significance of allelic percentage of braf c.1799t > a (v600e) mutation in papillary thyroid...
TRANSCRIPT

ORIGINAL ARTICLE – TRANSLATIONAL RESEARCH AND BIOMARKERS
Significance of Allelic Percentage of BRAF c.1799T [ A (V600E)Mutation in Papillary Thyroid Carcinoma
Shih-Ping Cheng, MD, PhD1,2,6, Yi-Chiung Hsu, PhD5, Chien-Liang Liu, MD1,2, Tsang-Pai Liu, MD1,2,
Ming-Nan Chien, MD1,3, Tao-Yeuan Wang, MD1,4, and Jie-Jen Lee, MD, PhD1,2,6
1Mackay Junior College of Medicine, Nursing, and Management, Taipei, Taiwan; 2Department of Surgery,
Mackay Medical College and Mackay Memorial Hospital, Taipei, Taiwan; 3Division of Endocrinology and Metabolism,
Department of Medicine, Mackay Medical College and Mackay Memorial Hospital, Taipei, Taiwan; 4Department of
Pathology, Mackay Medical College and Mackay Memorial Hospital, Taipei, Taiwan; 5Institute of Statistical Science,
Academia Sinica, Taipei, Taiwan; 6Graduate Institute of Medical Sciences and Department of Pharmacology, Taipei
Medical University, Taipei, Taiwan
ABSTRACT
Background. Somatic BRAF mutation is frequently
observed in papillary thyroid carcinoma (PTC). Recent
evidence suggests that PTCs are heterogeneous tumors
containing a subclonal or oligoclonal occurrence of BRAF
mutation. Conflicting results have been reported concern-
ing the prognostic significance of the mutant allele
frequency. Our present aim was to investigate the associ-
ation between the percentage of BRAF c.1799T [ A
(p.Val600Glu) alleles and clinicopathological parameters
in PTC.
Methods. Genomic DNA was extracted from fresh-frozen
specimens obtained from 50 PTC patients undergoing total
thyroidectomy. The BRAF mutation status was determined
by Sanger sequencing. The percentage of mutant BRAF
alleles was quantified by mass spectrometric genotyping,
pyrosequencing, and competitive allele-specific TaqMan
PCR (castPCR).
Results. Positive rate of BRAF mutation was 72 % by Sanger
sequencing, 82 % by mass spectrometric genotying, and 84 %
by pyrosequencing or castPCR. The average percentage of
mutant BRAF alleles was 22.5, 31, and 30.7 %, respectively.
There was a good correlation among three quantification
methods (Spearman’s rho = 0.87–0.97; p \ 0.0001). The
mutant allele frequency was significantly correlated with
tumor size (rho = 0.47–0.52; p \ 0.01) and extrathyroidal
invasion. The frequency showed no difference in pathological
lymph node metastasis.
Conclusions. The percentage of mutant BRAF alleles is
positively associated with tumor burden and extrathyroidal
invasion in PTC. Relatively good correlations exist among
mass spectrometric genotyping, pyrosequencing, and cast-
PCR in quantification of mutant BRAF allele frequency.
Papillary thyroid carcinoma (PTC) is the most common
malignant tumor of the thyroid gland. Thyroid cancer
incidence has increased substantially over the last decade,
and this change is primarily attributed to an increase in
PTC.1,2 Although most PTCs are curable or controllable by
the combination of surgery, radioactive iodine ablation,
and thyrotropin suppression, a considerable number of
patients die of persistent or recurrent disease that is
refractory to conventional therapy.3 With a growing
understanding of molecular oncology, therapeutic agents
that target activating genetic alterations in thyroid cancer
have been rapidly developed.4
The v-raf murine sarcoma viral oncogene homolog B
(BRAF) mutation occurs frequently in PTC.5 The most
common BRAF mutation comprises a single base trans-
version at codon 600 in exon 15, identified as c.1799T [ A
(p.Val600Glu) and generally referred to as V600E. The
prevalence of BRAF mutation was found to be increased
significantly over a 15-year period, and it was proposed
Electronic supplementary material The online version of thisarticle (doi:10.1245/s10434-014-3723-5) contains supplementarymaterial, which is available to authorized users.
� Society of Surgical Oncology 2014
First Received: 31 October 2013
J.-J. Lee, MD, PhD
e-mail: [email protected]
Ann Surg Oncol
DOI 10.1245/s10434-014-3723-5

that this change may contribute to the increasing incidence
of thyroid cancer.6 BRAF c.1799T [ A mutation greatly
increases the kinase activity and is associated with elevated
transcriptional output of the mitogen-activated protein
kinase (MAPK) pathway.7,8
Data from meta-analyses consistently indicate that the
presence of BRAF mutation in thyroid cancer is associated
with extrathyroidal invasion, lymph node metastasis,
advanced TNM stage, and disease recurrence.5,9–11 If thy-
roid cancer cells harboring BRAF mutation are biologically
more aggressive, tumors containing more BRAF mutation-
positive cells will theoretically have a worse outcome. In
this regard, Guerra and colleagues used pyrosequencing to
quantify the percentage of mutant BRAF alleles, demon-
strating that the mutant allele frequency correlated with age
and tumor volume, and the odds ratio of recurrent disease
was 5.31-fold higher in PTCs harboring a high ([30 %)
percentage of mutant BRAF alleles.12 On the contrary,
Gandolfi et al. 13 found no association between the per-
centage of mutant alleles and metastatic behavior. The
reason for this discrepancy remains to be elucidated.
