separation of alkaline phosphatase enzymes in human serum using gel-filtration (sephadex g-200)...
TRANSCRIPT

SEPARATION OF ALKALINE PHOSPHATASE ENZYMES I N HUMAN SERUM USING GEL-FILTRATION
(SEPHADEX G-200) TECHNIQUES
KEVIN MCGEENEY, MSc JOSEPH DUNNE, BSc, JAMES J. FENNELLY, MD, MRCPIX, AND
With the a id of gel filtration techniques (Sephadex G-200) the alkaline phos- phatase (Bessey-Lowry-Brock) distribution patterns have been studied in the serum of control human subjects and of those with conditions known to affect total enzyme levels. Protein was scanned a t 254 and 280 m p a n d the 19S, 7S, and 4s peaks thus obtained were used as points of reference. T h e characteristic control serum revealed one sharp peak of enzyme activity in the 7s protein region. A similar bu t sharper peak was found in osteomalacia and Pagets’ disease. In contrast, in malignant bone conditions 10.4%, i n metastatic malig- nant liver disease 31.36% and in nonmalignant liver disease 12.7% of total enzyme moved with the 19s proteins. The patterns found in various conditions are reproducible, and that of metastatic malignant liver disease is particularly characteristic. The significance of the macromolecular-moving enzyme is discussed and is being investigated.
VARIETY OF CARCINOMAS snow GREATLY A elevated alkaline phosphatase activity and in such cases there is usually a correspond- ingly high total serum alkaline phosphatase.16 A significant rise in total serum alkaline phos- pha tase, however, is not specific to carcinomas, as it occurs also in non-malignant conditions such as Paget’s Disease, osteomalacia, hepatitis and cirrhosis. Many methods, including starch- gel electrophoresis by Rosenberg,13 DEAE cellulose by Grossberg, Harris and Schlamo- wit28 and immunochemical studies by Schla- mowitz and Rodansky,l4 and B ~ y e r , ~ have been used in attempting to establish charac- teristic alkaline phosphatase patterns for var- ious diseased states, but the results obtained
From the Department of Medicine and Therapeutics, Woodview, University College, Dublin, and St. Paul’s Chemotherapy Unit, Harolds Cross, Dublin, Ireland.
* Director, St. Paul’s Chemotherapy Unit. Address for Reprints: Department of Medicine and
Therapeutics, Woodview, University College, Dublin, Ireland.
The authors are indebted to TENOVUS (Wales) for financial support in carrying out this work.
J. J. F. acknowledges the assistance of the Department of Medicine and Therapeutics, U. C. D., and K. McC. acknowledges the generous gift of a Uvicord and frac- tion collector from the Medical Research Council of Ireland.
Received for publication May 11, 1966. ** Alkaline Phosphatase.
have not been of sufficient clarity for applica- tion to clinical work generally.
Prompted by the findings of phosphatase enzymes of different gel-filtration characteris- tics in human tissues,6 we have used this tech- nique to assess possible variation in the mole- cular forms of alkaline phosphatases in human serum. The serum A.P.+ * gel-filtration pattern in normal, malignant and non-malignant con- ditions associated with abnormal phosphatase levels, has been studied in 43 cases, and the results are presented in this communication.
MATERIALS AND METHODS
Gel-filtration: Sephadex G-200 (lot no. T049, particle size 140-400 mesh) was allowed to swell over 72 hours in distilled water and then mounted in a vertical column 2x50 cm. The gel was equilibrated over 48 hours with 0 . 0 5 ~ Tris buffer containing 1 . 0 ~ NaCl at pH 8.0. Samples of serum (1.0 ml) diluted 1.3 with Tris NaCl buffer were eluted through the column with the same buffer at a flow rate of 10-15 ml/hour. Collected with a L.K.B. Eraction collector were 2.0 ml fractions.
Protein: The eluent was scanned continously for protein at 254 mp using an L.K.B. uvi- cord ultraviolet absorptiometer. The fractions were read at 280 mp on a Beckman spectro- photometer.
71

72 CANCER January 1967
RESULTS
Vol. 20
20 30 40 50 6 0 7 0
% B E D V O L U M E
FIG. 1. Gel-filtration pattern of serum proteins and alkaline phosphatase in control serum. Protein -, Enzyme.. . . . .
