sickle cell trait: more bad news for the kidneys?
TRANSCRIPT

MARCH/APRIL 2015 VoLuMe 12 Issue 2AsH NeWs AND RePoRTs®
(Cont. on page 2)
JAK2 V617F 10 Years Later: Dr. Dameshek’s Prophecy FulfilledRoss L. Levine, MD,1 anD D. GaRy GiLLiLanD, MD, PhD2
1. Laurence Joseph Dineen Chair in Leukemia Research, Human oncology and Pathogenesis Program, Leukemia service, Department of Medicine, Memorial sloan-Kettering Cancer Center, new york, ny
2. President and Director, Fred Hutchinson Cancer Research Center, seattle, Wa
For more than a century, clinicians have recognized myeloproliferative neoplasms (MPNs) as disorders that are characterized by expansion of different myeloid lineages, with
important clinical sequelae. However, the seminal insight into these diseases came when Dr. William Dameshek wrote in an editorial in Blood that MPNs share specific clinical features including thrombosis, bleeding, and an increased risk of progression to leukemia.1 This critical insight led to the classification of the different MPNs as a set of clinically related myeloid malignancies. However, his prescience did not stop there; he hypothesized that MPNs were caused by an “undiscovered stimulus” and implored the field to investigate the biologic basis of the different MPNs. Although it took more than 50 years, 2005 marked the year that the field began realizing his vision.
over a span of just a few weeks in the spring of 2005, four different groups published their findings on the identification of the somatic JAK2 V617F mutation in 90 percent of patients with polycythemia vera (PV) and in approximately 50 percent of patients with essential thrombocythemia (eT) and primary myelofibrosis (PMF).2-5 The approaches used by each group were quite distinct. Dr. William Vainchenker’s group used elegant functional studies and biochemistry to implicate the JAK2 signaling pathway in MPN proliferation. Dr. Radek skoda and colleagues mapped the region of 9q24 uniparental disomy6 to pinpoint JAK2 mutations, and Dr. Tony Green and colleagues
PeRsPeCTive: JAK2 v617F: 10 yeaRs LaTeR – Dr. Srdan Verstovsek reflects on the clinical experience with JAK inhibitors.
asK THe HeMaToLoGisTs – Drs. Frits Van Rhee and David Fajgenbaum discuss approaches to Castleman disease.
Mini RevieW: LaBiLe iRon – Drs. Ioav Cabantchik and Eliezer Rachmilewitz cover toxicity in iron overload.
THe inTeRnaTionaL HeMaToLoGisT – ASH’s Visitor Training Program connects a Nigerian hematologist with Roswell Park Cancer Institute.
3 4 6 14
D I F F U S I O N
sickle Cell Trait: More Bad news for the Kidneys?naik RP, Derebail vK, Grams Me, et al. association of sickle cell trait with chronic kidney disease and albuminuria in african americans. JaMa. 2014;312:2115-2125.
CHaRLes T. Quinn, MD, Ms
Dr. Quinn indicated no relevant conflicts of interest.
approximately one in 12 African Americans and 300 million people worldwide have sickle cell trait. Sickle cell trait arose as such a common, balanced polymorphism during human history because it affords protection against severe forms of malaria. Despite this clear benefit, sickle cell trait is also associated with a handful of adverse effects. Its
association with exertion-related heat illness and sudden death, although very rare in absolute terms, has garnered the most attention in the press, the legal system, and the pages of The Hematologist.1 The kidney, however, is the organ that is most commonly adversely affected by sickle cell trait. Classic microradioangiographic studies demonstrated that the vasa recta in the renal medulla are disrupted in sickle cell trait, although to a lesser extent than is seen in sickle cell anemia.2 Known renal manifestations of sickle cell trait include microscopic hematuria, renal papillary necrosis with gross hematuria, isosthenuria (a mild urinary concentrating defect), and renal medullary carcinoma (also quite rare in absolute terms). Sickle cell trait has also been associated with earlier progression to end-stage renal disease (ESRD) in people with autosomal-dominant polycystic kidney disease.3
In the general population, an important and largely unexplained observation is that African Americans have a higher risk of chronic kidney disease (CKD) and progression to ESRD than European Americans or Asian Americans. Some, but not all, of this risk has recently been attributed to variants of apolipoprotein L-1 encoded by APOL1.4 Might sickle cell trait, given its known adverse renal effects and high frequency in the African American population, additionally explain the racial disparity in the risk of CKD? Dr. Rakhi Naik and colleagues sought to answer this question. The investigators conducted a pooled analysis of more than 15,000 individuals from five population-based African American cohorts. Sickle cell trait status was genetically determined, and different models were adjusted for age, sex, proportion of African genetic ancestry, baseline diabetes, baseline hypertension, and the presence of APOL1 risk variants. Indeed, the investigators found that sickle cell trait was associated with incident and prevalent CKD, decline in the estimated glomerular filtration rate (eGFR), and albuminuria. These associations were independent of APOL1 risk variants. There was no association with ESRD in their analysis, but the number of incident ESRD cases was relatively small.
This study had a number of limitations. The causes of all cases of CKD were not recorded uniformly, direct genotyping of sickle cell trait status was not available for all individuals, potential modifying effects of co-inherited α-thalassemia were not studied,5 and APOL1 status was only available in two of the five pooled cohorts. Nevertheless, this was a rigorous study with many strengths given that it was a large, prospective, population-based sample of African Americans with detailed genotypic and phenotypic data that evaluated outcomes not studied before in individuals with sickle cell trait.
In summary, Dr. Naik and colleagues present a persuasive analysis that supports an association between sickle cell trait and the occurrence of CKD, decline in eGFR, and albuminuria in the African American population. Notably, the association of CKD with sickle cell trait was independent of APOL1 risk variants. These findings indicate that sickle cell trait is an additional genetic risk factor that can help to explain the racial disparity in the occurrence of CKD. Quantitatively, according to this analysis, sickle cell trait has a population-attributable risk for incident CKD of 6 percent. Important research like this accords well with ASH’s recently published research priorities for sickle cell disease, which include a specific call for an investment in research on sickle cell trait. Sickle cell trait is associated with numerous potential adverse effects, mainly renal; however, it is also important to remember that most individuals with trait will have no related health consequences. An ongoing challenge for hematologists is to communicate with our colleagues in other specialties and with the public about the results of such research on adverse effects of sickle cell trait without generating undue alarm. This can happen by continuing to demand and generate the best epidemiologic and medical evidence, and by always clearly communicating the magnitude of the risk of adverse effects of sickle cell trait. Websites that provide quality information in proper context about sickle cell trait, written primarily for the public include: www.cdc.gov/ncbddd/sicklecell/toolkit.html (from ASH and the Centers for Disease Control and Prevention) and www.sicklecelltrait.org (by Cincinnati Children’s Hospital Medical Center).
1. Abkowitz JL. Sickle cell trait and sports: is the NCAA a hematologist? The Hematologist. 2013;10:1-2.
2. Statius van Eps LW, Pinedo-Veels C, de Vries GH, et al. Nature of concentrating defect in sickle-cell nephropathy: microradioangiographic studies. Lancet. 1970;1:450-452.
3. Yium J, Gabow P, Johnson A, et al. Autosomal dominant polycystic kidney disease in blacks: clinical course and effects of sickle-cell hemoglobin. J Am Soc Nephrol. 1994;4:1670-1674.
4. Genovese G, Friedman DJ, Ross MD, et al. Association of trypanolytic ApoL1 variants with kidney disease in African Americans. Science. 2010;329:841-845.
5. Gupta AK, Kirchner KA, Nicholson R, et al. Effects of alpha-thalassemia and sickle polymerization tendency on the urine-concentrating defect of individuals with sickle cell trait. J Clin Invest. 1991;88:1963-1968.
TuFT
S P
Ho
To A
RC
HIV
ES
Dr. William Dameshek (1900-1969). Read Dr. Srdan Verstovsek's clinical perspective on JAK2 V617F on page 3.
ME
Mo
RIA
L S
LoA
N
KE
TTE
RIN
G C
AN
CE
R
CE
NTE
R

President’s Column
2 The Hematologist: ASH NewS AND RePORtS
AsH NeWs AND RePoRTs ®
IssN 1551-8779
Editor-in-Chief:Jason Gotlib, MD, MSStanford Cancer InstituteStanford, CA
Contributing Editors:Pamela S. Becker, MD, PhDUniversity of washingtonSeattle, wA
theresa Coetzer, PhDUniversity of the witwatersrandJohannesburg, South Africa
Adam Cuker, MD, MSUniversity of PennsylvaniaPhiladelphia, PA
David Garcia, MDUniversity of washingtonSeattle, wA
tracy I. George, MDUniversity of New MexicoAlbuquerque, NM
Jonathan Hoggatt, PhDHarvard UniversityCambridge, MA
Peter Johnson, MDSouthampton General HospitalSouthampton, United Kingdom
Mark J. Koury, MDVanderbilt UniversityNashville, tN
Ann LaCasce, MD, MScDana-Farber Cancer InstituteBoston, MA
Charles t. Quinn, MD, MSCincinnati Children’s Hospital Medical CenterCincinnati, OH
elizabeth Raetz, MDUniversity of UtahSalt Lake City, Ut
Noopur Raje, MDMassachusetts General HospitalBoston, MA
Managing Editor
Juana Llorens, MS
Graphic Designer
grayHouse design
American Society of Hematology2021 L Street, NW, Suite 900Washington, DC 20036 [email protected]
©2015 by the American Society of Hematology.
All materials contained in this newsletter are protected by copyright laws and may not be used, reproduced, or otherwise exploited in any manner without the express prior written permission of The Hematologist: ASH News and Reports. Any third-party materials communicated to The Hematologist become its copyrighted property and may be used, reproduced, or otherwise exploited by The Hematologist.
Contributing authors have declared any financial interest in a product or in potentially competing products, regardless of the dollar amount. Any such financial interest is noted at the bottom of the article.
Dr. Gotlib has no relevant conflicts of interest to disclose.
HematologistTHE
Earnest Support for Careers and Cures
In the past year, AsH provided more than $8 million in awards and scholarships to support hematologists in all stages of their careers. AsH supports career enhancement awards such as scholar Awards, Research Training Awards for Fellows (RTAF), and awards dedicated to increasing the number of underrepresented minority scholars in hematology. Furthermore, training
programs such as the Clinical Research Training Institute (CRTI) and Translational Research Training in Hematology (TRTH) are designed to give young researchers the pivotal tools, mentoring, and access to resources beneficial for a successful career in hematology. one of AsH’s newest awards, the AsH Bridge Grant Program, was designed to help preserve the careers of its talented member scientists whose vital research would not otherwise be accomplished due to across-the-board cuts to the National Institutes of Health (NIH) budget.
our members have historically turned to the society during times of need. With severe constraints on NIH research funding, AsH leadership felt strongly that we needed to do something bold to directly support our members during this very harmful funding downturn. During its 2012 spring retreat, the AsH executive Committee adopted a strong and proactive approach to combat this progressive decline in NIH research funding by allocating $9 million over three years specifically for R01 bridge funding. These monies were to be allocated for up to 30 meritorious bridge awards annually and would be focused on benefitting hematologists at all levels of their careers. The ultimate goal was to retain outstanding researchers in our field so that they could continue their critical research and prevent hematology research laboratories from closing. Amazingly, in approximately six months, AsH developed and implemented a program for members who had applied for an NIH R01 or equivalent who were denied funding for an NIH R01 or equivalent due to budget constraints. The AsH Bridge Grant Program has been lauded by our members, cited by the press, admired by the NIH, and copied by other societies. By all measures, this program has made a huge impact.
All AsH awards are designed with metrics and end points so that we are able to gauge the success of our initiatives. With that in mind, I am delighted to share two real-life examples of members who directly benefitted from this new AsH initiative. Drs. Merav socolovsky (university of Massachusetts Medical school) and Christopher Porter (university of Colorado school of Medicine) both cite the AsH Bridge Grant Program as essential in obtaining R01 funding, keeping their laboratories active during their interim funding crunch, and ultimately being critical to their successful academic promotions. Dr. Porter commented, “Due to the bridge funding, I did not have to reduce the size of my lab with personnel cuts prior to the award of the R01. Thus, AsH Bridge Grant funds directly promoted the advancement of our laboratory work leading to R01 funding.” Dr. socolovsky’s revised R01, submitted after being awarded an AsH Bridge Grant, scored 3 percent at the NIH (NIDDK). she stated that, “Without the AsH Bridge Grant, I would certainly not have obtained R01 funding.”
Drs. socolovsky’s and Porter’s achievements are just two examples of the multitude of hematologists who have directly benefitted from AsH’s awards and scholarships. AsH programs such as the HoNoRs Awards, the Minority Medical student Awards, and the scholar Awards, have yielded equally successful results that have helped promote our field’s research missions. Today, I’d like to recognize and celebrate all those whose careers have been advanced by the support they received from AsH. Congratulations to them … and to AsH!
David A. Williams, MD
Dr. Dameshek’s Prophecy Fulfilled(Cont. from page 1)
investigated key signaling pathways for somatic mutations in MPN patient samples. our collaborative efforts employed a novel ascertainment protocol to capture MPN samples, followed by high-throughput tyrosine kinome sequencing to uncover the JAK2 V617F allele. Although the approaches were different, the results were the same, and we all realized the importance of this discovery and its potential impact.
At the time, the field rapidly moved to translate this discovery into the clinical setting, and many of us believed it would have major implications for the diagnosis and therapy of PV, eT, and MF. This has indeed turned out to be the case. JAK2 molecular testing is now an essential aspect of the diagnosis of the different MPNs, with mutational testing for JAK2 V617F being the standard of care worldwide. However, there have been many surprises along the way since the discovery of JAK2 V617F. It has taken almost a decade to identify most of the somatic mutations that govern JAK2 V617F–negative MPNs, including JAK2 exon 12 mutations in PV7 and thrombopoietin receptor (MPL) mutations eT and PMF.8 More recently, two groups identified recurrent mutations in the calreticulin (CALR) gene in the majority of JAK2/MPL–wild-type MPN patients.9,10 Although there are still many questions that remain, our knowledge of the genetic basis of the different MPNs has increased dramatically since 2005, and we now have a molecular framework of the different MPNs, which can inform mechanistic and translational studies. More importantly, the discovery of JAK2 mutations suggested that JAK-sTAT signaling was a central feature of MPN pathogenesis, which led to the development
LetteRS tO tHe eDItOR SOLICItAtIONThe Hematologist welcomes letters of up to 200 words. Please include a postal address, email address, and phone number. Publication will be based on editorial decisions regarding interest to readers and space availability. we may edit letters for reasons of space or clarity. The Hematologist reserves the right to publish your letter, unless it is labeled “not for publication.”
Letters should be sent to:
Juana Llorens, Managing editor The Hematologist: ASH News and Reports2021 L Street, Nw, Suite 900 washington, DC 20036

President’s Column
The Hematologist: ASH NewS AND RePORtS 3
Dr. Dameshek’s Prophecy Fulfilled(Cont. from page 1)
and approval of the JAK1/JAK2 inhibitor ruxolitinib for patients with MF, and more recently for PV patients with resistance or intolerance to hydroxyurea.11
We recognize that there is still much to learn. At the time of the discovery of JAK2, we hypothesized that subsequent genomic studies would elucidate the basis for phenotypic pleiotropy of JAK2-mutant MPNs; however we still do not know why JAK2 mutations are observed in a spectrum of different MPNs with varying clinical presentations and outcomes. Additionally, although the discovery of JAK2 mutations has led to the clinical development of JAK kinase inhibitors, there remains a pressing need to understand the basis for JAK2-inhibitor sensitivity and resistance, and to develop novel therapeutic approaches and combination strategies to improve patient outcomes. Toward that end, we have been able to identify bypass mechanisms by which JAK2 can be activated in JAK2 inhibitor “persistent” cells and patient samples. This has led us to investigate whether novel therapeutic approaches, including Hsp90 inhibitors and type II JAK2 inhibitors, can be used to improve JAK2 targeting and to increase therapeutic efficacy. We are confident that these challenges will be solved by our field.
However, in our view, the discovery of the JAK2 V617F mutation has meant much more. In 2004, MPN investigators presented their work at the AsH annual meeting in a single Tuesday-morning simultaneous oral session with no more than 50 people in the room. Now, thousands of annual meeting attendees can hear about developments
JAK Inhibitors: “Life is Good, Stable is Good”sRDan veRsTovseK, MD, PhD
Professor of Medicine; Director, Hanns a. Pielenz Clinical Research Center for Myeloproliferative neoplasms; Department of Leukemia, MD anderson Cancer Center, Houston, TX.
in MPNs, including numerous preclinical models, genomic studies, and clinical trials of novel agents in various stages of development. In short, JAK2 V617F was a disruptive breakthrough that re-energized the field and ushered in the modern era of MPN biology. on a personal note, this discovery was the impetus for one of the authors to start his career (R.L.), and there are many other investigators whose careers were accelerated, inspired, and based on this seminal finding. If not for the vision and support of the senior MPN investigators who led these initial efforts, we would not have a vibrant field of innovative and collaborative researchers and clinicians who continue to make discoveries that elucidate biology and help MPN patients on a daily basis.