Methods to detect BRAF mutation have not been stan-
dardized. Conventional DNA sequencing is binary (present
or absent) and takes no account of the ratio of mutated
DNA to wild type. Contemporary technological develop-
ments in genotyping are advantageous in terms of cost,
throughput, scalability, and sensitivity.14 The primary aim
of this study was to perform a multiplatform analysis to
characterize the biological significance of the percentage of
BRAF c.1799T [ A alleles in PTC. The secondary aim was
to compare different methods for quantification of mutant
BRAF allele frequency.
PATIENTS AND METHODS
Patients and Tissue Samples
This study was approved by the Institutional Review
Board of Mackay Memorial Hospital (12MMHIS175). All
patients provided written informed consent before the
procurement of tissue specimens.
A total of 50 patients who underwent total thyroidec-
tomy for PTC were consecutively selected. Five patients
who underwent lobectomy for follicular adenoma were
also included as negative controls. All patients were
euthyroid at the time of surgery and were not taking any
medications that could affect serum thyrotropin levels.
PTC tissues from the center of the lesions and corre-
sponding normal thyroid tissues from the contralateral
lobes of the same patient were obtained. All PTC tissue
samples were carefully dissected to exclude surrounding
normal tissue. Tissues were immediately snap-frozen in
liquid nitrogen and stored at -80 �C. The tissue diagnosis
was confirmed by frozen section.
Genomic DNA Extraction
Genomic DNA was extracted using the QIAamp DNA
mini kit (Qiagen, Valencia, CA, USA) according to the
manufacturer’s instructions. Serial dilutions of DNA from
B-CPAP thyroid cancer cells (homozygous BRAF mutation
?/?) were used as positive controls.15
Sanger Sequencing
Exon 15 of the BRAF gene was amplified using a spe-
cific custom-made oligonucleotide primer pair (electronic
supplementary Table 1). The PCR products were subjected
to sequencing reaction using the forward primer and Big-
Dye terminator V3.1 cycle sequencing reagents (Applied
Biosystems, Life Technologies, Carlsbad, CA, USA). DNA
sequence was read on an ABI PRISM 3730xL DNA
analyzer.
Mass Spectrometric Genotyping
The iPLEX assay is a single-base primer extension
assay.16 Locus-specific PCR primers and allele-specific
detection primers (electronic supplementary Table 1)
were designed using MassARRAY Assay Design software
(Sequenom Inc., San Diego, CA, USA). Allele detection
was performed using matrix-assisted laser desorption/
ionization time-of-flight mass spectrometer (MALDI-TOF
MS). The mass spectrograms were analyzed by the
MassARRAY TYPER software 4.0. All analyses showed a
very high call rate ([95 %, the median of call
rate [97 %), and a very high consistency rate between
blind duplicates ([97 %).
Pyrosequencing Analysis
Primer design (electronic supplementary Table 1) was
carried out using the PyroMark Assay Design software 2.0
(Qiagen). The biotinylated PCR products were attached to
Streptavidin-Sepharose beads (Amersham, GE Healthcare
Bio-Sciences, Piscataway, NJ, USA) and processed to
obtain single-stranded DNA using the PSQ 96 Sample
Preparation Kit. The sequencing-by-synthesis reaction of
the complementary strand was automatically performed
using the PyroMark Gold Q24 reagents (Qiagen) according
to kit specifications. The percentage of mutant alleles was
then calculated by PyroMark Q24 version 2.0.6 software
using the allele quantification mode.
S.-P. Cheng et al.

Competitive Allele-Specific TaqMan PCR
The BRAF mutation status was also determined with a
commercially available TaqMan Mutation Detection Assay
(Applied Biosystems). Competitive allele-specific TaqMan
PCR (castPCR) using the BRAF_476_mu probe for the
detection of BRAF c.1799T [ A mutation were run in
triplicates on an Applied Biosystems 7900HT Fast Real-
Time PCR System. The mutant allele frequency was
determined by comparing the cycle threshold (Ct) values of
the wild-type and mutant allele assays (DCt) in reference to
the control samples using Mutation Detector software 2.0.
The percentage of mutant BRAF alleles was calculated as
% = 1/(2DCt) 9 100.17
Statistical Analysis
Statistical analyses were performed using STATA 11.0
(Stata Corp., College Station, TX, USA) and GraphPad
Prism 6.02 (GraphPad Software, La Jolla, CA, USA).
Continuous variables were compared using the Mann–
Whitney test for two groups or Kruskal–Wallis test and
Dunn’s procedure for more than two groups. Chi square,
Fisher’s exact test, or Cochran-Armitage trend test were
used to compare categorical variables. For correlation
studies, Spearman’s rank-correlation test was used.
Throughout the analysis, p-values \ 0.05 (two-sided
hypotheses) were considered to be statistically significant.
RESULTS
Patients Characteristics
The study cohort consisted of 40 (80 %) female and 10
(20 %) male patients. Mean age at diagnosis was 47 years.
A total of 16 (32 %) patients with clinically apparent nodal
metastasis (cN1) had therapeutic central compartment neck
dissection with or without lateral neck dissection. The
remaining 34 (68 %) patients without preoperative or
intraoperative evidence of central neck metastases under-
went prophylactic central compartment dissection. Forty-
seven tumors were classical PTC (including five non-
incidental microcarcinomas), two were follicular variant
PTC, and one was solid variant PTC. Mean tumor size was
2.3 cm. Eight patients showed histological evidence of
chronic lymphocytic thyroiditis in the corresponding nor-
mal thyroid tissue. The numbers of tumor-infiltrating
lymphocytes were not specifically determined in the study.