Alkaline phosphatase: Activity was meas- ured using a modification of the Bessey-Lowry- Brock4 method. The incubation mixture con- tained 2.3 x 1 0 . 4 ~ p-nitrophenylphosphate (Sigma) 0 . 1 7 2 ~ 2 methyl2 amino-1 propanol buffer and 5 mm mg++ (MgC12) at pH 10.0. In the assay 0.5 ml of the fractions were in- cubated at 37 C for 30 mins. The enzymatic reaction was stopped by addition of 2.0 ml. of a solution containing 8 vols. of 0.5 N NaOH and 2 vols. of 0 . 1 ~ EDTA.11 Solutions were then read at 410 mp on a Beckman spec- trophotometer. A reagent analytical blank was carried for all samples and readings were cor- rected accordingly. Optical density readings were converted into pmoles of p-nitrophenol from a standard curve. Alkaline phosphatase is expressed in this communication in inter- national units.
Blood samples: Blood for study was obtained from patients with conditions known to affect total serum alkaline phosphatase levels, con- trols being medical and laboratory personnel. The sera have been divided into five main groups:
1. Normals or controls; 2. Serum from patients with metastatic liver disease-primary lesions stomach, colon, breast and bile duct; 3. Serum from patients with neoplastic bone lesions of both primary nature and metastatic nature from prostate, thyroid and stomach; 4. Serum from patients with non-neoplas- tic liver disease-infective hepatitis, chronic hepatitis and cirrhosis; 5. Serum from patients with benign bone lesions-Paget's disease and osteomalacia.
The sera were stored at -20 C and thawed out slowly before being placed on the col- umns.
Extensive studies have been carried out by Flodin and Killander7 on the fractionation of human serum proteins by gel-filtration on Sephadex G-200. They found that the serum proteins are eluted in 3 main peaks, in order of decreasing molecular size. By a variety of methods including ultracentrifrigation and various types of electrophoresis they have shown the main protein composition of these peaks to be as follows.
Peak 1-Alpha 2 and B, macroglobulins and Alpha and Beta lipoproteins, mainly 19s proteins
Peak 2-y-globulins, mainly 7s proteins Peak 3-Albumin, 4s proteins
The serum protein elution pattern has proved a useful guide in reference to the posi- tion of the phosphatases in all our experi- ments.
Controls: For the purpose of this communi- cation, enzyme peaks will be referred to as 19s peak or 7s peak. Figures 1-5 show the charac- teristic serum A.P. pattern obtained in the five groups studied. The pattern in normals is of one homogeneous peak of enzyme activity in the 7s-globulin region. In some of the normals studied, however, a slight tailing off of enzyme activity into the 19s protein peak region was observed. This was not a "peak" of activity as such, but we have quantitated it in the tables outlining the percentage mean distribu- tion of 19s and 7s peaks of A.P. (Table 1). Thus in the ten normals studied, the percent- age of 19s peak enzyme varied from 0.0 to 7.6%, the mean distribution being 2% for 19.5 peak enzyme and 98% for the 7s peak enzyme.
TABLE 1. Gel-filtration Distribution Pattern in Control Serum
% enzyme distribution
7s peak Initial 19.5 peak
T.P. 0 .0 100.0 O.M. J.M. M.M. J.G. J.D. J.F. M.G. M.C.
0.0 100.0 4 . 8 95.2 5 .4 94.6 7.6 92.4 0.0 100.0 0.2 99.8 0.0 100.0 0.0 100.0 __
MEAN DISTRIBUTION 2.0 98.0
S.D. = 2.0.
No. 1 SEPARATION OF ALKALINE PHOSPHATASE ENZYMES * Diinne et al. 73
2 2 2 . 5 II 25 ' . 20 -
- N ?.
a. k 20 30 40 50 60 70 a
2 2 2 . 5
> n t ..-.
1.5 1 10 l 5 2 5 4 0
.... 0 2
:: g 1.0
J 0 .5 : i..: **,.