JAK2 V617F represented a key finding at a critical time that helped to usher in the modern era of precision medicine. We now take for granted that molecular genetic studies can be used to diagnose cancer patients, to risk stratify patients into different subsets, and to guide the development and use of molecularly targeted therapies in the clinic. The identification of JAK2 V617F provided the impetus for the next decade of genomic insights in nearly all human malignancies. We are at a different place now because of this discovery; in countless ways, it has changed the lives of scientists, physicians, and, most importantly, patients.
Dr. Levine and Dr. Gilliland indicated no relevant conflicts of interest.
1. Dameshek W. some speculations on the myeloproliferative syndromes. Blood. 1951;6:372-375.
2. Baxter eJ, scott LM, Campbell PJ, et al. Acquired mutation of the tyrosine kinase JAK2 in human myeloproliferative disorders. Lancet. 2005;365:1054-1061.
3. James C, ugo V, Le Couedic JP, et al. A unique clonal JAK2 mutation leading to constitutive signalling causes polycythaemia vera. Nature. 2005;434:1144-1148.
4. Kralovics R, Passamonti F, Buser As, et al. A gain-of-function mutation of JAK2 in myeloproliferative disorders. N engl J Med. 2005;352:1779-1790.
5. Levine RL, Wadleigh M, Cools J, et al. Activating mutation in the tyrosine kinase JAK2 in polycythemia vera, essential thrombocythemia, and myeloid metaplasia with myelofibrosis. Cancer Cell. 2005;7:387-397.
6. Kralovics R, Guan Y, Prchal JT. Acquired uniparental disomy of chromosome 9p is a frequent stem cell defect in polycythemia vera. exp Hematol. 2002;30:229-236.
7. scott LM, Tong W, Levine RL, et al. JAK2 exon 12 mutations in polycythemia vera and idiopathic erythrocytosis. N engl J Med. 2007;356:459-468.
8. Pikman Y, Lee BH, Mercher T, et al. MPLW515L is a novel somatic activating mutation in myelofibrosis with myeloid metaplasia. PLos Med. 2006;3:e270.
9. Klampfl T, Gisslinger H, Harutyunyan As, et al. somatic mutations of calreticulin in myeloproliferative neoplasms. N engl J Med. 2013;369:2379-2390.
10. Nangalia J, Massie Ce, Baxter eJ, et al. somatic CALR mutations in myeloproliferative neoplasms with nonmutated JAK2. N engl J Med. 2013;369:2391-2405.
11. Verstovsek s, Mesa RA, Gotlib J, et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N engl J Med. 2012;366:799-807.
As we opened the first three clinical trials of JAK inhibitors in the summer of 2007 at MD Anderson Cancer Center, there was palpable enthusiasm and much anticipation among both physicians and patients. I vividly
remember my first patient who enrolled in the phase I/II trial of ruxolitinib (the very first person in the world to be treated with a JAK inhibitor, in fact). He was an older man with massive splenomegaly and hepatomegaly resulting in ascites and swelling of the legs, severely compromising his ambulation and quality of life. In addition to worsening ane-mia, he developed substantial weight loss, cachexia, night sweats, low-grade fevers, and overwhelming fatigue – classic features of progressive myelofibrosis. He was refractory to standard therapies and was very anxious to start on this new therapy – so much so that he spent one month in a hotel in Houston (he was from Florida) waiting for the trial to begin. In short, this trial was his only hope. None of us knew what would happen. We were cautiously optimistic. JAK inhibitors were the first targeted therapies to be tested in myelofibrosis (MF), but would the drug be tolerable? What would be its effects? We didn’t know.
That first month, during which we enrolled the first three patients in the first dose cohort, was quite amazing. Within one month of starting ruxolitinib, the first patient’s spleno-megaly disappeared, and his hepatomegaly was reduced. His ascites and leg swelling markedly improved, as did his systemic symptoms. His energy level significantly improved. It was an unbelievable transformation. He was able to return to his daily activities, and several months later, upon return to Florida, resumed playing golf – his favorite pastime that he had given up more than a year prior owing to progressive disease. He went on to live another three years with a very good quality of life before eventually succumbing to MF.
The third patient we enrolled was a patient of Dr. Hagop Kantarjian, chairman of our leukemia department. The patient was a woman in her late 50s with a spleen so large, she looked as though she were nine months pregnant. Within two weeks of taking ruxolitinib, her spleen began shrinking, and after one month, her spleen was 50 percent smaller. Her energy level improved, and she began to gain weight. Her improvements were so dramatic that I called Dr. Kantarjian to come to my clinic so he could see for himself her transformation. Amazingly, to date, this patient is still enrolled in the same trial and has been taking ruxolitinib now for 7½ years – the longest anyone in the world has been treated with a JAK inhibitor.
We were awe-struck by the dramatic transformations of these first few patients. These patients were very sick and were unable to participate in most of their normal daily activities. The JAK inhibitor gave them their lives back. Along with the large reductions in splenomegaly, their symptoms also began to lessen. Patients regained their appetites and started gaining weight. Life was good again. of course, along with triumph comes disappointment. By the traditional criteria with which we would evaluate a response in hematologic malignancies, these patients would have been considered “failures” as none of them achieved complete or partial remissions. However, the improvements in symptoms and quality of life could not be denied.
This marked a turning point in the way we think about and treat myeloproliferative neoplasms (MPNs). We began to question how we define clinical benefit. The develop-ment of the MF symptom assessment form (MF-sAF)1 has allowed us to measure and quantify symptoms and qual-ity of life, fundamentally transforming the way we assess therapeutic responses in MPNs. The change in the MPN symptom assessment form (MPN-sAF) was accepted by the u.s. Food and Drug Administration as a secondary end point in their evaluation of ruxolitinib. This was the first time in malignant hematology that symptom improvement was used as a secondary end point in a phase III approval study (the CoMFoRT-I study).2 A 50-percent reduction in the MPN-sAF is now included as a response in the revised response criteria for MF published in 2013 and is included as a primary or secondary end point in all clinical studies of new therapies in MF.3 Furthermore, we now know, after a series of long-term follow-up analyses, that in addition to improving symptoms and quality of life, ruxolitinib also prolongs patients’ lives, altering the natural course of the disease.4-6 so, although JAK inhibitors are not curative and do not eradicate the disease (exceptions exist), they have given people their quality of life back for much longer than expected. I recently saw another patient who had been on a JAK inhibitor since fall 2007 when she came to see us. At that time, she was using a wheelchair and had advanced MF. At this most recent clinic visit, she took out a photo of her family that displayed four young children, all less than five years of age. Then she said, “If it were not for this therapy, I would not have seen my four grandkids. Life is good. stable is good.” I cannot agree more, as I have learned to value “stable.” It is not always about achieving a response by tra-ditional response criteria, but rather helping patients live longer with a good quality of life.
During the past 10 years, we have also learned that the story is much more complicated than we had initially realized. We now know that there are other mutations other than JAK2 V617F driving upregulated JAK-sTAT signaling (e.g., MPL, CALR, and potentially others). Recurrent mutations in genes involved in epigenetic regulation (ASXL1, IDH 1/2, EZH2), splicing (SRSF2), and other cellular functions have been identified, and these likely contribute to the heterogeneity in the clinical presentation of patients with MF and other MPNs.7 Ten years since the discovery of JAK2 V617F, we are now combining novel therapies that target other pathways (e.g., epigenetic inhibitors, Hedgehog pathway inhibitors, PI3K inhibitors, and others) with JAK inhibitors to bring added benefits to patients, such as improving anemia, reducing bone marrow fibrosis, and always trying to extend the duration and quality of life. Additionally, drugs targeting cellular functions other than cell signaling and epigenetic regulation (e.g., imetelstat, which targets telomerase, and the anti-fibrotic agent PRM-151) are exciting areas of clinical development in MF. There is so much more to do, and JAK inhibitors are only the beginning.
Dr. Verstovsek receives research support for the conduct of clinical studies from Incyte Corporation, AstraZeneca, Lilly oncology, Roche, Geron, Ns Pharma, Bristol Myers squibb, Celgene, Infinity Pharmaceuticals, Gilead, seattle Genetics, Promedior, CTI BioPharma Corp. (formerly Cell Therapeutics, Inc.), Galena BioPharma, and Pfizer.
1. Mesa RA, et al. The Myelofibrosis symptom Assessment Form (MFsAF): an evidence-based brief inventory to measure quality of life and symptomatic response to treatment in myelofibrosis. Leuk Res. 2009;33:1199-1203.
2. Verstovsek s, et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N engl J Med. 2012;366:799-807.
3. Tefferi A, et al. Revised response criteria for myelofibrosis: International Working Group-Myeloproliferative Neoplasms Research and Treatment (IWG-MRT) and european LeukemiaNet (eLN) consensus report. Blood. 2013;122:1395-1398.
4. Cervantes F, et al. Three-year efficacy, safety, and survival findings from CoMFoRT-II, a phase 3 study comparing ruxolitinib with best available therapy for myelofibrosis. Blood. 2013;122:4047-4053.
5. Vannucchi AM, et al. A pooled overall survival analysis of the CoMFoRT studies: 2 randomized phase 3 trials of ruxolitinib for the treatment of myelofibrosis [abstract]. Blood. 2013;122:abstr 2820.
6. Verstovsek s, et al. Three-year efficacy, overall survival, and safety of ruxolitinib therapy in patients with myelofibrosis from the CoMFoRT-I study. Haematologica. 2015 [epub ahead of print].
7. Vannucchi AM, et al. Mutations and prognosis in primary myelofibrosis. Leukemia. 2013;27:1861-1869.
P e R S P e C t I V e

4 The Hematologist: ASH NewS AND RePORtS
Ask the HematologistsFRiTs van RHee, MD, PhD, MRCP(uK), FRCPath,1 anD DaviD FaJGenBauM, MD, Msc2
1. Professor of Medicine, Myeloma institute for Research and Therapy, university of arkansas for Medical sciences; Co-Founder and scientific Board Member Castleman Disease Collaborative network; Little Rock, aR
2. adjunct assistant Professor of Medicine, Department of Hematology/oncology, university of Pennsylvania; Co-Founder and executive Director Castleman Disease Collaborative network; Philadelphia, Pa
ASH does not recommend or endorse any specific tests, physicians, products, procedures, or opinions, and disclaims any representation, warranty, or guaranty as to the same. Reliance on any information provided in this article is solely at your own risk.
The QuestionWhat are your treatment approaches to Castleman disease with the advent of anti–interleukin-6 therapy?
our ResponseCastleman disease (CD) describes a group of heterogeneous lymphoproliferative disorders that share common histopatho-logical lymph node changes. CD can present with localized (unicentric CD or uCD) or generalized lymphadenopathy (multicentric CD or MCD). MCD should be further divided into human herpesvirus 8 (HHV-8) –positive and HHV-8–nega-tive MCD (Table). The latter is also referred to as idiopathic MCD (iMCD). MCD patients can exhibit a spectrum of clinical features from mild flu-like symptoms to sepsis-like multiorgan failure.1 It is important to distinguish these three entities since they require entirely different therapeutic approaches.
uCDuCD presents with lymphadenopathy confined to one lymph node region, and many patients are asymptomatic. symptoms are usually due to compression of vital structures such as the trachea, blood vessels, or nerves. uCD occurs most frequently in younger females. The diagnosis is made when excisional lymph node biopsy shows characteristic Castleman changes. Approximately 90 percent of uCD cases demonstrate the hyaline vascular (HV) subtype. The other 10 percent of patients with uCD demonstrate mixed cellularity or plasmacytic (PC) pathology and may have constitutional symptoms such as fever, fatigue, and weight loss. uCD is not associated with HHV-8 or HIV infection. There is an increased association with lymphoma, which may have been present all along, or the uCD may “transform” into lymphoma. The etiology of uCD is poorly understood, and there is usually no excess interleukin-6 (IL-6) secretion. Limited studies have demonstrated abnormal cytogenetics or evidence of monoclonality in stromal cells, but the significance of these findings is unknown.2 surgical extirpation is curative in 95 percent of uCD cases.3 unresectable cases can be treated with rituximab and steroids, which may induce complete responses or shrink the mass sufficiently to make it resectable. uCD lymphadenopathy is highly vascularized, and embolization is a further therapeutic option. Involution of lymphadenopathy after radiotherapy has also been reported. Difficult cases require a multimodal approach and are best managed at an experienced center.
HHV-8–Positive MCDHHV-8–positive MCD presents with generalized lymphadenopathy and constitutional symptoms and can progress to multiorgan failure leading to death. The disease is driven by the excessive release of viral IL-6, which is encoded by the HHV-8 virus and drives human IL-6, IL-10, and vascular endothelial growth factor (VeGF) secretion. HHV-8–positive MCD was first described during the AIDs epidemic and is classically thought to be due to lytic replication of HHV-8 in the setting of HIV infection.4 However, there are also patients with HHV-8–positive MCD who are HIV negative. These patients may have another cause for immunosuppression that impairs their control of HHV-8.5 Approximately 10 to 20 percent of individuals have been exposed to HHV-8, and the virus remains dormant in B lymphocytes. A diagnosis of HHV-8–positive MCD can be rendered if the patient has 1) a pathologic diagnosis of CD made on an excisional lymph node biopsy and 2) actively replicating HHV-8 virus detected in the peripheral blood by molecular testing (quantitative polymerase chain reaction [PCR]) or a positive stain of the lymph node for the HHV-8 latency associated nuclear antigen (LANA-1). HIV-positive, HHV-8–positive MCD patients may have coexistent Kaposi sarcoma and are prone to develop HIV-associated lymphomas. Lymph node pathology shows plasmacytic or
plasmablastic changes, and the plasma cells may exhibit light chain restriction. Intranodal microlymphomas have also been reported. HHV-8–positive MCD is effectively treated with rituximab, which depletes the reservoir of HHV-8–positive cells and significantly reduces the risk of lymphoma.6 More severely afflicted patients may additionally require etoposide. some experts recommend maintenance therapy with valganciclovir. HIV-positive patients should receive appropriate HAART therapy.7 The value of tocilizumab, which blocks the human IL-6 receptor is the subject of ongoing studies. siltuximab, which is a monoclonal antibody to IL-6, has not been studied in HHV-8–positive MCD because it did not bind to viral IL-6 in preclinical studies.
iMCD HHV-8–negative MCD patients present with generalized lymphadenopathy and constitutional symptoms, and can also develop multiorgan failure. The disease can wax and wane, be gradually progressive, or have severe episodic flares resulting in death.8 In a recent literature review, 22 percent of HHV-8–negative MCD patients had died by a median follow-up time of 29 months.9 HHV-8–negative MCD is driven by pro-inflamma-tory hypercytokinemia, most notably of IL-6, which leads to: anemia; anasarca due to hypoalbuminemia from IL-6–mediated liver dysfunction and VeGF-mediated vascular permeability; and systemic inflammation with elevated esR, CRP, and fibrin-ogen.8 some patients may develop kidney, liver, and bone marrow failure and succumb to their disease. Patients with HHV-8–negative MCD may also have one or more features of PoeMs (polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes) syndrome, or a concurrent PoeMs syndrome.10 Patients with one or more features of PoeMs often have less florid constitutional symptomatology.
The etiology of the pro-inflammatory hypercytokinemia in iMCD has not yet been identified. The pathologic cell and the responsible intracellular inflammatory pathway responsible for producing the IL-6 in these patients has also not been elu-cidated. Hypothesized etiologies include an unknown virus, a small population of malignant cells, or germline genetic muta-tions in the immune system.1 No single gene causing iMCD has been identified, but systematic sequencing has not been performed. The disease may be influenced by ethnicity and genetic factors such as a polymorphism of the IL-6 receptor.11 Asian patients may demonstrate violaceous skin lesions or interstitial pneumonitis usually not seen in other populations. Currently, a diagnosis of iMCD can be made when patients have 1) histopathology typical of CD on excisional lymph node biopsy, 2) multiple regions of enlarged lymph nodes, 3)
negative quantitative PCR for HHV-8 in the peripheral blood or negative LANA-1 staining of the lymph node biopsy, and 4) systematic exclusion of diseases known to demonstrate Castleman-like histopathology (e.g., systemic lupus erythe-matosus, epstein-Barr virus, lymphoma, IgG4-associated lymphadenopathy). Hence, both HHV-8–positive and –negative MCD are not purely pathologic diagnoses. efforts are currently underway to establish international consensus around clinical, pathologic, and exclusion criteria for the diagnosis of iMCD. Although the PC variant predominates in iMCD, HV and mixed pathology have also been reported.
