section 2 insulin therapy in type 1 and type 2 diabetes 37
TRANSCRIPT
Section 2
Insulin Therapy in Type 1and Type 2 Diabetes
37

Initiating Insulin Therapy• Add single dose of basal insulin– Glargine, detemir, or NPH– Usually administered at bedtime
• Use conservative starting dose– 10 units (empiric)– 0.1 to 0.2 units/kg– 0.3 to 0.4 units/kg if severe hyperglycemia
41
Initiating Insulin Therapy• Adjust dose according to fasting SMBG– Typical titration 1–2 units every few days– Treat to target range for fasting glucose• ADA: 70–130 mg/dL• AACE: <110 mg/dL
– May use product-specific titration instructions• Continue oral agent(s) at same dosage
(eventually reduce)
42American Diabetes Association Standards of Medical Care in Diabetes—2012AACE Medical Guidelines for Clinical Practice for Developing a Diabetes Mellitus Comprehensive Care Plan (2011)

Intensifying Insulin Therapy• A1C ≥7% after 2–3 months with fasting blood
glucose in target range• Perform SMBG before meals, bedtime• Add prandial (bolus) insulin based on time of
out-of-range result– Before lunch: add breakfast dose– Before dinner: add lunch dose– Before bedtime: add dinner dose
43
Intensifying Insulin Therapy• Insulin options– Insulin aspart– Insulin glulisine– Insulin lispro– Regular insulin– NPH insulin
• Dosing considerations– Typical initial dose: 4–5 units– Typical titration: 2–3 units every 2–3 days
44
Intensifying Insulin Therapy• Continue other agents?– Metformin– Thiazolidinediones (glitazones)– Sulfonylureas, glinides– α-Glucosidase inhibitors– DPP-4 inhibitors– GLP-1 receptor agonists– Colsevelam– Bromocriptine
45
• 62-year-old Caucasian woman with type 2 diabetes
• Weight: 219 lb• Medications– Insulin glargine (Lantus®)
42 units at bedtime– Metformin (Glucophage®
XR) 1,000 mg twice daily– Pioglitazone (Actos®) 45 mg
once daily46
Insulin Mini-Case 1
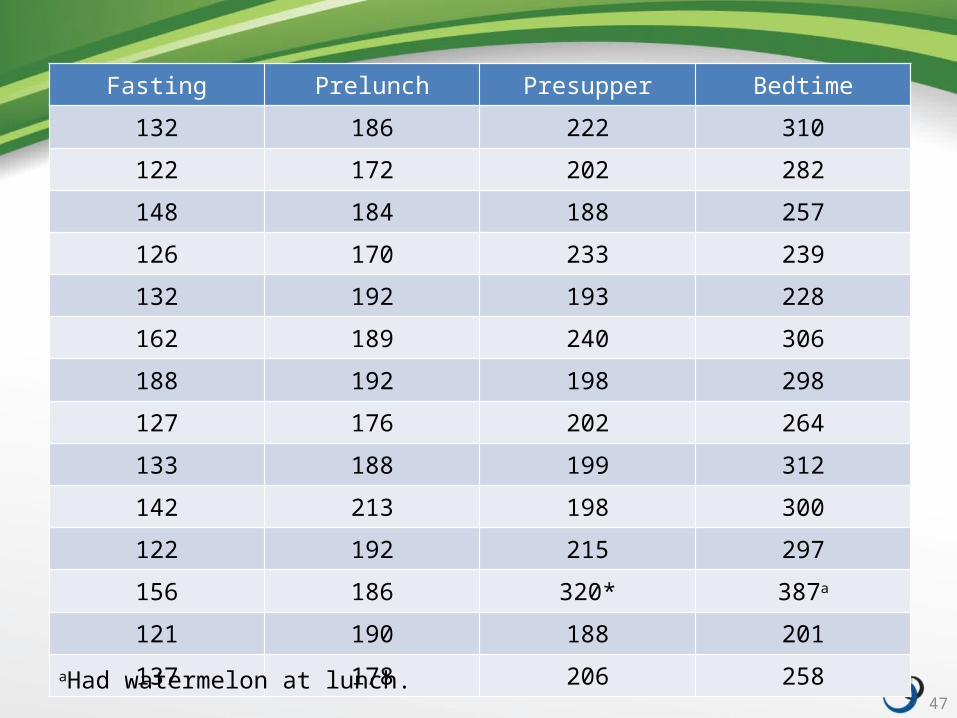
Fasting Prelunch Presupper Bedtime
132 186 222 310
122 172 202 282
148 184 188 257
126 170 233 239
132 192 193 228
162 189 240 306
188 192 198 298
127 176 202 264
133 188 199 312
142 213 198 300
122 192 215 297
156 186 320* 387a
121 190 188 201
137 178 206 258
47
aHad watermelon at lunch.
• How should insulin therapy be adjusted?
• Continue current medications?
48
Insulin Mini-Case 1
Pattern Management• Review SMBG data for general patterns• Identify trends– Three or more similar glucose values at the same
time each day• Discuss with patient possible causes of values
outside target– Food from previous meal?– Activity?– Insulin dose?
74