. . 0 4
0 0
a. k 20 30 40 50 60 70 a
% BED V O L U M E Q
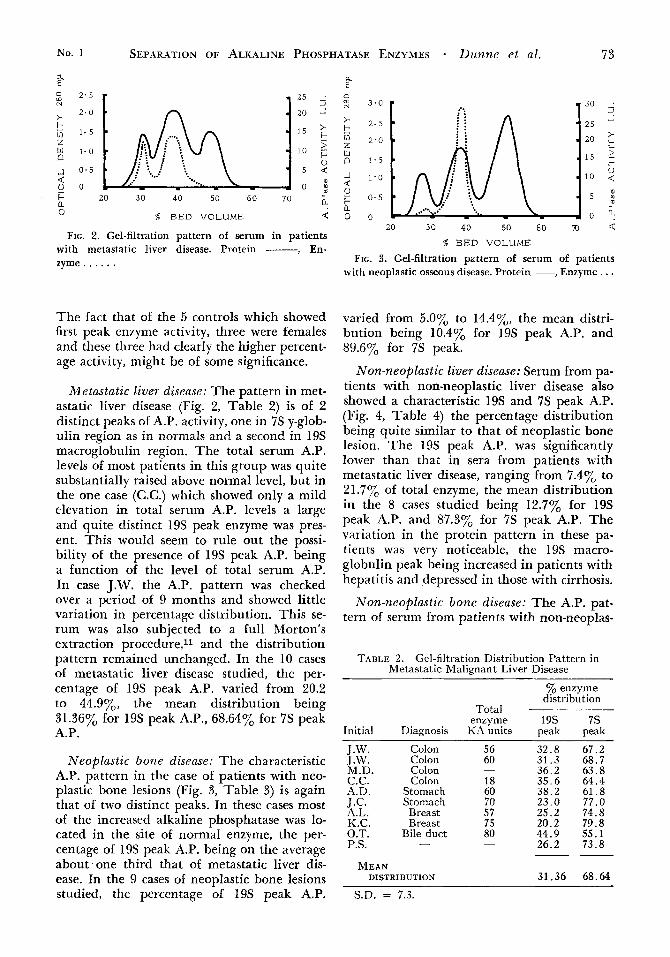
FIG. 2. Gel-filtration pattern of serum in patients with metastatic liver disease. Protein - , En- zyme . . . . . .
0
The fact that of the 5 controls which showed first peak enzyme activity, three were females and these three had clearly the higher percent- age activity, might be of some significance.
Metastatic liver diseuse: The pattern in met- astatic liver disease (Fig. 2, Table 2) is of 2 distinct peaks of A.P. activity, one in 7s y-glob- ulin region as in normals and a second in 19s macroglobulin region. The total serum A.P. levels of most patients in this group was quite substantially raised above normal level, but in the one case (C.C.) which showed only a mild elevation in total serum A.P. levels a large and quite distinct 19s peak enzyme was pres- ent. This would seem to rule out the possi- bility of the presence of 19s peak A.P. being a function of the level of total serum A.P. In case J.W. the A.P. pattern was checked over a period of 9 months and showed little variation in percentage distribution. This se- rum was also subjected to a full Morton's extraction procedure,ll and the distribution pattern remained unchanged. In the 10 cases of metastatic liver disease studied, the per- centage of 19s peak A.P. varied from 20.2 to 44.9%, the mean distribution being 31.36% for 19s peak A.P., 68.64% for 75 peak A.P.
Neoplastic bone disease: The characteristic A.P. pattern in the case of patients with neo- plastic bone lesions (Fig. 3, Table 3) is again that of two distinct peaks. In these cases most of the increased alkaline phosphatase was lo- cated in the site of normal enzyme, the per- centage of 19s peak A.P. being on the average about one third that of metastatic liver dis- ease. In the 9 cases of neoplastic bone lesions studied, the percentage of 19s peak A.P.
T o m N
i
rn z w
-I d
b a 0
t
n
0
3 . 0
2 . 5
2 ' 0
1.5
1 ' 0
0 . 5
0
3 0
25
20
15
10
5
0 20 30 40 50 60 70 <
% BED VOLUME
FIG. 3. Gel-fiItration pattern of serum of patients with neoplastic osseous disease. Protein -, Enzyme . . .
varied from 5.0% to 14.4y0, the mean distri- bution being 10.4% for 19s peak A.P. and 89.6% for 7s peak.
Non-neoplastic liver diseuse: Serum from pa- tients with non-neoplastic liver disease also showed a characteristic 19s and 7s peak A.P. (Fig. 4, Table 4) the percentage distribution being quite similar to that of neoplastic bone lesion. The 19s peak A.P. was significantly lower than that in sera from patients with metastatic liver disease, ranging from 7.4% to 21.7y0 of total enzyme, the mean distribution in the 8 cases studied being 12.7% for 19s peak A.P. and 87.3% for 7s peak A.P. The variation in the protein pattern in these pa- tients was very noticeable, the 19s macro- globulin peak being increased in patients with hepatitis and depressed in those with cirrhosis.