Of 34 patients undergoing prophylactic central com-
partment dissection, 13 (38 %) showed microscopic nodal
metastasis. Therefore, a total of 29 (58 %) had pathological
nodal metastasis (pN1). The final TNM stage was deter-
mined on the basis of pathological data. One patient had
evidence of lung metastasis at the time of diagnosis, and
she was classified as TNM stage 2 because of her young
age. Tumor size was associated with clinical and patho-
logical lymph node metastasis (p = 0.016 and 0.025,
respectively).
Mutational Analysis by Sanger Sequencing
Tumor BRAF mutation was found in 36 (72 %) of 50
PTCs. No mutation was found in the contralateral normal
tissues or five follicular adenomas, indicating that this
mutation was somatically acquired and tumor-specific. As
shown in Table 1, the tumors with BRAF mutation were
associated with larger tumor size (p = 0.015), higher
probabilities of extrathyroidal invasion (p = 0.002), and
more advanced TNM stage (p = 0.003). Two (40 %) of
five microcarcinomas were positive for BRAF mutation.
Tumor BRAF mutation status was not associated with
TABLE 1 Clinicopathological parameters and BRAF c.1799T [ A
mutation status determined by Sanger sequencing
BRAF
mutation
? (n = 36)
BRAF
mutation
- (n = 14)
p Value
Female sex 29 (81) 11 (79) 1.000
Age at diagnosis
(years)a52 (37–58) 37 (32–51) 0.125
Body mass index
(kg/m2)a24.5 (21.6–28.9) 23.4 (19.4–25.8) 0.266
Body weight (kg)a 63 (52–76) 58 (56–65) 0.496
Tumor size (cm)a 2.2 (1.5–3.3) 1.4 (1.0–2.2) 0.015
Thyroiditis 4 (11) 4 (29) 0.197
Extrathyroidal
invasionb0.002
None 9 (25) 10 (71)
Microscopic 12 (33) 3 (21)
Macroscopic 15 (42) 1 (7)
Multifocality 13 (36) 4 (29) 0.746
Lymphovascular
invasion
12 (33) 2 (14) 0.295
Clinical lymph node
metastasis
13 (36) 3 (21) 0.501
Pathological lymph
node metastasis
21 (58) 8 (57) 1.000
TNM stageb 0.003
I 15 (42) 11 (79)
II 0 (0) 2 (14)
III 9 (25) 1 (7)
IV 12 (33) 0 (0)
Data are expressed as number (%) or median (interquartile range)a Mann–Whitney testb Cochran-Armitage trend test
Allelic Percentage of BRAF Mutation

clinical or pathological lymph node metastasis (p = 0.501
and 1.000, respectively).
Mutational Analysis by Mass Spectrometry
The percentage of mutant BRAF alleles in genomic
DNA from 50 PTCs was determined by mass spectrometric
genotyping (Fig. 1a). There was no mutant allele in nine
PTCs and five follicular adenomas. For 41 (82 %) PTCs
carrying BRAF mutation, the range of mutant allele fre-
quency was 3.2–35.2 %, with a mean and median of 22.5
and 25.2 %, respectively. Overall, five samples failed to be
