sedative and hypnotic - lecture-notes.tiu.edu.iq
TRANSCRIPT

Sedative and HypnoticAsmaa A.

Sedative is a drug that reduces excitement and calms the person.Hypnotic is a drug that produces sleep resembling normal sleep.
Sleep: The phases of sleep include
Non-rapid eye movement (NREM) sleep
Rapid eye movement (REM) sleep.

-NREM sleep is divided into stage 0, 1, 2, 3, and 4.
Normally, about 50% of sleep time is spent in stage 2. Slow-wave sleepincludes stage 3 and 4.
-REM your mind rests and collates data and lightest, sleep, most likelyto awaken.
REM sleep constitutes about 30% of the sleep time and lasts for 5–30min in each cycle of sleep.

Types of sleep disorder and their treatment

Classification of sedatives and hypnotics
1.Benzodiazepines: Diazepam, oxazepam, lorazepam, flurazepam,nitrazepam, temazepam, clonazepam, clobazam, chlordiazepoxide,triazolam, midazolam, alprazolam.
2.Barbiturates:
Long acting: Phenobarbitone, mephobarbitone.
Short acting: Pentobarbitone, secobarbitone, amobarbital.
Ultra-short acting: Thiopentone, methohexitone.
3.Other hypnotic agents: Zolpidem, zopiclone, zaleplon, eszopiclone,Ramelteon, antihistamines, antidepressants.
4. Other anxiolytic agents: Antidepressants, Buspirone.

1.Benzodiazepines
All benzodiazepines (BZDs) have a benzene ring fused to a seven-membered diazepine ring.
Sites of action
BZDs act at midbrain, limbic system, ascending reticular activating system (ARAS), brain stem, cerebellum, etc.
Mechanism of action
Benzodiazepines facilitate action of gamma-aminobutyric acid (GABA)—they potentiate inhibitory effects of GABA.




Metabolism

Pharmacological actions and therapeutic uses
1. Sedation and hypnosis: Benzodiazepines decrease time required tofall asleep (sleep latency).
The total sleep time is increased. They shorten all stages of NREMsleep except stage 2, which is prolonged. The duration of REM sleep isusually decreased. BZDs reduce night awakenings and producerefreshing sleep.
At present, BZDs are the preferred drugs for treatment of short-terminsomnia because:
• They have a wide therapeutic index.
• They cause near-normal sleep; less rebound phenomena onwithdrawal.

• They produce minimal hangover effects (headache and residualdrowsiness on waking).
• They cause minimal respiratory depression.
• They are less likely to cause tolerance and dependence when used forshort period.
• They have no enzyme-inducing property; hence drug interactions areless.
• They have a specific BZD receptor antagonist, flumazenil, for thetreatment of overdosage.
Long-term use of BZDs for insomnia is not recommended because oftolerance, dependence and hangover effects; but for occasional use by airtravellers, shift workers, etc. these drugs are ideal.

2.Anticonvulsant: Diazepam, lorazepam, clonazepam, clobazam, etc. haveselective anticonvulsant effect. Intravenous (i.v.) diazepam/lorazepam is usedto control life-threatening seizures in status epilepticus, tetanus, drug-induced convulsions, febrile convulsions, etc. Clonazepam is used in thetreatment of absence seizures.
3.Diagnostic (endoscopies) and minor operative procedures: IntravenousBZDs are used because of their sedative–amnesic–analgesic and muscle-relaxant properties.

4.Preanaesthetic medication: These drugs are used as preanaesthetic medicationbecause of their sedative–amnesic and anxiolytic effects. Hence, the patientcannot recall the perioperative events later.
BZDs do not cause true general anaesthesia (GA). Intravenous diazepam,lorazepam, midazolam, etc. are combined with other central nervous system(CNS) depressants to produce GA.
5.Antianxiety (anxiolytic) effect: Some of the BZDs (diazepam, oxazepam,alprazolam, lorazepam, chlordiazepoxide, etc.) have selective antianxiety actionat low doses. The anxiolytic effect is due to their action on limbic system.