Non-neoplastic bone diseuse: The A.P. pat- tern of serum from patients with non-neoplas-
TABLE 2. Gel-filtration Distribution Pattern in Metastatic Malignant Liver Disease
% enzyme distribution
Total - enzyme 19s 7s
Initial Diagnosis KA units peak peak
J.W. Colon 56 32.8 67.2 T.W. Colon 60 3 1 . 3 68.7 M.D. Colon - 36.2 63 .8 C.C. Colon 18 3.5.6 64.4 A.D. Stomach 60 38.2 61.8 J.C. Stomach 70 23.0 77.0 A.L. Breast 57 25.2 74.8 K.C. Breast 75 20.2 79.8 O.T. Bile duct 80 44.9 55.1 P.S. - - 26.2 73.8 --
MEAN DISTRIBUTION 31.36 68.64
S.D. = 7.3.

74 CANCER January 1967 Vol. 20
g 2 . 5
> 2 - 0
IJI i - 5 z
N
t
2 1.0
-1 0 - 5 d 0 - 0 1
TABLE 3. Gel-filtration Distribution Pattern in Neoplastic Osseous Disease (S.D. = 3.1)
% enzyme distribution
Total
r * 2 5 . . 20 - > ?
' a 15 t I . 10
0 n - 5 4
- - A o :
m
enzyme Initial Diagnosis KA units - J.H. Prostate J.G. Prostate M.L. Prostate O.C. Prostate M.K. Prostate C.E. Prostate E.S. Gastric M.G. Thyroid A.Q. Osteogen sarc.
MEAN DISTRIBUTION
100.0 124.5 34.6
27.0 -10.0 80.0
140.0 26.3
-
19s 7s peak peak
5 .0 95.0 12.8 87.2 6 .3 93.7 8 .3 91.7
14.0 86.0 9 . 4 90.6
14.4 85.6 11.4 88.6 12.0 88.0 10.4 89.6
tic bone lesions (Fig. 5, Table 5 ) was very similar to that of normal serum-one single homogeneous peak of activity in the 7s peak region with a very slight tailing off of activity into the 19s peak region-although in this group the second peak A.P. was greatly ele- vated as compared to normal serum. In the 6 cases studied the percentage of the 19s peak A.P. varied from 0% to 2.6%, the mean dis- tribution being 1.48% for 19s peak A.P. and 98.52% for 7s peak.
DISCUSSION
From these studies it appears that 5 types
1. Normal serum with one peak of activity with a normal protein distribution;
2. Nonmali<gnant osseous disease with an exaggeration of this peak combined with a normal protein pattern;
3. Primary and metastatic malignant os- seous disease with a small extra peak in
of enzyme pattern are obtained:
a 20 30 40 50 60 7 0 a. 0 4
% BED VOLUME
FIG. 4. Gel-filtration pattern of serum of patients with non-malignant liver disease. Protein -, Enzyme. . . . . .
TABLE 4. Gel-filtration Pattern of Serum of Patients with Non-neoplastic Liver Disease
Initial Diagnosis
Total enzyme
KA units
% enzyme distribution
19s 7s peak peak
A.S. Cirrhosis M.H. Cirrhosis F.F. Cirrhosis D.F. Inf. hepatitis M.M. Inf. hepatitis O.C. Hepatitis J.H. Hepatitis A.B. Chr. hepatitis
M E A S DISTKIRUTION
-
30
7.5 92.5 10.2 89.8 1 5 . 1 84.9 7 .4 92.6
27.1 72.9 1 2 . 3 87.7 13.5 86.5 8 . 5 91.5
12.7 87.3
the macromolecular region with minor changes in protein patterns;
4. Nonmalignant liver disease with a mac- romolecular enzyme peak and varying protein abnormalities;
5. Metastatic malignant liver disease with a prominent macromolecular enzyme with marked protein abnormalities.
There is still controversy as to the exact na- ture or source of serum alkaline phosphatase in normal subjects. These differences in opin- ion usually relate to the different techniques being used by the workers in question. Using starch gel, Kowlesserlo suggested an osseous origin, whereas the studies of Hodson and Latner,s using the same techniques, indicated a hepatic origin.
Estborn6 studied tissues and control serum using Sephadex G-200 and noted that bone phosphatase moved with the 19s proteins, whereas the liver enzyme moved with both 19s and 7s proteins. The control serum used

No. 1 SEPARATION OF ALKALINE PHOSPHATASE ENZYMES - Dunne et al. 75
showed main enzyme activity in the 7s region, with a smaller enzyme peak in the 19s region. He concluded that normal serum enzyme is of hepatic origin. Our finding that the enzyme in serum of Paget’s disease moves in the 7s re- gion would appear to be at variance with his finding of bone enzyme in the 19s protein region. In fact our findings suggest that nor- mal serum phosphatase is of bony origin. However, in hepatic conditions there is in addition to the extra or abnormal 19s peak, an increase in the size of the normal 7s peak. This latter fact could be attributed to failure of hepatic excretion of normal serum enzyme. Gel-filtration studies of extracts of various tis- sues similar to those of Estborn, will help to elucidate this point.
