placed in an increasingly
more dorsiflexed position. After 4 to 6
weeks in the cast, it is advanced to a
plantigrade position. With the cast in
place, the patient is instructed to begin
isometric gastrocnemius-soleus complex
exercises once weight bearing is tolerated.
• A recent trend toward a more functional
rehabilitation program is gaining
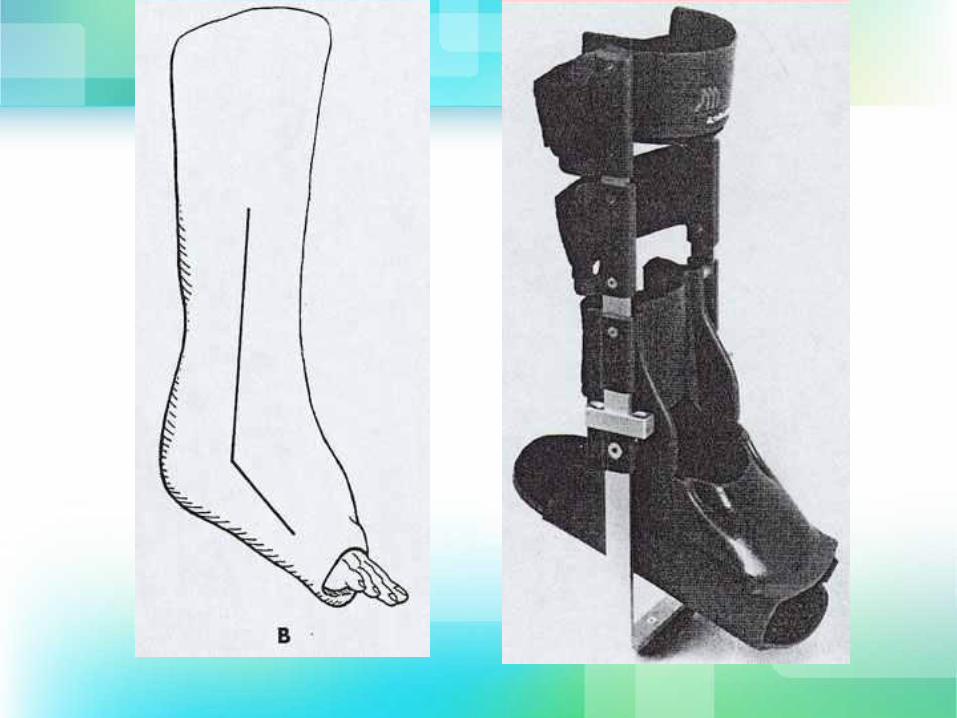
popularity. These protocols use an anterior
plaster slab or an orthosis/walking boot
for 6 weeks allowing full range of motion
with the exception of dorsiflexion beyond
neutral.
• The long period of immobilization
increases the likelihood of muscle atrophy,
joint stiffness, cartilage atrophy,
degenerative arthritis, adhesions, and
deep venous thrombosis. In contrast, early
mobilization limits atrophy, promotes fiber
polymerization to collagen, and increases
the organization of collagen at the repair
site, which ultimately increases muscle
and tendon strength
Rehabilitation Program
Following cast removal, gentle passive
range of motion of the ankle and subtalar
joints is initiated.
After 2 weeks, progressive resistance
exercises (PREs) are added to the
regimen.
This is followed by aggressive gait training
exercises at about 10 weeks following the
injury (nonoperative patients) or surgery
(operative patients), leading toward
activity-specific maneuvers and a return to
activities at 4-6 months