assigned to positive BRAF mutation by Sanger sequencing
(90 % concordance). These discordant samples showed a
mutant allele frequency from 3.2 to 13.5 % (mean 6.6 %).
Tumor size varied from 1.3 to 4.0 cm (mean 2.4 cm).
There was no significant difference in characteristics
between the cases with concordant results and those with
discordant results, except for a lower frequency of mutant
allele in the discordant samples.
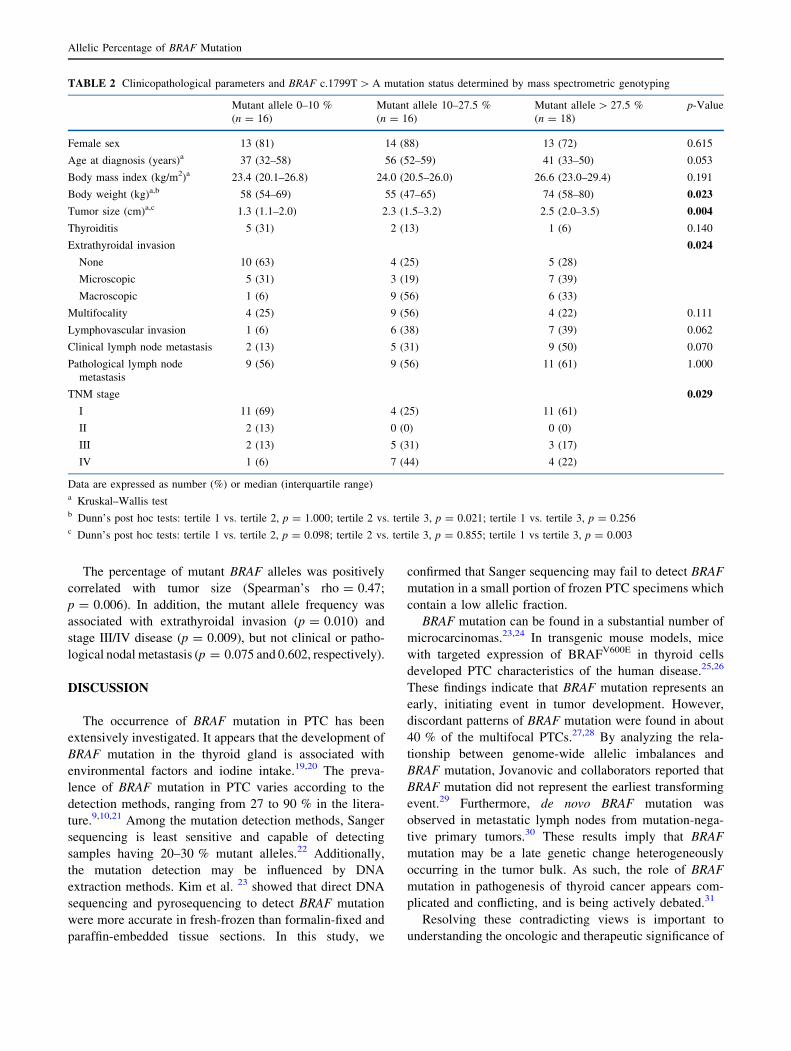
Patients were categorized on the basis of mutant allele
frequency into tertiles (Table 2). Tumor BRAF mutation
was associated with body weight (p = 0.023), tumor size
(p = 0.004), extrathyroidal invasion (p = 0.024), and
TNM stage (p = 0.029). There was no difference in
extrathyroidal invasion and TNM stage between the second
and third tertile (p = 0.347 and 0.113, respectively). A
seemingly higher disease stage in the second tertile may
reflect the relatively older age in this subgroup. As shown
in Fig. 1b, there was a strong positive correlation between
tumor size and mutant allele frequency (Spearman’s
rho = 0.47; p = 0.0005). Analyzed from another per-
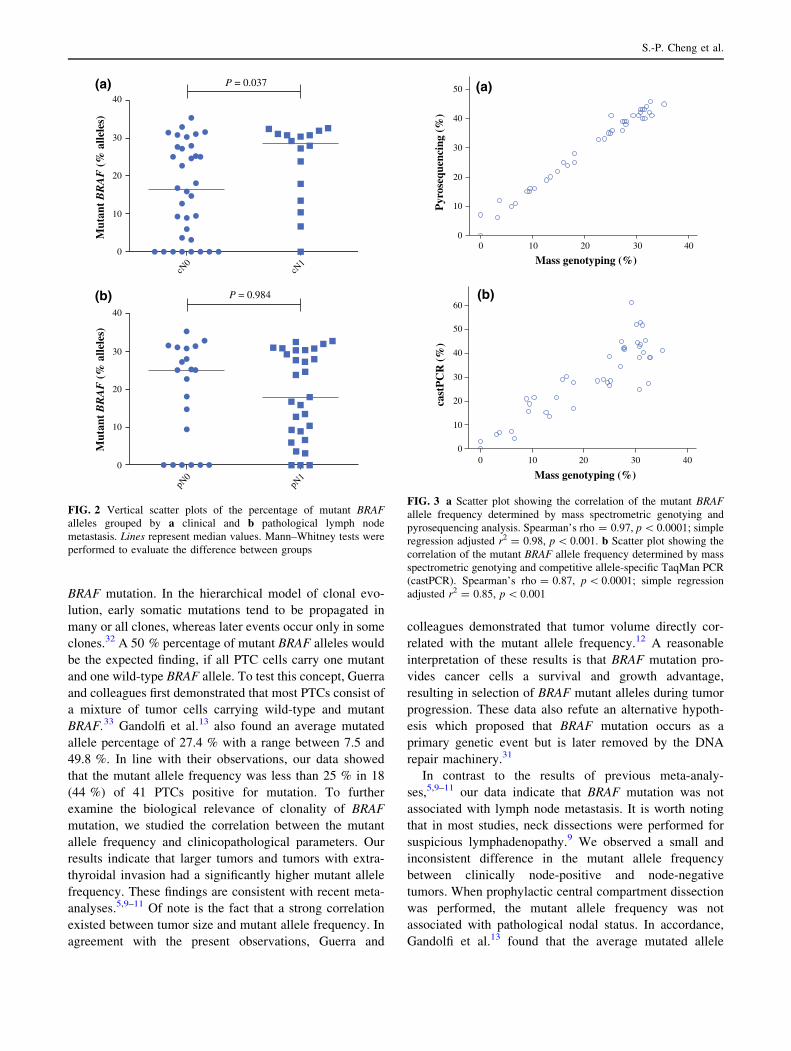
spective, PTC in association with clinical nodal metastasis
showed a mutant allele percentage significantly higher than
cN0 PTC (p = 0.037; Fig. 2a). There was no difference in
the mutant allele frequency between PTC with or without
pathological nodal metastasis (p = 0.984; Fig. 2b).
Mutational Analysis by Pyrosequencing
The percentage of mutant BRAF alleles from five fol-
licular adenomas varied from 3 to 5 %. Therefore, the
cutoff was set at 5 %, consistent with previous reports.12,13
For 42 PTCs positive for BRAF mutation, the range of
mutant allele frequency was 6–46 %, with a mean and
median of 31 and 36 %, respectively. The mutant allele
frequency was highly consistent between mass spectro-
metric genotying and pyrosequencing (Fig. 3a). One
patient with a 7 % BRAF mutation allele based on py-
rosequencing analysis had no mutant BRAF allele
detectable by mass spectrometry (98 % concordance).
The percentage of mutant BRAF alleles was strongly
correlated with tumor size (Spearman’s rho = 0.52;
p = 0.0001), but not age (p = 0.782) or body weight
(p = 0.100). Comparing medians of the mutant allele fre-
quency, significant differences were observed in
extrathyroidal invasion (p = 0.034) and clinical nodal
metastasis (p = 0.041), but not pathological nodal metas-
tasis (p = 0.937). Tumor BRAF mutation determined by
pyrosequencing was associated with higher probabilities of
stage III/IV disease (p = 0.018).