The exact significance of the enzyme peak in the 19s macroglobulin region is not known at present. There are at least five possible ex- planations. First, it could represent polymer- ization of a normal enzyme. The position of the 7s peak phosphatase in the elution dia- gram suggests a molecular weight of 120,000 to 150,000 which is in agreement with An- drewsl and others.5 The first peak phosphatase occurring in the macroglobulin region and thus totally excluded from the Sephadex G-200 gel, seems to suggest a molecular weight of at least 200,000, and possibly much larger since G-201) Sephadex may have a higher exclusion point than this figure.2 Schlesinger and Levin- thal,l5 working on E. coli phosphatase have succeeded in splitting the enzyme into sub- units with acetate treatment. To attempt this experiment on 19s peak serum phosphatase at the moment, bearing in mind the compara- tively low enzyme content of serum compared to that of tissue or E coli extracts, would not be feasible as the quantities of serum required would be enormous.
The second possibility is that the occurence of this 19s peak enzyme could be due to link- age of abnormal protein with normal enzyme. Angeletti et aL3 found that, while there was great similarity between the protein of differ- ent tumors, there was poor correlation be- tween proteins of tumors and their tissue of origin. There was no correlation in our studies between the percentage of enzyme in the 19s peak and the amount of protein in that peak. T h e 19s protein peak was most prominent in the patients with hepatitis whose first peak enzyme was 10.4% of the total on average, whereas the least prominent 19s protein peak was in those patients with metastatic liver
T A B L E 5. Gel-filtration Distribution Pattern in Nonmalignant Osseous Disease
% enzyme distribution
Total
Initial Diagnosis
T.B. Osteomalacia J.C. Osteomalacia C.D. Osteomalacia M.D. Osteomalacia J.B. Pagets disease A.E. Pagets disease
MEAN DISTRIBUTION
- . . ~ . ~
enzyme 19s 7s KAunits peak peak
17.3 2 . 6 97.4 64.0 0.9 99.1 13.5 1.4 98.6 26.0 0 .0 100.0
200.0 2 .0 98.0 44.0 2.0 98.0 ~-
1.48 98.52
S.D. = 0.83.
disease whose 19s peak enzyme was 31.36% of the total. Using a modification of Morton’s Butanol extraction procedure,lo we have ex- tracted and purified the alkaline phosphatase of pooled 100 ml lots of serum from patients with metastatic liver disease prior to gel- filtration. The 19s and 7s peaks of phospha- tase were still present, while according to the 254 mp protein scan, there was practically no protein present after this extensive extraction procedure. This fact would appear to argue against a protein enzyme linkage as the cause of the abnormal phosphatase peak; however, further studies are required in this line.
T h e third possibility is that the 19s peak phosphatase could represent carriage by lipo- proteins which are known to affect movements of enzymes in starch gel. After both Morton’s Butanol extraction11 and dextran sulphate precipitation17 (both methods for removal of lipoproteins) were applied to serum of a pa- tient with metastatic liver disease (Case C.C.) no change in the 19s peak phosphatase was noted. This seems to rule out lipoprotein car- riage in this case. However, when serum from a patient with infective hepatitis (Case M.M.) was treated with dextran sulphate, the first peak A.P. disappeared and instead of two distinct peaks as before, the pattern now was that of one distinct 7s peak A.P. with a slight tailing off of activity into the 19s peak, as in normals. Since further study must be made as to the precise mode of action of dextran sulphate, further implications of the above finding cannot be discussed at the present; this finding, however, does suggest the possi- bilities that the 19s peak serum phosphatase is a feature of malignancy only and that the presence of this peak phosphatase in cases of

76 CANCER January 1967 VOl. 20
non-neoplastic liver disease is due to lipopro- tein carriage, and is thus an artefact.
The fourth possibility is that linkage with carbohydrate such as sialic acid is responsible for the presence of 19s peak phosphatase. Moss et a1.12 demonstrated a change of elec- trophoretic pattern of kidney phosphatase when this enzyme was treated with neurami- dase.12 Their studies were carried out on kid- ney phosphatases.