6.Muscle relaxant (centrally acting): They reduce skeletal muscle tone byinhibiting polysynaptic reflexes in the spinal cord. The relaxant effect ofBZDs is useful in spinal injuries, tetanus, cerebral palsy and to reduce spasmdue to joint injury or sprain.
7. To treat alcohol-withdrawal symptoms.
8.Conscious sedation: A type of sedation that induces an altered state ofconsciousness that minimizes pain and discomfort through the use of painrelievers and sedatives.


Pharmacokinetics
Benzodiazepines are usually given orally or intravenously andoccasionally by rectal route (diazepam) in children. The rate of absorptionfollowing oral administration is variable; absorption is erratic fromintramuscular (i.m.) site of administration; hence rarely used.
They have a large Vd. They have a short duration of action on occasionaluse because of rapid redistribution, hence are free of residual (hangover)effects, even though elimination half-life is long.
Benzodiazepines are metabolized in liver. Some of them produce activemetabolites that have long half-life; hence cumulative effects may beseen. The metabolites are excreted in urine. BZDs can cross placentalbarrier.

Adverse effects
Benzodiazepines have a wide margin of safety. They are generally welltolerated. The common side effects are drowsiness, confusion, blurredvision, amnesia, disorientation, tolerance and drug dependence.
Withdrawal after chronic use causes symptoms like tremor, insomnia,restlessness, nervousness and loss of appetite.
Use of BZDs during labour may cause respiratory depression and hypotoniain the newborn (Floppy baby syndrome).
In some patients, these drugs may produce paradoxical effects, i.e.convulsions and anxiety.

Inverse Agonists (β-Carboline)
Their interaction with BZD receptors will produce anxiety and convulsions.
Benzodiazepine Antagonist ( Flumazenil)
Flumazenil competitively reverses the effects of both BZD agonists (CNSdepression) and BZD-inverse agonists (CNS stimulation). Flumazenil is notused orally because of its high first-pass metabolism.
It is given by i.v. route and has a rapid onset of action. Flumazenil is used inthe treatment of BZD overdosage and to reverse the sedative effects of BZDsduring general anaesthesia.
Adverse effects include confusion, dizziness and nausea. It may precipitatewithdrawal symptoms (anxiety and convulsions) in dependent subjects.