HHV-8-negative MCD has been historically managed with corticosteroids, rituximab, and/or chemotherapeutic agents derived from the CHoP regimen. Corticosteroids may temporarily control symptoms, but patients relapse on tapering. Rituximab has not been systematically evaluated in iMCD and a limited number of case reports suggest that patients often relapse. Monoclonal antibodies targeting IL-6 have been recently developed and more rigorously evaluated. A single-arm study of 28 Japanese patients on tocilizumab demonstrated a high response rate in terms of symptoms, laboratory parameters, and reduction in lymphadenopathy.12 siltuximab was evaluated in a double-blind, placebo-controlled, randomized study using a control arm of best supportive care including up to 60 mg of prednisone. The combined durable symptomatic and tumor response was 34 percent, and 50 percent of patients remained on drug for the duration of the study. This study provided the first placebo-controlled evidence for an iMCD therapy, and siltuximab is the first drug approved for iMCD by the u.s. Food and Drug Administration and european Medicines Agency. Both siltuximab and tocilizumab are safe and well-tolerated.13 For patients who do not respond to anti–IL-6 therapy, immunosuppressants, immunomodulators, biologics, and cytotoxic chemotherapies, including cyclosporine, sirolimus, bortezomib, thalidomide, anakinra, interferon-α, cyclophosphamide, and etoposide, have been reported to have some success in case reports or small series.
Choice of Therapy for iMCDIn the authors’ opinion, patients with iMCD should first be treated with anti–IL-6 therapy approved in that region (siltuximab in North America and the european union; tocilizumab in Japan). Patients with few symptoms or laboratory abnormalities suggestive of little excess IL-6 may not respond well to anti–IL-6 blockade and should be considered for rituximab and steroids. Patients with severe hypercytokinemia and organ failure may not respond
4 The Hematologist: ASH NewS AND RePORtS
*Symptoms: fevers, night sweats, anorexia, weight loss, fatigue. Laboratory abnormalities: anemia, thrombocytopenia or thrombocytosis, elevated C-reactive protein, Westergren erythrocyte sedimentation rate, fibrinogen, hypergammaglobulinemia, abnormal renal function, increased interleukin-6 (IL-6), vascular endothelial growth factor, interleukin-10.
Abbreviations: QPCR, quantitative polymerase chain reaction; LANA-1, latency associated nuclear antigen.
Type of Castleman
Disease
Type of Lymphadenopathy
Pathology iL-6–Driven inflammatory
syndrome*
virologic status Treatment
unicentric Localized 90 percent hyaline vascular
Typically not • Negative for HHV-8 by QPCR or negative LANA-1 stain
Complete excision
Multicentric HHV-8–Positive
Generalized ± hepatosplenomegaly
Plasmacytic orplasmablastic
Yes • Positive for HHV-8 by QPCR
• May be positive for HIV
• Rituximab ± etoposide
• optional valganci-clovir maintenance
Multicentric HHV-8–Negative(Idiopathic)
Generalized ± hepatosplenomegaly
Mostly plasmacytic, but can be hyaline vascular or mixed cellularity
Yes, but variable clinical presenta-tion from mild to very severe
• Negative for HHV-8 by QPCR or Negative LANA-1 stain
• Negative for HIV
• Siltuximab
• Tocilizimab
• Rituximab
• Chemotherapy in severe cases
Table. Features of the Different Types of Castleman Disease

The Hematologist: ASH NewS AND RePORtS 5The Hematologist: ASH NewS AND RePORtS
t H e P R A C t I C I N G H e M A t O L O G I S t
sufficiently to anti–IL-6 targeting monoclonal antibodies, and they require combination chemotherapy or consideration of experimental treatment. Dosing intervals can be spaced out in selected patients responding to anti-IL-6 therapy. Progressive motor polyneuropathy suggesting coexistent PoeMs does not respond well to rituximab or to IL-6–targeted therapy, and these patients require autologous stem cell transplantation as part of their treatment plan.
The FutureThe introduction of rituximab has been a major advance in HHV-8–positive MCD, while therapy with IL-6–targeting monoclonal antibodies is an important innovation in iMCD. However, anti–IL-6 therapy is not effective for all patients, and it is not curative, as cessation of treatment results in relapse. In 2012, we co-founded the Castleman Disease Collaborative Network (CDCN; www.castlemannetwork.org) to accelerate research and elucidate the pathogenesis of MCD. In 2.5 years, we have assembled a 23-member scientific Advisory Board representing seven countries; built a global community of more than 200 researchers and physicians worldwide; leveraged the community to establish and execute an international research agenda; and engaged patients throughout the entire process. We are currently finalizing plans to establish a global registry/natural history study, which we believe will be crucial for establishing diagnostic criteria and improving patient care. We also plan to launch viral discovery, serum proteomics, intracellular inflammatory pathway identification, and sequencing studies. We invite you to register on our website, attend our annual meeting that occurs during the AsH annual meeting, conduct research, contribute samples for research, and encourage your patients to enroll in our registry.
Dr. Van Rhee and Dr. Fajgenbaum indicated no relevant conflicts of interest.
1. Fajgenbaum DC, Van Rhee F, Nabel Cs. HHV-8-negative, idiopathic multicentric Castleman disease: novel insights into biology, pathogenesis, and therapy. Blood. 2014;123:2924-2933.
2. Chang KC, Wang YC, Hung LY, et al. Monoclonality and cytogenetic abnormalities in hyaline vascular Castleman disease. Mod Pathol. 2014;27:823-831.
3. Talat N, Belgaumkar AP, schulte KM. surgery in Castleman’s disease: a systematic review of 404 published cases. Ann surg. 2012;255:677-684.
4. Dupin N, Diss TL, Kellam P, et al. HHV-8 is associated with a plasmablastic variant of Castleman disease that is linked to HHV-8-positive plasmablastic lymphoma. Blood. 2000;95:1406-1412.
5. Dossier A, Meignin V, Fieschi C, et al. Human herpesvirus 8-related Castleman disease in the absence of HIV infection. Clin Infect Dis. 2013;56:833-842.
6. Gerard L, Michot JM, Burcheri s, et al. Rituximab decreases the risk of lymphoma in patients with hiv-associated multicentric Castleman disease. Blood. 2012;119:2228-2233.
7. Bower M. How I treat HIV-associated multicentric Castleman disease. Blood. 2010;116:4415-4421.
8. van Rhee F, stone K, szmania s, et al. Castleman disease in the 21st century: an update on diagnosis, assessment, and therapy. Clin Adv Hematol oncol. 2010;8:486-498.
9. Fajgenbaum DC, Liu A, Ruth J, et al. HHV-8-negative, idiopathic multicentric Castleman disease (iMCD): a description of clinical features and therapeutic options through a systematic literature review [abstr]. Blood. 2014;124:4861a.
10. Dispenzieri A, Armitage Jo, Loe MJ, et al. The clinical spectrum of Castleman’s disease. Am J Hematol. 2012;87:997-1002.
11. stone K, Woods e, szmania sM, et al. Interleukin-6 receptor polymorphism is prevalent in HIV-negative Castleman disease and is associated with increased soluble interleukin-6 receptor levels. PLos one. 2013;8:e54610.
12. Nishimoto N, Kanakura Y, Aozasa K, et al. Humanized anti-interleukin-6 receptor antibody treatment of multicentric Castleman disease. Blood. 2005;106:2627-2632.
13. van Rhee F, Wong Rs, Munshi N, et al. siltuximab for multicentric Castleman’s disease: a randomised, double-blind, placebo-controlled trial. Lancet oncol. 2014;15:966-974.
Q&A With Dr. Donald PagliaArtist, physician-scientist, and longtime ASH member Dr. Donald Paglia talks about both of his ongoing contributions to ASH – its famous logo and his annual donations to help further the careers of others.
Can you share a little about the history of asH’s logo?
The evolution of our logo has a long and “interesting” history. The Society had no logo until an early president asked an artist friend of his to create one. It was indeed a brilliant design: four circles in a diamond configuration with two opposing circles connected by a thready isthmus, as though pulling apart in cell division.
That initial design was adopted and used by ASH until my principal mentor, Dr. Eugene Cronkite, became President in 1971. During our annual meeting in San Francisco that year, I was on a year’s leave of absence from uCLA and painting intensively in preparation for my first solo art exhibition. I should have recognized then that the ASH logo displayed so prominently throughout the meeting venue was more than just a little familiar. In fact, it was identical to the trademark of a primary supplier of artists’ materials, displayed on virtually every tube of oil paint in my studio. When I pointed this out to Eugene, he immediately apologized to the supplier about the inadvertent transgression, and they viewed it as a “no-harm, no-foul” incident since ASH had terminated its usage. Fortunately, that was in a far less litigious time.
How did you become involved in the current logo design?
The current ASH logo resulted from an international competition organized under Dr. Frank Bunn’s leadership as ASH president. Proposals were submitted by the membership, and mine was eventually selected, but not without controversy. Some felt there might be too much resemblance to the classical yin yang symbol of Chinese philosophy and wanted to avoid any such philosophical, religious, or other connotations. Certainly, none was intended. The design evolved from my attempt to have every component of ASH membership graphically represented – a challenging goal for a group that was rapidly differentiating into multiple subspecialists.
What is the logo’s intended symbolism?
The paramount goals in logo design are symbolism and simplicity, not necessarily in that order. I chose the circle as a universal symbol that can mean whatever we choose it to mean. The left portion was meant to be a stylized droplet representing all those who are engaged, clinically or in research, with the fluid components of blood, such as transfusion medicine and coagulation. Progressively smaller circles within the negative space on the right represent those of us focused more specifically on white cells, red cells or platelets, respectively. A laurel branch surrogate at the bottom of the logo is not DNA as some interpret, but was intended to represent a generic protein molecule that progresses from intact on the left to fragmented on the right, symbolically extending through the clinical spectrum from normality and wellness to disorder and dyscrasias.
To this day, I remain honored that the pen-and-ink original hangs on a wall in the office of my friend, Frank Bunn, and that the Society continues to value it as representative of our organizational identity.
What is your strongest motivator for supporting asH programs?
I support ASH programs as one tangible means to acknowledge my indebtedness to others. My annual donations are designated to honor (or memorialize) the individuals to whom I owe so much, personally as well as professionally. I have been privileged to be taught and befriended by, to come under the guidance of, and to be inspired by so many who inhabit this pantheon of Hematology. The enormity of such debts can only be compensated by extending their legacies into the future. That is not an original concept, but, like the ASH logo, it still works for me.
Visit www.hematology.org/foundation to learn how you can support ASH programs.
2015 ASH Meeting on Hematologic MalignanciesJoin your colleagues in Chicago this September for the premier meeting on malignant hematology. The 2015 ASH Meeting on Hematologic Malignancies is your opportunity to hear top experts discuss the latest developments in clinical care and to get answers to your most challenging patient care questions.
At the heart of the program are numerous “How I Treat” sessions covering core malignancies, including leukemia, lymphoma, myelodysplastic syndromes, myeloma, and myeloproliferative neoplasms. These presentations focus sharply on evidence-based treatment approaches, ranging from standard of care to novel agents. The meeting will also spotlight peer-reviewed, clinical research. All submitted abstracts will be considered for presentation as posters, while authors of the top abstracts will be invited to present their research at an oral session.
The meeting will be held September 17-19, 2015, at the Fairmont Chicago. Be sure to save the date, and stay tuned for more information on registration, abstract submission, and program updates. Learn more on the website.
N e w S A N D R e P O R t S
Type of Castleman
Disease
Type of Lymphadenopathy
Pathology iL-6–Driven inflammatory
syndrome*
virologic status Treatment
unicentric Localized 90 percent hyaline vascular
Typically not • Negative for HHV-8 by QPCR or negative LANA-1 stain
Complete excision
Multicentric HHV-8–Positive
Generalized ± hepatosplenomegaly
Plasmacytic orplasmablastic
Yes • Positive for HHV-8 by QPCR
• May be positive for HIV
• Rituximab ± etoposide
• optional valganci-clovir maintenance
Multicentric HHV-8–Negative(Idiopathic)
Generalized ± hepatosplenomegaly
Mostly plasmacytic, but can be hyaline vascular or mixed cellularity
Yes, but variable clinical presenta-tion from mild to very severe
• Negative for HHV-8 by QPCR or Negative LANA-1 stain
• Negative for HIV
• Siltuximab
• Tocilizimab
• Rituximab
• Chemotherapy in severe cases
PH
oTo
Co
uR
TES
Y o
F LA
RR
Y R
. WA
GN
ER
, WA
GN
ER
PH
oTo
AR
T

6 The Hematologist: ASH NewS AND RePORtS
Iron homeostasis relies on a regulated network of systemic and cellular mechanisms for the acquisition, transportation and cellular utilization of the
metal.1 once in inner body fluids, iron is swiftly captured by a chemically shielded vehicle (transferrin) that circulates and safely delivers it to cells commensurate with their metabolic needs. In the cellular milieu, most of the iron is also protein-associated, either directly or via heme or iron-sulfur-cluster moieties. However, the biosynthesis of these groups depends to a large extent on the availability of a basal level of redox-active and mobilizable iron, which we define as labile cell iron (LCI), often also referred to as the labile iron pool.2 The obligatory maintenance of a physiological level of labile iron is not devoid of potential liabilities, as labile iron has the capacity to catalyze the conversion of natural reactive oxygen intermediates (RoIs) of the respiratory chain (e.g., o2
-·and H2o2) to noxious reactive oxygen species (Ros; e.g., oH·) that can damage proteins, lipids, and nucleic acids. This creates a continuous burden on cells to swiftly eliminate RoIs by enzymatic reactions (superoxide dismutase, peroxidases, and catalases) aided by reducing/antioxidant agents such as glutathione and the cellular reductants NADPH and NADH. Moreover, being devoid of extrusion tools to relieve themselves of iron, cells must cope with fluctuations in labile iron levels by balancing iron intake according to utilization, and also by producing the requisite amount of ferritin units to absorb “surplus” labile iron (Figure).
It is widely accepted that a disruption of links in systemic or cellular iron networks can lead to an aberrant buildup of cell iron, either due to excessive amounts of circulating iron in the plasma and/or by a mismatch in cell iron distribution. Cells endowed with limited iron shielding capacities and/or antioxidant power are the most susceptible to damage generated by iron accumulated in mitochondria, the primary site of RoI/Ros formation. This is classically demonstrated in cell and animal models of systemic iron overload disorders (IoDs) that recapitulate the clinical scenario of patients with primary or transfusional hemosiderosis. In that scenario, an outpouring of iron from gut or reticuloendothelial cells that is not matched locally by sufficient circulating apotransferrin not only leads to an upsurge in plasma iron, but also to the accumulation of forms of iron not bound to transferrin (NTBI†) .3-5 such forms can infiltrate cells opportunistically by resident transporters or channels, resulting in tissue iron overload and end-organ failure. Cellular siderosis with pathologic outcomes in single or multiple organs (brain, heart, endocrine glands), or hematopoietic cells are also found in the absence of plasma Io (e.g., Freidreich Ataxia; Figure). This regional type of siderosis generally results from abnormalities (genetic or acquired) in cell iron utilization6 that perpetuate metal and oxidative damage to the cell.2 However, in either systemic or regional siderosis, it is the labile iron pool that builds up in mitochondria and results in siderotic damage that, in some cases, can be prevented or significantly reduced by chelators that can gain access to the organelle.2
The etiopathologic features of siderosis described herein are of clinical importance because they determine to a large extent the guidelines for clinical assessment of hemosiderosis. Those guidelines rely presently on surrogate markers of liver iron storage such as serum ferritin (when not confounded by inflammation) and increasingly on measurements of organ-accumulated metal assessed by noninvasive multiorgan spectroscopy (T2 and T2* MRI) that detects signals associated with clusters of iron composed of ferritin and/or hemosiderin units.7,8 However, as these markers are essentially end-organ indicators of iron accumulation, but not the actual perpetrators of siderotic cell damage or the direct targets of chelators that neutralize labile iron, their detection might be out of phase with natural disease progression or with functional response to treatment. Could markers associated with upstream factors of impending iron overload, such as plasma NTBI or labile
Labile iron: Potential Toxicity in iron overload Disorders
Zvi ioav CaBanTCHiK, PhD,1 anD eLieZeR a. RaCHMiLeWiTZ, MD2
1. Professor emeritus, a&M Dellapergola Chair in Life sciences, Hebrew university of Jerusalem, edmond and Lilly safra Campus Givat Ram, Jerusalem, israel2. Professor emeritus of Medicine, Hadassah Medical school of the Hebrew university of Jerusalem; Hematology Department, edith Wolfson Medical Center, Holon, israel
plasma iron (LPI), or with downstream factors such as LCI changes in particular cell types, provide information of clinical value? such information could potentially be useful for early detection of iron overload and also for assessing the adequacy of a chelation regimen in continuously maintaining LPI-free plasma.
until recently, plasma NTBI and its chemically labile component LPI have been measured extensively in healthy individuals and in patients with congenital or acquired IoDs (e.g., thalassemia major and intermedia, sickle cell disease, myelodysplastic syndrome, bone marrow transplantation, chemotherapy, hemochromatosis, etc.),5,9-11 particularly during treatment. Briefly, those studies indicated that: 1) either NTBI or LPI is virtually undetectable in normal individuals and detectable in greater than 90 percent of patients with transferrin saturation (TsAT) greater than 70 to 75 percent; 2) administration of chelators such as deferrioxamine (DFo; intravenously), deferiprone (DFP; orally), or deferasirox (DFR; orally) can virtually eliminate LPI within minutes (DFo) or within one to two hours (DFo or DFR) and maintain it at basal levels (< 0.2 mM) for different time periods, depending on the dose and frequency of chelator administration (vis-á-vis its pharmacokinetics and the rate at which NTBI resurges in the plasma of a given patient); and 3) chelation regimens can attain daily coverage from LPI resurgence in most thalassemia intermedia patients treated with either DFP (25 mg/kg twice daily) or DFR (20 mg/kg once daily) and in 40 percent of thalassemia major patients treated thrice daily with DFP (total 75 mg/kg) or with DFR (40 mg/kg once daily), whereas combined treatment of daily DFP and nightly DFo can attain full-day coverage in greater than 95 percent of patients.9 A decisional algorithm to start iron chelation in thalassemia major patients has been proposed on the basis of threshold TsAT values which in poly-transfused patients are invariably accompanied by the presence of LPI.12
Although NTBI and LPI methodologies still need to be clinically validated and standardized for different IoDs, they have reached a stage where they can not only provide insights into the pathobiology of hemosiderosis, but can also serve as diagnostic tools for identifying the presence of potentially toxic species in plasma whose selective elimination is not only attainable but also recommended.