Mutational Analysis by castPCR
Five follicular adenomas were in the range of 0.03–
1.7 % mutant allele. A conservative 2.5 % cutoff was
chosen to avoid unreliable estimates due to stochastic
fluctuations in low copy number situations.18 In concor-
dance with the results obtained by pyrosequencing, 42
PTCs were positive for BRAF mutation based on castPCR
assay. The range of mutant allele frequency was 3.0–
61.6 %, with a mean and median of 30.7 and 29.1 %,
respectively. The mutant allele frequency was moderately
correlated between mass spectrometric genotying and
castPCR assay (Fig. 3b). A similar correlation coefficient
was observed between pyrosequencing and castPCR
(Spearman’s rho = 0.87; p \ 0.0001).
0
10
20
BR
AF
c.1
799T
>A (
% a
llele
s)
30
40
00
10
20
30
40
1 2 3
Tumor size (cm)
Mut
ant
alle
le f
requ
ency
(%
)
4 5 6
(a)
(b)
FIG. 1 a The percentage of mutant BRAF c.1799T [ A (p.Val600-
Glu) alleles detected by mass spectrometric genotyping in 50
papillary thyroid carcinomas. b Scatter plot showing the correlation
between tumor size and the percentage of mutant BRAF alleles. Lines
represent simple linear regression ±95 % confidence interval. Spear-
man’s rho = 0.47, p = 0.0005; simple regression adjusted r2 = 0.21,
p = 0.001
S.-P. Cheng et al.
The percentage of mutant BRAF alleles was positively
correlated with tumor size (Spearman’s rho = 0.47;
p = 0.006). In addition, the mutant allele frequency was
associated with extrathyroidal invasion (p = 0.010) and
stage III/IV disease (p = 0.009), but not clinical or patho-
logical nodal metastasis (p = 0.075 and 0.602, respectively).
DISCUSSION
The occurrence of BRAF mutation in PTC has been
extensively investigated. It appears that the development of
BRAF mutation in the thyroid gland is associated with
environmental factors and iodine intake.19,20 The preva-
lence of BRAF mutation in PTC varies according to the
detection methods, ranging from 27 to 90 % in the litera-
ture.9,10,21 Among the mutation detection methods, Sanger
sequencing is least sensitive and capable of detecting
samples having 20–30 % mutant alleles.22 Additionally,
the mutation detection may be influenced by DNA
extraction methods. Kim et al. 23 showed that direct DNA
sequencing and pyrosequencing to detect BRAF mutation
were more accurate in fresh-frozen than formalin-fixed and
paraffin-embedded tissue sections. In this study, we
confirmed that Sanger sequencing may fail to detect BRAF
mutation in a small portion of frozen PTC specimens which
contain a low allelic fraction.
BRAF mutation can be found in a substantial number of
microcarcinomas.23,24 In transgenic mouse models, mice
with targeted expression of BRAFV600E in thyroid cells
developed PTC characteristics of the human disease.25,26
These findings indicate that BRAF mutation represents an
early, initiating event in tumor development. However,
discordant patterns of BRAF mutation were found in about
40 % of the multifocal PTCs.27,28 By analyzing the rela-
tionship between genome-wide allelic imbalances and
BRAF mutation, Jovanovic and collaborators reported that
BRAF mutation did not represent the earliest transforming
event.29 Furthermore, de novo BRAF mutation was
observed in metastatic lymph nodes from mutation-nega-
tive primary tumors.30 These results imply that BRAF
mutation may be a late genetic change heterogeneously
occurring in the tumor bulk. As such, the role of BRAF
mutation in pathogenesis of thyroid cancer appears com-
plicated and conflicting, and is being actively debated.31
Resolving these contradicting views is important to
understanding the oncologic and therapeutic significance of
TABLE 2 Clinicopathological parameters and BRAF c.1799T [ A mutation status determined by mass spectrometric genotyping
Mutant allele 0–10 %
(n = 16)
Mutant allele 10–27.5 %
(n = 16)
Mutant allele [ 27.5 %
(n = 18)
p-Value
Female sex 13 (81) 14 (88) 13 (72) 0.615
Age at diagnosis (years)a 37 (32–58) 56 (52–59) 41 (33–50) 0.053
Body mass index (kg/m2)a 23.4 (20.1–26.8) 24.0 (20.5–26.0) 26.6 (23.0–29.4) 0.191
Body weight (kg)a,b 58 (54–69) 55 (47–65) 74 (58–80) 0.023
Tumor size (cm)a,c 1.3 (1.1–2.0) 2.3 (1.5–3.2) 2.5 (2.0–3.5) 0.004
Thyroiditis 5 (31) 2 (13) 1 (6) 0.140
Extrathyroidal invasion 0.024
None 10 (63) 4 (25) 5 (28)
Microscopic 5 (31) 3 (19) 7 (39)
Macroscopic 1 (6) 9 (56) 6 (33)
Multifocality 4 (25) 9 (56) 4 (22) 0.111
Lymphovascular invasion 1 (6) 6 (38) 7 (39) 0.062
Clinical lymph node metastasis 2 (13) 5 (31) 9 (50) 0.070
Pathological lymph node
metastasis
9 (56) 9 (56) 11 (61) 1.000
TNM stage 0.029
I 11 (69) 4 (25) 11 (61)
II 2 (13) 0 (0) 0 (0)
III 2 (13) 5 (31) 3 (17)
IV 1 (6) 7 (44) 4 (22)
Data are expressed as number (%) or median (interquartile range)a Kruskal–Wallis testb Dunn’s post hoc tests: tertile 1 vs. tertile 2, p = 1.000; tertile 2 vs. tertile 3, p = 0.021; tertile 1 vs. tertile 3, p = 0.256c Dunn’s post hoc tests: tertile 1 vs. tertile 2, p = 0.098; tertile 2 vs. tertile 3, p = 0.855; tertile 1 vs tertile 3, p = 0.003
Allelic Percentage of BRAF Mutation
BRAF mutation. In the hierarchical model of clonal evo-
lution, early somatic mutations tend to be propagated in
many or all clones, whereas later events occur only in some
clones.32 A 50 % percentage of mutant BRAF alleles would