Pattern Management• Should changes in food/carbohydrate amount
or timing of intake be made?• Should physical activity be more regular,
increased, decreased?• Should the insulin regimen be adjusted?
75
• 54-year-old African American woman with type 2 diabetes
• A1C: 9.2%• Medications
– Humalog® Mix75/25TM (insulin lispro)• 16 units each morning• 10 units each evening
– Metformin (Glucophage® XR) 1,000 mg twice daily
49
Insulin Mini-Case 2
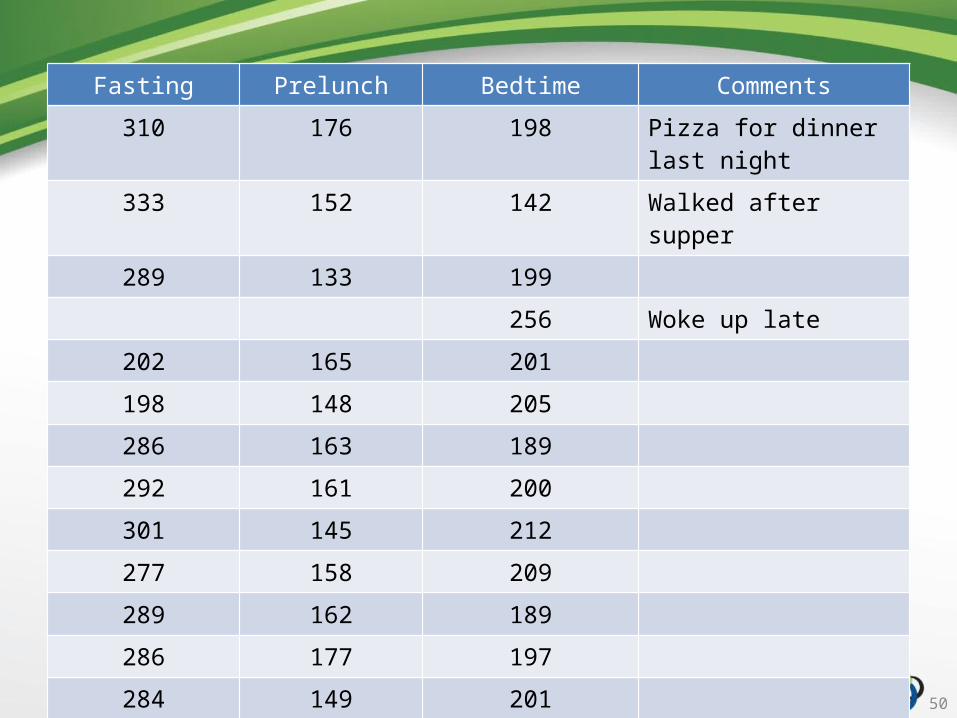
Fasting Prelunch Bedtime Comments
310 176 198 Pizza for dinner last night
333 152 142 Walked after supper
289 133 199
256 Woke up late
202 165 201
198 148 205
286 163 189
292 161 200
301 145 212
277 158 209
289 162 189
286 177 197
284 149 201
303 159 182
50