†Note: The three-decades-old term “plasma NTBI”3 has lately
M I N I R e V I e w
been amply recognized in the pathophysiology of systemic iron overload as a pathological component of plasma iron composed of chemical forms (not bound to transferrin) that can infiltrate cells and overload them with iron. The capturing of plasma NTBI by iron chelators and their elimination from circulation provides the basis for “iron overload” prevention in various IoDs. However, the intrinsically apophatic “NTBI” term should not be used for iatrogenic NTBI agents such as iron polymers used clinically for parenteral iron supplementation or iron chelates that are formed in vivo following chelation treatment.
Dr. Cabantchik and Dr. Rachmilewitz indicated no relevant conflicts of interest.
1. Ganz T. systemic iron homeostasis. Physiol Rev. 2014;93:1721-1741.
2. Cabantchik ZI. Labile iron in cells and body fluids: physiology, pathology, and pharmacology. Front Pharmacol. 2014;5:45.
3. Hershko C, Graham G, Bates GW, et al. Non-specific serum iron in thalassaemia: an abnormal serum iron fraction of potential toxicity. Br J Haematol. 1978;40:255-263.
4. Breuer W, Hershko C, Cabantchik ZI. The importance of non-transferrin bound iron in disorders of iron metabolism. Transfus sci. 2000;23:185-192.
5. Brissot P, Ropert M, Le Lan C, et al. Non-transferrin bound iron: a key role in iron overload and iron toxicity. Biochim Biophys Acta. 2012;1820:403-410.
6. Rouault TA. Iron metabolism in the CNs: implications for neurodegenerative diseases. Nat Rev Neurosci. 2013;14:551–564.
7. Detterich J, Noetzli L, Dorey F, et al. electrocardiographic consequences of cardiac iron overload in thalassemia major. Am J Hematol. 2012;87:139-144.
8. Baksi AJ, Pennell DJ. Randomised controlled trials of iron chelators for the treatment of cardiac siderosis in thalassaemia major. Pharmacology. 2014;5:2014.
9. Zanninelli G, Breuer W, Cabantchik ZI. Daily labile plasma iron as an indicator of chelator activity in thalassaemia major patients. Br J Haematol. 2009;147:744-751.
10. Hider RC, silva AM, Podinovskaia M, et al. Monitoring the efficiency of iron chelation therapy: the potential of nontransferrin-bound iron. Ann N Y Acad sci. 2010;1202:94-99.
11. Aydinok Y, evans P, Manz CY, et al. Timed non-transferrin bound iron determinations probe the origin of chelatable iron pools during deferiprone regimens and predict chelation response. Haematologica. 2012;97:835-841.
12. Danjou F, Cabantchik ZI, origa R, et al. A decisional algorithm to start iron chelation in patients with beta thalassemia. Haematologica. 2014;99:e38-e40.
Figure
The Hematologist: ASH NewS AND RePORtS 7
t H e H e M A t O L O G I S t A D V O C A t e
H E A D L I N E S F R O M Washington
President Announces Precision Medicine Initiative as Part of 2016 Budget Proposal; Continued Advocacy by Hematologists Needed to Protect Funding for NIH
Congressional leaders are in the midst of planning for the annual spending bills, including federal funding for the National Institutes of Health (NIH). The process
formally began with the Administration’s budget proposal, which was released on February 2.
Just prior to the release of his budget request, President obama announced a new Precision Medicine Initiative to “pioneer a new model of patient-powered research that promises to accelerate biomedical discoveries and provide clinicians with new tools, knowledge, and therapies to select which treatments will work best for which patients.” To launch the initiative, the President’s fiscal year 2016 (FY 2016) budget seeks to provide a $215 million investment for the NIH together with the u.s Food and Drug Administration (FDA) and the office of the National Coordinator for Health Information Technology (oNC) to support this effort, including:
• $130 million to NIH for development of a voluntary national research cohort of a million or more volunteers to propel our understanding of health and disease and set the foundation for a new way of doing research through engaged participants and open, responsible data sharing.
• $70 million to the National Cancer Institute (NCI), part of NIH, to scale up efforts to identify genomic drivers in cancer and apply that knowledge in the development of more effective approaches to cancer treatment.
• $10 million to the FDA to acquire additional expertise and advance the development of high-quality, curated databases to support the regulatory structure needed to advance innovation in precision medicine and protect public health.
• $5 million to the ONC to support the development of interoperability standards and requirements that address privacy and enable secure exchange of data across systems.
Although additional details of the FY 2016 proposal – including an overall funding level for NIH – were not yet known, the obama Administration had previously announced plans to provide a major spending boost for both domestic programs and the military, and to reverse the across-the-board budget limits currently in place.
It is important to remember that the President’s nonbinding budget proposal merely sets forth the Administration’s priorities and is just one step in a lengthy federal budget process. Absent a change in current law, the fiscal year spending measures, covering the 12-month period starting october 1, 2015, are restricted by the 2011 Budget Control Act, which limits federal discretionary spending through 2021. In the coming weeks, obama Administration representatives will be called to testify before Congress on the President’s proposals and the House and senate Appropriations Committees will begin drafting legislation establishing actual federal spending levels for FY 2016.
As the FY 2016 budget process continues, lawmakers need to understand the impact that unpredictable funding and potential funding cuts will have on research and patients, and the need for them to recognize the value of biomedical research by maintaining the investment in the NIH. Grassroots support is critical in order to have a voice in the congressional budget process to ensure that the NIH does not experience additional cuts in funding. Members of the AsH Committee on Government Affairs will be in Washington in March to meet with Members of Congress and advocate in support of increased funding for biomedical research, but the society needs the help of all of its members in continuing to focus attention on this and other issues of importance to hematology. Please look for AsH Legislative Alerts and visit the AsH website for updates on the FY 2016 budget process and for information about how you can contact your senators and representative to protect NIH funding in FY 2016.
For additional information on how to join the AsH Grassroots Network and participate in the society’s advocacy efforts, visit the AsH Advocacy Center at www.hematology.org/advocacy or contact AsH Legislative Advocacy Manager Tracy Roades at [email protected].
Congressional Leaders Unveil “21st Century Cures” Draft Proposal
In late January, House energy and Commerce Committee Chairman Fred upton (R-MI) unveiled a discussion draft of a long-awaited plan designed to accelerate
the discovery, development and delivery of promising new treatments and cures. The discussion document and accompanying summary and white paper culminate a year of hearings, roundtables, and white papers under an initiative that is designed to transform the clinical trials process and ultimately speed the pace of new medical cures and treatments. The discussion document covers a wide range of topics, from the regulation of drugs and devices and modernizing the clinical trials process, to data sharing, Medicare coverage of new technologies, and health information technology interoperability. The draft plan includes proposals for new advisory bodies and approval pathways but does not mention funding increases for agencies such as the NIH or FDA. Additional information on the entire initiative, including the full text of the draft proposal, may be found on the energy and Commerce Committee website at http://energycommerce.house.gov/cures.
In releasing the draft document, the energy and Commerce Committee said it will “continue on an aggressive schedule to introduce 21st Century Cures legislation and ultimately send a bill to President obama’s desk for signature by the end of the year.” senate Health, education, Labor, and Pensions Committee Chairman Lamar Alexander (R-TN) and senator Richard Burr (R-NC) have announced plans to pursue a similar effort in the senate.
AsH is in the process of reviewing the proposal and the potential impact on hematology. As always, AsH encourages comments from its members. If you have any questions or comments, please contact AsH Legislative Advocacy Manager Tracy Roades at [email protected].
ASH Comments on NIH Draft Policy Regarding Use of Single IRBs in Clinical Research
In January, AsH submitted comments on the NIH recent draft policy to promote the use of single institutional review boards (IRBs) in multi-site clinical research studies. AsH
agrees that all NIH-funded multisite studies carried out in the united states, whether supported through grants, contracts, or the NIH intramural program, should be able to use a single IRB. Doing so will help achieve greater efficiencies in the initiation of studies across NIH’s entire clinical research portfolio. exceptions to the policy would be allowed if local IRB review is necessary to meet the needs of specific populations or where it is required by federal, state, or tribal laws or regulations. The full text of the society’s comments may be found on the AsH website at www.hematology.org. AsH will continue to monitor the issue and inform members on how the policy will affect practicing hematologists.

8 The Hematologist: ASH NewS AND RePORtS8 The Hematologist: ASH NewS AND RePORtS
the FXI-ASo 200-mg group, and 3% in the FXI-ASo 300-mg group). There was only one major bleeding event (in the FXI-ASo 300-mg group). Injection site reactions occurred in 26 percent of patients in the FXI-ASo groups, but were generally mild and did not result in discontinuation of study drug.
Dr. Büller and colleagues provide valuable proof of concept that targeting FXI is a potentially effective and safe antithrombotic strategy. The clinical potential of FXI-ASo itself may be limited by relatively slow onset and offset of antithrombotic effect, need for subcutaneous administration, and frequent injection site reactions. Nevertheless, its promising performance in the present study engenders enthusiasm for development of alternative approaches to FXI inhibition, including small molecule and antibody inhibitors.
The study results also challenge two widely held “common sense” dogmas in coagulation. First, activation of the extrinsic pathway by tissue factor at the site of surgery has long been viewed as the predominant mechanism of postoperative VTE. The antithrombotic efficacy of FXI-ASo suggests that the intrinsic pathway has an important and previously underappreciated role in the pathophysiology of this disorder, perhaps through activation by DNA, RNA, and inorganic polyphosphates released from damaged cells (Figure). Second, antithrombotic therapy has traditionally been viewed as a double-edged sword – an inevitable trade-off between antithrombotic efficacy and bleeding risk. In keeping with preclinical data,1,2 FXI-ASo reduced thrombosis without increasing bleeding, although the study was not powered to detect differences in bleeding rates between treatment groups. Larger studies with patient-important outcomes will be needed to confirm whether targeting FXI can prevent clinically meaningful thrombosis while sparing hemostasis.
1. Tucker EI, Marzec uM, White TC, et al. Prevention of vascular graft occlusion and thrombus- associated thrombin generation by inhibition of factor XI. Blood. 2009;113:936-944.
2. Yau JW, Liao P, Fredenburgh JC, et al. Selective depletion of factor XI or factor XII with antisense oligonucleotides attenuates catheter thrombosis in rabbits. Blood. 2014;123:2102-2107.
3. Salomon o, Steinberg DM, Zucker M, et al. Patients with severe factor XI deficiency have a reduced incidence of deep-vein thrombosis. Thromb Haemost. 2011;105:269-273.
Factor Xi antisense: a Challenge to Common senseBüller HR, Bethune C, Bhanot s, et al. Factor Xi antisense oligonucleotide for prevention of venous thrombosis. n engl J Med. 2015;372:232-240.
aDaM CuKeR, MD, Ms
Dr. Cuker indicated no relevant conflicts of interest.
animal studies suggest that inhibition of factor XI (FXI) prevents thrombosis without disrupting hemostasis.1,2 Epidemiologic data indicate that patients with congenital FXI deficiency are protected from venous thromboembolism (VTE), even though their bleeding phenotype is variable and often quite mild.3 on the
basis of these observations, Dr. Harry Büller and colleagues hypothesized that targeting FXI may provide effective antithrombotic therapy without the bleeding risk associated with conventional anticoagulants. They used a FXI antisense oligonucleotide (FXI-ASo) to test this hypothesis. FXI-ASo binds FXI messenger RNA in hepatocytes (the site of FXI synthesis) with high specificity, targeting the messenger RNA (mRNA) for degradation before it can be translated to protein. FXI synthesis is thus curtailed, resulting in reduced plasma FXI levels (Figure).
In a randomized, open-label, phase II trial, the authors assigned 300 adults scheduled for elective unilateral total knee arthroplasty to daily subcutaneous enoxaparin 40 mg (n = 75) or subcutaneous FXI-ASo at a dose of 200 mg (n = 147) or 300 mg (n = 78). Because of its slow onset of action, FXI-ASo was initiated five weeks before surgery and given again at 33, 31, 28, 21, 14, and seven days before surgery, at six hours after surgery, and at three days after surgery. Enoxaparin was initiated either the evening before surgery or six to eight hours after surgery and continued through at least postoperative day 8. The primary efficacy outcome was VTE, defined as a composite of symptomatic VTE or silent deep vein thrombosis (DVT), identified by mandatory bilateral lower extremity venography between postoperative days 8 and 12. The principal safety outcome was major and clinically relevant non-major bleeding. An independent committee blinded to treatment assignment adjudicated all outcomes.
The treatment groups were well-balanced at study entry. Mean perioperative FXI levels were normal (0.93 u/mL) in the enoxaparin group and were reduced in a dose-dependent fashion in the 200-mg (0.38 u/mL) and 300-mg (0.20 u/mL) groups. The primary efficacy outcome occurred in 30 percent, 27 percent, and 4 percent of the treatment groups, respectively. The FXI-ASo 200-mg regimen was non-inferior to, and the 300-mg regimen was superior to enoxaparin for prevention of VTE. Most VTE events were silent below-the-knee DVTs; only three events (one in the enoxaparin group and two in the FXI-ASo 200-mg group) were symptomatic. The incidence of the principal safety outcome was not significantly different between the treatment groups (8% in the enoxaparin group, 3% in
effect of FXi-aso on the Coagulation system. FXi-aso (isis 416858) is a factor Xi (FXi)–targeted second-generation antisense oligonucleotide. Tissue damage after surgery exposes tissue factor and results in the release of DNA, RNA, and inorganic polyphosphate from damaged cells and from activated platelets and neutrophils. Tissue factor binds factor VIIa and initiates the extrinsic pathway of coagulation, whereas DNA, RNA, and polyphosphate activate factor XII and initiate the intrinsic pathway of coagulation. FXI–targeted antisense oligonucleotide attenuates the intrinsic pathway by binding to factor XI messenger RNA (mRNA) in the liver, which results in ribonuclease H1 (RNase H1) –mediated degradation of FXI messenger RNA, thereby preventing protein synthesis and reducing circulating FXI levels.
From The New England Journal of Medicine, Harry R. Büller, Claudette Bethune, Sanjay Bhanot, et al, Factor XI Antisense oligonucleotide for Prevention of Venous Thrombosis, Volume 372, Page 233 Copyright © 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.

The Hematologist: ASH NewS AND RePORtS 9
variation in Cancer Risk: nature, nurture, and Random ChanceTomasetti C, vogelstein B. Cancer etiology: variation in cancer risk among tissues can be explained by the number of stem cell divisions. science. 2015;347:78-81.
TRaCy i. GeoRGe, MD
Dr. George indicated no relevant conflicts of interest.
The Hematologist: ASH NewS AND RePORtS 9
Drs. Tomasetti and Vogelstein clustered different cancers into two types using an “extra risk score” (ERS), which was defined as the product of the total number of stem cell divisions and the lifetime risk for each cancer type (Figure 2, available online only). Tissue types with a high ERS were those with a high cancer risk relative to the number of stem-cell divisions. They found that high-ERS tumors were known to have hereditary risk factors or environmental links and designated such tumors as “deterministic [D-tumors]” given the strong effect that such factors had on the risk of tumor development. In contrast, low-ERS tumors were termed “replicative [R-tumors]” as their risk was mostly strongly affected by the stochastic process of stem-cell divisions with minimal known contributions by hereditary predisposition or environmental mutagens. The authors stressed that even for D-tumors such as familial adenomatous polyposis (FAP) related to inherited mutations in the APC tumor suppressor gene, “replicative effects are essential.” They noted that the rate of FAP colon cancers are 30-fold greater than that of FAP cancers of the duodenum, which they link to the 150-fold increased number of stem cell divisions in colonic versus duodenal tissue. The authors also cited the example of melanoma and basal cell carcinoma, which share the same carcinogenic exposure [and dose] of ultraviolet light. They proposed that the much greater frequency of basal cell cancers vs. melanoma relates to the higher number of divisions within skin epidermal basal cells compared with melanocytes.