be the expected finding, if all PTC cells carry one mutant
and one wild-type BRAF allele. To test this concept, Guerra
and colleagues first demonstrated that most PTCs consist of
a mixture of tumor cells carrying wild-type and mutant
BRAF.33 Gandolfi et al.13 also found an average mutated
allele percentage of 27.4 % with a range between 7.5 and
49.8 %. In line with their observations, our data showed
that the mutant allele frequency was less than 25 % in 18
(44 %) of 41 PTCs positive for mutation. To further
examine the biological relevance of clonality of BRAF
mutation, we studied the correlation between the mutant
allele frequency and clinicopathological parameters. Our
results indicate that larger tumors and tumors with extra-
thyroidal invasion had a significantly higher mutant allele
frequency. These findings are consistent with recent meta-
analyses.5,9–11 Of note is the fact that a strong correlation
existed between tumor size and mutant allele frequency. In
agreement with the present observations, Guerra and
colleagues demonstrated that tumor volume directly cor-
related with the mutant allele frequency.12 A reasonable
interpretation of these results is that BRAF mutation pro-
vides cancer cells a survival and growth advantage,
resulting in selection of BRAF mutant alleles during tumor
progression. These data also refute an alternative hypoth-
esis which proposed that BRAF mutation occurs as a
primary genetic event but is later removed by the DNA
repair machinery.31
In contrast to the results of previous meta-analy-
ses,5,9–11 our data indicate that BRAF mutation was not
associated with lymph node metastasis. It is worth noting
that in most studies, neck dissections were performed for
suspicious lymphadenopathy.9 We observed a small and
inconsistent difference in the mutant allele frequency
between clinically node-positive and node-negative
tumors. When prophylactic central compartment dissection
was performed, the mutant allele frequency was not
associated with pathological nodal status. In accordance,
Gandolfi et al.13 found that the average mutated allele
0
cN0
cN1
10
20
Mut
ant
BR
AF
(%
alle
les)
30
40
P = 0.037
0
pN0
pN1
10
P = 0.984
Mut
ant
BR
AF
(%
alle
les)
20
30
40
(a)
(b)
FIG. 2 Vertical scatter plots of the percentage of mutant BRAF
alleles grouped by a clinical and b pathological lymph node
metastasis. Lines represent median values. Mann–Whitney tests were
performed to evaluate the difference between groups
00
10
20
30
40
50
10 20
Mass genotyping (%)
Pyr
oseq
uenc
ing
(%)
30 40
00
10
20
30
40
50
60
10 20
Mass genotyping (%)
cast
PC
R (
%)
30 40
(a)
(b)
FIG. 3 a Scatter plot showing the correlation of the mutant BRAF
allele frequency determined by mass spectrometric genotying and
pyrosequencing analysis. Spearman’s rho = 0.97, p \ 0.0001; simple
regression adjusted r2 = 0.98, p \ 0.001. b Scatter plot showing the
correlation of the mutant BRAF allele frequency determined by mass
spectrometric genotying and competitive allele-specific TaqMan PCR
(castPCR). Spearman’s rho = 0.87, p \ 0.0001; simple regression
adjusted r2 = 0.85, p \ 0.001
S.-P. Cheng et al.

percentage was significantly lower in corresponding met-
astatic nodes compared with the primary PTCs (18.6 vs.
28.6 %). Therefore, it is likely that cancer cells harboring
BRAF mutation do not really have enhanced metastatic
capacity. More frequent lymph node metastasis observed
in BRAF mutation-positive tumors may result from a lar-
ger tumor burden and more extensive extrathyroidal
invasion. It was recently showed that BRAF mutation was
the only independent predictor of central compartment
lymph node metastasis in PTC;34 however, the design of
the study was biased by including BRAF status as a cri-
terion for prophylactic nodal dissection.
A plethora of genetic and phenotypic heterogeneity
comes from ongoing genetic instability within a cancer.
Most of the spontaneous mutations are evolutionarily
neutral or deleterious. Rare mutations that confer compet-
itive advantage can be selected for by Darwinian forces and
will eventually become predominant. Nonetheless,
achieving clonal dominance can take a long time, partly
because of spatial constraints.35 Our findings have impor-
tant biological implications in that they point out the
possibility that activating BRAF mutation may not neces-
sarily be an initiating prerequisite in PTC tumorigenesis,
but this secondary genetic alteration provides a survival
advantage to cancer cells, and accumulates. The fact that
the mutant allele frequency was associated with extrathy-
roidal invasion also makes it unlikely that expansion
emerges from fixation of neutral mutations over time
(genetic drift). Our results seemingly suggest that quanti-
tative assessment of mutation frequency provides no
additional information on clinical significance of BRAF
mutation (Tables 1 and 2). However, even a small portion
of mutation-negative tumor cells may hamper efficacy of
BRAF-targeted therapy. In RAS/RAF wild-type tumors,
RAF kinase inhibitors may paradoxically activate the
MAPK pathway in an RAS-dependent manner, thus
enhancing tumor growth in xenograft models.36 Further
studies may be undertaken to determine the effects of
clonality measures on clinical response to BRAF-targeted
therapy.