• How should insulin therapy be adjusted?
51
Insulin Mini-Case 2
Multiple InjectionInsulin Regimens
52
53
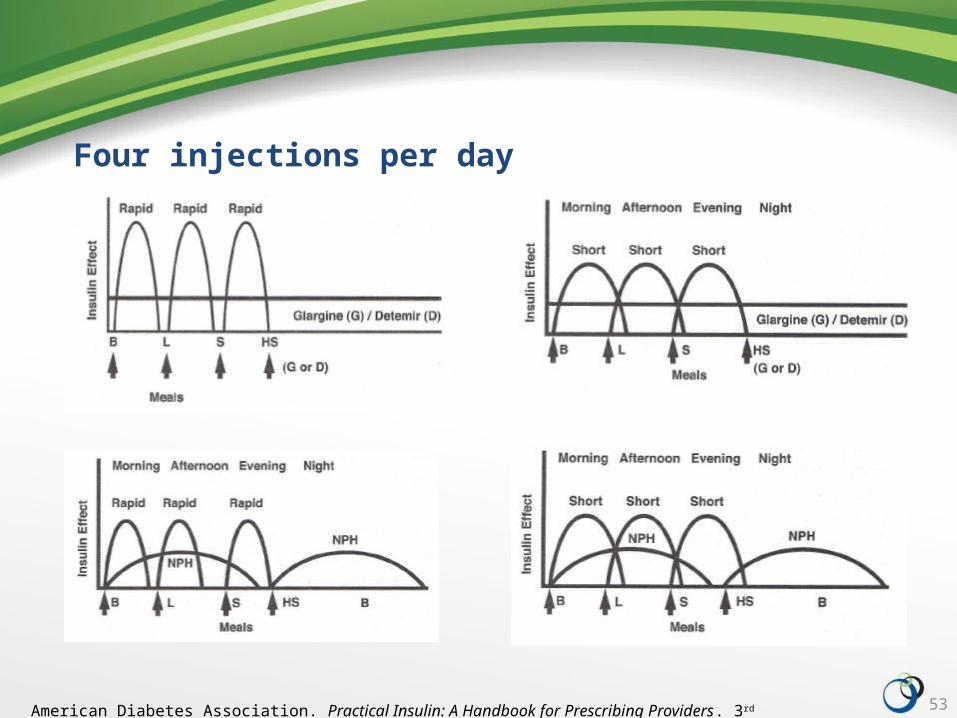
Four injections per day
American Diabetes Association. Practical Insulin: A Handbook for Prescribing Providers. 3rd ed. 2011.

Initiating Insulin in Type 1 Diabetes• Typical starting dose: 0.5–0.7 units/kg/day• Basal insulin: ½ to ⅔ of total daily dose• Bolus insulin: ½ to ⅓ of total daily dose,
divided among meals• Titrate doses as needed
56
• 19-year-old Caucasian man newly diagnosed with type 1 diabetes
• Weight: 137 lb• A1C: 11.6%• Blood glucose: 256 mg/dL• Spilling ketones
57
Insulin Mini-Case 3a
• Determine total daily dose– 0.6 units/kg/day
• Determine individual doses– 50% basal/50% bolus
58
Insulin Mini-Case 3a

Adjusting Insulin DosesOut-of-Range Result Insulin Component to Adjust
Postbreakfast/prelunch Prebreakfast rapid-acting/short-acting insulin
Postlunch/presupper Prelunch rapid-acting/short-acting insulinMorning NPH
Midafternoon Long-acting insulinMorning NPH
Postsupper/bedtime Presupper rapid-acting/short-acting insulin
Early morning Long-acting insulinEvening NPH
59American Diabetes Association. Practical Insulin: A Handbook for Prescribing Providers. 3rd ed. 2011.
Refining Insulin Doses• Correction insulin– Correction factor (insulin sensitivity factor)– Correction dose
• Insulin-to-carbohydrate ratio– Insulin to cover ingested carbohydrate
• Pattern management– Insulin doses determined or adjusted by trends in
SMBG data
60
Correction Factor• Amount of rapid-acting or short-acting insulin
needed to return an elevated blood glucose level to target level– Quantifies degree of change in blood glucose
value expected with injection of 1 unit insulin
61
Correction Factor • For the average patient, 1 unit of insulin will
lower blood glucose by 50 mg/dL– For insulin-sensitive individuals, 1 unit may lower
blood glucose by as much as 100 mg/dL– For insulin-resistant individuals, 1 unit may lower
blood glucose by as little as 25 mg/dL
62
Correction Factor• 1800 rule– 1800 ÷ total daily dose of insulin (TDD)– Example• 1800 ÷ 50 units = 36• 1 unit of rapid-acting or short-acting insulin will lower
blood glucose by 36 mg/dL
• Also 2000, 1700, 1500 rules– Higher rule value = lower risk of hypoglycemia
63
Correction Dose• Current blood glucose − target blood glucose =
amount of glucose over target• Amount of glucose over target ÷ correction
factor = correction dose
[Blood glucose now] − [Goal blood glucose]
Correction factor
64

• 19-year-old Caucasian man with type 1 diabetes
• Experiencing unexpected elevations in blood glucose due to school-related stress
65
Insulin Mini-Case 3b
• Recall TDD– 37 units/kg/day
• Determine correction factor– Use rule of 1800
• Calculate correction dose– Current blood glucose:
320 mg/dL– Blood glucose goal: 120 mg/dL
66
Insulin Mini-Case 3b
Insulin-to-Carbohydrate Ratio• Amount of rapid-acting or short-acting insulin
needed to “cover” carbohydrates in meals and snacks
• Patient may have different insulin-to-carbohydrate ratios for different meals
67
Insulin-to-Carbohydrate Ratio• How to calculate– Determine average carbohydrate grams for each
meal and snack– Divide carbohydrate grams by units of insulin
administered (with appropriate glucose control)
68
Insulin-to-Carbohydrate Ratio• Information needed– Detailed, accurate food records for at least 3 days• To determine total carbohydrate grams eaten at meals
and snacks
– Units of rapid-acting or short-acting insulin administered with each meal and snack
– Premeal and postmeal blood glucose levels
69
Insulin-to-Carbohydrate Ratio• Sample calculation– Average carbohydrate grams at dinner: 55 g– Administered 9 units rapid-acting insulin with
appropriate return of glucose to baseline– 55 g ÷ 9 units = 1 unit of insulin per 6 g
carbohydrates– Insulin-to-carbohydrate ratio 1:6
70