The public health implications of such findings are controversial and attention grabbing. For example, does primary prevention even matter for replicative tumors? These data will certainly prompt a rethinking of the role for primary versus secondary prevention strategies based on D- versus R-tumor types and how resources should be optimally allocated to manage cancer risk. While these implications are debated, this new model of carcinogenesis is reshaping how we view the relative contributions of nature, nurture, and random chance.
While it is commonly understood that the environment and heredity contribute to the development of cancer, what if something else contributed to carcinogenesis? Johns Hopkins university School of Medicine researchers Dr. Cristian Tomasetti, from the Division of Biostatistics and Bioinformatics in
the department of oncology, and Dr. Bert Vogelstein, the Clayton Professor of oncology, Howard Hughes investigator, and co-director of the Ludwig Center for Cancer Genetics and Therapeutics, postulated that the stochastic effects associated with the cumulative number of divisions within stem cells of each organ contribute to the lifetime risk of cancer arising in that organ. From the literature they identified 31 tissue types from which the number of stem cells had been quantified. They then plotted the total stem cell divisions for each tissue during the average lifetime of a human (x axis) versus the lifetime risk for cancer of that same type using Surveillance, Epidemiology, and End Results (SEER) data on the y-axis (Figure). The results show a significant positive correlation (Spearman’s rho = 0.81; p < 3.5 × 10-8). This finding suggests that 65 percent of the variation in cancer risk among different tissue types is attributable to the total number of stem cell divisions. They postulate that the stochastic effects of DNA replication, not environmental or inherited factors, are the major contributor to human carcinogenesis.
Whether you call the stochastic process of stem cell divisions “random chance” or “bad luck” is controversial, but highly quotable. Multiple news publications misinterpreted the data from this article, stating incorrectly that two-thirds of cancers are due to random mutations. In fact, as the authors state, roughly two-thirds of the difference in the risk of cancer between different cancers is due to the number of tissue-specific stem cell divisions. This stochastic process of DNA replication in stem cells and its relationship to cancer implies that errors during DNA replication (somatic mutations) affect the risk for carcinogenesis.
Figure
stochastic (replicative) factors versus environmental and inherited factors: R-tumor versus D-tumor classification. The adjusted ERS (aERS) is indicated next to the name of each cancer type. R-tumors (green) have negative aERS and appear to be mainly due to stochastic effects associated with DNA replication of the tissues’ stem cells, whereas D-tumors (blue) have positive aERS. Importantly, although the aERS was calculated without any knowledge of the influence of environmental or inherited factors, tumors with high aERS proved to be precisely those known to be associated with these factors. From Tomasetti C, Vogelstein B. Cancer etiology: Variation in cancer risk among tissues can be explained by the number of stem cell divisions. Science. 2015;347:78-81.
Reprinted with permission from AAAS.

10 The Hematologist: ASH NewS AND RePORtS10 The Hematologist: ASH NewS AND RePORtS
ann LaCasCe, MD, Msc
Dr. LaCasce indicated no relevant conflicts of interest.
PeTeR JoHnson, MD
Dr. Johnson indicated no relevant conflicts of interest.
Memory Games in the Lymph node: The inflammatory origins of Follicular Lymphomasungalee s, Mamessier e, Morgado e, et al. Germinal center reentries of BCL2-overexpressing B cells drive follicular lymphoma progression. J Clin invest. 2014;124:5337-5351.
Follicular lymphoma (FL) is characterized by the apoptosis-suppressing overexpression of BCL2 protein in mature B cells, driven in most cases by the t(14;18)(q32;q21) translocation. FL usually follows an indolent course and may be preceded by a
slow accumulation of precursor cells in the lymph nodes and peripheral blood, so called follicular lymphoma in situ (FLIS) and follicular lymphoma-like cells (FLLC), respectively. The presence of the t(14;18) in apparently healthy individuals indicates that other molecular events are required for the development of lymphoma, but until now it has been difficult to map the process by which these precursor cells might progress to malignancy. This series of experiments from the group of Dr. Bertrand Nadel and Dr. Sandrine Roulland at the Aix-Marseille université in Marseille, France, builds upon their previous work on FLIS by using an elegant mouse model of early FL to track memory B cell behavior and relating this to human t(14;18) cells.
The model used in this study was the BCL2tracer mouse, which has a human BCL2 transgene that is only activated upon inversion during V(D)J recombination, creating a mosaic that mimics the sporadic occurrence of the t(14;18) translocation. These mice carry BCL2-rearranged cells at a low frequency, much as in the human condition, and a single round of immunization using sheep red blood cells did not substantially alter this. However, in the presence of long-term antigenic stimulation by repeated challenges over nine months, there was a marked accumulation of BCL2-rearranged cells in the memory and germinal center compartments, which expressed IgM on their surface. This finding was reproduced following adoptive transfer of transgenic B cells from chronically stimulated animals into wild-type mice, where they accumulated in germinal centers with features reminiscent of FLIS. This points to the re-circulation of memory B cells, with the BCL2-overexpressing clones having a survival advantage over normal B cells. The BCL2-rearranged cells were analyzed by exome sequencing, which showed a high frequency of mutations (G > A and C > T transitions) characteristic of activation-induced cytidine deaminase (AID) activity, a feature of germinal center processing.
Parallel studies in human subjects were carried out by testing healthy organ donors for the presence of t(14;18) cells in the blood, bone marrow, and spleen. They found that most of the t(14;18) cells resided in the lymphatic tissues or bone marrow, that they co-expressed BCL2 and BCL6, and that the translocated alleles showed somatic hypermutation and class switch recombination, all in keeping with an arrested germinal center–like phenotype. Analysis of the level of clonal divergence in these cells by fluctuation long-range polymerase chain reaction (to cover both the switch region and the BCL2/Jh junction) revealed an extraordinarily high level of intraclonal variation, with multiple subclones detected in different tissues by comparing somatic hypermutation and class switch events. This level of variation is not seen in normal memory B cells, reinforcing the idea that t(14;18) cells enjoy a survival advantage that leads to their repeated passage through germinal center reactions, accumulating mutations that predispose them to malignant transformation.
This study fits with other work1 examining the effect of repeated immune stimulation on B-cell dynamics, which has shown that IgM+ memory cells can re-enter germinal centers, possibly as a means of evolving and updating the repertoire of responses. This normal process may be subject to a takeover by long-lived and maturation-arrested t(14;18)–bearing cells, allowing the accumulation of highly mutated cells with a high risk of further transformative events. This would suggest that recurrent or chronic immune stimulation could provide an important predisposing factor for FL. It also highlights the role of AID activity in driving intraclonal variation, and another recent article2 highlighted the poor prognostic implications of mutations within the BCL2 coding region.
1. Dogan I, Bertocci B, Vilmont V, et al. Multiple layers of B cell memory with different effector functions. Nat Immunol. 2009;10:1292-1299.
2. Correia C, Schneider PA, Dai H, et al. BCL2 mutations are associated with increased risk of transformation and shortened survival in follicular lymphoma. Blood. 2015;125:658-667.
PD-1 inhibition and Hodgkin Lymphoma: a Perfect Therapeutic Match
ansell sM, Lesokhin aM, Borrello i, et al. PD-1 blockade with nivolumab in relapsed or refractory Hodgkin’s lymphoma. n engl J Med. 2015;372:311-319.
although the majority of patients with Hodgkin lymphoma (HL) are cured with up-front therapy, the long-term outcome of patients who relapse after autologous stem cell transplantation is poor, despite the availability of brentuximab vedotin (BV). Advances in the understanding of the molecular pathogenesis of HL have led to novel therapeutic
targets. Reed-Sternberg (RS) cells are surrounded by an environment rich in inflammatory cells, including lymphocytes, which are not only ineffective in mounting an immune response against the RS cells but also support their growth and survival. Recent studies have identified amplification of chromosome segment 9p, which contains the genes that encode for the programmed death 1 and 2 ligands (PDL1 and PDL2), as the most common genetic aberration in RS cells in the nodular sclerosis subtype of classical HL.The JAK2 gene is also found on chromosome 9p, and increased JAK-STAT signaling results in further up-regulation of PD-1 ligands. PDL1 and PDL2 bind to PD-1 found on T cells, leading to inhibition of activation and proliferation (Figure).
Nivolumab, a humanized IgG4 monoclonal antibody directed against PD-1, has been studied in numerous solid malignancies, including melanoma, with promising activity. Given the strong rationale for its possible efficacy in HL, an expansion cohort of HL patients was included in the phase I study. Patients received 3 mg/kg of nivolumab on week 1 and 4, then every two weeks until complete remission, progression, or a maximum of two years. Twenty-three patients were treated, of whom 18 underwent prior autologous stem cell transplantation. Eighteen previously received BV, and 15 received both. All treated patients had a decrease in disease burden, and the overall response rate was 87 percent, consisting of partial and complete response rates of 17 percent and 70 percent, respectively. Among patients who underwent stem cell transplantation and received BV, 87 percent achieved an objective response with 80 percent partial remissions. All three patients who received BV but were transplant naïve achieved a partial remission. The progression-free survival at 24 weeks for all patients was remarkable at 86 percent, and the median overall survival has not yet been reached. In terms of toxicity, the most common adverse events were rash and thrombocytopenia. Twenty-two percent of patients developed grade 3 adverse events, including immune-mediated toxicities of pneumonitis, pancreatitis, and colitis. There were no grade 4 or 5 adverse effects.
Accompanying correlative studies investigated the expression of programmed death ligands. using FISH assays in 10 available patient samples, three to 15 copies of PDL1 and PDL2 were identified and occurred as a result of amplification, copy number gains, or polysomy of chromosome 9p. In addition, RS cells stained positive for nuclear phospho-STAT3, reflecting active JAK-STAT signaling.
Immune checkpoint blockade through the inhibition of PD-1 represents a rational therapeutic approach in HL, with activity in heavily pretreated patients. Further investigation is necessary to determine the durability of responses and immune-related toxicities in this patient population. Additional evaluation of this approach in histologic subtypes other than nodular sclerosis and in EBV-associated HL is also warranted. Moving forward, combining PD-1 inhibitors with BV, as well as other novel agents, holds the promise of highly effective treatment without the use of combination chemotherapy.
Cell survival &proliferation Lys9
Activechromatin
JMJD2C
IL-4R
Tyr41P
Jak2
PD-L2PD-L1
Lys9
Jak2JMJD2C
Repressivechromatin
P
Chromo-shadowdomain
HP1αChromodomain
MeTyr41
IL-13
IL-1
3RA
1γ
9p24amplification
PD-L2PD-L1
IL-4
R
Jak2
PD-L
1
PD-L
2
Myc
T cell blockadevia PD-1
Nucleus
c
Reprinted by permission from Macmillan Publishers Ltd: Nature Immunology. Rui L, Schmitz R, Ceribelli M, et al. Malignant pirates of the immune system. 12:933-940, copyright 2011.
Model for the Pathogenesis of PMBL and Hodgkin LymphomaFigure

The Hematologist: ASH NewS AND RePORtS 11The Hematologist: ASH NewS AND RePORtS 11
DaviD GaRCia, MD
Dr. Garcia indicated no relevant conflicts of interest.
anDReW J. yee, MD, anD nooPuR s. RaJe, MD
Dr. yee and Dr. Raje indicated no relevant conflicts of interest.
More evidence supporting a Conservative approach to Red Blood Cell TransfusionHolst LB, Haase n, Wetterslev J, et al. Lower versus higher hemoglobin threshold for transfusion in septic shock. n engl J Med. 2014;371:1381-1391.
although the Transfusion Requirements in Critical Care (TRICC) trial1 showed the benefits of a conservative transfusion strategy more than 15 years ago, many physicians remain skeptical about the safety of lower
hemoglobin thresholds for red cell transfusion in critically ill patients. In particular, evidence from at least some clinical studies2,3 has suggested that higher hemoglobin targets may be advantageous for patients with septic shock.
To better define the benefits and risks of different hemoglobin thresholds for red blood cell (RBC) transfusion, Dr. Lars Holst and colleagues conducted a multicenter, parallel-group trial that randomized intensive care unit (ICu) patients with septic shock to receive one unit of leukoreduced red cells either at a hemo-globin concentration of 9 g/dL or less (higher threshold) or at a hemoglobin concentration of 7 g/dL or less (lower threshold). The primary outcome measure was death at 90 days.
The Transfusion Requirements in Septic Shock (TRISS) trial was conducted at 32 sites in Denmark, Sweden, Norway, and Finland between December 2011 and December 2013. Randomization was stratified by study site and by the presence or absence of active hematologic cancer. More than 85 percent of screened patients were randomized; the most common reason for exclusion was prior transfusion of RBCs. of 1,005 patients who underwent randomization, 998 (99.3%) were included in the primary outcome (mortality) analysis. The baseline clinical characteristics of the two groups were similar, including age (median age, 67 years for both groups) and severity of illness scores. Although approximately 14 percent of patients in each group had chronic cardiovascular disease, patients with acute myocardial infarction were excluded. The median number of RBC units received was less in the lower threshold group (one unit vs. four units).
Ninety days after study entry, overall mortality was 43 percent in the lower-threshold group, and 45 percent in the higher-threshold group (relative risk, 0.94; 95% CI, 0.78 to 1.09; p=0.44). Neither adjustment for baseline risk factors nor per-protocol analyses altered the findings. Secondary outcome measures included the use of life support at days 5, 14, and 28 after randomization; serious adverse reactions (including transfusion-related acute lung injury and transfusion-associated circulatory overload) while in the ICu; and cerebral, myocardial, limb, or intestinal ischemic events while in the ICu. No statistically significant difference between treatment groups was observed for any of these secondary endpoints.
The TRISS investigators and study sites deserve credit for a very well designed and highly successful study of persons with septic shock (but no evidence of acute myocardial infarction). Recruiting patients with critical illness is difficult, and the high enrollment rate among eligible individuals is impressive. In addition to highlighting the very grave prognosis associated with septic shock, the TRISS trial has identified yet another patient population in which lower hemoglobin concentrations should be tolerated. Patients randomized to higher hemoglobin thresholds fared no worse than the patients in the intervention group, but they were exposed to more than twice the number of RBC units and did not experience a risk reduction for any of the reported outcomes (primary or secondary). Considering the previous high-quality evidence4 favoring more conservative transfusion thresholds, the TRISS trial shows that clinicians should think carefully before recommending hemoglobin thresholds higher than 7 g/dL in patients with septic shock.
1. Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care: Transfusion requirements in critical care investigators, Canadian Critical Care Trials Group. N Engl J Med. 1999;340:409-417.
2. Park DW, Chun BC, Kwon SS, et al. Red blood cell transfusions are associated with lower mortality in patients with severe sepsis and septic shock: a propensity-matched analysis*. Crit Care Med. 2012;40:3140-3145.
3. Vincent JL, Sakr Y, Sprung C, et al. Are blood transfusions associated with greater mortality rates? Results of the Sepsis occurrence in Acutely Ill Patients study. Anesthesiology. 2008;108:31-39.
4. Carson JL, Carless PA, Hebert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012;10:CD002042.
Transitioning to an “all oral Therapy” for Multiple Myeloma with the novel Proteasome inhibitor ixazomib
Kumar sK, Berdeja JG, niesvizky R, et al. safety and tolerability of ixazomib, an oral proteasome inhibitor, in combination with lenalidomide and dexamethasone in patients with previously untreated multiple myeloma: an open-label phase 1/2 study. Lancet oncol. 2014;15:1503-1512.
since their introduction more than 10 years ago, proteasome inhibitors (PI) such as bortezomib and, more recently carfilzomib, have emerged as a mainstay of treatment in multiple myeloma (MM).1 Bortezomib has been one of the driving forces behind the remarkable continued improvements in survival in MM.2 Its importance has been demonstrated in all aspects of MM care, from the relapsed and refractory setting
to upfront treatment, either as part of induction therapy prior to autologous stem cell transplantation or as part of the treatment in patients who are not eligible for high-dose therapy. However, one of the significant limiting toxicities of bortezomib appreciated during its initial use has been peripheral neuropathy, though this has been largely mitigated through weekly dosing and subcutaneous administration.3
Ixazomib (previously known as MLN9708) is a new oral PI with promising preclinical data showing superior pharmacodynamics and antitumor activity compared with bortezomib.4 Proteasome inhibitors, when given in combination with immunomodulatory drugs (IMiDs) such as lenalidomide as RVD (lenalidomide, dexamethasone, and bortezomib)5 or cyclophosphamide as VCD (bortezomib, cyclophosphamide, and dexamethasone),6 have been extremely effective in producing deep responses with excellent tolerability, and these regimens are standard treatment for newly diagnosed patients who are eligible for high-dose therapy.