The final possibility is that this finding rep- resents an abnormal enzyme which is present only in the conditions described. This possi- bility will be checked when the enzyme is purified from the malignant and normal tis- sues and subjected to full kinetic studies. A particular value of these studies is in the
identification of the cause for an elevated serum phosphatase where the underlying con- dition is not known. Our studies so. far have indicated this in the case of bony disease. The A.P. in benign bone lesions came out consist-
ently in one peak, whereas the A.P. in both primary and secondary malignant bone condi- tions came out in two distinct peaks. The sharp homogeneous peak in non-malignant bony conditions is obviously of osseous origin. In malignant bone conditions the 7s peak A.P. appears again to be of osseous origin, but the abnormal 19s peak may arise from the malignant process itself. The origin of the 19s peak in hepatic conditions is not clear; it may be of primary hepatic origin as in the case of hepatitis, but in metastatic liver disease the peak A.P. may contain both hepatic and neo- plastic components.
In conclusion we feel that the study of mul- tiple phosphatases (nonspecific) in serum us- ing gel-filtration shows distinctive patterns in particular conditions. At present the tests can differentiate primary bone conditions from primary hepatic conditions and it appears to help in deciding the presence of neoplastic disease.
REFERENCES
1. Andrews, P.: Estimation of the molecular weights of proteins by sephadex gel-filtration. Biochem. J. 91:222, 1964.
2. -* . The gel-filtration behaviour of proteins related to their molecular weights over a wide range. Ibid. 96:595, 1965.
3. Angellette, P. U., Suntzeff, V., and Moore, B. W.: Chromatographic patterns of protein and enzymes in extracts of rhabdomyosarcoma and muscle in mice. Cancer Res. 20: Sept. 1961.
4. Bessey, 0. A., Lowry, 0. H., and Brock, M. S.: Method for rapid determination of alkaline phos- phatase with five cubic millimeters of serum. J. Biol. Chem. 164:321, 1964.
5. Boyer, S. H.: Human organ alkaline phosphatases -Discrimination by several means including starch gel electrophoresis of antienzyme enzyme supernatent fluids. Ann. N.Y. Acad. Ski. 103:938, 1964.
6. Estborn, B.: Separation of phosphatase emzymes by gel-filtration. Klin. Chem. Heft. 253, 1964.
7. Flodin, P., and Killander, J.: Fractionation of human serum proteins by gel-filtration. Biochem. Biophys. Acta. 63:403, 1962.
8. Grossberg, A. L., Harris, E. H., and Schlamowitz, M.: Enrichment and separation of alkaline phosphatase activities of human tissues by chromatography on cellulose on exchange absorbents. Arch. Biochem. Biophys. 93:269, 1961.
9. Hodson, A. W., Latner, A. L., and Raine, L.: Isoenzymes of alkaline phosphatase. CZin. Cha'm. Actu. 7:255, 1962.
10. Knowlessar, 0. D., Haeffner, L. J., and Riley, E. M.: Localisation of serum leucine aminopeptidases, 5-nucleotidase and nonspecific alkaline atosphatase by starch-gel electrophoresis-Clinical and biochemical significance in disease states. Ann. N.Y. Acad. Sci. 9 4 836, 1961.
11. Morton, R. K.: The purification of alkaline phos- phatase of animal tissues. Biochem. J. 57:595, 1954.
12. Moss, D. W., Eaton, R. H., Smith, J. K., and Whitby, L. G.: Alteration in the electrophoretic mo- bility of alkaline phosphatases after treatment with neuramidase. Biochem. J. 98(3):32C, 1966.
13. Rosenberg, I. N.: Zone electrophoresis of serum alkaline phosphatase. J. Clin. Inuest. 38:630, 1959.
14. Schlamowitz, M., and Bodansky, 0.: Tissue sources of human alkaline phosphatase as determined by immunochemical procedures. J. B i d . Chem. 234: 1433, 1959.
15. Schlesinger, M. 'J., and Lovinthal. C.: Hybrid protein formation of E. coli alkaline phosphatase leading to 'in vitro' complementation. J . Mol. Biol. 7:1, 1963.
16. Stadtman, J. D.: Alkaline phosphatases. I n The Enzymes, vol. 5 , 2nd ed., Boyer, Lardy and Myrbach, eds. New York/London, Academic Press, 1961; p. 55.
17. Walton, K. W., and Scott, P. J.: Estimation or low-density (beta) lipoproteins of serum in health and disease using large molecular weight dextran- sulphate. J. CZin. Path. 17:627, 1964.