Insulin-to-Carbohydrate Ratio• Rule of 500– Alternate method of calculating insulin-to-
carbohydrate ratio– 500 ÷ TDD
71
• 24-year-old Hispanic woman with type 1 diabetes
• Weight: 118 lb• Uses insulin glargine
(Lantus®) 22 units once daily
• Guesses at prandial doses
72
Insulin Mini-Case 4

• Calculate the insulin-to-carbohydrate ratio– Use rule of 500– Use 0.6 units/kg/day for insulin dose
73
Insulin Mini-Case 4
76
Patient Case Claire Green
• What do Claire’s SMBG results tell you?
• What changes (if any) should Claire make?
77
Claire Green
• How should Claire adjust her insulin regimen for her night out with the girls?
78
Claire Green
Hypoglycemia
79
Hypoglycemia• Risk factors– Missed or irregular meals– Physical activity– Alcohol consumption
• Symptoms
80

81
Hypoglycemia ManagementCHECK
TREAT
CHECK
EAT
82
Insulin Therapy Updates
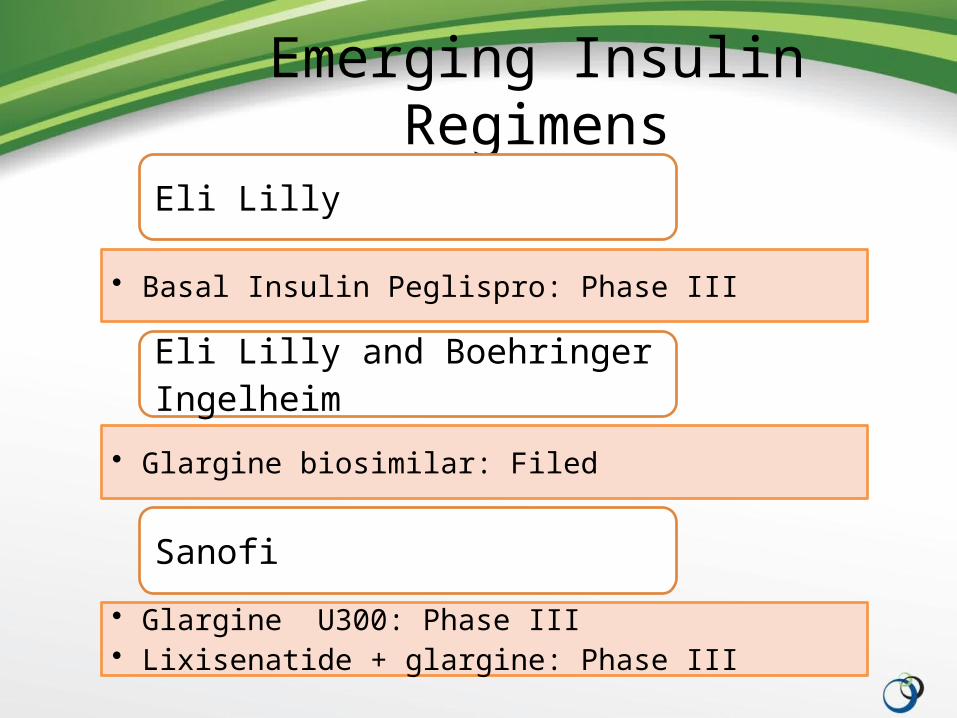
Emerging Insulin Regimens
Eli Lilly
• Basal Insulin Peglispro: Phase III
Eli Lilly and Boehringer Ingelheim
• Glargine biosimilar: Filed
Sanofi
• Glargine U300: Phase III• Lixisenatide + glargine: Phase III

Emerging Insulin Regimens
Novo Nordisk
• Degludec + aspart (Ryzodeg): Filed• Degludec (Tresiba): Filed• Degludec + liraglutide (IDegLira): Phase III; Filed in Europe• Faster insulin aspart (FIAsp): Phase III
Insulin’s about to get really exciting!
Questions?
84

LUNCH
85