The phase I/II study by Dr. Shaji Kumar and colleagues evaluates the use of ixazomib as the PI in this triplet combination with lenalidomide and dexamethasone in newly diagnosed patients. In this trial, patients received induction treatment according to a conventional 28-day schedule of lenalidomide 25 mg on days 1 to 21 and dexamethasone 40 mg weekly with ixazomib orally on days 1, 8, 15. After 12 cycles, patients continued ixazomib as maintenance. Stem cell collection and high-dose melphalan and autologous stem cell transplantation were permitted. The study enrolled 65 patients (15 patients in phase I; 50 patients in phase II).
This all-oral triplet combination was well tolerated, and the adverse event profile, including rates of neutropenia and thrombocytopenia, was typical of other triplet combinations. Importantly, the rate of grade ≥ 3 peripheral neuropathy was low at 6 percent, though it was comparable to rates observed when bortezomib is administered subcutaneously instead of intravenously. A notable adverse event of this regimen was skin rash in 55 percent of patients, which was grade ≥ 3 in 17 percent. While rash is common with lenalidomide-based regimens, grade ≥ 3 skin-related events are rare, and this was the most common reason for dose reduction in this trial. By comparison, when ixazomib is given weekly as a single agent in patients with relapsed disease, the rate of grade ≥ 3 rash was less (3%).7 The significance of rash with ixazomib and how it may be potentiated in other MM drug combinations remains to be seen. With a median follow-up of 14.3 months, this regimen was active, similar to RVD, with an overall response rate of 92 percent and a very good partial response rate or better of 58 percent.
Treatment paradigms for multiple myeloma are moving toward extended courses of treatment, in both the upfront and in the relapsed setting. These shifts are motivated by the findings in the FIRST trial,8 which found improved progression-free survival with treatment to progression with lenalidomide-dexamethasone, and in maintenance therapy with lenalidomide after transplantation.9 For the older patient population, modifications in schedule and dosing (for example, RVD-lite), have allowed the benefits of triplet combination to reach this group which traditionally has been more challenging to treat.10 Recently, the ASPIRE trial showed unprecedented activity for the combination of carfilzomib with lenalidomide and dexamethasone in relapsed and refractory patients, reaffirming the role of combining a PI and an IMiD.11 The availability of an oral, active, well-tolerated PI is thus an important and welcome advance for the MM community. Bortezomib and carfilzomib require weekly or twice weekly visits for treatment, and their prolonged schedules of treatment are a major time commitment for patients and their caretakers. As shown in the study by Dr. Kumar and colleagues, ixazomib has a favorable toxicity profile and is effective, and its long half-life affords a convenient weekly schedule. Another oral PI, oprozomib, is also in clinical trials.12 An oral PI will significantly enhance accessibility and the feasibility of optimal treatment strategies, especially for older patients. We await future trials to determine the best drugs to partner with ixazomib, as well as sequencing and maintenance approaches, and finally, studies of oprozomib and other oral PIs.
1. Moreau P, Richardson PG, Cavo M, et al. Proteasome inhibitors in multiple myeloma: ten years later. Blood. 2012;120:947-959.
2. Kumar SK, Dispenzieri A, Lacy MQ, et al. Continued improvement in survival in multiple myeloma: changes in early mortality and outcomes in older patients. Leukemia 2014;28:1122-1128.
3. Moreau P, Pylypenko H, Grosicki S, et al. Subcutaneous versus intravenous administration of bortezomib in patients with relapsed multiple myeloma: a randomised, phase 3, non-inferiority study. Lancet oncol. 2011;12:431-40.
4. Kupperman E, Lee EC, Cao Y, et al. Evaluation of the proteasome inhibitor MLN9708 in preclinical models of human cancer. Cancer Res. 2010;70:1970-1980.
5. Richardson PG, Weller E, Lonial S, et al. Lenalidomide, bortezomib, and dexamethasone combination therapy in patients with newly diagnosed multiple myeloma. Blood. 2010;116:679-686.
6. Kumar S, Flinn I, Richardson PG, et al. Randomized, multicenter, phase 2 study (EVoLuTIoN) of combinations of bortezomib, dexamethasone, cyclophosphamide, and lenalidomide in previously untreated multiple myeloma. Blood. 2012;119:4375-4382.
7. Kumar SK, Bensinger WI, Zimmerman TM, et al. Phase 1 study of weekly dosing with the investigational oral proteasome inhibitor ixazomib in relapsed/refractory multiple myeloma. Blood. 2014;124:1047-1055.
8. Benboubker L, Dimopoulos MA, Dispenzieri A, et al. Lenalidomide and dexamethasone in transplant-ineligible patients with myeloma. N Engl J Med. 2014;371:906-917.
9. McCarthy PL, owzar K, Hofmeister CC, et al. Lenalidomide after stem-cell transplantation for multiple myeloma. N Engl J Med. 2012;366:1770-1781.
10. o’Donnell E, Laubach JP, Yee AJ, et al. A phase II study of modified lenalidomide, bortezomib, and dexamethasone (RVD lite) for transplant-ineligible patients with newly diagnosed multiple myeloma [abstract]. Blood. 2014:124:abstr 3454.
11. Stewart AK, Rajkumar SV, Dimopoulos MA, et al. Carfilzomib, lenalidomide, and dexamethasone for relapsed multiple myeloma. N Engl J Med. 2015;372:142-152.
12. Vij R, Savona M, Siegel DS, et al. Clinical profile of single-agent oprozomib in patients (pts) with multiple myeloma (MM): updated results from a multicenter, open-label, dose escalation phase 1b/2 study [abstract]. Blood. 2014:abstr 34.
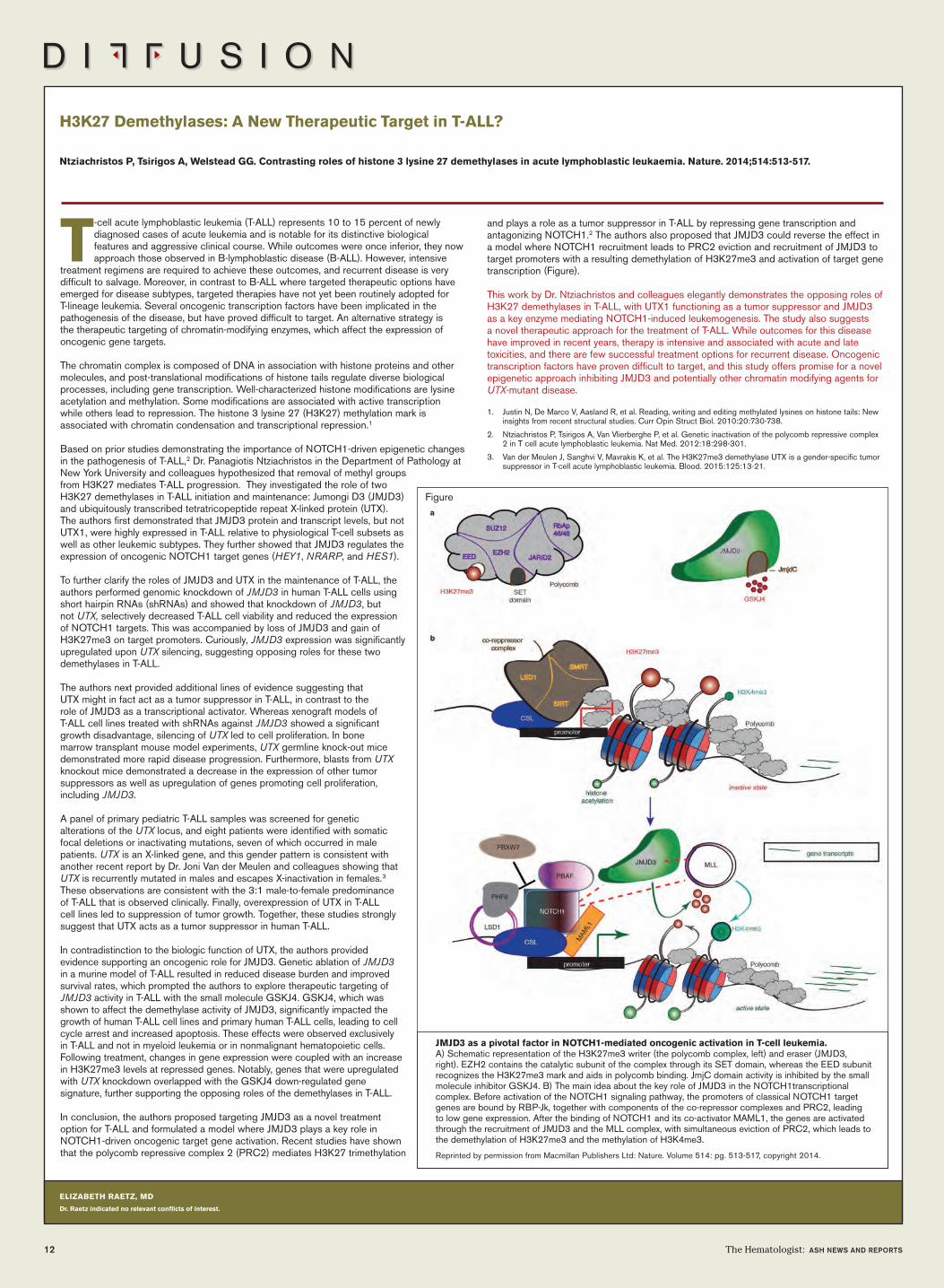
eLiZaBeTH RaeTZ, MD
Dr. Raetz indicated no relevant conflicts of interest.
T-cell acute lymphoblastic leukemia (T-ALL) represents 10 to 15 percent of newly diagnosed cases of acute leukemia and is notable for its distinctive biological features and aggressive clinical course. While outcomes were once inferior, they now approach those observed in B-lymphoblastic disease (B-ALL). However, intensive
treatment regimens are required to achieve these outcomes, and recurrent disease is very difficult to salvage. Moreover, in contrast to B-ALL where targeted therapeutic options have emerged for disease subtypes, targeted therapies have not yet been routinely adopted for T-lineage leukemia. Several oncogenic transcription factors have been implicated in the pathogenesis of the disease, but have proved difficult to target. An alternative strategy is the therapeutic targeting of chromatin-modifying enzymes, which affect the expression of oncogenic gene targets.
The chromatin complex is composed of DNA in association with histone proteins and other molecules, and post-translational modifications of histone tails regulate diverse biological processes, including gene transcription. Well-characterized histone modifications are lysine acetylation and methylation. Some modifications are associated with active transcription while others lead to repression. The histone 3 lysine 27 (H3K27) methylation mark is associated with chromatin condensation and transcriptional repression.1
Based on prior studies demonstrating the importance of NoTCH1-driven epigenetic changes in the pathogenesis of T-ALL,2 Dr. Panagiotis Ntziachristos in the Department of Pathology at New York university and colleagues hypothesized that removal of methyl groups from H3K27 mediates T-ALL progression. They investigated the role of two H3K27 demethylases in T-ALL initiation and maintenance: Jumongi D3 (JMJD3) and ubiquitously transcribed tetratricopeptide repeat X-linked protein (uTX). The authors first demonstrated that JMJD3 protein and transcript levels, but not uTX1, were highly expressed in T-ALL relative to physiological T-cell subsets as well as other leukemic subtypes. They further showed that JMJD3 regulates the expression of oncogenic NoTCH1 target genes (HEY1, NRARP, and HES1).
To further clarify the roles of JMJD3 and uTX in the maintenance of T-ALL, the authors performed genomic knockdown of JMJD3 in human T-ALL cells using short hairpin RNAs (shRNAs) and showed that knockdown of JMJD3, but not UTX, selectively decreased T-ALL cell viability and reduced the expression of NoTCH1 targets. This was accompanied by loss of JMJD3 and gain of H3K27me3 on target promoters. Curiously, JMJD3 expression was significantly upregulated upon UTX silencing, suggesting opposing roles for these two demethylases in T-ALL.
The authors next provided additional lines of evidence suggesting that uTX might in fact act as a tumor suppressor in T-ALL, in contrast to the role of JMJD3 as a transcriptional activator. Whereas xenograft models of T-ALL cell lines treated with shRNAs against JMJD3 showed a significant growth disadvantage, silencing of UTX led to cell proliferation. In bone marrow transplant mouse model experiments, UTX germline knock-out mice demonstrated more rapid disease progression. Furthermore, blasts from UTX knockout mice demonstrated a decrease in the expression of other tumor suppressors as well as upregulation of genes promoting cell proliferation, including JMJD3.
A panel of primary pediatric T-ALL samples was screened for genetic alterations of the UTX locus, and eight patients were identified with somatic focal deletions or inactivating mutations, seven of which occurred in male patients. UTX is an X-linked gene, and this gender pattern is consistent with another recent report by Dr. Joni Van der Meulen and colleagues showing that UTX is recurrently mutated in males and escapes X-inactivation in females.3 These observations are consistent with the 3:1 male-to-female predominance of T-ALL that is observed clinically. Finally, overexpression of uTX in T-ALL cell lines led to suppression of tumor growth. Together, these studies strongly suggest that uTX acts as a tumor suppressor in human T-ALL.
In contradistinction to the biologic function of uTX, the authors provided evidence supporting an oncogenic role for JMJD3. Genetic ablation of JMJD3 in a murine model of T-ALL resulted in reduced disease burden and improved survival rates, which prompted the authors to explore therapeutic targeting of JMJD3 activity in T-ALL with the small molecule GSKJ4. GSKJ4, which was shown to affect the demethylase activity of JMJD3, significantly impacted the growth of human T-ALL cell lines and primary human T-ALL cells, leading to cell cycle arrest and increased apoptosis. These effects were observed exclusively in T-ALL and not in myeloid leukemia or in nonmalignant hematopoietic cells. Following treatment, changes in gene expression were coupled with an increase in H3K27me3 levels at repressed genes. Notably, genes that were upregulated with UTX knockdown overlapped with the GSKJ4 down-regulated gene signature, further supporting the opposing roles of the demethylases in T-ALL.
In conclusion, the authors proposed targeting JMJD3 as a novel treatment option for T-ALL and formulated a model where JMJD3 plays a key role in NoTCH1-driven oncogenic target gene activation. Recent studies have shown that the polycomb repressive complex 2 (PRC2) mediates H3K27 trimethylation
12 The Hematologist: ASH NewS AND RePORtS
and plays a role as a tumor suppressor in T-ALL by repressing gene transcription and antagonizing NoTCH1.2 The authors also proposed that JMJD3 could reverse the effect in a model where NoTCH1 recruitment leads to PRC2 eviction and recruitment of JMJD3 to target promoters with a resulting demethylation of H3K27me3 and activation of target gene transcription (Figure).
This work by Dr. Ntziachristos and colleagues elegantly demonstrates the opposing roles of H3K27 demethylases in T-ALL, with uTX1 functioning as a tumor suppressor and JMJD3 as a key enzyme mediating NoTCH1-induced leukemogenesis. The study also suggests a novel therapeutic approach for the treatment of T-ALL. While outcomes for this disease have improved in recent years, therapy is intensive and associated with acute and late toxicities, and there are few successful treatment options for recurrent disease. oncogenic transcription factors have proven difficult to target, and this study offers promise for a novel epigenetic approach inhibiting JMJD3 and potentially other chromatin modifying agents for UTX-mutant disease.
1. Justin N, De Marco V, Aasland R, et al. Reading, writing and editing methylated lysines on histone tails: New insights from recent structural studies. Curr opin Struct Biol. 2010:20:730-738.
2. Ntziachristos P, Tsirigos A, Van Vlierberghe P, et al. Genetic inactivation of the polycomb repressive complex 2 in T cell acute lymphoblastic leukemia. Nat Med. 2012:18:298-301.
3. Van der Meulen J, Sanghvi V, Mavrakis K, et al. The H3K27me3 demethylase uTX is a gender-specific tumor suppressor in T-cell acute lymphoblastic leukemia. Blood. 2015:125:13-21.
H3K27 Demethylases: a new Therapeutic Target in T-aLL?
ntziachristos P, Tsirigos a, Welstead GG. Contrasting roles of histone 3 lysine 27 demethylases in acute lymphoblastic leukaemia. nature. 2014;514:513-517.