A limitation of our study is the inability to exclude
stromal contamination. Tumor samples always have some
degree of contamination by normal stromal, endothelial,
and inflammatory cells. The mutant allele frequency in
unselected cells would be lower than that in laser-captured
PTC cells.33 Nonetheless, the average percentage of mutant
BRAF alleles analyzed by different methods in the present
study (22.5 to 31 %) was compatible with those of recent
reports (21.9 to 27.4 %).12,13 Using next-generation
sequencing, Nikiforova and colleagues also demonstrated
that the mutant allele frequency was 18–44 % (mean 34 %)
in PTCs, corresponding to 36–88 % of cells with hetero-
zygous mutation.37
CONCLUSIONS
The percentage of mutant BRAF alleles in PTC is sig-
nificantly associated with tumor burden and extrathyroidal
invasion. A positive correlation between the mutant allele
frequency and tumor size implies that BRAF mutation may
play a role in tumor progression.
ACKNOWLEDGMENT The authors would like to thank the
Translational Core Laboratories of National Translational Medicine
and Clinical Trial Resource Center for technical assistance in
MALDI-TOF MS experiments. This work was supported by the
National Science Council of Taiwan (100-2314-B-195-001-MY3) and
Mackay Memorial Hospital (MMH-10206 and MMH-E-102-10).
DISCLOSURES Shih-Ping Cheng, Yi-Chiung Hsu, Chien-Liang
Liu, Tsang-Pai Liu, Ming-Nan Chien, Tao-Yeuan Wang, and Jie-Jen
Lee have nothing to disclose.
REFERENCES
1. Cramer JD, Fu P, Harth KC, Margevicius S, Wilhelm SM.
Analysis of the rising incidence of thyroid cancer using the sur-
veillance, epidemiology and end results national cancer data
registry. Surgery. 2010;148:1147–52.
2. Husson O, Haak HR, van Steenbergen LN, et al. Rising inci-
dence, no change in survival and decreasing mortality from
thyroid cancer in The Netherlands since 1989. Endocr Relat
Cancer. 2013;20:263–71.
3. Eustatia-Rutten CF, Corssmit EP, Biermasz NR, Pereira AM,
Romijn JA, Smit JW. Survival and death causes in differentiated
thyroid carcinoma. J Clin Endocrinol Metab. 2006;91:313–9.
4. Kapiteijn E, Schneider TC, Morreau H, Gelderblom H, Nortier
JW, Smit JW. New treatment modalities in advanced thyroid
cancer. Ann Oncol. 2012;23:10–8.
5. Xing M. BRAF mutation in papillary thyroid cancer: pathogenic
role, molecular bases, and clinical implications. Endocr Rev.
2007;28:742–62.
6. Mathur A, Moses W, Rahbari R, Khanafshar E, Duh QY, Clark O,
et al. Higher rate of BRAF mutation in papillary thyroid cancer over
time: a single-institution study. Cancer. 2011;117:4390–5.
7. Wan PT, Garnett MJ, Roe SM, et al; Cancer Genome Project.
Mechanism of activation of the RAF-ERK signaling pathway by
oncogenic mutations of B-RAF. Cell. 2004;116:855–67.
8. Pratilas CA, Taylor BS, Ye Q, Viale A, Sander C, Solit DB, et al.
(V600E)BRAF is associated with disabled feedback inhibition of
RAF-MEK signaling and elevated transcriptional output of the
pathway. Proc Natl Acad Sci USA. 2009;106:4519–24.
9. Li C, Lee KC, Schneider EB, Zeiger MA. BRAF V600E mutation
and its association with clinicopathological features of papillary
thyroid cancer: a meta-analysis. J Clin Endocrinol Metab.
2012;97:4559–70.
10. Kim TH, Park YJ, Lim JA, Ahn HY, Lee EK, Lee YJ, et al. The
association of the BRAF(V600E) mutation with prognostic fac-
tors and poor clinical outcome in papillary thyroid cancer: a
meta-analysis. Cancer. 2012;118:1764–73.
11. Tufano RP, Teixeira GV, Bishop J, Carson KA, Xing M. BRAF
mutation in papillary thyroid cancer and its value in tailoring
initial treatment: a systematic review and meta-analysis. Medi-
cine (Baltimore). 2012;91:274–86.
12. Guerra A, Fugazzola L, Marotta V, Cirillo M, Rossi S, Cirello V,
et al. A high percentage of BRAFV600E alleles in papillary
Allelic Percentage of BRAF Mutation

thyroid carcinoma predicts a poorer outcome. J Clin Endocrinol
Metab. 2012;97:2333–40.
13. Gandolfi G, Sancisi V, Torricelli F, Ragazzi M, Frasoldati A,
Piana S, et al. Allele percentage of the BRAF V600E mutation in
papillary thyroid carcinomas and corresponding lymph node
metastases: no evidence for a role in tumor progression. J Clin
Endocrinol Metab. 2013;98:E934–42.
14. MacConaill LE. Existing and emerging technologies for tumor
genomic profiling. J Clin Oncol. 2013;31:1815–24.
15. Cheng SP, Liu CL, Hsu YC, Chang YC, Huang SY, Lee JJ.
Expression and biologic significance of adiponectin receptors in
papillary thyroid carcinoma. Cell Biochem Biophys. 2013;65:
203–10.