Competitive antagonism. BZDR, benzodiazepine receptor
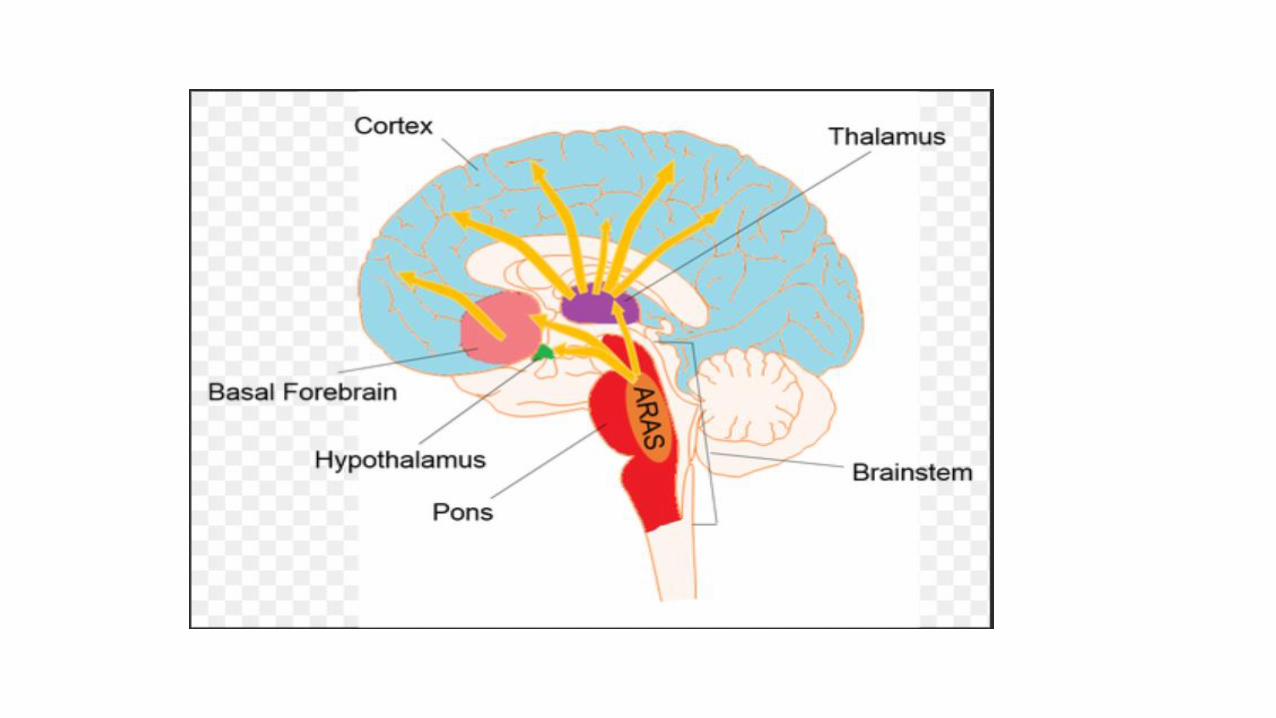
2.Barbaturate
All barbiturates are derivatives of barbituric acid. They are nonselective CNS depressants and act at many sites, ascending reticular activating system (ARAS) being the main site.
Mechanism of action
Barbiturates have GABA-facilitatory action—they potentiate inhibitory effects of GABA.



Pharmacological actions and uses
1.Sedation and hypnosis: Barbiturates were used in the treatment ofinsomnia.
They decrease (sleep latency, duration of REM sleep, stage 3 and 4 ofNREM sleep). They cause marked alteration of sleep architecture. Atpresent, barbiturates are not recommended because:
• They have a low therapeutic index.
• They cause rebound increase in REM sleep on stoppage of therapy.

• They cause marked respiratory depression.
• They produce marked hangover effects (headache and drowsiness onwaking).
• They cause high degree of tolerance and drug dependence.
• They are potent enzyme inducers and cause many drug interactions.
• They have no specific antidote.

2.General anaesthesia (GA): Ultra-short-acting barbiturates (thiopentoneand methohexitone) are used for the induction of GA.
3.Anticonvulsant: Phenobarbitone has anticonvulsant effect and is used inthe treatment of status epilepticus and generalized tonic–clonic seizures(GTCS).

Adverse effects
1.The common side effects are drowsiness, confusion, headache, ataxia,hypotension and respiratory depression.
2.Hypersensitivity reactions like skin rashes, itching and swelling of facemay occur.
3.Tolerance develops to their sedative and hypnotic actions on repeated use.
4. Physical and psychological dependence develops on repeated use.
5.Prolonged use of phenobarbitone may cause megaloblastic anaemia byinterfering with absorption of folic acid from the gut.

6.They may precipitate attacks of acute intermittent porphyria; hencebarbiturates are contraindicated in porphyria.
7.In case of acute barbiturate poisoning, the signs and symptoms aredrowsiness, restlessness, hallucinations, hypotension, respiratorydepression, convulsions, coma and death.
Drug interactions
Barbiturates are potent inducers of hepatic microsomal enzymes andreduce the effectiveness of coadministered drugs (e.g. oralcontraceptives, oral anticoagulants, oral hypoglycaemics, etc.).