JMJD3 as a pivotal factor in noTCH1-mediated oncogenic activation in T-cell leukemia. A) Schematic representation of the H3K27me3 writer (the polycomb complex, left) and eraser (JMJD3, right). EZH2 contains the catalytic subunit of the complex through its SET domain, whereas the EED subunit recognizes the H3K27me3 mark and aids in polycomb binding. JmjC domain activity is inhibited by the small molecule inhibitor GSKJ4. B) The main idea about the key role of JMJD3 in the NoTCH1transcriptional complex. Before activation of the NoTCH1 signaling pathway, the promoters of classical NoTCH1 target genes are bound by RBP-Jk, together with components of the co-repressor complexes and PRC2, leading to low gene expression. After the binding of NoTCH1 and its co-activator MAML1, the genes are activated through the recruitment of JMJD3 and the MLL complex, with simultaneous eviction of PRC2, which leads to the demethylation of H3K27me3 and the methylation of H3K4me3.
Reprinted by permission from Macmillan Publishers Ltd: Nature. Volume 514: pg. 513-517, copyright 2014.
Figure

The Hematologist: ASH NewS AND RePORtS 13
THeResa CoeTZeR, PhD
Dr. Coetzer indicated no relevant conflicts of interest.
PaMeLa s. BeCKeR, MD, PhD
Dr. Becker indicated no relevant conflicts of interest.
a novel Gene Therapy strategy Provides Hope for HemophiliaBarzel a, Paulk nK, shi y, et al. Promoterless gene targeting without nucleases ameliorates haemophilia B in mice. nature. 2015;517:360-364.
Recent technological advances in genome engineering have facilitated targeted stable transgene expression for gene therapy applications. In particular, site-specific endonucleases are efficient agents for
targeted gene editing, whereby the endonuclease gene is typically delivered into cells by viral vectors and expressed under control of a vector-borne promoter. Recombinant adeno-associated virus (rAAV) vectors are commonly used in human clinical trials since they are derived from a nonpathogenic virus, are not immunogenic, and allow high gene-targeting rates. The rAAV can exist as several different serotypes, which differ in the composition of their capsid protein coat and are thus able to transduce various cell types.
However, despite promising results, adverse effects such as off-target endonuclease cleavage events, as well as activation of neighboring genes (including oncogenes) by the integrated vector-borne promoter, remain a major concern.
Dr. Adi Barzel and colleagues at Stanford in California have circumvented these issues with a novel approach using a promoterless, endonuclease-independent rAAV for gene targeting. As proof of concept, they used hemophilia B mice and targeted the human coagulation factor IX (F9) to the albumin gene locus, which is highly expressed in the liver, and demonstrated amelioration of the bleeding diathesis. They used the liver-tropic rAAV8 serotype and an innovative experimental strategy. The vector was engineered by inserting 5’ and 3’ homology arms spanning the stop codon of the mouse albumin (Alb) gene. A codon-optimized human F9 cDNA without the gene promoter, preceded by a 2A-peptide coding sequence, was then inserted in between the arms. Homologous recombination resulted in integration of the 2A-F9 coding sequence immediately 5’ of the Alb stop codon. This created a fused gene under control of the strong albumin promoter, which compensated for the lack of the F9 promoter. Transcription resulted in a fused mRNA coding for a polyprotein composed of albumin, 2A peptide and F9. Since 2A peptides are self-processing peptides derived from RNA viruses, inclusion of the 2A peptide is a critical component of these researchers’ ingenious strategy. During translation, the 2A peptide impairs normal peptide bond formation using a ribosomal skipping mechanism, which allows multiple proteins to be produced from a single vector. This process adds approximately 20 amino acids to the C terminus of albumin, which is the first translated protein, but this does not diminish its function. The F9 protein gains a single proline at the amino terminus, which does not adversely affect its processing in the endoplasmic reticulum and subsequent secretion. This strategy therefore does not disrupt the robust expression of hepatic albumin and results in stoichiometric expression of the F9 protein.
The engineered rAAV8-F9 vector was injected into neonatal and adult hemophilia B mice and plasma F9 levels between 7 and 20 percent of normal were achieved, which remained stable for up to 20 weeks. The treated mice also had normal coagulation times. The researchers demonstrated that F9 protein was only produced from on-target integration, since a vector-borne promoter was absent. Integration only occurred in about 0.5 percent of the hepatic albumin alleles; however, since the Alb locus has high transcriptional activity and 2A ribosome skipping was highly efficient, therapeutic levels of F9 clotting factor were achieved. using an inverse control vector, they found no evidence of off-target events, and no liver toxicity was observed. Apart from this favorable safety profile, another advantage of their strategy is that due to targeted vector integration, there should not be a loss of expression of the transgene over time, even in dividing tissues.
For the reasons outlined here, this exciting new gene therapy strategy should be a prime candidate for clinical assessment in the context of hemophilia and other inherited enzyme deficiencies, where long-term stable expression of relatively low levels of a therapeutic protein can ameliorate disease symptoms.
The origin of Therapy-Related aML Lies Deep Within
Wong Tn, Ramsingh G, young aL, et al. Role of TP53 mutations in the origin and evolution of therapy-related acute myeloid leukaemia. nature. doi: 10.1038/nature13968
it is indeed tragic that the consequence of the initial, potentially curative therapy of cancer can be a second, rapidly progressive fatal condition, therapy-related myelodysplastic syndrome (t-MDS), and/or acute myeloid leukemia (t-AML). t-MDS and t-AML are difficult to manage – from a psychological standpoint, as patients are now devastated by an aggressive additional malignancy after what may have
been a long course of prior surgery, radiation, and/or chemotherapy; and from a therapy standpoint, as there are typically poor outcomes due to chemotherapy drug resistance. The highest rates of t-MDS/AML are observed after treatment of breast cancer or lymphoma. It has been assumed that because of chemotherapy- and radiation-induced DNA damage, t-MDS/AML patients would exhibit many more mutations compared to de novo AML, and perhaps more novel mutations as well. The most common mutated gene in t-MDS/AML is the TP53 (tumor protein p53) tumor suppressor gene.
Dr. Terrence Wong, Dr. Giridharan Ramsingh, and Dr. Andrew Young and colleagues at Washington university in St. Louis have debunked prior theory on the origin of therapy-related hematopoietic disorders after performing whole genome sequencing of 22 cases of t-AML. They observed a similar rate of all types of mutations (single-nucleotide variants, small insertions or deletions [indels], and transversions [substitution of purine for pyrimidine or vice versa]) for t-AML patients compared to de novo AML, or secondary (from MDS) AML patients. There were an average of 10.2 ± 7.1 missense, nonsense, in-frame indel, or frameshift mutations per t-AML genome. Abnormalities of chromosomes 5 or 7 or complex cytogenetics were observed in 55 percent of the cases. The comparison de novo data were derived from 199 AML genomes or exomes,1 or 150 de novo MDS cases with extensive sequencing of candidate genes.2,3 For patients with t-AML, there was a higher frequency of mutations of TP53 (33% vs. 8%) and ABC (ATP-binding cassette) transporter proteins (that mediate cancer drug resistance), and a lower frequency of DNMT3A and NPM1 mutations, than in de novo AML. A multivariate analysis in 52 patients with t-AML revealed poor overall survival for those with KRAS or NRAS mutations (hazard ratio [HR], 5.33; p=0.002), IDH2 mutation (HR, 5.49; p=0.004), or TP53 mutation (HR, 3.52; p= 0.001).
For four of seven cases examined, the same TP53 mutation was present at low frequency (0.003% to 0.7%) in mobilized blood leukocytes or bone marrow three to six years before development of t-MDS/AML, and for two of the four patients, before any chemotherapy was administered. Development of the TP53 mutation preceded the del(5q) and del(7q) cytogenetic abnormalities that often occur in t-MDS and t-AML, or other driver mutations such as ETV6. By roughly five years from the initial detection of the abnormal clone to development of t-MDS or t-AML, TP53 mutation-bearing clones comprised 45 percent of the cells.
Given the lack of a significant increased number of mutations, implying that the issue of development of t-AML was not due to widespread DNA damage, the authors hypothesized that the TP53 mutated clone developed clonal dominance due to a competitive survival advantage. To prove this, the investigators used mixed bone marrow chimeras of wild-type and heterozygous mutant Tp53 (Tp53+/-) in mice to show that the Tp53+/- mutant clones indeed developed a competitive advantage after either chemotherapy or irradiation. These data are consistent with the notion that chemoradiotherapy leads to t-MDS and t-AML due to suppression of normal hematopoiesis and expansion of TP53-mutated clones.
Recent publications have documented the development of age-related clonal hematopoiesis,4-6 including recurring AML mutations in a moderate proportion of healthy individuals. Dr. Wong and colleagues also examined healthy individuals aged 68 to 89 years and found that nine of 19 evaluable cases harbored TP53 mutations, with a variant allele frequency of 0.01 to 0.37 percent. Knowing that these mutations exist in healthy individuals, several questions arise for patients undergoing treatment with chemoradiotherapy: 1) Should these individuals be screened for TP53 and ABC transporter mutations? 2) What is the role of serial monitoring of mutant allele burden? 3) Could changes in the clonal architecture be used to reliably predict development of overt t-MDS/AML, and therefore, a basis for early intervention strategies? This work provides a more solid framework to start addressing some of these complex but important questions for our patients.
1. The Cancer Genome Atlas Research Network. Genomic and epigenomic landscapes of adult de novo acute myeloid leukemia. N Engl J Med. 2013;368:2059-2074.
2. Walter MJ, Shen D, Ding L, et al. Clonal architecture of secondary acute myeloid leukemia. N Engl J Med. 2012;366:1090-1098.
3. Walter MJ, Shen D, Shao J, et al. Clonal diversity of recurrently mutated genes in myelodysplastic syndromes. Leukemia. 2013:27;1275-1282.
4. Xie M, Lu C, Wang J, et al. Age-related mutations associated with clonal hematopoietic expansion and malignancies. Nat Med. 2014;20:1472-1478.
5. Genovese G, Kähler AK, Handsaker RE, et al. Clonal hematopoiesis and blood-cancer risk inferred from blood DNA sequence. N Engl J Med. 2014;371:2477-2487
6. Jaiswal S, Fontanillas P, Flannick J, et al. Age-related clonal hematopoiesis associated with adverse outcomes. N Engl J Med. 2014;371:2488-2498.
Development of t-aML due to clonal expansion of the TP53-mutated clone. Chemotherapy imposes selection for the TP53 mutated clone leading to a higher representation (middle panel). Additional driver mutations lead to expansion of leukemic clones (right panel). SNVs=single nucleotide variants.
Reprinted by permission from Macmillan Publishers Ltd: Nature. 2014 Dec 8. doi: 10.1038/nature13968, copyright 2014.
Figure

14 The Hematologist: ASH NewS AND RePORtS
Clinical Trials Corner
Can Prolyl Hydroxylase Inhibition Treat ePo-Deficient Anemia of Renal Failure With Fewer Vascular Complications Than ePo Itself?
StUDY tItLe: A Phase 3, Multicenter, Randomized, Open-label, Active-Controlled Study of the Safety and Efficacy of Roxadustat in the Treatment of Anemia in Dialysis Patients
CLINICALtRIALS.GOV IDeNtIFIeR: NCT02174731
COORDINAtOR: AstraZeneca Research and Development
SPONSOR: AstraZeneca in collaboration with FibroGen
PARtICIPAtING CeNteRS: Multiple sites in the united states and other countries.
ACCRUAL GOAL: 1,425
StUDY DeSIGN: This is a phase III safety and efficacy trial that compares the time to first occurrence of death from any cause, nonfatal myocardial infarction, or nonfatal stroke in dialyzed subjects with renal failure whose anemias are treated with the prolyl hydroxylase inhibitor, roxadustat, with that of individuals treated with the active control, re-combinant human erythropoietin (rhePo). Dialyzed patients with renal failure who are anemic and either treated with rhePo or a rhePo-associated erythropoiesis-stimulating agent (esA) are randomized 1:1 to receive roxadustat or rhePo. Both groups have a target hemoglobin range of 11 ± 1 g/dL. secondary outcomes are changes in mean hemo-globin from baseline, time to rescue therapy with rhePo or red blood cell transfusion, and time to other major vascular events including vascular access thrombosis, deep-vein thrombosis, pulmonary embolism, hypertensive emergency, and heart failure or unstable angina requiring hospitalization.
RAtIONALe: The cloning of ePo has allowed for the large-scale production of rhePo for clinical use, most success-fully in anemic patients with renal failure. Peritubular interstitial cells in the kidney cortex produce the large ma-jority of ePo, and most patients with renal failure develop anemia secondary to deficient ePo production by their diseased kidneys, although iron deficiency and decreased iron mobilization due to increased inflammatory cytokines contribute to renal failure anemia.1 Along with successful treatment of the anemia in renal disease patients, rhePo
treatment also causes an increased incidence of exacer-bated hypertension and adverse cardiovascular events, including myocardial infarctions and strokes, especially when the anemia correction approaches normal hemoglo-bin levels.2
The cloning of ePo also led to the discovery of specific se-quences termed hypoxia responsive elements in the 5ʹ and 3ʹ flanking regions of the ePo gene that bind the transcription factor, hypoxia inducible factor (HIF). HIF regulates the en-hanced ePo production resulting from tissue hypoxia caused by anemia. The HIF1α or HIF2α component of the HIF tran-scription factor complex is rapidly degraded under normoxic conditions when it is hydroxylated on two specific prolines by three HIF hydroxylases that have non-heme ferrous iron at their active sites.3,4 These enzymes use molecular oxygen and the Krebs cycle intermediate α-ketoglutarate as cosubstrates in reactions that hydroxylate HIF and oxidatively decarboxyl-ate α-ketoglutarate to succinate. Thus, HIF hydroxylases act as hypoxia sensors at an interface of oxygenation and energy metabolism.4 Prolyl hydroxylated HIFα components are rec-ognized by von Hippel-Lindau protein (pVHL), which medi-ates their polyubiquitination with subsequent proteasomal degradation. under hypoxic conditions, HIF1α and HIF2α are not hydroxylated due to decreased oxygen availability. Non-hydroxylated HIF1α or HIF2α dimerizes with constitutively produced HIFβ and forms the active HIF complex that induces target gene transcription. Although ePo is produced mainly in renal cortical interstitial cells, HIF is produced in all cells. HIF2α mediates EPO transcription, but HIF1α and HIF2α can induce transcription of many genes in a wide variety of cells, including those encoding proteins that 1) increase iron ab-sorption and mobilization (duodenal cytochrome b, divalent metal transporter-1, transferrin, transferrin receptor, and heme oxygenase-1),1 2) shift energy metabolism from aerobic to an-aerobic (glucose transporters, glycolytic enzymes, and lactate dehydrogenase),3,4 and 3) promote neovascular development (vascular endothelial growth factor and angiopoietins).3
Compared with rhePo administration in anemic renal failure patients, HIFα stabilization by prolyl hydroxylase inhibition with subsequent increases in endogenous ePo production has an additional potential advantage of improving iron absorption and mobilization, thereby facilitating anemia correction. Furthermore, HIF-mediated neovascular activity has been associated with decreased cardiac damage from myocardial ischemia,3 suggesting that the cardiovascular complications accompanying anemia correction in patients with renal failure might be decreased with prolyl hydroxyl-ation inhibition compared with rhePo administration. These potential advantages of prolyl hydroxylase inhibitors are
accompanied by potential drawbacks. pVHL mutations that increase HIF activity and cause polycythemia in von Hippel-Lindau and Chuvash polycythemia syndromes are associated with increased microvascular tumors, pulmonary hyperten-sion, and cerebrovascular disease.1,3,4 Increased HIF activity with its enhancement of anaerobic metabolism is associated with aggressive growth of malignancies.3,4 Neovascular activ-ity from increased HIF may accelerate tumor vessel growth in patients with unrecognized malignancies and may exacerbate retinopathy in diabetics, who represent a significant propor-tion of patients with renal failure.
COMMeNt: In a phase I trial, an orally administered ana-logue of α-ketoglutarate competitively inhibited HIF prolyl hydroxylases and increased plasma ePo levels of patients with renal failure.5 Preliminary results from a phase II clini-cal trial of roxadustat, another oral α-ketoglutarate analogue inhibitor of prolyl hydroxylases, showed increased ePo levels and maintenance of target hemoglobin.6 The ongoing phase III roxadustat trial [NCT02174731] will have a target hemoglobin range that is less than that seen in previous rhePo clinical trials associated with increased vascular events, but the outcome should help determine whether HIF prolyl hydroxylase inhibition decreases the incidence of vascular events compared with rhePo administration dur-ing the treatment of renal failure anemia. Furthermore, the trial may help determine whether any of the potential draw-backs of prolyl hydroxylase inhibition will be problematic.
1. Haase VH. Regulation of erythropoiesis by hypoxia-inducible factors. Blood Rev. 2013;27:41-53.
2. Fishbane s, Besarab A. Mechanism of increased mortality risk with erythropoietin treatment to higher hemoglobin targets. Clin J Am soc Nephrol. 2007;2:1274-1282.
3. semenza GL. oxygen sensing, homeostasis, and disease. N engl J Med. 2011;365:537-547.
4. Ratcliffe PJ. oxygen sensing and hypoxiasignalling pathways in animals: the implications of physiology for cancer. J Physiol. 2013;591:2027-2042.