16. Thomas RK, Baker AC, Debiasi RM, Winckler W, LaFramboise
T, Lin WM, et al. High-throughput oncogene mutation profiling
in human cancer. Nat Genet. 2007;39:347–51.
17. Pfaffl MW. A new mathematical model for relative quantification
in real-time RT-PCR. Nucleic Acids Res. 2001;29:e45.
18. Kloos RT, Reynolds JD, Walsh PS, Wilde JI, Tom EY, Pagan M,
et al. Does addition of BRAF V600E mutation testing modify
sensitivity or specificity of the Afirma Gene Expression Classifier
in cytologically indeterminate thyroid nodules? J Clin Endocrinol
Metab. 2013;98:E761–8.
19. Frasca F, Nucera C, Pellegriti G, Gangemi P, Attard M, Stella M,
et al. BRAF(V600E) mutation and the biology of papillary thy-
roid cancer. Endocr Relat Cancer. 2008;15:191–205.
20. Guan H, Ji M, Bao R, Yu H, Wang Y, Hou P, et al. Association of
high iodine intake with the T1799A BRAF mutation in papillary
thyroid cancer. J Clin Endocrinol Metab. 2009;94:1612–7.
21. Jeong D, Jeong Y, Park JH, Han SW, Kim SY, Kim YJ, et al.
BRAF (V600E) mutation analysis in papillary thyroid carcinomas
by peptide nucleic acid clamp real-time PCR. Ann Surg Oncol.
2013;20:759–66.
22. Lade-Keller J, Romer KM, Guldberg P, Riber-Hansen R, Hansen
LL, Steiniche T, et al. Evaluation of BRAF mutation testing
methodologies in formalin-fixed, paraffin-embedded cutaneous
melanomas. J Mol Diagn. 2013;15:70–80.
23. Kim HS, Kim JO, Lee DH, Lee HC, Kim HJ, Kim JH, et al.
Factors influencing the detection of the BRAF T1799A mutation
in papillary thyroid carcinoma. Oncol Rep. 2011;25:1639–44.
24. Virk RK, Van Dyke AL, Finkelstein A, Prasad A, Gibson J, Hui P,
et al. BRAFV600E mutation in papillary thyroid microcarcinoma:
a genotype-phenotype correlation. Mod Pathol. 2013;26:62–70.
25. Knauf JA, Ma X, Smith EP, Zhang L, Mitsutake N, Liao XH,
et al. Targeted expression of BRAFV600E in thyroid cells of
transgenic mice results in papillary thyroid cancers that undergo
dedifferentiation. Cancer Res. 2005;65:4238–45.
26. Charles RP, Iezza G, Amendola E, Dankort D, McMahon M.
Mutationally activated BRAF(V600E) elicits papillary thyroid
cancer in the adult mouse. Cancer Res. 2011;71:3863–71.
27. Park SY, Park YJ, Lee YJ, Lee HS, Choi SH, Choe G, et al.
Analysis of differential BRAF(V600E) mutational status in
multifocal papillary thyroid carcinoma: evidence of independent
clonal origin in distinct tumor foci. Cancer. 2006;107:1831–8.
28. Giannini R, Ugolini C, Lupi C, Proietti A, Elisei R, Salvatore G,
et al. The heterogeneous distribution of BRAF mutation supports
the independent clonal origin of distinct tumor foci in multifocal
papillary thyroid carcinoma. J Clin Endocrinol Metab.
2007;92:3511–6.
29. Jovanovic L, Delahunt B, McIver B, Eberhardt NL, Grebe SK.
Most multifocal papillary thyroid carcinomas acquire genetic and
morphotype diversity through subclonal evolution following the
intra-glandular spread of the initial neoplastic clone. J Pathol.
2008;215:145–54.
30. Vasko V, Hu S, Wu G, Xing JC, Larin A, Savchenko V, et al.
High prevalence and possible de novo formation of BRAF
mutation in metastasized papillary thyroid cancer in lymph nodes.
J Clin Endocrinol Metab. 2005;90:5265–9.
31. Xing M. BRAFV600E mutation and papillary thyroid cancer:
chicken or egg? J Clin Endocrinol Metab. 2012;97:2295–8.
32. Aparicio S, Caldas C. The implications of clonal genome evo-
lution for cancer medicine. N Engl J Med. 2013;368:842-51.
33. Guerra A, Sapio MR, Marotta V, Campanile E, Rossi S, Forno I,
et al. The primary occurrence of BRAF(V600E) is a rare clonal
event in papillary thyroid carcinoma. J Clin Endocrinol Metab.
2012;97:517–24.
34. Howell GM, Nikiforova MN, Carty SE, Armstrong MJ, Hodak
SP, Stang M T, et al. BRAF V600E mutation independently
predicts central compartment lymph node metastasis in patients
with papillary thyroid cancer. Ann Surg Oncol. 2013;20:47–52.
35. Marusyk A, Polyak K. Tumor heterogeneity: causes and conse-
quences. Biochim Biophys Acta. 2010;1805:105–17.
36. Hatzivassiliou G, Song K, Yen I, Brandhuber BJ, Anderson DJ,
Alvarado R, et al. RAF inhibitors prime wild-type RAF to activate
the MAPK pathway and enhance growth. Nature. 2010;464:431–5.
37. Nikiforova MN, Wald AI, Roy S, Durso MB, Nikiforov YE.
Targeted next-generation sequencing panel (ThyroSeq) for
detection of mutations in thyroid cancer. J Clin Endocrinol
Metab. 2013;98:E1852–60.
S.-P. Cheng et al.