3.Non-Benzodiazepine hypnotics
A. Zolpidem: Zolpidem mainly produces hypnotic effect—decreases sleeplatency and increases duration of sleep time in insomnia. It produces near-normal sleep like BZDs with minimal alteration in REM sleep; causesminimal hangover effects and rebound insomnia; less likely to producetolerance and drug dependence; lacks anticonvulsant, antianxiety andmuscle-relaxant effects.
It is given orally, well absorbed, metabolized in liver and excreted in urine.It has a short duration of action and is used for short-term insomnia. Theactions of zolpidem are antagonized by flumazenil.
The common side effects are headache, confusion, nausea and vomiting.

B.Zopiclone: Zopiclone is orally effective and is used for short-termtreatment of insomnia. It produces near-normal sleep like BZDs. Theside effects are headache, drowsiness, GI disturbances and metallictaste.
C.Zaleplon: It is useful in sleep-onset insomnia. It is the shortest-actingnon-BZD hypnotic.
D.Eszopiclone: It is used orally for long-term treatment of insomnia.

E.Ramelteon
Ramelteon is a selective agonist at the MT1 and MT2 subtypes of melatoninreceptors.
Melatonin is a hormone secreted by the pineal gland that helps to maintain thecircadian rhythm underlying the normal sleep–wake cycle.
Stimulation of MT1 and MT2 receptors by ramelteon is thought to induce andpromote sleep.
Ramelteon is indicated for the treatment of insomnia characterized by difficultyfalling asleep (increased sleep latency).

It has minimal potential for abuse, and no evidence of dependence orwithdrawal effects has been observed. Therefore, ramelteon can beadministered long term.
Common adverse effects of ramelteon include dizziness, fatigue, and
somnolence.
Ramelteon may also increase prolactin levels.


F. Antihistamines
Some antihistamines with sedating properties, such as diphenhydramine,hydroxyzine, and doxylamine, are effective in treating mild types ofsituational insomnia. However, they have undesirable side effects (suchas anticholinergic effects) that make them less useful than thebenzodiazepines and the nonbenzodiazepines. Some sedativeantihistamines are marketed in numerous over-the-counter products.

F. Antidepressants
The use of sedating antidepressants with strong antihistamine profileshas been ongoing for decades.
Doxepin, an older tricyclic agent with SNRI mechanisms ofantidepressant and anxiolytic action, was recently approved at low dosesfor the management of insomnia.
Other antidepressants, such as trazodone, mirtazapine, and other oldertricyclic antidepressants with strong antihistamine properties are usedoff-label for the treatment of insomnia.





4.Other anxiolytic agents
A. Antidepressants
Many antidepressants are effective in the treatment of chronic anxietydisorders and should be considered as first-line agents, especially in patientswith concerns for addiction or dependence.
Selective serotonin reuptake inhibitors (SSRIs, such as escitalopram orparoxetine) or serotonin/norepinephrine reuptake inhibitors (SNRIs), such asvenlafaxine or duloxetine) may be used alone or prescribed in combinationwith a low dose of a benzodiazepine during the first weeks of treatment.
SSRIs and SNRIs have a lower potential for physical dependence than thebenzodiazepines and have become first-line treatment for GAD.

B. Buspirone
Buspirone is useful for the chronic treatment of GAD and has an efficacycomparable to that of the benzodiazepines. It has a slow onset of action andis not effective for short-term or “as-needed” treatment of acute anxietystates.
The actions of buspirone appear to be mediated by serotonin (5-HT1A)receptors, although it also displays some affinity for D2 dopamine receptorsand 5-HT2A serotonin receptors.
In addition, buspirone lacks the anticonvulsant and muscle-relaxantproperties of the benzodiazepines.
The frequency of adverse effects is low, with the most common effectsbeing headaches, dizziness, nervousness, nausea, and light-headedness.
Sedation and psychomotor and cognitive dysfunction are minimal, anddependence is unlikely.
Buspirone does not potentiate the CNS depression of alcohol.