5. Bernhardt WM, Wiesener Ms, scigalla P, et al. Inhibition of prolyl hydroxylases increases erythropoietin production in esRD. J Am soc Nephrol. 2010;21:2151-2156.
6. Provenzano R, Besarab A, Dua sL, et al. FG-4592, a novel oral hypoxia-inducible factor prolyl hydroxylase inhibitor (HIF-PHI), maintains hemoglobin levels and lowers cholesterol in hemodialysis (HD) patients: phase 2 comparison with epoetin alfa [abstract]. J Am soc Nephrol. 2012;23:428A.
– Mark J. Koury, MD
Dr. Koury indicated no relevant conflicts of interest.
Tamunomieibi Wakama, MD, is a visiting physician at Roswell Park Cancer Institute (RPCI) thanks to a Visitor Training Program (VTP) grant from ASH that was awarded to Vishala Neppalli, MD, assistant professor of oncology in the Department of Pathology & Laboratory Medicine at RPCI.
Twenty such grants are awarded by ASH each year, enabling talented hematologists, scientists, and/or laboratory staff from developing countries to receive training on a specific hematology topic or technique under the mentorship of an ASH member at institutions where both resources and staff are readily available. The program’s goal is to build hematology capacity in developing countries and to improve research and patient care globally.
Dr. Neppalli developed the 12-week curriculum to address the clinical and educational needs of Dr. Wakama and his institution in Nigeria. The training program is supported by grants from ASH and the National Hospital, Abuja. In Nigeria, Dr. Wakama is a fellow of the National Postgraduate Medical College of Nigeria and works as a consultant at the National Hospital, Abuja, where he cares for patients with diverse hematologic disorders, including hematologic malignancies. He also trains residents, fellows, and clinical laboratory staff.
At RPCI, Dr. Wakama has become proficient in several aspects of diagnostic hematopathology, with particular emphasis on flow cytometry and integrated diagnosis in neoplastic hematopathology.
“Diagnosis of hematologic malignancies is complex,” says Dr. Neppalli. “But it is easy to take for granted at centers such as RPCI, where we have a sizeable pathology
department with dedicated hematopathologists, in addition to highly specialized ancillary laboratories devoted to bone marrow, lymph node pathology, flow cytometry, cytogenetics, and molecular studies.”
In Nigeria, Dr. Wakama serves as both clinician and pathologist to his patients. The responsibility for determining the specific leukemia type or hematologic disorder rests on his shoulders.
“At my hospital, diagnostic hematopathology is very limited and relies mainly on morphology examination of tissue, blood, and bone marrow, with minimal ancillary tests,” explains Dr. Wakama. “Where such tests are required, we must send them elsewhere with a resultant long turnaround time and high cost, which have a negative impact on proper and prompt patient care.”
other challenges he faces at his home institution include the lack of an integrated approach to specimen handling and reporting of diagnostic information. The tissue specimens, including bone marrow core biopsies, are processed and reported by surgical pathology, independent of hematology correlation with concurrent diagnostic specimens. Gaps in the interpretation and integration of these diagnostic tests can lead to diagnostic inaccuracies and erroneous treatment plans.
asH Program Helps Bring a nigerian Hematologist to Roswell Park Cancer institute for Training
Dr. Tamunomieibi Wakama and Dr. Vishala Neppalli at Roswell Park Cancer Institute.

The Hematologist: ASH NewS AND RePORtS 15
D e C e M B e R 1 8 , 2 0 1 4
Collins Pw, Young G, Knobe K, et al. Recombinant long-acting glycoPeGylated factor IX in hemophilia B: a multinational randomized phase 3 trial. Blood 2014;124:3880-3886.
In this week’s Blood, Dr. Peter Collins and colleagues report the results of a phase III randomized trial of two doses of prophylaxis with long-acting pegylated recombinant fac-tor IX (rFIX) versus on-demand therapy in patients with hemophilia B. Weekly prophylaxis was well tolerated and associated with low bleeding rates and improved quality of life. At the higher prophylactic dose (40 Iu/kg/week), two-thirds of patients had no bleeding episodes in target joints throughout the year-long trial. Both prophylactic regimens led to protective predose levels of FIX. This signals an ex-citing major advance in the therapy of hemophilia B.
J a n u a R y 1 , 2 0 1 5
Van der Meulen J, Sanghvi V, Mavrakis K, et al. the H3K27me3 demethylase UtX is a gender-specific tumor suppressor in t-cell acute lymphoblastic leukemia. Blood. 2015;125:13-21
T-cell acute lymphoblastic leukemia (T-ALL) is an aggres-sive leukemia that occurs much more frequently in males. In this week’s plenary paper, Dr. Joni van der Meulen and colleagues offer an explanation for this gender predilec-tion. They report that a gene on the X chromosome, uTX, is recurrently mutated in male T-ALL and does not undergo X-inactivation in female stem cells or ALL blasts. Further stud-ies demonstrate that uTX functions as a tumor suppressor gene in T-ALL both in vitro and in vivo. This X-linked tumor suppressor illuminates the male predominance of T-ALL and offers a new therapeutic entry point for ALL therapy through manipulation of uTX pathway-related demethylation.
Dr. Bob Löwenberg (editor-in-Chief) and Dr. Nancy Berliner (Deputy editor-in-Chief) have combined efforts to identify some of the most outstanding Blood articles that have appeared either in print or online during the two-month interval between issues of The Hematologist. The goal is to underscore the remarkable research that is published in Blood and to highlight the exciting progress that is being made in the field.
eDItORS’
CHOICe ››
Padmanabhan A, Jones CG, Bougie Dw, et al. Heparin-independent, PF4-dependent binding of HIt antibodies to platelets: implications for HIt pathogenesis. Blood. 2015;125:155-161.
theodore e. warkentin, Jo-Ann I. Sheppard, F. Victor Chu Plasma exchange to remove HIt antibodies: dissociation between enzyme-immunoassay and platelet activation test reactivities. Blood. 2015;125:195-198.
Two papers in this week’s Blood elucidate the patho-genesis and management of heparin-induced thrombo-cytopenia and thrombosis (HIT). In the first, Dr. Anand Padmanabhan and colleagues demonstrate that HIT anti-bodies can be separated into those that activate platelets in the absence of heparin and those that do not. Antibod-ies detected in the serotonin release assay (sRA) fall into the former category, likely explaining the observation of “delayed HIT” that can persist following discontinuation of heparin. In the second, this important distinction is fur-ther delineated in examining patients undergoing plasma exchange for the removal of HIT antibodies, most com-monly to allow cardiac/vascular surgery using heparin. Dr. Theodore Warkentin and colleagues report that the test of choice for monitoring this procedure is the sRA, as a positive eLIsA for PF4 antibodies may persist despite exchange. However, a negative sRA predicts for safe hep-arin administration in this emergency setting.
J a n u a R y 7, 2 0 1 5
Stritt S, wolf K, Lorenz V, et al. Rap1-GtP–interacting adaptor molecule (RIAM) is dispensable for platelet integrin activation and function in mice. Blood. 2015;125:219-222.
Platelet aggregation at sites of vascular injury is essential for hemostasis as well as thrombosis. Platelet adhesive-ness is dependent on agonist-induced inside-out activa-tion of heterodimeric integrin receptors by a mechanism involving the recruitment of the large cytoskeletal protein talin-1 to the cytoplasmic integrin tail. Previous studies had suggested a critical role of the adaptor molecule Rap1-GTP-Interacting adaptor molecule (RIAM) for talin-1 recruitment and integrin activation. The plenary paper in this week’s Blood by Dr. simon stritt et al reports the paradigm shifting finding that RIAM is not at all necessary for integrin activation and function in mouse platelets. The investigators show both inside-out and outside-in β3- and β1-integrin activation are unaltered in RIAM-null mice. Also adhesion and aggregation responses of whole platelets under both static and flow conditions are entirely normal, and hemostasis and arterial thrombus formation are indistinguishable between wild-type and RIAM-null mice.
Sasaki H, Kurotaki D, Osato N, et al. transcription factor IRF8 plays a critical role in the development of murine basophils and mast cells. Blood. 2015;125:358-369.
Basophils and mast cells act in host defense against patho-gens and allergic disorders. Little is known about the fac-tors that control the development of basophils and mast cells, and the existence of a bipotential “basophil-mast cell progenitor” remains unsettled. In this issue of Blood, Dr. Haruka sasaki et al demonstrate that the transcription fac-tor interferon regulatory factor-8 (IRF8) is strictly required for the development of basophils in mice. The investigators reveal a molecular mechanism by which IRF8 acts down-stream via Gata2 and present data documenting the lineage potential of putative “basophil-mast cell progenitors.”
J a n u a R y 1 4 , 2 0 1 5
Raghu1 H, Cruz C, Rewerts CL, et al. transglutaminase factor XIII promotes arthritis through mechanisms linked to inflammation and bone erosion. Blood. 2015;125:427-437.
There is increasing evidence that coagulation factors moonlight as mediators of inflammation, primarily through the integrin-mediated interaction of fibrin with inflamma-tory cells. In this week’s plenary paper, Dr. Harini Raghu and colleagues elucidate a novel role for transglutaminase factor XIII (fXIII) in inflammatory arthritis, demonstrating proinflammatory effects independent of its activity in fibrin cross-linking. They demonstrate that fXIII knockout animals have decreased expression of RANKL and TRAP, leading to decreased osteoclastogenesis, which leads to preserva-tion of collagen and bone in the setting of collagen-induced arthritis. These studies further demonstrate the pleiotropic role of coagulation in the realm of inflammation and sug-gest that targeting fXIII might improve inflammatory arthri-tis and degenerative bone disease.
J a n u a R y 2 1 , 2 0 1 5
Milner JD, Vogel tP, Forbes L, et al. early-onset lymphoproliferation and autoimmunity caused by germline StAt3 gain-of-function mutations. Blood. 2015;125:591-599.
Haapaniemi eM, Kaustio M, Rajala HLM, et al. Autoimmunity, hypogammaglobulinemia, lymphoproliferation, and mycobacterial disease in patients with activating mutations in StAt3. Blood. 2015;125:639-648.
Recently, germ line heterozygous sTAT3 gain-of-function mutations have been identified in five patients with early-onset multiorgan autoimmune disease, including type 1 diabetes, and growth retardation. In this week’s issue of Blood, in two independent studies by Dr. Joshua Milner et al and Dr. emma Haapaniemi et al report that sTAT3 gain-of-function mutations are responsible for multiorgan au-toimmunity, autoimmune cytopenia, lymphoproliferation, and immune deficiency. In this week’s plenary paper, Dr. Milner et al describe 13 new cases in 10 families. Both stud-ies extend and detail the clinical and biologic phenotype of sTAT3 hyperactivity and also provide further insights into the underlying mechanistic consequences.
Celik H, Mallaney C, Kothari A, et al. enforced differentiation of Dnmt3a-null bone marrow leads to failure with c-Kit mutations driving leukemic transformation. Blood. 2015;125:619-628
Mayle A, Yang L, Rodriguez B. Dnmt3a loss predisposes murine hematopoietic stem cells to malignant transformation. Blood. 2015;125:629-638.
The incidence of acquired mutations of the DNMT3A gene rises progressively with increasing age. DNMT3A mutations as early (“founding”) mutations may set the stage for sub-sequent evolution towards a variety of hematological ma-lignancies, in particular, myelodysplastic syndromes and acute myeloid leukemia. In this issue of Blood, Dr. Hamza Celik et al and Dr. Allison Mayle et al report in separate studies that loss of Dnmt3a in murine hematopoietic stem cells (HsCs) perturbs blood cell formation. Furthermore, irradiated mice transplanted with Dnmt3a-null HsCs die of hematological malignancies within one year. The leukemia cells in these animals have acquired additional mutations, frequently in genes encoding signaling molecules involved in proliferation. These studies with the Dnmt3a-null mouse stem cell model recapitulate and cast further light on the development of hematological malignancies with DNMT3A mutations in humans.
An integral aspect of the VTP is for the mentor to devise a program for the trainee that encompasses specific techniques and knowledge that the trainee will be able to implement at his or her home institution and that will lead directly to better patient care and/or research. Dr. Wakama’s hospital in Nigeria has already purchased the equipment to establish and implement flow cytometry services.
With the collaboration of Dr. Neppalli, Dr. Paul Wallace (director, Department of Flow & Image Cytometry), and Dr. George Deeb (associate director, Laboratory of Clinical Flow Cytometry), Dr. Wakama learned to develop cost-effective flow cytometry panels and strategies that he will be able to implement upon his return home. He will then train his colleagues and other personnel, further improving hematopathology capabilities and patient care. “I will also have the ongoing benefit of the established contact with Dr. Neppalli and RPCI, which will continue to bridge knowledge gaps.”
In addition, Dr. Wakama participated in RPCI’s clinical educational programs for technologists as well as the lymphoma multidisciplinary tumor board, initiated and directed by Dr. Neppalli. “I experienced firsthand the importance of these conferences and how they create common diagnostic ground and establish effective communication across the hospital laboratories. I hope to
start similar programs when I return home to bring about a sustainable and knowledge-driven change in our work flow.”
“It is an honor to be selected as a mentor to train an international physician through ASH,” says Dr. Neppalli. “Institutions and the mentors selected are recognized for their expertise at the international level, and it highlights the quality of education and clinical expertise RPCI faculty bring to the field of hematology. I thank my colleagues, specifically Dr. George Deeb and Dr. Paul Wallace, who contributed to the training modules, as well as the clinical technologists who made this possible.”
one aspect of his training at RPCI that Dr. Wakama won’t likely need in Nigeria is his experience coping with snow such as the historic storm that buried Western New York in several feet of snow in November 2014.
“I had seen snow before in Europe, but nothing of this magnitude,” says Dr. Wakama. “I woke in the middle of the night to see only white all over and the atmosphere aglow. It was a beauty to behold and I was delighted to be part of history. It was an experience I won’t soon forget.”
t H e I N t e R N A t I O N A L H e M A t O L O G I S t

w H A t ’ S O N t H e w e B
As technology and the web have evolved, so too have ASH’s
online offerings. Now, beyond the ASH website, you can
download ASH apps for your smartphone or tablet, follow ASH
on twitter (www.twitter.com/ASH_hematology), and find ASH
videos on Youtube (www.youtube.com/user/ASHWebmaster).
Read The Hematologist online at
www.hematology.org/thehematologist,
and catch up on the latest news in
the field of hematology right on your
desktop, mobile phone, or tablet.
M a R K y o u R C a L e n D a R
March
1 asH active/international membership applications due Washington, DC www.hematology.org/membership
6 early-bird registration for Highlights of asH in Latin america ends Washington, DC www.hematology.org/highlights
10 applications for the 2015 Minority Medical student award due Washington, DC www.hematology.org/awards
12 applications for the 2015 Clinical Research Training institute in Latin america due Washington, DC www.hematology.org/awards
12-14 The national Comprehensive Cancer network’s (nCCn) annual Conference Hollywood, FL www.nccn.org
16 applications for the 2015 Latin american Training Program due Washington, DC www.hematology.org/awards
18 application for the asH-aMFDP award due Washington, DC www.hematology.org/awards
27 application deadline for the Clinical Research Training institute Washington, DC www.hematology.org/awards
april
3 advance registration for Highlights of asH in Latin america ends Washington, DC www.hematology.org/highlights
6 nomination Packages for the 2015 asH Mentor award due Washington, DC www.hematology.org/awards
10 applications for the 2015 visitor Training Program due Washington, DC www.hematology.org/awards
15 asH Bridge Grant application deadline Washington, DC www.hematology.org/awards
18-22 american association for Cancer Research’s (aaCR) annual meeting Philadelphia, PA www.aacr.org
23-24 2015 Highlights of asH in Latin america Cartagena, Colombia www.hematology.org/highlights
May
6-9 american society of Pediatric Hematology/oncology’s (asPHo) annual meeting Phoenix, AZ www.aspho.org
29- american society of Clinical oncology (asCo) annual meeting
Jun. 2 Chicago, IL www.am.asco.org
June
17-20 13th international Conference on Malignant Lymphoma Lugano, Switzerland www.lymphcon.ch
For additional meetings dates and award deadlines, visit www.hematology.org
the ASH teaching Cases have been revamped to offer users a more visually engaging design, interactive feedback, access to cases through mobile devices, and the ability to save progress and complete cases at one’s convenience.
the ASH teaching Cases are perfect for teaching medical students about standard approaches to classic hematologic problems across malignant, non-malignant, adult, and pediatric disease areas and topics. they are designed to simulate the steps involved in diagnosing a patient, from taking the history and performing a physical exam, to ordering and interpreting lab tests, to making a final diagnosis and following the clinical course of the disease.
Visit https://ashacademy.org/Product/TeachingCasesList for more information, and send feedback to [email protected].
asH Teaching CasesCheck out the updates to one of the ASH Academy's most popular learning tools.